OPPE and Hospital Performance Evaluation
|
|
|
- Rudolph Sanders
- 6 years ago
- Views:
Transcription
1 OPPE and Hospital Performance Evaluation 2012 Midas+ User Symposium Gary O. Goldsmith, MD Mount Auburn Hospital Cambridge, Massachusetts
2 Handout Note This handout only includes selected slides It is anticipated that ideas, insights and additional material will develop in the course of the workshop
3 Introduction Goals Format Outline Questions


4 Q&S Graphic Novel Software: Snagit (

5 Where are you with OPPE? 1. Newbies 2. Early 3. Middle 4. Good shape 5. Experts


6 Mount Auburn Hospital Harvard Teaching Hospital Community-oriented ~200 beds ~1000 medical staff Q&S CPOE Meditech AQC Blue Cross Medicare Pioneer ACO


7 Variation Common theme Practice styles Hospital involvement
8 Software Meditech MIDAS+ Statit rl Solutions
9 Quality & Safety Susan Abookire, Director Andrew Gardner, Data Manager 3 data analysts
10 Boston Medicine

11 Gorillas Tertiary Partners (Mass General/Brigham & Women s) Beth Israel Deaconess Tufts Medical Center Boston Medical Center For profit Steward Health Care System

12 Mt. Auburn Hospital Catchment Area

13 Fewer beds

14 Higher occupancy

15 Community vs. Teaching

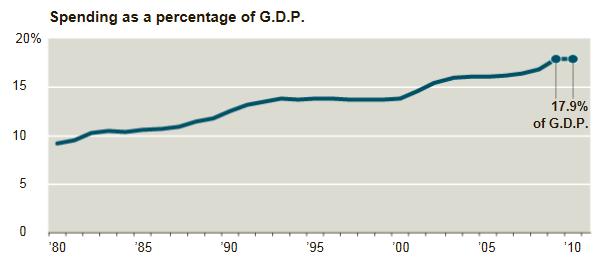
16 Health Care Costs 16

17 Uninsured Patients 1.8%

18 Health Reform Higher Costs
19 Challenges Financial Competitive Morale Reporting Quality Yours
20 The Ecology of OPPE Musings about OPPE and its environment Things you know about healthcare costs The sudden healthcare crisis Outliers/means, improvement/risk Where data people (us) fit in Accountable Care Organizations
21 Increasing costs
22 but
23 slowing? In Hopeful Sign, Health Spending Is Flattening Out NYTimes 4/28/12 Much of the slowdown is because of the recession but some of it to changing behavior by consumers and providers of health care. In 2009 and 2010, total nationwide health care spending grew less than 4 percent per year, the slowest annual pace in more than five decades. CMS Experts were surprised at a drop in spending on some hospitalized seniors people enrolled in Medicare, whose coverage the recession should not affect. If the growth in Medicare were to come down to a rate of only 1 percentage point a year faster than the economy s growth, the projected long-term deficit would fall by more than one-third.
24 Compared to

25 Where does $ go?
26 Maxims Beware the man with a simple solution to a complex problem. He s not always wrong, but rarely entirely right. Good quality is a side effect of good care and good care is a side effect of good quality. Identify the outliers, move the mean.
27 Risk/Improvement Improvement How much? How many? Other Risk Likelihood Severity Detection Other

28 ACO (Accountable Care Organization)
29 Limits other options

30 Here s Mount Auburn
31 CMS Innovation Center Accountable Care Organization (ACO) Medicare Shared Savings Program Advanced Payment Initiative Comprehensive Primary Care Initiative Bundled Payments for Care Improvement Initiative to Reduce Avoidable Hospitalizations Community Based Care Transition Independence at Home Demonstration
32 Coming soon to a hospital near you Independence at Home Demonstration 1) Delaware 2) Florida 3) Georgia 4) Kentucky 5) Massachusetts 6) Michigan 7) New York 8) North Carolina 9) Ohio 10) Oregon 11) Texas 12) Wisconsin
33 ACO 18 States 1) Arizona 2) California 3) Colorado 4) Florida 5) Illinois 6) Indiana 7) Iowa 8) Maine 9) Massachusetts 10) Michigan 11) Minnesota 12) Nevada 13) New Mexico 14) New York 15) Pennsylvania 16) Texas 17) Vermont 18) Wisconsin
34 What is an ACO? Group of doctors, hospitals, providers Group practice IPA Partnerships Hospitals Health centers
35 Five in Boston Pioneer Medicare ACO Atrius Health Beth Israel (BIDPO) MACIPA Partners Healthcare Steward Health Care Medical group practice Network of IPAs IPA Integrated delivery system Integrated delivery system
36 ACO: CMS Goals High quality Coordinated care Reduced costs Risk-sharing/Savings-sharing Medical Home model
37 A Glimpse of the Future Population-based payment Paradox: population management only succeeds by intense focus on the individual Significant outpatient focus Fee for service Medicare HIT focus: >50% PCPs MU certified EHR Robust quality measures 33 Measures Medicare Shared Savings Program
38 33 measures in 4 Quality Domains Care coordination/patient safety (6) Preventive health (8) At-risk populations: Diabetes (6) Hypertension (1) Ischemic Vascular Disease (2) Heart Failure (1) Coronary Artery Disease (2) Patient/caregiver experience (7)
39 Care coordination/patient safety 1. Risk-Standardized, All Condition Readmission 2. COPD or Asthma in Older Adults (AHRQ PQI #5) 3. Congestive Heart Failure (AHRQ PQI #8 ) 4. % PCP Qualify for EHR Incentive Payment 5. Medication Reconciliation After Inpatient D/C 6. Falls: Screening for Fall Risk
40 Preventive health 1. Influenza Immunization 2. Pneumococcal Vaccination 3. Adult Weight Screening and Follow-up 4. Tobacco Use Assessment/Cessation Intervention 5. Depression Screening 6. Colorectal Cancer Screening 7. Mammography Screening 8. Screening for High Blood Pressure
41 At-risk Populations 1. Hemoglobin A1c Control (<8 percent) 2. Low Density Lipoprotein (<100) 3. Blood Pressure <140/90 4. Tobacco Non Use 5. Aspirin Use 6. Hemoglobin A1c Poor Control (>9 percent) 7. Controlling High Blood Pressure 8. Complete Lipid Panel and LDL Control (<100 mg/dl) 9. Use of Aspirin or Another Antithrombotic 10. Beta-Blocker Therapy for (LVSD) 11. Drug Therapy for Lowering LDL-Cholesterol 12. ACE Inhibitor or ARB Therapy
42 Patient/caregiver experience 1. Timely Care, Appointments, and Information 2. How Well Your Doctors Communicate 3. Patients Rating of Doctor 4. Access to Specialists 5. Health Promotion and Education 6. Shared Decision Making 7. Health Status/Functional Status CAHPS -
43 Perception Reality OPPE depends on how you look at it The view from other perspectives Think like an anthropologist Others perceptions of OPPE Not mission-critical Make-work Only important to administration
44 Stakeholders in OPPE? Informaticists Hospitals Physicians Regulators???

45 Strategies Strong support Physician champion Powerful committee Q&S department CEO OPPE Aikido Defend yourself Redirect force Protect your attacker
46 OPPE Aikido Become an ally Bearer of bad news Help to make it better Help solve problems Educate Work together Put some control in their hands TJC did Indicators and timing: organized medical staff
47 Strategies: getting started Identify respected believers Mine what you re already doing Payers: CMS, Leapfrog Quality entities: NSQIP, STS (CT surgery) Regulators: State, Federal Public reporting: CMS, BCBS Get their input What do they do? The Rolling Stones
48 Strategies: Easy Hard Easy Procedure-based (events) Hard Surgery GI Pulmonary Medicine ( cognitive ) (processes) Consults Time-based Revisits, follow up
49 Strategies Take an active role Build an indicator Revise Repeat
50 Meetings: Chairman s day 5: :30 7:00 Wake up Desk work Med Exec Committee Patients Dept planning meeting Patients Charts, dictation Meet with problem physician Prepare presentation PTA meeting
51 Meetings Anthropologist You: commonalities, DB one-to-many Them: unique, intrusive, questionable value One on one Repetitive Be patient, but persistent


52 Usual first meeting 5 min late 10 min explain OPPE 15 min busy work bureaucratic intrusion useless waste of time duplication of effort administrative boondoggle 15 min lack of time inadequate resources no support staff administrative demands other responsibilities 15 min work
53 Anthropologist: doctors Competitive Strive for excellence Do the best for their patients Data- and detail-oriented; skeptical Defined/restricted by their work Chronically stressed Fearful of litigation Usual range of personalities

54 Kubler-Ross Denial Anger Bargaining Depression Acceptance
55 Loss of control Medicine: struggle for control over biology, behavior, environment Incomplete knowledge, limited technology Do an inherently imperfect job perfectly Personalities Past: practice medicine, solve problems Now: quality, efficiency, regulation, being watched intertwined with clinical activity Patients
56 Being heard People have to feel they have been heard Each person was given two ears and one tongue, so that we may listen more than speak. Rabbi Kerry M. Olitzky and Lori Forman, Sacred Intentions Native Americans Talking Stick - give the person holding it the honor of speaking while all the others have the duty to listen. One of the most common complaints they don t feel heard. Douglas Stone, Bruce Patton, and Sheila Heen, Difficult Conversations: How to Discuss What Matters Most Understanding what someone is saying doesn t mean that you agree with him. Whether you agree is not the issue in the listening process. Center for Conflict Resolution
57 Meetings: Strategies Big goal: not to win, but to complete task Immediate goal: indicators, leave You can t succeed by fighting with people Be flexible Don t debate every detail Acknowledge when they re right Hmm. There s some truth in that. We should work on it.
58 Meetings: Strategies Explain Handouts, references Teach Practical Reframe the task We have to do this Useful to chiefs/chairs, departments, doctors Do you want to be their IS department?
59 Meetings: Strategies Have a practical starting place Choices, suggestions Henry s list Datavision Internet Friends, associates
60 Meetings: Strategies Create ownership/control Involved in the process If we don t do this, someone else will Relevant measures, not arbitrary requirements What makes sense to them? If reject, redirect Examples: Other departments did X,Y,Z Suggest resources Colleagues Other institutions Professional organizations
61 Meetings: Strategies Anticipate problems Variation Practice styles and affiliations Solo/Group Coverage Defined populations/open to all Prepaid/FFS Clinical practice Own patients/hospitalists Hospital relationships Admit/refer Low volume
62 Meetings: Strategies Seduce them with data Have something to present Volumes, a few measures Teachable moments Aha! Moments Follow up Summarize Next steps Set timetables Write up your notes,
63 Specifics:TJC What does TJC do? Creates standards OPPE goals Identify problems Timely resolution
64 Specifics: What do you need? A defined process Who reviews performance data How often will it be reviewed How will it be used (re: privileges) How are data incorporated into credentials file Approved Criteria Organized Medical Staff Documentation A plan Referenced by bylaws/governing documents
65 Specifics: FPPE My opinion: TJC unclear re: purpose, focus Granting privileges New staff Additional privileges Problems Previously Focused Review
66 Specifics: OPPE Maintaining privileges TJC Six competencies (suggested, not required) Identify and resolve problems Ongoing Every 6 months? 8 months? Is more often better? Diminishing returns Much of data is quarterly or semi-annual Perhaps identify a few for dashboard
67 What is your role? Gather data Convert data to information
68 Commercial Product Rollout Identify customers/clients/users Customer feedback during development Adequate resources Clear objectives Right process Position your product Give them what they need Find motivated people/early adopters Leverage past success From various sources
69 Who? decides what data to use? Organized medical staff Departments gathers, organizes and presents data? You sees and reviews data? Chair/chief, CMO, QA, MEC, Cred Comm Whole department? Individual physicians? If not, should they? When?
70 When? 6 vs 8 months Enough time to evaluate How much time to prepare, distribute? Maintenance, repetition
71 Where? Actions re: privileges must be documented Where stored? No requirement that it be stored continuously in credentials file. <source?> Simple: who, what, when reviewed and results Credential files Separate peer-review-protected folder
72 How? Simple/Complex Manual Hardware/software Process Iterative, agile
73 What? -1 Clinical Medical record Chart review Direct observation Discussion with others Consultants, surg assistants, nurses, admin M&M conferences Infection rates Guideline compliance CME participation
74 What? - 2 Quality Outcomes Incidents Complaints Peer reviews Rule violations Patients Complaints, complements Surveys
75 What? - 3 Volume Procedure performed in past two years? Regular procedures Emergency procedures Simulations? Layered approach General: Everyone (may vary between depts.) Specialty-specific: everyone Specialty-specific: subsets Specific departments
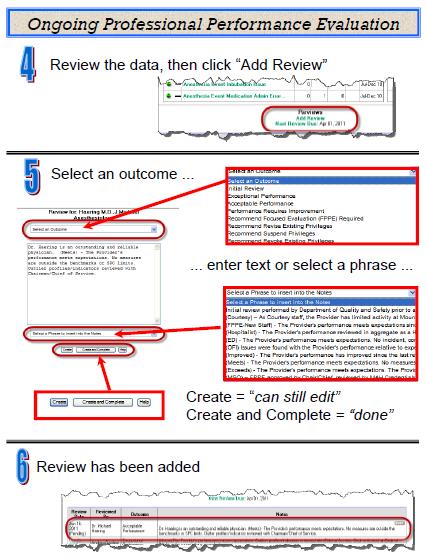
76 What? - 4 Review options OFI CME/training/proctoring/mentoring/suspension Meets expectations No issues, doing well, meetings, teaching, call Exceeds expectations OR times/los/outcomes/patient satisfaction Positive as well as negative Share gains/wins
77 Challenges -1 Technical issues clean data Maintenance time/resource commitment Midlevels CNM/CRNA/PA/NP TJC: equivalent to medical staff process Intensity: Inpatient higher; Outpatient lower
78 Challenges - 2 Zero data is, in fact, data Low/No-volume providers Increasing trend Retired/part-time Surgeons mostly in surgicenters Options Hospitals may use peer recommendations when there is insufficient peer review data to assess a practitioner s competence. Refer and Follow MS , EP2
79 Challenges 3 What kind of institution are you? No EMR non-discrete data What if everyone passes a measure? Risk adjustment Benchmarks Attribution Skeptics Cookbook medicine Your list


80 Thank you
81 CMS Innovation Center Some references Accountable Care Organizations Summary and Analysis of the Final Rule: Summary.pdf ACO 2012 Program Analysis Service-Payment/sharedsavingsprogram/ downloads//aco_qualitymeasures.pdf
82 Some references TJC Standards BoosterPak for FPPE/OPPE /downloads/boosterpak_fppe_oppe_final. pdf Navigating TJC OPPE Requirements asqqps7_info.shtml
83 Some references Top Ten Barriers to Dispute Resolution TopTenBarriers.html Listening A Tool for Resolving Conflict
84 OPPE and Hospital Performance Evaluation 2012 Midas+ User Symposium Gary O. Goldsmith, MD Mount Auburn Hospital Cambridge, Massachusetts
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
ACO Information Required to be Published on ACO Website per CMS Regulations
 ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Quality Measurement, Population Health and Payment Reform
 Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
3/29/2013. Effective ACO Compliance. Objectives THE HEALTH CARE DILEMMA: ARE ACOS THE ANSWER? HCCA Compliance Institute April 21, 2013
 Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Shared Savings Program ACO Public Reporting Instructions. with Pre-Populated Template
 Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Holding the Line: How Massachusetts Physicians Are Containing Costs
 Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
Shared Savings Program ACO Public Report
 ACO ame and Location Shared Savings Program ACO Public Report University of Health Alliance Accountable Care Organization, LLC 1227 E. Rusholme Street Davenport, 52803 ACO Primary Contact Primary Contact
ACO ame and Location Shared Savings Program ACO Public Report University of Health Alliance Accountable Care Organization, LLC 1227 E. Rusholme Street Davenport, 52803 ACO Primary Contact Primary Contact
Meaningful Use: a Primer
 Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Slide 1. Slide 2 Rural Princeton. Slide 3 Agenda Rural ACO RURAL ACOS CAN WORK AND LEAD THE WAY
 Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
=======================================================================
 ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
Top Reasons to Become an AmeriHealth Caritas Virginia Provider. amerihealthcaritas.com
 Top Reasons to Become an AmeriHealth Caritas Virginia Provider amerihealthcaritas.com WHO WE ARE About AmeriHealth Caritas AmeriHealth Caritas Family of Companies ( AmeriHealth Caritas ) is a national
Top Reasons to Become an AmeriHealth Caritas Virginia Provider amerihealthcaritas.com WHO WE ARE About AmeriHealth Caritas AmeriHealth Caritas Family of Companies ( AmeriHealth Caritas ) is a national
Improving Clinical Outcomes
 Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Shared Savings Program ACO Public Reporting Instructions. with Pre-Populated Template
 Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Restructuring Healthcare The Role of Technology
 Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO ame and Location Illinois Health Partners ACO, LLC 1100 West 31st Street Suite 300 Downers Grove, Illinois 60515 ACO Primary Contact Primary Contact ame Teri Kaneski Primary Contact Phone umber 630-527-3055
ACO ame and Location Illinois Health Partners ACO, LLC 1100 West 31st Street Suite 300 Downers Grove, Illinois 60515 ACO Primary Contact Primary Contact ame Teri Kaneski Primary Contact Phone umber 630-527-3055
MBQIP Quality Measure Trends, Data Summary Report #20 November 2016
 MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
Framing Rural Health Value Webinar Series
 600 East Superior Street, Suite 404 I Duluth, MN 55802 I Ph. 800.997.6685 or 218.727.9390 I www.ruralcenter.org Framing Rural Health Value Webinar Series Data Measurement, Outcomes and Impact Kami Norland
600 East Superior Street, Suite 404 I Duluth, MN 55802 I Ph. 800.997.6685 or 218.727.9390 I www.ruralcenter.org Framing Rural Health Value Webinar Series Data Measurement, Outcomes and Impact Kami Norland
Critical Access Hospitals and HCAHPS
 Critical Access Hospitals and HCAHPS Michelle Casey, MS Senior Research Fellow and Deputy Director University of Minnesota Rural Health Research Center June 12, 2012 Overview of Presentation Why is HCAHPS
Critical Access Hospitals and HCAHPS Michelle Casey, MS Senior Research Fellow and Deputy Director University of Minnesota Rural Health Research Center June 12, 2012 Overview of Presentation Why is HCAHPS
Maximizing the Financial Performance of Employed Physicians
 Maximizing the Financial Performance of Employed Physicians Presented by: Health Directions, LLC Sabrina Burnett, Vice President HFMA Kentucky Chapter Summer Institute, July 24, 2014 About Health Directions,
Maximizing the Financial Performance of Employed Physicians Presented by: Health Directions, LLC Sabrina Burnett, Vice President HFMA Kentucky Chapter Summer Institute, July 24, 2014 About Health Directions,
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations
 Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO Name and Location Physician Quality Partners, LLC 1505 Doctors Circle Building B Wilmington, North Carolina 28401 ACO Primary Contact Primary Contact Name Lydia Newman, MPP Primary Contact Phone Number
ACO Name and Location Physician Quality Partners, LLC 1505 Doctors Circle Building B Wilmington, North Carolina 28401 ACO Primary Contact Primary Contact Name Lydia Newman, MPP Primary Contact Phone Number
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Note: Accredited is the highest rating an exchange product can have for 2015.
 Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
ACO Name and Location ACO Primary Contact
 ACO ame and Location Chrysalis Medical Services, LLC 4888 Loop Central Drive Suite 700 Houston, Texas 77081 ACO Primary Contact Primary Contact ame Adrienne Opalka Primary Contact Phone umber 914-281-0827
ACO ame and Location Chrysalis Medical Services, LLC 4888 Loop Central Drive Suite 700 Houston, Texas 77081 ACO Primary Contact Primary Contact ame Adrienne Opalka Primary Contact Phone umber 914-281-0827
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Pioneer Accountable Care Organization Model: General Fact Sheet May 22, 2012
 Pioneer Accountable Care Organization Model: General Fact Sheet May 22, 2012 The Pioneer ACO Model is a CMS Innovation Center initiative designed to support organizations with experience operating as Accountable
Pioneer Accountable Care Organization Model: General Fact Sheet May 22, 2012 The Pioneer ACO Model is a CMS Innovation Center initiative designed to support organizations with experience operating as Accountable
Medicare Physician Group Practice Demonstration
 Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY
 A CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY Introduction... 2 Surgical Procedures/Medical Conditions... 2 Patient Outcomes... 2 Patient Outcomes Quality Indexes... 3 Patient Outcomes
A CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY Introduction... 2 Surgical Procedures/Medical Conditions... 2 Patient Outcomes... 2 Patient Outcomes Quality Indexes... 3 Patient Outcomes
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
2015 State Hospice Report 2013 Medicare Information 1/1/15
 2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
Elizabeth Mitchell December 1, Transforming Healthcare in an Uncertain Environment
 Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Current Medicare Advantage Enrollment Penetration: State and County-Level Tabulations
 Current Advantage Enrollment : State and County-Level Tabulations 5 Slide Series, Volume 40 September 2016 Summary of Tabulations and Findings As of September 2016, 17.9 million of the nation s 56.1 million
Current Advantage Enrollment : State and County-Level Tabulations 5 Slide Series, Volume 40 September 2016 Summary of Tabulations and Findings As of September 2016, 17.9 million of the nation s 56.1 million
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
ACO GPRO 2016 Ready to Report Basics GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017
 ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
 3+ 3+ N = 155, 442 3+ R 2 =.32 < < < 3+ N = 149, 685 3+ R 2 =.27 < < < 3+ N = 99, 752 3+ R 2 =.4 < < < 3+ N = 98, 887 3+ R 2 =.6 < < < 3+ N = 52, 624 3+ R 2 =.28 < < < 3+ N = 36, 281 3+ R 2 =.5 < < < 7+
3+ 3+ N = 155, 442 3+ R 2 =.32 < < < 3+ N = 149, 685 3+ R 2 =.27 < < < 3+ N = 99, 752 3+ R 2 =.4 < < < 3+ N = 98, 887 3+ R 2 =.6 < < < 3+ N = 52, 624 3+ R 2 =.28 < < < 3+ N = 36, 281 3+ R 2 =.5 < < < 7+
CRITICAL ACCESS HOSPITAL NETWORK OF EASTERN WASHINGTON
 CRITICAL ACCESS HOSPITAL NETWORK OF EASTERN WASHINGTON Applying Health Information Technology to Impact Rural Population Health Sue Deitz, MPH February 9, 2015 Please note that the views expressed by the
CRITICAL ACCESS HOSPITAL NETWORK OF EASTERN WASHINGTON Applying Health Information Technology to Impact Rural Population Health Sue Deitz, MPH February 9, 2015 Please note that the views expressed by the
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
ACO Update. LVHN Scholarly Works. Lehigh Valley Health Network. Lehigh Valley Health Network. Spring 2017
 Lehigh Valley Health Network LVHN Scholarly Works ACO Update Newsletters Spring 2017 ACO Update Lehigh Valley Health Network Follow this and additional works at: https://scholarlyworks.lvhn.org/acoupdate
Lehigh Valley Health Network LVHN Scholarly Works ACO Update Newsletters Spring 2017 ACO Update Lehigh Valley Health Network Follow this and additional works at: https://scholarlyworks.lvhn.org/acoupdate
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
Percent of Population Under Age 65 Uninsured, 2013, 2014, and 2015
 Exhiit 1 Percent of Population Under Age 65 Uninsured, 13, 14, and 15 13 14 15
Exhiit 1 Percent of Population Under Age 65 Uninsured, 13, 14, and 15 13 14 15
Anthem BlueCross and BlueShield HMO
 Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
Medicare & Medicaid. William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA
 Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
MACRA and MIPS. How Medicare Meaningful Use and PQRS are Changing
 MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016
 BACKGROUND HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016 Federal legislation (42 CFR 484.36) requires that Medicare-certified home health agencies employ home health aides who are trained and evaluated
BACKGROUND HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016 Federal legislation (42 CFR 484.36) requires that Medicare-certified home health agencies employ home health aides who are trained and evaluated
Meaningful Use Is a Stepping Stone to Meaningful Care
 Meaningful Use Is a Stepping Stone to Meaningful Care Liz Johnson, RN-BC, MS, FCHIME, FHIMSS, CPHIMS Chief Clinical Informaticist and Vice President of Applied Clinical Informatics Tenet Healthcare Corporation
Meaningful Use Is a Stepping Stone to Meaningful Care Liz Johnson, RN-BC, MS, FCHIME, FHIMSS, CPHIMS Chief Clinical Informaticist and Vice President of Applied Clinical Informatics Tenet Healthcare Corporation
TABLE 3c: Congressional Districts with Number and Percent of Hispanics* Living in Hard-to-Count (HTC) Census Tracts**
 Census Tracts**") living Alaska 00 47,808 21,213 44.4 Alabama 01 20,661 3,288 15.9 Alabama 02 23,949 6,614 27.6 Alabama 03 20,225 3,247 16.1 Alabama 04 41,412 7,933 19.2 Alabama 05 34,388 11,863 34.5 Alabama 06 34,849 4,074
living Alaska 00 47,808 21,213 44.4 Alabama 01 20,661 3,288 15.9 Alabama 02 23,949 6,614 27.6 Alabama 03 20,225 3,247 16.1 Alabama 04 41,412 7,933 19.2 Alabama 05 34,388 11,863 34.5 Alabama 06 34,849 4,074
Ambulatory Surgical Centers in Florida
 Ambulatory Surgical Centers in Florida A Presentation to the Commission on Healthcare and Hospital Funding David Shapiro, MD, CASC, CHCQM, CHC, CPHRM, LHRM Definitions Ambulatory Surgery Centers (ASCs)
Ambulatory Surgical Centers in Florida A Presentation to the Commission on Healthcare and Hospital Funding David Shapiro, MD, CASC, CHCQM, CHC, CPHRM, LHRM Definitions Ambulatory Surgery Centers (ASCs)
TABLE 3b: Congressional Districts Ranked by Percent of Hispanics* Living in Hard-to- Count (HTC) Census Tracts**
 Census Tracts**") Rank State District Count (HTC) 1 New York 05 150,499 141,567 94.1 2 New York 08 133,453 109,629 82.1 3 Massachusetts 07 158,518 120,827 76.2 4 Michigan 13 47,921 36,145 75.4 5 Illinois 04 508,677 379,527
Rank State District Count (HTC) 1 New York 05 150,499 141,567 94.1 2 New York 08 133,453 109,629 82.1 3 Massachusetts 07 158,518 120,827 76.2 4 Michigan 13 47,921 36,145 75.4 5 Illinois 04 508,677 379,527
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Aggregating Physician Performance Data Across Health Plans
 Aggregating Physician Performance Data Across Health Plans March 2011 A project funded by The Robert Wood Johnson Foundation Measures Included in The Pilot: 1. Breast cancer screening 2. Colorectal cancer
Aggregating Physician Performance Data Across Health Plans March 2011 A project funded by The Robert Wood Johnson Foundation Measures Included in The Pilot: 1. Breast cancer screening 2. Colorectal cancer
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Evaluation of Pharmacy Delivery Models
 Evaluation of Pharmacy Delivery Models As Required By House Bill 1, 84th Legislature, Regular Session, 2015 (Article II, Health and Human Services Commission, Rider 83) Health and Human Services Commission
Evaluation of Pharmacy Delivery Models As Required By House Bill 1, 84th Legislature, Regular Session, 2015 (Article II, Health and Human Services Commission, Rider 83) Health and Human Services Commission
Statutory change to name availability standard. Jurisdiction. Date: April 8, [Statutory change to name availability standard] [April 8, 2015]
![Statutory change to name availability standard. Jurisdiction. Date: April 8, [Statutory change to name availability standard] [April 8, 2015]](/thumbs/83/87461560.jpg "Statutory change to name availability standard. Jurisdiction. Date: April 8, [Statutory change to name availability standard] [April 8, 2015]") Topic: Question by: : Statutory change to name availability standard Michael Powell Texas Date: April 8, 2015 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Connecticut
Topic: Question by: : Statutory change to name availability standard Michael Powell Texas Date: April 8, 2015 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Connecticut
Design for Nursing Home Compare 5-Star Rating System: Users Guide
 Design for Nursing Home Compare 5-Star Rating System: Users Guide December 2008 Contents Introduction...1 Methodology...3 Survey Domain...3 Scoring Rules...3 Rating Methodology...4 Staffing Domain...5
Design for Nursing Home Compare 5-Star Rating System: Users Guide December 2008 Contents Introduction...1 Methodology...3 Survey Domain...3 Scoring Rules...3 Rating Methodology...4 Staffing Domain...5
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Table of Contents. Bellin Health Lessons from a Successful Medicare Pioneer ACO
 Bellin Health Lessons from a Successful Medicare Pioneer ACO March 31, 2016 Table of Contents I. We Are Doing Some Good Things Rating Agency Actions II. Who We Are Bellin Health s Platform Organizational
Bellin Health Lessons from a Successful Medicare Pioneer ACO March 31, 2016 Table of Contents I. We Are Doing Some Good Things Rating Agency Actions II. Who We Are Bellin Health s Platform Organizational
Policy CHCS. Brief. Leveraging the Medicaid Primary Care Rate Increase: The Role of Performance Measurement. Center for Health Care Strategies, Inc.
 CHCS Center for Health Care Strategies, Inc. Policy Brief Leveraging the Medicaid Primary Care Rate Increase: The Role of Performance Measurement By David Marc Small and Tricia McGinnis, Center for Health
CHCS Center for Health Care Strategies, Inc. Policy Brief Leveraging the Medicaid Primary Care Rate Increase: The Role of Performance Measurement By David Marc Small and Tricia McGinnis, Center for Health
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
Hospitals and Healthcare Reform: What Does The Affordable Care Act Mean for Facilities Big and Small?
 INFORM+INSPIRE Hospitals and Healthcare Reform: What Does The Affordable Care Act Mean for Facilities Big and Small? William D. Hayes, Ph.D. NCOIL Institute for Insurance Policy March 9, 2013 1 U.S. spending
INFORM+INSPIRE Hospitals and Healthcare Reform: What Does The Affordable Care Act Mean for Facilities Big and Small? William D. Hayes, Ph.D. NCOIL Institute for Insurance Policy March 9, 2013 1 U.S. spending
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
The long and winding road to Accountable Care
 The long and winding road to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute John E. Wennberg Distinguished Professor Geisel School of Medicine The long and winding road Past
The long and winding road to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute John E. Wennberg Distinguished Professor Geisel School of Medicine The long and winding road Past
Aiming Higher. A State Scorecard on Health System Performance. Joel C. Cantor and Dina Belloff
 Rutgers Center for State Health Policy Aiming Higher A State Scorecard on Health System Performance Joel C. Cantor and Dina Belloff Rutgers Center for State Health Policy Cathy Schoen, Sabrina K.H. How,
Rutgers Center for State Health Policy Aiming Higher A State Scorecard on Health System Performance Joel C. Cantor and Dina Belloff Rutgers Center for State Health Policy Cathy Schoen, Sabrina K.H. How,
Improving Care for Dual Eligibles through Health IT
 Los Angeles, October 31, 2012 Presentation Improving Care for Dual Eligibles through Health IT The National Dual Eligibles Summit Duals Market is sizable Medicare and Medicaid Populations Medicaid Total
Los Angeles, October 31, 2012 Presentation Improving Care for Dual Eligibles through Health IT The National Dual Eligibles Summit Duals Market is sizable Medicare and Medicaid Populations Medicaid Total
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
The American Legion NATIONAL MEMBERSHIP RECORD
 The American Legion NATIONAL MEMBERSHIP RECORD www.legion.org 2016 The American Legion NATIONAL MEMBERSHIP RECORD 1920-1929 Department 1920 1921 1922 1923 1924 1925 1926 1927 1928 1929 Alabama 4,474 3,246
The American Legion NATIONAL MEMBERSHIP RECORD www.legion.org 2016 The American Legion NATIONAL MEMBERSHIP RECORD 1920-1929 Department 1920 1921 1922 1923 1924 1925 1926 1927 1928 1929 Alabama 4,474 3,246
Use of Medicaid MCO Capitation by State Projections for 2016
 Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Anthem BlueCross and BlueShield
 Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Commercial HMO) Accredited Accreditation Commercial
Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Commercial HMO) Accredited Accreditation Commercial
Practices for Improving Population Health
 Practices for Improving Population Health February 13, 2014 1 Healthy Counties Initiative Sponsors 2 Webinar Recording and Evaluation Survey This webinar is being recorded and will be made available online
Practices for Improving Population Health February 13, 2014 1 Healthy Counties Initiative Sponsors 2 Webinar Recording and Evaluation Survey This webinar is being recorded and will be made available online
Improving Care for the Chronically Ill. Linda Magno Director, Medicare Demonstrations
 Improving Care for the Chronically Ill Linda Magno Director, Medicare Demonstrations Medicare Spending for Beneficiaries with Chronic Conditions The 20 percent of beneficiaries with 5+ chronic conditions
Improving Care for the Chronically Ill Linda Magno Director, Medicare Demonstrations Medicare Spending for Beneficiaries with Chronic Conditions The 20 percent of beneficiaries with 5+ chronic conditions
5 x 7 Notecards $1.50 with Envelopes - MOQ - 12
 5 x 7 Notecards $1.50 with Envelopes - MOQ - 12 Magnets 2½ 3½ Magnet $1.75 - MOQ - 5 - Add $0.25 for packaging Die Cut Acrylic Magnet $2.00 - MOQ - 24 - Add $0.25 for packaging 2535-22225 California AM-22225
5 x 7 Notecards $1.50 with Envelopes - MOQ - 12 Magnets 2½ 3½ Magnet $1.75 - MOQ - 5 - Add $0.25 for packaging Die Cut Acrylic Magnet $2.00 - MOQ - 24 - Add $0.25 for packaging 2535-22225 California AM-22225
ACO Name and Location. ACO Primary Contact. Organizational Information. Page 1 of 8
 ACO ame and Location Essential Care Partners, LLC 5900 Southwest Parkway Building 3 Austin, Texas 78735 ACO Primary Contact Primary Contact ame Jeff Spight Primary Contact Phone umber 914-597-2073 Primary
ACO ame and Location Essential Care Partners, LLC 5900 Southwest Parkway Building 3 Austin, Texas 78735 ACO Primary Contact Primary Contact ame Jeff Spight Primary Contact Phone umber 914-597-2073 Primary
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
A Clinically Integrated Network. R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015
 A Clinically Integrated Network R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015 HHS has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to
A Clinically Integrated Network R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015 HHS has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to
FINANCING BRIEF. Implementation of Health Reform for Children s Mental Health HEALTH REFORM PROVISIONS EXPLORED
 FINANCING BRIEF Implementation of Health Reform for Children s Mental Health Beth A. Stroul, M.Ed. Jonathan Safer-Lichtenstein, B.S. Linda Henderson-Smith, Ph.D., LPC Lan Le, M.P.A. MAY 2015 The National
FINANCING BRIEF Implementation of Health Reform for Children s Mental Health Beth A. Stroul, M.Ed. Jonathan Safer-Lichtenstein, B.S. Linda Henderson-Smith, Ph.D., LPC Lan Le, M.P.A. MAY 2015 The National
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
Issue Brief February 2015 Affordable Care Act Funding:
 CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2015 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010- The Patient Protection and Affordable
CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2015 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010- The Patient Protection and Affordable
Medicare & Medicaid EHR Incentive Program Final Rule. Implementing the American Recovery & Reinvestment Act of 2009
 Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Hospital Compare Quality Measures: 2008 National and Florida Results for Critical Access Hospitals
 Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
VOLUME 35 ISSUE 6 MARCH 2017
 VOLUME 35 ISSUE 6 MARCH 2017 IN THIS ISSUE Index of State Economic Momentum The Index of State Economic Momentum, developed by Reports founding editor Hal Hovey, ranks states based on their most recent
VOLUME 35 ISSUE 6 MARCH 2017 IN THIS ISSUE Index of State Economic Momentum The Index of State Economic Momentum, developed by Reports founding editor Hal Hovey, ranks states based on their most recent
The Significant Lack of Alignment Across State and Regional Health Measure Sets: An Analysis of 48 State and Regional Measure Sets, Presentation
 The Significant Lack of Alignment Across State and Regional Health Measure Sets: An Analysis of 48 State and Regional Measure Sets, Presentation Kate Reinhalter Bazinsky Michael Bailit September 10, 2013
The Significant Lack of Alignment Across State and Regional Health Measure Sets: An Analysis of 48 State and Regional Measure Sets, Presentation Kate Reinhalter Bazinsky Michael Bailit September 10, 2013
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Quality Incentive Programs. By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital
 Quality Incentive Programs By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital Housekeeping 1. Using the control panel - Use the control panel on the right side of your screen
Quality Incentive Programs By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital Housekeeping 1. Using the control panel - Use the control panel on the right side of your screen
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by February 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Alabama 3.7 33 Ohio 4.5 2 New Hampshire 2.6 19 Missouri 3.7 33 Rhode Island 4.5
States Ranked by February 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Alabama 3.7 33 Ohio 4.5 2 New Hampshire 2.6 19 Missouri 3.7 33 Rhode Island 4.5
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by November 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Indiana 4.4 37 Georgia 5.6 2 Nebraska 2.9 20 Ohio 4.5 37 Tennessee 5.6
States Ranked by November 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Indiana 4.4 37 Georgia 5.6 2 Nebraska 2.9 20 Ohio 4.5 37 Tennessee 5.6