5/5/2014. A National Best Practice Overview May Lauran Hardin MSN, RN CNL
|
|
|
- Hugo Lindsey
- 6 years ago
- Views:
Transcription

1 A National Best Practice Overview May 2014 Lauran Hardin MSN, RN CNL Disclosure Lauran Hardin I have no financial relationships with commercial interests with products or services relevant to today s presentation. I will not be discussing unapproved or investigational uses of products or devices. 1

2 The Situation Robert Wood Johnson Foundation reports 5% of the population uses nearly half of total healthcare spending ( topic areas/health policy/health carecosts/healthcarecostsfastfacts.html Recent analysis identifies High frequency Patients or Super Utilizers who they are is poorly understood Successful Population Health strategies include management of these high cost patients Shift in Payment Strategy Old Model=VOLUME New Model=VALUE Rewards Unit Cost (FFS) Minimal focus on care efficiency and patient centeredness Limited alignment with quality Care delivered based on preference Silos of Care Rewards for Volume Rewards health outcomes and population health (GPS) Focus on decreased cost and improved patient experience Alignment with quality & safety Consistent Evidence based practice Integrated networks of care Rewards for Value 4 2


3 Our Challenge The Burning Platform and Nobile Mission Young Man Complex Medical Disease Gastroparesis Substance Dependence In a PCMH High frequency: 10 ED visits, 8 IP admissions, 65 day LOS in 12 months Outcomes Trust and Engagement Shared Plan Cross Continuum Evidence Based Intervention Tools for patient, family and staff 2 ED, 2 Inpatient admissions 8 day LOS in 12 months 3

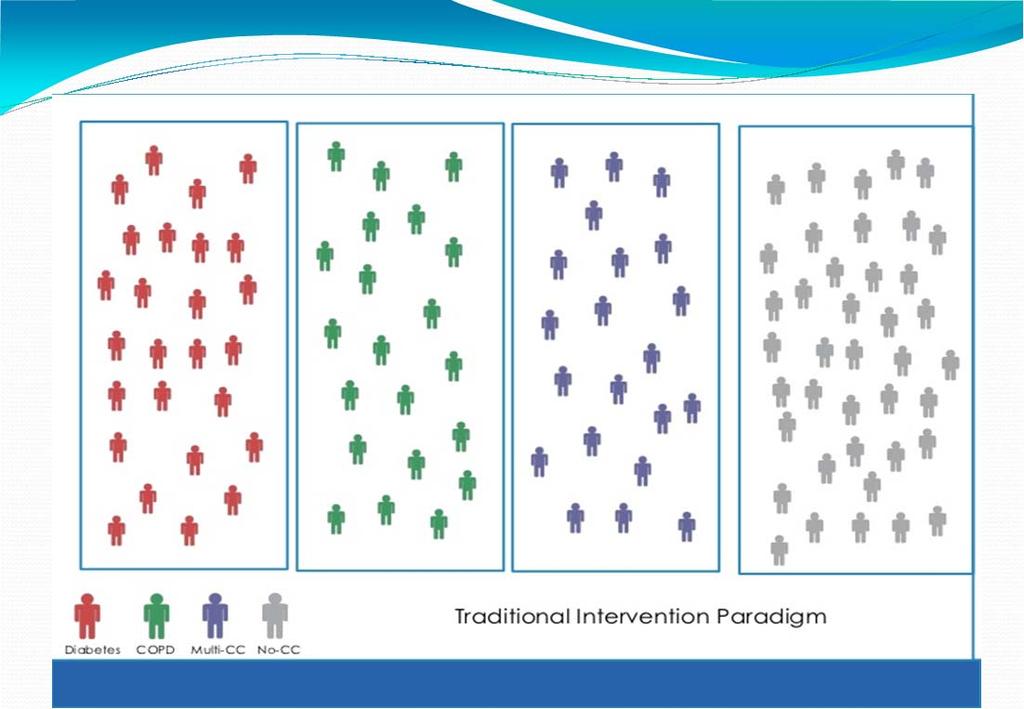
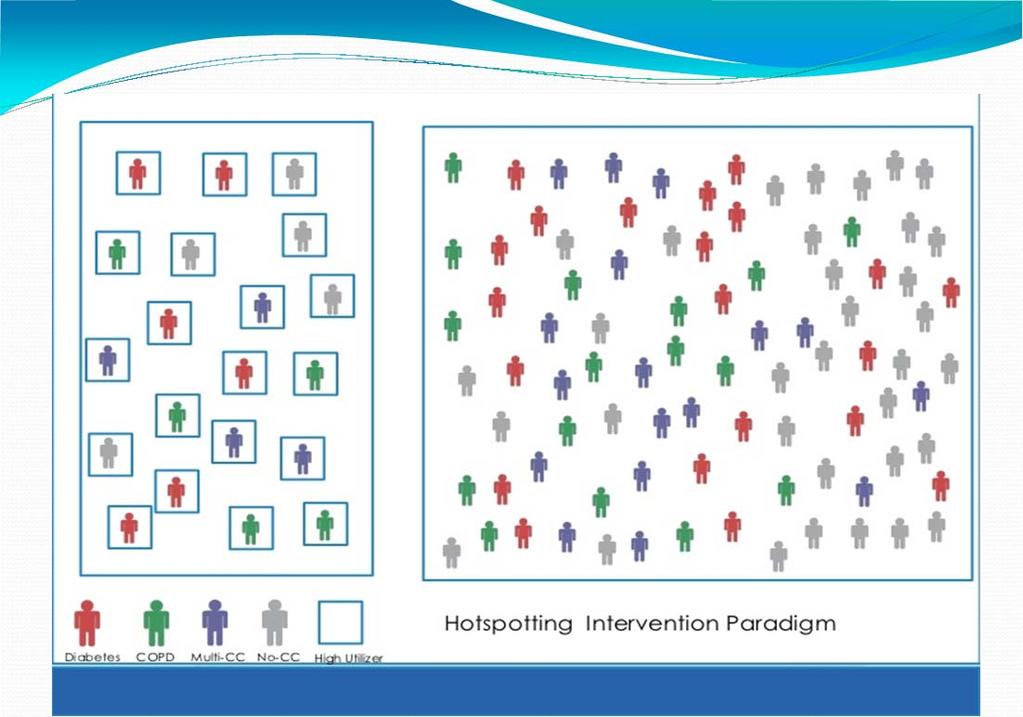
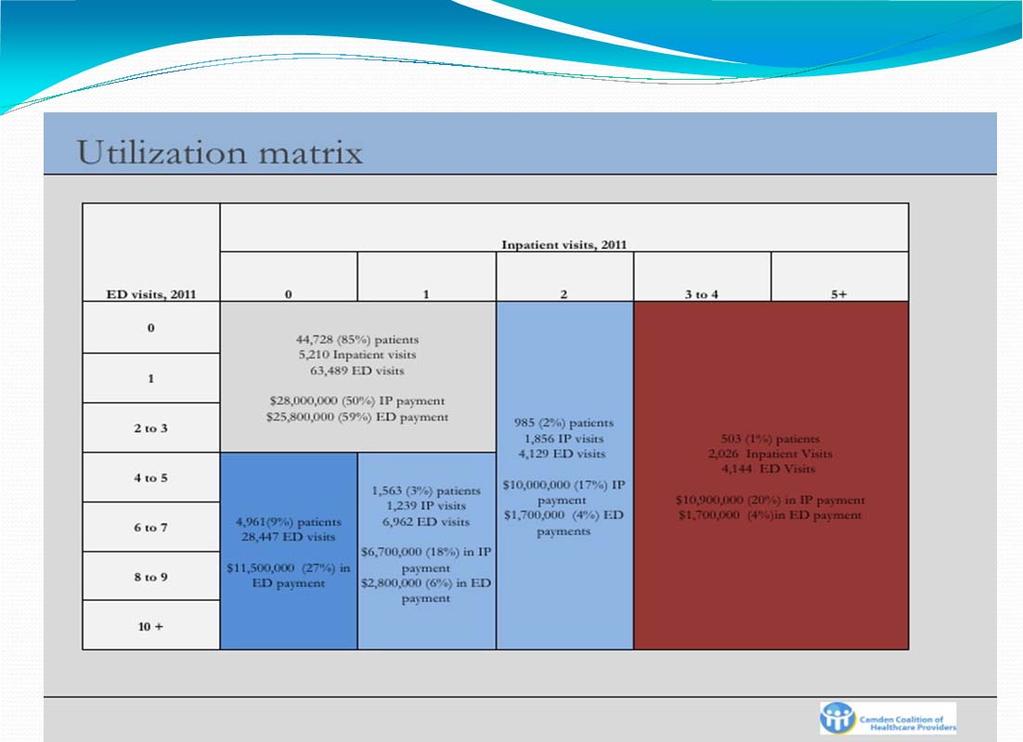
4 Who are the High Frequency Patients? Definition Dr. Jeffrey Brenner Executive Director/Medical Director, Camden Coalition of Healthcare Providers, MacArthur Genius Award Super Utilizer = Patients who accumulate large numbers of ED visits and hospital admissions which might have been prevented by relatively inexpensive early interventions and primary care. (Brenner, 2013; Mann, 2013 CMMS) 8 4


5 A Population View Source: Healthcare Risk Adjustment and Predictive Modeling by Ian Duncan 9 Risk Stratification Playbook for Population Health, The Advisory Board Company 5
6 6

7 What is root cause of high frequency access? 7



8 Patient with COPD and Kidney Disease with Insurance Transition Coordinator Pulmonology Equipment Company Dialysis Nurse Navigator PCMH/ Complex Care Mgr Hospital Homecare CM Insurance CM Patient with COPD and Diabetes and no Insurance: ED = PCP Community Agencies ED=PCP Equipment Company 8
9 Significant Root Cause Issues Psychiatric Illness Substance Use Disorder Alcohol, Prescription Drugs Homelessness Access Cultural Preference Domestic Violence/Abuse/Trauma Electronic Health Record Challenges System Competency Challenges 17 5/5/2014 Mental Health and Substance Use Disorder 8.9 Million persons have co occurring disorders Only 7.4 percent of individuals receive treatment for both conditions with 55.8 percent receiving no treatment at all. Untreated mental illness and substance use disorders lead to more deaths than traffic accidents, HIV/AIDS, and breast cancer combined Centers for Medicare and Medicaid Services (CMS) data show nearly one in four people with mental or substance use disorders lack health insurance. For those with both mental illness and substance use issues the figure is 30 percent 18 (SAMHSA retrieved January 7, 2014 from occurring/topics/data/disorders.aspx) 9

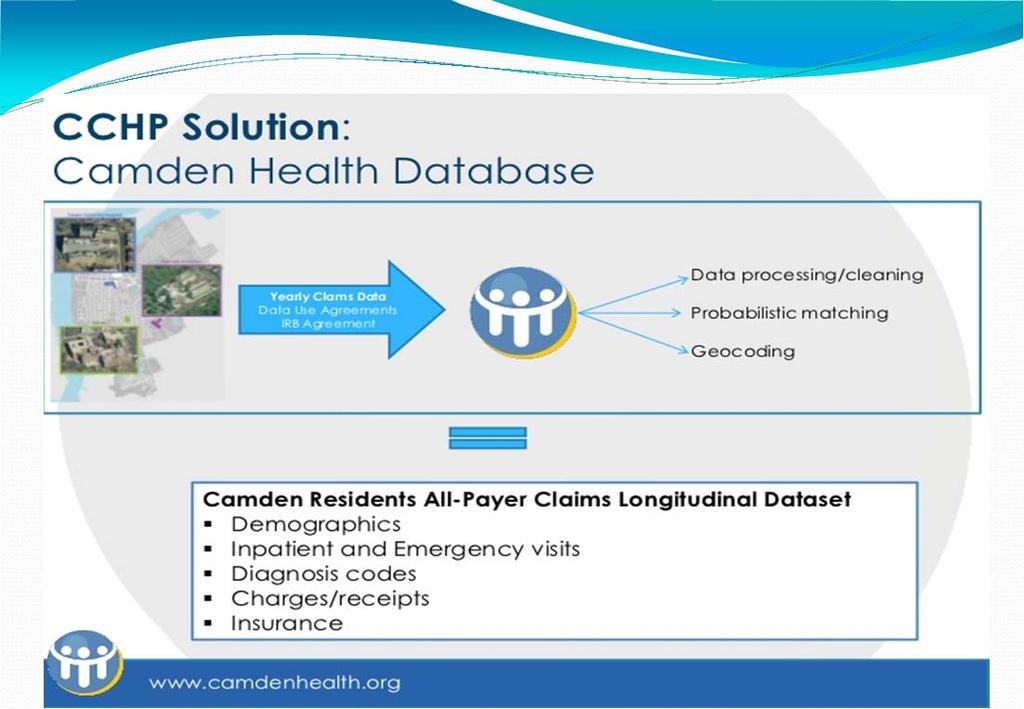
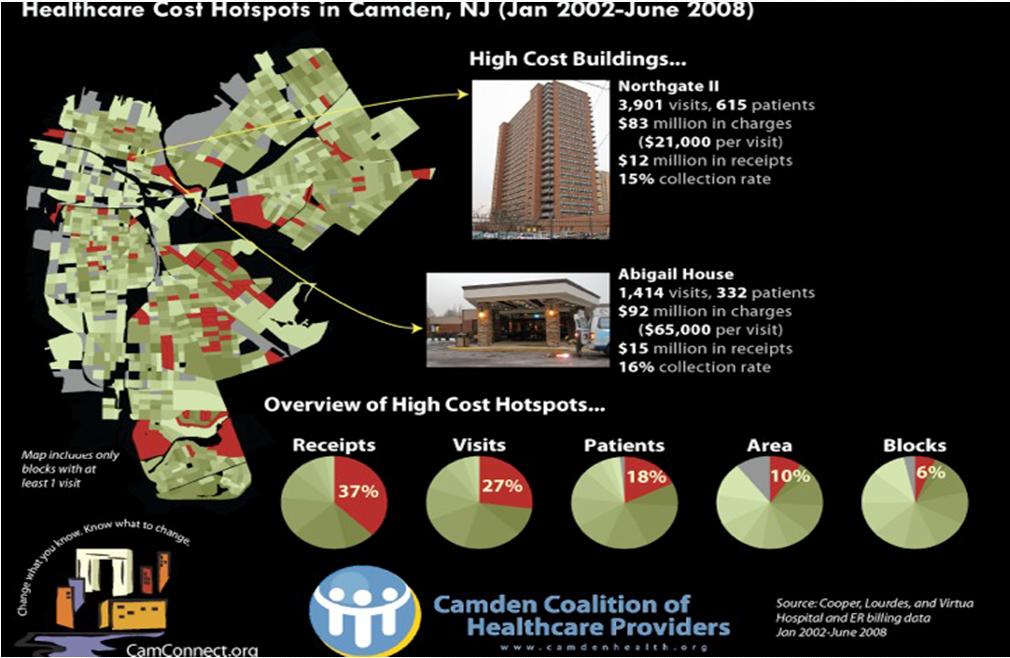
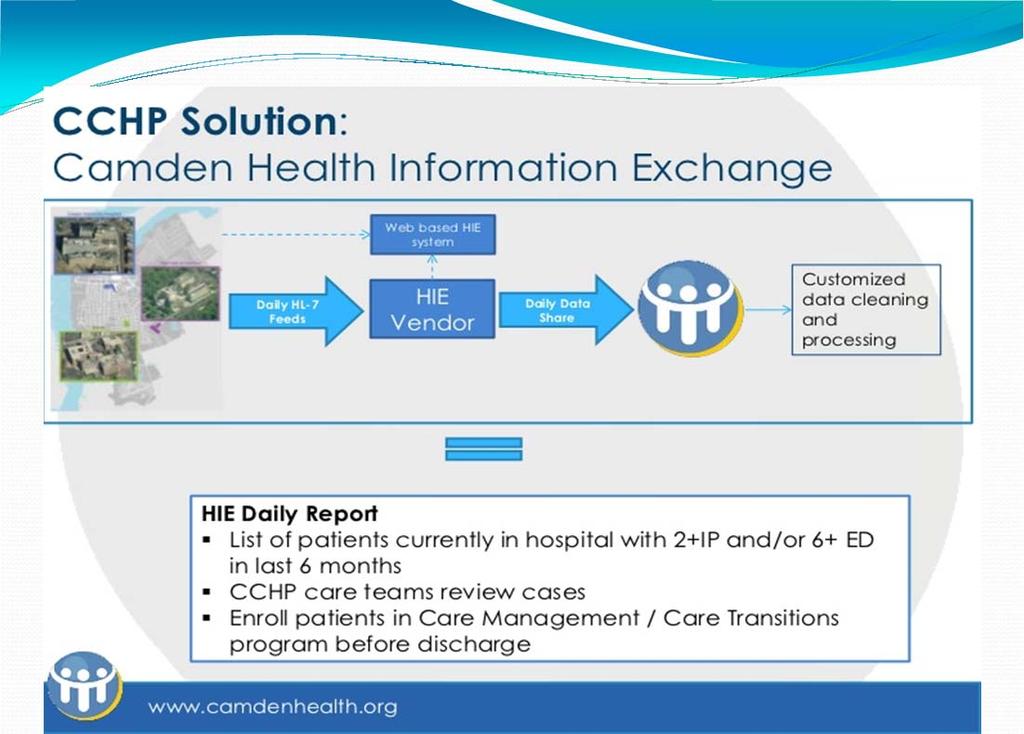
10 National Best Practice Camden Coalition of Healthcare Providers Bending the Cost Curve Founder of Hot Spotting Community Coalition Community HIE Care Intervention Teams Train Camden Residents to participate in decision making over healthcare resources Community Transformation Research and Training Center Dr Jeffrey Brenner Executive Director/Medical Director, Camden Coalition of Healthcare Providers, MacArthur Genius Award 10
11 11
12 12

13 For a Wealth of Information sitelearning/resources/care intervetions/ 13

14 Health Quality Partners The Fountain of Youth Dr Advance Preventive Care Home Based Nurse Case Management Evidence Based Intervention Frail Medicare Patients Ken Coburn MD MPH President Health Quality Partners 10 Year RCT Death Rate decreased 24% Hospitalization decreased 33% Cost decreased 22% For More Information Ezra Klein Article

15 Center for Integrative Medicine Ambulatory ICU R. Corey Waller MD, MS, FACEP, ABAM Director, Center for Integrative Medicine Medical Staff Chief, Division of Pain Management Comprehensive Bio Psycho Social Model Clinic MD/PA/MSW >10 ED Visits for >2 years Follow for 6 9 months and transition to PCP Pregnant Substance Dependent patients and Super Utilizers Spectrum Health has shown a 3.2 million year over year decrease in charges for patients seen in CIM For More Information how.htm?doc_id= Waller.pdf 15

16 Complex Care Portal Rapid Cycle Care Transformation Lauran Hardin MSN, RN CNL Director Complex Care Portal Program Population Analysis, risk stratification and financial modeling for CIN Expert Intervention Center Mentor/Potentiate Existing Resources Build Infrastructure in system Embed Evidence Based Tools Build Community Partnerships Portal Structure 2.0 RN FTEs Virtual Team built around the patient with all other disciplines >700 patients served in one year 5 10 new patients added weekly Significant reduction in ED/UC, Inpatient/Observation admissions, LOS Quality/Safety works whether patient engages or not Entry Criteria: Complex = high frequency, extended LOS, complicated issues 16


17 Seeing Beyond the Acute Episode of Care (Aggregate Patient Story/Stock Photo) Young 30 year old Woman Chronic Pain & Dependent on legally prescribed Narcotics (overuse) Pregnant and Hiding it from Providers Accessing multiple EDs for narcotics Multiple CT Scans Outcome Cross Continuum/ED Plan of Care Decreased Overtesting Referral to Comprehensive Clinic 33 5/5/2014 Meeting the Needs of Vulnerable Populations (Aggregate Patient Story/Stock Photo) Male 48 years old Alcoholism and Substance Use Disorder Significant Psychiatric Issues Fragile life circumstances Lives with a friend Outcome Safe plan for patient and staff Link to CPI techniques Reminder to see the whole person 34 5/5/

 207 620 8538 (fax) For More Information: http://www.")
18 Coordinating Across Systems (Aggregate Patient Story/Stock Photo) Female 78 years old Dementia with Agitation Lives in Long Term Care Frequent UTIs Outcome Safe plan for patient and staff Evidence Based Pathway Cross Continuum Agency Collaboration 35 5/5/2014 Maine Quality Counts Collaborative Community Care Helena Peterson RN, MPH, CPHQ Program Manager, Community Care Teams Maine Quality Counts 16 Association Dr, P.O. Box 16 Manchester, ME (cell) (fax) For More Information: ycounts.org/ 18

19 Community Care Teams Multi disciplinary, community based, practiceintegrated care teams Build on successful models (NC, VT, NJ) Support patients & practices in Pilot sites, helping patients overcome barriers to care, improve outcomes Receive PMPM payments from Medicaid, Medicare, commercial payers Key element of cost reduction strategy, targeting high cost patients to reduce avoidable costs (ED use, admits) Maine PCMH Pilot Community Care Teams Environment Schools Transportation Workplace Housing Care Mgt Outpatient Services Family Food Systems High need Individual PCMH Practice Med Mgt Specialists Shopping Coaching Income Behav. Health & Sub Abuse Hospital Services Heat Faith Community Literacy Physical Therapy 38 19
20 Maine Community Care Team Referral Process Alignment of CM Resources (Pre-referral) Identify Patients & Respond Engage Patients CCT Interventions - Graduation CCT develops report capacity: portals, hospital data, HIN CCT identifies patient from data Pt referred to CCT CCT develops workflows & comm systems w/cm resources & practices Practice aware of CCT & other CM options Practice enables EHR access for CCT. Practice identifies point person to make CM referrals Payer/ external CM identifies pt Practice identifies pt Yes CM accepts pt Meets criteri a? Other appropriat e CM? Notify practice Notify pt No No Yes Engage pt: face to face, call or letter Notify practice Outreach successful? No 1st pass, 2 nd pass & disch letter Yes No, plateau or lost to followup Meet pt Set goals, expectations, disch plan Home visit Further visits/referrals: health educator, telehealth, transportation, hospice etc) Goals met? Yes Discharge Graduate DRAFT H. Peterson 01/22/2014 Notify practice Monitor utilization Additional Resources Southcentral Foundation Nuka Model of Care Community Centered, Team Based Model Anchorage, Alaska Nuka_Model_of_Care_Provides_Career_Growth_for_Frontline_Staff.pdf Commonwealth Care Alliance Model of care for Dual Eligible Patients Boston, Massachusetts program/our model of care Project RED (re engineered discharge ) 20
21 Roles in an Interdisciplinary Team Interdisciplinary Team Physician Case Manager MSW Pharmacist Psychiatrist Community Health Worker/Health Coach Resource Coordinator Financial Services Support 21
22 Key Functions Chronic Disease/Medical Management Medication Reconciliation Care Transitions Navigation Health Promotion & Education Mental Health/Trauma Informed Care Access to Resources Preventive Care Shared Plan Cross Systems Building Trust Next Steps in Hot Spotting 22

23 Promising Practices Research and Core Competency Development Open Source Development Telemedicine Group Visits Same Day Appointments/Call Center Approach PCMH and Practice Redesign Paramedicine Trauma Informed Care For More Information Lauran Hardin MSN, RN CNL Complex Care CNL Mercy Health Saint Mary s 200 Jefferson SE Grand Rapids MI lauran@octoberday.com hardinlj@mercyhealth.com 23
MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000
 28 PC sites serve 115,000") 1 MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000 KENNEBEC VALLEY COMMUNITY CARE TEAM JOAN ORR MCHES, MBA DIRECTOR ACCOUNTABLE
1 MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000 KENNEBEC VALLEY COMMUNITY CARE TEAM JOAN ORR MCHES, MBA DIRECTOR ACCOUNTABLE
Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients
 Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients Lisa M. Letourneau MD, MPH May 2013 Maine PCMH Pilot & CCT Leadership DHA s Maine Quality
Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients Lisa M. Letourneau MD, MPH May 2013 Maine PCMH Pilot & CCT Leadership DHA s Maine Quality
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
CENTER FOR INTEGRATIVE MEDICINE
 CENTER FOR INTEGRATIVE MEDICINE R. Corey Waller MD, MS, FACEP, ABAM Director, Center for Integrative Medicine Medical Staff Chief, Division of Pain Management Medical Staff Chief, Division of Pain Management
CENTER FOR INTEGRATIVE MEDICINE R. Corey Waller MD, MS, FACEP, ABAM Director, Center for Integrative Medicine Medical Staff Chief, Division of Pain Management Medical Staff Chief, Division of Pain Management
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Innovative Coordinated Care Models
 Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014
 Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Implementing Integrated, Interdisciplinary Clinical Care Management in the Patient-Centered Medical Home
 University of Massachusetts Medical School escholarship@umms Commonwealth Medicine Publications Commonwealth Medicine 11-23-2013 Implementing Integrated, Interdisciplinary Clinical Care Management in the
University of Massachusetts Medical School escholarship@umms Commonwealth Medicine Publications Commonwealth Medicine 11-23-2013 Implementing Integrated, Interdisciplinary Clinical Care Management in the
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Healthcare Transformation at. Cherokee Health Systems
 Dennis S. Freeman Chief Executive Officer Cherokee Health Systems Healthcare Transformation at Cherokee Health Systems Blending Behavioral Health Providers into the Patient-Centered Medical Home Speaker
Dennis S. Freeman Chief Executive Officer Cherokee Health Systems Healthcare Transformation at Cherokee Health Systems Blending Behavioral Health Providers into the Patient-Centered Medical Home Speaker
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW. MetroHealth Medical Center
 Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Approaches to Extending Complex Care Models into the Community: Emerging Evidence
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement
 Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Maryland s Integrated Care Network. Heading into Year Three
 Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
The New Frontier: Value- Based Payment Models
 The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature
 New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
2015 Quality Improvement Work Plan Summary
 2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together
 Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care Management
 FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care 2.a.i-Create Integrated Delivery System THIS PROJECT IS MANDATORY FOR ALL PARTICIPATING PROVIDERS
FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care 2.a.i-Create Integrated Delivery System THIS PROJECT IS MANDATORY FOR ALL PARTICIPATING PROVIDERS
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The Medical Home Model: What Is It And How Do Social Workers Fit In?
 I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
National ACO Summit. Third Annual. June 6 8, Follow us on Twitter and use #ACOsummit.
 Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. Opening Plenary Session Welcome and Overview Mark McClellan, MD, PhD Director, Engelberg Center for Health
Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. Opening Plenary Session Welcome and Overview Mark McClellan, MD, PhD Director, Engelberg Center for Health
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego
 David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego Describe need for programs targeting homeless high utilizers of emergency
David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego Describe need for programs targeting homeless high utilizers of emergency
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010
 Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Best Practices. SNP Alliance. October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees
 SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
From Bundles to Global Capitation: Aligning Care Models to Payment Models. The 16 th Annual Population Health Colloquium Philadelphia, PA
 From Bundles to Global Capitation: Aligning Care Models to Payment Models The 16 th Annual Population Health Colloquium Philadelphia, PA March 8, 2016 The U.S. Payer Market is Committed to Dramatically
From Bundles to Global Capitation: Aligning Care Models to Payment Models The 16 th Annual Population Health Colloquium Philadelphia, PA March 8, 2016 The U.S. Payer Market is Committed to Dramatically
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Arkansas PCMH: Transformational Success Story. William Golden MD MACP Medical Director, AR Medicaid UAMS Prof. Int. Med and Public Health
 Arkansas PCMH: Transformational Success Story William Golden MD MACP Medical Director, AR Medicaid UAMS Prof. Int. Med and Public Health International Challenge All Health Systems Have Service Demand and
Arkansas PCMH: Transformational Success Story William Golden MD MACP Medical Director, AR Medicaid UAMS Prof. Int. Med and Public Health International Challenge All Health Systems Have Service Demand and
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Physical Health Integration Within Behavioral Healthcare: Promising Practices
 Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Caring for the Underserved - Innovative Pharmacy Practice Integration
 Caring for the Underserved - Innovative Pharmacy Practice Integration Sarah T. Melton, PharmD, BCPP, BCACP, FASCP Associate Professor Pharmacy Practice Clinical Pharmacist, Johnson City Community Health
Caring for the Underserved - Innovative Pharmacy Practice Integration Sarah T. Melton, PharmD, BCPP, BCACP, FASCP Associate Professor Pharmacy Practice Clinical Pharmacist, Johnson City Community Health
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential
 A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format: