LESSONS FROM OREGON S FQHC ALTERNATIVE PAYMENT METHODOLOGY PILOT
|
|
|
- Emil Singleton
- 6 years ago
- Views:
Transcription
1 LESSONS FROM OREGON S FQHC ALTERNATIVE PAYMENT METHODOLOGY PILOT

2 VALUE-BASED PAYMENT REFORM ACADEMY NASHP Craig Hostetler June 14, 2016
3 Why Are We Doing This?

4 Why Take the Risk? Our stakeholders wanted something better Patients Payers Providers & support staff Recruitment getting harder Increased pressure Transparency and accountability increasing Payment moving from volume to value
5 OPCA s goal for Alternative Payment Advanced Care Model (APCM) Lead the development of and align payment with an efficient, effective, and emerging care model that achieves the Quadruple Aim in Oregon CHCs
6 Gaining CHC Buy-In Providers asked for payment change to support PCMH Started with a small group of advanced PCMH clinics Developed a rough model Approached state, gained interest/champions Presented to Oregon Primary Care Association (OPCA) board and then membership Important that all CHCs work together instead of cutting own deal

7 Starting the Conversation with Medicaid Our missions are aligned Payment reform should make primary care more effective Value-based pay makes sense Must account for behavioral and socio-economic barriers Let s work together on a bridge to value-based pay
8 Adjusting/Stratifying for Patient Complexity Not adjusting could increase disparities Hong et. al., Relationships Between Patient Panel Characteristics and Primary Care Physician Clinical Performance Rankings, Journal of the American Medical Association, 9/8/10. Chien et.al., Do Physician Organizations Located in Lower Socioeconomic Status Areas Score Lower on P4P Measures?, Journal of General Internal Medicine, 12/13/11 Paying for health homes in the safety net Long A., Phillips K., Hoyer D., Payment Models to Support Patient-Centered Medical Home Transformation: Addressing Social, Behavioral, and Environmental Factors, Qualis Health, 8/11. Not adjusting could penalize safety net Tyo et. al., Methodological Challenges for Measuring Primary Care Delivery to Pediatric Medicaid Beneficiaries Who Use CHCs, American Journal Of Public Health, 2/13.
9 Medicaid Relationship Critical Partnership between state, OPCA and CHCs is very strong Regular face-to-face and phone discussions Working together to remove barriers with a focus on better patient care The success of APM as measured by better cost, quality, access and patient experience is at the forefront Measuring social determinants of health (SDoH) to inform care interventions & payment
10 What s in it for the State? Predictable cost per-member-per-month (PMPM) Promotes patient engagement/outreach to unengaged Gain a lot more information on cost, quality, access Develop relationship with PCA and CHCs to improve and be accountable to value Support the next phase of transformation after PCMH Allows FQHCs to better align with coordinated care organization (CCO) requirements Ultimately, it s about better care for the patient
11 What s in it for the MCO? Promotes robust, team-based care Clinics are testing SDoH interventions Predictable payment PMPM Can integrate with current payment reform efforts Promotes engagement of all assigned patients Alignment with value-based payments by taking away need to produce visit
12 PCA Resources Required Meeting facilitation/project management Financial expertise to help develop rates Data analysis and presentation Learning community development and support Onboarding new clinics Additional cost to PCA - $500,000 annually
13 Oregon s Alternative Payment Methodology (APM) and Safety Net Clinics NASHP Value-Based Payment Reform Academy June 14, 2016 Don Ross, Manager Program Policy, Oregon Medicaid

14 Oregon Medicaid Health Systems Transformation and Coordinated Care Organizations Recognition that health care costs are unsustainable and that we do not get the health outcomes for the amount of money that we spend After 100s of hours of stakeholder meetings, tribal consultation and community meetings, a health transformation plan for Oregon s Medicaid program is being implemented Triple Aim: Better Health, Better Care, Lower Costs!!

15 Other Current innovations under way Health Homes Patient-Centered Primary Care Homes (PCPCHs) More than 500 clinics have applied and been certified as PCPCHs in Oregon and many of them are FQHCs and RHCs All Oregon FQHCs in the APM pilot are certified PCPCHs and changed their model of care due to this certification and opportunities presented by pilot
16 Health System Transformation & Alternative Payment Methodology Health Centers in Oregon are positioning themselves to benefit from CCO requirements by helping the state develop an APM that is aligned with Transformation objectives to move away from increased billing of office visits, and to integrate and coordinate services and management of patient needs in care teams: Without suffering reduced revenue into the practice With increased satisfaction of patients and physicians While increasing access and quality of outcomes

17 Why change from PPS to PMPM? The PPS encounter rate payments reward FQHCs that bill the most services Difficulty recruiting and retaining professional level staff due to hamster wheel of churning out office visits (run harder for more revenue) PPS payment mechanism not centered around patient s health and outcomes Time from service date to receiving payment sometimes greater than 1 year Providers more frequently working at the top of their licensure w/ care teams centered around the patient



18 Developing the APM Initiated by the Oregon Primary Care Association (OPCA) in partnership with member FQHCs, SPA approved summer 2012 Proposed the OHA pay FQHCs a per-member permonth (PMPM) payment based on historical revenue and utilization Each FQHC s encounters and revenue for the prior year were used to determine the PMPM rates First APM FQHCs joined in March 2013: OHSU Family Medicine at Richmond Mosaic Medical Virginia Garcia Memorial Health Centers
19 Key Elements of APCM The Financial Model
 Agree to Accountability Plan and Learning Community")
20 Participation Requirements 3 year commitment 30 day emergency exit All sites, all patients Some services carved out (mental health, dental, OB for now) Agree to Accountability Plan and Learning Community participation
21 Key Financial Elements Creating Day 1 lists, 18 month lookback New patient engagement, face-to-face with licensed provider Attribution end date after 1 st visit with FQHC/RHC/IHS 2 visits with another provider Reconciliation quarterly with annual settlement, if necessary; PPS is floor

22 Basic Rate Construct PMPM payment MCO payment like anyone else s Wrap based on prior year Separate bonus payments

23 What s In? PPS scope of primary care What s Out? Patients - Open card, Medi-Medi, SBHC Prenatal Pharmacy Inpatient Mental, oral health (coming later)
24 Key Elements Care Model
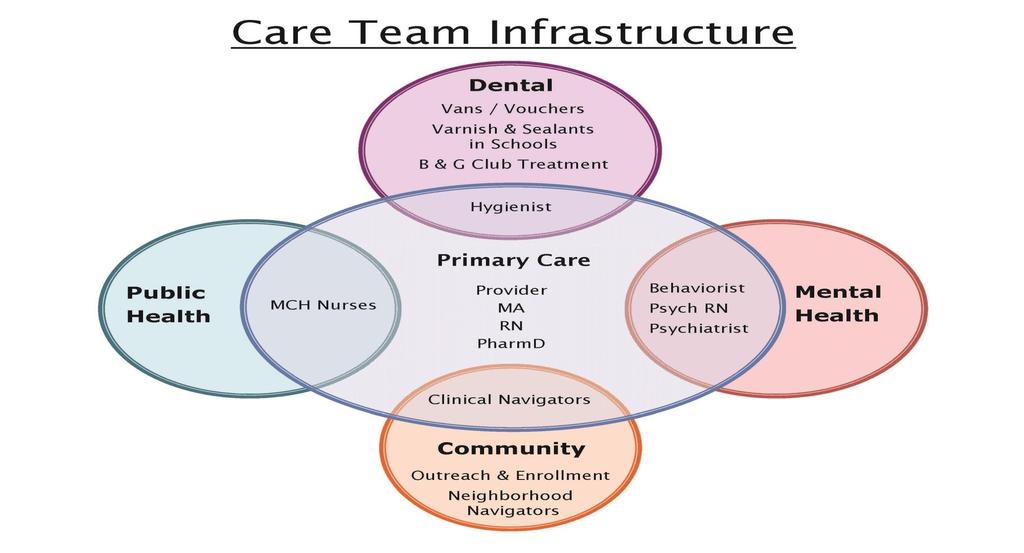
25 Five Strategies Use actionable and real time data Increase access through new visit types Build care teams that are a reflection of patient needs Partner with patients to cocreate and provide selfmanagement services Enhance appropriate care and work to reduce unnecessary emergency department utilization and ambulatory care sensitive admissions
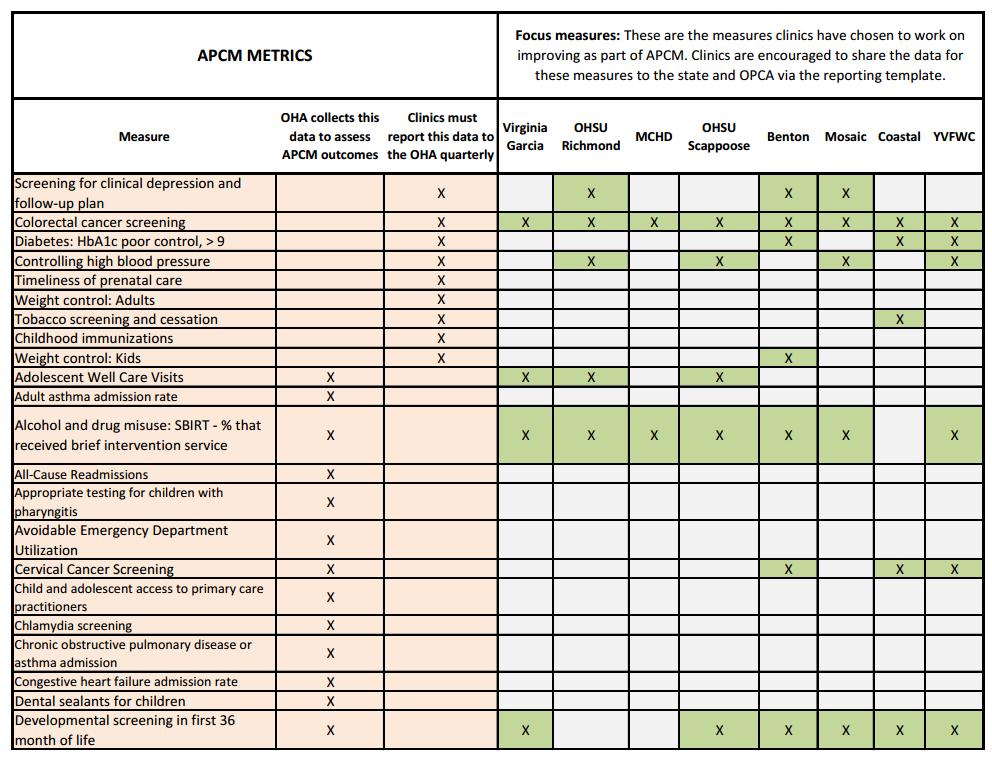
26 Data Track 9 CCO measures, 5 UDS measures, and 1 utilization measure. Focus on two of the clinical measures. Sustain or improve patient satisfaction. Meaningful engagement Document visits and engagement touches with 70% of established patients on an annual basis. Oregon APCM Metrics and Accountability Plan Cost of care Maintain or reduce adjusted per capita costs. Use risk adjustment methods based on TCOC. Match services and resources to complex care needs. Segmentation Identify a population and use tool to learn more about bio-psychosocial needs. Improve quality through segmentation.
27
28 Engagement Touches New Visit Types Coordination and Integration Education, Wellness and Community Support Outreach and Engagement Home visit billable encounter (auto) E-visit (MyChart - auto) Telemedicine Encounter (auto) Telephone Visit (auto) Home visit nonbillable encounter Information Management Coordinating Care: Dental Clinical Follow-up and Transitions Warm Hand-Off Transportation Assistance Health Education Supportive Counseling Education Provided in Group Setting Support Group Participant Exercise Class Participant Flowsheet - screening tools (auto) Panel Management Outreach Case Management Accessing Community Resource
29 Segmentation Strategy 29 Use data and analytics to figuring out people falling through the cracks in areas of quality metrics trying to improve. Figure out health disparities, account for social and behavioral factors, and drilldown to a subset of 100 patients. Interview at least 10 people using a SDoH Screening Tool (PRAPARE+) to better understand their health challenges. Create a therapeutic alliance with the people you interview; learn to understand them more holistically. Apply learnings to your subpopulation. Improve health for group by experimenting with: Design new visit type, new role, new partnerships
30 Outcomes Year one report from OPCA and state contractor under production Model appears budget neutral per patient, per year APM reconciliations have not triggered payment to date. State concerned about access MCO payments appear level Clinical quality indicators appear to be holding or improving in most cases, Optumas report Signs of improvement in total health care utilization Access under ACA posed a challenge to broader transformation
31 Lessons Learned
 Cascade of other financial implications: Budgeting Panel Size")
32 Payment Model Lessons Model should be hand in hand with payment Cash flow issue for state Data/Outcomes should be clear, thoughtful, aligned This is a Partnership requiring constant refinement and trouble shooting: With Medicaid, MCOs, between clinics, IT/HCCNs Financial stability as a requirement to participate (NOT a consequence) Cascade of other financial implications: Budgeting Panel Size Provider Reimbursement

33 Advanced Care Model: Lessons Learned Never separate from payment Consider immensity of change & competing demands Create less time pressure Plan for data collection Add ACM teams at all participating sites Co-create OPCA-ACM teams Keep learning (co-design is messy)

34 PMPM Rate Development Utilizing the FQHCs wraparound revenue, CCO payments, and member months, the Wrap Cap PMPM Rate was developed Utilizing the FQHCs FFS revenue for opencard patients, the Open-Card PMPM Rate was developed Each health center has both types of PMPM rates Rate Calculation example: CY 2012 $1,000,000/25,000 member months = $40 PMPM

35 Attribution: The Patient Lists From FQHC s go-live date, we allow an 18 month look-back Patients receiving care at the health center in the prior 18 months are attributed, and PMPM payments issue to the health center each month Patient lists are uploaded by the health center using MMIS Provider Web Portal
36 Attribution, continued NEW patients may be enrolled with the health center after an encounter is registered PMPM payments begin on the day patient is established at health center Patients are moved by the state when they establish care with a different primary care provider, so they retain choice of providers- PMPM payments stop and/or are recouped The health centers now have a tangible list of patients for whom they are responsible for improving health and outcomes With revenue delivered on time each month, health centers may focus on delivering the right care at the right time for the patient and their family


37 What if Health Centers Stop Seeing Patients?! After detaching their revenue from the billable office visit, how do we know they are taking care of their patients? Monitor quarterly reports on Touches Monitor quarterly Quality Metric Reports Monitor their encounter data by analyzing their PPS equivalency, quarterly
 that drive transformation of the delivery model, and improve patient health, outcomes and quality of")
38 Touches Reports Touches are also known Enabling Services Flexible Services (CCOs) Core Services (PCPCHs) Alternative Services Non billable, non-reimbursable services as: The OHA has encouraged FQHCs to focus on the non-billable services (touches) that drive transformation of the delivery model, and improve patient health, outcomes and quality of life



39 Touches Reports, continued Some of the touches currently being reported include: - Referrals to community resources, coordinating clinical follow-ups, coordinating transitions in care settings, exercise classes, education provided in group settings, support groups, non-billable warm hand-offs, non-billable home visits, among many others!
40 What Health Centers are Saying Since beginning (APM), Virginia Garcia has seen high-impact changes that have allowed our organization to better pursue our core mission in Washington and Yamhill Counties. By utilizing APM, we now have the time to do the work of being a Patient Centered Primary Care Home and optimize the core practices of our patient teams. Virginia Garcia Memorial Health Center REaCH Team (Richmond Engagement and Community Health) is a multidisciplinary team focused on high-utilizer patients. Activities include linking patients to Outreach Workers who help connect to community resources, navigate healthcare system, support self-management, etc. A Care Coordinator tracks Richmond patients when admitted and using Emergency Room to ensure coordinated follow-up care or touch is made. OHSU Richmond Family Medicine
, to target complex patients with high emergency department and in-patient utilization.")
41 What Health Centers are Saying, continued APM model of care helps support a hotspotting team we ve assembled, referred to as the Community Care Coordination Team (comprised of a Family Nurse Practitioner, Mental Health Specialist, and Community Health Worker), to target complex patients with high emergency department and in-patient utilization. This work has resulted in a 76% reduction in ED visits and an 82% reduction in hospital admissions. These drops in utilization have resulted in 74% reductions in hospital charges for over 190 patients. Virginia Garcia Memorial Health Center (self reported data)
42 What Health Centers are Saying, continued APM is allowing VG the flexibility with addressing preventive care and behavior change through an innovative program such as our Teaching Kitchen, where a cohort of 8 to 12 patients are engaged in an 8 week class on cooking nutritious meals. Virginia Garcia Memorial Health Center VG is integrating other wellness activities such as low-impact exercise, physical therapy, acupuncture, Zumba, and tai chi as part of the care plan for patients. Virginia Garcia Memorial Health Center Social Workers began Dialectical Behavioral Therapy group visits focusing on REaCH patients and others with depression, anxiety, anger issues and usually history of some sort of trauma which interferes with treatment of chronic or other conditions. The groups meet for 6 week courses and are well attended. OHSU Richmond
43 Quality Metric Reports Each APM HC currently submits quarterly reports on the following metrics: Tobacco Screenings Depression Screenings Diabetes Control Cervical Cancer Screenings Weight Control: Adults and Kids HTN Controlled (most recent BP less than 140/90) Childhood Immunizations % of patients that would recommend their care team % of patient visits with assigned care team % of patients assigned by CCO that have been established
44 1 st Year Metrics: How are they Doing? For January 1 st 2013 through December 31 st 2013: Tobacco Screenings hit and remained at 100% Weight control for kids increased by 145%! Childhood immunizations increased 115%! Patients with a favorable survey response regarding their care team averaged 96% among the health centers (a 50% increase)!
45 Cost Performance Analytics ongoing ED and hospital inpatient are clearly reduced Total cost of care (TCC)? Cost and utilization of referred services Sub-capitation arrangements of CCOs Pharmacy costs Where do savings accrue short and long term?
46 Payment Reconciliation Reports Health Centers submit Payment Reconciliation reports each quarter detailing all of their encounters and payments Federal statutory requirements guarantee that health centers will be reimbursed at least equal to what PPS payments would have been, the PPS Equivalent Actual Encounters X PPS Rate = PPS Equivalent If actual payments are below the PPS equivalency, the OHA will issue an annual settlement check

47 Looking forward The OPCA hosts quarterly Advanced Payment and Care Model summits where the health centers, national health care experts, and the Oregon Health Authority share insights and engage in planning the future of the APM program Quality Metric reports expected to evolve and align with CCO Incentive Measures so that health centers can better assist CCOs in accomplishing Triple Aim goals

48 Looking forward, continued Currently, APM PMPM payments are issued for Medical services only Mental health, dental health, prenatal/ob services are carved-out and pay at the PPS encounter rate Medical encounters are billed, but $0 pay in the MMIS Ongoing work to carve mental health and OB services into the PMPM rates
49 Lessons Learned System Functionality Do you have a way to process the methodology you ve chosen? Attribution details - Leakage, look back, adds and deletes, no duplicate payment and no free care What to carve out and for how long? OB, Oral (primary and specialty), Mental Health and SUD

50 Alternative Payment: Perspective from Point of Care NASHP FQHC Payment Reform Meeting June 2016 Sherlyn Dahl
51 CHC of Benton & Linn Counties Integrated Public Health, Mental Health, Primary Care, Dental Services Public entity FQHC with Benton County sites; Corvallis (includes admin, Mental Health & Public Health) South Corvallis (also a School-Based Health Center) Monroe (also a School-Based Health Center) Alsea Additional sites in Linn County Lebanon Sweet Home Served 9,200 patients in 2015
 Mental Health: Integrated & Specialty")

52 Services Medical: Patient Centered Primary Care Home Primary Care Family Planning School Based Health Center (Lincoln & Monroe) Mental Health: Integrated & Specialty Behavioral Health Adult Mental Health Children s Mental Health Addiction Services Dental Services to Children Varnish & sealant program Adult Hygiene Van & Voucher program 52
53 Transforming Payment Alternative Payment Methodology Pilots
54 OHA/OPCA APM Pilot Started July 1, 2014 Paid a monthly PMPM (per member per month) for all engaged patients PMPM is for wrap portion of Medicaid payment Required reporting on touches Quarterly reconciliation 54
55 CCO Alternative Payment Pilot Started January 2015 Methodology for payment Paid a monthly PMPM (per member per month) for enrolled Oregon Health Plan (OHP) patients Rate of PMPM based on the rate group the member is assigned 6,000 IHN members assigned 2,500 3,000 not yet seen by clinic Monthly member reconciliation Quarterly reporting Access, Outcome, & Utilization Metrics 55
56 Transforming Care Delivery Patient Centered Primary Care Home (PCPCH)
57 Prep for APM: Right Size Care Team Core Team Providers (2) Medical Assistants (2) Scheduler Additional Members Panel Manager RN Care Coordinator Behaviorist Clinical Navigator Clinical Pharmacist Hired additional staff (5 FTE across all sites) 57
58 Additional Preparation Assess assignment process, accessing member data from the CCO, & matching clinic patients to CCO lists Defined touches & reporting process Assessed EHR capability to generate needed reports Assessed space; team pod & consult rooms Determined panel size & complexity 58
59 Initial Focus of Care Team Shared office space & communication Refine roles & work flow Role of Panel Manager & all team members Supported working at top of license Identified care coordination work Managing panels Scheduling processes Team communication (scrubbing & huddles) Patient engagement in care & self management Proactive Care Prevention & Screening Recall system for follow-up of chronic conditions 59
60
61 Next Layer of Focus Patient engagement Initial contact for newly assigned Access for assigned but not yet seen by provider Appropriate utilization Use of ED & Urgent Care Leakage to other primary care providers Expanding Access Matching team resources & expertise to panel characteristics Quality Improvement Improving clinical outcome priorities Assessing Social Determinants of Health Interface with community, Public Health 61
62 Impact & Takeaways
63 Clinical Impact of APM Detached payment from a provider visit/schedule Increased reliance on team Added FTE to fully staff teams Exploring alternative methods for access Team member visits Navigators Group visits Enhanced focus on quality & outcomes Resources for innovation & integration 63

64 Benefits Financial predictability Resources for innovation Better care Improved access 64

65 Be Prepared Staff time in preparation for APM & on-going work with reconciliation Increase team staffing Increase staffing to create, generate, & distribute reports Lots of change Work flow adjustments Roles & responsibilities Areas of focus 65
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Oregon s Safety Net Incorporating Value-based payment into system reform. Don Ross, Manager Program and Planning October 18, 2016
 Oregon s Safety Net Incorporating Value-based payment into system reform Don Ross, Manager Program and Planning October 18, 2016 Oregon chose a new way Better Health, Better Care and Lower Costs Transform
Oregon s Safety Net Incorporating Value-based payment into system reform Don Ross, Manager Program and Planning October 18, 2016 Oregon chose a new way Better Health, Better Care and Lower Costs Transform
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
Oregon Primary Care Association s APCM Introduction/Overview
 APM Rate Setting Process 1 Oregon Primary Care Association s APCM Introduction/Overview Laura Sisulak, Strategic Projects Senior Director Oregon Primary Care Association APM Rate Setting Process 2 Oregon
APM Rate Setting Process 1 Oregon Primary Care Association s APCM Introduction/Overview Laura Sisulak, Strategic Projects Senior Director Oregon Primary Care Association APM Rate Setting Process 2 Oregon
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Medicaid MOA Update and Payment Reform Visioning Session
 Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Robert Wood Johnson Foundation Payment Reform Evaluation Project. Oregon Primary Care Association. August 2015 Report
 Robert Wood Johnson Foundation Payment Reform Evaluation Project Transforming Payment for Oregon s Community Health Centers through an Alternative Payment Methodology Oregon Primary Care Association August
Robert Wood Johnson Foundation Payment Reform Evaluation Project Transforming Payment for Oregon s Community Health Centers through an Alternative Payment Methodology Oregon Primary Care Association August
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Partnering with Managed Care Entities A Path to Coordination and Collaboration
 Partnering with Managed Care Entities A Path to Coordination and Collaboration Presented by: Caroline Carney Doebbeling, MD, MSc Chief Medical Officer, MDwise May 9, 2013 Agenda Are new care models on
Partnering with Managed Care Entities A Path to Coordination and Collaboration Presented by: Caroline Carney Doebbeling, MD, MSc Chief Medical Officer, MDwise May 9, 2013 Agenda Are new care models on
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Progress Highlights. January
 Progress Highlights January 2013 - March 2014 Goals & Outcomes at a Glance Training & TA Quality Data Transparency* Equity Social determinants Policy agenda Viability Value National influence Service &
Progress Highlights January 2013 - March 2014 Goals & Outcomes at a Glance Training & TA Quality Data Transparency* Equity Social determinants Policy agenda Viability Value National influence Service &
Innovative Coordinated Care Models
 Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
July 30, 2018 at 5:00 pm via electronic submission to: Transformation Department NW Walnut Blvd
 In compliance with the Americans with Disabilities Act, this document can be made available in alternate formats such as large print, Web based communications, and other electronic formats. To request
In compliance with the Americans with Disabilities Act, this document can be made available in alternate formats such as large print, Web based communications, and other electronic formats. To request
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
THE FQHC ALTERNATIVE PAYMENT METHODOLOGY TOOLKIT:
 JULY 2017 THE FQHC ALTERNATIVE PAYMENT METHODOLOGY TOOLKIT: Fundamentals Of Developing A Capitated FQHC APM A Guide for Primary Care Associations and Health Centers AUTHORED AND PREPARED FOR NACHC BY:
JULY 2017 THE FQHC ALTERNATIVE PAYMENT METHODOLOGY TOOLKIT: Fundamentals Of Developing A Capitated FQHC APM A Guide for Primary Care Associations and Health Centers AUTHORED AND PREPARED FOR NACHC BY:
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
ACO Model Fits Pediatrics Well
 ACOs and Pediatrics James M. Perrin, MD, FAAP Professor of Pediatrics, Harvard Medical School John C. Robinson Chair of Pediatrics, Associate Chair MassGeneral Hospital for Children Immediate Past President,
ACOs and Pediatrics James M. Perrin, MD, FAAP Professor of Pediatrics, Harvard Medical School John C. Robinson Chair of Pediatrics, Associate Chair MassGeneral Hospital for Children Immediate Past President,
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Updated August 24, 2015
 FQHC Payment Reform Demonstration Q & A The following Q&A describes the FQHC Payment Reform Demonstration, also commonly referred to as the Wrap Cap. A visual of the payment flow can be found at the end.
FQHC Payment Reform Demonstration Q & A The following Q&A describes the FQHC Payment Reform Demonstration, also commonly referred to as the Wrap Cap. A visual of the payment flow can be found at the end.
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Oregon Health Leadership Council: High Value Patient Centered Care Model
 February 21, 2013 Oregon Health Leadership Council: High Value Patient Centered Care Model Mini Summit VII: Intensive Outpatient Care Programs Denise L. Honzel Executive Director Oregon Health Leadership
February 21, 2013 Oregon Health Leadership Council: High Value Patient Centered Care Model Mini Summit VII: Intensive Outpatient Care Programs Denise L. Honzel Executive Director Oregon Health Leadership
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
kaiser medicaid and the uninsured commission on O L I C Y
 P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
Oregon s Health System Transformation & The Innovator Agent Role
 Oregon s Health System Transformation & The Innovator Agent Role Joell E. Archibald, RN, BSN, MBA Estela Gomez, MSW Belle Shepherd, MPH OHA Transformation Center Innovator Agents Background: Oregon s Health
Oregon s Health System Transformation & The Innovator Agent Role Joell E. Archibald, RN, BSN, MBA Estela Gomez, MSW Belle Shepherd, MPH OHA Transformation Center Innovator Agents Background: Oregon s Health
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL
 PROGRAM DESIGN AND BUDGET PROPOSAL") LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
Ambulatory Care Practice Trends and Opportunities in Pharmacy
 Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Value-Based Payment Reform Academy: Advancing Value-Based Payment Methodologies for FQHCs and RHCs
 Value-Based Payment Reform Academy: Advancing Value-Based Payment Methodologies for FQHCs and RHCs FOR AUDIO, PLEASE DIAL: (866) 740-1260 ACCESS CODE: 2383339 MARCH 10, 2016 2:00-3:00PM ET This work is
Value-Based Payment Reform Academy: Advancing Value-Based Payment Methodologies for FQHCs and RHCs FOR AUDIO, PLEASE DIAL: (866) 740-1260 ACCESS CODE: 2383339 MARCH 10, 2016 2:00-3:00PM ET This work is
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
WHAT IS PRAPARE ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 WHAT IS PRAPARE 2 PRAPARE: PROTOCOL
ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 WHAT IS PRAPARE 2 PRAPARE: PROTOCOL
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
Medicaid 101: The Basics for Homeless Advocates
 Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Designing a Medicaid ACO Program: Insights from Trailblazing States
 Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
PRIMARY CARE RENEWAL. PCR Core Components: Change Packages
 PRIMARY CARE RENEWAL PCR Core Components: Change Packages PCR Change Packages Purpose Define core PCR practice components For each component, create common understanding of: Assumptions Purpose Principles
PRIMARY CARE RENEWAL PCR Core Components: Change Packages PCR Change Packages Purpose Define core PCR practice components For each component, create common understanding of: Assumptions Purpose Principles
The MetroHealth System
 The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive
The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
OHA s Quality & Accountability Metrics: Measuring CCO Performance. State of Oregon Research Academy September 17, 2014
 OHA s Quality & Accountability Metrics: Measuring CCO Performance State of Oregon Research Academy September 17, 2014 Health System Transformation: Achieving the Triple Aim 2 Our Health System Transformation
OHA s Quality & Accountability Metrics: Measuring CCO Performance State of Oregon Research Academy September 17, 2014 Health System Transformation: Achieving the Triple Aim 2 Our Health System Transformation
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
10/6/2017. FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction. Agenda. Incentives in PPS: what does excludable mean?
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
Iowa Medicaid: Innovations & Initiatives
 Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
Central Oregon Integrated Care Collaborative: Operational Strategies for Success
 Central Oregon Integrated Care Collaborative: Operational Strategies for Success 1 May 8, 2018 2 Welcome! Mike Franz, MD, DFAACAP, FAPA Medical Director, Behavioral Health, PacificSource Thanks to the
Central Oregon Integrated Care Collaborative: Operational Strategies for Success 1 May 8, 2018 2 Welcome! Mike Franz, MD, DFAACAP, FAPA Medical Director, Behavioral Health, PacificSource Thanks to the
Agenda STATE OF TENNESSEE 12/7/2016
 STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
ROCKY MOUNTAIN HEALTH PLANS REGIONAL ACCOUNTABLE ENTITY ORIENTATION GUIDE Region 1 An Introduction for Providers March 2018
 ROCKY MOUNTAIN HEALTH PLANS REGIONAL ACCOUNTABLE ENTITY ORIENTATION GUIDE Region 1 An Introduction for Providers March 2018 rmhpcommunity.org 0 TABLE OF CONTENTS Table of Contents... 1 About This Guide...
ROCKY MOUNTAIN HEALTH PLANS REGIONAL ACCOUNTABLE ENTITY ORIENTATION GUIDE Region 1 An Introduction for Providers March 2018 rmhpcommunity.org 0 TABLE OF CONTENTS Table of Contents... 1 About This Guide...
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Primary Care Home 2017 A Rural Heath Perspective
 Patient Centered Primary Care Home 2017 A Rural Heath Perspective Megan Bowen, Site Visitor Patient Centered Primary Care Home Program, Oregon Health Authority Jill Boyd, MPH, CCRP, Primary Care Transformation
Patient Centered Primary Care Home 2017 A Rural Heath Perspective Megan Bowen, Site Visitor Patient Centered Primary Care Home Program, Oregon Health Authority Jill Boyd, MPH, CCRP, Primary Care Transformation
DST Strategic Planning QUARTER ONE 2018
 2018 DST Strategic Planning QUARTER ONE 2018 2018 DST STRATEGIC PLANNING Contents IHN-CCO DST History and Evolution: 2012-2017... 2 2012... 2 2013... 2 2014... 2 2015... 3 2016... 3 2017... 4 Collective
2018 DST Strategic Planning QUARTER ONE 2018 2018 DST STRATEGIC PLANNING Contents IHN-CCO DST History and Evolution: 2012-2017... 2 2012... 2 2013... 2 2014... 2 2015... 3 2016... 3 2017... 4 Collective
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts
 PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
State Approaches to Providing Health-Related Supportive Services through Medicaid
 State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
Oregon Health Authority Patient-Centered Primary Care Home Program. May 2013
 Oregon Health Authority Patient-Centered Primary Care Home Program May 2013 Presentation Objectives Provide a brief background on Oregon s Patient-Centered Primary Care Home Program and vision for practice
Oregon Health Authority Patient-Centered Primary Care Home Program May 2013 Presentation Objectives Provide a brief background on Oregon s Patient-Centered Primary Care Home Program and vision for practice
Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value
 Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value Leinaala Kanana, Director of Community Health AANHPI Summit May 26, 2017 ~ San Francisco, California
Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value Leinaala Kanana, Director of Community Health AANHPI Summit May 26, 2017 ~ San Francisco, California
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
PCA/HCCN Health Center Program Update
 PCA/HCCN Health Center Program Update National Association of Community Health Centers Community Health Institute August 30, 2016 Tonya Bowers, MHS Acting Associate Administrator Bureau of Primary Health
PCA/HCCN Health Center Program Update National Association of Community Health Centers Community Health Institute August 30, 2016 Tonya Bowers, MHS Acting Associate Administrator Bureau of Primary Health
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017
 Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Tribal Recommendations to Integrate the Indian Health Care Delivery System Into Oregon s Coordinated Care Organizations (H.B.
 Tribal Recommendations to Integrate the Indian Health Care Delivery System Into Oregon s Coordinated Care Organizations (H.B. 3650) January 9, 2012 Executive Summary House Bill 3650 establishes the Oregon
Tribal Recommendations to Integrate the Indian Health Care Delivery System Into Oregon s Coordinated Care Organizations (H.B. 3650) January 9, 2012 Executive Summary House Bill 3650 establishes the Oregon