Donor Information Packet
|
|
|
- Claire Bradley
- 6 years ago
- Views:
Transcription
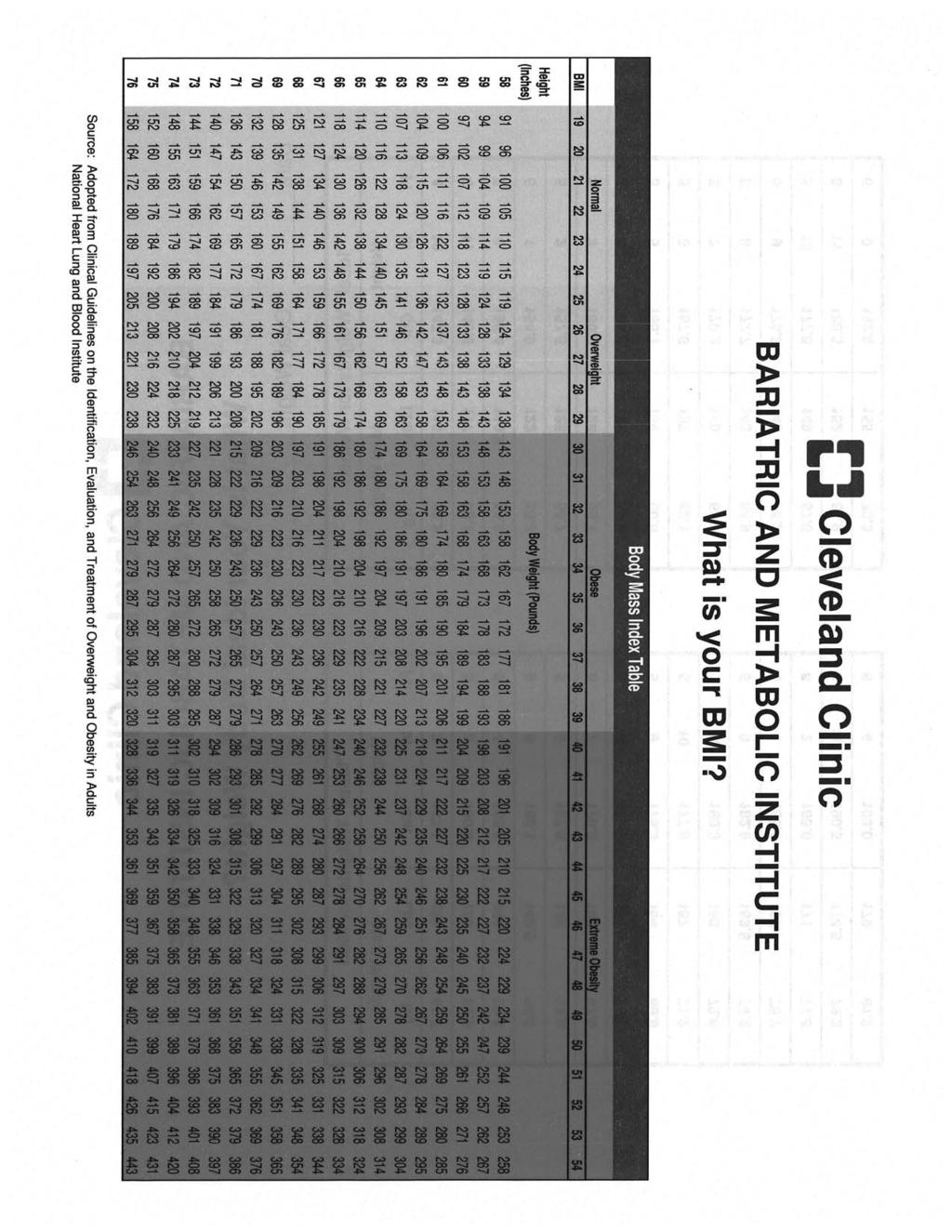
1 Donor Information Packet Thank you for your interest in Cleveland Clinic s. Body donation is a unique opportunity to leave a legacy that will truly have an impact on the future of medicine. As you read through the enclosed materials, you will find helpful information to aid you in making such an important decision. We also encourage you to visit our website at clevelandclinic.org/bodydonation. Of particular interest is the video message from the program s director and stories about our donors. If you decide that body donation is right for you, you can pre register with the program by completing the enclosed two page registration form and returning it to us via one of the methods noted below. Mail: Cleveland Clinic BodyDonation@ccf.org Fax: After we receive the completed form, it will be processed and an acknowledgement letter and donor cards will be mailed. You can expect to receive the information within a few weeks but if the situation is time sensitive, please let us know and we will provide it immediately. If you have questions, contact the program s administrative office at or at BodyDonation@ccf.org. Office hours are Monday through Friday from 8 a.m. to 5 p.m. We greatly appreciate your consideration. Enclosures: Answers to FAQs Brochure Registration Form Body Mass Index (BMI) Table



2 Answers to FAQs About the Program How many bodies does the program receive annually? In 2014 we received 168 body donations, and 421 people preregistered with the program. How are bodies used? Bodies are used for various medical education purposes, the advancement of medical science and research for the development of medical products and techniques. Will you make sure my organs go to someone in need? No, we do not handle organ donation. To find out more about organ donation, contact your local organ procurement organization. LifeBanc serves Northeast Ohio and can be reached at Can a body be donated for the study of a specific disease? No, we do not conduct disease-specific studies nor can we accept a body that is designated for such studies. Can the family receive a report specifying how the body was used? No, we do not provide verbal or written reports following studies. Conditions for Acceptance If I have an autopsy, will you accept my body? If the coroner determines that an autopsy is needed for an investigation and you are pre-registered with this program, we can accept the body following the autopsy. If you are not pre-registered with the program, we cannot accept the body. If the autopsy is elective, we cannot accept the body, regardless of registration status. If I donate organs, will you accept my body? If you are pre-registered with this program, the donation of most organs is allowable. The only exclusions are long bones and skin, which must be intact. If you have not pre-registered with this program, we cannot accept the body. Can you accept a body if death was caused by an accident, homicide or suicide? These situations are determined on a case-by-case basis. When Death Occurs What should we do if death occurs at home? If hospice is involved, contact them following the instructions they gave you. They will come to the home to pronounce death and make the proper notifications, including the report to us. If hospice is not involved, call 911. Who contacts the to report the death? Someone who is authorized to contact us, such as a nurse or first responder, should do so. We will obtain the required information and make sure the body is acceptable for donation. If the family contacts us, we will advise them how to proceed. What is the telephone number to report a death? The authorized representative (see above) should call and tell the operator they re calling to report a death for the. The operator will connect them to the appropriate person. Someone from the program is available 24 hours a day, 7 days a week. Survivor Concerns How will the body get to Cleveland Clinic? If death occurs within 100 miles of Cleveland Clinic s main campus (9500 Euclid Ave., ), we will make the transportation arrangements and cover the associated costs. The body will be transported as soon as possible, usually within a few hours depending upon time of day, distance and weather conditions. If death occurs outside the 100-mile range, transportation arrangements and costs are the responsibility of the donor/donor family. You may wish to contact a local funeral home in advance to discuss transportation options. Is there a cost or financial obligation to the survivors with regard to body donation? Cleveland Clinic assumes all costs except when the death occurs outside the 100-mile range, as mentioned above. Do we need the services of a funeral director to handle any portion of the body donation? Only if death occurs outside the 100-mile range, as mentioned above. Can we have a funeral when the body is donated? A traditional funeral is not possible but many families do have a memorial service, without the body present. Can we view the body after it arrives at Cleveland Clinic? No, family and friends must say their final farewells before the body is transported to Cleveland Clinic. How do we get the death certificate? We process the death certificate and then send it to the certifying physician or coroner. Upon completion, it is filed with and obtainable from the health department in the city (or county) where death occurred. How do we place an obituary in the newspaper? To place an obituary, contact the newspaper directly. They will need to verify certain details before the ad is placed. They can contact us, and we will confirm the information for them. Can the obituary acknowledge that the body was donated to the program? Yes. Some suggested language: NAME donated his/her body to the Cleveland Clinic for the advancement of medical science. Does the program accept monetary donations? We appreciatively accept monetary donations in memory of our donors. The donations are deposited into an account that supports the annual memorial service. Please make checks payable to Cleveland Clinic Education Institute and include the donor s name on the subject line. The mailing address is: Cleveland Clinic How do we contact the program? You can contact the program s administrative office at or at BodyDonation@ccf.org. Office hours are Monday through Friday from 8 a.m. to 5 p.m.


3 Annual Memorial Service A memorial service is held annually at Cleveland Clinic s main campus to honor the individuals whose bodies were received by the program during that year. The service usually takes place in May, and an invitation is mailed to each donor s representative about a month in advance. During the service, we celebrate together those who lived their lives with a spirit of generosity and service to others. We offer words of gratitude and remembrance, with the hope that as we celebrate these special people, their legacy will live on. Team Richard L. Drake, PhD Director, Director of Anatomy, Cleveland Clinic Lerner College of Medicine Jennifer M. McBride, PhD Associate Director, Director of Histology, Cleveland Clinic Lerner College of Medicine Lisa Gucwa Administrative Coordinator, Body Donation Program I want to express my sincere gratitude to you and your loved ones. Your loved ones gave us a priceless gift. They gave themselves. They gave themselves to help others by helping us. Through their donation they became our tutors. Sarah, Lerner College Class of 2015 Through selfless generosity, knowledge grows Questions? Please call or us at BodyDonation@ccf.org. Lake View Cemetery's Community Mausoleum clevelandclinic.org/bodydonation Education Institute

4 Why Donate Your Body People have a variety of reasons for wanting to donate their body to medical science. Many people do so because they value education. Often they are educators themselves. They appreciate the education they received when they were younger, and their commitment to paying it forward becomes their legacy. Simplify the Process by Pre-registering By pre-registering with the program, you are taking a practical approach to help ensure that your wishes will be met. You also simplify the process for your survivors. Simply complete the enclosed registration form and return it to us. Upon receipt, we will mail you an acknowledgement letter and donor cards. We will remember your generosity for years to come. Thank you for the gift to our training. Briana, Lerner College Class of 2018 Thank you for the incredible and selfless generosity that you and your loved ones have demonstrated though their donations. These gifts mean so much to us. Rachel, Lerner College Class of 2016 Others donate their bodies to medicine because they value medical care they personally received. For many, it was a treatment that worked, confirmation that medicine is evolving and that we re helping more people now than ever before. For others, it was a treatment that failed, a signal that we need to learn more, work harder. In either case, the value is in the medical breakthroughs that result when education, research and innovative thinking converge. And some are repaying a gift they received years before, having learned their way around the human body through the generosity of another. We cannot thank you and your loved ones enough for your tremendous contribution to our education. Andrew, Lerner College Class of 2017 Through your generosity and sacrifice, we have all been made better physicians. Your gift will benefit our patients for a lifetime. Thank you so much. Jason, Lerner College Class of 2016 Thank you for your lasting contribution to the next generation of physicians. Their gifts will not be forgotten. Rebecca, Lerner College Class of 2018 The human body is marvelous and, yes, mysterious. We may never learn everything there is to know about our bodies or how to treat every ailment that plagues us, but by advancing medical science and through the selfless generosity of donors, knowledge grows. If you pre-register with the program and later change your mind, just contact us. We will update our records to reflect that you have withdrawn from the program and then mail you a letter stating the same. They gave the last thing that they had to give. They paid it forward and so will we. Thank you. Jordan, Lerner College Class of 2017 General Conditions for Acceptance The minimum age for body donation is 18; there is no upper age limit. Prospective donors should pre-register with the program, as mentioned above. However, if someone dies without having pre-registered with the program, it is possible for the next of kin to donate the body. We cannot accept a body when there is: severe trauma (advanced decomposition, serious injury, septic shock) presence of an infectious disease such as hepatitis, HIV/AIDS, Creutzfeldt-Jakob disease, methicillin-resistant Staphylococcus aureus (MRSA) or clostridium difficile (C. diff) extreme obesity (BMI above 39) Other considerations: death must occur within the state of Ohio some limitations exist with regard to autopsy and organ donation (see answers to FAQs) some limitations exist with regard to cause of death (see answers to FAQs) During Our Studies The program maintains a securely locked anatomy laboratory. Bodies are treated with the utmost care and are always handled in a respectful and dignified manner. Studies could take anywhere between several weeks and 18 months. Upon completion, the remains are individually cremated. Cremated Remains When the ashes are ready for final disposition, we mail a notification letter to the donor s representative asking them to contact us regarding their wishes. The cremated remains can either be given to the family or interred in the program s niche at the historic Lake View Cemetery, an option we are pleased to offer, free of charge. The niche is located in the cemetery s Community Mausoleum, and the inscription reads Cleveland Clinic. A memorial stone, located at the mausoleum entrance, acknowledges our donors as well. Following interment, the burial record is accessible on the cemetery s website, and visitors have the option of sharing additional information, memories and photos. The cemetery itself is open to the public every day of the year.
5 Registration Form The information on this form is required for registration purposes and will ultimately be used for the death certificate. Please carefully complete the entire form. If an item is unknown or unobtainable, write that in the space; do not leave blank entries. Please keep your registration current by updating any information that changes. Select Type: New Registration Registration Update Donor s Full Legal Name Address City Number and Street Apartment/Unit or Village/Township State Zip County In City Limits? Yes No Phone Number Address (if applicable) Date of Birth / / Sex Male Female Social Security Number Month Day Year Birthplace City and State or Foreign Country Race (White, Black or African American, American Indian, etc.) Hispanic Origin? Yes No If yes, specify origin Marital Status Never married Married Married but separated Divorced Widowed Spouse s Name (if applicable) (prior to first marriage) Education 8 th grade or less 9 th 12 th, no diploma High School Graduate or GED College, but no degree Associate degree Bachelor s degree Master s degree Doctorate/Professional degree Occupation Business/Industry Type (prior to retirement) Ever Serve in the US Armed Forces? Yes No If yes, specify details Branch Air Force Army Coast Guard Department of Defense Marine Corps Navy Other Entry Date / / Separation/Discharge Date / / Month Day Year Month Day Year Separation/Discharge Type Honorable General Other Than Honorable Bad Conduct Dishonorable Father s Name Mother s Name (prior to first marriage) Next of Kin s Name Relationship Address City Number and Street Apartment/Unit or Village/Township State Zip County Phone Page 1 of 2
6 Disposition of Cremated Remains Upon completion of our studies, which could take anywhere between several weeks and 18 months, the remains are individually cremated. Please specify below your wishes regarding final disposition of the cremated remains. Placed in program s niche at Lake View Cemetery Assumed by next of kin Next of kin should decide when that time comes Health Information This item is optional and not required for registration. If you so wish, you may provide a brief overview of your health history. Donor s Consent I hereby instruct, in the presence of the following witnesses, that it is my desire to donate my body after death to Cleveland Clinic for teaching purposes, scientific research, or for such purposes as the authorized representatives of Cleveland Clinic shall, in their sole discretion, deem advisable. I understand that this form is not used for organ donation purposes and that a copy of this signed statement will be placed on file with Cleveland Clinic. My signature below indicates that the information on this form is accurate and true to the best of my knowledge. Donor s Printed Legal Name Signature Date Witnesses Two witnesses are required; they must be 18 years or older and not affiliated with Cleveland Clinic. Witness #1 can be any person you choose. Witness #2 must be a disinterested witness, meaning someone other than spouse, domestic partner, child, parent, sibling, grandchild, grandparent, or guardian of the individual who makes, amends, revokes, or refuses to make an anatomical gift; or another adult who exhibits special care and concern for the individual. We, the undersigned, have witnessed the signing of this document by the donor. Witness #1 Witness #2 Name Address City/State/Zip Signature Name Address City/State/Zip Signature Return the completed registration form to Cleveland Clinic by mail, or fax. Upon receipt, the form will be processed and the acknowledgement letter/donor cards will be mailed. If you have questions, contact the program s administrative office at BodyDonation@ccf.org or at Mail Cleveland Clinic BodyDonation@ccf.org Fax Do not write in the section below, for office use only. Date Received Date Processed THIS IS A LEGAL DOCUMENT UNDER THE UNIFORM ANATOMICAL GIFT ACT OR SIMILAR LAWS Page 2 of 2 Rev. 10/2016
7
Information on Donating Your Body to OHSU s Body Donation Program
 Information on Donating Your Body to OHSU s Body Donation Program About us: Founded in 1976, Oregon Health and Science University s Body Donation Program is the oldest non-profit whole body donation program
Information on Donating Your Body to OHSU s Body Donation Program About us: Founded in 1976, Oregon Health and Science University s Body Donation Program is the oldest non-profit whole body donation program
Forms Required for Anatomical Donation
 Forms Required for Anatomical Donation Vital Statistics Provides relevant information on the body donor as well as the name and address of the next-of-kin. Declaration of Consent In the event the body
Forms Required for Anatomical Donation Vital Statistics Provides relevant information on the body donor as well as the name and address of the next-of-kin. Declaration of Consent In the event the body
Bereavement and Resource Guide. University Medical Center New Orleans
 Bereavement and Resource Guide University Medical Center New Orleans WHEN YOUR LOVED ONE DIES The loss of a loved one, whether suddenly or following a long illness, is extremely difficult. The days that
Bereavement and Resource Guide University Medical Center New Orleans WHEN YOUR LOVED ONE DIES The loss of a loved one, whether suddenly or following a long illness, is extremely difficult. The days that
Anatomical GIFT PROGRAM. Elon University Anatomical Gift Program
 Anatomical GIFT PROGRAM Elon University Anatomical Gift Program WHY DONATE? Dissection and study of the human body constitutes an invaluable and indispensable part of healthcare education. Each year at
Anatomical GIFT PROGRAM Elon University Anatomical Gift Program WHY DONATE? Dissection and study of the human body constitutes an invaluable and indispensable part of healthcare education. Each year at
INFORMATION FOR DONORS
 INFORMATION FOR DONORS For those who in death have helped the living. This booklet is dedicated to the donors of the Joan C. Edwards School of Medicine at Marshall University The Human Gift Registry Room
INFORMATION FOR DONORS For those who in death have helped the living. This booklet is dedicated to the donors of the Joan C. Edwards School of Medicine at Marshall University The Human Gift Registry Room
Family Care Health Centers
 Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
CITY OF BRANDON POLICE DEPARTMENT APPLICATION FOR EMPLOYMENT. ALL applicants MUST attach items 1, 2, 3, 4 I. PERSONAL HISTORY
 CITY OF BRANDON POLICE DEPARTMENT APPLICATION FOR EMPLOYMENT MAIL OR DELIVER TO: THE CITY OF BRANDON 1000 MUNICIPAL DRIVE P.O. BOX 1539 BRANDON, MS 39043 ATTN: PERSONNEL Date: Notice: Application MUST
CITY OF BRANDON POLICE DEPARTMENT APPLICATION FOR EMPLOYMENT MAIL OR DELIVER TO: THE CITY OF BRANDON 1000 MUNICIPAL DRIVE P.O. BOX 1539 BRANDON, MS 39043 ATTN: PERSONNEL Date: Notice: Application MUST
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
Advance Directives. Advance Care Planning & Required Forms. Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s)
") Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s) Advance Directives Advance Care Planning & Required Forms Keep this document for your records and make copies for
Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s) Advance Directives Advance Care Planning & Required Forms Keep this document for your records and make copies for
Advance Directive. Durable Power of Attorney for Healthcare (Patient Advocate Designation)
") Advance Directive Durable Power of Attorney for Healthcare (Patient Advocate Designation) Introduction This document provides a way for an individual to create a Durable Power of Attorney for Healthcare
Advance Directive Durable Power of Attorney for Healthcare (Patient Advocate Designation) Introduction This document provides a way for an individual to create a Durable Power of Attorney for Healthcare
Patient Registration Form Pediatrics
 Patient Registration Form Pediatrics For Office Use Only: Visit Date: Initials: PATIENT INFORMATION Preferred Language: English Spanish Other: Patient s Last Name First Middle Initial Date of Birth Sex
Patient Registration Form Pediatrics For Office Use Only: Visit Date: Initials: PATIENT INFORMATION Preferred Language: English Spanish Other: Patient s Last Name First Middle Initial Date of Birth Sex
EMPLOYMENT APPLICATION
 EMPLOYMENT APPLICATION Page 1 of 3 This Employment Application will remain active for one year from the date of completion APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State
EMPLOYMENT APPLICATION Page 1 of 3 This Employment Application will remain active for one year from the date of completion APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State
Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT. I,, (name) designate and appoint: (name of agent) (address)
 designate and appoint: (name of agent) (address)") INSTRUCTIONS KANSAS ADVANCE DIRECTIVE PAGE 1 OF 5 Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT PRINT YOUR NAME PRINT THE NAME, ADDRESS, AND TELEPHONE NUMBERS
INSTRUCTIONS KANSAS ADVANCE DIRECTIVE PAGE 1 OF 5 Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT PRINT YOUR NAME PRINT THE NAME, ADDRESS, AND TELEPHONE NUMBERS
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
EAST OHIO CONFERENCE JOHN M. ROSEBERRY COMMISSION ON RELIGION AND RACE SCHOLARSHIP GRANT SCHOLARSHIP APPLICATION
 EAST OHIO CONFERENCE JOHN M. ROSEBERRY COMMISSION ON RELIGION AND RACE SCHOLARSHIP GRANT WHAT? SCHOLARSHIP APPLICATION WHO IS ELIGIBLE? ANY RACIAL ETHNIC COLLEGE BOUND STUDENT WHO IS A MEMBER OF A LOCAL
EAST OHIO CONFERENCE JOHN M. ROSEBERRY COMMISSION ON RELIGION AND RACE SCHOLARSHIP GRANT WHAT? SCHOLARSHIP APPLICATION WHO IS ELIGIBLE? ANY RACIAL ETHNIC COLLEGE BOUND STUDENT WHO IS A MEMBER OF A LOCAL
Advance Directive. my wish for: my voice my choice. health care power of attorney and living will
 health care power of attorney and living will print your name date of birth for information contact: patient relations at 910 615-6120 my voice my choice. my wish for: The person I want to make care decisions
health care power of attorney and living will print your name date of birth for information contact: patient relations at 910 615-6120 my voice my choice. my wish for: The person I want to make care decisions
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Health Care Proxy Appointing Your Health Care Agent in New York State
 Health Care Proxy Appointing Your Health Care Agent in New York State The New York Health Care Proxy Law allows you to appoint someone you trust for example, a family member or close friend to make health
Health Care Proxy Appointing Your Health Care Agent in New York State The New York Health Care Proxy Law allows you to appoint someone you trust for example, a family member or close friend to make health
HEALTH CARE POWER OF ATTORNEY
 HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
CALIFORNIA Advance Directive Planning for Important Health care Decisions
 CALIFORNIA Advance Directive Planning for Important Health care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
CALIFORNIA Advance Directive Planning for Important Health care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Vermont Advance Directive for Health Care
 Vermont Advance Directive for Health Care Prepared by the Vermont Ethics Network Explanation and Instructions You have the right to give instructions about what types of health care you want or do not
Vermont Advance Directive for Health Care Prepared by the Vermont Ethics Network Explanation and Instructions You have the right to give instructions about what types of health care you want or do not
GEORGIA Advance Directive Planning for Important Health Care Decisions
 GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
Georgia Advance Directive for Health Care
 Georgia Advance Directive for Health Care By: (Print Name) Date of Birth: (Month/Day/Year) This advance directive for health care has four parts: PART ONE PART TWO PART THREE HEALTH CARE AGENT. This part
Georgia Advance Directive for Health Care By: (Print Name) Date of Birth: (Month/Day/Year) This advance directive for health care has four parts: PART ONE PART TWO PART THREE HEALTH CARE AGENT. This part
Mobile Mammo Registration Instructions
 Mobile Mammo Registration Instructions 1. Call to schedule your appointment @ 239-936-4068 2. Fill out the following forms Note: All forms must be completed even if you were a previous patient on RRC Mobile
Mobile Mammo Registration Instructions 1. Call to schedule your appointment @ 239-936-4068 2. Fill out the following forms Note: All forms must be completed even if you were a previous patient on RRC Mobile
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS ADMISSION PACKET
 SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS 62992 ADMISSION PACKET LETTER AND ADMISSION PROCEDURE FOR PRACTICAL NURSING PROGRAM. COMPLETED APPLICATIONS FOR THE FALL 2016 PRACTICAL NURSING PROGRAM CAN BE
SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS 62992 ADMISSION PACKET LETTER AND ADMISSION PROCEDURE FOR PRACTICAL NURSING PROGRAM. COMPLETED APPLICATIONS FOR THE FALL 2016 PRACTICAL NURSING PROGRAM CAN BE
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Southwest Florida Public Service Academy 4312 E. Michigan Ave. Ft. Myers FL Tel: (239) Fax: (239)
 Fax: (239)") Southwest Florida Public Service Academy 4312 E. Michigan Ave. Ft. Myers FL 33905 Tel: (239) 334-3897 Fax: (239) 334-8794 Todd Everly, Director Robert Martin III, Corrections Coordinator Jack Thomson,
Southwest Florida Public Service Academy 4312 E. Michigan Ave. Ft. Myers FL 33905 Tel: (239) 334-3897 Fax: (239) 334-8794 Todd Everly, Director Robert Martin III, Corrections Coordinator Jack Thomson,
Instruction Sheet for Completing Health Care Power of Attorney/Living Will (Please discard instruction sheet after completion of document)
") Instruction Sheet for Completing Health Care Power of Attorney/Living Will (Please discard instruction sheet after completion of document) Overview The attached Power of Attorney for Health Care form is
Instruction Sheet for Completing Health Care Power of Attorney/Living Will (Please discard instruction sheet after completion of document) Overview The attached Power of Attorney for Health Care form is
Fall Dear Students, Parents and Guardians,
 Fall 2018 Dear Students, Parents and Guardians, Thank you for your interest in the Student/Partner Alliance (S/PA) scholarship program. Our scholarship is intended for motivated students who have already
Fall 2018 Dear Students, Parents and Guardians, Thank you for your interest in the Student/Partner Alliance (S/PA) scholarship program. Our scholarship is intended for motivated students who have already
HAMILTON COUNTY SHERIFF S OFFICE 1000 SYCAMORE STREET, ROOM 110 CINCINNATI, OHIO OR HAMILTON AVE, PATROL HEADQUARTERS
 HAMILTON COUNTY SHERIFF S OFFICE 1000 SYCAMORE STREET, ROOM 110 CINCINNATI, OHIO 45202 OR 11021 HAMILTON AVE, 45231 PATROL HEADQUARTERS POSITION APPLIED FOR DATE THE HAMILTON COUNTY SHERIFF S OFFICE CONSIDERS
HAMILTON COUNTY SHERIFF S OFFICE 1000 SYCAMORE STREET, ROOM 110 CINCINNATI, OHIO 45202 OR 11021 HAMILTON AVE, 45231 PATROL HEADQUARTERS POSITION APPLIED FOR DATE THE HAMILTON COUNTY SHERIFF S OFFICE CONSIDERS
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE
 YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
What to do when a Veteran Passes Away
 What to do when a Veteran Passes Away This is some good information you may want to print it out and put in a safe place for your spouse or family members. Over the weekend I received a call from the wife
What to do when a Veteran Passes Away This is some good information you may want to print it out and put in a safe place for your spouse or family members. Over the weekend I received a call from the wife
Lives (circle one): in assisted living with a relative alone
: in assisted living with a relative alone") Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Frequently Asked Questions and Forms
 1-877-209-8086 www.wvendoflife.org Advance Directives for Health Care Decision-Making in West Virginia Frequently Asked Questions and Forms FORMS INSIDE: Living Will - Medical Power of Attorney Combined
1-877-209-8086 www.wvendoflife.org Advance Directives for Health Care Decision-Making in West Virginia Frequently Asked Questions and Forms FORMS INSIDE: Living Will - Medical Power of Attorney Combined
ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL")
") ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL") NOTE: YOU SHOULD USE THIS DOCUMENT TO GIVE YOUR HEALTH CARE PROVIDERS INSTRUCTIONS TO WITHHOLD OR WITHDRAW LIFE-PROLONGING MEASURES IN CERTAIN SITUATIONS.
ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL") NOTE: YOU SHOULD USE THIS DOCUMENT TO GIVE YOUR HEALTH CARE PROVIDERS INSTRUCTIONS TO WITHHOLD OR WITHDRAW LIFE-PROLONGING MEASURES IN CERTAIN SITUATIONS.
Georgia Advance Directive for Healthcare
 Navicent Health Georgia Advance Directive for Healthcare GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) PART ONE HEALTH CARE AGENT This part allows you to choose
Navicent Health Georgia Advance Directive for Healthcare GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) PART ONE HEALTH CARE AGENT This part allows you to choose
HAMILTON COUNTY SHERIFF S OFFICE SPECIAL DEPUTY APPLICATION
 HAMILTON COUNTY SHERIFF S OFFICE SPECIAL DEPUTY APPLICATION The classification of Special Deputy is a voluntary, non-compensated position affiliated with the Sheriff s Office and requires the individual
HAMILTON COUNTY SHERIFF S OFFICE SPECIAL DEPUTY APPLICATION The classification of Special Deputy is a voluntary, non-compensated position affiliated with the Sheriff s Office and requires the individual
Advance Directive. including Power of Attorney for Health Care
 Advance Directive including Power of Attorney for Health Care Overview This is a legal document, developed to meet the legal requirements for Wisconsin. This document provides a way for a person to create
Advance Directive including Power of Attorney for Health Care Overview This is a legal document, developed to meet the legal requirements for Wisconsin. This document provides a way for a person to create
CITY OF PLANT CITY 302 W. REYNOLDS STREET P. O. BOX C PLANT CITY, FLORIDA PHONE (813)
") CITY OF PLANT CITY 302 W. REYNOLDS STREET P. O. BOX C PLANT CITY, FLORIDA 33564 PHONE (813) 659-4200 DATE: Your application will be removed from active status one year from this date. Name: Position &
CITY OF PLANT CITY 302 W. REYNOLDS STREET P. O. BOX C PLANT CITY, FLORIDA 33564 PHONE (813) 659-4200 DATE: Your application will be removed from active status one year from this date. Name: Position &
CALIFORNIA Advance Directive Planning for Important Health Care Decisions
 CALIFORNIA Advance Directive Planning for Important Health Care Decisions Caring Info 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National
CALIFORNIA Advance Directive Planning for Important Health Care Decisions Caring Info 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National
WEST VIRGINIA Advance Directive Planning for Important Health Care Decisions
 WEST VIRGINIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
WEST VIRGINIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Give Kids A Chance 150 West Flagler Street Suite 2200 Miami, Florida 33130
 Executive Director: Brian J. McDonough Give Kids A Chance 150 West Flagler Street Suite 2200 Miami, Florida 33130 SCHOLARSHIP CRITERIA Give Kids A Chance is offering scholarship grants in the amount of
Executive Director: Brian J. McDonough Give Kids A Chance 150 West Flagler Street Suite 2200 Miami, Florida 33130 SCHOLARSHIP CRITERIA Give Kids A Chance is offering scholarship grants in the amount of
Citrus County Tax Collector s Office Application for Employment
 Citrus County Tax Collector s Office Application for Employment We are an equal opportunity employer and do not unlawfully discriminate in employment. No question on this application is used for the purpose
Citrus County Tax Collector s Office Application for Employment We are an equal opportunity employer and do not unlawfully discriminate in employment. No question on this application is used for the purpose
Advance Directive Durable Power of Attorney for Healthcare-Living Will For Name Date of Birth Address City/State/Zip: Phone #
 Advance Directive Durable Power of Attorney for Healthcare-Living Will For Name Date of Birth Address City/State/Zip: Phone # On Document Preparation Date: Part I: Choosing a Healthcare Agent to make my
Advance Directive Durable Power of Attorney for Healthcare-Living Will For Name Date of Birth Address City/State/Zip: Phone # On Document Preparation Date: Part I: Choosing a Healthcare Agent to make my
For more information and additional resources go to Name:
 Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
ADVANCE MEDICAL DIRECTIVES
 Advance Directives ADVANCE MEDICAL DIRECTIVES The "Montana Rights of the Terminally Ill Act" (also known as the Montana Living Will Act") allows individuals the maximum possible control over their own
Advance Directives ADVANCE MEDICAL DIRECTIVES The "Montana Rights of the Terminally Ill Act" (also known as the Montana Living Will Act") allows individuals the maximum possible control over their own
NEBRASKA Advance Directive Planning for Important Health Care Decisions
 NEBRASKA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
NEBRASKA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
MICHIGAN Advance Directive Planning for Important Health Care Decisions
 MICHIGAN Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
MICHIGAN Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
MARYLAND Advance Directive Planning for Important Healthcare Decisions
 MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Info 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Info 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
Rural Electric Cooperative s 2018 Scholarship Program. Deadline Monday, February 12, 2018
 Rural Electric Cooperative s 2018 Scholarship Program Deadline Monday, February 12, 2018 Purpose 1. To provide assistance to high school seniors to further their education. 2. To promote understanding,
Rural Electric Cooperative s 2018 Scholarship Program Deadline Monday, February 12, 2018 Purpose 1. To provide assistance to high school seniors to further their education. 2. To promote understanding,
NAME SS# ADDRESS CITY STATE ZIP. TELEPHONE (home) (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE
 (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE") REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
PROFILE OF THE MILITARY COMMUNITY
 2004 DEMOGRAPHICS PROFILE OF THE MILITARY COMMUNITY Acknowledgements ACKNOWLEDGEMENTS This report is published by the Office of the Deputy Under Secretary of Defense (Military Community and Family Policy),
2004 DEMOGRAPHICS PROFILE OF THE MILITARY COMMUNITY Acknowledgements ACKNOWLEDGEMENTS This report is published by the Office of the Deputy Under Secretary of Defense (Military Community and Family Policy),
A PERSONAL DECISION
 A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION
 Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Application Requirements to be considered for Approval:
 338 Grapevine Hwy. Hurst, Texas 76054 phone: 817.503.1500 toll-free: 877.203.9111 fax: 817.503.1551 www.mhstx.org Application Requirements to be considered for Approval: Please print your answers using
338 Grapevine Hwy. Hurst, Texas 76054 phone: 817.503.1500 toll-free: 877.203.9111 fax: 817.503.1551 www.mhstx.org Application Requirements to be considered for Approval: Please print your answers using
To Whom It May Concern: Enclosed is the Power of Attorney for Health Care form which you requested.
 DIVISION OF PUBLIC HEALTH 1 WEST WILSON STREET P O BOX 2659 Jim Doyle MADISON WI 53701-2659 Governor State of Wisconsin 608-266-1251 Helene Nelson FAX: 608-267-2832 Secretary Department of Health and Family
DIVISION OF PUBLIC HEALTH 1 WEST WILSON STREET P O BOX 2659 Jim Doyle MADISON WI 53701-2659 Governor State of Wisconsin 608-266-1251 Helene Nelson FAX: 608-267-2832 Secretary Department of Health and Family
MARYLAND Advance Directive Planning for Important Healthcare Decisions
 MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT
 TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
Form B - For those enrolled in other insurance
 Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Teddy Forstmann Scholarship Program Application Instructions
 2015-2016 Application Instructions APPLICATION DEADLINE: FRIDAY, AUGUST 21, 2015,,. Applications postmarked AFTER this deadline may not be awarded. Please be sure to keep in contact regularly with your
2015-2016 Application Instructions APPLICATION DEADLINE: FRIDAY, AUGUST 21, 2015,,. Applications postmarked AFTER this deadline may not be awarded. Please be sure to keep in contact regularly with your
Captain Jennifer J. Harris, USMC Memorial Scholarship
 The Harris Family Presents The 2017 Captain Jennifer J. Harris, USMC Memorial Scholarship JROTC for College or Military Expenses Amount $1,000 Due Date May 8, 2017 Send to Captain Jennifer J. Harris, USMC
The Harris Family Presents The 2017 Captain Jennifer J. Harris, USMC Memorial Scholarship JROTC for College or Military Expenses Amount $1,000 Due Date May 8, 2017 Send to Captain Jennifer J. Harris, USMC
Durable Power of Attorney for Health Care and Health Care Directive
 Durable Power of Attorney for Health Care and Health Care Directive and HIPAA Privacy Authorization Form Frequently Asked Questions and Answers, Instructions, and Forms Distributed as a public service
Durable Power of Attorney for Health Care and Health Care Directive and HIPAA Privacy Authorization Form Frequently Asked Questions and Answers, Instructions, and Forms Distributed as a public service
REVISED 2005 EDITION. A Personal Decision
 REVISED 2005 EDITION A Personal Decision Practical information about determining your future medical care, including living wills, powers of attorney for health care, mental health treatment preference
REVISED 2005 EDITION A Personal Decision Practical information about determining your future medical care, including living wills, powers of attorney for health care, mental health treatment preference
REVISOR ACF/JP A
 1.1... moves to amend S.F. No. 3656, the second engrossment, in conference 1.2 committee, as follows: 1.3 Page 406, delete article 25 and insert: 1.4 "ARTICLE 25 1.5 HEALTH-RELATED LICENSING BOARDS 1.6
1.1... moves to amend S.F. No. 3656, the second engrossment, in conference 1.2 committee, as follows: 1.3 Page 406, delete article 25 and insert: 1.4 "ARTICLE 25 1.5 HEALTH-RELATED LICENSING BOARDS 1.6
Filer Police Department 300 Main Street Office: P.O. Box 140 Dispatch: Filer, Idaho Fax:
 Filer Police Department 300 Main Street Office: 208 326-4123 P.O. Box 140 Dispatch: 208 735-1911 Filer, Idaho 83328 Fax: 208 326-5004 www.cityoffiler.com 911 Emergency EQUAL OPPORTUNITY EMPLOYER Prospective
Filer Police Department 300 Main Street Office: 208 326-4123 P.O. Box 140 Dispatch: 208 735-1911 Filer, Idaho 83328 Fax: 208 326-5004 www.cityoffiler.com 911 Emergency EQUAL OPPORTUNITY EMPLOYER Prospective
Health Care Directives
 Fact Sheet Health Care Directives What is a Health Care Directive? A Health Care Directive is a document that lets you leave instructions about your health care and name a Health Care Agent. A Health Care
Fact Sheet Health Care Directives What is a Health Care Directive? A Health Care Directive is a document that lets you leave instructions about your health care and name a Health Care Agent. A Health Care
SANTA FE STRONG VICTIMS FUND FINAL PROTOCOL. July 24, 2018
 SANTA FE STRONG VICTIMS FUND FINAL PROTOCOL July 24, 2018 The May 18 th attack at Santa Fe High School was an atrocity that has devastated our community. This unspeakable act of evil has been countered
SANTA FE STRONG VICTIMS FUND FINAL PROTOCOL July 24, 2018 The May 18 th attack at Santa Fe High School was an atrocity that has devastated our community. This unspeakable act of evil has been countered
SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS ADMISSION PACKET
 SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS 62992 ADMISSION PACKET LETTER AND ADMISSION PROCEDURE FOR ASSOCIATE DEGREE NURSING PROGRAM COMPLETED APPLICATIONS FOR THE 2017 ADN PROGRAM CAN BE SUBMITTED TO
SHAWNEE COMMUNITY COLLEGE ULLIN, ILLINOIS 62992 ADMISSION PACKET LETTER AND ADMISSION PROCEDURE FOR ASSOCIATE DEGREE NURSING PROGRAM COMPLETED APPLICATIONS FOR THE 2017 ADN PROGRAM CAN BE SUBMITTED TO
NJ Sharing Network Foundation Presents Scholarships for
 NJ Sharing Network Foundation Presents Scholarships for 2017-18 NJ Sharing Network Foundation is pleased to announce the availability of two (2) scholarships, the Missy s Miracle Scholarship and the Betsy
NJ Sharing Network Foundation Presents Scholarships for 2017-18 NJ Sharing Network Foundation is pleased to announce the availability of two (2) scholarships, the Missy s Miracle Scholarship and the Betsy
NORTH CAROLINA Advance Directive Planning for Important Health Care Decisions
 NORTH CAROLINA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National
NORTH CAROLINA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Table of Contents. Note from the Editor
 Note from the Editor This "Survivors Guide" in no way can answer all the questions that can arise in the event of a death of a loved one. Rather it is provided to assist you in finding the answers and
Note from the Editor This "Survivors Guide" in no way can answer all the questions that can arise in the event of a death of a loved one. Rather it is provided to assist you in finding the answers and
L e g a l I s s u e s i n H e a l t h C a r e
 Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
Summer Youth Employment Program Application Packet for 2018 for Youth Ages 14-24
 KAWERAK, INC. Education, Employment, and Supportive Services Summer Youth Employment Program P.O. Box 948 Nome, AK 99762 Phone: 907-443-4351 Toll Free: 1-800-450-4341 Fax: 907-443-4485 or 907-443-4479
KAWERAK, INC. Education, Employment, and Supportive Services Summer Youth Employment Program P.O. Box 948 Nome, AK 99762 Phone: 907-443-4351 Toll Free: 1-800-450-4341 Fax: 907-443-4485 or 907-443-4479
Signature: Signed by GNT Date Signed: 05/26/2015
 Atlanta Police Department Policy Manual Standard Operating Procedure Effective Date: June 1, 2015 Applicable To: All employees Approval Authority: Chief George N, Turner Signature: Signed by GNT Date Signed:
Atlanta Police Department Policy Manual Standard Operating Procedure Effective Date: June 1, 2015 Applicable To: All employees Approval Authority: Chief George N, Turner Signature: Signed by GNT Date Signed:
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
August 19-24, 2014 (Tuesday-Sunday)
") What is EDGE Adventure Camp? A five day Catholic camp with sports & activities including canoeing, kayaking, giant rope swing, water sports and more! Live music, catechesis, Mass, praise & worship and
What is EDGE Adventure Camp? A five day Catholic camp with sports & activities including canoeing, kayaking, giant rope swing, water sports and more! Live music, catechesis, Mass, praise & worship and
COLORADO Advance Directive Planning for Important Health Care Decisions
 COLORADO Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
COLORADO Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Health Care Directive
 Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
INSTRUCTIONS FOR YOUR CALIFORNIA ADVANCE HEALTH CARE DIRECTIVE
 California maintains an Advance Directive Registry. By filing your advance directive with the registry, your health care provider and loved ones may be able to find a copy of your directive in the event
California maintains an Advance Directive Registry. By filing your advance directive with the registry, your health care provider and loved ones may be able to find a copy of your directive in the event
Planning Ahead: How to Make Future Health Care Decisions NOW. Washington
 Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Fundraising for CFC International
 Fundraising for CFC International Improving the quality of life through family support, research, and education Thank you for expressing interest in conducting a fundraiser to raise money for CFC International.
Fundraising for CFC International Improving the quality of life through family support, research, and education Thank you for expressing interest in conducting a fundraiser to raise money for CFC International.
Hillside Memorial Park and Mortuary Advance Health Care Directive
 Hillside Memorial Park and Mortuary Advance Health Care Directive Advance Health Care Directive This booklet lets you name another individual as an agent to make health care decisions for you if you are
Hillside Memorial Park and Mortuary Advance Health Care Directive Advance Health Care Directive This booklet lets you name another individual as an agent to make health care decisions for you if you are
Directive to Physicians and Family or Surrogates Advance Directives Act (see , Health and Safety Code) Directive
 Directive") Directive to Physicians and Family or Surrogates Advance Directives Act (see 166.033, Health and Safety Code) This is an important legal document known as an Advance Directive. It is designed to help you
Directive to Physicians and Family or Surrogates Advance Directives Act (see 166.033, Health and Safety Code) This is an important legal document known as an Advance Directive. It is designed to help you
Department of Defense DIRECTIVE
 Department of Defense DIRECTIVE NUMBER 1350.4 April 28, 2001 Certified Current as of December 1, 2003 SUBJECT: Legal Assistance Matters Incorporating Change 1, June 13, 2001 USD(P&R) Reference: (a) Title
Department of Defense DIRECTIVE NUMBER 1350.4 April 28, 2001 Certified Current as of December 1, 2003 SUBJECT: Legal Assistance Matters Incorporating Change 1, June 13, 2001 USD(P&R) Reference: (a) Title
Delta Phi Chi Military Sorority, Inc.
 Delta Phi Chi Military Sorority, Inc. 2018 Application Checklist COMPLETED APPLICATION (5 Pages) PHOTO ID-Front & Back (Ensure PII is concealed) DD 214-Discharged Applicants (Ensure PII is concealed) Military
Delta Phi Chi Military Sorority, Inc. 2018 Application Checklist COMPLETED APPLICATION (5 Pages) PHOTO ID-Front & Back (Ensure PII is concealed) DD 214-Discharged Applicants (Ensure PII is concealed) Military
HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed.
 Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
NEW PATIENT PACKET. Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone. Address: Driver s License #:
 Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Adventure Club. Before and After School Care Enrollment Packet. Before and After School Care Mission:
 Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Signature (Patient or Legal Guardian): Date:
: Date:") X-Ray Patient Information: [ ] Male [ ] Female Patient Name: Date of Birth: / / SS#: Mailing Address: City: State: Zip: Phone # s: (Home) (Work) (Cell) Referring Physician: Phone #: /Fax#: Additional Physician:
X-Ray Patient Information: [ ] Male [ ] Female Patient Name: Date of Birth: / / SS#: Mailing Address: City: State: Zip: Phone # s: (Home) (Work) (Cell) Referring Physician: Phone #: /Fax#: Additional Physician:
CONNECTICUT Advance Directive Planning for Important Health Care Decisions
 CONNECTICUT Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
CONNECTICUT Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
714 Beacon Street, Newton Centre, MA,
 Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Parent/Guardian Names: Cell Phone: School: Parent/Guardian Signature: Date:
 SPIRIT OF AMERICA BOATING SAFETY PROGRAM Offered by Sailing Center Chesapeake & St. Mary s College of Maryland Open to students who have completed 6 th, 7 th, or 8 th grades in 2017. Summer 2017 Student
SPIRIT OF AMERICA BOATING SAFETY PROGRAM Offered by Sailing Center Chesapeake & St. Mary s College of Maryland Open to students who have completed 6 th, 7 th, or 8 th grades in 2017. Summer 2017 Student
Admission Requirements
 Admission Requirements All Applicants: ATI TEAS V entrance exam is required for ALL applicants in addition the requirements listed below. Applicants must have at least a 60% Adjusted Individual Total Score
Admission Requirements All Applicants: ATI TEAS V entrance exam is required for ALL applicants in addition the requirements listed below. Applicants must have at least a 60% Adjusted Individual Total Score
II. How strictly I want my agent to follow my instructions:
 MY HEALTH CARE CHOICES (OPTIONAL SUPPLEMENT) 1 of 4 Personal Health Care Instructions Communication Form Name: Kaiser MRN#: I. How much I want to know about my condition: (Please mark statement 1 or 2.)
MY HEALTH CARE CHOICES (OPTIONAL SUPPLEMENT) 1 of 4 Personal Health Care Instructions Communication Form Name: Kaiser MRN#: I. How much I want to know about my condition: (Please mark statement 1 or 2.)
HEALTH CARE DIRECTIVE
 1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
MASSACHUSETTS ADVANCE DIRECTIVES
 MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
AMERICAN AMBULANCE SERVICE, INC.
 AMERICAN AMBULANCE SERVICE, INC. Proud to be a tobacco and smoke-free environment ONE AMERICAN WAY, NORWICH, CT 06360 VOLUNTEER APPLICATION GENERAL INFORMATION Date Name Last First MI Address Street City
AMERICAN AMBULANCE SERVICE, INC. Proud to be a tobacco and smoke-free environment ONE AMERICAN WAY, NORWICH, CT 06360 VOLUNTEER APPLICATION GENERAL INFORMATION Date Name Last First MI Address Street City