Prevention of Retained: Small Miscellaneous Items (SMIs) Unretrieved Device Fragments (UDFs) Needles
|
|
|
- Moses Hubbard
- 6 years ago
- Views:
Transcription

1 Prevention of Retained: Small Miscellaneous Items (SMIs) Unretrieved Device Fragments (UDFs) Needles Verna C. Gibbs MD Director, NoThing Left Behind Professor of Surgery UCSF; Staff Surgeon, SFVAMC
2 This FREE webinar is sponsored by a TWO YEAR ( ) CALIFORNIA COLLABORATIVE IN SURGICAL PATIENT SAFETY
3 Ground Rules This presentation is intended to be a job aide The goal is to help participants clarify their thinking which should lead to clearer and stronger actions Policy translation is site specific Predicated on the use of the Sponge ACCOUNTing System
4 Four Classes of Items 1. Soft Goods a) Surgical Sponges* b) Surgical Towels* c) Dressing sponges, Towels, Packs, Prep Swabs, Gauze pledgets 2. Small Miscellaneous Items (SMI) includes parts of instruments 3. Sharps/Needles 4. Instruments (the whole instrument) *cotton soft goods that contain a radiopaque marker for X-ray detection


5 Retained Surgical Items
6 National Quality Forum Serious Reportable Events (SRE) 2011 Update Event Unintended retention of a foreign object in a patient after surgery or other invasive procedure Applicable Settings: Hospitals Outpatient/Officebased Surgery Centers Ambulatory Practice Settings/ Office-based Practices Long-term Care/ Skilled Nursing Facilities Additional Specifications Includes medical or surgical items intentionally placed by provider(s) that are unintentionally left in place Excludes: a) objects present prior to surgery or other invasive procedure that are intentionally left in place; b) objects intentionally implanted as part of a planned intervention and; c) objects not present prior to surgery/procedure that are intentionally left in when the risk of removal exceeds the risk of retention (such as microneedles, broken screws) Implementation Guidance This event is intended to capture: Occurrences of unintended retention of objects at any point after the surgery/ procedure ends regardless of setting (post anesthesia recovery unit, surgical suite, emergency department, patient bedside) and regardless of whether the object is to be removed after discovery Unintentionally retained objects (including such things as wound packing material, sponges, catheter tips, trocars, guide wires) in all applicable settings
7 When is it Retained? It s considered to be retained if the item is in the patient! AFTER SURGERY When is it after surgery?
8 After Surgery is After all incisions have been closed in their entirety Devices have been removed Final surgical counts have concluded Patient has been taken from the operating/procedure room
9 Small Miscellaneous Items Small Miscellaneous Items and Unretrieved Device Fragments (UDFs) are frequently retained Increasingly reported! 70% of retained items in the Minnesota Hospital Association reports! 50% of items from the California Dept of Public Health! Majority of items from California Hospital Patient Safety Organization voluntary reporting system! Probably the second most common item other places (e.g. Pennsylvania, VA reports) have been bundled in the instrument category
10 The California Story CDPH reports from 10/25/ /24/2013 (7 years) where hospitals received administrative penalties of $25,000 - $100, Retained Surgical Item cases 43 cases involving Soft Goods 28 laps ; 12 raytex; 3 towels (1 ROT) 23 cases of Small Miscellaneous Items and UDFs 9 cases of a retained Instrument (56% are visceral retractors)
11 SMI Data Project Collaboration with CHPSO Reports are Patient Safety Work Product! Confidential! Privileged! Deidentified Illinois, Michigan, Missouri, Nebraska, North Carolina, California, Tennessee participated ended October 2012 Together with data from NLB sources there are 105 cases
12 Observations Problems with the quality of reporting insufficient information provided ~20% had no info [13/67] Of material cases, 54% had a retained SMI/UDF [29/54] 10/54 cases;18% were near miss but the information provided was so sketchy often difficult to discern
13 Observations In this series, Orthopedic surgeons had 38% of the UDF s followed by vascular proceduralists leaving guidewires, sheaths, stents and parts of wires and sheaths in vascular spaces. It was difficult to determine how many of these items were removed
14 Retained Items Guidewires, portions of vascular sheaths, introducers, stents 2.5 foot plastic drape 2.5 cm temporary neck pin stapler head in rectum 1x8" xeroform gauze ring band sizer for heart valve sizing Raney clips blade extender electrocautery tip tip of Bullard laryngoscope 8x5mm metal screw cap 3.5 cm piece of lumbar drain catheter Piece of screwdriver head retractor blade patellar protector metal portion of Heart String device piece of Rhotan dissector 2-4mm drill bits x 10 cases Suture sleeve of AICD lead 4 cm portion of fetal scalp electrode 5mm tip of right angle clamp piece of Weck cell sphere plastic tip of bipolar device endoscopic anti-fog solution bottle Steinman pin Breakaway part of lami bolt Part from Capio device Portion of uterine manipulator Nasal suction bulb
15 Interesting Findings Needles are the most frequently miscounted items in the OR yet very few reports of retained needles Under-reporting of retention or just miscounted? Objects post laparoscopic hysterectomy retained in the vagina increasingly reported
16 California AP events 7 years of public reporting currently includes cases from only 5 years reports = 15 cases/year! 43 cases (57%) soft goods 11/43 (26%) Ob 7 > Gyn 4 cases 28 laps; 12 raytex; 3 towels! 23 cases (31%) SMI+UDFs! 9 cases (12%) instruments! 0 cases sharps
17 CDPH 2011 FOIA request by CHPSO 114 releasable reports! 52 (46%) no information! 8 not RSI cases + no info = 53%! 26 (23%) soft goods! 19 (17%) UDFs! 7 (6%)SMI + UDFs = 23%! 2 retained sharps (1 needle/1 blade)! 0 instruments
18 UHC 2011 University Health Consortium 100 academic medical centers 428 RSI* reports! 171 (40%)UDFs! 137 (32%) soft goods! 77 (18%) Instruments (I doubt this! more likely SMI s + Instruments) + UDFs = 58%! 43 (10%) sharps *TJC definition Williams, JACS Sept 2014
19 NLB Vernacular Two Types of Case based on LOCATION of event I. OR CASES a. Radiopaque items b. Non-Radiopaque items II. Non-OR CASES
20 OR Cases Radiopaque Items Screws, bolts, parts of retractors Wires, baskets Drill bits, metallic fragments Stapler heads, suction tips NLB Vernacular
21 Radiopaque Items Identify early if something is missing Usually will be the scrub person! the circulating nurse is out of the field! the surgeon is focused on operation! discovery in SPD is too late Obtain an intraoperative x-ray Usually can find and retrieve these items Recognition is key
22 OR Cases Non-Radiopaque Items Plastic trocars, vessel loops, Rubber stoppers, flanges, eye protectors Tips from tunneling devices Pieces of wood NLB Vernacular
23 Non- Radiopaque Items Identify early if something is missing Usually will be the scrub person! the circulating nurse is out of the field! the surgeon is focused on operation! discovery in SPD is too late Obtain an intraoperative x-ray - why? Make a plan for further post-operative studies e.g. CT scan Report the incorrect final item count
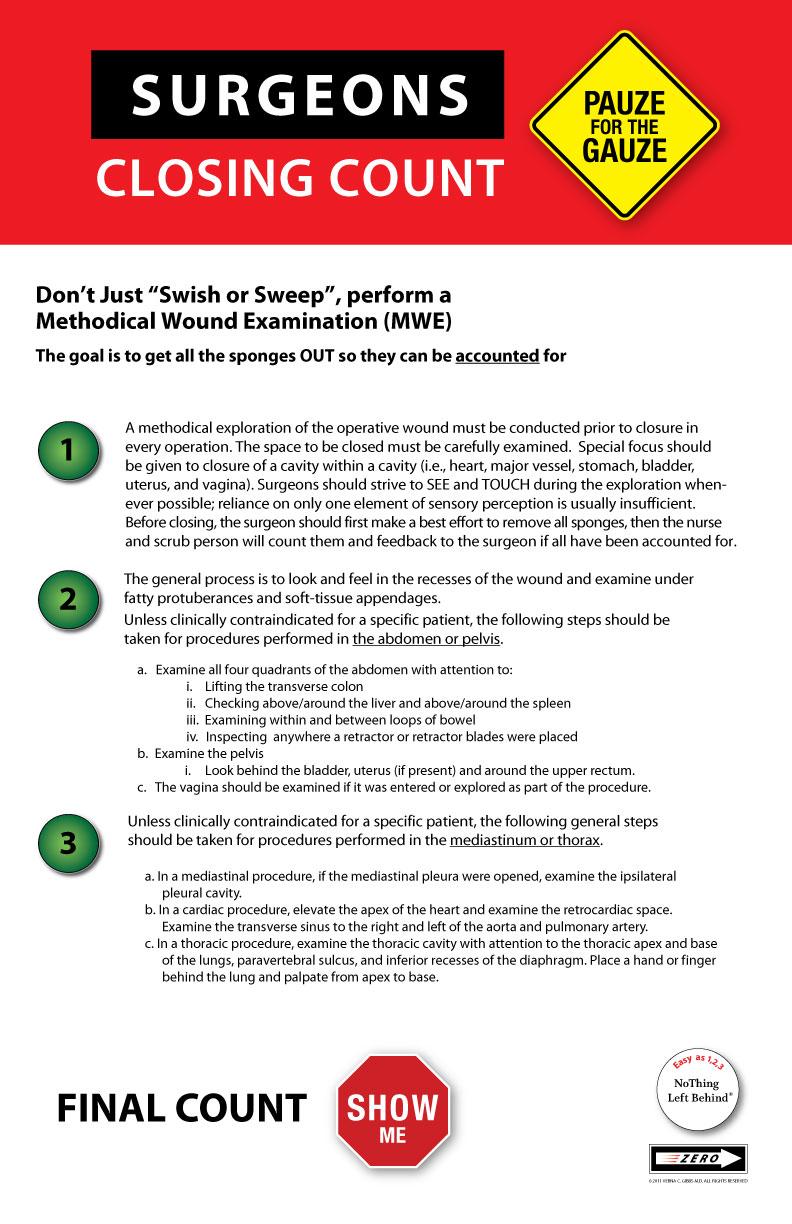
24 Surgeon Every case should have a methodical wound examination performed before closing Use two sensory modalities touch and sight It s a human endeavor which might fail, but should be done
25
26 Scrub Position Content experts on materiel! Check condition of all items passed and returned on the field! Requires knowledge about instruments, tools, surgical items! Standardized back table! Must speak up and question if something is amiss NLB Vernacular


27 Standardize Tables Reduce variation on how STs set up and maintain back tables Aids with discovery of a missing item Everything in its place Not my table Beyond counting
28 Non-OR Cases 1) Intravascular! Everywhere: cardiology, radiology, anesthesiology, ICU! Guidewires, catheters, sheaths, introducers 2) Interstitial! Subcutaneous space, breast tissue! Catheter parts, broken drains, wires NLB Vernacular

29 Guidewires Interventional Radiology can successfully remove these >90% of the time IF recognized and removed early Late discovery leads to fibrous adherence


30 Removal is desired MRI procedures problematic Magnetic fields can cause movement, migration Radiofrequency fields cause heating
31 Retention Prevention At least for Guidewires: Prevention! Proceduralist competency and expertise Training and experience! CLABSI protocol has last element on checklist: Guidewire is IN THE KIT Mitigation of Harm:! Immediate Post-procedure CXR

32 Infusion Device Pieces 2) Interstitial! Subcutaneous space Insertion and removal techniques lead to retention Post- removal inspection of device is key
33 Why do they occur? Catheter and guide wire fractures that result in UDFs can be caused by these inappropriate techniques: withdrawing a catheter through or over a needle shaping a device to conform to the patient s anatomy when the device wasn t designed to be reshaped
34 Why do they occur? using undue force and torque (rotational force) on insertion or withdrawal improperly manipulating a catheter using devices that are too small or too large using a device for an off-label purpose
35 Essential causes A. Provider errors and mistakes in use of the device! This is the most common finding B. Provider uses the device correctly but there is a problem with the device! 1) Manufacturer defects! 2) Worn and Used equipment! 3) New Unfamiliar Devices Multiple separable parts Non-radiopaque pieces of a multipart device
36 Essential causes A. Provider errors and mistakes in use of the device! This is the most common finding B. Provider uses the device correctly but there is a problem with the device! 1) Manufacturer defects! 2) Worn and Used equipment! 3) New Unfamiliar Devices Multiple separable parts Non-radiopaque pieces of a multipart device
37 Unretrieved Device Fragments Unretrieved Device Fragments (UDFs) Official FDA nomenclature, not bits and pieces Broken parts or pieces of devices and surgical items These are the items where the risk of retrieval > risk of retention mantra is frequently invoked

38 ECRI s Top 10 Emergency Care Research Institute #7 Retained devices and unretrieved fragments Second most common RSI
39 Device Fragments can lead to serious adverse events US FDA notification Jan 2008 Local tissue reaction, infection, thrombosis, perforation, obstruction, emboli Center for Devices and Radiological Health (CDRH) receives ~1000 adverse event reports a year related to UDFs TipsandArticlesonDeviceSafety/ucm htm

40 Disclosure vs. reporting Retained small item or UDF. Clinical decision NOT to remove.?? can cause harm DISCLOSE TO THE PATIENT Discuss about reporting Engage with OR leadership to hone multistakeholder prevention strategies

41 TJC Recommendations Log In Request Guest Access Contact Us Careers JCR Web Store Press Room Forgot password? Log In Help Search Go Accreditation Certification Standards Measurement Topics About Us Daily Update Home > About Us Joint Commission FAQ Page Sentinel Event - Retained foreign object after surgery Sometimes a needle or screw will break leaving a fragment behind. Is this a reviewable sentinel event? What about a retained sponge following vaginal delivery? When, exactly, is after surgery?" Why was this particular point in the process selected as the definition of after surgery?" Sentinel Event - Retained foreign object after surgery Q: Sometimes a needle or screw will break leaving a fragment behind. Is this a reviewable sentinel event? A: In some cases, a broken needle or screw fragment is recognized at the time of surgery and a clinical judgment is made to leave the fragment in the patient. That decision is based on an assessment of the relative risks of leaving it in versus removing it. It would therefore not be considered an unintentionally retained foreign object. back to top Q: What about a retained sponge following vaginal delivery? A: A retained sponge after a vaginal delivery is a reviewable sentinel event. The new language in the definition of reviewable sentinel events is, Unintended retention of a foreign object in a patient after surgery or other procedure. Note that it says other procedure not other invasive procedure. Vaginal delivery in the hospital is not an invasive procedure, but it is a procedure. More to the point, a retained sponge in this circumstance is indicative of the same underlying systemic problems that could cause other retained foreign body situations. back to top Q: When, exactly, is after surgery?" A: After surgery is any time after completion of the skin closure; even if the patient is still in the OR under anesthesia. Wednesday 7:36 CST, May 7, 2014 not an unintentionally retained foreign object so not a sentinel event so no RCA and no reporting required back to top Q: Why was this particular point in the process selected as the definition of after surgery?" A: The decision to define after surgery as the completion of skin closure was based on the premise that a failure to identify and correct an unintended retention of a foreign object prior to that point in the procedure represents a significant system failure, which requires analysis and redesign. It also places the patient at additional risk by virtue of extending the surgical procedure and time under anesthesia. back to top Can't find what you are looking for? Ask your own question? Ask a question about Sentinel Event - Retained foreign object after surgery Contact Us Site Map Copyright-Privacy Policy 2014 The Joint Commission, All Rights Reserved
42 NQF Required Reporting Serious Reportable Events (SRE) 2011 Update Event Unintended retention of a foreign object in a patient after surgery or other invasive procedure Applicable Settings: Hospitals Outpatient/Officebased Surgery Centers Ambulatory Practice Settings/ Office-based Practices Long-term Care/ Skilled Nursing Facilities Additional Specifications Includes medical or surgical items intentionally placed by provider(s) that are unintentionally left in place Excludes: a) objects present prior to surgery or other invasive procedure that are intentionally left in place; b) objects intentionally implanted as part of a planned intervention and; c) objects not present prior to surgery/procedure that are intentionally left in when the risk of removal exceeds the risk of retention (such as microneedles, broken screws) Implementation Guidance This event is intended to capture: Occurrences of unintended retention of objects at any point after the surgery/ procedure ends regardless of setting (post anesthesia recovery unit, surgical suite, emergency department, patient bedside) and regardless of whether the object is to be removed after discovery Unintentionally retained objects (including such things as wound packing material, sponges, catheter tips, trocars, guide wires) in all applicable settings

43 CDPH rules
44 Recommendations So the NQF does not consider the unretrieved device fragments a SRE so probably not required to report Except in California you must report Voluntarily report to MedSun system Even if there is no requirement to report, should DISCLOSE to the patient and should conduct an RCA To inform the patient have to have info
45 When device breaks Collect all available parts Sequester them do NOT throw them away Consider getting an x-ray of site Obtain information about the item e.g. model #, lot and serial number Save an unbroken item for comparison with damaged goods Complete an incident report Report to MedSun
46 Med Sun The FDA Safety Information and Adverse Event Reporting Program Report on the FDA s MedWatch website! Select Report a Serious Medical Product Problem Online! Select Health Professional or Consumer/Patient on the right side of the page to begin the report
47 Patient Disclosure 1. Advise patients of the existence and nature of the UDF (show them what the item looks like). Include the following information: 1. material composition of the UDF, 2. the measurement/size of the fragment, 3. location, 4. x-rays findings with interpretation, 5. potential for injury e.g. migration, infection, embolization, thrombosis and 6. any procedures or treatments to be avoided or to be obtained

48 Retained Needles Most frequent item associated with miscounts What injury results from a lost suture needle? Do we have to take an xray if a miscount occurs? Discuss needles by SIZE of the needle not by size of the suture
49 Can cause symptoms Retained needle in eye Retained needle after thyroidectomy Retained needle in pelvis, causing pelvic pain,! hysterectomy Needles associated with symptoms were >13mm CT pelvis retained 34mm needle
50 What to do? Develop a rational needle management plan to prevent lost needles and reduce # of xrays Best effort for risk reduction Determine a size cut-off where xrays won t be taken for lost needle Discuss needles by SIZE of needle not by size of the suture
51 Animal model Cadaver pig model insertion of 39 surgical needles from 4-77mm Random selection of 9 segments in abdomen 8 plain radiographs 5 independent radiologists reviewed films Reviewers knew they were looking for surgical needles Ponrartana S. et.al. Annal of Surg 247:8, 2008
52 Results Total of 195 needles for each reviewer 69% overall sensitivity 135/195 detected 80% specificity - 32 false positives Needle size significant predictor of sensitivity (p<0.0001)! 4-10mm 29%! 11-24mm 84%! >25mm 99% Detection sensitivity under 50% for needles <10mm

53 Small Needle Detection Even if they can be seen, would they be removed?
54 Phantom X-ray model Skull Skull Pelvis Pelvis Dense bone Less dense Dense bone So1 2ssue Needle / torchar type metric, 40mm, 1/2c, taper V V V V 3-0, 2.0 metric, 24mm, 3/8c, reverse cutting V V V V 5-0, 1.0 metric, 8.0mm, 1/4, spatula N V V V 6-0, 0.7 metric, 11mm, 3/8c, reverse cutting V V V V 6-0, 0.7 metric, 8.0mm, 3/8c, reverse cutting N B V V 6-0, 1.0 metric, 6.5mm, 3/8c, spatula N V N V 7-0, 0.5 metric, 6.5mm, 3/8c, spatula B V B V 8-0, 0.4 metric, 7mm, 1/2c, spatula N N N V 9-0, 0.3 metric, 5.5mm, 1/2c, spatula N N N V 9-0, 0.3 metric, 5mm, 3/8c, taper N N N N 9-0, 0.3 metric, 3.8mm, 3/8c, taper N N N N 10-0, 0.2 metric, 16mm, straight spatula N N N V 10-0, 0.2 metric, 13mm, 1/4c, tapercut N N N V 10-0, 0.2 metric, 6.5mm, 3/8c, spatula N N N B 10-0, 0.2 metric, 5.5mm, 1/2c, spatula N N N B 19 gauge trochar plug V V V V 20 gauge trochar plug V V V V 23 gauge trochar plug N B V V Legend: V: Visible B: Barely visible N: Not visible Courtesy of St. Louis University

55 Define Large as >15mm L A R G E L A R G E
56 What to do? Develop a rational needle management plan to prevent lost needles Best effort for risk reduction All needles come back to scrub person on a needle holder to the safety zone Needles are put in needle container Keep numbers low Think and manage needles by SIZE of the needle not size of the suture


57 Needle Management Safety Zone Not any thing on the back table. Rectangular pan, made of plastic. Not metal magnitizes the instruments Sorting strategy Large vs Small

58 Dry Erase Board

59 Large Goes in Foam


60 Keep numbers low
61 A Needle Algorithm Keep numbers of needles on back table low ( <30), use needle counter boxes Separate small from large (>15mm) needles If a MISCOUNT occurs: look for needle then! If large needle (>15mm) get xray! If small needle no xray: unlikely will see needle on xray, unlikely will be able to find it, unlikely to result in injury Document the incorrect needle count and decisions if the needle isn t found Disclose to the patient
62 Close Calls If nothing else, start reporting near miss events Use this as an OR improvement opportunity Review them to change/improve practice
63 What to do? A 9mm needle was unaccounted for at the end of an open heart surgery. Do we have to disclose to the patient? Do we have to report this event to CDPH?
64 Answer This is an incorrect final count for needles and sharps Disclose to the patient, give them an option..?get a CT scan with 4-5mm cuts or not If +, you know where the needle is If -, you know that the needle isn t in the patient No CT?, You do not know with certainty that the needle is NOT in the patient. Report it to CDPH Do NOT charge the patient for the CT it s need is a consequence of error
65 Patient Disclosure Practitioner s obligation to disclose is based on norms of medical ethics, professionalism, public policy and law Ethical tenets of the standards of non-maleficence, beneficence, autonomy and justice apply Respect for autonomy requires avoidance of interfering with an individuals decision-making and presents an obligation of the MD to provide the necessary information for the patient to make a true decision Notions of justice fairness and equity require that patients be informed

66 Perspective Anecdotal observation as disclosure has been more widely enforced we have seen a decrease in the number of risk of retrieval > risk of retention cases.. hmmmmm

67 Apologies to MasterCard

68
BECAUSE.. RSI are considered to be NEVER EVENTS and the Incidence is STILL > ZERO
 HOSPITALS BECAUSE.. RSI are considered to be NEVER EVENTS and the Incidence is STILL > ZERO Culture Trumps Strategy: Implementation Barriers in RSS Prevention Verna C. Gibbs MD Director, NoThing Left Behind
HOSPITALS BECAUSE.. RSI are considered to be NEVER EVENTS and the Incidence is STILL > ZERO Culture Trumps Strategy: Implementation Barriers in RSS Prevention Verna C. Gibbs MD Director, NoThing Left Behind
NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual
 NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual ã2018 Verna C. Gibbs M.D. all rights reserved July 2018 San Francisco, California NoThing
NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual ã2018 Verna C. Gibbs M.D. all rights reserved July 2018 San Francisco, California NoThing
Department of Veterans Affairs VHA Directive Washington, DC March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS
 Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
What we have learned:
 What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
POLICY - JOB AID NoThing Left Behind : Prevention of Retained Surgical Items Multi-Stakeholder Policy
 POLICY - JOB AID NoThing Left Behind : Prevention of Retained Surgical Items Multi-Stakeholder Policy 2015 Verna C. Gibbs M.D. all rights reserved February 2015 San Francisco, California NoThing Left Behind
POLICY - JOB AID NoThing Left Behind : Prevention of Retained Surgical Items Multi-Stakeholder Policy 2015 Verna C. Gibbs M.D. all rights reserved February 2015 San Francisco, California NoThing Left Behind
NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual
 NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual ã2018 Verna C. Gibbs M.D. all rights reserved July 2018 San Francisco, California NoThing
NoThing Left Behind The Prevention of Retained Surgical Items Multi-Stakeholder PolicyJob Aid-Reference Manual ã2018 Verna C. Gibbs M.D. all rights reserved July 2018 San Francisco, California NoThing
NoThing Left Behind Points of Confusion with The Players and The Policies
 NoThing Left Behind Points of Confusion with The Players and The Policies July 2014 Your health comes first with us You re the reason we launched the Patient Safety First program, where we work hand-in-hand
NoThing Left Behind Points of Confusion with The Players and The Policies July 2014 Your health comes first with us You re the reason we launched the Patient Safety First program, where we work hand-in-hand
Webinar SURGICAL OBJECT SURVEILLANCE. Kyung Jun, RN, MSN, CNOR January 22, 2014
 Webinar SURGICAL OBJECT SURVEILLANCE Kyung Jun, RN, MSN, CNOR January 22, 2014 TITLE Please vote for best title regarding preventing retained surgical item SOS : Surgical Object Surveillances? What Goes
Webinar SURGICAL OBJECT SURVEILLANCE Kyung Jun, RN, MSN, CNOR January 22, 2014 TITLE Please vote for best title regarding preventing retained surgical item SOS : Surgical Object Surveillances? What Goes
Consensus Reports and Recommendations to Prevent Retained Surgical Items
 Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
SPONGE ACCOUNTing SYSTEM AUDIT TOOL
 Verna C. Gibbs M.D. NoThing Left Behind SPONGE ACCOUNTing SYSTEM Nurses use a standardized process to put sponges in hanging plastic holders and document the counts on a wall-mounted dry-erase board in
Verna C. Gibbs M.D. NoThing Left Behind SPONGE ACCOUNTing SYSTEM Nurses use a standardized process to put sponges in hanging plastic holders and document the counts on a wall-mounted dry-erase board in
OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment
 ACCREDITATION STANDA RDS INTRAOPERATIVE CARE OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment A minimum of two perioperative nurses are
ACCREDITATION STANDA RDS INTRAOPERATIVE CARE OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment A minimum of two perioperative nurses are
Purpose/goal. Statementt. Objectives After. Requirements. Sponsorship. reading this. 2. Read and. review the. completion. This activity was.
 INSTRUCTIONS & DISCLOSURE STATEMENT Course 10: Perform Sponge, Sharp, and Instrument Counts Purpose/goal Statementt The purpose of this chapter is to describe the perioperative nurse s role in preventing
INSTRUCTIONS & DISCLOSURE STATEMENT Course 10: Perform Sponge, Sharp, and Instrument Counts Purpose/goal Statementt The purpose of this chapter is to describe the perioperative nurse s role in preventing
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.13.28 Responsible Vice President: EVP & CEO Health System Subject: Patient Risk, Treatment, and Safety Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.13.28 Responsible Vice President: EVP & CEO Health System Subject: Patient Risk, Treatment, and Safety Responsible Entity:
SARASOTA MEMORIAL HOSPITAL POLICY
 PS1013 SARASOTA MEMORIAL HOSPITAL POLICY TITLE: PREVENTION OF RETAINED SURGICAL ITEMS: SOFT GOODS, SHARPS AND INSTRUMENTS EFFECTIVE DATE: REVIEW/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner:
PS1013 SARASOTA MEMORIAL HOSPITAL POLICY TITLE: PREVENTION OF RETAINED SURGICAL ITEMS: SOFT GOODS, SHARPS AND INSTRUMENTS EFFECTIVE DATE: REVIEW/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner:
DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2748 Worth Road JBSA Fort Sam Houston, Texas
 DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2748 Worth Road JBSA Fort Sam Houston, Texas 78234-6000 MEDCOM Regulation 21 January 2015 No. 40-49 Medical Services SURGICAL COUNTS
DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2748 Worth Road JBSA Fort Sam Houston, Texas 78234-6000 MEDCOM Regulation 21 January 2015 No. 40-49 Medical Services SURGICAL COUNTS
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC April 3, 2006
 Department of Veterans Affairs VHA DIRECTIVE 2006-018 Veterans Health Administration Washington, DC 20420 PREVENTION OF RETAINED SURGICAL ITEMS 1. PURPOSE: This Veteran Health Administration (VHA) Directive
Department of Veterans Affairs VHA DIRECTIVE 2006-018 Veterans Health Administration Washington, DC 20420 PREVENTION OF RETAINED SURGICAL ITEMS 1. PURPOSE: This Veteran Health Administration (VHA) Directive
Preventing unintended retained foreign objects
 A complimentary publication of Issue 51, October 17, 2013 The Joint Commission Preventing unintended retained foreign objects Published for Joint Commission accredited organizations and interested health
A complimentary publication of Issue 51, October 17, 2013 The Joint Commission Preventing unintended retained foreign objects Published for Joint Commission accredited organizations and interested health
Surgical counts are an established routine. An OR nurse performs them dozens
 Patient safety Human factors, education help sharpen the OR count process Surgical counts are an established routine. An OR nurse performs them dozens of times a month. But when you dissect the process
Patient safety Human factors, education help sharpen the OR count process Surgical counts are an established routine. An OR nurse performs them dozens of times a month. But when you dissect the process
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Validation of Surgical Sponge Counts Using Technology
 CME ONLINE Validation of Surgical Sponge Counts Using Technology An Online Continuing Medical Education Activity Sponsored By Grant Funds Provided By Welcome to Validation of Surgical Sponge Counts Using
CME ONLINE Validation of Surgical Sponge Counts Using Technology An Online Continuing Medical Education Activity Sponsored By Grant Funds Provided By Welcome to Validation of Surgical Sponge Counts Using
MRI Patient Screening and History
 Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
STANDARDIZED PROCEDURE VENTRICULAR SEPTAL DEFECT (VSD) CLOSURE ASSIST (Neonatal, Peds)
 CLOSURE ASSIST (Neonatal, Peds)") I. Definition A ventricular septal defect is an abnormal opening in the wall (septum) that divides the two lower chambers of the heart (ventricles). A ventricular septal defect closure is a procedure performed
I. Definition A ventricular septal defect is an abnormal opening in the wall (septum) that divides the two lower chambers of the heart (ventricles). A ventricular septal defect closure is a procedure performed
Z: Perioperative Nursing Specialty
 Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Surgery Road Map. General practices. Road map sections
 Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Prevention of Unintentionally Retained Foreign Objects During Vaginal Deliveries
 Health Care Protocol: Prevention of Unintentionally Retained Foreign Objects During Vaginal Deliveries Fourth Edition January 2012 The information contained in this ICSI Health Care Protocol is intended
Health Care Protocol: Prevention of Unintentionally Retained Foreign Objects During Vaginal Deliveries Fourth Edition January 2012 The information contained in this ICSI Health Care Protocol is intended
Prevention of Retained Foreign Objects
 Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Your facility is having a baby boom. The number of cesarean births is
 Clinical management Ensuring a comparable standard of care for cesarean deliveries Your facility is having a baby boom. The number of cesarean births is exceeding the obstetrical unit s capacity. Administrators
Clinical management Ensuring a comparable standard of care for cesarean deliveries Your facility is having a baby boom. The number of cesarean births is exceeding the obstetrical unit s capacity. Administrators
Revised Surgical Rotation Case Requirements, Core Curriculum for Surgical Technology, 6 th edition
 TO: FROM: Surgical Technology Program Directors AST ARC/STSA NBSTSA DATE: October 29, 2014 RE: Revised Surgical Rotation Case Requirements, Core Curriculum for Surgical Technology, 6 th edition Dear Surgical
TO: FROM: Surgical Technology Program Directors AST ARC/STSA NBSTSA DATE: October 29, 2014 RE: Revised Surgical Rotation Case Requirements, Core Curriculum for Surgical Technology, 6 th edition Dear Surgical
VERMONT2008 Patient Safety, Surveillance, and Improvement System
 VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Wrong Site, Wrong Procedure, Wrong Person Surgery
 Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
AI had been engaged in work in Surgical
 Interview with a uality Leader: Dr. Verna Gibbs on Surgical Safety Susan V. White, Interviewer Vol. 34 No. 6 November/December 2012 21 native of New Jersey and a third-generation physician, Dr. Verna Gibbs
Interview with a uality Leader: Dr. Verna Gibbs on Surgical Safety Susan V. White, Interviewer Vol. 34 No. 6 November/December 2012 21 native of New Jersey and a third-generation physician, Dr. Verna Gibbs
Preventing Wrong-Site Surgery Through Implementation of Evidenced-Based Best Practices
 Preventing Wrong-Site Surgery Through Implementation of Evidenced-Based Best Practices Robert Yonash, RN, CPPS Pennsylvania Patient Safety Authority Patient Safety Liaison, Southwest Region Objectives
Preventing Wrong-Site Surgery Through Implementation of Evidenced-Based Best Practices Robert Yonash, RN, CPPS Pennsylvania Patient Safety Authority Patient Safety Liaison, Southwest Region Objectives
INCIDENT POLICY Page 1 of 15 July 2017
 Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
STANDARDIZED PROCEDURE HEPATIC ARTERY INFUSION OF CHEMOTHERAPY (Adults, Peds)
") I. Definition Hepatic arterial infusion (HAI) of chemotherapy is accomplished by a small drug delivery system or pump that is implanted in a subcutaneous pocket in the lower abdomen. The pump reservoir
I. Definition Hepatic arterial infusion (HAI) of chemotherapy is accomplished by a small drug delivery system or pump that is implanted in a subcutaneous pocket in the lower abdomen. The pump reservoir
JOB DESCRIPTION: SURGICAL TECHNOLOGIST
 1507.00. JOB DESCRIPTION: SURGICAL TECHNOLOGIST 1507.01. The Standards & Guidelines for the Accreditation of Educational Programs in Surgical Technology have been approved by the Association of Surgical
1507.00. JOB DESCRIPTION: SURGICAL TECHNOLOGIST 1507.01. The Standards & Guidelines for the Accreditation of Educational Programs in Surgical Technology have been approved by the Association of Surgical
Pediatric Medical Device Development and Safety. Jacqueline N. Francis, MD, MPH Medical Officer, PSRB, ODE, CDRH, FDA
 Pediatric Medical Device Development and Safety Jacqueline N. Francis, MD, MPH Medical Officer, PSRB, ODE, CDRH, FDA This presentation represents the professional opinion of the speaker and is not an official
Pediatric Medical Device Development and Safety Jacqueline N. Francis, MD, MPH Medical Officer, PSRB, ODE, CDRH, FDA This presentation represents the professional opinion of the speaker and is not an official
PATIENT REGISTRATION. Street City State Zip WORK INJURY/ ACCIDENT
 PATIENT REGISTRATION, Last First M.I. SEX: Male Female DOB: / _/ AGE: MARITAL STATUS: SS#: - - PHYSICIAN: ADDRESS: Street City State Zip (HOME) (WORK) TEL: - - TEL: - _- CELL: - _- EMAIL: PRIMARY INSURANCE:
PATIENT REGISTRATION, Last First M.I. SEX: Male Female DOB: / _/ AGE: MARITAL STATUS: SS#: - - PHYSICIAN: ADDRESS: Street City State Zip (HOME) (WORK) TEL: - - TEL: - _- CELL: - _- EMAIL: PRIMARY INSURANCE:
Legal & Ethical Issues in Vascular Access Minimizing Risk and Liability of Venous Catheter Access Maurizio Gallieni, MD Ospedale San Carlo Borromeo
 Legal & Ethical Issues in Vascular Access Minimizing Risk and Liability of Venous Catheter Access Maurizio Gallieni, MD Ospedale San Carlo Borromeo Milano, Italy President, the Vascular Access Society
Legal & Ethical Issues in Vascular Access Minimizing Risk and Liability of Venous Catheter Access Maurizio Gallieni, MD Ospedale San Carlo Borromeo Milano, Italy President, the Vascular Access Society
BERGEN COMMUNITY COLLEGE
 SUR 202 Course Syllabus Credits: 2 BERGEN COMMUNITY COLLEGE DIVISION OF HEALTH PROFESSIONS SURGICAL TECHNOLOGY PROGRAM HOSPITAL CLINICAL Instructors- Carolan Sherman CST, RN, BSN, MSN E-Mail- Mary Chmielewski
SUR 202 Course Syllabus Credits: 2 BERGEN COMMUNITY COLLEGE DIVISION OF HEALTH PROFESSIONS SURGICAL TECHNOLOGY PROGRAM HOSPITAL CLINICAL Instructors- Carolan Sherman CST, RN, BSN, MSN E-Mail- Mary Chmielewski
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: HEMODIALYSIS TEMPORARY CATHETER (INSERTION, DRESSING CHANGE, REMOVAL, MEDICATION AND BLOOD DRAWS, DISCONTINUATION OF MEDS AND IV FLUIDS)
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: HEMODIALYSIS TEMPORARY CATHETER (INSERTION, DRESSING CHANGE, REMOVAL, MEDICATION AND BLOOD DRAWS, DISCONTINUATION OF MEDS AND IV FLUIDS)
STANDARDIZED PROCEDURE REMOVAL OF EXTERNAL VENTRICULAR DRAINAGE CATHETER OR INTRACRANIAL PRESSURE DEVICE (Adult, Peds)
") I. Definition This procedure will take place when a neurosurgery physician deems appropriate. The purpose of this standardized procedure is to allow the Advanced Health Practitioner to safely remove an
I. Definition This procedure will take place when a neurosurgery physician deems appropriate. The purpose of this standardized procedure is to allow the Advanced Health Practitioner to safely remove an
Venepuncture, obtaining blood cultures and managing blood samples
 Venepuncture, obtaining blood cultures and managing blood samples Aims To ensure that students are able to demonstrate the safe and correct technique for venepuncture, obtaining blood cultures and managing
Venepuncture, obtaining blood cultures and managing blood samples Aims To ensure that students are able to demonstrate the safe and correct technique for venepuncture, obtaining blood cultures and managing
Certified PICC Ultrasound Inserter CPUI Renewal Application
 APPLICATION FOR CPUI CERTIFICATION RENEWAL This form renews CPUI PICC Certification by documentation and does not establish competency. Competency must be established by the employer and facility. Name
APPLICATION FOR CPUI CERTIFICATION RENEWAL This form renews CPUI PICC Certification by documentation and does not establish competency. Competency must be established by the employer and facility. Name
PLASTIC AND HAND SURGERY CORE OBJECTIVES
 PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
Appendix A.1 SURGICAL TECHNOLOGIST WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE
 WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE A.1-1 WORK PROCESS SCHEDULE O*NET-SOC CODE: 29-2055.00 RAPIDS CODE: 1051CB This schedule is attached to and a part of these Standards for the above
WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE A.1-1 WORK PROCESS SCHEDULE O*NET-SOC CODE: 29-2055.00 RAPIDS CODE: 1051CB This schedule is attached to and a part of these Standards for the above
Accreditation Program: Hospital Chapter: National Patient Safety Goals
 Universal Protocol Accreditation Program: Hospital Chapter: National Patient Safety Goals The organization meets the expectations of the Universal Protocol. UP.01.01.01 Conduct a pre-procedure verification
Universal Protocol Accreditation Program: Hospital Chapter: National Patient Safety Goals The organization meets the expectations of the Universal Protocol. UP.01.01.01 Conduct a pre-procedure verification
PATIENT INFORMATION: CONTACT INFORMATION: EMERGENCY CONTACT: EMERGENCY PHONE: RESPONSIBLE PARTY (IF OTHER THAN PATIENT)
") PATIENT REGISTRATION PATIENT INFORMATION: NAME:,, (M.I.) ADDRESS:,, (Street) (City) (State) (Zip) SEX: MALE FEMALE DOB: / / AGE: MARITAL STATUS: SS #: / / REFERRING PHYSICIAN: CONTACT INFORMATION: (CELL):
PATIENT REGISTRATION PATIENT INFORMATION: NAME:,, (M.I.) ADDRESS:,, (Street) (City) (State) (Zip) SEX: MALE FEMALE DOB: / / AGE: MARITAL STATUS: SS #: / / REFERRING PHYSICIAN: CONTACT INFORMATION: (CELL):
STANDARDIZED PROCEDURE LUMBAR DRAIN INSERTION (Adults, Peds)
") I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
Frequently Asked Questions Quality-Based Physician Incentive Program (QPIP)
") Frequently Asked Questions Quality-Based Physician Incentive Program (QPIP) As a UnitedHealthcare network care provider, you have options on where your patients who are our plan members receive their surgical
Frequently Asked Questions Quality-Based Physician Incentive Program (QPIP) As a UnitedHealthcare network care provider, you have options on where your patients who are our plan members receive their surgical
Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO. An Illinois Hospital Association Company
 Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO An Illinois Hospital Association Company Today s Roadmap Objectives: 1. Explain the PSQIA and PSO Basics 2. Learn
Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO An Illinois Hospital Association Company Today s Roadmap Objectives: 1. Explain the PSQIA and PSO Basics 2. Learn
Surgical Technology. Washburn Institute of Technology. Program Number Target Population. Description. Entry Requirements.
 Surgical Technology Organization Washburn Institute of Technology Program Number 51.0909 Instructional Level Certificate Target Population Post-secondary Description This program provides an opportunity
Surgical Technology Organization Washburn Institute of Technology Program Number 51.0909 Instructional Level Certificate Target Population Post-secondary Description This program provides an opportunity
Having a portacath insertion in the x-ray department
 Having a portacath insertion in the x-ray department This leaflet provides information about a portacath insertion, including the benefits, risks and any alternatives. It also explains what you can expect
Having a portacath insertion in the x-ray department This leaflet provides information about a portacath insertion, including the benefits, risks and any alternatives. It also explains what you can expect
Welcome to Scott & White Memorial Hospital. Perioperative Services
 Welcome to Scott & White Memorial Hospital Perioperative Services What is a Perioperative Nurse? A perioperative nurse is a nurse who provides patient care, manages, teaches, and studies the care of patients
Welcome to Scott & White Memorial Hospital Perioperative Services What is a Perioperative Nurse? A perioperative nurse is a nurse who provides patient care, manages, teaches, and studies the care of patients
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Global Days Policy. Approved By 7/12/2017
 Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
NURSE PRACTITIONER (NP) CLINICAL PRIVILEGES ORTHOPEDIC SURGERY
 CLINICAL PRIVILEGES ORTHOPEDIC SURGERY") Name: Page 1 Initial Appointment (initial privileges) Reappointment (renewal of privileges) All new applicants must meet the following requirements as approved by the governing body effective: / /. Applicant:
Name: Page 1 Initial Appointment (initial privileges) Reappointment (renewal of privileges) All new applicants must meet the following requirements as approved by the governing body effective: / /. Applicant:
Surgical Fires: Prevention and Safety
 Surgical Fires: Prevention and Safety MedPro Group Patient Safety & Risk Solutions The ECRI Institute estimates that 200 to 240 surgical fires occur annually in the United States, with some of them causing
Surgical Fires: Prevention and Safety MedPro Group Patient Safety & Risk Solutions The ECRI Institute estimates that 200 to 240 surgical fires occur annually in the United States, with some of them causing
NEOSHO COUNTY COMMUNITY COLLEGE COURSE SYLLABUS. Course Prefix/Number: SURG 103 Principles and Practices of Surg. Tech. Lab
 COURSE IDENTIFICATION NEOSHO COUNTY COMMUNITY COLLEGE COURSE SYLLABUS Course Prefix/Number: SURG 103 Course Title: Principles and Practices of Surg. Tech. Lab Division: Allied Health Program: Surgical
COURSE IDENTIFICATION NEOSHO COUNTY COMMUNITY COLLEGE COURSE SYLLABUS Course Prefix/Number: SURG 103 Course Title: Principles and Practices of Surg. Tech. Lab Division: Allied Health Program: Surgical
Issue Date Review Date Version July 2017 July 2022 V6
 Trust Policy Instrument Counts during Invasive Procedures Purpose Issue Date Review Date Version July 2017 July 2022 V6 This policy identifies the correct procedure for counting instruments and bio-medical
Trust Policy Instrument Counts during Invasive Procedures Purpose Issue Date Review Date Version July 2017 July 2022 V6 This policy identifies the correct procedure for counting instruments and bio-medical
NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS. Principles and Practices of Surgical Technology Lab
 NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS COURSE IDENTIFICATION Course Code/Number: SURG 103 Course Title: Principles and Practices of Surgical Technology Lab Division: Applied Science (AS)
NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS COURSE IDENTIFICATION Course Code/Number: SURG 103 Course Title: Principles and Practices of Surgical Technology Lab Division: Applied Science (AS)
SAMPLE Perioperative Self-Assessment Questionnaire
 SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
WPSC Teleconference Avoiding Never Events. Linda Furkay, PhD, RN Patient Safety Adverse Event Officer
 Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
Introduction to Perioperative Nursing
 C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application
C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application
Powered by WHO Extranet DataCol Tool for Situational Analysis to Assess Emergency and Essential Surgical Care Reference: Objective:
 Powered by WHO Extranet DataCol Tool for Situational Analysis to Assess Emergency and Essential Surgical Care Reference: WHO Integrated Management for Emergency & Essential Surgical Care (IMEESC) toolkit:
Powered by WHO Extranet DataCol Tool for Situational Analysis to Assess Emergency and Essential Surgical Care Reference: WHO Integrated Management for Emergency & Essential Surgical Care (IMEESC) toolkit:
393 PICC INSERTION USING ULTRASONOGRAPHY AND MICRO INTRODUCER TECHNIQUE 06/10/03 1
 393 ULTRASONOGRAPHY AND MICRO INTRODUCER TECHNIQUE 06/10/03 1 POLICY: General Information: 1. RN s validated to insert PICCs with the additional training in the use of ultrasonography (U/S) and microintroduction
393 ULTRASONOGRAPHY AND MICRO INTRODUCER TECHNIQUE 06/10/03 1 POLICY: General Information: 1. RN s validated to insert PICCs with the additional training in the use of ultrasonography (U/S) and microintroduction
Welcome to Baylor Scott & White Hillcrest. A Perioperative Services Orientation
 Welcome to Baylor Scott & White Hillcrest A Perioperative Services Orientation What does "Perioperative" mean? When a patient is cared for in the Perioperative setting, they receive care preoperatively,
Welcome to Baylor Scott & White Hillcrest A Perioperative Services Orientation What does "Perioperative" mean? When a patient is cared for in the Perioperative setting, they receive care preoperatively,
ETHICAL CONSIDERATIONS THAT ARISE IN LONG TERM CARE PART 2 REPORTING OBLIGATIONS
 ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION. August 9, :00 a.m. 12:00 p.m. CT
 AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION August 9, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Marina Levin, Program Manager HRET 11:00 11:05AM 2
AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION August 9, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Marina Levin, Program Manager HRET 11:00 11:05AM 2
Procedure. Applies To: UNM Hospitals Responsible Departments: All Revised: 9/2009 updated: 8/2013. Title: Universal Protocol / Time Out
 Title: Universal Protocol / Time Out Applies To: UNM Hospitals Responsible Departments: All Revised: 9/2009 updated: 8/2013 Procedure Patient Age Group: ( ) N/A (X) All Ages ( ) Newborns ( ) Pediatric
Title: Universal Protocol / Time Out Applies To: UNM Hospitals Responsible Departments: All Revised: 9/2009 updated: 8/2013 Procedure Patient Age Group: ( ) N/A (X) All Ages ( ) Newborns ( ) Pediatric
Global Surgery Package
 Private Property of Florida Blue. This payment policy is Copyright 2017 Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
Private Property of Florida Blue. This payment policy is Copyright 2017 Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
New Jersey Department of Health Report Preparation Team. Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics
 2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Department of Neurological Surgery John Radcliffe Hospital Thalamotomy and Pallidotomy Pre-operative information for people with tremor and/or
 Department of Neurological Surgery John Radcliffe Hospital Thalamotomy and Pallidotomy Pre-operative information for people with tremor and/or Parkinson s disease We have been able to help many people
Department of Neurological Surgery John Radcliffe Hospital Thalamotomy and Pallidotomy Pre-operative information for people with tremor and/or Parkinson s disease We have been able to help many people
Peripherally Inserted Central Catheter
 UW MEDICINE PATIENT EDUCATION Peripherally Inserted Central Catheter Understanding your PICC procedure and consent form Please read this handout before reading and signing the form Special Consent for
UW MEDICINE PATIENT EDUCATION Peripherally Inserted Central Catheter Understanding your PICC procedure and consent form Please read this handout before reading and signing the form Special Consent for
Deep Brain Stimulation (DBS) Pre-operative information for people with Tremor
 Pre-operative information for people with Tremor") Oxford University Hospitals NHS Trust Department of Neurological Surgery John Radcliffe Hospital Deep Brain Stimulation (DBS) Pre-operative information for people with Tremor We have been able to help
Oxford University Hospitals NHS Trust Department of Neurological Surgery John Radcliffe Hospital Deep Brain Stimulation (DBS) Pre-operative information for people with Tremor We have been able to help
Caring for Your Jackson Pratt Drainage System
 Caring for Your Jackson Pratt Drainage System This booklet was originally written by Barbara Cree-Loveless, RN and Cynthia Knauer, RN, MS Introduction This booklet describes how to care for your Jackson
Caring for Your Jackson Pratt Drainage System This booklet was originally written by Barbara Cree-Loveless, RN and Cynthia Knauer, RN, MS Introduction This booklet describes how to care for your Jackson
DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2050 Worth Road Fort Sam Houston, Texas
 DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2050 Worth Road Fort Sam Houston, Texas 78234-6010 MEDCOM Circular 29 May 2008 No. 40-17 Expires 29 May 2010 Medical Services PREVENTING
DEPARTMENT OF THE ARMY HEADQUARTERS, UNITED STATES ARMY MEDICAL COMMAND 2050 Worth Road Fort Sam Houston, Texas 78234-6010 MEDCOM Circular 29 May 2008 No. 40-17 Expires 29 May 2010 Medical Services PREVENTING
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
SURGICAL CASE MANAGEMENT THEORY
 THEORY Course Syllabus Course Number: STAP 0145A OHLAP Credit: No OCAS Code: None Course Length: 30 Hours Career Cluster: Health Science Career Pathway: Therapeutic Services Career Major(s): Surgical Technologist
THEORY Course Syllabus Course Number: STAP 0145A OHLAP Credit: No OCAS Code: None Course Length: 30 Hours Career Cluster: Health Science Career Pathway: Therapeutic Services Career Major(s): Surgical Technologist
IMPLEMENTING QSEN: CHALLENGES & OPPORTUNITIES
 IMPLEMENTING QSEN: CHALLENGES & OPPORTUNITIES Margaret Rowberg, DNP, APN Jennifer Lillibridge, RN, PhD California State University, Chico School of Nursing FOCUS OF PRESENTATION Objectives Present results
IMPLEMENTING QSEN: CHALLENGES & OPPORTUNITIES Margaret Rowberg, DNP, APN Jennifer Lillibridge, RN, PhD California State University, Chico School of Nursing FOCUS OF PRESENTATION Objectives Present results
Resources for Your Business. OSHA Recordkeeping: Requirements & Best Pracices
 Resources for Your Business OSHA Recordkeeping: Requirements & Best Pracices Essentials Risk Management Resources from Key Risk This presentation provides general information and suggestions related to
Resources for Your Business OSHA Recordkeeping: Requirements & Best Pracices Essentials Risk Management Resources from Key Risk This presentation provides general information and suggestions related to
Principles In developing these recommendations the Consensus Panel first established the following principles for anesthesia outcomes capture:
 Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
A new option for you. What is the Primo Port?
 Totally Implantable Port Patient Information Synchronizing Medical Innovation with Global Markets A new option for you Your treatment may require frequent injections of medicine, or other IV fluids directly
Totally Implantable Port Patient Information Synchronizing Medical Innovation with Global Markets A new option for you Your treatment may require frequent injections of medicine, or other IV fluids directly
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
Jersey Shore University Medical Center Ob/Gyn Residency Program Educational Goals and Objectives for GYNECOLOGY PGY
 These are the Educational Goals and Objectives for the Gynecology Rotation. Please review and become familiar with these goals and objectives. The Chief Resident on the Gynecology Rotation is responsible
These are the Educational Goals and Objectives for the Gynecology Rotation. Please review and become familiar with these goals and objectives. The Chief Resident on the Gynecology Rotation is responsible
Sample Reportable Events
 Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES
 WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS
 Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Ambulatory Surgical Center (ASC) INFECTION CONTROL SURVEYOR WORKSHEET
 INFECTION CONTROL SURVEYOR WORKSHEET") Ambulatory Surgical Center (ASC) INFECTION CONTROL SURVEYOR WORKSHEET Name of State Agency or AO (please print at right): HFAP Instructions: The following is a list of items that must be assessed during
Ambulatory Surgical Center (ASC) INFECTION CONTROL SURVEYOR WORKSHEET Name of State Agency or AO (please print at right): HFAP Instructions: The following is a list of items that must be assessed during
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE
 How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
Patient Instructions after Surgery: Caring for your Drain(s)
") Patient Instructions after Surgery: Caring for your Drain(s) A surgical drain is a soft, flexible, plastic tube that is connected to a plastic collection bulb. Drains are used to prevent fluid from collecting
Patient Instructions after Surgery: Caring for your Drain(s) A surgical drain is a soft, flexible, plastic tube that is connected to a plastic collection bulb. Drains are used to prevent fluid from collecting
Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt
 Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
INFECTION CONTROL SURVEYOR WORKSHEET
 Attachment 2 Exhibit 351 INFECTION CONTROL SURVEYOR WORKSHEET Instructions: The following is a list of items that must be assessed during the on-site survey, in order to determine compliance with the infection
Attachment 2 Exhibit 351 INFECTION CONTROL SURVEYOR WORKSHEET Instructions: The following is a list of items that must be assessed during the on-site survey, in order to determine compliance with the infection
NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS. Principles and Practices of Surgical Technology Lab
 NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS COURSE IDENTIFICATION Course Code/Number: SURG 103 Course Title: Principles and Practices of Surgical Technology Lab Division: Applied Science (AS)
NEOSHO COUNTY COMMUNITY COLLEGE MASTER COURSE SYLLABUS COURSE IDENTIFICATION Course Code/Number: SURG 103 Course Title: Principles and Practices of Surgical Technology Lab Division: Applied Science (AS)