Building an Evidence Base for Clinical Practice: Role of Pragmatic Trials Gary E. Rosenthal, MD
|
|
|
- Godfrey Hudson
- 6 years ago
- Views:
Transcription
1 Building an Evidence Base for Clinical Practice: Role of Pragmatic Trials Gary E. Rosenthal, MD Roy J. Carver Chair in Internal Medicine Professor and Interim Chairman, Department of Internal Medicine Director, University of Iowa Institute for Clinical and Translational Science November 7, 2014 *
2 Clinical Practice in the US: Biopsy Total expenditures of $2.9 trillion in 2013 (18% of GDP) Per capita expenses 50% higher than next most expensive nation (Norway) & 2.5 times higher than median for other industrialized nations Comparative study of 7 nations (US, UK, Australia, NZ, Canada, Germany, & Netherlands) US ranked last or next to last on measures of access, safety, efficiency, care coordination, & equity (Commonwealth Fund) Significant variation in costs across US Higher costs do not yield higher quality
 Quality")
3 State Rankings for 24 Quality Measures & Medicare Spending (Baicker & Chandra, Health Affairs 2004) Quality Spending
4 Recent estimates: Inescapable Diagnosis: Little Bang for the Buck 30% of Medicare spending could be avoided without worsening patient outcomes (Dartmouth Institute) 1/3 of healthcare expenditures is wasteful (Berwick, 2012)
5 Little Bang for the Buck: Lack of High Quality Evidence Underlying factors complex but include the lack of high quality clinical evidence on what works in healthcare Less than 20% of interventions used in common clinical practice based on evidence from RCTs Many RCTs study homogeneous populations limits generalizability to large percent of patients in routine practice, including those with multiple comorbidities who drive substantial healthcare spending.
6 How Can We Build the Necessary Evidence Base to Improve Clinical Practice? Traditional multi-site RCTs are expensive $50 to 250 million Thus, new paradigms urgently needed to create high quality evidence to inform clinical decision making Learning Health Systems Practice-based pragmatic trials
7 Overview of Presentation Present working definitions of a learning health system and a practice-based pragmatic clinical trial Contrast differences between pragmatic trials and traditional clinical trials Review methodological and cultural issues that must be addressed to: Advance agendas in pragmatic trials and practicebased research and enable creation of high value learning health systems
8 Learning Health System: What is It? (Institute of Medicine, 2007) A delivery system in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience. *

9 * Learning Health System (Green, 2012)
10 Learning Health System: What s Different? 1. Tight integration between research and practice such that research findings directly inform practice and key issues faced by practitioners become the focus of future research projects 2. Research is conducted in routine practice settings with modest research infrastructures 3. Health system resources, such as the EMR, are an integral part of the infrastructure
11 Pragmatic Clinical Trials Term first used by Schwarz and Llellouch in 1967 (J Chron Dis 1967; 20: ) Distinguished between trials that were explanatory in orientation and trials that were pragmatic Explanatory: aimed at mechanistic understanding discover if a difference exists between two treatments that are specified by strict definitions Pragmatic: aimed at clinical decision-making discover which treatment would be preferred as the treatments would be administered in clinical practice
12 Differences in Explanatory & Pragmatic Approaches to Trial Design (Schwarz & Lellouch, 1967) Possible study comparing XRT alone and XRT plus sensitizing drug administered 30 days prior to XRT Explanatory approach to control group XRT preceded by 30-day period in which no Rx given XRT + drug group and XRT alone control group receive XRT at same time Pragmatic approach to control group XRT given right after decision to use XRT is made XRT + drug and XRT alone groups control receive XRT at different time
13 Differences Between Pragmatic and Explanatory Trials Differences in Study Populations Explanatory trials often enroll homogeneous patients with few comorbid conditions to reduce response variation PCTs have fewer patient selection criteria & seek to enroll more heterogeneous populations may have higher external validity but lower internal validity PCTs may require larger sample sizes because of patient heterogeneity
14 Differences Between Pragmatic and Explanatory Trials (cont.) Differences in Treatment & Control Groups Explanatory trials often compare new treatments to placebo treatments and may not compare a new treatment to existing treatments PCTs typically compare two or more standard of care treatments, often for which there is clinical equipoise In PCTs, patients & clinicians typically not blinded to treatment assignment however, allocation to study groups should be random and assessment of outcomes should be blinded
15 Differences Between Pragmatic and Explanatory Trials (cont.) Differences in the Intervention Being Tested Explanatory interventions typically delivered by specialized practitioners in highly controlled settings to maximize intervention fidelity Pragmatic interventions: delivered in routine practice settings with modest infrastructures to support delivery of intervention incorporate flexibility to account for the individual needs of patients & capabilities of delivery settings
16 Differences Between Pragmatic and Explanatory Trials (cont.) Other Important Issues PCTs may require longer follow-up to track outcomes reflecting real life concerns of patients & may be better suited to study chronic conditions that require treatment over many years Analysis typically based on intention-to-treat approach recognizing that treatment cross-over may be more common than in explanatory trials
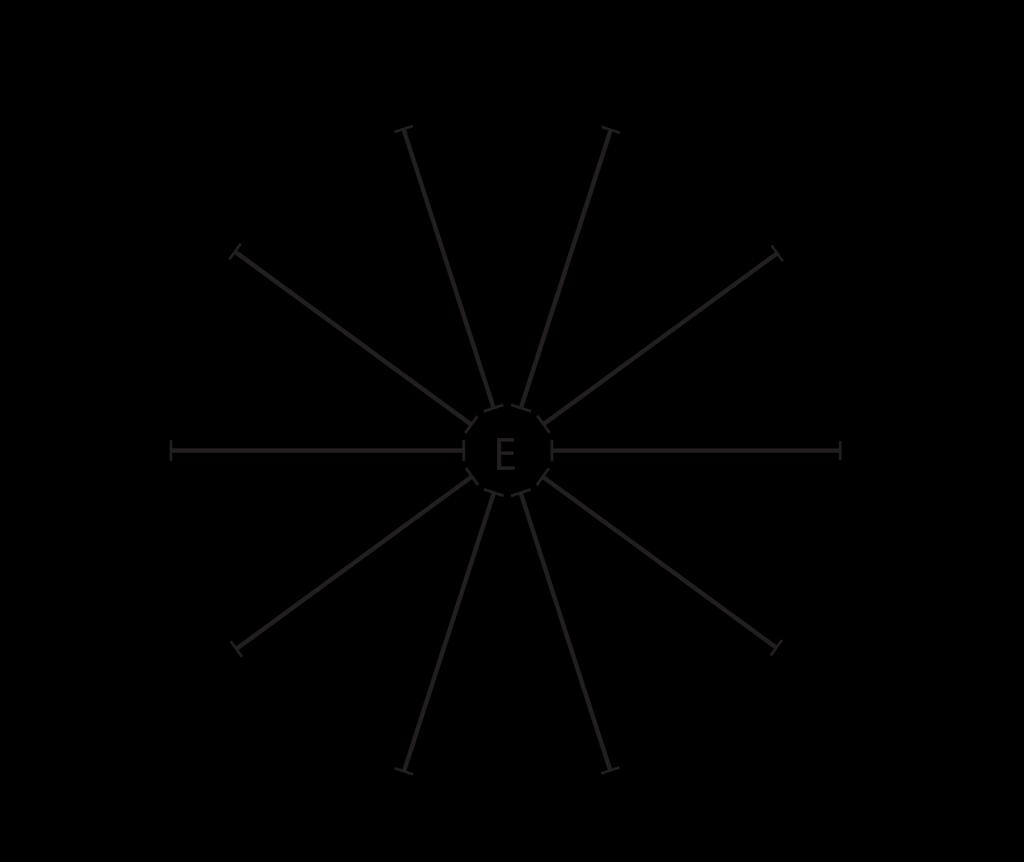
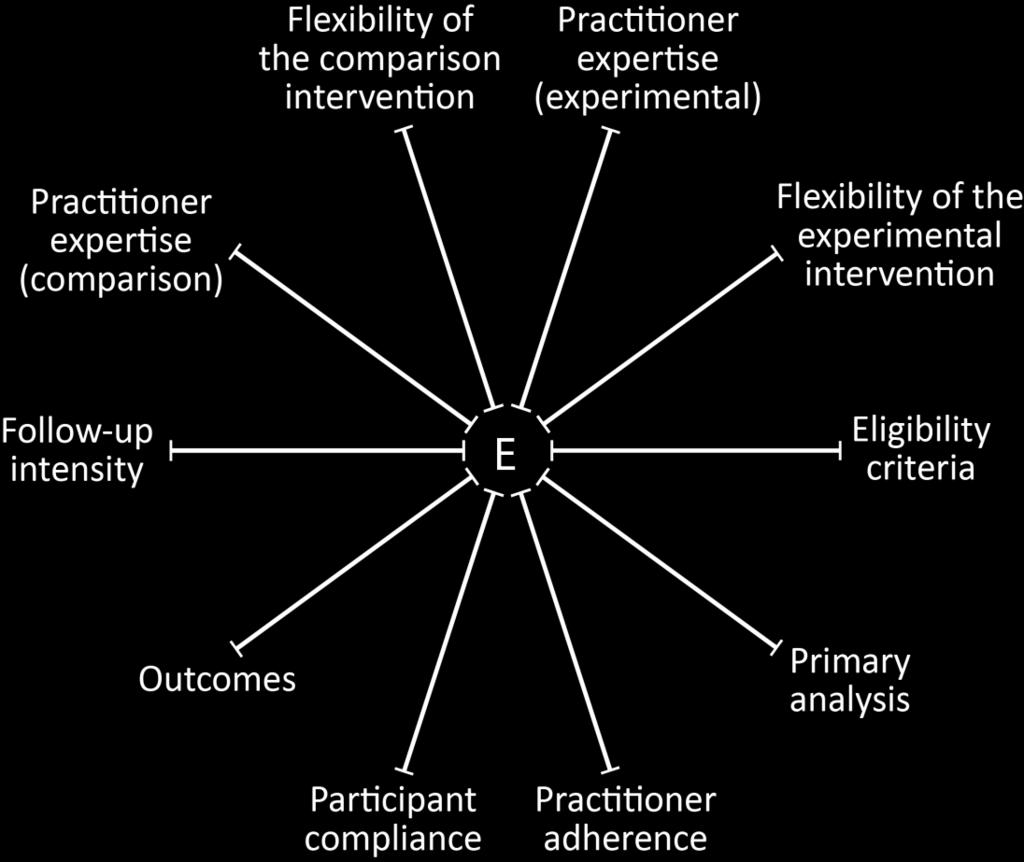
17 Pragmatic-Explanatory Continuum Indicator Summary (PRECIS) (Thorpe, CMAJ 2009)


18 Classification of Trials Using PRECIS 1. Self-Administered vs. Observed TB Rx 2. North American CEA Trial 3. Low Dose ASA Study in Pregnancy 4. ASA in Pre-eclampsia
19 Pragmatic Trial Example: Night Time Dosing of Antihypertensives Goal of Study Examine the impact of nighttime dosing of antihypertensive medications by comparing rates of adverse CV events in patients randomized to take their once daily BP medications either in the morning or at night
20 Rationale for Night Time Dosing Trial BP exhibits circadian variability lower during sleep ( nighttime dipping ) with increase on arising (may explain excess risk of AMI during early am) Sleep BP stronger predictor of CV risk than daytime BP Lack of nighttime dipping associated with excess CV risk Many q day BP meds do not sustain plasma levels for full 24 hours and when taken in AM, may not promote nighttime dipping or protect against AM surge in BP 3 recent RCTs trials found that patients taking 1 or more BP meds at night had a 65% reduction in CV events
21 Why is Nighttime Dosing an Ideal Topic for a Pragmatic Trial? HTN is common problem & major CV risk factor Eligible patients can be identified through EMR Key endpoints (adverse CV events) can be captured through the EMR and other extant data sources Nighttime dosing can be implemented in practice without the need for sophisticated infrastructure Intervention has high potential for sustainability if pragmatic trial confirms prior clinical trials
22 Night Time Dosing: Overview of Trial Design Eligibility Criteria Age years with HTN & > 1 comorbid condition that increases cardiovascular risk 2 or more ambulatory visits in past 12 months to General Medicine or Family Medicine clinics Prescriptions for > 1 once-daily anti-hypertensives (excluding diuretics) Informed consent obtained using online interactive consent module or mailed consent letter Patients followed for months with f/u contacts every 6 months via online portal or paper survey
23 Night Time Dosing: Overview of Trial Design (cont.) CV events obtained from EMR, online or paper surveys, & extant data (Medicare claims & death certificates) Death Hospitalizations for AMI, IHD, CHF, stroke coronary, cerebral, or peripheral revascularization Sample size ~ 20,000 patients (8-9 sites) to detect 10-15% difference in event rates for composite endpoint of the above CV events Estimated Cost: $10 million ($500 patient) 10-15% of cost of traditional multi-site hypertension trial
24 Pragmatic Trial Example: Targeted versus Universal Decolonization to Prevent ICU Infection (Huang SS et al, New Engl J Med 2013; 368: ) Goal of Study Compare targeted decolonization and universal decolonization strategies to prevent healthcare associated MRSA infections in ICU patients
25 Targeted versus Universal Decolonization: Overview of Trial Design Cluster-randomized trial of 74,256 patients in 74 ICUs in 47 HCA hospitals Hospitals randomly assigned to 1 of 3 strategies 1. Universal MRSA screening with isolation of all MRSA carriers 2. Targeted decolonization (universal screening with isolation, and decolonization of MRSA carriers) 3. Universal decolonization (i.e., no screening, and decolonization of all patients)
26 Targeted versus Universal Decolonization: Overview of Trial Design (cont.) Primary Endpoint ICU-attributable, MRSA infections Secondary Endpoints ICU bloodstream infections caused by MRSA and by any other pathogen Endpoints compared in 12-month baseline and 18- month intervention period for each of the 3 strategies Data Sources: Census and unit location data for each patienta Microbiology, pharmacy, & administrative data Pathogens attributed to an ICU infection if collection date between 3 rd day after ICU admission and 2 nd day after ICU discharge
27 Targeted versus Universal Decolonization: Results MRSA infections (Intervention to Baseline hazard ratio): Screening & Isolation 0.92 Targeted Decolonization 0.75 * Universal Decolonization 0.63 * Bloodstream infections with any pathogen / MRSA: Screening & Isolation 0.99 / 1.23 (NS) Targeted Decolonization 0.78 * / 1.23 (NS) Universal Decolonization 0.56 * / 0.72 * P<.05
28 Targeted versus Universal Decolonization: Why is this Study a Pragmatic Trial? 3 strategies compared are approaches that are commonly used to reduce ICU infections in practice Strategies were administered in the course of routine care by hospital nursing personnel Clinical cultures were obtained at the clinician s discretion All data obtained from corporate data warehouses no independent data collection Validation of infections based on standard CDC criteria that are used in practice to attribute infections
29 Key Issues in Advancing PCTs and Creating Learning Health Systems 1. Improve efficiency of subject recruitment 2. Develop reliable clinical phenotypes from EMR data and improve the quality of information captured in the EMR 3. More effective strategies for engaging healthcare systems and physicians in practice-based PCTs 4. Decrease regulatory barriers for conducting low-risk PCTs
30 Key Issues in Advancing PCTs and Creating Learning Health Systems 1. Improve efficiency of subject recruitment 2. Develop reliable clinical phenotypes from EMR data and improve the quality of information captured in the EMR 3. More effective strategies for engaging healthcare systems and physicians in practice-based PCTs 4. Decrease regulatory barriers for conducting low-risk PCTs
31 Improve Efficiency of Subject Recruitment Inadequate recruitment is one of the biggest challenges to the US clinical research enterprise and one of the biggest concerns of NIH Overall, clinical trials enrollment rates dropped from 75% in 2000 of what was initially planned to 59% in 2006, while subject retention rates fell from 69% to 48% during same period More than 80% of trials are delayed at least one month because of unfulfilled enrollment
32 Enhancing Subject Recruitment: EMR Approaches to Identifying Subjects (Embi, Arch Int Med 2005) Developed clinical trial alert (CTA) in Epic for DM trial that identified patients on the basis of diagnosis, age (> 40), and HgbA1C (> 7.4%) Targeted to 10 endocrinologists and 104 general internists at the point of care CTA prompted MDs to consider additional criteria that could not be reliably obtained from the EMR MD could then send referral order to coordinator if patient interested in participating
33 EMR Approaches to Identifying Subjects: Results (Embi, Arch Int Med 2005): Compared enrollment in the 12 months before and the four months after CTA was implemented. 12 month Control Period - 5 MDs referred 68 patients to study coordinator, of whom 35 were ultimately enrolled enrollment rate of 2.9 patients per month 4 month Intervention Period - 42 MDs 238 patients, of whom 48 were ultimately enrolled enrollment rate of 6.0 per month
34 EMR Approaches to Identifying Subjects: Recent UI Experience NIH funded randomized trial of intervention to increase visual processing speed in older adults. EMR-based algorithm used to identify patients in General Medicine and Family Medicine clinics who: (1) were > 50 years; (2) had > 2 clinic visits in past 12 months; and (3) didn t have diagnosis of dementia Of 5743 eligible patients identified and sent single mailing, 996 expressed interest in participating Of these, 681 enrolled over a 6-month period.
35 Key Issues in Advancing PCTs and Creating Learning Health Systems 1. Improve efficiency of subject recruitment 2. Develop reliable clinical phenotypes from EMR data and improve the quality of information captured in the EMR 3. More effective strategies for engaging healthcare systems and physicians in practice-based PCTs 4. Decrease regulatory barriers for conducting low-risk PCTs
36 Develop More Reliable Clinical Current Challenges Phenotypes from EMR Data Majority of information in EMRs contained in clinical notes in free text formats difficult to extract given current limitations in NLP methods Variability across different EMRs in capturing diagnostic & phenotypic information particularly problematic for diagnoses (tremendous variability even from clinic to clinic in individual institutions) Limited standardization of phenotypic definitions for most clinical conditions
37 Impact of Unreliable Phenotypes (Abrams et al, Circulation 2009) Research question: What is the impact of comorbid depression on in-hospital mortality Sample: 21,745 consecutive admissions to VA hospitals for AMI 2 approaches for defining comorbid depression: - Inpatient: diagnoses recorded during the incident admission - Outpatient: diagnoses recorded during prior clinic visits
38 Results: Impact of Unreliable Phenotypes (Abrams et al, Circulation 2009) Prevalence of depression: - Inpatient diagnoses 10% - Outpatient diagnoses 24% Adjusted odds of death for patients with depression, relative to patients without depression (1.0) - Inpatient diagnoses 0.89 (95% CI, ) - Outpatient diagnoses 1.19 (95% CI, )
39 What s Needed Develop More Reliable Clinical Phenotypes from EMR Data 1. Develop library of computable definitions to enable phenotyping for important clinical conditions 2. Validate definitions across different EMR systems and different institutions 3. Synthesize best practices for entering data into EMR 4. Standardize approaches used by clinicians in entering clinical data elements into the EMR (increase use of structured data fields and flowsheets)
40 Key Issues in Advancing PCTs and Creating Learning Health Systems 1. Improve efficiency of subject recruitment 2. Develop reliable clinical phenotypes from EMR data and improve the quality of information captured in the EMR 3. More effective strategies for engaging healthcare systems and physicians in practice-based PCTs 4. Decrease regulatory barriers for conducting low-risk PCTs
41 More Effective Strategies for Engaging Healthcare Systems and Physicians 1. Study designs & interventions that can be easily embedded into practice & not impede clinic workflow 2. Greater attention to obtaining input from front-line clinicians regarding prioritization of research topics & project implementation strategies 3. Integrating incentives into faculty reward systems (e.g., PCT involvement as factor in promotion, providing RVUs for subject recruitment) 4. Create institutional cultures that value knowledge generation
42 Key Issues in Advancing PCTs and Creating Learning Health Systems 1. Improve efficiency of subject recruitment 2. Develop reliable clinical phenotypes from EMR data and improve the quality of information captured in the EMR 3. More effective strategies for engaging healthcare systems and physicians in practice-based PCTs 4. Decrease regulatory barriers for conducting low-risk PCTs
43 Hastings Center Report (Kass & Faden): Research-Treatment Distinction Features currently used to distinguish research from practice. Research involves - Systematic investigation to produce generalizable knowledge - Less net clinical benefit & greater risk than practice - Introduces burdens or risks that are otherwise not part of patients clinical management - Use of protocols that dictate which treatments patients receive Systematically identifies problems with each of the 5 features and concludes that features are out of date
44 Hastings Center Report (Kass & Faden): Ethics Framework in a LHCS 1. Moral priority on learning healthcare professionals & institutions have novel obligation to contribute to learning in health care 2. Similar obligation extends to patients justified by principle of the common good, (i.e., members of a society have a common interest in ensuring an affordable, high quality healthcare system 3. Obligation to address unjust inequalities LHCS has obligation to decrease inequalities in evidence base for clinical decision making & in healthcare outcomes
45 Take Home Points 1. PCTs hold enormous potential for decreasing the cost of answering questions about the effectiveness of interventions commonly used in clinical practice 2. The success of national agendas in PCTs will depend on innovative strategies to: Improve the efficiency of subject recruitment; Standardize clinical phenotypes that can be obtained from EMR data Decrease regulatory hurdles to conducting practicebased research of standard of care treatments Engage clinicians & reward their participation in PCTs
46 Take Home Points (cont.) 4. PCTs can be a central feature of true learning health systems in which. science, informatics, incentives, and culture are aligned for continuous improvement & innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience. 5. Academic medical centers are uniquely positioned and have a societal obligation to drive the creation of learning health systems that generate the evidence needed to practice high value care
Research Opportunities to Improve Hypertension Control
 Research Opportunities to Improve Hypertension Control Barry L. Carter, Pharm.D., FCCP, FAHA, FASH The Patrick E. Keefe Professor in Pharmacy Department of Pharmacy Practice and Science College of Pharmacy
Research Opportunities to Improve Hypertension Control Barry L. Carter, Pharm.D., FCCP, FAHA, FASH The Patrick E. Keefe Professor in Pharmacy Department of Pharmacy Practice and Science College of Pharmacy
Pay-for-Performance: Approaches of Professional Societies
 Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes. James X. Zhang, PhD, MS The University of Chicago
 Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Cluster randomization for Clinical Effectiveness Research. Richard Platt, MD, MSc Harvard Medical School and Harvard Pilgrim Health Care Institute
 Cluster randomization for Clinical Effectiveness Research Richard Platt, MD, MSc Harvard Medical School and Harvard Pilgrim Health Care Institute REDUCE MRSA Trial Randomized Evaluation of Decolonization
Cluster randomization for Clinical Effectiveness Research Richard Platt, MD, MSc Harvard Medical School and Harvard Pilgrim Health Care Institute REDUCE MRSA Trial Randomized Evaluation of Decolonization
Pragmatic Trial Designs Capturing Endpoints and Integrating Data from Non-Linked Sources
 Pragmatic Trial Designs Capturing Endpoints and Integrating Data from Non-Linked Sources Matthew T. Roe, MD, MHS Duke Clinical Research Institute Conflict of Interest Statement Matthew T. Roe, MD, MHS
Pragmatic Trial Designs Capturing Endpoints and Integrating Data from Non-Linked Sources Matthew T. Roe, MD, MHS Duke Clinical Research Institute Conflict of Interest Statement Matthew T. Roe, MD, MHS
Conducting Comparative Effectiveness Research in the Real World:
 Conducting Comparative Effectiveness Research in the Real World: An Anthropologic Perspective Marilyn Laken, PhD, RN Professor of Nursing MUSC Topic Areas: Anthropologic Perspective Background: Anthropology,
Conducting Comparative Effectiveness Research in the Real World: An Anthropologic Perspective Marilyn Laken, PhD, RN Professor of Nursing MUSC Topic Areas: Anthropologic Perspective Background: Anthropology,
Kaiser Permanente Northern California Large Scale Hypertension Control Program
 Kaiser Permanente Northern California Large Scale Hypertension Control Program Marc Jaffe, MD Clinical Leader, Kaiser Northern California Cardiovascular Risk Reduction Program Clinical Leader, Kaiser National
Kaiser Permanente Northern California Large Scale Hypertension Control Program Marc Jaffe, MD Clinical Leader, Kaiser Northern California Cardiovascular Risk Reduction Program Clinical Leader, Kaiser National
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Version 1.0 (posted Aug ) Aaron L. Leppin. Background. Introduction
 Aaron L. Leppin. Background. Introduction") Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Conducting patient-oriented pragmatic trials in Ontario: opportunities and challenges
 Conducting patient-oriented pragmatic trials in Ontario: opportunities and challenges CTO 2015 Clinical Trials Conference Toronto, Ontario March 5th Dean Fergusson Senior Scientist & Director, Clinical
Conducting patient-oriented pragmatic trials in Ontario: opportunities and challenges CTO 2015 Clinical Trials Conference Toronto, Ontario March 5th Dean Fergusson Senior Scientist & Director, Clinical
The REDUCE MRSA Trial. Randomized Evaluation of Decolonization vs. Universal Clearance to Eliminate MRSA
 The REDUCE MRSA Trial Randomized Evaluation of Decolonization vs. Universal Clearance to Eliminate MRSA 1 Disclosures The REDUCE MRSA investigative team is conducting a follow up trial in non-critical
The REDUCE MRSA Trial Randomized Evaluation of Decolonization vs. Universal Clearance to Eliminate MRSA 1 Disclosures The REDUCE MRSA investigative team is conducting a follow up trial in non-critical
University of Iowa Institute for Clinical and Translational Science (ICTS)
") University of Iowa Institute for Clinical and Translational Science (ICTS) Gary E. Rosenthal, MD Professor of Internal Medicine and Health Management and Policy Director, Institute for Clinical & Translational
University of Iowa Institute for Clinical and Translational Science (ICTS) Gary E. Rosenthal, MD Professor of Internal Medicine and Health Management and Policy Director, Institute for Clinical & Translational
England: Europe s healthcare reform laboratory? Peter C. Smith Imperial College Business School and Centre for Health Policy
 England: Europe s healthcare reform laboratory? Peter C. Smith Imperial College Business School and Centre for Health Policy Total health care expenditure as % of GDP by country, 1960-2006 18 16 14 12
England: Europe s healthcare reform laboratory? Peter C. Smith Imperial College Business School and Centre for Health Policy Total health care expenditure as % of GDP by country, 1960-2006 18 16 14 12
Topic 7: Pilot and Feasibility Testing
 Topic 7: Pilot and Feasibility Testing Wendy Weber, ND, PhD, MPH National Center for Complementary and Integrative Health (NCCIH) Collaboratory epct Training Workshop Overview Importance of piloting the
Topic 7: Pilot and Feasibility Testing Wendy Weber, ND, PhD, MPH National Center for Complementary and Integrative Health (NCCIH) Collaboratory epct Training Workshop Overview Importance of piloting the
Inaugural Barbara Starfield Memorial Lecture
 Inaugural Barbara Starfield Memorial Lecture Wonca World Conference Prague, June 29, 2013 Copyright 2013 Johns Hopkins University,. Improving Coordination between Primary and Secondary Health Care through
Inaugural Barbara Starfield Memorial Lecture Wonca World Conference Prague, June 29, 2013 Copyright 2013 Johns Hopkins University,. Improving Coordination between Primary and Secondary Health Care through
Click to edit Master title style
 Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Cardiovascular Disease Prevention: Team-Based Care to Improve Blood Pressure Control
 Cardiovascular Disease Prevention: Team-Based Care to Improve Blood Pressure Control Task Force Finding and Rationale Statement Table of Contents Intervention Definition... 2 Task Force Finding... 2 Rationale...
Cardiovascular Disease Prevention: Team-Based Care to Improve Blood Pressure Control Task Force Finding and Rationale Statement Table of Contents Intervention Definition... 2 Task Force Finding... 2 Rationale...
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO
 CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO Disclaimers My current position I am not offering advice on clinical integration Items
CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO Disclaimers My current position I am not offering advice on clinical integration Items
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System
 Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System Karen Davis President, The Commonwealth Fund IOM Workshop Series: The Policy Agenda September
Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System Karen Davis President, The Commonwealth Fund IOM Workshop Series: The Policy Agenda September
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
The Learning Healthcare System Building Effective, Affordable Care
 The Learning Healthcare System Building Effective, Affordable Care Brent James, MD, MStat Executive Director, Institute for Health Care Delivery Research Outline 1. Change accelerates: Health reform =
The Learning Healthcare System Building Effective, Affordable Care Brent James, MD, MStat Executive Director, Institute for Health Care Delivery Research Outline 1. Change accelerates: Health reform =
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Background and Issues. Aim of the Workshop Analysis Of Effectiveness And Costeffectiveness. Outline. Defining a Registry
 Aim of the Workshop Analysis Of Effectiveness And Costeffectiveness In Patient Registries ISPOR 14th Annual International Meeting May, 2009 Provide practical guidance on suitable statistical approaches
Aim of the Workshop Analysis Of Effectiveness And Costeffectiveness In Patient Registries ISPOR 14th Annual International Meeting May, 2009 Provide practical guidance on suitable statistical approaches
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Comparative Effectiveness Research and Patient Centered Outcomes Research in Public Health Settings: Design, Analysis, and Funding Considerations
 University of Kentucky UKnowledge Health Management and Policy Presentations Health Management and Policy 12-7-2012 Comparative Effectiveness Research and Patient Centered Outcomes Research in Public Health
University of Kentucky UKnowledge Health Management and Policy Presentations Health Management and Policy 12-7-2012 Comparative Effectiveness Research and Patient Centered Outcomes Research in Public Health
Long term commitment to a new vision. Medical Director February 9, 2011
 ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Medical Device Reimbursement in the EU, current environment and trends. Paula Wittels Programme Director
 Medical Device Reimbursement in the EU, current environment and trends Paula Wittels Programme Director 20 November 2009 1 agenda national and regional nature of EU reimbursement trends in reimbursement
Medical Device Reimbursement in the EU, current environment and trends Paula Wittels Programme Director 20 November 2009 1 agenda national and regional nature of EU reimbursement trends in reimbursement
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers
 Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
HIMSS Submission Leveraging HIT, Improving Quality & Safety
 HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
From Private Practice to an Integrated Health System: Playing to Your Strengths
 From Private Practice to an Integrated Health System: Playing to Your Strengths Mark Schickendantz, MD Director, Cleveland Clinic Center for Sports Health Associate Professor of Surgery, Cleveland Clinic
From Private Practice to an Integrated Health System: Playing to Your Strengths Mark Schickendantz, MD Director, Cleveland Clinic Center for Sports Health Associate Professor of Surgery, Cleveland Clinic
Incentives and Penalties
 Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
Models of Nurse-led Integrative care globally
 Models of Nurse-led Integrative care globally Dr. Catriona Jennings, Cardiovascular Specialist Nurse Imperial College London and CCNAP Chair World Heart Federation African Summit Khartoum, Sudan October
Models of Nurse-led Integrative care globally Dr. Catriona Jennings, Cardiovascular Specialist Nurse Imperial College London and CCNAP Chair World Heart Federation African Summit Khartoum, Sudan October
Academic Clinical Practice Work Group Strategic Plan DRAFT June 3, 2014
 Academic Clinical Practice Work Group Strategic Plan DRAFT June 3, 2014 The Academic Clinical Practice work group conducted a SWOT exercise and considered the following questions in its deliberations on
Academic Clinical Practice Work Group Strategic Plan DRAFT June 3, 2014 The Academic Clinical Practice work group conducted a SWOT exercise and considered the following questions in its deliberations on
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Disclosures. Platforms for Performance: Clinical Dashboards to Improve Quality and Safety. Learning Objectives
 Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Ethics for a learning health care system: The Common Purpose Framework. Nancy E. Kass, ScD Johns Hopkins Berman Institute of Bioethics
 Ethics for a learning health care system: The Common Purpose Framework Nancy E. Kass, ScD Johns Hopkins Berman Institute of Bioethics Project Team Ruth Faden, PhD, MPH Nancy Kass, ScD Tom Beauchamp, PhD
Ethics for a learning health care system: The Common Purpose Framework Nancy E. Kass, ScD Johns Hopkins Berman Institute of Bioethics Project Team Ruth Faden, PhD, MPH Nancy Kass, ScD Tom Beauchamp, PhD
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
2011 Electronic Prescribing Incentive Program
 2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
JH-CERSI/FDA Workshop Clinical Trials: Assessing Safety and Efficacy for a Diverse Population
 JH-CERSI/FDA Workshop Clinical Trials: Assessing Safety and Efficacy for a Diverse Population Use of Epidemiologic Studies to Examine Safety in Diverse Populations Judy A. Staffa, Ph.D, R.Ph. Director
JH-CERSI/FDA Workshop Clinical Trials: Assessing Safety and Efficacy for a Diverse Population Use of Epidemiologic Studies to Examine Safety in Diverse Populations Judy A. Staffa, Ph.D, R.Ph. Director
Using Secondary Datasets for Research. Learning Objectives. What Do We Mean By Secondary Data?
 Using Secondary Datasets for Research José J. Escarce January 26, 2015 Learning Objectives Understand what secondary datasets are and why they are useful for health services research Become familiar with
Using Secondary Datasets for Research José J. Escarce January 26, 2015 Learning Objectives Understand what secondary datasets are and why they are useful for health services research Become familiar with
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010)
") Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
Issue Brief. EHR-Based Care Coordination Performance Measures in Ambulatory Care
 November 2011 Issue Brief EHR-Based Care Coordination Performance Measures in Ambulatory Care Kitty S. Chan, Jonathan P. Weiner, Sarah H. Scholle, Jinnet B. Fowles, Jessica Holzer, Lipika Samal, Phillip
November 2011 Issue Brief EHR-Based Care Coordination Performance Measures in Ambulatory Care Kitty S. Chan, Jonathan P. Weiner, Sarah H. Scholle, Jinnet B. Fowles, Jessica Holzer, Lipika Samal, Phillip
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
DANNOAC-AF synopsis. [Version 7.9v: 5th of April 2017]
![DANNOAC-AF synopsis. [Version 7.9v: 5th of April 2017]](/thumbs/77/75232655.jpg "DANNOAC-AF synopsis. [Version 7.9v: 5th of April 2017]") DANNOAC-AF synopsis. [Version 7.9v: 5th of April 2017] A quality of care assessment comparing safety and efficacy of edoxaban, apixaban, rivaroxaban and dabigatran for oral anticoagulation in patients
DANNOAC-AF synopsis. [Version 7.9v: 5th of April 2017] A quality of care assessment comparing safety and efficacy of edoxaban, apixaban, rivaroxaban and dabigatran for oral anticoagulation in patients
Healthcare- Associated Infections in North Carolina
 2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
U.S. Healthcare Problem
 U.S. Healthcare Problem U.S. Federal Spending GDP (%) Source: Congressional Budget Office This graph shows that government has to spend a lot of more money in healthcare in the future and it is growing
U.S. Healthcare Problem U.S. Federal Spending GDP (%) Source: Congressional Budget Office This graph shows that government has to spend a lot of more money in healthcare in the future and it is growing
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Ambulatory Care Practice Trends and Opportunities in Pharmacy
 Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Engineering a Learning Healthcare System
 Engineering a Learning Healthcare System The Department of Veterans Affairs Point of Care Research Program Ryan E. Ferguson, ScD, MPH Acting Center Director, VA CSP Coordinating Center Deputy Director,
Engineering a Learning Healthcare System The Department of Veterans Affairs Point of Care Research Program Ryan E. Ferguson, ScD, MPH Acting Center Director, VA CSP Coordinating Center Deputy Director,
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT
 April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
IMPROVING YOUR CLINICAL TRIAL & ENHANCING THE PATIENT EXPERIENCE
 ebook IMPROVING YOUR CLINICAL TRIAL & ENHANCING THE PATIENT EXPERIENCE Applying a patient-centered approach to enhance clinical trial performance, improve data quality, and ensure safety and efficacy.
ebook IMPROVING YOUR CLINICAL TRIAL & ENHANCING THE PATIENT EXPERIENCE Applying a patient-centered approach to enhance clinical trial performance, improve data quality, and ensure safety and efficacy.
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS
 USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS January 2018 Funded by generous support from the California Hospital Association (CHA) Copyright 2018 by HealthImpact. All rights reserved.
USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS January 2018 Funded by generous support from the California Hospital Association (CHA) Copyright 2018 by HealthImpact. All rights reserved.
Pediatric Population Health
 JANUARY 25, 2018 Swedish Pediatric CME 2018 Pediatric Population Health Michael Dudas, MD Chief of Pediatrics, Virginia Mason Medical Center Co-Chair, Health Care Transformation Committee, WCAAP 1 Objectives
JANUARY 25, 2018 Swedish Pediatric CME 2018 Pediatric Population Health Michael Dudas, MD Chief of Pediatrics, Virginia Mason Medical Center Co-Chair, Health Care Transformation Committee, WCAAP 1 Objectives
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care Update
 Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Last Updated: June 21, 2013 Table of Contents Search Strategy... 2 What existing
Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Last Updated: June 21, 2013 Table of Contents Search Strategy... 2 What existing
Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors
 Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors TECHNICAL REPORT July 2, 2014 Contents EXECUTIVE SUMMARY... iii Introduction... iii Core Principles... iii Recommendations...
Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors TECHNICAL REPORT July 2, 2014 Contents EXECUTIVE SUMMARY... iii Introduction... iii Core Principles... iii Recommendations...
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Banner Health Friday, February 20, 2015
 Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
N.E.W.T. Level Measurement:
 N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
Definitions/Glossary of Terms
 Definitions/Glossary of Terms Submitted by: Evelyn Gallego, MBA EgH Consulting Owner, Health IT Consultant Bethesda, MD Date Posted: 8/30/2010 The following glossary is based on the Health Care Quality
Definitions/Glossary of Terms Submitted by: Evelyn Gallego, MBA EgH Consulting Owner, Health IT Consultant Bethesda, MD Date Posted: 8/30/2010 The following glossary is based on the Health Care Quality
INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION
 INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION CASE STUDY October 2016 1 AGENDA 1 2 3 INTRODUCTIONS Speaker and System 4 Q+A VALUE OF INTEGRATED DATA Why effective ACOs require EHR, Claims, and
INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION CASE STUDY October 2016 1 AGENDA 1 2 3 INTRODUCTIONS Speaker and System 4 Q+A VALUE OF INTEGRATED DATA Why effective ACOs require EHR, Claims, and
Accountable Care Collaborative: Transforming from Volume to Value
 Accountable Care Collaborative: Transforming from Volume to Value Risk Segmentation and Modeling American Medical Group Association Gary Piefer, MD, MS, FAAFP, FACPE Thursday June 14, 2010 WellMed Agenda
Accountable Care Collaborative: Transforming from Volume to Value Risk Segmentation and Modeling American Medical Group Association Gary Piefer, MD, MS, FAAFP, FACPE Thursday June 14, 2010 WellMed Agenda
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Targeted technology and data management solutions for observational studies
 Targeted technology and data management solutions for observational studies August 18th 2016 Zia Haque Arshad Mohammed Copyright 2016 Quintiles Your Presenters Zia Haque Senior Director of Data Management,
Targeted technology and data management solutions for observational studies August 18th 2016 Zia Haque Arshad Mohammed Copyright 2016 Quintiles Your Presenters Zia Haque Senior Director of Data Management,
Opportunities and Issues Related to BH Services in Primary Care
 Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Impactful Virtual Health in a Value-Based World. Healthcare Perspective
 Impactful Virtual Health in a Value-Based World Healthcare Perspective VIRTUAL HEALTH NOT ONLY ALLOWS PROVIDERS TO CONNECT WITH PATIENTS OUTSIDE OF THE TRADITIONAL CLINIC OR HOSPITAL LOCATIONS, BUT ALSO
Impactful Virtual Health in a Value-Based World Healthcare Perspective VIRTUAL HEALTH NOT ONLY ALLOWS PROVIDERS TO CONNECT WITH PATIENTS OUTSIDE OF THE TRADITIONAL CLINIC OR HOSPITAL LOCATIONS, BUT ALSO
Advances in Osteopathic Medicine
 Advances in Osteopathic Medicine Moving the value of osteopathic care from patients to populations Richard Snow DO, MPH Applied Health Services - Principal Choptank Community Health System Primary Care
Advances in Osteopathic Medicine Moving the value of osteopathic care from patients to populations Richard Snow DO, MPH Applied Health Services - Principal Choptank Community Health System Primary Care
A Primer on Activity-Based Funding
 A Primer on Activity-Based Funding Introduction and Background Canada is ranked sixth among the richest countries in the world in terms of the proportion of gross domestic product (GDP) spent on health
A Primer on Activity-Based Funding Introduction and Background Canada is ranked sixth among the richest countries in the world in terms of the proportion of gross domestic product (GDP) spent on health
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser