The National Audit of the Management of Familial Hypercholesterolaemia 2010
|
|
|
- Kelly Young
- 6 years ago
- Views:
Transcription



1 The National Audit of the Management of Familial Hypercholesterolaemia 2010 NATIONAL REPORT December 2010 Funded by: Royal College of Physicians, London British Heart Foundation Heart UK Cardiac Network Co-ordinating Group, Wales Conducted by: Clinical Standards Department, Royal College of Physicians, London Advised and approved by: The National Audit of Familial Hypercholesterolaemia Steering Group 1
2 CONTENTS Page AUTHORS 3 ACKNOWLEDGEMENTS 3 FOREWORD 4 EXECUTIVE SUMMARY 5 Key Findings 6 Key Recommendations 7 INTRODUCTION 8 Aims of the national audit 8 RESULTS 9 Summary of results 9 Comparing small and large audit sites 11 Conclusions 11 METHOD 12 Standards 12 Objective 12 National audit 13 Audit evaluation 15 PART 1: ORGANISATIONAL AUDIT 18 Section 1: Set Up 18 Section 2: Clinical Time 24 Section 3: Management of FH 26 Section 4: Cascade Testing 27 Section 5: Trust Services 29 Section 6: Patient Information 30 Section 7: Service Improvement 31 PART 2: CLINICAL AUDIT 32 Section 0 : General Information 32 Section 1: Diagnosis 36 Section 2: Pedigree 42 Section 3: Assessment 44 Section 4: Treatment 45 Section 5: Advice 53 Section 6: Cascade Testing 54 Section 7: (Annual) Review 56 APPENDICES 1: Steering Group 59 2: Glossary 61 3: Organisational Data 63 4: Comparison of Large vs Small Sites 64 5: Reliability Cases 68 6: FH Audit Participants 75 7: Site Feedback Survey 81 2
3 Report Authors This report was prepared by: Kristina Pedersen, National Familial Hypercholesterolaemia Audit Project Manager, Clinical Standards Department, Royal College of Physicians, London Professor Steve E. Humphries, Director, Centre for Cardiovascular Genetics, British Heart Foundation Laboratories, London and National Familial Hypercholesterolaemia Audit Project Director, Clinical Standards Department, Royal College of Physicians, London Michael Roughton, Medical Statistician, Clinical Standards Department, Royal College of Physicians, London Joseph Besford, National Familial Hypercholesterolaemia Audit Project Coordinator, Clinical Standards Department, Royal College of Physicians, London To reference this work: Pedersen KMV, Humphries SE, Roughton M, Besford JS. National Clinical Audit of the Management of Familial Hypercholesterolaemia 2010: Full Report. Clinical Standards Department, Royal College of Physicians, December 2010 Acknowledgements The time and effort given by all of the people who contributed to the development of the proforma and web-tool, and the NHS staff who undertook the audit is acknowledged (see Appendix 6). In particular, the following are thanked: members of the Working Group and Steering Group (see Appendix 1) Netsolving Limited who undertook the development of the audit web-tool all those who supported the project by providing their advice, direction and ideas 3
4 Foreword By the National Familial Hypercholesterolaemia Audit Project Director Professor Steve E. Humphries, The best way to limit the damage caused by coronary heart disease is to identify those at risk as early as possible. The greatest opportunity for such disease prevention lies in diagnosing and treating people with familial hypercholesterolaemia and screening their families. Currently there are some 100,000 undiagnosed people in the UK at risk of heart disease due to familial hypercholesterolaemia. NICE published guidelines in 2008 setting out how people with familial hypercholesterolaemia should be diagnosed and treated, and very importantly, how their families should be screened. The audit reported here evaluates services two years after publication of these guidelines. The results provide extremely helpful information. The current treatment of people identified with familial hypercholesterolaemia is good. However, there are clearly apparent inadequacies in the screening programme, both in terms of cascade testing and in the use of DNA testing. While it is reassuring that those with this common disorder are being well managed the results clearly show a great missed opportunity, if cascade testing is not being effectively implemented. In order to achieve this, several key issues about the effective commissioning of services for patients with familial hypercholesterolaemia needs to be addressed I am extremely grateful to all who have contributed to the work of the audit. Not only does it demonstrate how a full national audit can most effectively be carried out but it also gives us initial indications of the ways in which services need to be improved to help reduce the future burden of coronary heart disease in this group of patients. Professor Steve E. Humphries, December
5 Executive Summary Following the publication of the National Institute for Health and Clinical Excellence (NICE) guideline for familial hypercholesterolaemia (FH) 1 and the pilot audit published in 2009, we report here the findings of the national clinical audit to investigate the care received by individual patients who have FH. A 2008 survey 2 showed that ~15,000 adults and ~500 children with FH are being managed in UK lipid clinics. This audit has examined roughly 15% of adults and 30% of the children currently identified, and is likely to be a good representation of current practice. Why do this audit? FH is one of the most common monogenic inherited conditions in clinical practice. The prevalence of FH in the UK is about 1 in 500 (very similar to type1 diabetes). FH patients have an increased risk of premature coronary heart disease (CHD). Approximately 50% of men and 30% of women with FH, if untreated, will have developed clinically evident coronary heart disease by the age of 55 years 3. Effective treatment is available to prevent early onset heart disease for individuals with FH. This comprises treatment with a statin to reduce their low-density lipoprotein cholesterol (LDL-C) combined with life style changes, particularly smoking cessation. This clinical approach results in a very significant reduction in their CHD mortality risk, such that welltreated patients with FH can achieve a normal life expectancy 4. In the UK over 85% of the estimated 120,000 people who are thought to be affected remain undiagnosed 2,5. National audit based on agreed standards and evidence-based guidelines is expected to improve clinical practice, and thereby significantly reduce the mortality and morbidity associated with FH. NICE has estimated the annual cost impact of fully implementing the guideline in England to be 7.9 million in the first year of implementation, which equates to additional costs of 16,000 for a population of 100, Within three years considerable savings are estimated because of coronary events avoided and these will increase in the long-term. Ongoing treatment costs would be expected to reduce progressively as higher intensity statins (often indicated for FH) come off patent. How was the audit carried out in England, Wales, Northern Ireland and Scotland? Audit standards and indicators were developed from the NICE Clinical Guideline for the Identification and Management of Familial Hypercholesterolaemia (2008) 1. The web-based tool developed to capture the audit data worked well. Data were supplied for 2324 adult and 147 child patients, and data were duplicated for 268 of these as part of an assessment of data reliability (see Appendix 5 for details). There were very few missing or contradictory data and the validation checks and balances in place on the web-tool worked well. Feedback suggested that, overall, participating acute hospitals (sites) found the audit a positive experience, and that it demonstrated their current progress in implementing the NICE 1 National Institute for Health and Clinical Excellence (NICE) CG71: Clinical Guideline for the Management of Familial Hypercholesterolaemia (2008) Slack J. Risks of ischaemic heart-disease in familial hyperlipoproteinaemia stats. Lancet 1969;2: Neil A, Cooper J, Betteridge J, Capps N, McDowell I, Durrington P, Seed M, Humphries, SE on behalf of the Simon Broome Familial Hyperlipidaemia Register Group. Reductions in all-cause, cancer, and coronary mortality in statin-treated patients with heterozygous familial hypercholesterolaemia: a prospective registry study. European Heart Journal (2008) 29, Marks D, Thorogood M, Farrer JM, Humphries SE. Census of clinics providing specialist lipid services in the United Kingdom. J Public Health (Oxf) 2004;26:
6 guideline and identifying areas for improvements. Sites stated they would encourage others to take part in future national audits. Who should read the audit report? This report is for consultants, GPs, nurses, dieticians, commissioners and other staff who care for people with familial hypercholesterolaemia. The Key Findings from the Organisational and Clinical Audit: The clinical management in lipid clinics is of a good standard for individual patients who have been diagnosed with FH. Organisational aspects of the care pathway for FH are still being developed, but current resources are inadequate to cope with the identification of the predicted FH relatives of affected cases UK wide. This includes access to trained staff (86% of sites had no lipid specialist nurses), IT provision and pedigree drawing. There is a major lack of family cascade testing, whether carried out on the basis of lipid levels or, more effectively, by a DNA diagnosis. While there is good access to DNA diagnosis and funding for DNA testing in the devolved provinces, access and funding in England is poor. There is a shortfall in child-focused services throughout the country, with only 26% of sites offering paediatric FH services. Where such services were audited they are of a good standard. While good management of FH patients is occurring in both small and large sites, there is some evidence that small sites adhere less fully to key aspects of the guideline. This is particularly with respect to annual review, collection of detailed pedigree data and initiation of cascade testing. There are several key areas of clinical practice which appear to be sub-optimal in many sites. Trusts providing services for FH patients should urgently consider ways to improve these deficits by developing the necessary structures and funding streams, including commissioning that could improve the identification of people with FH and thereby enable treatment to prevent premature heart disease. 6
7 KEY RECOMMENDATIONS Acute trusts (England, Scotland and Northern Ireland) / Integrated Trusts (Wales) Commissioning arrangements need urgently to be reviewed for key elements of the services for FH patients, both at national and local levels. Several aspects of the care pathways for FH patients need to be implemented, including shared care arrangements between hospital and primary care and better links between with several other specialties, including paediatrics. Additional resources will be needed to cope with the care of new FH patients identified by cascade testing. Training to address the shortage of staff with key skills will be required. Systems need to be developed and implemented to carry out comprehensive cascade testing. This will require trained health professionals with the appropriate skills to follow up the families of index patients, improved IT resources, including an FH patient database, and pedigree drawing. The establishment of multidisciplinary teams should be encouraged since they appear to achieve better implementation of the guidelines and management of FH patients. Resources are needed for DNA diagnosis and Clinical Genetics input. Based on published data, cascade testing alone will find less than 50% of the predicted 100,000 unidentified FH patients in the UK, and other methods for finding FH probands will need to be explored. National Organisations: Given that FH families are geographically dispersed, cascade testing may be facilitated by a specifically funded UK FH Register to which all FH cases would be notified It is recommended that a second UK wide audit of services should be commissioned to start in
8 Introduction Aims of the national audit Familial hypercholesterolaemia (FH) is a common inherited disorder of lipid metabolism causing high levels of low-density lipoprotein cholesterol (LDL-C), which leads to early coronary heart disease (CHD). Roughly half of men with FH, if untreated, will have developed clinically evident CHD by the age of 55 years, and roughly one third of women by 60 years 3. A significant reduction in the mortality and morbidity associated with the disease can be achieved through changes in lifestyle and the use of statins to lower cholesterol, but currently the vast majority of affected individuals in the UK remain undiagnosed (probably 85% of the predicted 120,000 cases) 2.Testing the families of known cases of FH (cascade testing) can identify those with FH, and data obtained from a large ongoing project in Holland and a DH pilot project in the UK indicates this is cost-effective. It is widely recognised that cascade testing will only identify less than 50% of these predicted cases 1,2 and several other approaches for identifying new FH probands have been proposed 1,6,7 To date, the cost effectiveness of these approaches has not been evaluated. In August 2008 the National Institute for Health and Clinical Excellence (NICE) published evidence-based recommendations for the diagnosis and management of FH (CG71, 2008) 1. Using these recommendations as the standard, we present here the results of the national audit of the management of FH. The audit initiated and carried out by the Royal College of Physicians between January 2010 and December 2010, and was funded by the British Heart Foundation, Heart UK, Cardiac Network Co-ordinating Group, Wales and Royal College of Physicians, London. The audit was carried out on a national basis in England, Wales, Scotland and Northern Ireland. The considerable efforts of NHS hospital health professionals and clinical audit staff have enabled a maximum return rate of 83% of the invited acute trusts (sites) in England, Northern Ireland and Integrated Trusts in Wales. In Scotland four health boards took part in the audit. Based on the audit data collected from these 122 sites, this report presents a detailed examination of the range of clinical outpatient services provided and the quality of management of FH patients across the United Kingdom. It details the current level of implementation of the standards set out in the NICE FH guideline in participating sites, and identifies several key areas where NICE-recommended standards are not being achieved and from which recommendations for service improvement can be made. The correction of these deficits could be achieved by promoting the development of the necessary structures and funding streams, which could dramatically improve the identification of people at risk of premature heart disease because of FH, and enable preventative treatment. You are encouraged to consider the key messages and recommendations in the report. Finally, thank you to everyone who helped in the design, performance and analysis of this UK National Audit of the Management of Familial Hypercholesterolaemia. 6 Gray J, Jaiyeola A, Whiting M, Modell M, Wierzbicki AS: Identifying patients with familial hypercholesterolaemia in primary care: an informatics-based approach in one primary care centre. Heart. 94(6), (2008). 7 Wald DS, Bestwick J, Wald NJ. Child-parent screening familial hypercholesterolaemia; a screening proposal based on a metaanalysis BMJ 335:
9 RESULTS Summary of results This first national audit of the management of 2324 FH adults and 147 children has shown significant needs for improvement and development of services for people with FH. Acute trusts, as providers of service, and primary care trusts in England (PCTs) / local health boards in Wales (LHBs) / NHS Boards in Scotland and The Health and Social Care Board for Northern Ireland, as Commissioners of services, are not yet working together effectively to develop an action plan to address the gaps in service provision. Patient Management For the identified cases clinical management is good. There is good documentation of family history and the majority of case notes contained pedigree information and evidence that diagnosis was made after excluding secondary causes of hypercholesterolaemia. Only 44% of the adult patients achieved the recommended target of 50% reduction in LDL-C from the untreated level. Overall, treated LDL-C was reduced from a median of 6.1mmol/l to 3.5mmol/l (mean reduction 37%, median 33%, IQR 23% - 47%). On average, sites reported 1 Consultant PA per week for lipid management of which on average 35% is spent on management of FH patients. 86% of sites had no lipid specialist nurses. This level of staffing is unlikely to be adequate if GP referral numbers increase markedly. Only 26% of sites have a specialist service for the management of young people with FH. The majority of sites had no documented policy for the diagnosis or cascade testing of FH, or an integrated care pathway or clinical management strategy for the management of FH. While many sites have shared care arrangements with General Practice, Cardiology, Obstetrics etc, most of these are informal. Provision of written advice about diet, exercise, smoking and alcohol consumption was good, although for 38% of females of reproductive age there was no documentation of discussion of contraceptive advice. 82% of adults and 88% of children have had an annual review in secondary care. Cascade and DNA testing Currently 42% of sites report having no database for FH patients. Only 12% of sites have a commissioned cascade testing service. Only 15% of sites received NHS funding for DNA testing. In individuals where DNA testing has been carried out, a mutation was detected in 62% of adults and 65% of children. When the family mutation is known the child has been offered a DNA test in 94% of cases. Small and Large Sites Half of the sites see less than 20 new adult patients and 50 follow up patients per year, while a quarter of sites see more than 50 new and 140 follow up patients per year. 9
10 While good management of FH patients is occurring in both small and large sites (small = one or less Consultant PA per week), there is some evidence that small sites adhere less fully to key aspects of the guideline with respect to annual review, collection of detailed pedigree data and initiation of cascade testing. Presentation of results The NICE Guideline recommendations audited are presented at the beginning of each section. Following this there is a summary of the results with figures reflecting the national picture. Unless otherwise stated the percentages reported are of all relevant patients, the denominator being dependent on which aspects are applicable. Throughout this report the results for the two patient groups (adults and children) are shown separately. Key differences compared to the pilot audit (June 2009) The pilot audit was based on only 14 sites and we recognised that as volunteers they may represent sites that were already active in developing FH services and we anticipated that the results from a national audit may show an overall lesser degree of implementation of the NICE guideline. Conversely, in the last year many sites may have already started to implement the guidelines and so results may show better achievements. While we do not believe it is appropriate to carry out any formal statistical comparisons between the two data sets, some trends are noteworthy: 1. Key recommendations with regard to the collection of pedigree data, annual review, the initiation of cascade testing, access to dietary and smoking cessation clinics, and availability of written patient information material were similar. A similar high number of sites still had no formal policy for the diagnosis and cascade testing of FH, or an integrated care pathway or clinical management strategy for the management of FH. 2. Only 15% of sites have access to funded DNA testing which is the same as in the pilot. 3. The 28% of adults who have had a DNA test is similar to that seen in the pilot. This is likely to reflect the ongoing DNA testing activities in Scotland, Wales and Northern Ireland. 51% of children have had a DNA test. Better implementation of NICE guideline than in the pilot phase of the audit 4. 30% of sites report that FH care is subject to regular audit, which is considerably higher than the 7% reported in the pilot audit. 5. In adults, the treated lipid levels fall short of the target 50% reduction recommended by NICE. However, 44% of the adult patients achieved the 50% target in the national audit, compared to 33% in the pilot phase. Poorer implementation of the NICE guideline than in pilot phase 6. 42% of sites compared to 14% in the pilot, report no form of paper or electronic database for FH patients. 7. Only 12% of sites have access to a formal cascade testing system, with 14% saying this is in development, compared to 21% and 29% in the pilot. 8. Only 7% of sites reported specific links to a patient or service user group (15% in pilot), with 6% (vs 21%) reporting that this is in development. Comparison between countries A separate report will be prepared for each of the devolved provinces, and here a comparative analysis is only presented for two key questions. There was significant regional variation in the level of DNA testing, with all 137 patients from Northern Ireland (NI) recorded as having had a DNA test compared with 430/2041 (21%) in England, 23/25 (66%) in Scotland and 10
11 34/111 (31%) in Wales. There was also regional variation in the extent to which cascade testing was commissioned, with this figure being 5% in England, 25% in NI, 75% in Scotland and 83% in Wales. Comparing small and large audit acute hospitals (sites) We have addressed the issue as to whether key aspects of the NICE guideline implementation are carried out equally in small and large audit sites. Following discussions with the Steering Group, it was decided to divide sites on the basis of the number of (PA) Consultant sessions and there were 62 small sites with one or less Consultant PA per week and 60 large sites with more than one. Six key questions were examined from the organisational data and eleven from the clinical data (full results from these are presented in Appendix 2). For the majority of these questions there were no statistically significant differences between the small and large sites. The main issues identified were: In 44% of small sites, FH patients were seen in the Diabetes and Endocrinology Directorate versus 20% in large sites (p = 0.005). In large sites the majority of FH patients were seen in the Chemical Pathology Directorate (70% vs 53% p = 0.057). Larger sites tended to have more input from local genetic services than small sites (64% versus 22% p = % of large sites had in-clinic access to specialist dietary advice while only 19% of small sites had this service, although overall more than 90% of both sites had access to specialist dietary advice. Significantly more large sites had a pedigree or family tree in the notes (93% versus 84% p = 0.001,) and in large sites this was presented as a family tree as opposed to being written (61% versus 46 % p = 0.001). In large sites, a smaller percentage of patients were not on any statin treatment (14.5% versus 18.2% p = 0.03). A higher percentage of patients in large sites were on any other treatment (48.5% vs 43% p = 0.01). Both pre-treatment and post treatment LDL-C levels were slightly higher in small sites (6.6 vs 6.4 mmol/l p = 0.05 and 3.8 vs 3.6 mmol/l p = respectively). However, the reduction in LDL-C levels were similar in both large and small sites with a mean reduction of 38% for large sites and 40% for small sites (p=0.557). It is noteworthy that the proportion of patients where DNA mutation testing had been performed was similar in large and small sites (27% versus 29%), as was the proportion where the mutation had been identified (62% versus 62%). In large sites, in a significantly higher proportion of patients there was evidence that the process of cascade testing had been initiated (74.5% versus 62% p = 0.001). In large sites a significantly higher proportion of patients notes showed evidence of a letter to the GP stating the diagnosis of FH (90% versus 80% p = 0.001). In large sites a significantly higher proportion of patients had had an annual review in the hospital setting compared to small sites (84% versus 79% p = 0.001). Conclusions While good management of FH patients is being delivered at both small and large sites, there is some evidence that small sites adhere less fully to key aspects of the guideline. This is particularly with respect to annual review, collection of detailed pedigree data and initiation of cascade testing 11
12 Method Standards The audit was based on the standards in the NICE Guideline 71 Identification and Management of Familial Hypercholesterolaemia published in August Objective The aim of the audit was to develop and evaluate audit tools to measure current practice in the management of FH against the recommendations identified in the NICE Guideline (NICE CG71, 2008). The audit comprised two elements: Organisational audit to explore the organisation and resources available for people with FH in clinics with expertise in lipid disorders (mostly lipid clinics). The Organisational Audit was divided into seven elements: 9. Set Up 10. Clinical Time 11. Management of FH 12. Cascade Testing 13. Trust Services 14. Patient Information 15. Service Improvement Clinical audit to review the clinical management and process of care of consecutive sample of people (adults and children) attending outpatient clinics in relation to their FH, assessing: Section 1: Diagnosis Section 2: Pedigree Section 3: Assessment Section 4: Treatment Section 5: Advice Section 6: Cascade Testing Section 7: (Annual) Review The audit required data to be collected from policy documents and patient records. Direction on where the data may be located were provided in accompanying help notes. Target population for the clinical audit The audit focused on outpatient FH services for adults and children. Governance of the audit The project was supervised by a multidisciplinary Steering Group, which included one person with FH as a patient representative. The Working Group was comprised of a eight members from the Steering Group. The Working Group and Steering Group developed indicators for the audit derived from the NICE evidence-based guideline. The project management and governance standards were in line with those employed by the Clinical Standards Department, Royal College of Physicians. 12
13 Development of Audit Indicators The audit indicators were drawn from the NICE guideline s key priorities for implementation, in particular: 16. prescribing a high intensity statin to achieve a greater than 50% reduction in LDL- C concentration 17. offering a DNA test 18. using systematic methods of cascade testing for the identification of people with FH 19. testing children by the age of 10 years, which should be carried out in a child/young person focused setting 20. giving women and girls on statins information about contraception (because of the slight risk of birth defects in babies conceived whilst taking a statin) 21. having an annual structured review. Pilot exercise The questions for the full national audit were updated based on the feedback received during the pilot phase of the study. Fourteen acute hospital sites were recruited and undertook the pilot exercise in April Data were collected for 248 patients. National audit In England, Wales and Northern Ireland 134 sites were recruited of which 118 participated. Four sites from Scotland also took part in the audit. Inclusion criteria The audit sampled adults and children with a definite or possible diagnosis of FH (as per the NICE guideline). For this audit children are considered under 16 years of age. The focus of the audit was people with FH who were accessing outpatient services for the third clinic appointment or greater. Sites were requested to select cases for clinical audit from the first 40 consecutive cases with a diagnosis of FH (ICD 10 Code E78. 0) visiting a clinic with expertise in lipid disorders for the third time or more between 1 st April 3 rd September The numbers were chosen, following statistical advice, to provide the minimum necessary to enable a meaningful analysis comparing individual sites so that local services can be benchmarked against the overall national figure. It was recognised at pilot stage that the majority of sites would not identify 40 cases. Exclusion criteria 1. Patients who have a possible or definite diagnosis of FH attending their first or second clinic appointment 2. Patients with lipid disorders other than FH. Recruitment of acute sites Acute hospital trusts (sites) were recruited via letters to their chief executive, medical director, any identified FH lead, and clinical audit or effectiveness managers. They were asked to provide details of leads and contacts. Participation Of the 142 sites invited to participate, 134 sites registered for the project. Of these, 122 site provided data for the organisational audit and 102 sites supplied clinical data on one or both groups of patients (adults and children). Three of the four sites participating in Scotland also submitted patient data. There were 2324 adults (94%) and 147 children (6%) in sample
14 adults and 3 children were duplicated as part of the inter-auditor reliability analysis (see page 16 for further details). A 2008 survey of UK lipid clinics 2 suggested that ~15,000 adults and ~500 children with FH are being managed in lipid clinics so this audit has examined roughly 15% of adults and 30% of the children currently identified. It is therefore likely give a good representation of current practice. Cases entered Number of adult and paediatric cases entered by country is as follows: Country Adults cases Paediatric cases England Northern Ireland Wales Scotland 35 0 Data collection tool The Organisational Audit required entry of hospital management data to the web-based data collection tool. It required the auditor to have access to the information and an understanding of how each element of the FH service is organised. The Clinical Audit comprised a clinical case note audit of consecutive clinic attendances of patients with FH, retrospectively identified between 1 st April 2010 and 3 rd September Sites were encouraged to develop a mechanism for identifying all applicable FH cases attending outpatient clinics. This could be done by: allocating a doctor or nurse to contact all clinics to identify patients and log these for subsequent data collection from case notes shortly after the clinic visit OR, using a log book to identify patients and entering the data at a later stage It may be that the Patient Administration System (PAS) or local FH database can be used to cross check the capture of all FH cases. The audit tools were designed to measure the implementation of the NICE Clinical Guideline. Support and Information for participating sites As soon as sites were recruited and had provided their contact details they were kept up to date with monthly newsletters or by . The National Audit of Management of Familial Hypercholesteroaemia (FH Audit) website ( was regularly updated and included a frequently asked question sheet. Support information was provided for auditors, giving definitions and guidance on how to answer each audit question for the patient groups. Sites were advised to gather data initially and to enter this onto the web-tool once data collection from various sources was complete. All sites were fully prepared for the audit by the second week of March 2010 in readiness to begin data collection. Data collection continued into September Information governance Data were collected via a secure website (as above). Individual patient consent is not required where unidentifiable patient data is used for audit purposes. No patient identifiable information was collected. Sites were asked not to put any information that may identify the patient in the free text comments boxes. Data entry to the web tool To improve quality of data entry, the web-tool had built in validation checks. Web-tool help notes were provided and a help desk was available to sites during data collection by and 14
15 phone. Sites were asked to refer to the web-tool user notes to aid data entry and the support information to clarify any of their answers. Each site was provided with their own unique password and site code. Many data entry items required a simple YES or NO response but sometimes other options were possible, i.e. not relevant. Inter-auditor reliability Sites were asked to re-audit their first 5 cases, using a different auditor, and returning to the clinical notes again as the source of audit data. Fifty nine sites reported 268 re-audited cases. Reliability (agreement between auditors) is not the same as validity (suitability or accuracy of measure). However establishing good agreement between auditors is an important part of the process of validation. The levels of agreement were generally encouraging. There were some questions with poorer results where comments made by participants shed light on possible ambiguity, and here detail can be added to the help notes or on the data collection tool in the future. For a more detailed summary of the reliability analyses see Appendix 5. Analysis of data Data were held securely and analysed at the Royal College of Physicians Clinical Standards Department. The software used was Stata version 11.1 Audit Evaluation Objective The national audit successfully developed audit tools to measure the current practice in the management of FH against the recommendations identified in the NICE Guideline (CG71, 2008). The NICE guideline was also used in Scotland although it is not formally recognised. Target population The audit was successful in its aim to audit the management of adults and children with FH. Data were supplied for 2471 patients, and data were duplicated for 268 of these as part of an assessment of inter-rater reliability (see Appendix 5 for details). Development of audit indicators In general, the audit tool enabled the level of implementation of the NICE guideline to be measured. There is need for the audit tool to be more concise in some areas for the re-audit. Lipoprotein measurements at diagnosis There was evidently some difficulty for a minority of the patients in finding the correct set of lipoprotein measurements used at diagnosis. This can be seen by comparing the years recorded in the data. In future rounds of audit, this should be used to validate the data as it is typed into the web-tool. Pedigree Section 2 of the clinical audit proforma relates to the FH patient s pedigree. NICE advises that 3 generations should be captured in the pedigree. This can be interpreted in one of two ways: capturing first, second and third generation or first-degree, second-degree and thirddegree relatives. The two sets of definitions are different (see glossary, Appendix 2). Despite rigorous scrutiny by the Working and Steering Groups this only came to light during the pilot audit in This section was rectified in the full national audit. Annual review The audit asked whether the patient had a structured annual review since the initial diagnosis. Since patients were only included in the audit if they were attending the clinic over the data collection period, those who had been discharged from care by the clinic would not be included in the audit 15
16 Paediatrics It is of relevance that the NICE guidelines only partially address some important differences between adult and paediatric services. For example in paediatrics there is a need for smoking prevention programs rather than smoking cessation programs. Inclusion criteria Overall, sites found it straightforward to select eligible patients. 20 sites were able to enter 40 cases or greater. Audited patients were only those attending their third clinic appointment or greater, so as to obtain information about key activities that occur later in the care pathway, such as cascade testing, annual review etc. Recruitment of sites The aim of the audit was to audit all acute trusts in the country that see FH patients; 142 sites were invited to participate and 134 sites registered to undertake the audit Participation Of the 134 sites who registered to participate, 122 completed the organisational audit and 102 submitted one or more clinical cases. Four sites from Scotland completed the organisational audit and three submitted clinical cases. Data collection tool The validation checks and balances in place on the web-tool worked well. The data collection tool requires minor enhancements to improve data validation. Inter-rater reliability Analysis of how different data collectors agreed on the information required for the clinical audit showed that most of the questions produce reliable answers. Some others provided us with feedback which has informed improvements in the help notes and the web-tool. Support and information Feedback suggests that overall sites were happy with the written information (help notes and newsletters) and helpdesk support provided. Evaluation of audit process Sites were encouraged to provide written/verbal feedback at all stages of the audit process. After the data collection period participating sites were asked to complete a survey detailing their experience of completing the audit process. A summary of the results can be found in appendix 5. Conclusion Overall the National Audit of the Management of Familial Hypercholesterolaemia was considered a success, with a high participation rate and meeting the objectives of the project. The audit has provided useful data on the level of implementation of the NICE guideline and has provided a good national picture of FH services nationally. 16
17 ORGANISATIONAL AND CLINICAL AUDIT FULL NATIONAL RESULTS 17
18 PART 1: ORGANISATIONAL AUDIT Section 1: Set up NICE GUIDELINE RECOMMENDATION Healthcare professionals should offer all children and young people diagnosed with, or being investigated for, a diagnosis of FH a referral to a specialist with expertise in FH in children and young people. This should be in an appropriate child/young personfocused setting that meets the standards within the National service framework for children, young people and maternity services (available from FH patients are managed in a spectrum of directorates, with the majority in Chemical Pathology, Diabetes, Cardiology or Internal Medicine. Although the majority of sites have a lead clinician responsible for FH care, less than 40% have someone with operational managerial responsibility for FH service and 96% do not run a dedicated FH clinic. There are many small sites, with half seeing less than 20 new adult patients and 50 follow up patients per year, with a quarter of sites seeing more than 50 new and 140 follow up patients per year. Currently only 7% of sites have a designated cascade testing clinic, with another 19% in development of this service. Only 26% of sites have a specialist service for the management of young people with FH. While many sites have shared care arrangements with General practice, Cardiology, Obstetrics, etc, most of these are informal. Currently only ~30% of sites report a partial paper or electronic database for FH patients. Type of hospital 1.1 What type of hospitals are in your trust? Sites were asked to tick all that apply. Teaching 55 (45.1%) District General 78 (63.9%) Provision of FH services 1.2 Does your trust provide outpatient services for the clinical management of: a. Adults with FH? 115 (94.3%) b. Children/young people (under 16s) with FH? 72 (59.0%) Of those sites who provide outpatient services for adults with FH (i.e. responded positively to 1.2 a) 18
19 1.3 Who provides the outpatient services for the clinical management of adults with heterozygous FH? Sites were asked to tick one answer option Provided by trust 113 (98.3%) Provided by a visiting service from another trust 0 (0%) By referring to another service or centre 2 (1.7%) 1.4 Who provides the outpatient services for the clinical management of adults with homozygous FH? Sites were asked to tick one answer option Provided by trust 39 (33.9%) Provided by a visiting service from another trust 0 (0%) By referring to another service or centre 76 (66.1%) Of those sites who provide outpatient services for children with FH (i.e. responded positively to 1.2 b) 1.5 Who provides the outpatient services for the clinical management of children with FH? Sites were asked to tick one answer option Provided by trust 64 (88.9%) Provided by a visiting service from another trust 1 (1.4%) By referring to another service or centre 7 (9.7%) Directorate / Care Group that FH is under 1.6 What Directorate/ Care Group is FH under? Tick all that apply Diabetes and Endocrinology 39 (32.0%) Cardiology / Cardiovascular 18 (14.8%) Chemical Pathology 75 (61.5%) General Medicine / General Internal 21 (17.2%) Specialist Medicine 3 (2.5%) Paediatrics 20 (16.4%) Other 4 (3.3%) The number of Directorates / Care Groups that FH was reported as coming under were One 81 (66.4%) Two 26 (21.3%) Three 13 (10.7%) Four 2 (1.6%) Managerial responsibility 1.7 Does your trust have someone with operational managerial responsibility for FH services? Yes 44 (36.1%) 19
20 1.8 Does your trust have a lead clinician responsible for FH care? Yes 86 (70.5%) Out-patient clinics 1.9 How many of the following outpatient clinics are there per month: Dedicated FH clinics Adults morning clinics (am) (96.7%) 1 1 (0.8%) 4 3 (2.5%) Adults afternoon clinics (pm) (97.5%) 1 2 (1.6%) 4 1 (0.8%) Paediatric morning clinics (am) (93.4%) (0.8%) 1 5 (4.1%) 2 2 (1.6%) Paediatric afternoon clinics (pm) (98.4%) 1 2 (1.6%) General lipid clinics Adults morning clinics (am) 0 44 (36.1%) (0.8&) 1 17 (13.9%) 2 8 (6.6%) 3 4 (3.3%) 4 31 (25.4%) 5 4 (3.3%) 6 3 (2.5%) 8 8 (6.6%) 15 1 (0.8&) 16 1 (0.8&) 20
21 Adults afternoon clinics (pm) 0 75 (61.5%) 1 15 (12.3%) 2 6 (4.9%) 3 3 (2.5%) 4 15 (12.3%) 5 4 (3.3%) 8 2 (1.6%) 10 2 (1.6%) Paediatric morning clinics (am) (95.9%) 1 3 (2.5%) 4 2 (1.6%) Paediatric afternoon clinics (pm) (98.4%) 1 1 (0.8%) 2 1 (0.8%) Other medical clinics (where FH patients are seen in relation to FH) Adults morning clinics (am) (84.4%) 1 3 (2.5%) 2 4 (3.3%) 4 9 (7.4%) 8 3 (2.5%) Adults afternoon clinics (pm) (90.2%) 1 5 (4.1%) 2 2 (1.6%) 4 2 (1.6%) 8 2 (1.6%) 10 1 (0.8&) Paediatric morning clinics (am) (90.2%) 1 6 (4.9%) 3 1 (0.8%) 4 3 (2.5%) 12 1 (0.8%) 15 1 (0.8&) 21
22 Paediatric afternoon clinics (pm) (94.3%) 1 3 (2.5%) 2 1 (0.8%) 4 1 (0.8%) 8 2 (1.6%) Designated cascade testing clinic 1.10 Does your trust have a designated clinic to test for FH by cascade testing? Yes 9 (7.4%) In development 23 (18.8%) No 90 (73.8%) Outpatient clinics 1.11 Please estimate how many patients with FH were seen in outpatient clinics in the last year (this should include definite, probable/possible): New adult patients Median 20 Inter quartile range 7-50 Min - Max Total 4276 New paediatric patients Median 0 Inter quartile range 0-4 Min - Max 0-38 Total 320 Adult patients in follow up Median 50 Inter quartile range Min - Max Total Paediatric patients in follow up Median 0 Inter quartile range 0-5 Min - Max 0-80 Total
23 Specialist services for management of young people 1.12 Does your trust have specialist services for the management of young people with FH? Yes 32 (26.2%) Sites answered 1.13 a & b if they answered yes to a. do your specialist services have access to paediatric phlebotomy? Yes 30 (93.8%) 1.13 b. Do you have family clinics? Yes 16 (50.0%) Shared care arrangements Formal arrangements are considered to be where there are written/ documented and agreed share care arrangements, with informal arrangements being where arrangements are in place however there is no written formal documentation to support this Do you have shared care arrangements in place with: a. General practice Yes - formal 7 (5.7%) Yes - informal 61 (50.0%) No 54 (44.3%) b. Cardiology Yes - formal 6 (4.9%) Yes - informal 53 (43.4%) No 63 (51.6%) c. Obstetrics Yes - formal 1 (0.8%) Yes - informal 17 (13.9%) No 104 (85.3%) d. Paediatrics Yes - formal 15 (12.3%) Yes - informal 44 (36.1%) No 63 (51.6%) e. LDL Apheresis services Yes - formal 11 (9.0%) Yes - informal 15 (12.3%) No 96 (78.7%) 23
24 Database of patients with FH 1.15 Do you have a paper database of patients with FH? Yes - complete 9 (7.4%) Yes - partially complete 33 (27.0%) No 80 (65.6%) 1.16 Do you have an electronic database of patients with FH? Yes - complete 8 (6.6%) Yes - partially complete 40 (32.8%) No 74 (60.7%) Section 2: Clinical time On average, sites reported 1 Consultant PA per week for lipid management of which on average 35% is spent on management of FH patients. 86% of sites had no lipid specialist nurses. Although all sites report some clinician and nurse time for FH patient management, it appears that this is unlikely to be adequate if GP referral numbers increase markedly. Clinical time There are 10 Consultant Programme Activities (PAs) per week. Sites were asked to indicate how many Consultant s PAs are devoted to specialist lipid management and how many Lipid Specialist Nurses they had in whole time equivalent (WTE) - for the purposes of the audit, one WTE is 37.5 hours. 2.1 In your trust, how much clinical time is devoted to specialist lipid management/fh by your employed staff: a. How many consultants programmed activities (PAs) are devoted to specialist lipid management? 0 16 (13.1%) (0.8%) 1 45 (36.9%) (0.8%) 2 28 (23.0%) (0.8%) 3 15 (12.3%) 4 7 (5.7%) 5 3 (2.5%) 6 2 (1.6%) 7 1 (0.8%) 8 2 (1.6%) Median (IQR) 1 (1-2.5) 24
25 b. On average, what proportion (%) of this is estimated to be spent on the management of FH? <10% 18 (17.0%) 11-20% 31 (29.3%) 21-40% 30 (28.3%) 41-60% 22 (20.8%) 61-80% 4 (3.8%) % 1 (0.9%) c. How many Lipid specialist nurses are there (WTE)? (86.1%) (0.8%) (0.8%) (0.8%) (0.8%) (0.8%) (0.8%) (0.8%) (1.6%) 1 5 (4.1%) (0.8%) 3 1 (0.8%) 4 1 (0.8%) Median (IQR) 0 (0-0) d. On average, what proportion (%) of this is estimated to be spent on the management of FH? <10% 2 (11.8%) 11-20% 3 (17.7%) 21-40% 3 (17.7%) 41-60% 3 (17.7%) 61-80% 2 (11.8%) % 4 (23.5%) 25
26 Section 3: Management of FH 80% of trusts formally classify patients according to the Simon Broome criteria and 67% offer an annual review, while 31% of sites routinely discharge FH patients once lipid levels are optimised. More than 60% of sites do not have a written policy of protocol for the diagnosis or cascade testing of FH nor an integrated care pathway for FH patients. Patient classification 3.1 Does your trust formally classify patients according to the Simon Broome criteria? Yes 97 (79.5%) No 23 (18.9%) Not applicable 2 (1.6%) Annual review 3.2 Does your trust routinely offer FH patients an annual review? Yes 82 (67.2%) Routine discharge 3.3 Does your trust routinely discharge FH patients once lipid levels are optimised? Yes 38 (31.2%) Written policy/protocol for clinical management of FH 3.4 a. Is there a written policy/protocol for the clinical management of FH? Yes 14 (11.5%) In development 33 (27.1%) No 75 (61.5%) Sites were asked to answer b-e if they answered yes to 3.4a b. Has this been formally approved by your trust? Yes 7 (50.0%) In progress 3 (21.4%) No 4 (28.6%) c. Does the policy include diagnostic criteria for FH? Yes 14 (100%) d. Does the policy include advice on cascade testing? Yes 11 (78.6%) e. Does the policy include advice on annual review? 26
27 Yes 11 (78.6%) Integrated care pathway/clinical management strategy 3.5 Is there an integrated care pathway/clinical management strategy for the management of FH? Yes 11 (9.0%) In development 34 (27.9%) No 77 (63.1%) Section 4: Cascade Testing NICE GUIDELINE RECOMMENDATION: Healthcare professionals should offer all people with FH a referral to a specialist with expertise in FH for confirmation of diagnosis and initiation of cascade testing. Cascade testing is as yet considerably under developed and only 12% have access to a formal system, with 14% saying this is in development. Input from local genetic services are only reported in 10 centres. Less than 10% have any form of dedicated IT software to help manage this service. 4.1 Is a service for cascade testing commissioned/funded for your trust/organisation? Yes 14 (11.5% 7 ) In development 17 (13.9%) No 91 (74.6%) See breakdown by country in appendix Is there access to a family cascade testing system for FH in your trust? Yes 26 (21.3%) In development 17 (13.9%) No 79 (64.8%) Sites answered 4.3 and 4.4 if answered yes to By country this figure was 5% in England, 25% in NI, 75% in Scotland and 83% in Wales) 4.3 If yes, how is this provided? Provided by trust 23 (88.5%) Provided by a visiting service from another trust 1 (3.9%) By referring to another service or centre 2 (7.7%) 27
28 4.4 If yes, who is responsible for the clinical governance of the cascade testing for families? Trust 16 (61.5%) Regional Clinical Genetics Service 8 (30.8%) Other 2 (7.7%) "No one" 1 "Blood forms to patient" 1 Sites answered 4.5 if answered Provided by trust to If provided by trust, does this include: a. Dedicated staff? Yes 11 (47.8%) In development 4 (17.4%) No 8 (34.8%) b. Formal input from the local Genetic services? Yes 10 (43.5%) In development 2 (8.7%) No 11 (47.8%) 4.6 Do the staff who are looking after individuals and families with FH routinely have access to: a. dedicated IT software Yes 10 (8.2%) In development 14 (10.7%) No 99 (81.1%) b. pedigree drawing software? Yes 6 (4.9%) In development 16 (13.1%) No 100 (82.0%) 28
29 Section 5: Trust services NICE GUIDELINE RECOMMENDATION Cascade testing using a combination of DNA testing and LDL-C concentration measurement is recommended to identify affected relatives of those index individuals with a clinical diagnosis of FH. While 97% of sites have access to an accredited laboratory for lipid measurements and the 82% for smoking cessation and 95% for dietary support, only 15% of sites have access to funded DNA testing. 5.1 Is DNA mutation testing for FH commissioned/funded for patients in your trust/organisation? Yes 18 (14.8%) In development 15 (12.3%) No 89 (73.0%) See breakdown by country in appendix Does your trust have arrangements for DNA mutation testing for FH patients attending your clinical service? Yes - funded 15 (12.3%) Yes - not funded 22 (18.0%) Available only in special cases 33 (27.1%) No 52 (42.6%) 5.3 Does your trust have a laboratory that is currently accredited (CPA) for testing lipid measurements? Yes 118 (96.7%) 5.4 Does your trust have routine access to HDL measurements? Yes 122 (100%) 5.5 Is there a smoking cessation support service that FH patients can be referred to? Yes 104 (82.3%) Smoking cessation support services included /PCT/LHB or NHS Stop Smoking Services. 5.6 Is there access to specialist dietary advice? Yes - in clinic 32 (26.2%) Yes - separate from clinic 84 (68.9%) No 6 (4.9%) 29
30 Section 6: Patient information NICE GUIDELINE RECOMMENDATIONS During the assessment and communication of familial risk, people should receive clear and appropriate educational information about FH, the process of family testing, DNA testing and the measurement of LDL-C concentration. A healthcare professional with expertise in FH should provide information to people with FH on their specific level of risk of coronary heart disease, its implications for them and their families, lifestyle advice and treatment options. The sites appear to have a wide range of information leaflets to help FH patients, but 29% report no leaflets available. Patient information 6.1 Which, if any, of the following information leaflets do you provide to FH patients/carers? a. British Heart Foundation leaflet(s) 36 (29.5%) b. Heart UK leaflet(s) 59 (48.4%) c. NICE information for the public 19 (15.6%) d. Trust leaflet 25 (20.5%) e. Other 34 (27.9%) 6.2 If yes, does the information provided cover the following subject areas? a. Diet 85 (97.7%) b. Exercise 79 (90.8%) c. Smoking 78 (89.7%) d. Alcohol 70 (80.5%) e. FH as a condition 70 (80.5%) f. Inheritance 65 (74.7%) g. Role of DNA testing 48 (55.2%) h. Treatment options 69 (79.3%) i. Treatment for children 49 (56.3%) j. Monitoring 56 (64.4%) k. DNA testing 42 (48.3%) l. Cascade testing 45 (51.7%) 30
31 Section 7: Service improvement Currently only 7% of sites report specific links to a patient or service user group, with 6% reporting that this is in development. 30% of sites report that FH care is subject to regular audit. Patient/service-user group 7.1 Does the FH service have specific links to a patient/service-user group? Yes 9 (7.4%) In development 7 (5.7%) No 106 (86.9%) Sites answered question 7.2 if they answered yes to Is the patient/service user group involved in planning and delivery of FH services? Yes 7 (77.8%) Regular audit 7.3 Is FH care delivered by the service subject to regular audit? Yes 36 (29.5%) Regular audit is considered be at least annually. This could be process and/or outcome audit. 31
32 PART 2: CLINICAL AUDIT Sites were asked to select cases for clinical audit from the first 40 consecutive cases with a diagnosis of FH (ICD 10 Code E78. 0) visiting a clinic with expertise in lipid disorders for the third time or more between 1 st April 3 rd September Data were submitted on 2471 patients and duplicates were entered for 268 of these. 102 sites collected these data, ranging from 1 to 103 patients, (median 21, inter-quartile range 8-28). Section 0: General information The audit information reflects the wide spectrum of FH patient care facilities throughout the UK. The age spectrum is very similar to that published by Neil et al in BMJ, and confirms the considerable underrepresentation of young adults (25-45years). The median age of the men is 49 years and for women is 55 years. Children are under-represented, with a mean age of 12.6 years. The survey has identified slightly more women than men (with the opposite trend in children) in keeping with the adult data seen in the pilot and the DH Audit project. Possible reasons for this include a survivor effect and since these were people attending their third clinic visit, women are more likely to re-attend than men. Of the 90% with ethnicity recorded, the distribution seen for adults is similar to that of the UK general population, with 92% being White, 5% from the Indian subcontinent and around 1% being African or Caribbean origin. A similar distribution was seen in the children. 0.1 Is this patient treated as a paediatric or adult case? Users could select either paediatric or adult Adult 2324 (94.1%) Paediatric 147 (5.9%) Auditor speciality/grade 0.2 Auditor Specialty: Adult Paediatric Chemical Pathology 1441 (62.0%) 31 (21.1%) Clinical Pharmacology 8 (0.3%) 0 (0%) Diabetology 110 (4.4%) 1 (0.7%) Endocrinology 92 (4.0%) 0 (0%) Paediatrics 0 (0%) 8 (5.4%) Specialist Lipid 549 (23.6%) 57 (38.8%) Clinical Effectiveness/Audit 25 (1.1%) 0 (0%) Paediatric Metabolic Disease 0 (0%) 24 (16.3%) Other 99 (4.3%) 26 (17.7%) 0.2a Auditor Grade Adult Paediatric 32
33 Consultant 1388 (60.4%) 75 (51.0%) Specialist Registrar 188 (8.2%) 4 (2.7%) Specialist Nurse 387 (16.8%) 34 (23.1%) Nurse 25 (1.1%) 2 (1.4%) Other 336 (14.5%) 32 (21.8%) Out-patient clinic type 0.3 In what clinic was the patient seen? FH clinic 119 (5.1%) 4 (2.7%) Lipid clinic 2063 (88.8%) 103 (70.1%) General medical clinic 24 (1.0%) 0 (0%) Paediatric clinic 0 (0%) 8 (5.4%) Other 118 (5.1%) 32 (21.8%) Patient demographics 0.4 Date of clinic Median 14 Jun Jun 2010 Lower quartile 11 May May 2010 Upper Quartile 19 Jul Jul 2010 Patients age at clinic Median Lower Quartile - Upper Quartile Min - Max
34 34
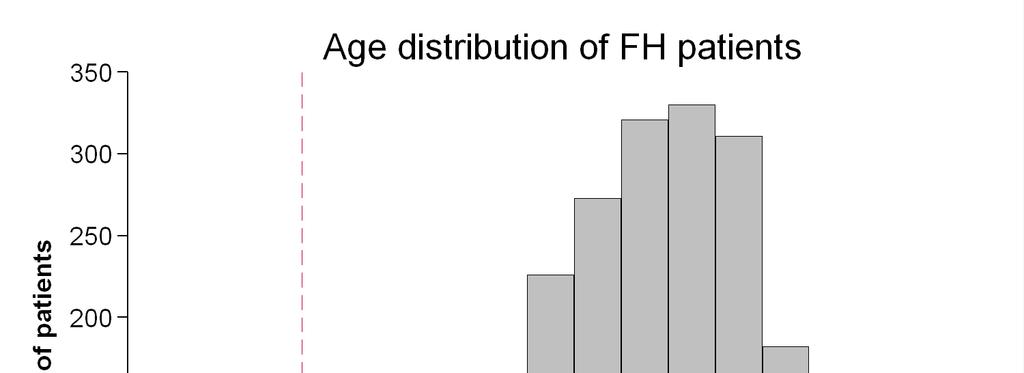
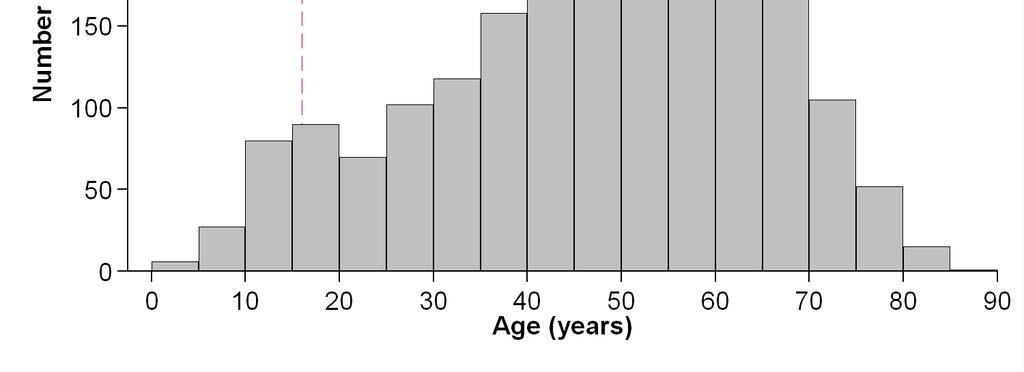
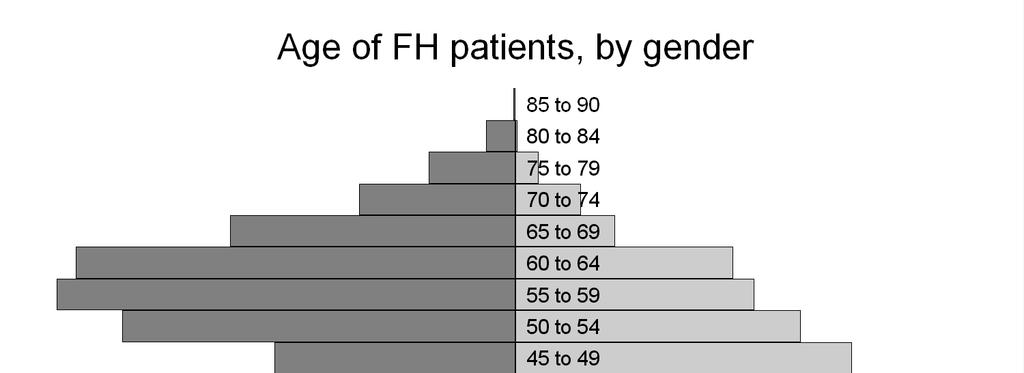
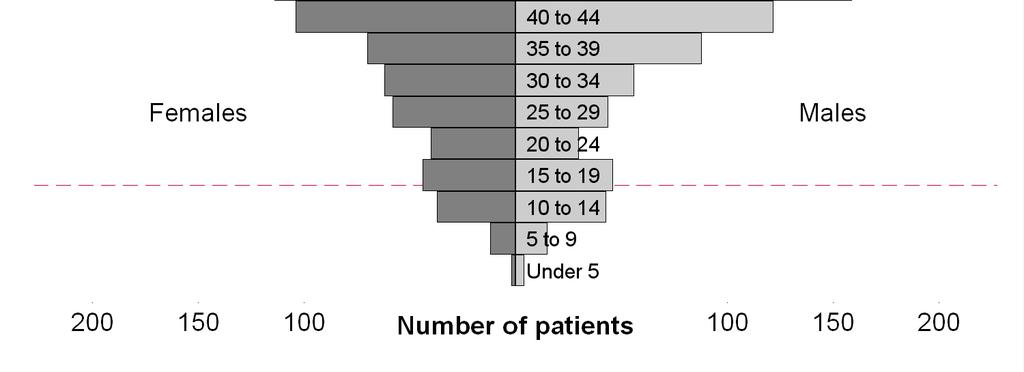
35 0.6 Patient s gender: Male 967 (41.6%) 83 (56.5%) Female 1357 (58.4%) 64 (43.5%) 0.7 Ethnic group White British 1756 (75.6%) 85 (57.8%) Irish 83 (3.6%) 7 (4.8%) Any other White background 81 (3.5%) 11 (7.5%) Asian of Asian British Indian 63 (2.7%) 6 (4.1%) Pakistani 22 (1.0%) 2 (1.4%) Bangladeshi 10 (0.4%) 1 (0.7%) Any other Asian background 25 (1.1%) 1 (0.7%) Black or Black British Carribean 11 (0.5%) 0 (0%) African 8 (0.3%) 0 (0%) Any other Black background 2 (0.1%) 0 (0%) Mixed White and Black Caribbean 2 (0.1%) 0 (0%) White and Black African 2 (0.1%) 0 (0%) White and Asian 4 (0.2%) 2 (1.4%) Any other mixed background 7 (0.3%) 0 (0%) Chinese / Other ethic group Chinese 12 (0.5%) 0 (0%) Any other ethnic group 13 (0.6%) 1 (0.7%) Not recorded 223 (9.6%) 31 (21.1%) 35
36 Section 1: Diagnosis NICE GUIDELINE RECOMMENDATIONS Healthcare professionals should exclude secondary causes of hypercholesterolaemia before a diagnosis of FH is considered. A diagnosis of FH should be made using the Simon Broome criteria, which include a combination of family history, clinical signs (specifically tendon xanthomata), cholesterol concentration and DNA testing. A family history of premature coronary heart disease should always be assessed in a person being considered for a diagnosis of FH. Healthcare professionals should offer people with a clinical diagnosis of FH a DNA test to increase the certainty of their diagnosis and to aid diagnosis among their relatives. The proportion of possible to definite FH adult patients of roughly 1.6 :1 is similar to that reported in the pilot and DH audit. It may be that the more difficult to manage DFH patients are being kept in the clinics for management. In children 54% had a diagnosis of Definite FH. The diagnosis of 49 adults with definite Homozygous FH appears unlikely given the expected prevalence of 1 per million, and inspection of the untreated and treated lipid levels of these reported patients indicates that at most five may fulfil the clinical criteria for true homozygous FH. The 27% of adults who had a DNA test is similar to that reported in the pilot audit. There was significant regional variation in the level of DNA testing, with all 137 patients from Northern Ireland recorded as having had one, compared with 430/2041 (21%) in England, 23/25 (66%) in Scotland and 34/111 (31%) in Wales. The figure in children was higher at 51%. The 0.9% of patients who had refused a DNA test is encouraging. Diagnosis was made using a non-fasting sample in only 2% of adults and there was good evidence that secondary causes of hypercholesterolaemia were excluded before a diagnosis of FH was considered (all greater than 90%). The range of lipid traits measured is appropriate and as expected for FH patients, although 28% did not have a full lipid profile in the notes on which the diagnosis was made. 46% of the individuals had evidence in the notes that a baseline ECG was considered. Patient diagnosis 1.1 What is the patient s diagnosis? (Sites were asked to tick one option) Definite Homozygous FH 49 (2.1%) 1 (0.7%) Definite heterozygous FH 834 (35.9%) 79 (53.7%) Probable/Possible FH 1352 (58.2%) 67 (45.6%) FH not clearly stated 89 (3.8%) 0 (0%) 36
37 1.1a Year of diagnosis (FH possible or definite)? Paediatric cases only Median NA 2007 Lower Quartile - Upper Quartile NA Min - Max NA Not recorded NA 11 History of CHD 1.2 Is there evidence in the notes that there is a history of CHD in the patient? Yes 559 (24.1%) 6 (4.1%) No 408 (17.6%) 87 (59.2%) Recorded as none 1357 (58.4%) 54 (36.7%) Coronary heart disease includes MI, CABG, PTCA, coronary angiography and angina. Premature Coronary Heart Disease (CHD) = <55 male, <65 female in relatives Blood relatives 1.3 Is there evidence in the notes that there are any blood relatives? Yes 2246 (96.6%) 144 (98.0%) No 52 (2.2%) 3 (2.0%) Recorded as none 26 (1.1%) 0 (0%) Premature coronary heart disease 1.4 Is there a record of premature coronary heart disease in the patient s blood relatives? Yes 1665 (71.6%) 115 (78.2%) No 268 (11.5%) 25 (17.0%) Recorded as none 391 (16.8%) 7 (4.8%) DNA testing 1.5 Is there evidence that the patient accepted or refused a DNA test for FH? Patient had DNA test - evidence of consent Patient had DNA test - no evidence of consent 508 (21.9%) 50 (34.0%) 116 (5.0%) 26 (17.7%) 37
38 Patient refused DNA test 21 (0.9%) 1 (0.7%) Patient not offered DNA test 1377 (59.3%) 53 (36.1%) Not recorded 302 (13.0%) 17 (11.6%) Diagnosis 1.6 Is there evidence that the diagnosis included assessment of the following clinical signs: a. corneal arcus? Yes 842 (36.2%) 21 (14.3%) No 400 (17.2%) 49 (33.3%) Recorded as none 1082 (46.6%) 77 (52.4%) b. tendon xanthoma? Yes 841 (36.2%) 36 (24.5%) No 286 (12.3%) 26 (17.7%) Recorded as none 1197 (51.5%) 85 (57.8%) Lipid profile 1.7 Did the lipid profile on which the diagnosis was made use a fasting sample or non fasting sample? Fasting 1853 (79.7%) 70 (47.6%) Not Fasting 51 (2.2%) 15 (10.2%) Not recorded 420 (18.1%) 62 (42.2%) Secondary causes of FH 1.8 Is there evidence that the following secondary causes of hypercholesterolaemia were excluded before a diagnosis of FH was considered? a. Diabetes 2152 (92.6%) 63 (42.9%) b. Renal failure 2147 (92.4%) 86 (58.5%) c. Hypothyroidism 2136 (91.9%) 85 (57.8%) d. Cholestasis 2106 (90.6%) 84 (57.1%) Diabetes: fasting Blood glucose or HBA1C. Renal Failure: U&E Hypothyroidism: TSH Lipoprotein measurements Sites were asked to record the lipid results of the blood test that confirmed the diagnosis of FH before treatment. 38
39 1.9 What were the lipid and lipoprotein measurements used to make the diagnosis? Pre-treatment levels in adults Year Median Lower Quartile - Upper Quartile Min - Max Fasting Yes 1662 (91.6%) 58 (76.3%) Cholesterol Median Lower Quartile - Upper Quartile Min - Max HDL Median Lower Quartile - Upper Quartile Min - Max Triglyceride Median Lower Quartile - Upper Quartile Min - Max LDL Median Lower Quartile - Upper Quartile Min - Max Not all lipid and lipoprotein measurements available in notes: Adult Paediatric The Simon Broome diagnostic cut-off for LDL-C is 4.7mmol/l in an adult and 4.0 in a child, and these data show 9% of adults and 13% of children are below these values. 39



40 While this may represent incorrect use of the criteria by the diagnosing clinicians, it may also be that untreated lipid levels are not available in the notes and the earliest recorded data may already be when the patient has started treatment Is there evidence in the notes that an ECG was carried out? 1.10 Yes 1060 (45.7%) NA 40


41 One adult patient with recorded triglyceride of 35.1 mmol/l at diagnosis has been excluded from these graphs for presentation purposes. 41
42 Section 2: Pedigree NICE GUIDELINE RECOMMENDATION When considering a diagnosis of FH, healthcare professionals with expertise in FH should use standardised pedigree terminology to document, when possible, at least a three generation pedigree. This should include relatives age of onset of coronary heart disease, lipid concentrations and smoking history. For deceased relatives, the age and cause of death, and smoking history should be documented. If possible, the index individual should verify this information with other family members. 91% of the adult notes and 83% of the paediatric notes contained a pedigree or family tree, with 56% being written or drawn by hand. 100% have information about the first generation relatives, but this number fell to 62% (vs 67%) in adult and 83% in paediatric notes in the second and less than 15 in the third generation relatives. Less than 50% of pedigrees included information about the relative s age, age of onset of CHD, smoking history etc. There is room for improvement in the way these data are collected. Pedigree 2.1 Is there a pedigree/family tree in the notes? Adult Paediatric Yes 2109 (90.8%) 122 (83.0%) Answer if answered yes to How is the pedigree/family tree recorded? (sites can tick more than one option) a. Drawn using software 59 (2.8%) 9 (7.4%) b. Drawn by hand 1188 (56.3%) 84 (68.9%) c. Written 1342 (56.3%) 67 (54.9%) 2. 3 Does the pedigree include the following family members: a. First-degree relatives Yes No Adult Paediatric Yes 2107 (99.9%) 122 (100%) b. Second-degree relatives Yes No Adult Paediatric Yes 1302 (61.7%) 101 (82.8%) c. Third-degree relatives Yes No Some Adult Paediatric 42
43 Yes 148 (7.0%) NA No 1653 (78.5%) NA Some 305 (14.5%) NA Sites who answered yes to 2.2 (a) (b) or (c) were asked to answer question 2.3 Data items recorded in pedigree 2.4 Are the following data items recorded: a. Relatives age Adult Paediatric Yes - for all 791 (37.5%) 27 (22.1%) Yes - for some 1128 (53.5%) 65 (53.3%) No 190 (9.0%) 30 (24.6%) b. Age of onset of coronary heart disease (if present)? Adult Paediatric Yes - for all 861 (40.8%) 32 (26.2%) Yes - for some 790 (37.5%) 74 (60.7%) No 458 (21.7%) 16 (13.1%) c. Information about tendon xanthoma? Adult Paediatric Yes - for all 35 (1.7%) 8 (6.6%) Yes - for some 178 (8.4%) 15 (12.3%) No 1896 (89.9%) 99 (81.2%) d. Information about total cholesterol? Adult Paediatric Yes - for all 180 (8.5%) 15 (12.3%) Yes - for some 1066 (50.6%) 51 (41.8%) No 863 (40.9%) 56 (45.9%) e. Smoking history of blood relatives with CHD? Adult Paediatric Yes - for all 147 (7.0%) 10 (8.2%) Yes - for some 298 (14.1%) 24 (19.7%) No 1664 (78.9%) 88 (72.1%) f. Cause of death recorded for deceased blood relatives Adult Paediatric Yes - for all 871 (41.3%) 30 (24.6%) Yes - for some 792 (37.6%) 57 (46.7%) No 446 (21.2%) 35 (28.7%) 43
44 Section 3: Assessment 73% of adults and 82% of children were reviewed by the consultant at their most recent clinic appointment. Height and weight was recorded in more than 90% of both adult and child notes. 3.1 What was the date of the patient s last (most recent) outpatient clinic appointment? Median 14 Jun Jun 2010 Lower quartile 11 May May 2010 Upper Quartile 19 Jul Jul Who reviewed the patient at their last (most recent) out-patient clinic appointment? Consultant 1692 (72.8%) 121 (82.3%) Specialist Registrar 272 (11.7%) 17 (11.6%) Specialist Nurse 112 (4.8%) 1 (0.7%) Other 248 (10.7%) 8 (5.4%) Height and weight 3.3 At the first clinic appointment was the patient s weight recorded? Yes 2178 (93.7%) 139 (94.6%) 3.4 At the first clinic appointment was the patient s height recorded? Adult Paediatric Yes 1884 (81.1%) 129 (87.8%) 3.5 At the last (most recent) clinic appointment was the patient s weight recorded? Yes 2095 (90.2%) 136 (92.5%) 44
45 Section 4: Treatment NICE GUIDELINE RECOMMENDATION Healthcare professionals should consider prescribing a high-intenstity statin to achieve a recommended reduction in LDL-C concentration of greater than 50% from baseline. In the adults, the treated LDL-C levels show a significant reduction from the untreated levels, down to 3.5mmol/l from a median of 6.1mmol/l (the mean reduction for individual patients was 37%, median 33%, IQR 23% - 47%). This does fall short of the target 50% reduction recommended by NICE, although since this is only the third clinic visit for some subjects some improvement may still be achieved. Overall, 720/1621 (44%) of the patients achieved the 50% target. The most common statin treatments are Atorvastatin and Rosuvastatin (35% each) and the reasons for not taking statins appear to be clearly stated. 48% of patients are also on Ezetimibe, with only 6% also on fibrates. Before commencement of treatment, muscle enzymes and transaminases were recorded as measured in only than 65% and 88% of cases (but we consider that levels may have been measured earlier in some of the remainder). In children mean treated LDL-C fell from 5.4mmol/l to 4.4mmol/l (mean reduction was 20%, median 18%, IQR 2% - 37%). 28% of the children were on Atorvastatin, 11% on Pravastatin and 15% on Simvastatin. 7 children were taking a resin and 3 ezetimibe. (Note there is no NICE target for lipid lowering in children). Lipoprotein results 4.1 What are the most recent lipid and lipoprotein results? Complete/latest lipid and lipoprotein measurements not available in notes: Year Median Lower Quartile - Upper Quartile Min - Max Fasting Yes 2045 (91.2%) 64 (72.7%) Cholesterol Median Lower Quartile - Upper Quartile Min - Max
46 HDL Median Lower Quartile - Upper Quartile Min - Max Trig Median Lower Quartile - Upper Quartile Min - Max LDL Median Lower Quartile - Upper Quartile Min - Max Not all lipid and lipoprotein measurements available in notes: Adult Paediatric Yes 132 (5.7%) 65 (44.2%) 46
47 47

48 One adult patient with recorded triglyceride of 35.1 mmol/l at diagnosis has been excluded from these graphs for presentation purposes. 48
 30 1 (0.1%) 0 (0%) 40 327 (42.8%) 3 (7.1%) 60 14 (1.8%) 0 (0%) 80 240 (31.4%) 1 (2.4%) Fluvastatin Adult Paediatric Yes 25 (1.1%) 0 (0%) Dose 20 10 (40.0%) NA 40 9 (36.0%) NA 80 6 (24.")
49 Lipid lowering drug therapy 4.2 What was the patients treatment at the time of the results? Atorvastatin Adult Paediatric Yes 764 (32.9%) 42 (28.6%) Dose (10.1%) 29 (69.1%) (13.7%) 9 (21.4%) 30 1 (0.1%) 0 (0%) (42.8%) 3 (7.1%) (1.8%) 0 (0%) (31.4%) 1 (2.4%) Fluvastatin Adult Paediatric Yes 25 (1.1%) 0 (0%) Dose (40.0%) NA 40 9 (36.0%) NA 80 6 (24.0%) NA Pravastatin Adult Paediatric Yes 63 (2.7%) 17 (11.6%) Dose (25.4%) 13 (76.5%) (33.3%) 4 (23.5) (41.3%) 0 (0%) Rosuvastatin 49
50 Adult Paediatric Yes 795 (34.2%) 0 (0%) Dose (13.8%) NA 8 1 (0.1%) NA (25.3%) NA 15 6 (0.8%) NA (29.9%) NA 25 0 (0.1%) NA (1.3%) NA (28.7%) NA Simvastatin Adult Paediatric Yes 355 (15.3%) 22 (15.0%) Dose (5.6%) 16 (72.7%) 15 0 (0%) 1 (4.6%) (14.9%) 5 (22.7%) 30 2 (0.6%) 0 (0%) (67.6%) 0 (0%) 50 1 (0.3%) 0 (0%) 60 8 (2.3%) 0 (0%) (8.7%) 0 (0%) Patient not receiving statin Adult Paediatric Yes 319 (13.7%) 65 (44.2%) b. (if applicable) Please indicate the reason(s) that this patient is not receiving statin. Sites were able to select more than one answer option. Patient intolerant to statin 159 (6.8%) 2 (1.4%) Patient/parent/carer declined 45 (1.9%) 12 (8.2%) Patient is planning to become or is pregnant/breastfeeding 39 (1.7%) NA Child under 10 years NA 0 (0%) Child 10 and over but low risk NA 11 (7.5%) Other 92 (4.0%) 43 (29.3%) c. Is the patient receiving any other treatment? Adult Paediatric Yes 1148 (49.4%) 13 (8.8%) 50
51 Sites only answered 4.2d-k if answer to 4.2c is yes d. Resin Cholestyramine Adult Paediatric Yes 26 (2.5%) 6 (46.2%) Dose 4 12 (46.2%) 3 (50.0%) 5 1 (3.9%) 0 (0%) 8 3 (11.5%) 2 (33.3%) 12 5 (19.2%) 1 (16.7%) 16 4 (15.4%) 0 (0%) 24 1 (3.9%) 0 (0%) Colesevelam Adult Paediatric Yes 64 (5.6%) 1 (7.7%) Dose 1 8 (12.5%) 0 (0%) 2 22 (34.4%) 0 (0%) 3 10 (15.6%) 1 (100%) 4 22 (34.4%) 0 (0%) 5 1 (1.6%) 0 (0%) 6 1 (1.6%) 0 (0%) e. Ezetimibe Adult Paediatric Yes 929 (80.9%) 3 (23.1%) Date started Median 28 Dec Apr 2004 Lower quartile 01 Nov Nov 2003 Upper quartile 23 Apr Sep 2010 f. Fenofibrate Adult Paediatric Yes 107 (9.3%) 1 (7.7%) Dose (49.5%) 0 (0%) (0.9%) 0 (0%) (0.9%) 0 (0%) (10.3%) 0 (0%) (38.3%) 1 (100%) g. Bezafibrate 51
52 Yes 6 (0.5%) 0 (0%) Dose (16.7%) NA (83.3%) NA h. Fish oil /Ω fatty acids Yes 95 (8.3%) 0 (0%) i. Nicotinic acid or derivative Yes 47 (4.1%) 1 (7.7%) j. Lipid apheresis (including Lp(a) apheresis) Yes 14 (1.2%) 1 (7.7%) k. Other Yes 147 (12.8%) 3 (23.1%) 4.3 Is there evidence that the following were measured before initiation of statin treatment: a. Muscle enzyme 1297 (64.7%) 63 (76.8%) b. Trasaminases 1766 (88.1%) 67 (81.7%) 4.4 Was this repeated within 3 months of starting statin treatment? (Paediatric only) Yes NA 38 (57.6%) 52
53 Section 5: Advice NICE GUIDELINE RECOMMENDATION People with FH should be given advice on diet, physical activity, weight management, smoking and alcohol consumption (see NICE guideline for full recommendations) When lipid-modifying drug therapy is first considered for women and girls, the risks for future pregnancy and the fetus while taking lipid-modifying drug therapy should be discussed. This discussion should be revisited at least annually. Healthcare professionals should give women and girls with FH specific information tailored to their needs and should offer a choice of effective contraceptive methods. The written advice to FH patients appears in the majority of patients to contain information about diet, exercise, smoking and alcohol consumption, with smoking status recorded in 96% of notes. Since 61% of the female patients were postmenopausal, many of the notes do not document discussion of contraceptive issues while on statins. Life-style advice 5.1 Is there written evidence that the patient/carer was given the following life-style advice? a. Diet 2000 (86.1%) 138 (93.9%) b. Exercise 1654 (71.2%) 112 (76.2%) c. Smoking 1659 (71.4%) 63 (42.9%) d. Alcohol 1541 (66.3%) 26 (17.7%) Smoking status 5.2 a. Is the smoking status of the patient recorded? Adult Paediatric Yes 2239 (96.3%) 48 (32.7%) b. If yes, please select the status: Adult Paediatric Smoker 334 (14.9%) 2 (4.2%) Ex smoker (quit for 6 months) 509 (22.7%) 0 (0%) Non smoker 1396 (62.4%) 46 (95.8%) Smoking cessation advice/referral 53
54 c. Was the patient given advice about or offered a referral to an intensive support service/smoking cessation? Offered referral 128 (38.2%) 0 (0%) Given written advice 93 (27.8%) 0 (0%) No referral or advice 113 (33.8%) 2 (100%) Contraception Question 5.3 applies to females of reproduction age who have received, or are under consideration for receiving, lipid modifying drug therapy. Lipid-modifying therapy should only be started after a discussion with the patient about the risks for future pregnancy and the foetus. 5.3 Was the need for contraception whilst taking statins discussed and documented? Yes 332 (24.5%) 15 (23.4%) No 203 (15.0%) 15 (23.4%) Patient not of reproductive age 822 (60.6%) 34 (53.1%) Section 6: Cascade Testing NICE GUIDELINE RECOMMENDATION Cascade testing using a combination of DNA testing and LDL-C concentration measurement is recommended to identify affected relatives of those index individuals with a clinical diagnosis of FH. This should include at least the first- and second- and, when possible, third-degree biological relatives. In individuals where DNA testing has been carried out a mutation was detected in 62% of adults and 65% of children; this suggests that majority of tests requested are in DFH patients. When the family mutation is known the child has been offered a DNA test in 94% of cases. The notes document that the need for cascade testing has been discussed in 84% of adult cases The process of cascade testing has been initiated in 72% of adults and 54% of paediatric cases. 54
55 Mutation testing 6.1 a. Is there evidence that DNA mutation testing has been performed? Adult Paediatric Yes 614 (26.4%) 76 (51.7%) b. If yes, was the mutation identified? Adult Paediatric Yes 379 (61.7%) 46 (64.5%) No 113 (18.4%) 13 (17.1%) Result not yet reported 122 (19.9%) 14 (18.4%) Cascade testing 6.2 Has the need for cascade testing (testing of relatives cholesterol) been discussed with the patient? (Adult patients only) Yes 1945 (83.9%) NA Answer 6.3 if answered yes to If the family mutation is known (yes to 6.1b) has the child been offered a DNA test? (Paediatric patients only) Yes NA 45 (93.8%) 6.3 Has the process of cascade testing been initiated? Adult Paediatric Yes 1412 (72.4%) 80 (54.4%) Contact with GP 6.4 a. Has a letter been written to the index case s GP stating the diagnosis of FH has been made? Yes 2015 (86.7%) 136 (92.5%) b. Does the letter state that at-risk relatives should be referred for testing? Yes 1331 (66.1%) 60 (44.1%) 55
56 Section 7: (Annual) Review NICE GUIDELINE RECOMMENDATIONS All people with FH should be offered a regular structured review that is carried out at least annually. A baseline electrocardiogram (ECG) should be considered for adults with FH. Structured review should include assessment of any symptoms of coronary heart disease and smoking status, a fasting lipid profile, and discussion about concordance with medication, possible side effects of treatment the patient may be experiencing, and any changes in lifestyle or lipid-modifying drug therapy that may be required to achieve the recommended LDL-C concentration. 82% of adults and 88% of children have had an annual review in secondary care, with less than 1% in primary care. In general, the notes indicate good achievement of the NICE targets with regard to questions of change in CVD status, side effects of drugs, and fertility and lifestyle issues and progress with cascade testing being addressed in the annual review. Structure annual review 7.1 a. Has the patient had a review carried out at least annually since the initial diagnosis? Yes - in a hospital setting 1905 (82.0%) 129 (87.8%) Yes - in primary care 32 (1.4%) 0 (0%) No - patient offered and declined 17 (0.7%) 3 (2.0%) No - not offered 95 (4.1%) 2 (1.4%) Not applicable 275 (11.8%) 13 (8.8%) b. If undertaken in a hospital setting, please give the dates of the last annual review 7.2 If the review was undertaken in a hospital setting, is there evidence in the notes that the annual review covered the following issues: a. Response to drugs? Adult Paediatric Yes 1806 (94.8%) 83 (64.3%) No 28 (1.5%) 1 (0.8%) Not applicable 71 (3.7%) 45 (34.9%) 56
57 b. Side effects? Adult Paediatric Yes 1610 (84.5%) 79 (61.2%) No 181 (9.5%) 4 (3.1%) Not applicable 114 (6.0%) 46 (35.7%) c. CVD status? Adult Paediatric Yes 1296 (68.0%) 48 (37.2%) No 609 (32.0%) 81 (62.8%) Not applicable 0 (0%) 0 (0%) d. Fertility issues? Adult Paediatric Yes 185 (16.6%) 10 (18.2%) No 164 (14.7%) 12 (21.8%) Not applicable 768 (68.8%) 33 (60.0%) e. Lifestyle? Adult Paediatric Yes 1375 (72.2%) 101 (78.3%) No 530 (27.8%) 28 (21.7%) Not applicable 0 (0%) 0 (0%) f. ECG? Adult Paediatric Yes 299 (15.7%) 3 (2.3%) No 1031 (54.1%) 51 (39.5%) Not applicable 575 (30.2%) 75 (58.1%) g. Progress with cascade screening? 7.2g Yes 886 (46.5%) 38 (29.5%) No 1019 (53.5%) 91 (70.5%) Not applicable 0 (0%) 0 (0%) 57
58 Appendices 58
59 Appendix 1: The Familial Hypercholesterolaemia Audit Steering Group The following individuals are members of the Steering Group. Those marked with also form the Working Group. Professor Steve Humphries Kristina Pedersen Dr Jonathan Potter Joseph Besford Rhona Buckingham Dr Chris Hendricks Claire Neuwirth Dr Mary Seed Michael Roughton Derek Lowe Katharine Young Jane Ingham Professor Roger Boyle Dr Cyril Chapman Dr Philip Adams Dawn Davies Leonard Levy Professor Andrew Neil Dr Ian McDowell Judy O Sullivan Dr Tim Wang Dr Devaki Nair Dr David Wald FH Audit Project Director / Professor of Cardiovascular Genetics at University College London FH Audit Project Manager, RCP Director of the Clinical Effectiveness and Evaluation Unit, RCP FH Audit Project Coordinator, RCP Clinical Effectiveness and Evaluation Unit Manager, RCP Representative from the Royal College of Paediatrics and Child Health. Consultant in Clinical Inherited Metabolic Disorders, Birmingham Children's Lipid Specialist Nurse at MRC Clinical Sciences Centre Imperial College Honorary Consultant Physician at Charing Cross, Imperial College Healthcare and recently member of the GDG for NICE FH guidelines Medical Statistician, Royal College of Physicians Medical Statistician, Royal College of Physicians Clinical Governance Manager, Royal Berkshire NHS Foundation Trust Director of Clinical Standards, RCP National Director for Heart Disease & Stroke / Vascular Programme at Department of Health Consultant in Clinical Genetics at Birmingham Women s Consultant Cardiologist at Royal Victoria Infirmary Newcastle upon Tyne s. Patient Representative on Nice Guideline and representative for Heart UK Vascular Programme, Department of Health Professor of Clinical Epidemiology, University of Oxford and Honorary Consultant Physician at the Churchill, Oxford Cardiac Networks Coordinating Group, Wales Operations Manager Heart Helpline at British Heart Foundation Consultant in Clinical Biochemistry at Royal Surrey County NHS Foundation Trust, Guildford and Frimley Park NHS Foundation Trust Consultant Chemical Pathologist and Lipidologist at Royal Free, Heart UK representative Consultant Cardiologist and Senior Lecturer, Barts and the London School of Medicine and British Cardiovascular Society, Specialist Society Representative. 59
60 Useful addresses / information British Heart Foundation Heart UK Heart UK Helpline hours: Tues & Thurs 10am to 4pm National Institute for Health and Clinical Excellence Royal College of Paediatrics and Child Health UK WHO Growth Charts 60
61 Appendix 2: Glossary (Adapted from NICE CG71) Adults with FH Cascade testing Children/young people Child-focused setting Family history First-degree relative Heterozygous FH High-intensity statin Homozygous FH Index individual (synonymous with proband ) Interquartile range (IQR) Lipid measurements/ concentrations/levels Median For the purposes of this guideline, adults includes all persons with familial hypercholesterolaemia (FH; heterozygous or homozygous) who are 16 years and older. Cascade testing is a mechanism for identifying people at risk of a genetic condition by a process of family tracing. For FH the test employed is measurement of low-density lipoprotein cholesterol (LDL-C) in the blood, and/or a DNA test if a disease-causing mutation has been identified in the index individual/proband (see below). For the purposes of this audit children are considered under 16 years of age. Child-focused refers to valuing the child s view and validating their voice in making decisions impacting their lives. A child-focused facility or space is one designed from the viewpoint of the service recipients. The structure and relationships within the family that relates information about diseases in family members. A person s biological parents, full brothers and sisters, and children. High LDL-C concentration in the blood caused by an inherited mutation from one parent only. People with FH are at increased risk of cardiovascular disease. Statins are classified as high intensity if they produce greater LDL-C reductions than simvastatin 40 mg (for example, simvastatin 80 mg and appropriate doses of atorvastatin and rosuvastatin). Very high LDL-C concentration in the blood caused by an inherited mutation from both parents. When a person inherits exactly the same affected gene from both parents this is called truly homozygous FH. When the mutations in the LDL receptor gene (or equivalent) are different, this state is called compound heterozygous. In general, the overall effect in both states is similar, in that LDL-C concentrations are very high. Both groups of patients have the same clinical pattern and high risk of cardiovascular disease. For clinical purposes, both homozygous FH and compound heterozygous FH can be regarded as behaving in a similar manner. Therefore, for the purposes of this audit the term homozygous FH is used to also encompass compound heterozygous FH. The original patient who is the starting point for follow-up of other members of a family when investigating for possible causative genetic factors of the presenting condition. The middle half of data, chosen so that one quarter of patients / sites are below it and one quarter above it. It provides an indication of how diverse clinical practice or case mix is. These terms refer to the measurement of total cholesterol (TC), triglycerides (TGs), high-density lipoprotein cholesterol (HDL-C), and LDL-C. LDL-C is not usually measured directly but calculated from the TC, TGs and HDL-C, most accurately by using a fasting sample. Such tests are usually done in a clinical biochemistry laboratory. When data are arranged from lowest value to highest, the median is in the middle. It is an average which is not unduly influenced by very high or very low values which may include some element of error. 61
62 Pedigree Premature coronary heart disease Proband Reliability Case Second-degree relative Simon Broome register Specialist Specialist centre Specialist services for young people Tendon xanthomata Third-degree relative A method of characterising the relatives of an index individual/case and their family relationship as well as problems or illnesses within the family. This information, often represented graphically as a family tree, facilitates analysis of inheritance patterns. Study of a trait or disease begins with the affected person (the index individual). The pedigree is drawn as the relatives are described. One begins with the siblings of the index individual and proceeds to the parents; relatives of the parents, including brothers, sisters, nephews, nieces, grandparents, and so on. At least three generations are usually included. Illnesses, hospitalisations, causes of death, miscarriages, abortions, congenital anomalies, and any other unusual features are recorded. For the purpose of this guideline, this refers to a coronary event that has occurred (1) before 55 years of age in a male index individual or 65 years of age in a female index individual, (2) before 60 years of age in a first-degree relative, or (3) before 50 years of age in a second-degree relative. The affected (index) individual through whom a family with a genetic disorder is ascertained. A reliability case is a duplicate entry of an existing case, entered by a different person. It is used to assess how robust the data are and how the questions have been interpreted. A person s biological grandparent, grandchild, uncle, aunt, niece, nephew, half sister or half brother. A computerised research register of people with FH, based in Oxford. Research from this voluntary register has led to several publications describing the natural history of FH in the UK. The Simon Broome criteria for diagnosis were based on a study of this group of people with FH. One who has expertise in a particular field of medicine by virtue of additional training and experience. For this audit, we use specialist to refer to a healthcare professional with an expertise in FH. The definition of a specialist centre is not rigid and is based on a combination of patient treatment services, numbers and ages of people attending there, the presence of a multi-disciplinary team (which may include, for example, physicians, lipidologists, specialist nurses and dietitians), the ability to manage the more unusual manifestations of the condition and the additional functions such as research, education and standard setting. Care is supervised by expert healthcare professionals but shared with local hospitals and primary care teams. Although details of the model may vary between patients and areas, the key is that specialist supervision oversees local provision with the patient seen at diagnosis for initial assessment and then at least annually for review. Specialist services for young people provide an area of care that is family focussed. A clinically detectable nodularity and/or thickening of the tendons caused by infiltration with lipid-laden histiocytes (macrophages in connective tissue). A distinctive feature of FH that most frequently affects the Achilles tendons but can also involve tendons on the back of the hands, elbows and knees. A person s biological great grandparent, great grandchild, great aunt, great uncle, first cousin, grand nephew or grand niece. 62
63 Appendix 3: Organisational data 4.1 Is a service for cascade testing commissioned/funded for your trust/organisation England NI Scotland Wales Total Yes 5 5% 1 25% 3 75% 5 83% 14 11% In development 16 15% 1 25% 0 0% 0 0% 17 14% No 87 81% 2 50% 1 25% 1 17% 91 75% 5.1 Is DNA mutation testing for FH commissioned/funded for patients in your trust/organisation? England NI Scotland Wales Total Yes 7 6% 4 100% 4 100% 3 50% 18 15% In development 15 14% 0 0% 0 0% 0 0% 15 12% No 86 80% 0 0% 0 0% 3 50% 89 73% 63
64 Appendix 4: Comparison of Large vs. Small sites There were 62 sites with 1 or less Consultant s programmed activities devoted to specialist lipid management (designated small sites), and 60 with sites with more than 1 PA (designated large sites) Organisational Audit 1.6 What Directorate/ Care Group is FH under? Tick all that apply Small site Large site p value Diabetes and Endocrinology 27 (43.6) 12 (20.0) Cardiology / Cardiovascular 12 (19.4) 6 (10.0) Chemical Pathology 33 (53.2) 42 (70.0) General Medicine / General Internal 10 (16.1) 11 (18.3) Specialist Medicine 2 (3.2) 1 (1.7) Paediatrics 9 (14.5) 11 (18.3) Other 2 (3.2) 2 (3.3) The number of Directorates / Care Groups that FH was reported as coming under were Small site Large site p value One 40 (64.5) 41 (68.3) Two 13 (21.0) 13 (21.7) Three 7 (11.3) 6 (10.0) Four 2 (3.2) 0 (0) 1.7 Does your trust have someone with operational managerial responsibility for FH services? Small site Large site p value Yes 23 (37.1) 21 (35.0) Do you have an electronic database of patients with FH? Small site Large site p value Yes - complete 4 (6.5) 6 (6.7) Yes - partially complete 17 (27.4) 23 (38.3) No 41 (66.1) 33 (55.0) Small site Large site p value Yes - complete 4 (6.5) 6 (6.7) Yes - partially complete 17 (27.4) 23 (38.3) No 41 (66.1) 33 (55.0) 4.5 If provided by trust, does this include: a. Dedicated staff? Small site Large site p value Yes 4 (44.4) 4 (28.6) In development 1 (11.1) 3 (21.4) No 4 (44.4) 7 (50.0)
65 b. Formal input from the local Genetic services? Small site Large site p value Yes 2 (22.2) 9 (64.3) In development 2 (22.2) 0 (0) No 5 (55.6) 5 (35.7) 5.5 Is there a smoking cessation support service that FH patients can be referred to? Small site Large site p value Yes 52 (83.9) 52 (86.7) Is there access to specialist dietary advice? Small site Large site p value Yes - in clinic 12 (19.4) 20 (33.3) Yes - separate from clinic 49 (79.0) 35 (58.3) No 1 (1.6) 5 (8.3) Clinical Audit 1.1 What is the patient s diagnosis? Small site Large site p value Definite Homozygous FH 9 (1.3) 41 (2.3) Definite heterozygous FH 262 (28.4) 651 (36.4) Probable/Possible FH 391 (57.3) 1028 (57.5) FH not clearly stated 20 (2.9) 69 (3.9) 1.5 Is there evidence that the patient accepted or refused a DNA test for FH? Small site Large site p value Patient had DNA test - evidence of consent Patient had DNA test - no evidence of consent 154 (22.6) 404 (22.6) (6.9) 95 (5.3) Patient refused DNA test 7 (1.0) 15 (0.8) Patient not offerered DNA test 395 (57.9) 1035 (57.9) Not recorded 79 (11.6) 240 (13.4) Small site Large site p value Patient had DNA test - evidence of consent Patient had DNA test - no evidence of consent 154 (22.6) 404 (22.6) (6.9) 95 (5.3) Patient refused DNA test 7 (1.0) 15 (0.8) Patient not offerered DNA test 395 (57.9) 1035 (57.9) Not recorded 79 (11.6) 240 (13.4) 2.1 Is there a pedigree/family tree in the notes? Small site Large site p value Yes 573 (84.0) 1658 (92.7) <
66 Small site Large site p value Yes 573 (84.0) 1658 (92.7) < How is the pedigree/family tree recorded? Small site Large site p value a. Drawn using software 1 (0.2) 67 (4.0) <0.001 b. Drawn by hand 261 (45.6) 1011 (61.0) <0.001 c. Written 378 (66.0) 1031 (62.2) What was the patients treatment at the time of the results? Small site Large site p value Atorvastatin 198 (29.0) 608 (34.0) Fluvastatin 6 (0.9) 19 (1.1) Pravastatin 16 (2.4) 64 (3.6) Rosuvastatin 239 (35.0) 556 (31.2) Simvastatin 99 (14.5) 278 (15.5) Patient not on statin 124 (18.2) 260 (14.5) Any other treatment 293 (43.0) 868 (48.5) Ezetimibe 242 (82.6) 690 (76.5) a. Is there evidence that DNA mutation testing has been performed? Small site Large site p value Yes 200 (29.3) 490 (27.4) b. If yes, was the mutation identified? Small site Large site p value Yes 123 (61.5) 305 (62.2) No 35 (17.5) 91 (18.6) Result not yet reported 42 (21.0) 94 (19.2) 6.2 Has the need for cascade testing (testing of relatives cholesterol) been discussed with the patient? (Adult patients only) Small site Large site p value Yes 503 (82.5) 1442 (84.4) If the family mutation is known (yes to 6.1b) has the child been offered a DNA test? (Paediatric patients only) Small site Large site p value Yes 20 (95.2) 25 (92.6) Has the process of cascade testing been initiated? Small site Large site p value Yes 358 (62.3) 1134 (74.5) < a. Has a letter been written to the index case s GP stating the diagnosis of FH has been made? Small site Large site p value 66
67 Yes 548 (80.4) 1603 (89.6) <0.001 b. Does the letter state that at-risk relatives should be referred for testing? Small site Large site p value Yes 338 (61.7) 1053 (65.7) a. Has the patient had a review carried out at least annually since the initial diagnosis? Small site Large site p value Yes - in a hospital setting 541 (79.3) 1493 (83.5) <0.001 Yes - in primary care 10 (1.5) 22 (1.2) No - patient offered and declined 5 (0.7) 15 (0.8) No - not offered 14 (2.1) 83 (4.6) Not applicable 112 (16.4) 176 (9.8) 67
68 Appendix 5: Reliability analyses Reliability (the agreement between auditors) is not the same as validity (the accuracy of measurements). However, establishing good agreement between auditors is an important part of the process of validation, as valid data by definition will have to reliable. For categorical data the kappa statistic was used to measure agreement. Kappa values of 0.41 to 0.60 are said to indicate moderate agreement, values of 0.61 to 0.80 indicate good agreement, whilst of 0.81 and above indicate excellent agreement. For each categorical question, two kappas are given. The first is the kappa when both auditors entered a response for a question, and the second is when only one auditor entered a response. The first kappa assesses agreement on the responses, whilst the second is an amalgamation of two separate components: whether the auditors agreed that the relevant information existed, and whether they agreed when they found the information. The advantage of kappa is that it measures the agreement seen in excess to that agreement which would be expected by chance. A kappa score of 1 means perfect agreement, whilst a kappa of 0 means agreement was no better than chance. In practice, any kappa value below 0.5 indicates inadequate agreement. We would want to see kappa values above 0.6 and preferably over 0.8.The kappa statistic measures agreement but cannot indicate the nature of disagreement between auditors. For continuous data, such as dates and years, descriptions of the percentage of cases agreeing to within certain thresholds are given. Summary Fifty nine sites reported 268 re-audited cases. The median number of reliability cases reported by these 59 sites was 5, with a range of 1 to 10. All 268 pairs of auditors agreed as to whether the cases they were entering was classed as an adult or paediatric patient. However, there were only 3 paediatric patients and therefore any questions relating solely to this group are not included in the reliability analysis due to the very small numbers involved. Median (IQR) kappa scores across all categorical questions were 0.69 (0.59, 0.89) when both auditors entered data (figure A1), and 0.70 (0.58, 0.88) when taking into account whether they thought the information was available (figure A2). Overall this is a good level of agreement, with little difference between the two kappa scores (p=0.47 and figure A3). This suggest there was no more of less agreement on the actual answer than on whether the information was available for that patient. The table below gives the median kappa scores for each section of the audit. Scores are consistent across each section, with none showing markedly poorer agreement than any other. Scores are highest in the sections detailing patient demographics and assessment, but these are also the sections with smallest number of questions. Section Number of categorical questions Kappa score for disagreements on answers Kappa score for disagreements on answers and eligibility

69 The question with the weakest reliability (kappa when both users entered data<0.5) were: 1.3 Is there evidence in the notes that there are any blood relatives? 1.9 Fasting 2.1 Is there a pedigree/family tree in the notes? 4.2d Colesevelam dose 4.3b Is there evidence that the following were measured before initiation of statin treatment: trasaminases? 5.2c Was the patient given advice about or offered a referral to an intensive support service/smoking cessation? 7.2f If the review was undertaken in a hospital setting, is there evidence in the notes that the annual review covered the following issues: ECG? Figure A1 Figure A2 69
National Clinical Audit of the Management of Familial Hypercholesterolaemia 2009: Pilot
 National Clinical Audit of the Management of Familial Hypercholesterolaemia 2009: Pilot FULL REPORT June 2009 Funded by: Department of Health, England Cardiac Network Co-ordinating Group, Wales Conducted
National Clinical Audit of the Management of Familial Hypercholesterolaemia 2009: Pilot FULL REPORT June 2009 Funded by: Department of Health, England Cardiac Network Co-ordinating Group, Wales Conducted
FACTS AND FIGURES 120, ,000 - The estimated number of people with FH in the UK
 HEART UK FH Primary Care Audit Programme There is an enormous opportunity to prevent the occurrence of coronary heart disease (CHD) by exploiting the information contained within GP electronic patient
HEART UK FH Primary Care Audit Programme There is an enormous opportunity to prevent the occurrence of coronary heart disease (CHD) by exploiting the information contained within GP electronic patient
Familial Hypercholesterolaemia Quality Improvement Tool Instruction Guide
 Familial Hypercholesterolaemia Quality Improvement Tool Instruction Guide PRIMIS development of this tool was part supported by independent funding from Amgen. Prepared by PRIMIS January 2017 The University
Familial Hypercholesterolaemia Quality Improvement Tool Instruction Guide PRIMIS development of this tool was part supported by independent funding from Amgen. Prepared by PRIMIS January 2017 The University
The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance
 Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Familial hypercholesterolaemia (FH) paediatric register. Annual progress report January December In association with:
 paediatric register. Annual progress report January December In association with:") Familial hypercholesterolaemia (FH) paediatric register Annual progress report January December 2014 In association with: Contents Ethics approvals 3 Overview of the FH paediatric register 3 Oversight
Familial hypercholesterolaemia (FH) paediatric register Annual progress report January December 2014 In association with: Contents Ethics approvals 3 Overview of the FH paediatric register 3 Oversight
Specialised Services Service Specification: Inherited Bleeding Disorders
 Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Newborn bloodspot screening
 Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Physiotherapy outpatient services survey 2012
 14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
European Reference Networks. Guidance on the recognition of Healthcare Providers and UK Oversight of Applications
 European Reference Networks Guidance on the recognition of Healthcare Providers and UK Oversight of Applications NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients
European Reference Networks Guidance on the recognition of Healthcare Providers and UK Oversight of Applications NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
UK Inflammatory Bowel Disease Audit 3rd Round
 UK Inflammatory Bowel Disease Audit 3rd Round Report of the results for the national organisational audit of paediatric inflammatory bowel disease services in the UK Prepared by the The UK IBD Audit Steering
UK Inflammatory Bowel Disease Audit 3rd Round Report of the results for the national organisational audit of paediatric inflammatory bowel disease services in the UK Prepared by the The UK IBD Audit Steering
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
European network of paediatric research (EnprEMA)
") 17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
#NeuroDis
 Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Final. Andrew McMylor / Dr Nicola Jones
 NHS Standard Contract - Service Specification Service Specification Service Final 24hour Ambulatory Blood Pressure Monitoring (24hrABPM) Commissioner Lead Lead Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
NHS Standard Contract - Service Specification Service Specification Service Final 24hour Ambulatory Blood Pressure Monitoring (24hrABPM) Commissioner Lead Lead Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Specialised Services Service Specification: CP57b. Genetic Testing for Inherited Cardiac Conditions
 Specialised Services Service Specification: CP57b Genetic Testing for Inherited Cardiac Conditions Document Author: Specialised Planner Executive Lead: Director of Finance Approved by: Management Group
Specialised Services Service Specification: CP57b Genetic Testing for Inherited Cardiac Conditions Document Author: Specialised Planner Executive Lead: Director of Finance Approved by: Management Group
Northern Ireland COPD Audit
 Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET
 NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
Therapeutic Apheresis Services. User Satisfaction Survey. April 2017
 Therapeutic Apheresis Services User Satisfaction Survey 2017 Claire Gillson Service Development Manager Therapeutic Apheresis Services Olivia Pirret National Administrator Therapeutic Apheresis Services
Therapeutic Apheresis Services User Satisfaction Survey 2017 Claire Gillson Service Development Manager Therapeutic Apheresis Services Olivia Pirret National Administrator Therapeutic Apheresis Services
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN)
") NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices
 Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices 1. Population Needs 1. NATIONAL AND LOCAL CONTEXT 1.1 NATIONAL CONTEXT 1.1.1 Overview of commissioning responsibilities
Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices 1. Population Needs 1. NATIONAL AND LOCAL CONTEXT 1.1 NATIONAL CONTEXT 1.1.1 Overview of commissioning responsibilities
UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose
 Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
National Health Promotion in Hospitals Audit
 National Health Promotion in Hospitals Audit Acute & Specialist Trusts Final Report 2012 www.nhphaudit.org This report was compiled and written by: Mr Steven Knuckey, NHPHA Lead Ms Katherine Lewis, NHPHA
National Health Promotion in Hospitals Audit Acute & Specialist Trusts Final Report 2012 www.nhphaudit.org This report was compiled and written by: Mr Steven Knuckey, NHPHA Lead Ms Katherine Lewis, NHPHA
Title: Climate-HIV Case Study. Author: Keith Roberts
 Title: Climate-HIV Case Study Author: Keith Roberts The Project CareSolutions Climate HIV is a specialised electronic patient record (EPR) system for HIV medicine. Designed by clinicians for clinicians
Title: Climate-HIV Case Study Author: Keith Roberts The Project CareSolutions Climate HIV is a specialised electronic patient record (EPR) system for HIV medicine. Designed by clinicians for clinicians
Reference costs 2016/17: highlights, analysis and introduction to the data
 Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
Results of censuses of Independent Hospices & NHS Palliative Care Providers
 Results of censuses of Independent Hospices & NHS Palliative Care Providers 2008 END OF LIFE CARE HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament.
Results of censuses of Independent Hospices & NHS Palliative Care Providers 2008 END OF LIFE CARE HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament.
The PCT Guide to Applying the 10 High Impact Changes. A guide from NatPaCT
 The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
Improving the quality of diagnostic spirometry in adults: the National Register of certified professionals and operators
 Improving the quality of diagnostic spirometry in adults: the National Register of certified professionals and operators September 2016 Improving the quality of diagnostic spirometry in adults: the National
Improving the quality of diagnostic spirometry in adults: the National Register of certified professionals and operators September 2016 Improving the quality of diagnostic spirometry in adults: the National
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
NHMC. Homecare Medicines Services: National Homecare Medicines Committee. History
 NHMC National Homecare Medicines Committee Homecare Medicines Services: History Version Date Reason for change Person responsible for change V1 12/06/2018 New NHMC RPS Handbook for Homecare Services -
NHMC National Homecare Medicines Committee Homecare Medicines Services: History Version Date Reason for change Person responsible for change V1 12/06/2018 New NHMC RPS Handbook for Homecare Services -
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes 1.1 Short title Medicines
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes 1.1 Short title Medicines
FSRH consultation response: the regulation of Medical Associate Professions in the UK by the Department of Health
 FSRH consultation response: the regulation of Medical Associate Professions in the UK by the Department of Health The Faculty of Sexual and Reproductive Healthcare (FSRH) welcomes the opportunity to respond
FSRH consultation response: the regulation of Medical Associate Professions in the UK by the Department of Health The Faculty of Sexual and Reproductive Healthcare (FSRH) welcomes the opportunity to respond
Implementation of the right to access services within maximum waiting times
 Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Therapeutic Apheresis Services. User Satisfaction Survey. June 2016
 Therapeutic Apheresis Services User Satisfaction Survey 2016 Claire Gillson Service Development Manager Therapeutic Apheresis Services Amy Clifford National Administrator Therapeutic Apheresis Services
Therapeutic Apheresis Services User Satisfaction Survey 2016 Claire Gillson Service Development Manager Therapeutic Apheresis Services Amy Clifford National Administrator Therapeutic Apheresis Services
General practitioner workload with 2,000
 The Ulster Medical Journal, Volume 55, No. 1, pp. 33-40, April 1986. General practitioner workload with 2,000 patients K A Mills, P M Reilly Accepted 11 February 1986. SUMMARY This study was designed to
The Ulster Medical Journal, Volume 55, No. 1, pp. 33-40, April 1986. General practitioner workload with 2,000 patients K A Mills, P M Reilly Accepted 11 February 1986. SUMMARY This study was designed to
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI
 COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
SERVICE SPECIFICATION FOR THE PROVISION OF NHS HEALTH CHECKS IN BOURNEMOUTH, DORSET AND POOLE
 Revised for: 1 April 2014 APPENDIX 2.4 SERVICE SPECIFICATION FOR THE PROVISION OF NHS HEALTH CHECKS IN BOURNEMOUTH, DORSET AND POOLE DORSET COUNTY COUNCIL Page 2 of 12 1. INTRODUCTION 1.1. This Specification
Revised for: 1 April 2014 APPENDIX 2.4 SERVICE SPECIFICATION FOR THE PROVISION OF NHS HEALTH CHECKS IN BOURNEMOUTH, DORSET AND POOLE DORSET COUNTY COUNCIL Page 2 of 12 1. INTRODUCTION 1.1. This Specification
TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN ENGLAND NOVEMBER 2016
 TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN ENGLAND NOVEMBER 2016 EXECUTIVE SUMMARY Whilst cancer survival is at its highest ever level, our health services are under considerable pressure.
TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN ENGLAND NOVEMBER 2016 EXECUTIVE SUMMARY Whilst cancer survival is at its highest ever level, our health services are under considerable pressure.
ORGANISATIONAL AUDIT
 [Type text] National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians,
[Type text] National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians,
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET
 NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 1 st September 2016 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 1 st September 2016 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
Primary Care Workforce Survey Scotland 2017
 Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
STP: Latest position. Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan. July 2016
 STP: Latest position Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan July 2016 Who s involved? NHS Commissioners East Riding of Yorkshire CCG Hull CCG North
STP: Latest position Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan July 2016 Who s involved? NHS Commissioners East Riding of Yorkshire CCG Hull CCG North
WAITING TIMES 1. PURPOSE
 Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Document Title Investigating Deaths (Mortality Review) Policy
 Policy") Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
DRAFT 2. Specialised Paediatric Services in Scotland. 1 Specialised Services Definition
 Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY
 PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
2015/16 CQUIN Schemes
 Barnet, Enfield & Haringey Mental Health Trust 2015/16 CQUIN Schemes Version: 3.0 Version Date Revision Author 1.0 30/03/15 Excel to Word Document A Bland 2.0 01/04/15 1 st Discussion with BEHMHT A Bland
Barnet, Enfield & Haringey Mental Health Trust 2015/16 CQUIN Schemes Version: 3.0 Version Date Revision Author 1.0 30/03/15 Excel to Word Document A Bland 2.0 01/04/15 1 st Discussion with BEHMHT A Bland
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health and Social Care Directorate Quality standards Process guide
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex
 in Wessex") Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Trends in Consultation Rates in General Practice 1995 to 2006: Analysis of the QRESEARCH database.
 Trends in Consultation Rates in General Practice 1995 to 2006: Analysis of the QRESEARCH database. Final Report to the Information Centre and Department of Health Authors Professor Julia Hippisley-Cox
Trends in Consultation Rates in General Practice 1995 to 2006: Analysis of the QRESEARCH database. Final Report to the Information Centre and Department of Health Authors Professor Julia Hippisley-Cox
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Northern Ireland Peer Review of Cancer MDTs. EVIDENCE GUIDE FOR LUNG MDTs
 Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
Cardiovascular Health Westminster:
 Cardiovascular Health Westminster: An integrated approach to CVD prevention and treatment Dr Adrian Brown/Anna Cox Consultant in Public Health Medicine NHS Westminster Why prioritise CVD Biggest killer
Cardiovascular Health Westminster: An integrated approach to CVD prevention and treatment Dr Adrian Brown/Anna Cox Consultant in Public Health Medicine NHS Westminster Why prioritise CVD Biggest killer
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Heart Conditions Delivery Plan
 Heart Conditions Delivery Plan Highest standard of care for everyone with or at risk of a heart condition Produced by the Heart Conditions Implementation Group January 2017 Crown copyright 2016 WG30635
Heart Conditions Delivery Plan Highest standard of care for everyone with or at risk of a heart condition Produced by the Heart Conditions Implementation Group January 2017 Crown copyright 2016 WG30635
Do quality improvements in primary care reduce secondary care costs?
 Evidence in brief: Do quality improvements in primary care reduce secondary care costs? Findings from primary research into the impact of the Quality and Outcomes Framework on hospital costs and mortality
Evidence in brief: Do quality improvements in primary care reduce secondary care costs? Findings from primary research into the impact of the Quality and Outcomes Framework on hospital costs and mortality
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary
 Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Psychological therapies for common mental illness: who s talking to whom?
 Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
Preventing Heart Attacks and Strokes The Size of the Prize
 Preventing Heart Attacks and Strokes The Size of the Prize Dr Matt Kearney General Practitioner and National Clinical Director for CVD Prevention NHS England and Public Health England The NHS needs a radical
Preventing Heart Attacks and Strokes The Size of the Prize Dr Matt Kearney General Practitioner and National Clinical Director for CVD Prevention NHS England and Public Health England The NHS needs a radical
Review of Follow-up Outpatient Appointments Betsi Cadwaladr University Health Board
 Review of Follow-up Outpatient Appointments Betsi Cadwaladr University Health Audit year: 2014-15 Issued: October 2015 Document reference: 487A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Betsi Cadwaladr University Health Audit year: 2014-15 Issued: October 2015 Document reference: 487A2015 Status of report This document has been prepared as part
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Senior Manager, Performance and Compliance.
 UHB 033 Version No: 1 Previous Trust / LHB Ref No: Senior Manager, Performance and Compliance.") Reference No: PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Trust 364 Documents to read alongside this Policy. Ministerial Letter EH/ML/004/09 WAG Rules for Managing
Reference No: PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Trust 364 Documents to read alongside this Policy. Ministerial Letter EH/ML/004/09 WAG Rules for Managing
Facing the Future: Standards for Paediatric Services. April 2011
 Facing the Future: Standards for Paediatric Services April 2011 Facing the Future: Standards for Paediatric Services April 2011 (First Published December 2010 and amended by RCPCH Council March 2011) 2011
Facing the Future: Standards for Paediatric Services April 2011 Facing the Future: Standards for Paediatric Services April 2011 (First Published December 2010 and amended by RCPCH Council March 2011) 2011
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Data, analysis and evidence
 1 New Congenital Heart Disease Review Data, analysis and evidence Joanna Glenwright 2 New Congenital Heart Disease Review Evidence for standards Joanna Glenwright Evidence to inform the service standards
1 New Congenital Heart Disease Review Data, analysis and evidence Joanna Glenwright 2 New Congenital Heart Disease Review Evidence for standards Joanna Glenwright Evidence to inform the service standards
Policy Summary. Policy Title: Policy and Procedure for Clinical Coding
 Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
Improving patient access to general practice
 Report by the Comptroller and Auditor General Department of Health and NHS England Improving patient access to general practice HC 913 SESSION 2016-17 11 JANUARY 2017 4 Key facts Improving patient access
Report by the Comptroller and Auditor General Department of Health and NHS England Improving patient access to general practice HC 913 SESSION 2016-17 11 JANUARY 2017 4 Key facts Improving patient access
Annual Complaints Report 2017/2018
 . Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
. Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
UK Renal Registry 13th Annual Report (December 2010): Appendix A The UK Renal Registry Statement of Purpose
: Appendix A The UK Renal Registry Statement of Purpose") Nephron Clin Pract 2011;119(suppl 2):c275 c279 DOI: 10.1159/000331785 Published online: August 26, 2011 UK Renal Registry 13th Annual Report (December 2010): Appendix A The UK Renal Registry Statement
Nephron Clin Pract 2011;119(suppl 2):c275 c279 DOI: 10.1159/000331785 Published online: August 26, 2011 UK Renal Registry 13th Annual Report (December 2010): Appendix A The UK Renal Registry Statement
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
How to use NICE guidance to commission high-quality services
 How to use NICE guidance to commission high-quality services Acknowledgement We are grateful to the many organisations and individuals who have contributed to the development of this guide. A list of these
How to use NICE guidance to commission high-quality services Acknowledgement We are grateful to the many organisations and individuals who have contributed to the development of this guide. A list of these
SUPPORTING DATA QUALITY NJR STRATEGY 2014/16
 SUPPORTING DATA QUALITY NJR STRATEGY 2014/16 CONTENTS Supporting data quality 2 Introduction 2 Aim 3 Governance 3 Overview: NJR-healthcare provider responsibilities 3 Understanding current 4 data quality
SUPPORTING DATA QUALITY NJR STRATEGY 2014/16 CONTENTS Supporting data quality 2 Introduction 2 Aim 3 Governance 3 Overview: NJR-healthcare provider responsibilities 3 Understanding current 4 data quality
South East London Interface Prescribing Policy including the NHS and Private Interface Prescribing Guide
 South East London Interface Prescribing Policy including the NHS and Private Interface Prescribing Guide 1. Introduction 1.1 This policy has been developed by the South East London Clinical Commissioning
South East London Interface Prescribing Policy including the NHS and Private Interface Prescribing Guide 1. Introduction 1.1 This policy has been developed by the South East London Clinical Commissioning
How NICE clinical guidelines are developed
 Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Appendix 1. Policy on the Dissemination, Implementation and Monitoring of National Clinical Guidance
 Appendix 1 Policy on the Dissemination, Implementation and Monitoring of National Clinical Guidance Policy Title: Executive Summary: Policy on the dissemination, implementation and monitoring of national
Appendix 1 Policy on the Dissemination, Implementation and Monitoring of National Clinical Guidance Policy Title: Executive Summary: Policy on the dissemination, implementation and monitoring of national
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation Team YHSCN HULL AND EAST YORKSHIRE HOSPITALS Hull And East Yorkshire Hospitals Haematology MDT (13-2H-1) - 2015 Peer Review Visit
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation Team YHSCN HULL AND EAST YORKSHIRE HOSPITALS Hull And East Yorkshire Hospitals Haematology MDT (13-2H-1) - 2015 Peer Review Visit
BRIEFING PACK. WatchBP Office ABI Microlife Health Management Ltd
 BRIEFING PACK WatchBP Office ABI Microlife Health Management Ltd Prepared by: NHS Technology Adoption Centre Suite 3E 1 Portland Street Manchester M1 3BE Telephone: 0161 200 1620 www.ntac.nhs.uk MICROLIFE
BRIEFING PACK WatchBP Office ABI Microlife Health Management Ltd Prepared by: NHS Technology Adoption Centre Suite 3E 1 Portland Street Manchester M1 3BE Telephone: 0161 200 1620 www.ntac.nhs.uk MICROLIFE
National care of the dying audit for hospitals, England Executive summary May 2014
 National care of the dying audit for hospitals, England Executive summary May 2014 Foreword We only have one chance to get end of life care right and sadly sometimes we don t. There are few surprises in
National care of the dying audit for hospitals, England Executive summary May 2014 Foreword We only have one chance to get end of life care right and sadly sometimes we don t. There are few surprises in
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
NHS. Challenges and improvements in diagnostic services across seven days. Improving Quality
 NHS Improving Quality NHS Improving Quality working in partnership with NHS England Challenges and improvements in diagnostic services across seven days 2 Foreword Across the country, hospitals and primary
NHS Improving Quality NHS Improving Quality working in partnership with NHS England Challenges and improvements in diagnostic services across seven days 2 Foreword Across the country, hospitals and primary
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
CVD Network: Lipid Specialists Advisory Group Handover/Legacy Document. June 2016
 CVD Network: Lipid Specialists Advisory Group Handover/Legacy Document June 2016 NHS England High quality care for all, now and for future generations. Version Control: Version Purpose / Change Author
CVD Network: Lipid Specialists Advisory Group Handover/Legacy Document June 2016 NHS England High quality care for all, now and for future generations. Version Control: Version Purpose / Change Author
Linda Cutter / Dr Charles Heatley. GP Practices and Community Pharmacies
 Schedule 2 Part A Service Specification Service Specification No. 04 Service Anti-coagulation Monitoring Levels 3, 4 & 5 Commissioner Lead Provider Lead Linda Cutter / Dr Charles Heatley GP Practices and
Schedule 2 Part A Service Specification Service Specification No. 04 Service Anti-coagulation Monitoring Levels 3, 4 & 5 Commissioner Lead Provider Lead Linda Cutter / Dr Charles Heatley GP Practices and
BARIATRIC SURGERY SERVICES POLICY
 BARIATRIC SURGERY SERVICES POLICY Please note that all Central Lancashire Clinical Commissioning Policies are currently under review and elements within the individual policies may have been replaced by
BARIATRIC SURGERY SERVICES POLICY Please note that all Central Lancashire Clinical Commissioning Policies are currently under review and elements within the individual policies may have been replaced by
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for