OASIS C2 Strategies for Success
|
|
|
- Norman Fox
- 6 years ago
- Views:
Transcription


1 OASIS C2 Strategies for Success Presented by Selman-Holman & Associates, LLC Selman Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting, Education and Products CoDR Coding Done Right CodeProUniversity 606 N. Bell Ave. Denton, Texas fax Teresa Northcutt, BSN, RN, HCS-D, HCS-H, COS-C 2 Data Elements: Standardization Standardization: Ideal State 3 Why revise the OASIS data set? Mainly to increase standardization with assessment item sets for other post acute settings and to enable calculation of standardized, cross-setting quality measures, a provision of Improving Medicare Post- Acute Care Transformation (IMPACT) Act of 2014 HH SNF Skilled Nursing Facility (Minimum Data Set) IRF Inpatient Rehab Facility (Patient Assessment Instrument) LTCH Long Term Care Hospital (Continuity Assessment Record and Evaluation (CARE) Data Set) 4
2 5 Standardized Patient Assessment Data Use of Standardized Assessment Data no later than Functional status HHA: January 1, 2019 Other categories Cognitive status and mental function Special services, treatments and interventions Medical conditions and comorbidities Impairments 6 OASIS C2 Changes Two new cross-setting items M1313, M2001 New items to risk adjust pressure ulcer measure M1028, M1060, GG0170C Item revisions, re-numbering Look back period, DRR, pressure ulcers New dash (-) response New guidance on wounds Pressure ulcers, surgical wounds Uses of OASIS data 8 7 Purposes of OASIS OBQI, PBQI, OBQM Risk adjustment of outcome measures HH Compare, Quality of Care STAR rating IMPACT Act measures PPS calculation for payment HH VBP Model



3 OASIS Data Timepoints The Definition of an Episode Can Be D I f f e r e n t 9 OASIS data are collected at the following time points: Start of care. Resumption of care following inpatient facility stay. Recertification within the last 5 days of each 60-day recertification period. Other follow-up during the home health episode of care. Transfer to inpatient facility. Discharge from home care. Death at home. Payment Episode: SOC to Recert to Recert to 10 SOC ROC Quality Episode AKA Outcome Episode Transfer Discharge Death at Home 11 Ramifications Resumption of Care is as important as SOC Discharge is as important as SOC or ROC Unplanned discharges without a visit to the home for assessment can be disastrous to your outcomes SOC, FU, FU, FU, FU, DC not good for your Home Health Compare outcomes 12 Risk Adjusted End Result Outcome Measures Improvement in Grooming Dyspnea Bathing Bed transferring Toilet transferring Toilet hygiene Eating Speech and language Management of Oral Meds Confusion Frequency UTIs Bowel incontinence Ambulation/locomotion Status of surgical wounds Behavior problem frequency Pain interfering w/activity Upper body dressing Lower body dressing Light meal prep Phone use Anxiety level Stabilization Grooming Bathing Bed transferring Light meal prep Phone Use Management of Oral Meds Speech and Language Cognitive Functioning Anxiety level Toilet transferring Toilet hygiene
![Risk Adjusted Utilization Outcome Measures Outcomes 13 14 Discharged to community [OASIS based] Acute care hospitalization (ACH) [Claims based] ACH during 1 st 60 days of HH Rehospitalization during](/docs-images/73/68861457/images/4-0.jpg "1 st 30 days of HH [OASIS based] ED use w hospitalization [Claims based] ED use w/o hospitalization ED use without hospital readmission during 1 st 30 days of HH ED use w/o hospitalization during 1")

4 Risk Adjusted Utilization Outcome Measures Outcomes Discharged to community [OASIS based] Acute care hospitalization (ACH) [Claims based] ACH during 1 st 60 days of HH Rehospitalization during 1 st 30 days of HH [OASIS based] ED use w hospitalization [Claims based] ED use w/o hospitalization ED use without hospital readmission during 1 st 30 days of HH ED use w/o hospitalization during 1 st 30 days of HH Outcomes are health status changes between two or more time points, where the term health status encompasses physiologic, functional, cognitive, emotional, and behavioral health. Outcomes are changes that are intrinsic to the patient. Outcomes are changes that result from care provided, or natural progression of disease and disability, or both. Outcomes are positive, negative, or neutral changes in health status. Outcomes Example At SOC, Mr. Brown was marked as a OASIS data items are arranged from least impaired or independent, to most impaired or dependent. Except for GG0170c The answer at SOC/ROC is compared to the answer at Transfer/DC to determine if there has been improvement, decline or stabilization on that particular outcome. X
5 Home Health Compare IMPACT Act Measure Domains 17 Subset of OASIS based quality performance Publicly reported Outcome measures that indicate how well HHAs assist patients in regaining or maintaining their ability to function Process measures that evaluate the rate of HHA use of specific evidence-based processes of care 18 Skin Integrity and Changes in Skin Integrity. Medication Reconciliation. Resource Use Measures, i.e. Total estimated Medicare Spending Per Beneficiary. Discharge to Community. All-Condition Risk Adjusted Potentially Preventable Hospital Readmission Rates. Began reporting with OASIS C2 New Measure/New Items New Measure/New Items New or worsened pressure ulcer M1313a M1313b M1313c Risk adjusters GG0170c (Transfer Assistance) M1620 (Bowel) (Not new) M1028 (Diabetes) M1060a (BMI) M1060b (BMI) Revised item (M1309) Three new items Covariates Drug Regimen Review Conducted with Follow-Up for Identified Issues M2001 (measure calculation) M2003 (at SOC/ROC) M2005 (at Transfer/DC)



6 Claims Based Measures Process Measures 21 Resource Use Measure: Total Estimated Medicare Spending per Beneficiary. Outcome Measure: Discharge to Community. Outcome Measure: Potentially Preventable 30-Day Post-Discharge Readmission Measure. 22 Process measures evaluate the rate of HHA use of specific evidence-based processes of care. The HH QRP process measures focus on high-risk, high-volume, problem-prone areas for home healthcare. Desirable care process: Larger numerator relative to the denominator indicates higher quality. Undesirable care process: Smaller numerator relative to the denominator indicates higher quality. 23 No Longer Included on the HH Quality Measures Table Removed from Home Health Compare Will be on HHC preview reports for several quarters Removed in January 2018 CASPER reports Still can be used for internal purposes through Tally Reports 24


7 26 Why does Home Health need STAR Ratings? 25 Home Health Compare information overwhelming to consumers 27 outcome and process measures provide information on quality performance to allow informed choice of a home health agency Consumers are accustomed to using a star rating system to compare and choose products and services Home Health STAR ratings offer a simple tool to aid consumers health care decision making 27 Types of STAR Ratings Quality of Patient Care STAR Ratings Formerly called the Home Health Compare STAR ratings Posted on HHCompare web site since July 2015 Based on OASIS data submitted by agencies for outcome and process measures and claims data for acute care hospitalization Patient Survey STAR Ratings New as of January 28, 2016 Based on Home Health Consumer Assessment of Healthcare Providers and Services (HHCAHPS) measures currently reported on HHCompare. 28 Quality of Patient Care STAR Rating Measures Outcome Measures Improvement in Ambulation Improvement in Bed Transferring Improvement in Bathing Improvement in Pain Interfering with Activity Improvement in Shortness of Breath Acute Care Hospitalization Process Measures Timely Initiation of Care Drug Education on all Medications Provided to Patient/Caregiver Influenza Immunization Received for Current Flu Season
8 29 Home Health STAR Rating: Agency Eligibility All Medicare-certified agencies are potentially eligible to receive a STAR rating Eligible agencies must have at least 20 completed quality episodes for data on a measure to be reported on HHCompare Eligible agencies must have reported data for 5 of the 9 quality and process measures Eligible agencies must have data for 40 or more patient surveys in the reporting period Eligible episodes must have a discharge date within the 12 month reporting period Eligible agencies must be at least 6 months old 30 Home Health STAR Rating: Calculation Each measure is rated, assigned a decile rating, adjusted ratings are averaged across the 9 measures, and rounded to the nearest 0.5. Each measure carries same importance Overall STAR ratings range from 1.0 to 5.0, reported in half star increments, with 3.0 stars as the middle category Updated quarterly in January, April, July and October 31 Why should I care about STAR ratings? 32 Acute Care Hospitalization Used by customers, referral sources and payers to choose home care providers Used by large agencies to influence decisions on mergers and acquisitions Value-Based Purchasing pilot project in nine states NOW uses ongoing performance on outcome and process measures to impact payment in future Some Medicare Advantage programs are cutting payments to agencies with STAR ratings below 5 Agency with 2 or 3-star rating will receive 75% of the standard episode payment rate Agency with 4-star rating will receive 85% of standard payment rate Uses claims based information The ACH and ED Use without Hospitalization measures evaluate patient admission to an acute care hospital and emergency department (without hospitalization), respectively, during the 60 days following the start of home health stay. Planned hospitalizations are not counted
9 33 Risk Adjustment Three types of risk adjustments: Exclusions: Patients whose outcomes are not under HHA control or for whom the outcome may be unavoidable are removed from the calculation. Stratification: Patients with similar risks for the outcome based on their clinical characteristics are grouped together, and the measure is calculated separately for each risk group. > 75 yo with Joint replacements Covariates: Patient characteristics that may affect risk for a certain outcome. 34 Episodes Excluded from Outcome Episodes Those episodes that score a zero at SOC / ROC For example patient is scored a zero on transferring transferring will not be evaluated on that particular patient for the rest of his stay Those episodes that don t change either up or down (unless there is a stabilization outcome for that particular measure) Episodes longer than one year Measure-specific exclusions 35 Risk Adjustment Statistical risk adjustment refers to a collection of analytic methods designed to separate the relationships of outcomes with care provided from the relationship of outcomes with natural progression of disease and disability. One of the major purposes of OASIS is to provide data items needed for risk adjustment. General intent of risk adjustment is to compensate or adjust for differences in case mix or risk factors (between agency and a comparison sample) that should be taken into consideration if outcomes are to be compared validly. Risk adjustment compensates or controls for the potential influence of case mix variables (i.e., risk factors) that can affect outcomes. 36 Process Measures Processes that promote good outcomes known as best practices Some require standardized validated tools Domains timely care care coordination patient assessment care planning care plan implementation education prevention
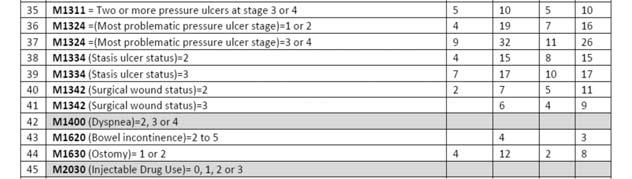
10 Standardized and Validated Tools Standardized Tools Integrated? A standardized and validated tool is one that 1) has been scientifically tested on a population with characteristics similar to that of the patient being assessed and shown to be effective in identifying ((the problem)); and 2) includes a standard response scale (e.g., a scale where patients rate pain from 0-10). The standardized tool must be appropriately administered as indicated in the instructions and must be relevant for the patient's ability to respond. CMS does not endorse a specific tool. There is no Medicare requirement that standardized assessment tools be embedded in agency s comprehensive assessment (except PHQ-2 in M1730). It is acceptable for clinician to supplement agency s comprehensive assessment with additional standardized assessment forms to meet the criteria for OASIS best practice items. Include form in medical record with comprehensive assessment. Q&A#1 April 2013 Potentially Avoidable Events Home Health Resource Group Emergent Care for Injury Caused by Fall Emergent Care for Wound Infections, Deteriorating Wound Status Emergent Care for Improper Medication Administration, Medication Side Effects Emergent Care for Hypo/Hyperglycemia Discharged to community needing wound care or medication assistance Discharged to community with behavioral problems Discharged to the community needing toileting assistance Discharged to the community with a unhealed stage 2 pressure ulcer Substantial Decline in 3 or more Activities of Daily Living Substantial Decline in Mngt of Oral Medications Development of Urinary Tract Infection Increase in Number of Pressure Ulcers OASIS is the basis for payment HHRG produced through grouper software Determined through certain OASIS responses Three domains Clinical Severity Functional Status Service utilization 45 HHRGs; 153 case mix weights C1F1S1 to C3F3S5 for four different equations (five different groupings) (five different C1F1S1s)


, diabetes and right fractured hip she sustained at the same time as her heart attack.")
11 Case Mix Coding Concepts Payment Case mix variables table Case mix diagnoses Case mix manifestation Non-Routine Supplies Only one diagnosis from each case mix group can earn points If the patient has an AMI and ASHD and CHF, points can only be earned once. Case mix manifestation codes can only earn points if an acceptable etiology is placed in the space preceding the manifestation. If the number of therapy visits is more or less than estimated at the beginning of the episode, then the scoring may shift. If a Z code is primary, and the next code down is case mix, then that diagnosis is counted as primary. Case Mix System Diagnosis Coding Mrs. Rose is admitted to home care after a CABG following a heart attack 3 weeks ago. Other co-morbidities include hypertension (stable with new medications), diabetes and right fractured hip she sustained at the same time as her heart attack. Aftercare is the focus of care along with rehab for the fracture. Her diabetes is also of concern. Her doctor documents her blood sugars are too high ( ), so her insulin dosage had increased. Her surgical wound is not epithelialized yet. There is one area of incisional separation 4 cm long. Dressing changes are ordered. She has 14 therapy visits ordered and it is an early episode. Other OASIS items have been answered like this: M1240 (Pain) 3 M1830 (bathing) 2 M1342 (surgical wound status) 3 M1840 (toileting) 2 M1810 (upper body dressing) 1 M1850 (transferring) 2 M1820 (lower body dressing) 2 M1860 (ambulation) 3 Z Aftercare circulatory I25.10 ASHD I21.3 Acute MI E11.65 Diabetes with hyperglycemia S72.001D Traumatic fracture hip, right, subsequent episode Z48.01 surgical dressing change

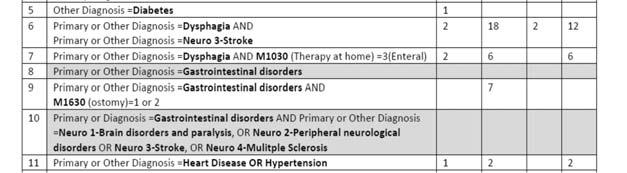
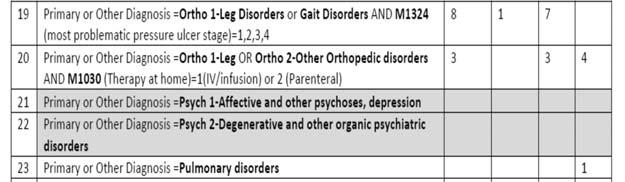
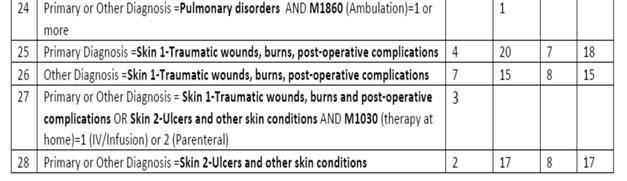
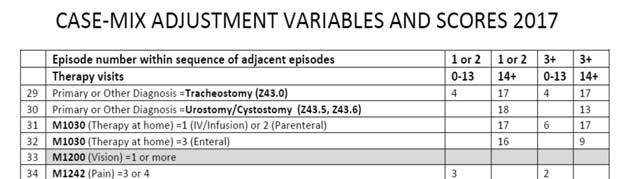


12 Add up the functional points


13 Now determine the score Value Based Purchasing 50 OASIS-based measures are reported on all Medicare FFS, Medicare Advantage, Medicaid FFS and Medicaid Managed Care patients The payer for the episode is one of the risk factors used in outcome risk adjustment Claims-based measures are only reported on the Medicare FFS population, since measures are only derived from Medicare claims data HHCAHPS-based measures are reported for all patients 18+ years old covered by Medicare or Medicaid who meet other criteria to be eligible for the survey Value Based Purchasing VBP Measures 51 OASIS measures are risk adjusted at the national level to compensate for differences in the patient population served by different home health agencies Measures Tables for VBP located at: Initiatives-Patient-Assessment- Instruments/HomeHealthQualityInits/HHQIQ ualitymeasures.html 52 OASIS-based measures (10): Improvement in Ambulation/Locomotion Improvement in Bed Transferring Improvement in Bathing Improvement in Dyspnea Improvement in Pain Interfering with Activity Improvement in Management of Oral Medication Education on All Medications Influenza and Pneumonia Vaccinations Discharge to Community
14 VBP Measures Nine States in VBP Pilot 53 Claims-based measures (2): Acute Care Hospitalization: Unplanned Hospitalization during the first 60 days of Home Health Emergency Department Use without Hospitalization HHCAHPS-based measures (5) HHVBP Secure Portal measures (3 New Measures) 54 Arizona Florida Iowa Maryland Massachusetts Nebraska North Carolina Tennessee Washington Value Based Purchasing Value Based Purchasing 55 Payment adjustments will be based on each HHA s Total Performance Score (TPS) in a given performance year (PY) on (1) a set of measures already reported via OASIS and HHCAHPS for all patients serviced by the HHA and select claims data elements, and (2) three New Measures where points are achieved for reporting data. 56 (1) A maximum payment adjustment of 3 percent (upward or downward) in CY 2018; (2) a maximum payment adjustment of 5 percent (upward or downward) in CY 2019; (3) a maximum payment adjustment of 6 percent (upward or downward) in CY 2020; (4) a maximum payment adjustment of 7 percent (upward or downward) in CY 2021; and, (5) a maximum payment adjustment of 8 percent (upward or downward) in CY2022.
15 Assessment OASIS Data Collection 58 Resources for OASIS Accuracy OASIS-C2 data set OASIS-C2 Guidance Manual, Ch. 3 Update for 2018 CMS OASIS Q&A s Oct. 2016, effective Jan CMS Quarterly Q&A s OEC for your state When guidance from two CMS resources conflicts use the most recent. When unable to find an exact answer use clinical judgement. 57 Patients 59 The How, Who, What & When of OASIS C1: the Patients, the CoPs, the Timepoints and the Conventions 60 OASIS data are collected for Medicare and Medicaid patients, 18 years and older, receiving skilled services, with the exception of patients receiving services for pre- or postnatal conditions. Includes Medicare Advantage plans, etc Patients receiving only personal care, homemaker, or chore services are excluded since these are not considered skilled services.
16 If OASIS is not required: Who can collect OASIS data? 61 HHAs must provide each patient, regardless of payment source, with a patient-specific comprehensive assessment that accurately reflects the patient s current health status. The comprehensive assessment must also identify the patient s continuing need for home care, medical, nursing, rehab, social and discharge planning needs. Only exception is housekeeping and chore services Comprehensive assessment includes drug regimen review. HHAs may continue to collect OASIS data on non- Medicare/non-Medicaid patients for agency use, BUT do not transmit the info. 62 Qualified clinicians RN PT ST OT (but not on SOC) Who CANNOT collect OASIS? SW LVN/LPN PTA OTA HHAides 63 The CoPs Comprehensive Assessment 64 Completion of Assessment 42 CFR CoPs OASIS 1. Initial assessment visit 2. Completion of the comprehensive assessment 3. Drug regimen review 4. Update of the comprehensive assessment 5. Incorporation of the OASIS data set Start of Care (SOC): Comprehensive assessment to be completed within 5 days after SOC Resumption of Care (ROC): Comprehensive assessment to be completed within 48 hours of inpatient facility discharge or agency knowledge of return home Comprehensive assessments to be completed within 48 hours of becoming aware of the patient s disposition: Transfer (TRN) to inpatient facility. Discharge (DC) from home care. Death at Home (Death). Other Follow-Up (FU). Recertification: Days of each 60 day episode
17 OASIS data items are not meant to be a comprehensive assessment Drug Regimen Review Not meant to be a complete assessment by themselves Integrate the OASIS data items into your own comprehensive assessment and throw the redundancy out Required at every comprehensive assessment NOT the same as the actual items M2001 Drug Regimen Review SOC/ROC M2003 Medication Follow-up SOC/ROC M2005 Medication Follow-up TRN/DC/Death M2010 High risk Medication Intervention SOC/ROC M2016 Patient Caregiver Drug Education Intervention TRN/DC A review of ALL medications the pt is currently using in order to identify any potential adverse effects and drug reactions, including ineffective drug therapy, significant side effects, significant drug interactions, duplicate drug therapy, and noncompliance with drug therapy. This requirement applies to all pts being serviced by the HHA, regardless of whether the specific requirements of OASIS apply. Initial Assessment Initial Assessment 67 Initial means FIRST visit Determines immediate care needs and eligibility for Medicare patients Must be conducted either Within 48 hours of referral Within 48 hours of return home On physician-ordered SOC date 68 Must be conducted by RN, unless therapy only case If therapy only Appropriate therapist may perform initial assessment OT may only complete initial assessment if need for OT establishes program eligibility (cannot perform a SOC on a Medicare patient)
18 Comprehensive Assessment M0030 SOC Date Completed in timely manner Consistent with patient s immediate needs No later than 5 days after SOC (SOC is day 0) May NOT be started prior to SOC (first billable visit) RN only, unless therapy only case May perform initial assessment and comprehensive assessment on same visit (usually what happens) or on different visits If no skilled service is delivered by the RN, the visit is not the SOC or reimbursable (will not be accepted by HAVEN as SOC) Date that the first reimbursable service is delivered A physician must specifically order that a particular covered service be furnished on the SOC date. All other coverage criteria must be met for this initial service to be billable and to establish the start of care. 71 SOC Determination for multidisciplinary cases A reimbursable service must be delivered to be considered the start of care for Medicare patients. For Medicare reimbursement (42CFR409.46), a physician must specifically order that a particular skilled service be furnished during the evaluation in which the agency accepts the beneficiary for treatment and all other coverage criteria must be met for this visit to be billable as a skilled nursing visit CFR Services that are allowable as administrative costs but are not separately billable include, but are not limited to, the following: (a) Registered nurse initial evaluation visits. Initial evaluation visits by a registered nurse for the purpose of assessing a beneficiary s health needs, determining if the agency can meet those health needs, and formulating a plan of care for the beneficiary are allowable administrative costs. If a physician specifically orders that a particular skilled service be furnished during the evaluation in which the agency accepts the beneficiary for treatment and all other coverage criteria are met, the visit is billable as a skilled nursing visit. Otherwise it is considered to be an administrative cost.
19 If the agency chooses to have an RN conduct the comprehensive assessment for therapy only cases, the RN should perform the assessment on the same day or within 5 days after the therapist s SOC date. 2-Q Any comprehensive assessment info collected prior to the SOC date may not contribute to the SOC comprehensive assessment. 2-Q36.1 Therapy only ordered Therapy has to complete comprehensive assessment with OASIS RN or Therapist may complete initial assessment OR No nursing need (no billable visits) Therapy establishes first billable visit (SOC). RN has to complete comprehensive assessment w/ OASIS on the same day or within 5 days after SOC What makes a visit skilled or billable? 76 Requirements for Therapy at SOC Therapy the evaluation itself is billable Nursing the assessment itself is not billable What makes nursing skilled? Intermittent medically recurring need What s the fix? Therapy does the initial assessment prior to, or on the same day as, the nurse completes comprehensive assessment with OASIS. If therapy does initial assessment, must get consent signed Nursing establishes the start of care with a truly billable visit. For skilled PT or SLP to perform the SOC visit for Medicare patient: 1. the HHA is expected to have orders from the patient s physician indicating the need for physical therapy or SLP prior to the initial assessment visit; 2. no orders are present for nursing at the start of care; 3. a reimbursable service must be provided; and 4. the need for this service establishes program eligibility for the Medicare home health benefit (42 CFR (a)(2). Occupational therapy does not establish program eligibility for Medicare home health benefit
20 One Non billable Nursing Visit One Non billable Nursing Visit We received an order for nursing and PT. The nurse conducted the initial assessment visit and determined that the patient did not have any justifiable nursing need, but did have a need for PT services. Because there was an order for nursing present with the original orders, is the RN required to complete the SOC comprehensive assessment? Or since nursing services are not necessary, can the PT complete the SOC comprehensive assessment on or within 5 days after the PT establishes the start of care? Since an order for nursing existed at the time of the initial referral, the RN must complete the initial assessment visit. If it is determined during the initial assessment visit, that the patient either did not have a need for nursing services and/or the patient declined all nursing services, the SOC will not be established by that visit. The RN can notify the physician that nursing will not be involved in the patient s care, and either continue on to complete the SOC comprehensive assessment (if the PT will be establishing the SOC that day), OR have the PT complete the SOC comprehensive assessment on or within 5 days after the PT establishes the start of care. 3 rd Q 2014 Who can conduct the assessment? 80 Nursing and therapy ordered Therapy has to do SOC and complete OASIS Nursing must complete initial assessment OR No nursing need (no billable visit) RN has to complete OASIS on the same day or within 5 days after SOC If the RN s entry in the case is known at SOC (i.e. the nursing is scheduled even if only for one visit) then the case is NOT therapy-only, and the RN should conduct the initial and SOC comprehensive assessment. PT establishes eligibility, not nursing If the order for the RN is not known at SOC and originates from a verbal order after SOC, then the case is therapy only at SOC, and the therapist can perform initial and SOC comprehensive assessment. 2-Q10 79
21 Who can conduct the assessment? Who Can Start First? 81 If therapy and aides are ordered: Because this is considered a therapyonly case (i.e. therapy is the only skilled service), the PT or ST could perform the comprehensive assessment and all subsequent assessments RN supervisory visits are not billable visits 2-Q11 82 If PT and HHA are ordered who can start first? The aide s visit is a reimbursable visit. Registered nurse does a non-billable initial assessment visit to establish needs and eligibility for a therapy only patient and sets up the aide care plan. The aide visits the same day as the RN. Do we now have a SOC date? 2-Q48 83 M0090 Date assessment completed No Later than 5 days after the SOC Polly Perfect, RN admits the patient to home care on 3/7 with a skilled visit. She calls the physician about a suspicious area on the patient s hip on 3/8, and what looks like duplicative medications. Therapist eval done 3/9 and the answer to M2200 is determined. Physician s office calls back on 3/10 with info confirming closed stage 3 ulcer on the hip and to DC one of the medications. Polly finishes entering the assessment info and turns in the SOC on 3/11. What is the SOC date? What is the M0090 date on the SOC assessment? 84 Comprehensive assessment must be updated and revised Not less frequently than the last 5 days of every 60 day episode beginning with the SOC date (days 56-60) (Follow-Up) Major decline or improvement in condition (Other Follow-Up) Within 48 hours of patient s return home from an inpatient facility admission of 24 hours or more for reasons other than diagnostic tests (ROC) At discharge (DC) All of these time points require a VISIT to the patient

22 85 Update of the Comprehensive Assessment Any qualified skilled discipline may perform the updates, e.g. the nurse does not have to perform the recert and the discharge just because the RN had to do the admission. RN, PT and OT are ordered at SOC PT and OT are continuing into the next episode OT continuing into the next episode What about SLP? 2-Q M0100 RFA SOC = first billable visit date POC established Discipline starting care may differ for different payors This is the appropriate response any time an initial HIPPS code (for a Home Health Resource Group) is required, whether or not the patient will be receiving ongoing services. Single Visits and Payment What if just one visit? 87 Per the CMS payment regulations as of January 2010, you must submit an OASIS assessment in order to be paid for a final claim under the Medicare PPS system. If you choose NOT TO BE PAID, there is no requirement to collect and transmit OASIS data if there has been only one visit. 2-Q42.2 The discharge OASIS is never mandated in situations of single visits in a quality episode (SOC/ROC to TRF/DC) 2-Q The patient is admitted to home care (single visit is made) and then the patient refuses any further visits, is an OASIS required? The agency is not required to assess the OASIS items, nor encode and submit their assessment (as of 12/2003). The comprehensive assessment would be placed in the medical record. HOWEVER, you cannot bill without an HHRG. If you want to be PAID for that single visit, you must collect, encode and submit the assessment.
23 What if just one visit? What happens if.. 89 What if you ve already completed OASIS (SOC or ROC), encoded and/or transmitted, and then no further visits are made? Conduct no further assessments. Document that no further visits occurred. Patient s name will appear on data system for 6 months If patient is readmitted, there will be a warning that OASIS is out of sequence but will not prevent OASIS from being transmitted 4b-Q21 90 During the SOC assessment the patient has dyspnea and has to be transferred to the hospital before the entire admission process is completed? If skilled care was provided and eligibility was established and the patient is not admitted to the facility, then the clinician still has five days after the SOC to complete the assessment. Has to be the same clinician. Answers can be changed after the patient returns from the facility to reflect new condition 2-Q17.1 What happens if Example and Ramifications 91 The patient is admitted to the hospital after ONE visit? You have two options: Readmit the patient when the patient is discharged from the hospital with a new SOC assessment. Place the first one in the medical record with explanation. The first SOC can only be billed if the OASIS was completed and transmitted. Transfer to Impatient Facility without Discharge and then Resume care when patient returns home. 2-Q SOC completed and then patient transferred into hospital. Readmit. No acute hospitalization counted against agency Start new with a new HHRG. Transfer and ROC Acute hospitalization when you didn t have a chance to even try to prevent hospitalization. Stuck with the original HHRG after the hospitalization (no opportunity for billing a SCIC) This is only true if just ONE visit is made!
24 What if No 93 An initial assessment with skilled service Start of Care (SOC) was performed on 6/24 (the SOC comprehensive assessment with OASIS was begun, but not completed). Later in the day, the patient was admitted to the hospital and returned home on 6/26. The comprehensive assessment with OASIS data collection was completed on 6/26, within the 5 day window. Since the comprehensive assessment was completed after the hospital admission, we did not do a Transfer or ROC. Was this correct? 94 In order to bill for the 6/24 visit, the SOC assessment should be completed within 5 days after the SOC date Transfer and Resumption of Care assessments (ROC) should be completed within 2 days after knowledge of a qualifying stay in the inpatient facility. At SOC, you may take up to 5 days after the SOC date to complete the SOC comprehensive assessment, noting that it must be completed by one clinician. When the patient returned to your care on 6/26 which was within the allowed 5 day assessment time frame, the same assessing clinician could complete the SOC comprehensive assessment that was begun on the first visit, updating previously completed items as necessary and completing the rest of the items. M0030, Start of Care Date, remains the date of the first billable visit. M0090, Date Assessment Completed, is the actual date the single clinician completed the assessment. So Even Non Billable Visit Counts 95 If the original assessing clinician could not complete the SOC comprehensive assessment that he/she began on the first visit 6/24, another qualified clinician would have to visit and complete a new SOC comprehensive assessment from beginning to end, within 5 days after the SOC date. Unless it had already been completed by someone else, the clinician who completes the SOC assessment on 6/26 may also complete the RFA 6- Transfer. The ROC assessment must be completed with 2 calendar days of the patient s inpatient facility discharge, and may also be completed on the 6/26 visit, by the same clinician who completes the SOC assessment and the OASIS Transfer data collection. July 2014 Q&A 96 If nursing performs a non-billable admit for a PT only case, the PT goes the same day completing an evaluation only, and there is no further need for therapy, are we required to complete the RFA 9 OASIS Discharge? For skilled Medicare and skilled Medicaid patients, OASIS data collection is required if more than one visit was made in a quality episode. In your scenario, the nurse made one visit and the PT made one visit. Therefore both the SOC (RFA 1) and DC (RFA 9) comprehensive assessments are required. This is true even if one of the visits was non-billable. 2-Q
25 97 M0032 Resumption of Care Date Specifies the date of the first visit following an inpatient stay by a patient receiving service from the home health agency (ROC date not necessarily the date assessment is done). Following an inpatient stay of 24 hours or longer For reasons other than diagnostic tests Need to update the Patient Tracking Sheet for the most recent ROC date 98 RFA 3 Resumption of Care If the patient returns home from an inpatient stay during the last 5 days of the episode Complete ROC, not Follow-Up ROC OASIS will determine the HHRG for the subsequent episode so answer M2200 and M0110 accordingly Returns home on day 54 what now? 3-Q5 My patient was released from the hospital and needed an injection that evening (Feb 26). The case manager was unavailable and planned to do the ROC assessment the following day (Feb 27). Could the on call nurse visit and give the injection before the resumption of care assessment is done? Is there a time frame in which care (by an LPN or others) can be provided prior to the completion of the ROC assessment? ROC date M0032 is. M0090 date on ROC assessment is. Can the LPN do the ROC visit? The assessment? There is no requirement that the ROC assessment be on the first visit. 2-Q bQ23.3 Didn t know the pt was in the hospital 100 Resumption of Care Can the RN do the ROC on a therapy only case before the therapist visits? The ROC assessment must be performed within 48 hours of the patient s return home after an inpatient facility stay (or within 48 hours of knowledge). Before or after the therapist visit. 4b-Q23.9 ROC date (M0032) is the first visit, regardless who makes it, or whether or not it is billable. 2-Q
26 Resumption of Care ROC Clarified again 07/13 and 01/14: No flexibility in performing ROC outside of timeframe: Within 48 hours of return home from an inpatient stay or within 48 hours of agency knowledge of inpatient stay If the standardized assessment is performed outside of those timeframes, you must answer No to M1240, M1300, M1730 and M1910, EXCEPT in certain unlikely circumstances. You must answer No to M2250 unless NA is the appropriate answer (unless you already had orders) M1240, Pain Assessment, M1300, Pressure Ulcer Risk Assessment, M1730, Depression Screening, and/or M1910, Falls Risk Assessment may be reported with "Yes" responses, if the relevant standardized, validated assessments were conducted by the assessing clinician within the 48 hour time frame, even if the ROC comprehensive assessment was completed after the 48 hour time frame. ROC Late Transfer and ROC 103 When the assessing clinician takes credit on M1240, M1300, M1730 and/or M1910 for standardized, validated assessments completed within the 48 hour time frame and the M0090 date indicates that the ROC comprehensive assessment was completed late (beyond the 48 hour time frame), clarifying documentation to support the reported OASIS responses is expected. If the relevant standardized, validated assessment was completed greater than 48 hours after inpatient facility discharge or greater than 48 hours after gaining knowledge of a qualifying stay in an inpatient facility, M1240, M1300, M1730 and M1910 must be answered "No". 104 A recert has been done and then we find out that the patient had an inpatient stay. When the agency becomes aware of a qualifying stay in an inpatient facility, a Transfer OASIS and Resumption of Care (ROC) assessment must be completed within 2 days of gaining the knowledge. You will receive a notice that the assessments have been submitted out of sequence. April 2014
27 ROC Situation One More ROC Situation 105 The RN visits the patient after his discharge from the hospital. She finds him in acute distress. She calls his doctor who directs the nurse to call 911. The patient is admitted back into the hospital. There is no requirement to collect OASIS data. Why? No requirement to collect OASIS data on one visit episodes (this is considered a quality episode) 2-Q19, The patient is admitted to the hospital during the episode. When making the ROC visit, the patient refuses further visits. If the visit is made, there is no requirement to collect OASIS data. Why? No requirement to collect OASIS data on one visit episodes (this is considered a quality episode) 2-Q19, Quiz 108 M0100 RFA 4 Recertification & RFA 5 Other Follow Up Patient returns home from hospital after transfer and needs PT visit for eval of equip, etc. PT determines no further visits are required. Is ROC assessment required? Is DC OASIS required? Is a DC summary required? 2-Q54.2 Days (Follow Up aka Recertification) Due to a major decline or improvement in patient condition (Other Follow-Up) Updates the patient s plan of care Your policy dictates when you have to do another assessment Has the patient improved or deteriorated beyond your expectations? Must be completed within 2 days of identifying major improvement or decline.
28 M0100 RFA 4 Recertification Late Recertification 109 If Days are missed, do not DC and readmit. M0090 is the date assessment is done Include in clinical documentation reason late Will get a warning message Legal considerations!! Example: Start of episode is October 15. Recert should have been done Oct 10-14, but due to error was not performed until October 18. M0090 is Oct. 18, but SOE is still October Q We missed completing a recertification assessment on a patient between days During the first visit in the new episode, the patient was transferred to the emergency room before the Recertification comprehensive assessment could be completed. The patient had a qualifying stay in an inpatient bed. What OASIS is due when we resume care of the patient? 111 Answer 112 Missed the Recert and Decided to DC Do not discharge the patient. A Transfer assessment (RFA 6) should be completed. If the patient returns to the HHA, a Resumption of Care (ROC) comprehensive assessment should be completed. The ROC will serve as both the Resumption of Care and the Recertification, establishing the PPS payment code for the next certification period. This demonstrates non-compliance with the Medicare comprehensive assessment update standard of the Conditions of Participation, but is the only option available due to the missed recertification. Care should be taken to monitor recertification dates to avoid this situation in the future Don t change your episode dates. If there was a need for continuing services into the next certification period, but the clinician missed completing the recertification assessment between day and on the first visit in the new episode it was determined the patient had reached goals and needed to be discharged, do I have to complete both the Recert and the Discharge OASIS? Yes. When a Recertification assessment is missed it should be completed as soon as possible. If the clinician determined the patient was ready for discharge on the first visit in the new episode, the Discharge comprehensive assessment is also required. The discharge is the endpoint of the quality episode, which is not captured with a recertification assessment. 3Q11.1
29 M0100 RFA 4 Recertification Transfer to Inpatient Facility 113 What if done too early? Do it over within the right time points. Even if into the next episode when you figure it out. 3-Q11.2, 4b-Q23.5 A clinician may start the comprehensive assessment on day 56 and complete it on any day on or before day 60. Only one clinician may complete though, so if Nurse A begins, then Nurse A must complete. 3-Q RFA 6 Transfer not DC Inpatient admission of 24 hours or longer Reasons other than diagnostic tests Patient expected to resume care Does not require a home visit If patient does not return, a DC visit/oasis is not required (a DC summary is required) RFA 7 Transfer with DC Inpatient admission of 24 hours or longer Reasons other than diagnostic tests Is not expected to return to home care or does not return by the end of the episode Does not require a home visit What is an admission? Inpatient Time Cumulative In order to qualify for the Transfer to Inpatient Facility OASIS assessment timepoint, the patient must meet 3 criteria: 1) Be admitted to the inpatient facility (not the ER, not an observation bed in the ER) 2) Reside as an inpatient for 24 hours or longer (does not include time spent in the ER) 3) Be admitted for reasons other than diagnostic testing only An admission to an inpatient facility for observation is not an admission for diagnostic testing only. Inpatient observation is considered a hospitalization. 4-Q23.7 If the patient was admitted to one inpatient facility bed then transferred to another, the Transfer OASIS would be required once a total of 24 hours have been spent as an inpatient, under an inpatient billing status. 4-Q23.01
30 117 Is this an admission? A patient is held for several days in an observation bed (referred to as a Patient Observation or PO bed) in the emergency or other outpatient department of a hospital to determine if the patient will be admitted to the hospital or sent back home. While under observation, the hospital did not admit the patient as an inpatient, but billed as an outpatient under Medicare Part B. Is this Emergent Care? With or without hospitalization? Should we complete a transfer, discharge the patient, or keep the patient? Inpatient vs outpatient observation 4-Q What is considered a diagnostic test? Tests, scans and procedures utilized to yield a diagnosis X-rays, UGI, CT scans Cardiac catheterization? Requires that each case be considered individually RFA 6 vs. RFA 7 RFA 6 vs. RFA If the HHA plans on the patient returning after their inpatient stay, RFA 6 should be completed. The RFA 7 is necessary only when the HHA does NOT anticipate the patient will be returning to care. 2-Q3 Providers should not discharge (use RFA 7) when goals have not been met at transfer. 2-Q3 What if we complete an RFA 6 and the patient does not return? No need to cancel and change to RFA 7 will be on data system for 6 months. 120 Medicare Claims Processing Manual, CMS Publication 100-4, Chapter 10, reads, A beneficiary does not have to be discharged from home care because of an inpatient admission. If an agency chooses not to discharge and the patient returns to the agency in the same 60-day period, the same episode continues. However, if an agency chooses to discharge, based on an expectation that the beneficiary will not return, the agency should recognize that if the beneficiary does return to them in the same 60-day period, the discharge is not recognized for Medicare payment purposes. All the home health services provided in the complete 60- day episode, both before and after the inpatient stay, should be billed on one claim."
31 121 Quiz Patient is transported to hospital and is placed on observation on June 26. On June 28, his status is changed to inpatient. What is the M0906 transfer date? What is the M0090 date on the transfer? 122 Quiz You make a routine visit and discover the patient was in the hospital for two days earlier in the week. You find that it was a qualifying stay in an inpatient facility. Within 2 calendar days of knowledge of transfer Complete the RFA 6 (TRN) and the RFA 3 (ROC) True or False? 4b-Q M0100 RFA 8 Death at home Complete Death at home while still under the care of the agency At home At church While in route to or before treatment in an ER Before inpatient admission (pronounced DOA) Exception--Complete transfer assessment INSTEAD, if Death while under care of facility (in ER) Regardless of length of time in the facility 2-Q Transfer or Death at Home? My patient died during outpatient surgery. Should I complete a transfer or a death at home? My patient collapsed at church and died in the ambulance on the way to the ER. Should I complete a transfer or a death at home? 2-Q
32 Visit or not? M0100 RFA 9 Discharge Transfer and Death at Home OASIS time points require data collection and not actual pt assessment findings, any RN, PT, OT or SLP may collect the data, as directed by agency policy. Not assessments, do not require the clinician to be in the physical presence of the pt. May be completed by chart review and telephone. It is not required that the clinician completing the data collection must have previously visited the pt. This guidance applies only to the Transfer and Death time points, as a visit is required to complete the comprehensive assessments and OASIS data collection at the Start of Care, Resumption of Care, Recertification, Other Follow-up and Discharge. 2-Q15.6, 4b-Q13.2 Not due to an inpatient facility admission Not due to death at home Visit required to complete assessment Except in cases of unexpected discharge Unplanned or unexpected discharges Assessment must report patient status at an actual visit Last visit conducted by a qualified clinician 2-Q37 with 7 different unplanned dc scenarios 127 Unplanned or Unexpected Discharges 128 Unplanned or Unexpected Discharges Who can complete the DC OASIS? Last qualified clinician (Not a LPN, PTA, COTA) that visited the patient should complete the DC comprehensive assessment Complete the OASIS based on patient s status and information available at the time of the last qualified clinician s visit What if the last qualified clinician is no longer available? DC matches the SOC or Do not complete the DC OASIS (CoP problem) How do you show that you completed the OASIS without a visit? ( based on visit of mm/dd/yyyy ) A supervisor in the office cannot create an assessment as if it were fact without seeing the patient. 2-Q37
33 129 Unplanned Discharge Do not include the reporting of any health status changes or service utilization that occurred after the date of the last qualified clinician s visit EXCEPT for completion of M2401 Intervention Synopsis, where the discharge OASIS can report any ordered interventions that were implemented up until the time of discharge (the M0906 date). This includes taking credit for education provided at a home visit by an LPN or therapy assistant. April Unplanned or Unexpected Discharge M0903 Date of last (most recent) home visit Date of the most recent visit by agency staff Last visit by any agency staff even if visit was not included on the POC M0906 Discharge date Determined by agency policy Can t be before last visit M0090 Date assessment completed Actual date agency completed assessment 131 Unplanned or Unexpected Discharges Mr. Shelton s daughter came to visit him and decided he can no longer live alone. She took him to live with her outside your service area, called agency to let you know Monday 7/27. The last visit to the patient was by a PTA on 7/23, last visit by qualified clinician was an RN on 7/12. RN did the DC OASIS paperwork on 7/27. Include the ER visit that occurred on 7/20? Consider all the teaching about heart failure symptoms that occurred after 7/12? Date of last visit? Date of discharge? 132 Last Qualified Clinician s Visit Events past this point are not included in DC assessment, but visits are still billable. Past 14 days starts here. Example Teaching Re: Heart Failure by LPN ER trip Teaching and Interventions included in M2401 Discharge M0090 Count as a Yes on M2401
34 133 Quiz: Which sequences of assessments are correct? SOC, with only one visit performed SOC, FU, Transfer, Discharge SOC, FU, FU, FU, DC SOC, FU, Transfer SOC, ROC, FU, DC 134 OASIS Conventions One Clinician Rule New in 2018 Manual Update 135 Collaboration is allowed on selected items, however only one clinician may complete the assessment If two clinicians are seeing the patient at the same time: May confer about interpretation of the assessment data Clinician performing the assessment follows up on any observations of patient status reported by other staff Clerical staff may complete demographic and agency ID items assessing clinician verifies 136 Agencies may have the comprehensive assessment completed by one clinician. If collaboration with other health care personnel and/or agency staff is utilized, the agency is responsible for establishing policies and practices related to collaborative efforts, including how assessment information from multiple clinicians will be documented within the clinical record, ensuring compliance with applicable requirements, and accepted standards of practice.
35 Conventions Conventions 137 Understand the time period under consideration for each item. Report what is true on the day of assessment unless a different time period has been indicated in the item or related guidance. Day of assessment is defined as the 24 hours immediately preceding the home visit and the time spent by the clinician in the home. For OASIS purposes, a care episode (also referred to as a quality episode) must have a beginning (that is, an SOC or ROC assessment) and a conclusion (that is, a Transfer or Discharge assessment) to be considered a complete care episode. 138 If the patient s ability or status varies on the day of the assessment, report the patient s usual status or what is true greater than 50% of the assessment time frame, unless the item specifies differently (for example, for M2020 Management of Oral Medications, M2030 Management of Injectable Medications, and M2100e Management of Equipment, instead of usual status or greater than 50% of the time, consider the medication or equipment for which the most assistance is needed). Not the average ability over a time period Minimize the use of NA and Unknown responses. New Convention Conventions 139 Some items allow a dash response M1028, M1060, M1313, GG0170C, M2001, M2003, M2005 A dash ( ) value indicates that no information is available, and/or an item could not be assessed. This most often occurs when the patient is unexpectedly transferred, discharged or dies before assessment of the item could be completed. CMS expects dash use to be a rare occurrence. 140 Responses to items documenting a patient s current status should be based on independent observation of the patient s condition and ability at the time of the assessment without referring back to prior assessments. Several process items require documentation of prior care, at the time of or since the time of the most recent SOC or ROC OASIS assessment. These instructions are included in item guidance for the relevant OASIS questions.
36 Conventions Conventions Combine observation, interview, and other relevant strategies to complete OASIS data items as needed (for example, it is acceptable to review the hospital discharge summary to identify inpatient procedures and diagnoses at Start of Care, or to examine the care notes to determine if a physician ordered intervention was implemented at Transfer or Discharge). However, when assessing physiologic or functional health status, direct observation is the preferred strategy. Complete OASIS items accurately and comprehensively, and adhere to skip patterns. Understand the definitions of words as used in the OASIS. Follow rules included in the Item Specific Guidance Stay current with evolving CMS OASIS guidance updates. CMS may post updates up to twice per year, in June and December, and quarterly Q&A s Conventions M0150 Current Payment Sources 143 Same day means by the end of the same day. When an OASIS item refers to assistance, this means assistance from another person unless otherwise specified within the item. Assistance is not limited to physical contact and includes both verbal cues and supervision. By midnight of the next calendar day has replaced one calendar day 144 OASIS is collected and transmitted for all adult Medicare or Medicaid patients (age 18 or over) receiving skilled health services from the HHA, except for patients receiving care for pre- and post-partum conditions. 1-Q1

37 145 M0150 Identifying payers to which any services provided during this home care episode and included on the Plan of Care will be billed by your home health agency. No pending payers Do not consider any equipment, medications, or supplies being paid for by the patient, in part or in full. 146 M0102 Date of Physician ordered SOC (ROC) Timepoints: Start of care, Resumption of care Specifies the date that home care services are ordered to begin, if the date was specified by the physician. The item refers to the order to start home care services (that is, provide the first covered service), regardless of the type of services ordered (for example, therapy only). 147 M0102 Date of Physician ordered SOC (ROC) 148 M0102 Date of Physician ordered SOC (ROC) If the originally ordered start of care is delayed due to the patient s condition or physician request (for example, extended hospitalization), then the date specified on the updated/revised order to start home care services would be considered the date of physician-ordered start of care (resumption of care). Because the State Operations Manual requires a visit within 48 hours of resumption of care following hospitalization, mark "N/A" if the physician orders a ROC date that extends beyond 2 calendar days of the inpatient facility discharge. New CoPs? In order to be considered a physicianordered SOC date, the physician must give a specific date to initiate care, not a range of dates. If a single date to initiate services is not provided, the initial assessment visit must be conducted within 48 hours of the referral or within 48 hours of the patient's return home from the inpatient facility.
38 M0104 Date of Referral M0104 Date of Referral If start of care is delayed due to the patient s condition or physician request (for example, extended hospitalization), then the date the agency received updated/revised referral information for home care services to begin would be considered the date of referral. This does not refer to calls or documentation from others such as assisted living facility staff or family who contact the agency to prepare the agency for possible admission. The date authorization was received from the patient's payer is NOT the date of the referral (for example, the date the Medicare Advantage case manager authorized service is not considered a referral date). Timepoints: SOC, ROC Specifies the referral date, which is the most recent date that verbal, written, or electronic authorization to begin home care was received by the home health agency. M0102 and M0104 for Late F2F M0104 Date of Referral 151 When a new Start of Care date is established based on the completion of a late face-to-face encounter for Medicare eligibility, report: M0102 Date of Physician-ordered SOC as NA M0104 Date of Referral as the day prior to the new Start of Care date January When an agency receives an initial "referral" or contact about a patient who needs service, the HHA must ensure this physician, or another physician will provide for the plan of care and ongoing orders. If a physician is willing to follow the patient, and provides adequate information (name, address/contact info, and diagnosis and/or general home care needs) regarding the patient, this is considered a valid referral. In cases where the referring physician is not going to provide orders and follow the patient, this is not a valid referral" for M rd Q 2014

39 M0104 Date of Referral M1000 Inpatient Facilities 153 In the example of a hospitalist who will not be providing an ongoing plan of care for the patient, the HHA must contact an alternate, or attending physician, and upon agreement from this following physician, for referral and/or further orders, the HHA will note this as the Referral date in M0104 (unless referral details are later updated or revised). If a general order to Evaluate for Home Care services (no discipline(s) specified) is received from a physician who will be following the patient, this constitutes a valid order, and per CoPs the RN must conduct the initial assessment visit to determine immediate care and support needs and eligibility for the Home Health benefit for Medicare patients. 3rd Q The purpose of this item is to establish the patient s recent health care history before formulating the Plan of Care. The amount and types of rehabilitation treatment the patient has received and the type of institution that delivered the treatment are important to know when developing the home health Plan of Care. Provides risk adjustment on several outcome and utilization measures. M1000 Inpatient Facilities M1011 Inpatient Diagnosis 155 SOC ROC The term past 14 days is the two-week period immediately preceding the start/resumption of care. This means that for purposes of counting the 14-day period, the date of admission is day 0 and the day immediately prior to the date of admission is day 1. Discharges on Day 0 should be included. Consider any inpatient stays with discharge dates within the 2 week period. Short-stay acute hospital (response 3) applies to most hospitalizations 156 Actively treated should be defined as receiving something more than the regularly scheduled medications and treatments necessary to maintain or treat an existing condition. No surgical codes. List the underlying diagnosis that was surgically treated. If a joint replacement was done for osteoarthritis, list the disease, not the procedure. No V, W, X, Y, or Z codes. List the underlying diagnosis.
40 SOC ROC FU M1011 Inpatient Diagnosis M The term past 14 days is the two-week period immediately preceding the Start/Resumption of Care date (or for Follow-Up, the M0090 Date Assessment Completed). This means that for purposes of counting the 14-day period, the date of Start of Care date is day 0 and the day immediately prior to the Start of Care date is day 1. If a diagnosis was not treated during an inpatient admission, it should not be listed. A diagnosis reported in M1011 Inpatient Diagnosis may also be reported in M1017 if within the 14 days prior to the SOC/ROC date the condition was new or exacerbated, required changes in the treatment regimen, AND the patient was discharged from an inpatient facility where the condition was actively treated. 159 M1017 Diagnoses Requiring Change Identifies if any change has occurred to the patient s treatment regimen, health care services, or medications within the past 14 days. Identify the patient s recent history by identifying new diagnoses or diagnoses that have exacerbated over the past 2 weeks. New onset of CHF 12 days ago, improved with treatment Mark "NA" if changes in the medical or treatment regimen were made because a diagnosis improved. UTI diagnosed 3 weeks ago, treated, improved and resolved Do not list resolved conditions 160 M1017 Diagnoses Requiring Change The intent of the item is not to identify diagnoses where all medical or treatment regimen changes in the last 14 days were related to improvement in a condition. If at any time in the last 14 days the patient requires a medical or treatment regimen change due to development of a new condition or lack of improvement or worsening of an existing condition, the diagnosis should be reported in M1017, even if the condition also showed improvement or stabilization during that time, or is improved at the time of SOC/ROC. 4bQ41.1


.")
41 1. Complete assessment 2. Plan Care 3. Describe pt with diagnoses in column 1 4. Codes added in column M1021 /M1023 Must comply with ICD-10-CM Conventions and Guidelines Primary diagnosis is the focus of home care services. When determining secondary diagnoses, consider coexisting conditions that are actively addressed in the Plan of Care as well as diagnoses that affect the patient s responsiveness to treatment and rehabilitative prognosis, even if the condition is not the focus of any home health treatment itself. The secondary diagnoses may or may not be related to a patient s recent hospital stay, but must have the potential to impact the skilled services provided by the HHA. 161 M1021 /M1023 M1021/1023 Diagnoses 163 All diagnoses must be documented in the medical record or referral information by the provider (physician or designee). If not, must be verified with provider document the confirmation. Diagnoses may change during the course of the home health stay due to a change in the patient s health status or a change in the focus of home health care. At each required OASIS time point, the clinician must assess the patient s clinical status and determine the primary and secondary diagnoses based on patient status and treatment plan at the time of the assessment. 164 The order that secondary diagnoses are listed should be determined by the degree that they impact the patient s health and need for home health care, rather than the degree of symptom control. For example, if a patient is receiving home health care for Type 2 diabetes that is controlled with difficulty, this diagnosis would be listed above a diagnosis of a fungal infection of a toenail that is receiving treatment, even if the fungal infection is poorly controlled.
.")

42 165 Data Sources Patient/caregiver interview Physician Physician orders Referral information Current medication list Effective October 1, 2016 the current ICD-10-CM List of Codes and Descriptions and the ICD-10-CM Official Guidelines for Coding and Reporting should be the source for coding (see Chapter 5 for link). For degree of symptom control, data sources may include patient/caregiver interview, physician, physical assessment, and review of past health history. M1028 Active Diagnoses This item identifies whether two specific diagnoses are present, and active. These diagnoses influence a patient's functional outcomes or increase a patient's risk for development or worsening of pressure ulcer(s). - means unable to assess Leave blank if the patient doesn t have either diagnosis Applicable Codes Coding Convention When diabetes and PVD/PAD are documented as diagnoses and no other cause is documented for the PVD/PAD, the classification assumes diabetes as the cause. So if the patient has Type 2 diabetes and also has PVD, it is coded as E11.51 Type 2 DM with peripheral angiopathy. Do NOT add a code from I73. Because the patient has both diagnoses documented, should both 1 and 2 be checked on M1028, even though no I70 or I73 is used?
 and no I-code is included? Yes.")
43 Diabetic PVD Steps for Assessment When a patient has diabetic peripheral vascular disease (PVD) or peripheral artery disease (PAD), should both items checked (as yes) even though these are combination codes (E-codes) and no I-code is included? Yes. If a diabetic patient has either PAD or PVD, both the diabetes mellitus item (2) and the PAD/PVD (1) items are checked in item M1028, Active Diagnoses 170 Transfer documents, Progress notes H&P DC Summary Step 1Identify Diagnosis Step 2 Determine if Diagnosis is Active Documentation states dx is active OR Active intervention Documentation Required M1028 Is the diagnosis active? Physician Item requires documentation in the medical record by: Nurse Practitioner Physician Assistant Clinical Nurse Specialist Other Authorized Licensed Staff, If Allowable Under State Licensure Laws Active diagnoses are diagnoses that have a direct relationship to the patient s current functional, cognitive, mood or behavior status; medical treatments; nurse monitoring; or risk of death at the time of assessment. Not resolved


44 173 Diagnosis during the timeframe Example Patient s admitting diagnosis is prediabetes. The assessing clinician finishes the assessment on the second day after SOC. On the 4 th day the PA calls and states further tests indicate patient has a diagnosis of diabetes and provides orders. The assessment should be updated and the M0090 date changed. This is only true if new information is obtained within the assessment time frame. 174 Practice Scenario Mr. B has Type 2 Diabetes Mellitus (DM) and takes metformin and glypizide daily. His healthcare regimen also includes regular blood glucose monitoring, exercise, and a diabetic diet. The physician progress note documents an active diagnosis of both DM with peripheral neuropathy and Peripheral Vascular Disease (PVD). How would you answer M1028? 4b Q46.3 Practice Scenario SOC ROC M1030 Therapies $ FU 175 Mr. J is admitted to home care services after surgery for a left total knee replacement. His medical record documents current active diagnoses of asthma and arthritis. How should the admitting clinician complete M1028? a. 1 b. Dash c. Leave blank 176 Identifies whether the patient is receiving intravenous, parenteral nutrition, or enteral nutrition therapy at home, whether or not the home health agency is administering the therapy. This item is not intended to identify therapies administered in outpatient facilities or by any provider outside the home setting.
, mark the applicable therapy.")
 hemodialysis or")
45 177 M1030 Therapies If the patient will receive such therapy as a result of this SOC/ROC or follow-up assessment (for example, the IV will be started at this visit or a specified subsequent visit; the physician will be contacted for an enteral nutrition order; etc.), mark the applicable therapy. Counts as IV/infusion therapy (response 1): intermittent medications or fluids via an IV line (including heparin or saline flushes). ongoing infusion therapy is being administered at home via central line, subcutaneous infusion, epidural infusion, intrathecal infusion, or insulin pump (Including implanted pumps) hemodialysis or peritoneal dialysis in the home 178 M1030 Therapies Does not count as IV/infusion therapy: IV catheter is present but not active (for example, site is observed only or dressing changes are provided) orders for an IV infusion to be given when specific parameters are present (for example, weight gain), but those parameters are not met on the day of the assessment. An irrigation or infusion of the bladder Flushing of a biliary tube with normal saline (January 2016) Enteral Nutrition (Response 3) if any enteral nutrition is provided. Does not count as Enteral nutrition Not currently used for nutrition, Water, medications or flush of a feeding tube Parenteral therapy (response 2) Triple lumen with TPN/lipids infusing in one port and flushing other Responses 1 and 2 Single lumen utilized for TPN with pre and post flush Response 2 only 179 M1041/M M1041 Influenza Vaccine TRN DC A care episode is one that includes both SOC/ROC and Transfer/Discharge. If no part of the care episode (from SOC/ROC to Transfer or Discharge) occurred during the time period from October 1 and March 31, mark No. Identifies whether the patient was receiving services from the home health agency during the time period for which influenza vaccine data are collected (October 1 and March 31).
46 181 M1046 Influenza Vaccine Received For a patient with any part of the home health episode (SOC/ROC to Transfer/Discharge) occurring between October 1 and March 31, identifies whether the patient received an influenza vaccine for this year s flu season, and if not, the reason why. This item meets National Quality Forum (NQF) standards for harmonization of influenza measures across care settings. Response 1 if your agency provided the influenza vaccine to the patient during this episode of care (SOC/ROC to Transfer/Discharge). Response 2 -your agency provided the flu vaccine for this year s flu season prior to this home health episode current patient given a flu vaccine by your agency during a previous roster billing situation during this year s flu season. 182 M1046 Influenza Vaccine Received Response 3 if patient/caregiver reports (or there is documentation in the clinical record) that patient received influenza vaccine for the current flu season from another provider. The provider can be the patient s physician, clinic, or health fair providing influenza vaccines Responses 1 or 2 or 3 may be selected even if the flu vaccine for this year s influenza season was provided prior to October 1 (that is, flu vaccine was made available early). Response 4 if the patient and/or healthcare proxy (for example, someone with power of attorney) refused the vaccine. Note: It is not required that the agency offered the vaccine. Select Response 4 only if the patient was offered the vaccine and he/she refused. Response 5 if the influenza vaccine is contraindicated for medical reasons. Medical contraindications include anaphylactic hypersensitivity to eggs or other component(s) of the vaccine, history of Guillain-Barre Syndrome within 6 weeks after a previous influenza vaccination, or bone marrow transplant within 6 months or other physician medical restriction. 183 M1046 Influenza Vaccine Received Response 6 if age/condition guidelines indicate that influenza vaccine is not indicated for this patient. Age/condition guidelines are updated as needed by the CDC. Detailed information regarding current influenza age/condition guidelines is posted to the CDC website (see link in Chapter 5). It is the agency s responsibility to make current guidelines available to clinicians. Response 7 if the vaccine is unavailable due to a CDC-declared shortage. Response 8 only if the patient did not receive the vaccine due to a reason other than Responses Example Patient admitted to HH on Sept 13 and given the vaccine on September 17. You are now discharging on December 10. Admit Sept 13 Vaccine October 1 DC Dec 10
 of Sept. 30th, but the date the Transfer OASIS was completed (M0090) was Oct. 2 nd. 4bQ62.2.2. Oct. 1 SOC Jan.")

47 Example Patient admitted to home care on January 2. The flu season is bad this year and is lingering on. He is given the flu vaccine on April 2. You are discharging from HH in July. 186 Example Flu vaccine given on Sept. 15th and there was a Transfer date (M0906) of Sept. 30th, but the date the Transfer OASIS was completed (M0090) was Oct. 2 nd. 4bQ Oct. 1 SOC Jan. 2 Vaccine April 2 DC July 187 More than one flu season in the episode If a patient's quality episode overlaps more than one influenza season, M1046 should be answered based on whether or not the agency gave the influenza vaccine for the current flu season. Admit Jan 1 Flu shot Jan 5 DC Oct 10 SOC ROC M1060 Height and Weight Self-report or paperwork from another setting is not acceptable 4bQ62.9 Use mathematical rounding Admit Jan 1 Flu shot Oct 2 DC Oct 10
48 189 M1060 These items support calculation of the patient s body mass index (BMI) using the patient s height and weight. Item Rationale Diminished nutritional and hydration status can lead to debility that can adversely affect wound healing and increase risk for the development of pressure ulcers. Height and weight measurements (and BMI calculation) assist staff in assessing the patient s nutrition and hydration status by providing a mechanism for monitoring stability of weight and BMI over a period of time. The measurement of height and weight for the calculation of BMI is one guide for determining nutritional status. Weight measurement is also used in assessment of heart failure. Policies and Procedures for Height and Weight Height Measuring height of bedbound and chairbound patients Contractured patients Weight Scales for admissions and ROC Patient scales Calibration May not be able to weight patients who cannot stand: Dash What is the answer? What is the answer? 191 Mrs. G has congestive heart failure and advanced osteoporosis. She is at risk for pathological fractures. She is pain free at rest but experiences severe pain when she moves. Daily weights have been discontinued as part of her prescribed medical care due to pain management. What can be done for best practices and what is the answer to M1060? 192 As part of the SOC comprehensive assessment, the registered nurse (R.N.) needs to obtain a height for Mr. B. who has had bilateral lower extremity amputations due to complications from diabetes. His legs are now uneven in length. Using a tape measure, the R.N. measures the patient s current height while the patient is lying in bed. She obtains two measurements: 64.4 inches and 60.8 inches. Answer M1060a Dash (the patient is unable to stand)
.")

49 SOC ROC M1100 Patient Living Situation M1100 Patient Living Situation Using the care provider s professional judgment, determine: First, determine living arrangement whether the patient lives alone, in a home with others, or in a congregate setting (usual status). Second, determine availability of assistance how frequently caregiver(s) are in the home and available to provide assistance if needed. If the patient has recently changed their living arrangement due to their condition, report the usual living arrangement prior to the illness, injury or exacerbation for which the patient is receiving care unless the new living arrangement is expected to be permanent. M1100 Patient Living Situation M1100 Patient Living Situation 195 Row a -- the patient lives alone in an independent (non-assisted) setting. For example, the patient lives alone in a home, in their own apartment, or in their own room at a boarding house. A patient with only live-in paid help is considered to be living alone. A patient who normally lives alone but temporarily has a caregiver staying in the home to provide assistance is considered to be living alone. A patient who lives alone but can obtain emergency help by phone or life-line, is still living alone. 196 Row b -- the patient lives with others in an independent (non-assisted) setting. For example, the patient lives with a spouse, family member or another significant other in an independent (nonassisted) setting. A patient who normally lives with others but is occasionally alone because caregiver(s) are traveling out of town is still considered to be living with others. Lives with family paid to provide care
50 M1100 Patient Living Situation M1100 Patient Living Situation 197 Row c -- the patient lives in an assisted living setting (assistance, supervision and/or oversight are provided as part of the living arrangement). For example, the patient lives alone or with a spouse or partner in an apartment or room that is part of an assisted living facility, residential care home, or personal care home. 198 Around the clock means there is someone available in the home to provide assistance to the patient 24 hours a day. Regular daytime means someone is in the home and available to provide assistance during daytime hours every day with infrequent exceptions. Regular nighttime means someone is in the home and available to provide assistance during nighttime hours every night with infrequent exceptions. Occasional/short-term assistance means someone is available to provide in-person assistance only for a few hours a day or on an irregular basis, or may be only able to help occasionally. No assistance available means there is no one available to provide any in-person assistance. M1100 Tips M1100 Examples 199 In-person assistance provided in the home of the patient. Not limited to ADLs and IADLs. If a person is in an assisted living or congregate setting with a call-bell that summons help, this is considered in-person assistance. Assistance via telephone is not included Use your professional judgment to determine if someone will be available to provide any assistance to the patient. If a person is living in the patient s home but is completely unable to or unwilling to provide any assistance to the patient, do not count them as a caregiver. Availability of assistance refers to the expected availability and willingness of caregiver(s) for this upcoming care episode. 200 Patient lives alone in her own apartment. Since her discharge from the hospital, her two daughters alternate staying with her during the day and night so that one of them is always there, except for the times when one goes out to run an errand or pick up a child at day care. Response = 01 (Patient still considered to be living alone, since daughters are only staying there temporarily. Daughters are providing round-the-clock care, even if one occasionally needs to be out of the house for brief periods.) Patient lives alone in her home but her son and daughterin-law live across the street. They bring the patient dinner every night and are available around the clock by telephone. Response = 04 (Son and daughter-in-law are not there to provide in-person assistance consistently, day or evening, even if they live across the street and are available by phone.)


51 M1100 Examples M1100 Examples 201 Patient lives with her daughter who works during the day but is home every evening and sleeps there every night. A paid aide comes in 3 days a week to assist with ADLs. Daughter has back problems that prevent her from lifting patient, but she assists the patient with dressing every morning and takes the patient to doctor s appointments. Response = 08 (Patient lives in a home with others who are available every night to offer in-person assistance. Even if the daughter can t meet all of patient s needs, she is available all night.) 202 Patient lives with her husband who has significant cognitive and functional impairments, is wheelchair bound, and is unable to provide the patient with any assistance. A member of the church comes by one evening a week and brings groceries. Response = 09 (Patient lives in a home with another person who is there 24 hours but is unavailable to provide assistance. Caregiver from church provides occasional assistance.) Patient lives alone in an apartment that is part of an ALF. The apartment does not have a call-bell but her contract with the ALF includes having a home health aide assist her with ADLs 2 hours every morning. Her son also comes over occasionally to assist with bills, groceries, and errands. Response = 14 (Patient is living in a congregate setting; one caregiver is available to assist for some part of every day on a regular basis, but not all day, another caregiver offers occasional assistance.) M1200 Vision M1200 Vision SOC ROC FU A magnifying glass (as might be used to read newsprint) is not an example of corrective lenses. Neither is an adaptive reader. Reading glasses (including "grocery store" reading glasses) are considered to be corrective lenses. Assessment strategies: In the health history interview, ask the patient about vision problems (for example, cataracts) and whether or not the patient uses glasses. Observe ability to locate signature line on consent form, to count fingers at arm s length and ability to differentiate between medications, especially if medications are self-administered. Be sensitive to requests to read, as patient may not be able to read though vision is adequate. Hard cervical collar; orbital swelling; blind in one eye: assess impact on functional vision. 4b-A64.1.



52 Newsprint Impaired Vision 205 Newsprint is intended to serve as an example of the size and type of print found in a newspaper, magazine or book, on medication or food labels, and on other products or documents that might be routinely encountered for day-to-day functioning. Rather than focusing on specific font sizes, the clinician should use clinical judgment to select the response to M1200 that best represents the patient s vision status, as it relates to managing in their home environment safely. Functional vision may involve assessing the patient s ability to read the label, identify colored medication bottle caps, differentiate medications based on pill size, color or shape and/or the use of other visual cues to carry out the daily activity of medication identification. April 2016 Q and A 206 Miss Turtle has severe kyphosis and limited neck mobility and cannot adequately see objects in her path creating a safety issue on ambulation. She can read med labels and newsprint. Is she considered to have partially (1) or severely (2) impaired vision? When selecting the correct response for M1200 Vision, the clinician is assessing the patient s functional vision, not conducting a formal vision acuity screen or distance vision exam to determine if the patient has 20/20 vision. Therefore physical deficits or impairments that limit the patient s ability to use their existing vision in a functional way would be considered. If physical deficit/impairments (like limited neck range of motion) prevent a patient from seeing objects in his path, affecting safe function in his environment, M1200 should be 2 severely impaired vision. M1210 Ability to Hear 208 Hearing spoken language and other sounds, e.g. alarms Hearing is evaluated with the patient wearing hearing aids or devices if he/she usually uses them. If evaluating ability to hear with hearing aids, be sure that the devices are in place, turned on, and that the hearing aids are working (for example, batteries are functional). UK response if the patient is not able to respond or if the patient s condition makes it impossible to assess hearing (for example, severe dementia, schizophrenia, unconscious).

53 209 M1220 Understanding of Verbal Content Identifies the patient s functional ability to comprehend spoken words and instructions in the patient s primary language. Both hearing and cognitive abilities may impact a patient's ability to understand verbal content. The UK response should be selected if the patient is not able to respond or if it is otherwise impossible to assess understanding of spoken words. For patients whose primary language differs from the clinician s, an interpreter may be necessary. If a patient can comprehend lip reading, they have the ability to understand verbal content, even if they are deaf. 210 M1230 Speech and Oral (Verbal) Expression of Language Identifies the patient s physical and cognitive ability to communicate with words in the patient s primary language. Does not address communicating in sign language, in writing, or by any nonverbal means. Augmented speech (for example, a trained esophageal speaker, use of an electrolarynx) is considered verbal expression of language. Presence of a tracheostomy requires further evaluation of the patient s ability to speak. Can the trach be covered to allow speech? If so, to what extent can the patient express him/herself? Response 5 for a patient who communicates entirely nonverbally (for example, by sign language or writing) or is unable to speak. Nonresponsive means that the patient is not able to respond. SOC ROC M1240 Formal Pain Assessment Responses No standardized, 0 0 no validated assessment conducted 1 Yes, and it does not indicate severe pain 2 Yes, and it indicates severe pain If the standardized, validated tool does not define levels of "severe" pain, then the agency or care provider should use the level(s) of pain identified in the tool that best reflect the concept of "severe." Not an appropriate tool for patient Did the assessment late Just didn t do it Appropriate tool was used correctly, according to protocol AND level of pain does not reach level of severe Appropriate tool was used correctly, according to protocol AND level of pain does reach level of severe
54 M1240 Timeframe Example 213 Timeframe is determined by the administration protocols associated with the exact standardized, validated tool that the clinician uses to assess pain. Examples of time frames stated in protocols include at the present time, and at its worst during the past 24 hours. If the tool selected has multiple sets of validated administration protocols, in order to standardize data collection agency policy may state which protocol the agency prefers the clinicians use. 214 The patient s present pain level is 3 but reports that this morning when she had to climb the stairs it was an 8. The agency s standardized, validated pain assessment tool rates the highest level in the past 24 hours. What is the response? 215 SOC ROC FU M1242 Frequency of Pain Interfering with Movement 216 M1242 Frequency of Pain Interfering with Movement Include all activities (for example, sleeping, recreational activities, watching television), not just ADLs. The presence of medication for pain or joint disease provides an opportunity to explore the presence of pain, when the pain is the most severe, activities with which the pain interferes, and the frequency of this interference with activity or movement. Be careful not to overlook seemingly unimportant activities (for example, the patient says she/he sits in the chair all day and puts off going to the bathroom, because it hurts so much to get up from the chair or to walk).
, monitoring heart rate, respiratory rate, perspiration, pallor, pupil size,")
55 217 M1242 Frequency of Pain Interfering with Movement Evaluating the patient s ability to perform ADLs and IADLs can provide additional information about such pain. Assessing pain in a nonverbal patient involves observation of facial expression (for example, frowning, gritting teeth), monitoring heart rate, respiratory rate, perspiration, pallor, pupil size, irritability, or use of visual pain scales (for example, FACES). The patient s treatment for pain (whether pharmacologic or nonpharmacologic) must be considered when evaluating whether pain interferes with activity or movement. Pain that is well controlled with treatment may not interfere with activity or movement at all All of the Time All of the time" means constantly throughout the day and night with little or no relief. Pain is also considered to be interfering if a patient stops performing an activity in order to avoid the pain. For the pain to be interfering "all the time" the frequency of the activity that was stopped in order to avoid pain must collectively represent all the hours of the day/night. Pain must wake them frequently at night. The clinician must use judgment based on observation and patient interview to determine if pain is interfering all the time. July 2013 Example 219 Your patient reports that her pain doesn t bother her as long as she moves slowly and doesn t sit in the same position for long. Once she takes her sleeping medication at night, she rests well. 220 Integumentary M1300s


56 Pressure Ulcer Defined Basics Regarding Pressure Ulcers A localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure. NPUAP Localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure, or pressure in combination with shear and/or friction. (CMS) NOT pressure ulcers: Serum filled blisters that are caused by shoes rubbing against the foot If the cause of a wound is solely a friction force which leads to visible skin impairment, such as the serum filled blister cited in the scenario, it would NOT be categorized as a pressure ulcer. The 2009 International NPUAP-EPUAP Pressure Ulcer Prevention and Treatment Clinical Practice Guideline eliminated reference to friction as a factor in pressure ulcer development. (January 2016) Does not include mucosal pressure ulcers 4bQ In 2004, based on advances in wound care research and the opinion of the National Pressure Ulcer Advisory Panel (NPUAP), it was determined that stage 1 and stage 2 (partial thickness) pressure ulcers can heal through the process of regeneration of the epidermis across a wound surface, known as epithelialization. Stage 3 and 4 (full thickness) pressure ulcers heal through a process of contraction, granulation, and epithelialization. They can never be considered "fully healed" but they can be considered closed when they are fully granulated and the wound surface is covered with new epithelial tissue. 223 What s New In OASIS C2? SOC ROC 224 M1300 Pressure Ulcer Assessment/ M1302 Risk NPUAP updated terminology for staging (Pressure ulcer became pressure injury) Home health agencies may adopt the NPUAP guidelines in their clinical practice and documentation. However, since CMS has adapted the NPUAP guidelines for OASIS purposes, the definitions do not perfectly align with each stage as described by NPUAP. When discrepancies exist between the NPUAP definitions and the OASIS scoring instructions provided in the OASIS Guidance Manual and CMS Q&As, providers should rely on the CMS OASIS instructions. Exception to the use of a standardized validated tool What constitutes risk?

.")
57 225 M1300 Pressure Ulcer Assessment DC 226 M1307 The Oldest Stage 2 Pressure Ulcer One clinician rule Within the timeframe Standardized validated tool plus clinical factors = response 2 Either the clinical factors or the standardized tool is checked Yes on M1302 if risk is identified T Response 1 if the oldest stage 2 pressure ulcer was already present when the SOC/ROC assessment was completed. Response 2 if the oldest stage 2 pressure ulcer was first identified since the most recent SOC/ROC visit (that is, since the last time the patient was admitted to home care or had a resumption of care after an inpatient stay). Enter onset date 227 M1307 The Oldest Stage 2 Pressure Ulcer Response NA if the patient has no stage 2 pressure ulcers at the time of discharge, or all stage 2 pressure ulcers have healed. SOC ROC FU DC 228 M1306 An ulcer that is suspected of being a stage 2, but is Unstageable, should not be identified as the oldest stage 2 pressure ulcer. For this item, Unstageable refers to pressure ulcers that are known to be present or that the care provider suspects may be present based on clinical assessment findings (for example, patient report of discomfort, past history of skin breakdown in the same area), but that are unobservable due to dressings or devices (for example, casts) that cannot be removed to assess the skin underneath. Yes Stage 2 or higher and unstageables No Stage 1 and all healed ulcers
58 New in OASIS C2 M Stage 3 and 4 (full thickness) pressure ulcers heal through a process of granulation (filling of the wound with connective/scar tissue), contraction (wound margins contract and pull together), and reepithelialization (covers with epithelial tissue from within wound bed and/or from wound margins). Once the pressure ulcer has fully granulated and the wound surface is completely covered with new epithelial tissue, the wound is considered closed, and will continue to remodel and increase in tensile strength. For the purposes of scoring the OASIS, the wound is considered healed at this point, and should no longer be reported as an unhealed pressure ulcer. 230 Agencies should be aware that the patient is at higher risk of having the site of a closed pressure ulcer open up due to damage, injury, or pressure, because of the loss of tensile strength of the overlying tissue. Tensile strength of the skin overlying a closed full thickness pressure ulcer is only 80% of normal skin tensile strength. Agencies should pay careful attention that preventative measures are put into place that will mitigate the re-opening of a closed ulcer. Implications M Closed stage 3 and stage 4 pressure ulcers will no longer provide points. Not the code, but how you answer the OASIS items. Closed stage 3 and stage 4 pressure ulcers do require skilled intervention. Assessment M2250 Prevention 232 Mr. Ross has been on service before and it took several months to heal up his stage 4 ulcer. Mr. Ross is being admitted back to your agency. The assessing clinician notes the shiny pink divot on the right hip. Only ulcer is a closed stage 4 then answer to M1306 is NO. (Note skip pattern.) OASIS response no pressure ulcer Clinical documentation epithelialized stage 4 ulcer located at M1350 Yes (skin lesion requiring ongoing assessment/intervention) Code according to stage? Up to you
59 Continue to code them? M1306 Synopsis 234 Guidance to not include them as pressure ulcers applies to the OASIS responses Section III of the official coding guidelines For reporting purposes the definition for other diagnoses is interpreted as additional conditions that affect patient care in terms of requiring: clinical evaluation; or therapeutic treatment; or diagnostic procedures; or extended length of hospital stay; or increased nursing care and/or monitoring. NO Stage 1 pressure ulcers. Healed Stage 2 pressure ulcers (once epithelialized no longer considered a pressure ulcer) Healed Stage 3 pressure ulcers (healed for the purposes of scoring OASIS continue to be at risk) Healed Stage 4 pressure ulcers (healed for the purposes of scoring OASIS continue to be at risk) YES Stage 2 pressure ulcers Stage 3 Unhealed Stage 4 Unhealed Unstageable presence of non-removable dressing/device presence of necrotic tissue that obscures visualization of stage 4 structures (bone, muscle, tendon or joint capsule) presence of eschar/slough Suspected deep tissue injury in evolution Stage Staging for the Purposes of OASIS 236 Red, pink wound bed No granulation Without slough No bruising Intact or open/ruptu red blister NOT solely from friction




60 Stage 2 Pressure Ulcer Stage A stage 2 ulcer also may present as a shiny or dry shallow ulcer without slough or bruising.* This stage should not be used to describe skin tears, tape burns, perineal dermatitis, maceration, or excoriation. * Bruising indicates suspected deep tissue injury. Bone, tendon or muscle is NOT exposed Slough may be present Undermining and tunneling may be present Granulation indicates healing Stage 3 Pressure Ulcer Stage 3 on Ankle The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue; stage 3 ulcers in these locations can be shallow. In contrast, areas of significant adiposity can develop extremely deep stage 3 pressure ulcers. Bone/tendon is not visible or directly palpable.

61 Stage 4 Stage 4 Pressure Ulcer Exposed bone or eschar May be slough or eschar present, but not obstructing wound bed Undermining or tunneling Granulation indicates healing Osteomye litis does not equate The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue; stage 4 ulcers in these locations can be shallow. stage 4 ulcers can extend into muscle and/or supporting structures (eg, fascia, tendon, or joint capsule); osteomyelitis is possible. Exposed bone/tendon is visible or directly palpable. Stage 4 Staging Tips Unstageable 243 Exposed bone, tendon or muscle Granulation and no exposed bone, tendon or muscle Slough or eschar Still a stage 4 Slough or eschar without exposed bone, tendon or muscle Stage based on previous documentation Unstageable (even if previously staged) 244 Known or likely but not stageable due to nonremovable dressing or device Includes those that are sutured Includes those with skin grafts that edges haven t healed yet (BUT NOT with OASIS-C2) Known or likely but not stageable due to coverage of wound bed by slough and/or eschar (no stage 4 structures can be visualized) Scab obscuring tissue loss. July 2013 Suspected deep tissue injury in evolution.


62 245 Unstageable: Non removable dressing 246 Unstageable: Eschar Slough Non-removable dressing/device includes, for example, a primary surgical dressing that cannot be removed, an orthopedic device, or cast. Include those that are sutured Every effort should be made to assess the wound if possible, unless there is clear direction that the dressing/device should not be removed. Coverage of bed by slough and/or eschar Slough: Non-viable yellow, tan, gray, green, or brown tissue; usually moist, can be soft, stringy, and mucinous in texture. Slough may be adherent to the base of the wound or present in clumps throughout the wound bed. Scab obscuring tissue loss Eschar: Dead or devitalized tissue that is hard or soft in texture; usually black, brown, or tan in color, and may appear scab-like. Necrotic tissue and eschar are usually firmly adherent to the base of the wound and often the sides/edges of the wound. Unstageable Deep Tissue Injury The true anatomic depth of soft tissue damage (and therefore stage) cannot be determined. The pressure ulcer stage can be determined only when enough slough and/or eschar is removed to expose the anatomic depth of soft tissue damage. Purple or maroon area of discolored intact skin due to damage of underlying soft tissue. Bruised appearance The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer, or cooler than adjacent tissue. intact skin or blood-filled blister Thin blister over dark wound bed

,")

63 249 Suspected DTI SOC ROC M1311 Current Number of Unhealed Pressure Ulcers FU DC M1311 Current Number of Unhealed Pressure Ulcers 252 Healed vs Unhealed Terminology referring to healed vs. unhealed ulcers refers to whether the ulcer is closed vs. open. Recognize, however, that Stage 1 pressure ulcers and Suspected Deep Tissue Injury (sdti), although closed (intact skin), would not be considered healed. Unstageable pressure ulcers, whether covered with a nonremovable dressing or eschar or slough, would not be considered healed. 251


64 253 Determining Present on Admission 254 M1311 Guidance For the OASIS, Present on Admission and Present at SOC/ROC have equivalent meanings. For each pressure ulcer, determine whether the pressure ulcer was present at the time of the most recent SOC/ROC, and did not form during this home health quality episode. For each line 1, report the number of pressure ulcers according to stage or definition of unstageable on the day of assessment. At FU or DC, report if that same pressure ulcer was present at the same stage at the most recent SOC/ROC. Example: The patient had a stage 3 pressure ulcer at SOC. The pressure ulcer is granulating at the time of recert. Row b would be marked 1 in line 1 and 1 in line 2. The pressure ulcer is still a stage 3, is current at the time of assessment (line 1) and is at the same stage as it was at the most recent SOC/ROC (line 2). Example: The patient had a stage 3 pressure ulcer at ROC. The pressure ulcer is a stage 4 at recert. The follow-up assessment should indicate: Row b (stage 3) line 1 would be marked 0 and line 2 is skipped. (No current stage 3.) Row c (Stage 4) line 1 is marked 1 and line 2 is marked 0. Even though it is the same pressure ulcer that was marked a stage 3 at ROC, it is not at the same stage as it was at ROC. 255 Determining Present on Admission 256 Practice If the pressure ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge assessment, its Present on Admission stage should be considered the stage at which it first becomes numerically stageable. If it subsequently increases in numerical stage, do not report the higher stage ulcer as being present at SOC/ROC when completing the Discharge assessment. Example: The pressure ulcer is covered with eschar and slough with no visualization of stage 4 structures at SOC. The second week of care the pressure ulcer is debrided and is staged as a pressure ulcer stage 3. The patient is now being recertified. The pressure ulcer is still a stage 3. The assessing clinician should report the current stage 3 in row b line 1. To determine how to answer line 2, walk forward from the SOC/ROC if the pressure ulcer was unstageable at that time until the clinical record mentions a stage. That is the stage that should be considered present at the SOC/ROC when answering line 2. The The pressure ulcer is covered with eschar and slough with no visualization of stage 4 structures at SOC. The second week of care the pressure ulcer is debrided and is staged as a pressure ulcer stage 3. The patient is now being recertified. The pressure ulcer is still a stage 3.

 within the assessment time frame, the initial stage of the pressure ulcer would be reported in M1311 at")

65 257 Practice The pressure ulcer at ROC was covered by a nonremovable dressing. The first documentation noted of stage during the episode is stage 2. At discharge the pressure ulcer is stage Determining Present on Admission The general standard of practice for patients starting or resuming care is that patient assessments are completed beginning as close to the actual time of the SOC/ROC as possible. If a pressure ulcer that is identified on the SOC date increases in numerical stage (worsens) within the assessment time frame, the initial stage of the pressure ulcer would be reported in M1311 at the SOC. Cannot Change Assessment on M1311 Does the instruction to code based on assessment as close to admission as possible, mean that if the ulcer is unstageable on Day 1 but debrided on Day 2, do we still report it as unstageable at SOC and leave it? Example: Pressure ulcer is covered with eschar and slough. Ulcer is debrided on day 3 of episode and ulcer is staged at 4. M1311 CANNOT be updated to stage 4. Example: Pressure ulcer is covered with a nonremovable dressing at SOC. Patient returns to clinic on day 3 and nurse documents on day 4 that it is a stage 3. M1311 CANNOT be updated to stage 3. Non Removable Dressing at SOC If the pressure ulcer is identified as a Stage 3 in the SNF documentation but is under a dressing that cannot be removed at the SOC, for M1311 do I identify a Stage 3 or unstageable pressure ulcer due to non-removable dressing? The only way you can report a pressure ulcer as unstageable due to non-removable dressing/device is by having documentation that there is indeed an ulcer underneath the dressing/device. In this case, since there is documentation of a Stage 3 pressure ulcer under the nonremovable dressing/device, you would report the ulcer as unstageable due to non-removable dressing/device. Once the dressing is removed, the ulcer would need to be assessed and staged. The SOC M1311 response of unstageable due to non-removable dressing/device should not be changed to Stage 3, since that was the pressure ulcer s status when first assessed upon admission.

66 Rationale Implications The initial clinical assessment that was conducted on the patient should be consistent with what is reported on the SOC. If the initial skin assessment completed on admission to home health services identifies a pressure ulcer, the stage of the pressure ulcer as identified on that initial clinical assessment is what should be reported on the SOC OASIS. Any subsequent changes in numerical staging would be reported on subsequent OASIS assessments. Therefore, if an unstageable pressure ulcer is identified as part of the initial skin assessment at SOC, this ulcer should be reported as unstageable on the SOC OASIS, regardless of whether it is subsequently debrided and stageable after the initial skin assessment (i.e., by Day 2). Case mix scoring comes from the answer to M1311 and M1324. No case mix points available for unstageable pressure ulcers in M1311. Cannot update M1311 during the first 5 days according to new instructions. The purpose of this policy is to get better information for outcome purposes. Q and A did NOT mention the same policy for M1324. Can the correct stage be updated in M1324??? Not a Change OASIS C2 Change A muscle flap, skin advancement flap, or rotational flap (defined as full thickness skin and subcutaneous tissue partially attached to the body by a narrow strip of tissue so that it retains its blood supply) performed to surgically replace a pressure ulcer is a surgical wound. It should not be reported as a pressure ulcer on M1311. Pressure ulcer with flap = surgical wound A pressure ulcer treated with a skin graft (defined as transplantation of skin to another site) should not be reported as a pressure ulcer and until the graft edges completely heal, should be reported as a surgical wound on M1340. Pressure ulcer with graft = surgical wound


67 265 Implications Pressure ulcers with skin grafts no longer count as pressure ulcers on the OASIS. Count them as surgical wounds. Coding guidelines state to code pressure ulcers with skin grafts as unstageable. Question: What do we code once the skin graft has healed? 266 More Practice At SOC, patient has three small stage 2 pressure ulcers on sacrum 267 More Practice At DC, sacral area is assessed: two of the stage 2 pressure ulcers have merged, and the third ulcer has increased to a stage More Practice At the SOC, patient admitted with four stage 2 pressure ulcers and one stage 3 pressure ulcer


68 More Practice Practice At recert, three of the stage 2 ulcers healed, however patient developed one additional new stage 3 pressure ulcer At the SOC, Ms. P was admitted with a diagnosis of cerebrovascular accident with right hemiparesis and assessed to have a 1 cm x 1 cm x < 0.1 cm Stage 2 pressure ulcer on her coccyx. Ms P continued DC M Ms. P continued to decline at home, with decreased appetite, frequent transient ischemic attacks, and a wish not to be hospitalized again. After a palliative care consult, the patient and family agreed to hospice care. Upon discharge from home care, Ms. P was noted to have a pressure ulcer completely covered with eschar on her left heel and a Stage 3 pressure ulcer 3 cm x 2 cm x 0.4 cm on her coccyx. 272





 will never be replaced with the same type of")

69 Response Specific Instructions Response Specific Instructions 273 Review the history of each current pressure ulcer. Compare the current stage at Discharge to past stages to determine whether any pressure ulcer currently present is new or at an increased numerical stage (worsened) when compared to the most recent SOC/ROC. Then, for each current stage, count the number of current pressure ulcers that are new or have increased in numerical stage since the last SOC/ROC was completed. This allows a more accurate assessment than simply comparing total counts at Discharge and most recent SOC/ROC. If a pressure ulcer increased in numerical stage from SOC (or ROC) to Discharge, it is considered worsened and would be included in counts of worsened pressure ulcers on M1313 at Discharge. 274 Do not reverse stage pressure ulcers as a way to document healing as it does not accurately characterize what is physiologically occurring as the ulcer heals. For example, over time, even though a Stage 4 pressure ulcer has been healing and contracting such that it is less deep, wide, and long, the tissues that were lost (muscle, fat, dermis) will never be replaced with the same type of tissue. Clinical standards require that this ulcer continue to be documented as a Stage 4 pressure ulcer until it has healed. Once the pressure ulcer has fully granulated and the wound surface is completely covered with new epithelial tissue, the wound is considered healed, and should no longer be reported as an unhealed pressure ulcer. A previously closed Stage 3 or Stage 4 pressure ulcer that breaks down again should be staged at its worst stage. M1313 Continued

70 Practice Practice Stage 4 on the coccyx at SOC and a stage 2 on the elbow. Stage 4 underwent a skin rotational flap. Stage 2 now a stage 3 Stage 2 at ROC. At DC it is 80% covered with slough no stage 4 structures visible. New stage 2 at different location. Unstageable M1313 Quiz 279 If the pressure ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, its Present on Admission stage should be considered the stage at which it first becomes numerically stageable. Scenario: At SOC, the pressure ulcer was unstageable. At a routine visit after SOC, it was staged as a stage 3. At discharge it is a stage 3. It is NOT worsened. Worsened means the pressure ulcer has increased in numerical stage. It does not mean other deterioration of the decubitus wound, such as infection or an increase in measurable size. 280 Scenario 1: You are completing Mrs. Sanchez s discharge comprehensive assessment. While assessing her skin, you determine she has two pressure ulcers. One is a stage 4 on her left buttock, and is 50 percent covered in slough, with observable muscle. The other is on her left elbow and is completely covered with eschar. You review her chart and find that at SOC the left elbow was a stage 2 and the buttock ulcer was a stage 3. How would you respond to M1313 Worsening in Pressure Ulcer Status since SOC/ROC?
71 M1313 Practice M1313 Quiz Scenario 2: You are completing Mr. Stone s discharge comprehensive assessment. When assessing his skin, you discover a stage 2 pressure ulcer on his right heel and a suspected deep tissue injury on his left heel. When you review the chart, you discover that he had no pressure ulcers at SOC. How would you respond to M1313 Worsening in Pressure Ulcer Status since SOC/ROC? M1313 Practice SOC ROC DC M1320 Healing Status No longer a good answer
; no signs or symptoms of infection; wound edges are open Early/Partial Granulation: wound with 25% of the wound bed covered with granulation")
72 285 Newly epithelialized = healed and no longer a pressure ulcer Healing Status Fully Granulating: wound bed filled with granulation tissue to the level of the surrounding skin or new epithelium; no dead space, no avascular tissue (eschar and/or slough); no signs or symptoms of infection; wound edges are open Early/Partial Granulation: wound with 25% of the wound bed covered with granulation tissue; <25% of the wound bed covered with avascular tissue (eschar and/or slough); may have dead space; no signs or symptoms of infection; wound edges open. Not Healing: wound with 25% avascular tissue (eschar and/or slough) OR signs/symptoms of infection OR clean but nongranulating wound bed OR closed/hyperkerat otic wound edges OR persistent failure to improve despite appropriate comprehensive wound management. 286 M1320 Status of Most Problematic Pressure Ulcer Determine which pressure ulcer(s) are observable: Includes all stage 2 or higher pressure ulcers that are not covered with a non-removable dressing or device, even if Unstageable When determining the healing status of a pressure ulcer for answering M1320, the presence of necrotic tissue does NOT make the pressure ulcer NA No observable pressure ulcer. A pressure ulcer with necrotic tissue (eschar/slough) obscuring the wound base cannot be staged, but its healing status is either Response 2 Early/Partial Granulation if necrotic or avascular tissue covers <25% of the wound bed, or Response 3 - Not Healing, if the wound has 25% necrotic or avascular tissue. SOC ROC FU DC M1322 Stage 1 Pressure Ulcer/INJURY NPUAP definition of a Stage 1 ulcer (Stage 1 ulcers may be difficult to detect in individuals with dark skin tones and may indicate "at risk" persons (a heralding sign of risk). Recognize that although Stage 1 pressure ulcers are closed (intact skin), they would not be considered healed. Intact skin with nonblanchable redness of a localized area usually over a bony prominence. The area may be painful, firm, soft, warmer, or cooler as compared to adjacent tissue. Darkly pigmented skin may not have a visible blanching; in dark skin tones only it may appear with persistent blue or purple hues.
73 SOC ROC FU DC M1324 M1324 Unstageable Most problematic may be the largest, the most advanced stage, the most difficult to access for treatment, the most difficult to relieve pressure, etc., depending on the specific situation A pressure ulcer is considered Unstageable if: it is covered with a non-removable dressing or device, such as a cast, that cannot be removed, or it is a suspected deep tissue injury in evolution, or the wound bed is obscured by some degree of necrotic tissue AND no bone, muscle, tendon, or joint capsule (Stage 4 structures) are visible. Note that if a Stage 4 structure is visible, the pressure ulcer is reportable as a Stage 4 even if slough or eschar is present. 291 M1324 Stage of Most Problematic Pressure Ulcer If a pressure ulcer is stage 4 at SOC and is granulating at the follow-up visit, the ulcer remains a stage 4 ulcer. A closed stage 3 or stage 4 pressure ulcer is no longer to be regarded as a pressure ulcer at its worst stage. A previously closed stage 3 or stage 4 pressure ulcer that breaks down again should be staged at its worst stage. 292 M1324 Stage of Most Problematic Pressure Ulcer In order to stage the pressure ulcer as a stage 4, bone, muscle, tendon, or joint capsule (stage 4 structures) must be visible. A pressure ulcer that has some degree of necrotic tissue (eschar or slough) or scabbing present that the clinician believes may be obscuring the visualization of stage 4 structures cannot be staged, even if it previously stageable.

74 293 Covered with Eschar; Now Granulated 294 M1324 Stage of Most Problematic Pressure Ulcer If a patient has an unstageable pressure ulcer due to black stable eschar at SOC and during the episode it peels off and leaves an area of newly epithelialized tissue, how should this be staged at Discharge on M1311? Epithelialized pressure ulcers are no longer reported. 4b, Q 89.5 We are recertifying a patient who had a stage 2 pressure ulcer at SOC that is now closed and only red. We understand not to back-stage but when a stage 2 pressure ulcer closes and is only red, is it now considered a stage 1 pressure ulcer? Or is it considered healed and gone in which we would no longer score it on OASIS? When a stage 2 ulcer re-epithelializes, it is considered "healed" and no longer reported in the OASIS data set. If you are describing a patient who now has non-blanchable redness at the same site where the stage 2 ulcer healed, then this would now be considered a new stage 1, as it has been caused by new pressure at the same site, and is not reversing the staging of a healed stage 2 ulcer. 295 M1324 Muscle Flap 296 Example Not Always the Same Ulcer If a pressure ulcer is closed with a muscle flap (defined as full thickness skin and subcutaneous tissue partially attached to the body by a narrow strip of tissue so that it retains its blood supply), the new tissue completely replaces the pressure ulcer. In this scenario, the pressure ulcer "goes away" and is replaced by a surgical wound. If the muscle flap healed completely, but then began to break down due to pressure, it would be considered a new pressure ulcer. If the flap had never healed completely, it would be considered a non-healing surgical wound. 4bQ94 Stage 3 on the left hip now fully granulating. Small pressure ulcer on elbow that is covered with slough. Patient keeps on removing dressing.
.")


75 SOC ROC FU DC 297 M1330 Does this patient have a Stasis Ulcer? SOC ROC FU DC 298 M1332 Current Number of Stasis Ulcers Identifies patients with ulcers caused by inadequate venous circulation in the area affected (usually lower legs). This lesion is often associated with stasis dermatitis. Stasis ulcers DO NOT include arterial lesions or arterial ulcers. Response 3--Information may be obtained from the physician or patient/caregiver regarding the presence of a stasis ulcer underneath the cast or dressing. 299 Counting Stasis Ulcers If areas of venous stasis ulceration are contiguous and developed at the same time, the entire area would be counted as one stasis ulcer. If the patient had a venous stasis ulcer and then later developed another venous stasis ulcer, and eventually the wound margins met, it would be counted as two ulcers, as long as it remains possible to differentiate one ulcer from another based on wound margins. Depending on the timing and progression, it may be difficult for the clinician to know that a current ulcer was once two ulcers, and/or where one ulcer ends and another begins for assessment/reporting purposes. It would be up the assessing clinician to determine the number of stasis ulcers in situations where multiple ulcers may have merged together. 300 Mixed Arterial and Venous Disease Venous stasis disease Arterial origin Mixed ulcers--mark as stasis ulcers In a situation where the patient has a mixture of venous stasis and arterial disease, the wound appearance and characteristics will often help the physician determine if the ulcer is venous, arterial, or mixed. Venous stasis ulcer, or a mixed arterial and venous ulcer mark in M1330. Arterial and it is receiving clinical assessment or intervention from the home health agency, the assessing clinician would document the wound in M1350 Skin Lesion or Open Wound. (January 2016)

76 301 Trauma Wound or Stasis Ulcer? SOC ROC FU DC 302 M1334 Status of Most Problematic Stasis Ulcer Our patient s lower extremity wound originated as a trauma wound due to a fall. The patient also has diagnoses of venous insufficiency and stasis dermatitis. The physician stated the wound is not healing due to the venous insufficiency. Is there a point in time when the wound is no longer classified as a traumatic wound and considered a stasis ulcer for M1330? Ulcers caused by inadequate circulation in the area affected. The healing process of other types of wounds, e.g. traumatic wounds, surgical wounds, burns, etc., may be impacted by the venous insufficiency, but it would not change the traumatic or surgical wound into a venous stasis ulcer. 1. Determine which stasis ulcers are observable 2. Determine which stasis ulcer is most problematic, then 3. Determine and report healing status 4bQ Healing Status SOC ROC FU DC M1340 Surgical Wound Fully Granulating: wound bed filled with granulation tissue to the level of the surrounding skin or new epithelium; no dead space, no avascular tissue (eschar and/or slough); no signs or symptoms of infection; wound edges are open Early/Partial Granulation: wound with 25% of the wound bed covered with granulation tissue; <25% of the wound bed covered with avascular tissue (eschar and/or slough); may have dead space; no signs or symptoms of infection; wound edges open. Not Healing: wound with 25% avascular tissue (eschar and/or slough) OR signs/symptoms of infection OR clean but non-granulating wound bed OR closed/hyperkeratoti c wound edges OR persistent failure to improve despite appropriate comprehensive wound management.
77 M1340 Surgical Wound Surgical Wounds 4b Q Old surgical wounds that have resulted in scar or keloid formation are not considered current surgical wounds and should not be included in this item. If the patient has both an observable and an unobservable wound, the best response is 1 Yes, patient has at least one observable surgical wound. Response 2 if the only surgical wound(s) is/are not observable. A wound is considered not observable if it is covered by a dressing/device (such as a cast) which is not to be removed per physician order. A surgical site closed primarily (with sutures, staples, or a chemical bonding agent) is generally described in documentation as a surgical wound until re-epithelialization has been present for approximately 30 days, unless it dehisces or presents signs of infection. After 30 days, it is generally described as a scar and should not be included in this item. Surgical Wounds Pressure ulcers with muscle flaps or skin grafts (breaks down during healing non healing surgical wound) Also can be a pressure ulcer and surgical wound at the same time Excised pressure ulcers Q94.1 Dialysis cath exit sites (AV fistulas, AV shunts)* Not A Surgical Wound Pressure ulcers sutured closed Paracentesis 4b-Q Surgical Wounds Surgical Wounds Surgical Wounds Implanted infusion devices* ON-Q catheter sites Implanted pumps* Cardiac cath by cutdown VANTAS implanted device* Electrodessication and curettage MammoSite breast brachytherapy *As long as present in body, regardless whether functional Not surgical wounds PICC line (tunneled and non-tunneled) Unless inserted centrally Cardiac cath by needle puncture Toenail removal Cryosurgery 307 Surgical Wound I&D with drain Excision Wound with drain even after drain pulled Shave, punch or excisional biopsy Repair of a internal trauma Take down of ostomy Burn with a skin graft Not Surgical Wounds I&D without drain I&D of foot ulcer with biopsy of bone 2nd Q 2015 Removal of a callus Repair of a traumatic laceration Burn with a skin graft Thoracotomy or any wound ending is otomy (ostomy) Surgical incision to insert chest tube 308

78 Surgical Wounds Surgical Wounds 310 Surgical Wounds Pacemakers and internal defibrillators until epithelialized for 30 days LVAD * VP shunts and burr holes Donor site for grafts Laparoscopic surgery, arthroscopy, and other minimally invasive surgery/procedure Kyphoplasty by open approach Not Surgical Wounds Pacemakers and internal defibrillators once epithelialized for 30 days Retention sutures, staple sites Kyphoplasty by percutaneous approach Cataract surgery Gynecological surgery via vaginal approach Mucous membranes (dental) Central venous catheters or central lines are those with the catheter tip located in the superior vena cava. Central lines can be peripherally inserted (i.e., basilic or cephalic vein in upper arm, or femoral vein in the groin) or centrally inserted (i.e., internal jugular vein in the neck, or subclavian or axillary vein in the chest). Central lines that are centrally inserted (as in the internal jugular example) ARE considered surgical wounds for M1340 because of the central insertion, even if the type of catheter inserted into the central vein was intended to be inserted peripherally. Central lines that are peripherally inserted are not considered surgical wounds. 4bQ How many surgical wounds? SOC ROC FU DC 312 M1342 Status of Most Problematic Surgical Wound 1. Determine which surgical wounds are observable 2. Determine which observable surgical wound is most problematic, then 3. Determine and report healing status
.")

79 313 Primary Intention The clinician must first assess if the wound is healing entirely by primary intention (wellapproximated with no dehiscence), or if there is a portion healing by secondary intention, (due to dehiscence, interruption of the incision, or intentional secondary healing). Surgical wounds healing by primary intention (approximated incisions) do not granulate, therefore the only appropriate responses would be Response 0 - Newly epithelialized or Response 3 - Not healing. 314 Primary Intention If the wound is healing solely by primary intention, observe if the incision line has reepithelialized. Epithelialization is regeneration of the epidermis across a wound surface. (If there is no interruption in the healing process, this generally takes within a matter of hours to three days post-operatively.) If there is not full epithelial resurfacing such as in the case of a scab adhering to underlying tissue, the correct response would be "Not healing" for the wound healing exclusively by primary intention. 315 Healing by Primary Intention 316 Healing by Secondary Intention

; no signs or symptoms or infection.")
80 Secondary Intention Secondary Intention 317 Healing by primary intention Healing by secondary intention 318 If it is determined that there is incisional separation, healing will be by secondary intention. Surgical incisions healing by secondary intention do granulate, therefore may be reported as "Not healing," "Early/partial granulation," "Fully granulating," and eventually "Newly epithelialized. Response 0 Newly epithelialized: Completely covered with new epithelium; no exudate; no avascular tissue (eschar and/or slough); no signs or symptoms or infection. Epithelialization is characterized by "Epidermal resurfacing" and means the opening created during the surgery is covered by epithelial cells. If epidermal resurfacing has occurred completely, the correct response in the OASIS would be "Newly epithelialized" until 30 days have passed without complication, at which time it is no longer a reportable surgical wound. 319 Healing in the Middle but Not on the Ends When a portion of the surgical wound is intact/healed, and a portion of the wound is open and healing by secondary intention, to determine the healing status consider the portion of the wound bed that is healing by secondary intention when applying the WOCN criteria of % of the wound bed covered with granulation tissue or % of wound bed covered with avascular tissue. If the surgical wound has more than one area healing by secondary intention, separated by one or more areas of intact/healed tissue, all open areas healing by secondary intention would be included as the "wound bed, when applying the percentages to determine healing status. See the WOCN Guidance on OASIS Skin and Wound Status Items at April 2016 Q and A 320 Primary intention Newly epithelialized = surgical wound for 30 days Healing Status Fully Granulating: wound bed filled with granulation tissue to the level of the surrounding skin or new epithelium; no dead space, no avascular tissue (eschar and/or slough); no signs or symptoms of infection; wound edges are open Early/Partial Granulation: wound with 25% of the wound bed covered with granulation tissue; <25% of the wound bed covered with avascular tissue (eschar and/or slough); may have dead space; no signs or symptoms of infection; wound edges open. Not Healing: wound with 25% avascular tissue (eschar and/or slough) OR signs/symptoms of infection OR clean but non-granulating wound bed OR closed/hyperkeratoti c wound edges OR persistent failure to improve despite appropriate comprehensive wound management.
81 321 Healing Status Venous Access Devices When a needle is inserted and removed from an implanted venous access device, it is possible that the skin that was pierced by the needle could have a resulting wound that would heal by secondary intention. Usually, with good access technique and current needle technology there will be no perceptible wound. Response 0 Newly epithelialized for implanted venous access devices and infusion devices when the insertion site is healed and without signs and symptoms of infection. 322 Healing Status Venous Access Devices Occasionally, if there was an extremely large bore needle or traumatic entry or removal, there may be a resulting wound that heals by secondary intention. In this situation, the accessing clinician would rely on the WOCN's OASIS Wound Guidance document to determine the healing status. Note that a scab is a crust of dried blood and serum and should not be equated to either avascular or necrotic tissue when applying the WOCN guidelines. Therefore while the presence of a scab does indicate that full epithelialization has not occurred in the scabbed area, the presence of a scab does not meet the WOCN criteria for reporting the wound status as "Not healing". 4bQ Some sites, because they are being held open by a line or needle, cannot fully granulate and may remain "nonhealing" while the line or needle is in place. 4bQ SOC ROC 323 M1350 Skin Lesion or Open Wound 324 M1350 Skin Lesion or Open Wound Not included Bowel ostomies (which are reported in OASIS item M1630) *ileostomies are considered bowel ostomies 3rdQ2014 Wounds resulting from cataract surgery, surgery to mucosal membranes, or gynecological surgical procedures by a vaginal approach Tattoos, piercings, and other skin alterations without ongoing assessment and/or clinical intervention by the home health agency as a part of the planned/provided care Any other skin lesions or open wounds that are not receiving clinical intervention

82 325 M1350 Skin Lesion or Open Wound Included A lesion is a broad term used to describe an area of pathologically altered tissue. All alterations in skin integrity are considered to be lesions. Examples of lesions include but are not limited to sores, skin tears, burns, ulcers, rashes, edema, burns, diabetic ulcers, cellulitis, abscesses and wounds caused by trauma of various kinds. PICC line and peripheral IV sites (not inserted centrally) Primary lesions, secondary lesions, changes in shape (edema), texture, color, breaks in skin and vascular lesions 4b-Q Included Non-bowel ostomies (for example, tracheostomies, thoracostomies, urostomies, jejunostomies, gastrostomies) Gastrostomies and jejunostomies are not considered bowel ostomies. (G tubes and J tubes are reported in M1350) 4b-Q Clinical Interventions are Necessary If clinical interventions (for example, cleansing, dressing changes, ongoing assessment) are being provided by the home health agency during the care episode What about that closed stage 3 or stage 4 pressure ulcer? 328 SOC ROC FU DC M1400 Short of Breath If patient uses oxygen continuously Assess with oxygen in use If the patient uses oxygen intermittently Assess without the use of oxygen If oxygen used at night due to positional dyspnea, report level of exertion that causes dyspnea w/o O2 Sleep apnea dyspnea
83 329 M1400 When is the patient dyspneic or noticeably Short of Breath? Chairfast or bedbound patient: Evaluate the level of exertion required to produce shortness of breath The chairfast patient can be assessed for level of dyspnea while performing ADLs or at rest Response 0 Patient has not been short of breath during the day of assessment M1400 When is the patient dyspneic or noticeably Short of Breath? 330 Chairfast or bedbound patient: Response 1 (When walking more than 20 feet ) Appropriate if demanding bed-mobility activities produce dyspnea in the bedbound patient (or physically demanding transfer activities produce dyspnea in the chairfast patient). Responses 2, 3, and 4 for assessment examples for these patients as well as ambulatory patients. M1400 Quiz 331 Assess and report what caused the patient to experience dyspnea on the day of the assessment. The examples included in Responses 2 and 3 are used to illustrate the degree of effort represented by the terms moderate and minimal. Response 3 - With minimal exertion or agitation includes the examples of eating, talking or performing other ADLs. The reference to other ADLs means activities of daily living that only take minimal effort to perform like grooming. 332 Dyspneic only in supine position Patient sleeps with 2 pillows or in recliner and currently not short of breath at rest and otherwise not SOB Environmental modifications: If the patient restricts an activity to remain free of dyspnea, they can be a 0 Go up stairs 2 steps at a time to avoid dyspnea can still be a 0

84 TRN DC M Cardiac Status M1501s 335 M1501 Symptoms in Heart Failure Patients Identifies if patient has experienced signs/ symptoms of heart failure at time of most recent SOC/ROC OASIS assessment or since that time If the patient had symptoms and was transferred without our knowledge, the answer is yes Consider New or ongoing heart failure symptoms since SOC/ROC OASIS 336 M1501 Symptoms in Heart Failure Patients Review clinical record physical assessment data weight trends clinical notes Dyspnea is a symptom of heart failure and while it may also be a symptom of another co-existing disease process, such as pneumonia, it would still be reported in M1501 and M1511, Heart Failure Followup, if the patient has a diagnosis of heart failure.

85 Not Assessed Not Assessed "Not assessed" means the patient with a diagnosis of heart failure was not assessed for symptoms of heart failure at the time of or at any time since the SOC/ROC OASIS assessment. No assessment of lung sounds occurred No assessment of lower limbs No assessment for dyspnea No assessment for orthopnea No assessment for weight gain A patient with CHF is admitted to the hospital and discharged with a new diagnosis such as hip fracture. The ROC visit and next visit focused on interventions related to the hip fracture, and no documentation of the heart failure assessment. Patient is unable to remain in the home and is transferred to a SNF. No CHF assessment between ROC and Transfer would mean that M1501 at Transfer would be "2-Not assessed". TRN DC M1511 Heart Failure Follow up M1511 Heart Failure Follow up Include any actions that were taken at least one time at the time of the last OASIS assessment or since that time. Response 0 - No action taken Interventions are not completed as outlined in this item Document the rationale in clinical record If Response 0 is selected, none of the other responses should be selected.
86 Same Day? M1511 Heart Failure Follow up 341 When completing M Heart Failure Follow-up, Response 1 is an appropriate response only if a physician responds to the agency communication with acknowledgment of receipt of information and/or further advice or instructions on the same day. Same day in this item means by the end of this calendar day, and is not the same as "within one calendar day", which is defined in M2002, Medication Follow-up as "until the end of the next calendar day". 4b-Q116.2 What if we left a message for the physician on the same day and the physician calls the patient on the same day but not us?? Response 1 cannot be marked. Has to be communication to the agency. 4b Response 3 Either the home care clinician reminds the patient to implement physician-established parameters for treatment or is aware that the patient is following physician-established parameters for treatment, e.g., took extra diuretic 4b-Q Response 4--Teaching must be in response to symptoms not preventive teaching Telehealth and interventions by telephone do count. Therapists providing written materials without assessment of understanding is not an educational intervention. 4b-Q Quiz Answer 343 Patient has symptoms of heart failure and the RN visits the next day. The RN instructs the patient to call the agency or call 911 if symptoms reoccur. The RN called the next day to check on the patient. Which options? Patient education or other clinical interventions But NOT: 2 Patient advised to get emergency treatment is NOT an appropriate response. Response 2 is only appropriate when the patient is advised to get emergency treatment when symptoms of heart failure require immediate treatment

 Patient has a urinary diversion that is pouched (ileal conduit, urostomy,")
87 SOC ROC DC M Elimination Status M1600s SOC ROC FU DC 347 M1610/M1615 Other types of incontinence 348 M1610 Urinary Incontinence or Urinary Catheter Presence Timepoints SOC/ROC/DC Response 0-No incontinence or anuria Patient has anuria or an ostomy for urinary drainage (e.g., an ileal conduit) Patient has a urinary diversion that is pouched (ileal conduit, urostomy, ureterostomy, nephrostomy), with or without a stoma
88 349 M1610 Urinary Incontinence or Urinary Catheter Presence Response 1-Patient is incontinent If patient is incontinent AT ALL (i.e., occasionally, only when I sneeze, sometimes I leak a little bit, etc.) Patient is incontinent or is dependent on a timed-voiding program Timed voiding is defined as scheduled toileting assistance or prompted voiding to manage incontinence based on identified patterns. Time voiding is a compensatory strategy; it does not cure incontinence. 350 M1610 Urinary Incontinence or Urinary Catheter Presence Response 2 Pt requires urinary catheter Catheter or tube is utilized for urinary drainage (even if catheterizations are intermittent). Patient requires the use of a urinary catheter for any reason (e.g., retention, postsurgery, incontinence, continent urinary diversions). Exceptions inserting catheter to irrigate bladder with antibiotic and capped tube with no plan to use for draining urine Select Response 2 and follow the skip pattern if the patient is both incontinent and requires a urinary catheter. 351 M1610 Urinary Incontinence or Urinary Catheter Presence What if the catheter was removed or inserted during the comprehensive assessment? Day of assessment doesn t apply If inserted, select response 2 If removed, select response 0 or 1 This refers to an indwelling catheter, not intermittent. 4b-Q One-time catheterization for the sole purpose of obtaining urine for laboratory testing or other diagnostic procedure would not be considered having a catheter for urinary drainage July M1610 Urinary Incontinence or Urinary Catheter Presence Does the patient admit having difficulty controlling the urine? Do you have orders to change a catheter? Is your stroke patient using an external catheter? Any odors? Consider Physiologic reasons Cognitive impairments Mobility problems


89 SOC ROC DC 353 M1615 When does Urinary Incontinence occur? Response 0 Timed-voiding defers incontinence Timed voiding determines the patient s pattern for voiding and schedules toileting to prevent episodes of leaking. The patient can self-schedule toileting or the caregiver can prompt or bring the patient to the toilet. Time voiding is a compensatory strategy; it does not cure incontinence. If timed voiding does not defer incontinence, do not select Response 0. If timed voiding defers incontinence, but there s an occasional accident, up to clinician to determine if in relevant past or if timed voiding is 100% effective. 4b-Q M1615 When does Urinary Incontinence occur? Response 1 Occasional stress incontinence Patient is unable to prevent escape of relatively small amounts of urine when coughing, sneezing, laughing, lifting, moving from sitting to standing position, or other activities (stress), which increase abdominal pressure. 355 M1615 When does Urinary Incontinence occur? Response 2,3,or 4 Urinary incontinence regularly Determine when the incontinence usually occurs May be secondary to a symptom not listed Response 2 During the night only Response 3 During the day only Includes incontinence during daytime naps. Response 4 During the day and night When the patient is incontinent when sleeping at night and up/awake during the day. SOC ROC FU DC 356 M1620 Bowel Incontinence Frequency

90 357 M1620 Bowel Incontinence Frequency Response 4 On a daily basis Indicates that the patient experiences bowel incontinence once per day. Response NA Patient has an ostomy for bowel elimination. Unknown Not an option at follow-up or discharge Bowel program no assumed incontinence 4b-Q Time Frame for Bowel Incontinence The timeframe under consideration is day of assessment and relevant past. This timeframe is directed by Response options "0-Very rarely or never has bowel incontinence" and "1-Less than once weekly." Considering these two options, the assessing clinician would need to consider bowel incontinence that was experienced beyond the past 7 days. The assessing clinician must use clinical judgment to determine how far into the past would be relevant to this home care admission. The assessing clinician may elect to re-assess bowel incontinence within the allowed timeframe and change her/his original response as well as M0090, Date Assessment Completed. 4bQ M1620 Bowel Incontinence Frequency Review the bowel elimination pattern Difficulty controlling stools Diarrhea Note cleanliness Around the toilet Clothing At F/U may ask the aide Consider Physiologic reasons Cognitive impairments Mobility problems SOC ROC FU 360 M1630 Ostomy for Bowel Elimination
 If an ostomy has been reversed, then the patient does not have an ostomy at the time of assessment Antegrade Colonic Enema therapy is provided by a catheter through an ostomy,")
 3rdQ2014 362 Neuro/Emotional/Behavioral M1700s SOC ROC DC M1700 Cognitive Functioning M1700 Cognitive Functioning 363 364 Consider: Patient s signs/symptoms of")
91 361 M1630 Ostomy for Bowel Elimination Addresses bowel ostomies ONLY Applies to any type of ostomy for bowel elimination (e.g., colostomy, ileostomy) If an ostomy has been reversed, then the patient does not have an ostomy at the time of assessment Antegrade Colonic Enema therapy is provided by a catheter through an ostomy, but is not considered a "bowel elimination ostomy". (Could be considered under M1350) 3rdQ Neuro/Emotional/Behavioral M1700s SOC ROC DC M1700 Cognitive Functioning M1700 Cognitive Functioning Consider: Patient s signs/symptoms of cognitive dysfunction over the past 24 hours. Amount of supervision and care the patient has required due to cognitive deficits Level of cognitive functioning- including alertness orientation comprehension concentration immediate memory for simple commands

92 M1700 Cognitive Functioning SOC ROC DC M1710 When Confused Patients with diagnoses such as dementia, delirium, development delay disorders, mental retardation, etc., will have various degrees of cognitive dysfunction. Patients with neurological deficits related to stroke, mood/anxiety disorders, or who receive opioid therapy may have cognitive deficits. 367 M1710 When Confused (Reported or Observed Within the Last 14 Days) May not relate directly to Item M1700 Assess specifically for confusion in the past 14 days. If it is reported that the patient is occasionally confused, identify the situation(s) in which confusion has occurred within the last 14 days, if at all. Report any episodes of confusion that occurred during the past 14 days, without regard to the cause of potential relevance of the confusion to this episode of care 368 What is the difference in what is measured in M1700 Cognitive Functioning and M1710 When Confused? M1700--Level of alertness, orientation, comprehension, concentration, and immediate memory for simple commands on the day of assessment (at the time of the assessment and in the preceding 24 hours). M1710, When Confused, is intended to identify the time of day or situations when the patient experienced confusion, if at all, during the past 14 days (Day of assessment and prior 14 days). 4b-Q123.9



93 369 M1700 Cognitive Functioning and M1710 When Confused If a patient is demonstrating confusion on the day of the assessment, it would be reported both in M1700 and M1710. If a patient was NOT confused on the day of assessment, but had experienced confusion during the prior 14 days, it would only be reported in M1710. If a patient has a cognitive impairment on the day of the assessment, that does NOT result in confusion, e.g.; forgetfulness, learning disabilities, concentration difficulties, decreased intelligence, it would only be reported in M b-Q123.9 SOC ROC DC 370 M1720 When Anxious Anxiety includes: Worry that interferes with learning and normal activities Feelings of being overwhelmed and having difficulty coping Symptoms of anxiety disorders 371 Nonresponsive M1710/M1720 Nonresponsive means that the patient is unable to respond or the patient responds in a way that you can t make a clinical judgment about the patient s level of orientation. Examples at 4b- Q124.1 Can still report confusion or anxiety during the past 14 days ask the caregiver or other source Nonresponsive pulls the patient from 30+ measures because may not expect to improve. If not expected to improve, NR is a good response. SOC ROC DC 372 M1730 Depression Screening


94 M1730 Depression Screening M1730 Depression Screening 373 Identifies if the home health agency screened the patient for depression using a standardized, validated depression screening tool. Response 0 if a standardized, validated depression screening was not conducted. If the clinician chooses not to assess the patient (because there is no appropriate depression screening tool available or for any other reason), Response 0 No should be selected. Response 1 if the PHQ-2 is completed, and mark the appropriate responses in rows a and b. Please note that the PHQ-2 instructions indicate that the patient is interviewed, not family or others. If the patient scores three points or more on the PHQ-2, then further depression screening is indicated. 374 When evaluating the patient, the clinician must first assess whether the PHQ-2 is the appropriate depression screening tool. If the PHQ-2 is appropriate (the patient appears to be cognitively and physically able to respond), then the instrument may be used. If, however, the patient is unable to answer the specific PHQ-2 questions when asked by the assessing clinician, e.g. the patient can't quantify how many days they have experienced the problems, the clinician can report in M1730 that the PHQ-2 was administered (Response 1), and select N/A - Unable to respond. Response 1-Yes may NOT be selected if the patient refuses to hear the questions or states they are too personal. Response 1 Yes may NOT be selected if the patient cannot understand the questions. M1730 Depression Screening SOC ROC DC M If the PHQ-2 is not used to assess the patient, you may choose to administer a different standardized, validated depression screening tool with instructions that may allow for information to be gathered by observation and caregiver interview as well as self-report. In this case, the clinician would select Response 2 or 3 for M1730, depending on the outcome of the assessment. Response 2 if the patient is screened with a different standardized, validated assessment AND the tool indicated the need for further evaluation. Response 3 if the patient is screened with a different standardized, validated assessment BUT the tool indicates no need for further evaluation. 376
95 377 M1740 Cognitive, behavioral, and psychiatric symptoms Behaviors can be observed by the clinician or reported by the patient, family, or others Consider problematic behaviors Severe enough to make the patient unsafe OR cause considerable stress to caregivers OR require supervision or intervention Consider frequency of behaviors 378 M1740 Cognitive, behavioral, and psychiatric symptoms The time frame under consideration for M1740, Cognitive, behavioral, and psychiatric symptoms that are demonstrated at least once a week, is defined in the wording of the item - "at least once a week". The phrase "at least once a week" means that a behavior was demonstrated multiple times in the recent, relevant past and the frequency of the occurrence was at least one time a week prior to and including the day of assessment. The assessing clinician will determine "recent, relevant past" based on the patient/caregiver interview, referral information, assessment findings, diagnoses and recent history of medical treatment and its effectiveness. 4b-Q M1740 M If a patient is alert and oriented, but decides not to use their cane because they think they don t need it (they are unsafe without it) or they decide they aren t going to take their diuretic because they are going to the doctor and don t want to have any accident, would you select Response 2 Impaired decision-making? 4b-Q The intent of M1740, Cognitive, behavioral, and psychiatric symptoms, is to capture specific behaviors that are a result of significant neurological, cognitive, behavioral, developmental or psychiatric limitations or conditions. It is not the intent of M1740 to report noncompliance or risky choices made by cognitively intact patients who are free of the aforementioned conditions. The assessing clinician will have to determine if the patient has a disorder that is causing her non-compliance or is the patient making a choice not to comply completely with physician's orders, cognizant of the implications of that choice.
96 381 Doesn t have to be a diagnosed disorder SOC ROC DC 382 M1745 Frequency of Disruptive Behavior Symptoms The behaviors identified for the purpose of responding to M1740 and M1745 could be determined to be associated with a significant neurological, behavioral or psychiatric disorder either by diagnosis and/or in the assessing clinician s clinical judgment. 383 M1745 Frequency of Disruptive Behavior Symptoms Consider if the patient has any problematic behaviors not just the behaviors listed in M1740 which jeopardize or could jeopardize the safety and well-being of the patient or caregiver. Then consider how frequently these behaviors occur. Include behaviors considered symptomatic of neurological, cognitive, behavioral, developmental, or psychiatric disorders. Use clinical judgment to determine if the degree of the behavior is disruptive or dangerous to the patient or caregiver. 384 ADLs/IADLs
97 385 Conventions Specific to ADLs/IADLs Identify the patient s ABILITY, not necessarily actual performance. "Willingness" and "adherence" are not the focus of these items. The level of ability refers to the patient s ability to safely complete specified activities. While the presence or absence of a caregiver may impact actual performance of activities, it does not impact the patient s ability to perform a task. Consider medical restrictions when determining ability. For example, if the physician has ordered activity restrictions, consider this when selecting the best response to functional items related to ambulation, transferring, bathing, etc. 386 Conventions Specific to ADLs/IADLs The patient s ability may change as the patient s condition improves or declines, as medical restrictions are imposed or lifted, or as the environment is modified. The clinician must consider what the patient is able to do on the day of the assessment. If ability varies over time, choose the response describing the patient s ability more than 50% of the time period under consideration. Understand what tasks are included and excluded in each item and select the OASIS response based only on included tasks. If the patient s ability varies between the different tasks included in a multi-task item, report what is true in a majority of the included tasks, giving more weight to tasks that are more frequently performed. 387 Conventions Specific to ADLs/IADLs Ability can be temporarily or permanently limited by: physical impairments (for example, limited range of motion, impaired balance) emotional/cognitive/behavioral impairments (for example, memory deficits, impaired judgment, fear) sensory impairments, (for example, impaired vision or pain) environmental barriers (for example, accessing grooming aids, mirror and sink, stairs, narrow doorways, location where dressing items are stored). Environmental barriers may be different dependent on the tasks. 388 Conventions Specific to ADLs/IADLs Response scales present the most optimal (independent) level first, then proceed to less optimal (most dependent) levels. Assessment Strategies Observation/demonstration is the preferred method Patient/caregiver interview Physical assessment Nutritional assessment Physician orders Plan of Care Referral information Review of past health history Service animals are considered devices, not assistance
98 Things to Remember Things to Remember 389 What is the difference between willingness and adherence (which do not impact OASIS scoring) and cognitive/mental/emotional/behavioral impairment (which may impact OASIS scoring)? In absence of pathology, patients may make decisions about how and when they perform their activities of daily living that may differ from what the clinician determines to be acceptable. A patient may choose to shave and brush his teeth infrequently because he doesn t value doing it at a frequency that the clinician deems as socially appropriate. There are differences in the frequency at which grooming or bathing is performed, or expected to be performed based on age, religion, culture and familial practices, and this is not necessarily indicative of pathology. 390 A patient may demonstrate that they can safely ambulate while using a walker, but then as a matter of choice, decide to walk without it. Another patient may demonstrate that they can safely ambulate while using a walker, but then consistently walk without it, forgetting that they have a walker. For the purposes of OASIS scoring, non-conformity or non-adherence should not automatically be considered indicative of a deeper psychological impairment. The assessing clinician will have to use clinical judgment to determine if the patient s actions are more likely related to impairment, or to personal choice made in awareness of the potential related risk. Bedfast Defined Access is Excluded "Bedfast refers to being confined to the bed, either per physician restriction or due to a patient's inability to tolerate being out of the bed." If the patient can tolerate being out of bed, they are not bedfast unless they are medically restricted to the bed. The patient is not required to be out of bed for any specific length of time. The assessing clinician will have to use her/his judgment when determining whether or not a patient can tolerate being out of bed. For example, a severely deconditioned patient may only be able to sit in the chair for a few minutes and is not considered bedfast as she/he is able to tolerate being out of bed. A patient with Multiple System Atrophy becomes severely hypotensive within a minute of moving from the supine to sitting position and is considered bedfast due to the neurological condition which prevents him from tolerating the sitting position. Patient s ability to access needed items and/or location where the task occurs is INCLUDED, unless specifically excluded in guidance M1845 Toileting hygiene excludes getting to the location where the toileting occurs M1870 Feeding/Eating Excludes getting to location where meal is consumed and excludes transporting food to the table M1880 Planning and Preparing Light meals excludes getting to location where meal prepared M1890 Telephone use Excludes getting to the location where the telephone is stored


 should be considered to have more ability in grooming.")
99 SOC ROC DC M1800 Grooming M1800 Grooming Excluding bathing, shampooing hair, and toileting hygiene. Getting to the area where grooming takes place is INCLUDED Patient's ability to safely perform grooming, given the current physical and mental/emotional/cognitive status, activities permitted, and environment. Select the response that best describes the patient s level of ability to perform the majority of grooming tasks. Patients able to do more frequently performed activities (for example, washing hands and face) but unable to do less frequently performed activities (trimming fingernails) should be considered to have more ability in grooming. SOC ROC FU DC M1810 Dress Upper Body SOC ROC FU DC M1820 Dress Lower Body
100 M1810/M1820 Dressing M1810/M1820 Dressing 397 Ability to obtain, put on, and remove upper body and lower body clothing. Assess ability to put on whatever clothing is routinely worn. Specifically includes the ability to manage zippers, buttons, and snaps if these are routinely worn. Prosthetic, orthotic, or other support devices applied to the upper body (for example, upper extremity prosthesis, cervical collar, or arm sling) and/or lower body (for example, lower extremity prosthesis, ankle-foot orthosis [AFO], or TED hose) should be considered as dressing items. Note that elastic bandages, including ACE Wrap brand, worn for support and compression should be considered as a dressing item, but wraps utilized solely to secure a wound dressing would not be considered a dressing (clothing) item for M1810 or M1820. Answer based on majority of tasks (items). Do NOT consider the importance of one item over another. 4b If a patient modifies the clothing they wear due to a physical impairment, the modified clothing selection will be considered routine if there is no reasonable expectation that the patient could return to their previous style of dressing. There is no specified timeframe at which the modified clothing style will become the routine clothing. The clinician will need to determine which clothes should be considered routine. It will be considered routine because the clothing is what the patient usually wears and will continue to wear, or because the patient is making a change in clothing options to styles that are expected to become the patient's new routine clothing. Patient must dress in stages due to shortness of breath Still can be independent M1810/M1820 Dressing M1810/M1820 Dressing 399 Assessment strategies: A combined observation/interview approach with the patient or caregiver is helpful in determining the most accurate response for this item. Ask the patient if he/she has difficulty dressing upper body. Observe the patient s general appearance and clothing and ask questions to determine if the patient has been able to dress independently and safely. Opening and removing garments during the physical assessment of the heart and lung provides an excellent opportunity to evaluate the upper extremity range of motion, coordination, and manual dexterity needed for dressing. Observe spinal flexion, joint range of motion, shoulder and upper arm strength, and manual dexterity during the assessment. The patient also can be asked to demonstrate the body motions involved in dressing. 400 How do you answer if a disabled person has everything in their home adapted for them; for instance, closet shelves & hanger racks have been lowered to be accessed from a wheelchair. Is the patient independent with dressing? Response 0 I have a patient who could not obtain his clothes, but could dress without assistance if clothes were laid out (Response 1). If the environment was adapted (a new usual storage place for clothing was selected) so that the patient could obtain, put on and remove the clothing without any assistance, would the patient then be considered independent in dressing? Answer based on what is true the day of assessment.
, and the patient can now access clothes from a location without anyone s help, then this new")

101 401 Environment Modification If the environment is modified (e.g., the patient decides to start storing clothing in the dresser instead of hanging in the closet), and the patient can now access clothes from a location without anyone s help, then this new arrangement could now represent the patient's current status (e.g., clothing s new usual storage area and patient's ability). The appropriate score would be a 0 if the patient was also able to put on and remove a majority of his clothing items safely. Temporary storage because of weakness 1 (Patient could then work to gain independence in accessing clothing from its usual storage location, or decide to make long-term environmental modifications, and possibly achieve improvement in the outcome if successful.) Permanent storage 0 SOC ROC FU DC 402 M1830 Bathing M1830 Bathing M1830 Bathing Specifically excludes washing face and hands, and shampooing hair. M1830, Bathing - The focus is on the patient's ability to access the tub/shower, transfer in and out, and bathe the entire body once the needed items are within reach. The ability to access bathing supplies and prepare the water in the tub/shower are excluded from consideration when assessing the patient's bathing ability. The amount of assistance the patient requires to get to the location bathing occurs would be considered. If the patient requires assistance (another person to provide verbal cueing, stand-by or hands-on assistance) to safely ambulate down the hallway and no other assistance with transfer and bathing, this is intermittent assistance, therefore M1830 Response 2 - Able to bathe in shower or tub with the intermittent assistance of another person should be reported. (April 2016 Q and A) If the patient requires standby assistance to bathe safely in the tub or shower or requires verbal cueing/reminders, then select Response 2 or Response 3, depending on whether the assistance needed is intermittent ( 2 ) or continuous ( 3 ). If the patient's ability to transfer into/out of the tub or shower is the only bathing task requiring human assistance, select Response 2. If a patient requires one, two, or all three of the types of assistance listed in Response 2 of M1830 but not the continuous presence of another person as noted in Response 3, then Response 2 is the best response.
102 M1830 Bathing M1830 Bathing 405 The patient s status should not be based on an assumption of a patient s ability to perform a task with equipment they do not currently have. If the patient does not have a tub or shower in the home, or if the tub/shower is nonfunctioning or not safe for patient use, the patient should be considered unable to bathe in the tub or shower. Responses 4, 5, or 6 would apply, depending on the patient's ability to participate in bathing activities. 406 Assessment strategies: Combined observation/interview approach Ask the patient what type of assistance is needed to wash entire body in tub or shower. Observe the patient s general appearance in determining if the patient has been able to bathe self independently and safely. Observe patient actually stepping into shower or tub to determine how much assistance the patient needs to perform the activity safely. Evaluate the amount of assistance needed for the patient to be able to safely bathe in tub or shower. The patient who only performs a sponge bath may be able to bathe in the tub or shower with assistance and/or a device. M1830 Bathing M1830 Bathing Given the following situations, what would be the appropriate responses to M1830? a) The patient's tub or shower is nonfunctioning or is not safe for use. b) The patient is on physician-ordered bed rest. c) The patient fell getting out of the shower on two previous occasions and is now afraid and unwilling to try again. If due to fear, she refuses to enter the shower even with the assistance of another person; either Response 4, 5, or 6 would apply, depending on the patient s ability at the time of assessment. If she is able to bathe in the shower when another person is present to provide required supervision/assistance, then Response 3 would describe her ability. d) The patient chooses not to navigate the stairs to the tub/shower. If the patient chooses not to navigate the stairs, but is able to do so with supervision, then her ability to bathe in the tub or shower is dependent on that supervision to allow her to get to the tub or shower. 4bQ134 My patient is allowed to bathe in the tub, but is medically restricted from getting the cast on his lower leg and foot wet. He is unable to put the water protection sleeve on, but once someone applies the protective sleeve for him, he can get into and out of the bathtub using a transfer bench and wash all of his body with a handheld shower. Does this medical restriction impact the patient's ability when scoring M1830, Bathing? In the scenario above, Response 2 is appropriate since the patient needs intermittent human assistance. 4bQ134.1


103 SOC ROC FU DC M1840 Toilet Transferring M1840 Toilet Transferring Observe the patient during transfer and ambulation to determine if the patient has difficulty with balance, strength, dexterity, pain, etc. Determine the level of assistance needed by the patient to safely get on and off the toilet or commode. Tasks related to personal hygiene and management of clothing are not considered when responding to this item. M1840 Toilet Transferring No Toilet Response 1 If the patient requires standby assistance to get to and from the toilet safely or requires verbal cueing/reminders. If the patient needs assistance getting to/from the toilet or with toileting transfer or both. If the patient can independently get to the toilet, but requires assistance to get on and off the toilet. Response 1 requires patient participation (effectively participate by contributing effort toward the completion of some of the included tasks) A patient who is unable to get to/from the toilet or bedside commode, but is able to place and remove a bedpan/urinal independently, should be marked Response 3. This is the best response whether or not a patient requires assistance to empty the bedpan/urinal. If the bedfast patient needs assistance to get on/off the bedpan, the appropriate M1840 Response is "4-Is totally dependent in toileting" even if they can place and remove the urinal. In the absence of a toilet in the home, the assessing clinician would need to determine if the patient is able to use a bedside commode (Response 2), or if unable to use a bedside commode, if he is able to use a bedpan/urinal independently (Response 3). If the patient is not able to use the bedside commode or bedpan/urinal as defined in the responses, or if such equipment is not present in the home to allow assessment, then Response 4 totally dependent in toileting would be appropriate.


104 SOC ROC DC M1845 Toileting Hygiene M1845 Toileting Hygiene Toileting hygiene includes several activities, including pulling clothes up or down and adequately cleaning (wiping) the perineal area. The focus is on the patient's ability to access needed supplies and implements, and manage hygiene and clothing once at the location where toileting occurs. The ability to access the toilet or bedside commode, transfer on and off the bedpan and to use the urinal are excluded from consideration when assessing the patient's toileting hygiene ability. Toileting hygiene includes the patient s ability to maintain hygiene related to catheter care and the ability to cleanse around all stomas that are used for urinary or bowel elimination (for example, urostomies, colostomies, ileostomies). The word assistance in this question refers to assistance from another person by verbal cueing/reminders, supervision, and/or stand-by or hands-on assistance. 415 M1845 Toileting Hygiene SOC ROC FU DC 416 M1850 Transferring Response 0 if the patient is independent in managing toileting hygiene and managing clothing. Response 1 if the patient is able to manage toileting hygiene and manage clothing IF supplies are laid out for the patient. If the patient can participate in hygiene and/or clothing management but needs some assistance with either or both activities, select Response 2. Includes standby assistance or verbal cueing.
105 M1850 Transferring M1850 Transferring Identifies the patient s ability to safely transfer from bed (current sleeping surface) to chair (and chair to bed), or position self in bed if bedfast. For most patients, the transfer between bed and chair will include transferring from a supine position in bed to a sitting position at the bedside, then some type of standing, stand-pivot, or sliding board transfer to a chair, and back into bed from the chair or sitting surface. If there is no chair in the patient s bedroom or the patient does not routinely transfer from the bed directly into a chair in the bedroom, report the patient s ability to move from a supine position in bed to a sitting position at the side of the bed, and then the ability to stand and then sit on whatever surface is applicable to the patient s environment and need, (for example, a chair in another room, a bedside commode, the toilet, a bench, etc.). Include the ability to return back into bed from the sitting surface. The need for assistance with gait may impact the Transferring score if the closest sitting surface applicable to the patient's environment is not next to the bed. 419 M1850 Transferring If your patient no longer sleeps in a bed (e.g. sleeps in a recliner or on a couch), you will assess the patient's ability to move from the supine position on their current sleeping surface to a sitting position and then transfer to another sitting surface, like a bedside commode, bench, or chair. Taking extra time and pushing up with both arms can help ensure the patient's stability and safety during the transfer process but does not mean that the patient is dependent. If standby human assistance were necessary to assure safety, then a different response level would apply. If they push up on tables, etc is the table an assistive device? 420 M1850 Transferring If the patient transfers either with minimal human assistance (but not device), or with the use of a device (but no human assistance), select Response 1. If the patient is able to transfer self from bed to chair, but requires standby assistance to transfer safely, or requires verbal cueing/reminders, select Response 1. For Response 1, minimal human assistance could include any combination of verbal cueing, environmental set-up, and/or actual hands-on assistance.
106 M1850 Transferring M1850 Transferring Response 1 Minimal human assistance could include any combination of verbal cueing, environmental set-up, and/or actual hands-on assistance, where the level of assistance required from someone else is equal to or less than 25% of the total effort to transfer and the patient is able to provide >75% of the total effort to complete the task. Examples of environmental set-up as it relates to transferring would be a patient who requires someone else to position the wheelchair by the bed and apply the wheelchair locks in order to safely transfer from the bed to the chair, or a patient who requires someone else to place the elevated commode seat over the toilet before the patient is able to safely transfer onto the commode. If the patient requires more than minimal assistance or requires both minimal human assistance and an assistive device to be safe, the appropriate score would be a 2. If the patient can bear weight and pivot, but requires more than minimal human assist, Response 2 should be marked. Able to bear weight refers to the patient's ability to support the majority of his/her body weight through any combination of weight-bearing extremities (for example, a patient with a weight-bearing restriction of one lower extremity may be able to support his/her entire weight through the other lower extremity and upper extremities). M1850 Transferring M1850 Transferring 423 The patient must be able to both bear weight and pivot for Response 2 to apply. If the patient is unable to do one or the other and is not bedfast, select Response 3. If the patient is bedfast, select Response 4 or 5, depending on the patient s ability to turn and position self in bed. Bedfast refers to being confined to the bed, either per physician restriction or due to a patient s inability to tolerate being out of the bed. 424 A patient who can tolerate being out of bed is not bedfast. If a patient is able to be transferred to a chair using a Hoyer lift, Response 3 is the option that most closely resembles the patient s circumstance; the patient is unable to transfer and is unable to bear weight or pivot when transferred by another person. Because he is transferred to a chair, he would not be considered bedfast ( confined to the bed ) even though he cannot help with the transfer. Responses 4 and 5 do not apply for the patient who is not bedfast. The frequency of the transfers does not change the response, only the patient s ability to be transferred and tolerate being out of bed.


107 SOC ROC GG0170C Or sofa, recliner or floor Mobility limitations can adversely affect wound healing and increase risk for the development of pressure ulcers. STEPS FOR ASSESSMENT Assess the patient s functional status based on direct observation and/or on report by the patient, caregiver/family. Patients should be allowed to perform activities as independently as possible, as long as they are safe. If caregiver assistance is required because patient's performance is unsafe or of poor quality, enter the response according to amount of assistance required to be safe. Activities may be completed with or without assistive device(s). Use of assistive device(s) to complete an activity should not affect the scoring of the activity. If the patient s self-care performance varies during the assessment time frame, report the patient s usual status, not the patient s most independent status and not the patient s most dependent status. GG0170C GG0170C 427 Enter 06 Independent, if the patient completes the activity by him/herself with no human assistance Enter 05 Setup or clean-up assistance, if the caregiver SETS UP or CLEANS UP; patient completes activity. Caregiver assists only prior to or following the activity, but not during the activity. For example, the patient requires assistance putting on a shoulder sling prior to the transfer, or requires assistance removing the bedding from off his/her lower body to get out of bed. Enter 04 Supervision or touching assistance, if the caregiver must provide VERBAL CUES or TOUCHING/ STEADYING assistance as patient completes activity. Assistance may be required throughout the activity or intermittently. For example, the patient requires verbal cueing, coaxing, or general supervision for safety to complete activity; or patient may require only incidental help such as contact guard or steadying assist during the activity. 428 Enter 03 Partial/moderate assistance, if the caregiver must provide LESS THAN HALF the effort. Caregiver lifts, holds, or supports trunk or limbs, but provides less than half the effort. Enter 02 Substantial/maximal assistance, if the caregiver must provide MORE THAN HALF the effort. Caregiver lifts or holds trunk or limbs and provides more than half the effort. Enter 01 Dependent, if the caregiver must provide ALL of the effort. Patient is unable to contribute any of the effort to complete the activity; or the assistance of two or more caregivers is required for the patient to complete the activity.
108 429 GG0170C If the patient does not attempt the activity and a caregiver does not complete the activity for the patient, report the reason the activity was not attempted. DO NOT USE THESE FOR DC GOAL Enter 07 Patient refused, if the patient refused to complete the activity. Enter 09 Not Applicable, if the patient did not perform this activity prior to the current illness, exacerbation, or injury. Code 88 Not attempted due to medical condition or safety concerns, if the activity was not attempted due to medical condition or safety concerns. If no information is available or assessment is not possible for reason other than above, enter a dash ( ) for 1-SOC/ROC Performance. A dash ( ) value is a valid response for this item. A dash ( ) value indicates that no information is available, and/or an item could not be assessed. This most often occurs when the patient is unexpectedly transferred, discharged or dies before assessment of the item could be completed. CMS expects dash use to be a rare occurrence. 430 GG0170C Discharge Goal The assessing clinician, in conjunction with patient and family input, can establish the discharge goal. Expected to make functional progress by discharge, the response reported for Discharge Goal will be higher (more independent) than the SOC/ROC Performance response. Not expected to make progress during the home health episode, but it is expected that the patient would be able to maintain his/her SOC functional level, the Discharge Goal response will be the same as the patient s SOC Performance response. If a patient with a progressive neurological condition is expected to rapidly decline, and that skilled therapy services may slow the decline of function, the Discharge Goal would be lower (more dependent) than the SOC/ROC Performance response. If the assessing clinician does not establish a Discharge Goal for the patient s bed mobility task, enter a dash ( ) for 2-Discharge Goal. 431 GG0170C Scoring Examples 432 GG0170C Scoring Examples 1. The patient pushes up from the bed to get himself from a lying to a seated position. The caregiver must provide steadying (touching) as the patient scoots himself to the edge of the bed and lowers his feet onto the floor. GG0170C1 SOC/ROC Performance: ENTER 04 Supervision or touching assistance Rationale: The patient required steadying/touching assistance in order to safely complete the task of lying on his back to sitting on the side of the bed. 2. The patient pushes up on the bed to attempt to get himself from a lying to a seated position as the OT provides much of the lifting assistance necessary for him to sit upright. The OT provides assistance as the patient scoots himself to the edge of the bed and lowers his feet to the floor. Overall, the OT must provide more than half of the effort to complete the task. GG0170C1 - SOC/ROC Performance: ENTER 02 Substantial/maximal assistance Rationale: The patient required the caregiver to provide lifting and assistance that represents more than half of the effort required to complete the task of lying on his back to sitting on the side of the bed.



109 GG0170C Scoring Examples GG0170C Scoring Examples The patient is obese and recovering from surgery for spinal stenosis with lower extremity weakness. The caregiver partially lifts the patient s trunk to a fully upright sitting position on the bed and minimally lifts each leg toward the edge of the bed. The patient then scoots toward the edge of the bed, placing both feet flat onto the floor. The patient completes most of the activity himself. GG0170C1 - SOC/ROC Performance: ENTER 03 Partial/moderate assistance Rationale: The patient required the caregiver to provide limited assistance that represents more than just verbal cues/touching/steadying, but less than half of the effort required to complete the task of lying on his back to sitting on the side of the bed The patient states he wishes he could get out of bed himself rather than depending on his wife to help. At the SOC the patient requires his wife to do most of the effort. Based on the patient s prior functional status, his current diagnoses, the expected length of stay, and his motivation to improve, the clinician expects that by discharge, the patient would likely only require assistance helping his legs off the bed to complete the supine to sitting task. GG0170C Scoring Examples Sleeping Surface 435 GG0170C1 - SOC/ROC Performance: ENTER 02 Substantial/maximal assistance GG0170C2 - Discharge Goal: Enter 03 Partial/moderate assistance Rationale: At the SOC, the patient required the caregiver to provide more than half of the effort required to complete the task. The assessing clinician and patient expect functional improvement so that by discharge the patient needs a caregiver to assistant, providing less than half of the effort. If the patient is not allowed to lay in a bed due to shoulder surgery but instead sleeps in a recliner, would we use code 88 or assess them in the recliner? If the patient s usual sleep surface is a recliner, the recliner can be considered the patient s bed for GG0170C. You would assess the patient's mobility in the recliner, treating the recliner as the bed.



110 Assistive Device If the patient sleeps in an electric recliner (which we are assessing as the patient s bed), and the patient pushes a button for the chair to return to a sitting position, is this considered assistance? If patients are able to use an assistive device themselves, the response code entered on the OASIS would be coded as a 06, Independent. Assistive Device Does Not Count If a patient uses a belt to go from lying to sitting on the side of the bed, but someone had to hand the belt to the patient, would that still be considered independent? For GG0170C, the use of an assistive device does not affect the scoring of the measure if the patient is able to perform the activity independently. If the patient usually requires a caregiver to hand them the assistive device to perform the activity, this would be scored as Code 5, Setup or clean-up assistance, because the patient requires setup assistance prior to performing the activity. Foresight is not 20/20 SOC ROC FU DC 440 M1860 Ambulation/Locomotion When the clinician chooses an answer for the goal on GG0170C2, is this just an opinion based on the assessment? Will it affect any outcomes if the goal chosen is not reached? The Discharge Goal score for GG0170C2 is a standardized item that is included in all post-acute care patient/resident assessment instruments. It is determined by the assessing clinician based on findings from the comprehensive assessment. The Discharge Goal is not expected to impact any of the home health quality measures in 2017, but may be used directly or indirectly in future quality measure calculation.
111 M1860 Ambulation/Locomotion M1860 Ambulation/Locomotion 441 Identifies the patient s ability and the type of assistance required to safely ambulate or propel self in a wheelchair over a variety of surfaces. Variety of surfaces refers to typical surfaces that the patient would routinely encounter in his/her environment, and may vary based on the individual residence. Regardless of the need for an assistive device, if the patient requires human assistance (hands on, supervision and/or verbal cueing) to safely ambulate, select Response 2 or Response 3, depending on whether the assistance required is intermittent ( 2 ) or continuous ( 3 ). 442 If the patient is safely able to ambulate without a device on a level surface, but requires minimal assistance on stairs, steps, and uneven surfaces, select Response 2 (requires human supervision or assistance to negotiate stairs or steps or uneven surfaces). If a patient does not require human assistance, but safely ambulates with a walker in some areas of the home, and a cane in other areas (due to space limitations, distances, etc.), select the response that reflects the device that best supports safe ambulation on all surfaces the patient routinely encounters (for example, Response 2 is appropriate if a walker is required for safe ambulation in the hallway and living room, even if there are some situations in the home where a cane provides adequate support.) M1860 Ambulation/Locomotion M1860 Ambulation/Locomotion 443 If a patient does not have a walking device but is clearly not safe walking alone, select Response 3, able to walk only with the supervision or assistance should be reported, unless the patient is chairfast. Responses 4 and 5 refer to a patient who is unable to ambulate, even with the use of assistive devices and/or continuous assistance. A patient who demonstrates or reports ability to take one or two steps to complete a transfer, but is otherwise unable to ambulate should be considered chairfast, and would be scored 4 or 5, based on ability to wheel self. Powered or manual version. 444 Note if the patient uses furniture or walls for support, or demonstrates loss of balance or other actions that suggest a need for additional support for safe ambulation. Observe patient s ability and safety on stairs. If a patient uses a wheelchair for 75% of their mobility and walks for 25% of their mobility, then should they be scored based on their wheelchair status because that is their mode of mobility >50% of the time? Or should they be scored based on their ambulatory status, because they do not fit the definition of chairfast? Item M1860 addresses the patient's ability to ambulate, so that is where the clinician's focus must be. Endurance is not included in this item. The clinician must determine the level of assistance is needed for the patient to ambulate and choose Response 0, 1, 2, or 3, whichever is the most appropriate.
112 M1860 Ambulation/Locomotion M1860 Ambulation/Locomotion My patient does not have a walking device but is clearly not safe walking alone. I evaluate him with a trial walker that I have brought with me to the assessment visit and while he still requires assistance and cueing, I believe he could eventually be safe using it with little to no human assistance. Currently his balance is so poor that ideally someone should be with him whenever he walks, even though he usually is just up stumbling around on his own. What score should I select for M1860? It sounds as though your assessment findings cause you to believe the patient should have someone with them at all times when walking (Response 3 ). When scoring M1860, clinicians should be careful not to assume that a patient, who is unsafe walking without a device, will suddenly (or ever) become able to safely walk with a device. Observation is the preferred method of data collection for the functional OASIS items, and the most accurate assessment will include observation of the patient using the device. Often safe use will require not only obtaining the device, but also appropriate selection of specific features, fitting of the device to the patient/environment and patient instruction in its use. My patient does not have an assistive device, but demonstrates the ability to walk safely constantly holding on to his caregiver. His neighbor loaned him a walker to try out during our assessment visit. My patient liked it and was safe walking on level surfaces with no help, but still needed help on the stairs. I have ordered a walker for the patient, and it will be delivered in 2 days. How do I score M1860 for the day of assessment? With or without the use of a walker? For M1860, the clinician must consider what the patient is able to do on the day of the assessment, which is the 24 hours that precedes the visit plus the time in the home. If at the time of assessment, (and prior to any teaching or interventions), the patient demonstrates the ability to ambulate safely with a walker and no assistance, then Response 2 - Requires use of a two-handed device to walk alone on level surfaces should be reported, as this is the patient s status on the day of assessment. This is true even if the walker does not belong to the patient and may not remain in the home. The clinician should not assume that the patient would be safe walking with a walker if no walker is available to allow assessment of the patient s status. April 2016 Q&A M1860 Ambulation/Locomotion M1860 Ambulation/Locomotion A patient is able to ambulate independently with a walker, but the patient chooses to not use the walker, therefore not being safe. Response #2, or Response #3? The OASIS items should report the patient s physical and cognitive ability, not their actual performance, adherence or willingness to perform an activity. You state the patient is able to ambulate independently with a walker, so we will assume you meant that the patient is able to ambulate without human assistance safely with the walker. This would be scored a 2 for M1860 Ambulation/Locomotion. You state the patient s actual performance is that he is unsafe ambulating because he chooses not to use his walker. This patient would still be scored a 2 unless, as you pointed out, the clinician identified some other physical, cognitive or environmental barrier that prevents the patient from utilizing his walker to assist with ambulation, e.g. fear, memory impairment, undisclosed pain associated with walker use, or other emotional, behavioral or physical impairments. If there was a barrier preventing the patient from safely utilizing the walker during ambulation, the clinician would need to determine if the patient needed someone to assist at all times in order to ambulate safely and if so, the appropriate score for M1860 would be a 3. If the patient only needed assistance intermittently, the correct response would be a 2. 4bQ Not safe even with assistance. 5-Chairfast, unable to ambulate and is unable to wheel self. Ambulates safely with a straight cane, but requires a stair lift to get up and down stairs in her home? If the patient requires no human assistance while ambulating and negotiating the stairs, but requires a stair lift to traverse the stairs safely, she would be scored a "2" for M1860 if she needs two hands to use the stair lift and a "1" if she only needs one hand to safely use the stair lift.


113 M1860 Ambulation/Locomotion Knee Scooter 449 Our patient requires maximum assistance to ambulate (over 75% of the effort necessary for ambulation is contributed by someone other than the patient) and only ambulates with the therapist during gait training activities. The patient is extremely unsafe when attempting to ambulate without the therapist s assistance. Still ambulatory Response 3 unless able to take only a few steps Minimal assistance (like in transferring) vs maximum assistance doesn t apply with ambulation 450 If a patient is safely using a knee scooter to facilitate non-weight bearing on one lower extremity, what response would be selected for M Ambulation? To determine the accurate response for M1860, the assessing clinician must determine if the knee scooter will be considered an assistive device for the purpose of ambulation. If the assessing clinician determines the knee scooter is an assistive device, then the clinician must determine if the patient is safe without the assistance of another person and assess the number of hands (one-hand or two-hands) the patient requires to safely use the device. One or Two Handed? How safe are they? Patient is wheelchair bound and cannot ambulate but can wheel self. Patient also has advanced dementia or cognitive decline and although the patient can wheel self independently, he/she is unable to do so with any purpose, (i.e., patient could not follow simple instructions to get to another room, or could not self-evacuate in the event of an emergency). What response should be selected? For M1860 Ambulation/Locomotion Responses 4 and 5, the assessing clinician must consider the non-ambulatory patient s ability to safely use the wheelchair, given the patient s current physical and mental/emotional/cognitive status, activities permitted, and environment. In the scenario cited, the patient s advanced dementia/cognitive decline is noted as a concern because the patient is unable to wheel self with purpose. Other than addressing safety on surfaces the patient would routinely encounter in their environment, CMS guidance does not detail specific criteria regarding patient ambulation or wheelchair use (i.e., how far the patient must walk, or wheel self; of if they use ambulation or wheelchair mobility with specific purpose, regularity, or efficiency). It is left to the judgment of the assessing clinician to determine the patient s ability (i.e., does the patient s mental status impacted his/her safety?) and select a response accordingly.



114 SOC ROC DC M1870 Feeding or Eating M1870 Feeding or Eating Excludes preparation of food items, and transport to the table. Based on the assistance needed by the patient to feed himself once the food is placed in front of him. Meal "set-up" (Response 1) includes activities such as mashing a potato, cutting up meat/vegetables when served, pouring milk on cereal, opening a milk carton, adding sugar to coffee or tea, arranging the food on the plate for ease of access, etc. -- all of which are special adaptations of the meal for the patient. 455 M1870 Feeding or Eating 456 SOC ROC DC M1880 Plan and Prepare Light Meals If a tube is being used to provide all or some nutrition, select Responses 3 or 4, depending on the patient s ability to take in nutrients orally. If a patient is being weaned from tube feeding, Responses 3 or 4 will continue to apply until the patient no longer uses the tube for nutrition, at which time, select Responses 0, 1, or 2. This is true, even if the tube remains in place, unused for a period of time. Responses 4 and 5 include non-oral intake. Response 5 is the best response for patients who are not able to take in nutrients orally or by tube feeding. This may be the case for patients who receive all nutrition intravenously (such as TPN) or for patients who are receiving only intravenous hydration. Ability to plan and prepare meals once the patient is in the meal preparation location.

 indicates the patient has the consistent physical and cognitive ability to plan and prepare meals.")
115 457 M1880 Current Ability to Plan and Prepare Light Meals Identifies the patient s physical, cognitive, and mental ability to plan and prepare meals, even if the patient does not routinely perform this task. In cases where a patient s ability is different for various light meal preparation tasks, pick the response that best describes the patient s level of ability to perform the majority of light meal preparation tasks. Response 0 (Able) indicates the patient has the consistent physical and cognitive ability to plan and prepare meals. Response 1 (Unable on a regular basis) indicates the patient has inconsistent ability to prepare light meals (for example, can t prepare breakfast due to morning arthritic stiffness, but can prepare other meals throughout day). Also if the patient has a newly prescribed diet Response 2 indicates patient does not have the ability to prepare light meals at any point during the day of assessment. 458 M1880 Current Ability to Plan and Prepare Light Meals While nutritional appropriateness of the patient s food selections is not the focus of this item, any prescribed diet requirements (and related planning/preparation) should be considered when selecting a response. When a patient s prescribed diet consists either partially or completely of enteral nutrition, the clinician must assess the patient s ability to plan and prepare their prescribed diet, including their knowledge of the feeding amount and ability to prepare the enteral feeding, based on product used. (Not including management of equipment) 459 SOC ROC M1900 Prior Functioning ADL/IADL 460 M1900 Prior Functioning ADL/IADL Timepoints: SOC ROC Specifically tub, shower, commode, and bed to chair transfers Independent means that the patient had the ability to complete the activity by him/herself (with or without assistive devices) without physical or verbal assistance from a helper. Needed some help means that the patient contributed effort but required help from another person to accomplish the task/activity safely. Dependent means that the patient was physically and/or cognitively unable to contribute effort toward completion of the task, and the helper must contribute all the effort. Wheelchair (with or without assistance) would be reported as Dependent in Ambulation If the patient was previously independent in some self-care tasks (or some transfers, or some household tasks), but needed help or was completely dependent in others, pick the response that best describes the patient s level of ability to perform the majority of included tasks.


116 461 SOC ROC M1910 Falls Risk Assessment Best Practice item MAHC-10 Fall Risk Assessment tool meets criteria of multi-factor, standardized, validated 462 M1910 Falls Risk Assessment For Responses 1 and 2, an agency may use a single comprehensive multi-factor falls risk assessment tool that meets the criteria as described in the item intent. Alternatively, an agency may incorporate several tools as long as one of them meets the criteria as described in the item intent. Use the scoring parameters specified in the tool to identify if a patient is at risk for falls. Response 1 if the standardized, validated response scale rates the patient as no-risk, low-risk, or minimal risk. Response 2 if the standardized, validated response scale rates the patient as anything above low/minimal-risk. If the tool does not provide various levels, but simply has a single threshold separating those at risk from those not at risk, then the patient scoring at risk should be scored as Response M1910 Falls Risk Assessment Medications In order to select Response 1 or 2, the falls risk assessment must be conducted by the clinician responsible for completing the comprehensive assessment during the time frame specified by CMS for completion of the assessment. Select Response 0 if: a standardized, validated multi-factor falls risk screening was NOT conducted by the home health agency, a standardized, validated multi-factor falls risk screening was conducted by the home health agency but NOT during the required assessment time frame, a standardized, validated multi-factor falls risk screening was conducted during the assessment time frame, but NOT by the assessing clinician. the patient is not able to participate in tasks required to allow the completion and scoring of the standardized, validated assessment(s) that the agency chooses to utilize. SOC and ROC Transfer and DC
.")
117 SOC ROC M2001 Defining Clinically Significant A potential clinically significant medication issue is an issue that in the care provider s clinical judgment, requires physician/physician-designee notification by midnight of the next calendar day (at the latest). The drug regimen review includes all medications, prescribed and over the counter (including TPN and herbals), administered by any route (for example, oral, topical, inhalant, pump, injection, intravenous and via enteral tube). Potential or actual clinically significant medication issues may include but are not limited to: adverse reactions to medications (such as a rash), ineffective drug therapy (analgesic that does not reduce pain), side effects (potential bleeding from an anticoagulant), drug interactions (serious drug-drug, drug-food and drugdisease interactions), duplicate therapy (generic name and brand name equivalent drugs are both prescribed), omissions (missing drugs from an ordered regimen), dosage errors (either too high or too low), and nonadherence (regardless of whether the nonadherence is purposeful or accidental). Bottom Line 3 Levels 467 Any of these circumstances listed above must reach a level of clinical significance that warrants notification of the physician/physician-designee for orders or recommendations by midnight of the next calendar day, at the latest. Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medication issue. 468 Drug regimen review activities we can address ourselves without physician intervention Drug regimen review activities we need to address with the physician, but not necessary by midnight of next calendar day Those issues which require physician input asap.

118 Your Judgment Upon discharge from the hospital, on the discharge summary the medication list is frequently documented. They are listed in sections under start taking these medications, continue taking these medications, and stop taking these medications. They have been reviewed by a physician. If the patient is taking any medications that have the potential to cause a significant issue, such as two different blood pressure medicines or pain medications, do we still notify the physician, even though the specific medications are documented on the discharge summary, and that has been reviewed already by a physician? As part of the OASIS assessment, it is the responsibility of the clinician to conduct the review on SOC/ROC and notify the responsible physician of any potential clinically significant issues. 470 M2001 Not Just Med Rec The drug regimen review in post-acute care is generally considered to include medication reconciliation, a review of all medications a patient is currently using and review of the drug regimen to identify, and if possible, prevent potential clinically significant medication issues. The drug regimen review includes all medications, prescribed and over the counter (including TPN and herbals), administered by any route (for example, oral, topical, inhalant, pump, injection, intravenous and via enteral tube). M2001 Collaboration SOC ROC M If portions of the drug regimen review (for example, identification of potential drug-drug interactions or potential dosage errors) are completed by agency staff other than the clinician responsible for completing the SOC/ROC OASIS, information on drug regimen review findings must be communicated to the clinician responsible for the SOC/ROC OASIS assessment so that the appropriate response for M2001 may be entered. Collaboration in which the assessing clinician evaluates patient status (for example, presence of potential ineffective drug therapy or patient nonadherence), and another clinician (in the office) assists with review of the medication list (for example, possible duplicate drug therapy or omissions) does not violate the requirement that the comprehensive patient assessment is the responsibility of and must be ultimately completed by one clinician. Agency policy and practice will determine this process and how it is documented. The M0090 date the date the assessment is completed would be the date the two clinicians collaborated and the assessment was completed.
 (still 2 way communication) Multiple")

119 Definition M2003 YES Two-way communication AND completion of the prescribed/recommended actions must have occurred by midnight of the next calendar day after the potential clinically significant medication issue was identified No new orders or instruction in response to timely reported potential clinically significant medication issue(s) (still 2 way communication) Multiple potential clinically significant medication issues identified-- all must be communicated to the physician/physician-designee, with completion of all prescribed/recommended actions occurring by midnight of the next calendar day. If the physician/physician-designee recommends an action that will take longer than the allowed time to complete, as long as by midnight of the next calendar day the agency has taken whatever actions are possible to comply with the recommended action. 475 M2003 Examples of recommended actions that would take longer than the allowed time to complete might include physician instruction to agency staff to continue to monitor the issue over the weekend and call if problem persists, or the physician instructs the patient to address the concern with his PCP on a visit that is scheduled in two days The actual type of actions recommended should be considered in determining if the agency has taken whatever actions are possible by midnight of the next calendar day. 476 M2003 NO If two potential clinically significant medication issues are identified at the SOC/ROC, both are communicated to the physician/physician-designee timely, and the physician/physician-designee provides a recommended action for each issue (for example, patient education for one medication, and a new dosage for another), if both recommended actions could have been addressed by midnight of the next calendar day, but only one was addressed. If a potential clinically significant medication issue was identified, and the clinician attempted to communicate with the physician, but did not receive communication back from the physician/physician designee until after midnight of the next calendar day
, do you still notify the doctor of a potential issue?")

120 Missing a RX On the SOC or ROC assessment, if the patient is missing a prescribed medication and unable to obtain it from the pharmacy (for example, due to the pharmacy being closed or a transportation issue), do you still notify the doctor of a potential issue? Is a follow-up phone call to the patient sufficient enough to ask if they did indeed obtain the medicine, or would a visit need to be made? Depending on the situation, the assessing clinician might determine that absence of a medication is a clinically significant issue appropriate for timely physician contact. A potential clinically significant medication issue is an issue that in the care provider s clinical judgment requires physician/physician-designee notification by midnight of the next calendar day (at the latest). Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medication issue. If a medication-related problem is identified and resolved by the agency staff (not requiring physician/physician-designee contact by midnight of the next calendar day), the problem does not need to be reported as an existing clinically significant problem in M2001. The manner in which the agency validates the resolution is a clinical practice question for the agency to determine. 478 Practice An issue regarding the refusal to take a medication is found during the drug regimen review, and in the assessing clinician s judgment she can resolve the problem with teaching. On the third day after SOC, the issue is not resolved. She then calls the physician who changes the medication on the 4 th day. How should M2001 be marked? A No issues found during the review B Issues found during the review C Patient is not taking any medications What about M2003? A No B Yes Midnight Comes Early at ROC TRN DC DAH M2005 ROC OASIS must be completed within 48 hours of patient discharge from facility or the agency being aware of the patient being discharged from a facility. If the OASIS assessment is done on the second day (hours 25 48) and a medication issue is identified, does the clinician still have until midnight of the following day to resolve the issue, or does the issue need to be resolved before the 48th hour is complete? 480 M2003, Medication Follow-up must also be answered within the timeframe allowed at the SOC/ROC to ensure compliance with the Conditions of Participation regarding the completion of the comprehensive assessment. If a medication problem is identified at SOC or ROC, physician communication and completion of prescribed/recommended actions must occur by midnight of the next calendar day after identification and before the end of the allowed assessment timeframe.
121 Example Quality Episodes 481 SOC ROC Issue resolved by nurse Physician responded Issue Physician did not respond TRN DC DAH Each time that an issue is found and rises to the level which requires physician intervention, was the physician notified, and did the physician respond (each time). M2005 states since SOC/ROC. Does that mean at the time of or since SOC/ROC? If the intent of the question was to go back to the SOC, why would ROC be in the question? Quality episodes can be calculated from a start of care or a resumption of care to the end of the care episode (transfer to an inpatient facility, discharge from the agency, or death). In completing M2005 at Transfer, Death or Discharge, you must review the documentation from that time point back to the time of or at any time since the most recent Start of Care or Resumption of Care. Use Your Judgment RN or Therapist?? How do we answer this item for a compliant degenerative joint disease patient who was noted to have pain symptoms of 4/10 (per patient) on SOC, who already is on a new narcotic analgesic during the past week? With this symptom, can we answer 0 = No, no issues found during review if we think this issue does not necessitate notifying the physician by midnight of the next business day? A potential clinically significant medication issue is an issue that in the care provider s clinical judgment requires physician/physician-designee notification by midnight of the next calendar day (at the latest). Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medication issue. Is it required that an RN do the drug regimen review in cases of therapy-only home health episodes? The RN is not required to do the drug regimen review in therapy-only home health episodes. The comprehensive assessment must include a review of all medications the patient is using in order to identify any potential adverse effects and drug reactions, including ineffective drug therapy, significant side effects and drug interactions, duplicate drug therapy, and noncompliance with drug therapy. Each agency must determine the capabilities of current staff members to perform comprehensive assessments, taking into account professional standards or practice acts specific to your State. No specific discipline is identified as exclusively able to perform this assessment. According to Federal guidelines, only RNs, physical therapists (PTs), occupational therapists (OTs), and speech and language pathologists (SLPs) are qualified to perform comprehensive assessments and collect OASIS data. In cases of therapy-only services, where the scope of practice for the therapist is limited by State, agency, or other policies/restrictions, the agency may instruct that the therapist collaborate with nursing to complete the drug regimen review.


122 RN or Therapist Dash Please clarify the difference between the national and State--level requirements regarding whether therapists are qualified to conduct medication reviews. The requirements presented in the OASIS and OASIS Guidance are Federal requirements. The comprehensive assessment must include a review of all medications the patient is using in order to identify any potential adverse effects and drug reactions, including ineffective drug therapy, significant side effects and drug interactions, duplicate drug therapy, and noncompliance with drug therapy. Each agency must determine the capabilities of current staff members to perform comprehensive assessments, taking into account professional standards or practice acts specific to your State. States may have more stringent guidance, and State-specific queries should be addressed to the appropriate State agency. No specific discipline is identified as exclusively able to perform this assessment. According to Federal guidelines, only RNs, PTs, OTs, and SLPs are qualified to perform comprehensive assessments and collect OASIS Data. There may be times because of an agency process that the drug regimen review is not completed within the assessment timeframe. Would that be an instance when a dash is used? A dash is expected to be a rare occurrence and indicates that no information is available and/or an item could not be assessed. This most often occurs when the patient is unexpectedly transferred, discharged, or dies before assessment of the item could be completed. Agencies must ensure that their processes are not a barrier to complete a drug regimen review within the given timeframe and should adjust their processes to ensure that a drug regimen review is completed as required. Physician does not respond 488 TRN DC M2016 If we are unable to resolve a medication issue before midnight of the next calendar day due to no physician reply, how is that reflected within the reporting structure for M2003 and M2005? How does it differentiate a no physician reply vs. no agency action? Moreover, what are the implications, if any, for the agency and/or the physician for a pattern of non-adherence to this best practice? M2001 does not offer the option of Drug regimen review not done. To answer M2003 and M2005, the review must be done. M2003 asks if the physician was contacted and the actions completed. If no issues were identified, there is no need to contact the physician; if issues were found, the communication and response are both needed. Selecting No for M2003 and M2005 indicates that the best practice of identifying a medication issue, reporting it to the physician, and completing the recommended/prescribed actions possible by midnight of the next calendar day was not accomplished. The item response choices for M2003 and M2005 do not identify the reason why the best practice was not met.


123 SOC ROC DC 489 M2020 Management of Oral Medications 490 M2020 Management of Oral Medications If patient s ability to manage oral meds varies from medication to medication, consider the medication for which the most assistance is needed when selecting a response. If the medication is ordered prn, and on the day of assessment the patient needed a reminder for this prn, then the patient would be a "2". If on the day of assessment, the patient did not need any prn medications, therefore no reminders, then assess the patient's ability on all of the medications taken on the day of assessment. Ch M2020 Management of Oral Medications Assess patient s ability to take medications reliably and safely at all times Identifies patient s ability, not willingness or compliance or actual performance Ability can be temporarily or permanently limited by: Physical impairments (e.g. limited manual dexterity) Emotional/cognitive/behavioral impairments (e.g., memory deficits, impaired judgment, fear) Sensory impairments, (e.g., impaired vision, pain) Environmental barriers (e.g. access to kitchen or medication storage area, stairs, narrow doorways) 492 M2020 Management of Oral Medications Includes all prescribed and OTC oral meds included on the POC Excludes topical, injectable and IV meds Excludes inhalation meds and sublingual meds (Oct 2012) Excludes swish and expectorate meds (Jan 2013) Meds given per gastrostomy or other tube are not po 4b-Q167.8 Does not include filling/reordering 4b-Q166 Swallow and absorbed through GI system!!
124 493 M2020 Management of Oral Medications Response 0 Patient sets up her/his own planner device and is able to take the correct med in the correct dosage at the correct time Response 1 Patient is independent in oral med administration, but requires another person to prepare individual doses (e.g., sets up a planner device) And/or if another person develops a drug diary or chart which the patient relies on to take meds appropriately 494 M2020 Management of Oral Medications Response 2 Patient requires another person to provide reminders What about a device that provides reminders? Who sets up the device? 4b-Q Examples of Response 3 4b Q A patient who decided not to take her new medications, because the varying doses worried her, and she was unsure of the instructions. There had not been a medi-planner set up, nor reminders tried. The clinician would select Response 3 because it is unclear until reassessment if the interventions will be successful. A patient who, upon assessment, was not able to take prescribed medications at the correct time and doses even though reminded. A patient who, on the day of assessment, was prescribed oral medications, but was unable to safely swallow. The patient is on multiple medications which span 3 times a day. Yesterday, the doctor started her on a varying dose of Prednisone. The patient admits to being confused about the directions and right dosage. The clinician observes that the med box the patient set up is filled correctly with all usual medications, but not correctly with the prescribed Prednisone administration. The clinician also notes that the medication for last evening remained in the pill planner. Upon questioning, the patient admits to being tired and forgetting to take her evening medication. The nurse discusses the use of an alarm clock to remind her to take her evening medication and fixes the Prednisone dosage for the rest of the week. Considering this patient needed help with setting up one medication (Response 1) and a reminder for another (Response 2) in the last 24 hrs, what is the correct scoring with rationale for this situation? 4b-Q
125 "3-Unable to take medication unless administered by another person because on the day of the assessment, the patient did not possess the ability to take the Prednisone at the correct time and dose and demonstrated that through her report and actions (required knowledge of the drug's dose and administration schedule ) Rationale: Day of assessment Do not report ability after skilled intervention, as this is not a reflection of what was true in the most dependent medication during the day of assessment. The patient has to demonstrate success at taking meds as ordered, at all times to move from a M2020 If the patient does not have her prescribed medications in the home because she cannot afford them and she does not plan on getting them, what is the most appropriate response for M2020? 4b-Q M2020 You are reporting the patient's ability to take all oral medications reliably and safely at all times on the day of the assessment. If the patient did not take her medications on the day of the assessment because they were not present in the home, you cannot make assumptions about a patient's ability to take medications she doesn t have. If the medications were not in the home, you would not be able to determine if she could take each medication at the correct time and dose. The patient's status would be reported as 3-Unable to take medications unless administered by another person. 500 Quiz Mrs. Wobble is unsteady while ambulating and requires supervision for ambulation. She possesses the knowledge to take her medications reliably and safely if the bottles are placed near, or if she has supervision while ambulating to the medication storage area. Please advise how this patient would be scored for M2020, Management of Oral Medications. The item intent instructions include guidance related to the patient s ability to access the medication, how does this play into the question when the physical impairment causes the patient to require human supervision or assistance and not the cognitive aspect (such as for reminders)? 4b-Q

 that are required for the patient to access and/or take the medication at the prescribed times, then the patient would NOT be")
126 Answer More Scenarios 501 M2020 reports a patient's ability on the day of the assessment to take the correct oral medications at all the correct times. This would include the tasks of accessing the medications from the location where they are routinely stored in the home, preparing the medications (including opening containers or mixing oral suspensions), selecting the correct dose and safely swallowing the medications, typically involving having access to a beverage. If someone other than the patient must do some part of the task(s) that are required for the patient to access and/or take the medication at the prescribed times, then the patient would NOT be considered independent (Response 0). 502 Scenario: Medications are routinely stored in the refrigerator located downstairs. The patient requires someone to assist them at medication administration time to walk to the location where the medications are routinely stored, or someone must retrieve the medications and bring them to the patient; Response "3" would apply. In this situation, just someone preparing the doses in advance did not enable the patient to self-administer their medications. Scenario: The patient requires someone to prepare the medication doses in advance (e.g. visually they can't discern the appropriate dose) and to walk with them at all times to be safe. Someone prepares the medi-planner and sets it within the patient's reach with the water they need to take the meds, the appropriate score is a "1", as the patient can access the medications from where they are routinely stored and has the water available to swallow the medication safely. 4b- Q More Scenarios If the medications were routinely stored in the kitchen and/or the water was not available for the patient to selfadminister and the patient required someone to assist them to the location where the meds were stored and or to water, the appropriate score would be a "3". Scenario: Patient does not need doses prepared in advance, but the medications are routinely stored in a location that the patient cannot access due to a physical, sensory, or environmental barrier. The patient is scored a "3". During the episode, an environmental modification was made, e.g. changing the medication storage and water supply to a location that the patient can access, the patient could be scored a "0" at the next OASIS data collection time point. 4b-Q SOC ROC FU DC 504 M2030 Management of Injectable Medications
127 505 M2030 Management of Injectable Medications Assess patient s ability to take all injectable meds reliably and safely at all times Excludes IV medications Infusions (i.e. meds given via pump) Meds given in the physician s office or other settings outside the home 4b-Q M2030 Management of Injectable Meds Response -0 Patient sets up own meds with correct med, dose and time Response -1 Patient independent in injectable med administration except that another person must prepare doses and/or if another person must develop a drug diary or chart Response -2 Reminders to take meds are necessary, regardless of whether the pt is independent or needs assistance in preparing individual doses and/or developing a drug diary or chart. Note: Reminders provided by a device that the patient can independently manage are not considered assistance or reminders 507 M2030 Management of Injectable Meds Response 3 Unable to take medication unless administered by another person The physician orders the nurse to administer the medication (represents a medical restriction against self-administration) if not for convenience 4b-Q168.2, If injectables are not in the home (whether currently due, due at a future point during the episode or prn) Response 3 - Unable to take injectable medication unless administered by another person is appropriate. If an injection is ordered but not administered the day of assessment, the clinician will use the assessment of the patient s cognitive and physical ability and make an inference regarding what the patient would be able to do. 4b-Q M2030 Management of Injectable Medications If patient s ability to manage injectable meds varies from medication to medication, consider the medication for which the most assistance is needed when selecting a response. The patient administers his own insulin safely and reliably but his doctor has ordered B12 IM. What response? 4b-Q168.4 What if the doctor wants the patient to come into his office for the IM injection? The doctor orders that the patient receive a flu vaccine?? 4b-Q





128 What does M2030 include? M2030 at Discharge 509 M2030 requires an assessment of the patient's cognitive and physical ability to draw up the correct dose accurately using aseptic technique, inject in an appropriate site using correct technique, and dispose of the syringe properly." My patient, at the SOC, was throwing his used needles and syringes into the trash. He stated he was never told how to properly dispose of them. 4b-Q If the patient lacked the knowledge regarding safe needle and syringe disposal on the day of the assessment, the patient was unable to take injectable medication unless administered by another person, Response 3. If the patient needed reminders regarding safe needle/syringe disposal, they would be scored a "2". 510 Scenario 1: The first two weeks of the episode, the patient had Lovenox SQ ordered. The patient is being discharged 4 weeks later with no injectable medications currently ordered. At discharge, is the answer NA - no injectable medications prescribed or do we assess their ability from earlier in the episode? Scenario 2: Is the order to administer the flu vaccine at the beginning of the episode included when selecting a response for M2030 at the Discharge assessment? Answer to both: If there are no current, ongoing orders for an injectable to be administered IM or SQ via needle and syringe in the home at the time of the assessment, the appropriate response is NA. 4b-Q SOC ROC DC M
129 513 Comparing ADL items to M Medicare s Answer We have a patient, who at discharge is able to bathe in the shower with assist of her daughter, however she prefers to sponge bathe at the sink and is able to do so independently now. The clinician has marked response 2 for M1830 to reflect her ability to perform safely. The question is should the clinician answer M2102a (caregiver assistance with ADLs) Response 1, reflecting assistance needed for showering as answered in M1830 or can the clinician choose response 0 no assistance needed because the patient is able to sponge bathe independently and safely. The patient is able to do all other ADLs independently. The clinician s documentation in the clinical record reports patient s preference with bathing. Our software system does give a warning if the response for M2102a is not consistent with the M18xx ADL questions/responses. However, it will allow the clinician to mark a different response, I just want to know the correct way to answer the question. M1830 addresses the patient s ability to bathe in the shower or tub, not actual performance, regardless of where or how the patient currently bathes. Willingness and adherence are not the focus of the item. If assistance is needed to bathe in the shower or tub, then the level of assistance needed must be noted, and Response 1, 2, or 3 should be selected. M2102 is based on the ability and willingness of the caregiver(s) (other than home health agency staff) to provide the assistance needed by the patient to perform ADLs, including bathing. The item does not specify the bathing must be in the tub or shower. In the scenario cited, the assessing clinician has determined the patient to be independent in all ADLs, including bathing. Therefore, a response of "0" for M2102a. would be appropriate. 515 M2102 Medications and Procedures/Treatments Row c Medication administration refers to any type of medication (prescribed or OTC) and any route of administration including oral, inhalant, injectable, topical, or administration via g-tube/j-tube, etc. Row d Medical procedures/treatments include procedures/treatments that the physician or physiciandesignee has ordered for the purpose of improving health status. Some examples of these procedures/treatments include wound care and dressing changes, range of motion exercises, intermittent urinary catheterization, postural drainage, electromodalities, etc. Devices such as TED hose, prosthetic devices, orthotic devices, or other supports that have a medical and/or therapeutic impact should be considered medical procedures/treatments, not as ADL/dressing items in Row a. 516 Equipment, Safety, Advocacy Row e Management of equipment refers to the ability to safely use medical equipment as ordered. Examples of medical equipment include oxygen, IV/infusion equipment, enteral/parenteral nutrition, ventilator therapy equipment or supplies, continuous passive motion machine, wheelchair, hoyer lift, etc. Flush only = syringe Row f Supervision and safety includes needs related to the ability of the patient to safely remain in the home. This category of assistance needs includes a wide range of activities that may be necessary due to cognitive, functional, or other health deficits. Such assistance may range from calls to remind the patient to take medications, to in-person visits to ensure that the home environment is safely maintained, to the need for the physical presence of another person in the home to ensure that the patient doesn t wander, fall, or for other safety reasons (for example, leaving the stove burner on). Row g Advocacy or facilitation of patient's participation in appropriate medical care includes taking patient to medical appointments, following up with filling prescriptions, or making subsequent appointments, etc.
 to meet that need.")
130 M2102 Generally Quiz If patient needs assistance with any aspect of a category of assistance (such as needs assistance with some IADLs but not others), consider the aspect that represents the most need and the availability and ability of the caregiver(s) to meet that need. If more than one response in a row applies, (for example, the caregiver(s) provides the assistance but also needs training or assistance), select the response that represents the greatest need ( caregiver(s) needs training/supporting services to provide assistance ). Response 3 if: Caregiver(s) not likely to provide indicates that the caregiver(s) has indicated an unwillingness to provide assistance, or that the caregiver(s) is/are physically and/or cognitively unable to provide needed care. Unclear if caregiver(s) will provide indicates that the caregiver(s) may express willingness to provide care, but their ability to do so is in question or there is reluctance on the part of the caregiver(s) that raises questions as to whether the caregiver will provide the needed assistance. I have a patient who has just started chemotherapy with IV access present. She is unable to take oral medications or food and has a gastrostomy tube that is being flushed with water to maintain patency. The patient is scheduled to return to the physician in two weeks for further assessment and to obtain enteral nutrition orders. How do I score M1030, M2020, M2102 at SOC? M1030, Therapies at Home - If the patient's IV access for the chemotherapy was ordered to be flushed in the home, Response 1 would be appropriate, otherwise it would be 4-NA, as the patient is not receiving one of the listed therapies at home. M2020, Management of Oral Medications, would be NA-No oral medications prescribed. M2102, Types and Sources of Assistance, e. Management of Equipment - Even though the patient's g-tube is only being flushed with water to maintain patency until the feeding is ordered, the patient/cg must maintain the enteral nutrition equipment, so it would be appropriate to assess and report the level of caregiver ability and willingness to provide assistance with managing the equipment. M Not Used Generally SOC ROC FU M2200 Therapy Need M2102. How is "Assistance needed, but no Caregiver(s) available" defined? Would it apply to a son who is managing equipment and assists with ADLs safely and independently, but is unwilling to assist with medication administration and is unable to take the patient to doctor's appointments? "4 - Assistance needed, but no non-agency caregiver(s) available" means the patient has no one involved in providing any level of care to them at all. In your example, the patient has a son who is providing some level of caregiver assistance; therefore, Response 4 would not be an appropriate response. If the son was willing and able to manage equipment and assist with ADLS, the appropriate responses for Row a and Row e would be "1- Non-agency caregiver(s) currently provide assistance". If the son was unwilling to assist with medication administration and unable to take the patient to doctor's appointments, the appropriate responses for Row c, Medication administration and Row g, Advocacy or facilitation would be " Response 3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will provide assistance because this response is defined as including situations where the caregiver is unwilling or unable to provide the needed care. 4b Q
131 M2200 Therapy Need M2200 Therapy Need 521 Therapy visits must Relate directly and specifically to a treatment regimen ordered by physician Be reasonable and necessary to the treatment of the patient s illness or injury Answer 000 if no therapy services are needed Answer NA when this assessment will not be used to determine a case mix group for Medicare, or other payers using a Medicare PPS-like model 522 How many combined therapy visits? Social work does not count as a therapy If therapy services are ordered, how many total visits are indicated over the 60-day payment episode? If number is uncertain, provide best estimate. Medicare will adjust both up and down based on the actual number of visits provided. Example You believe patient needs 6 therapy visits at the beginning of episode. You are paid RAP based on 6 therapy visits. Patient falls in episode and ends up with 16 visits. You will be paid final claim based on 16 visits. 523 How to Answer at ROC ROC in the last 5 days of the episode Answer based on estimated need for therapy in the next episode. ROC any other time in the episode Answer any way you d like (doesn t impact payment). Number of therapy visits in episode Number of therapy visits left to do NA No HHRG is needed (dependent on software) 000 4b-Q What if M0110 and M2200 are wrong? No action required. May correct M0110 by a narrative. 4b Claims will automatically be adjusted so CMS expects no extraordinary efforts to be taken after SOC, ROC or Follow up to ensure M0110 or M2200 is correct. Other Follow-up assessment is only required if your policy requires (Is it a major decline or improvement in the patient s condition?) 4b-Q23.18



 then becomes the date of the communication with the physician to")
132 525 M2250 AND M2401 Process Measures 526 SOC ROC M2250 Plan of Care Synopsis Step 1: Can you select Yes? Step 2: If you can t select yes, can you select NA? Step 3: If not yes, and not. NA, then select No M2250 Purpose Time Limits and M Identifies if the physician-ordered home health Plan of Care incorporates specific best practices. Included in the physician-ordered Plan of Care means that the patient condition has been discussed and there is agreement as to the Plan of Care between the home health agency staff and the physician. This question can be answered Yes prior to the receipt of signed orders if the clinical record reflects evidence of communication with the physician to include specified best practice interventions in the Plan of Care. Assuming all other OASIS information is completed, the Date Assessment Completed (M0090) then becomes the date of the communication with the physician to establish the Plan of Care that includes interventions listed in M Plan of Care orders must be in place within five days for SOC in order to respond Yes. For ROC, the Plan of Care orders must be in place within two days of inpatient discharge, or within two days of becoming aware of an inpatient discharge, in order to respond Yes to M2250.

133 529 M2250 at ROC If the ROC comprehensive assessment with OASIS was completed after the CMS-allowed 48 hour time frame, do all the best practice questions need to be answered NA? The ROC comprehensive assessment must be completed within 48 hours of discharge following a qualifying inpatient stay or within 48 hours of knowledge of a qualifying stay in an inpatient facility. If the ROC assessment is late, "Yes" may still be selected for the best practices in M2250, Plan of Care Synopsis, if the relevant orders were present within the 48 hour ROC time frame. If not present by the end of the 48 hour time frame, answer No, unless NA. 4bQ M2250 Plan of Care Synopsis SOC ROC For rows c-f: A formal or informal assessment can result in an NA response. 531 M2250 Plan of Care Synopsis SOC ROC 532 M2250 at SOC/ROC Select No when an order for the criteria of a best practice intervention has not been obtained within the assessment timeframe and NA does not apply.
 for a best practice intervention( s) AND 2. Evidence of implementati on of the order(s).")


134 Select Yes when at the time of or at any time since the most recent SOC/ROC assessment there is both: 1. An order(s) for a best practice intervention( s) AND 2. Evidence of implementati on of the order(s) Select NA when these criteria are met during the look back period. Rows b e: a FORMAL assessment must indicate a negative/no risk result If more than one assessment done during look back time period, all must be negative. 536 M2401 Select No when at the time of or since the most recent SOC/ROC assessment an order for the criteria of a best practice intervention(s): 1. Has not been obtained and/or 2. Has not been implemented and NA does not apply. 535
135 M2250 Patient Parameters M2250 Depression Screening 537 YES--If the Plan of Care includes specific parameters ordered by the physician for this specific patient or after reviewing the agency's standardized parameters with the physician, s/he agrees they would meet the needs of this specific patient, select Yes. NO--If there are no patient-specific parameters on the Plan of Care and the agency will not use standardized physician notification parameters for this patient, select No. NA--If the agency uses their own agency standardized guidelines, which the physician has NOT agreed to include in the Plan of Care for this particular patient, select NA. 538 YES-- If the physician-ordered Plan of Care contains orders for further evaluation or treatment of depression, AND/OR if the physician has been notified about a positive depression screen Examples of interventions for depression may include new or existing medications, adjustments to already-prescribed medications, psychotherapy, or referrals to agency resources (for example, social worker). If the patient is already under physician care for a diagnosis of depression, interventions may include monitoring medication effectiveness, teaching regarding the need to take prescribed medications, etc. NA If the patient has no diagnosis of depression AND does not meet criteria for further evaluation based on a formal or informal depression assessment, select NA (unless the physician has been notified about a positive depression screen, or orders for further evaluation or treatment of depression are present). If more than one depression screen was completed by the assessing clinician, all must be negative in order to select NA. 539 Depression or depression symptoms A patient has depressive symptoms as identified by a PHQ-2 score of 4, but the patient has no diagnosis or current treatment for depression. If the clinician notifies the physician of the depressive symptoms and is instructed to continue to monitor the patient, with no orders for specific treatment, what response would be selected for M2250d? After reporting the patient's positive depression screening to the physician, Yes may be selected. A physician order to continue to assess for signs of depression could be considered an intervention for depression and would also meet the criteria for the Yes response for M2250d but would not be required as long as the physician was notified that the patient had screened positive for depression. 4bQ M2250 Antidepressant Medication If the patient has a diagnosis of depression, the presence of an existing antidepressant medication in the medication profile/plan of Care is considered a depression intervention. If there is an anti-depressant ordered and no diagnosis of depression, the assessing clinician would need to confirm why the medication was prescribed as anti-depressants are often indicated for diagnoses other than depression. If the medication was not prescribed specifically for depression, it would not be considered a depression intervention. 4bQ172.9.
136 Assess Anyway Referral for Treatment 541 During a SOC visit, the assessing clinician determines the patient is not depressed, has no symptoms of depression and no diagnosis of depression. Because she has assessed for signs & symptoms of depression as part of her initial comprehensive assessment and will continue to assess the patient for signs & symptoms of depression as part of her psychosocial assessment during her revisits, she selects the intervention "Skilled observation and assessment of signs and symptoms of depression " on her Plan of Care. May we answer Yes on M2250, Row d since the Plan of Care has a depression intervention? If the clinician determines it would be appropriate for a specific patient and obtains an order for "Skilled observation and assessment for signs and symptoms of depression" from the physician during the SOC or ROC allowed timeframe, M2250d may be answered "Yes" even if the formal assessment was negative and/or the patient has not been formally diagnosed with depression. Note, just checking off an intervention on a Plan of Care does not equate to "obtaining a physician order." 4bQ If the patient s depression screen was positive and the assessing clinician suggests the patient join a depression support group or schedule an appointment with a psychiatrist, would this be considered a referral for other treatment? No. It has to be a physician s order. 4bQ Pain Assessment and Mitigation Monitor and Mitigate 543 YES--If the physician-ordered Plan of Care contains interventions to monitor AND mitigate pain. Examples of interventions to mitigate pain include medication, massage, visualization, and biofeedback. NO--If the physician-ordered Plan of Care contains orders for only one (or none) of the interventions (for example, pain medications but no monitoring plan), select No, unless NA applies. NA--If the clinician completed a formal or informal assessment that indicated the patient has no pain, select NA (unless orders for further monitoring and mitigating pain are present). If more than one pain assessment was completed by the assessing clinician, all must be negative in order to select NA. 544 An ordered pain medication is considered an intervention to mitigate pain. Assessing for the effectiveness of the pain medication is considered an intervention to monitor pain. If both the pain medication and an order related to pain assessment are included in the physician-ordered Plan of Care, M2250e would be Yes. 4bQ
137 Pressure Ulcer Prevention Moist Wound Treatment YES--If the physician-ordered Plan of Care includes planned clinical interventions to reduce pressure on bony prominences or other areas of skin at risk for breakdown. Planned interventions can include teaching on frequent position changes, proper positioning to relieve pressure, careful skin assessment and hygiene, use of pressure-relieving devices such as enhanced mattresses, etc. NA--If the clinician completed a formal or informal assessment that indicated the patient is not at risk for pressure ulcers (unless orders for interventions to reduce pressure on areas of skin at risk for breakdown are present). If more than one pressure ulcer risk assessment was completed by the assessing clinician, all must be negative in order to select NA. Row g. may be answered "Yes" if, by the end of the allowed assessment time period (5 days after SOC date/2 days after inpatient facility d/c for ROC) the physician-ordered Plan of Care includes orders for pressure ulcer treatment based on the principles of moist wound healing. The assessing clinician may also answer "Yes" in cases where the moist wound healing treatment was requested of the physician, by the end of the allowed assessment time period. It would not be required that the response from the physician be obtained in order to qualify as a "Yes". If the physician response is "No, moist wound healing is not appropriate for this patient, NA would be the correct response. The parallel item in M2401 does not offer any option that an order for treatment using principles of moist wound healing was requested from the MD. So at M2401 if the MD does not order treatment based on principles of moist wound healing, No" must be reported on Row f unless the patient meets the criteria listed to mark NA. 4bQ Intervention Synopsis 547 Ordered, attempted and not provided because of documented lack of need for the education May still answer yes Attempt was made to educate and the patient refused or otherwise declined to receive the needed instruction with no further attempt Should not be reported as being implemented. Multiple orders for interventions. Can we respond "Yes" to M2401 d if pain mitigation orders were implemented but not completed prior to discharge? May answer "Yes" if there is evidence that the required assessment component was implemented AND evidence that at least one of the pain mitigation orders were implemented. 4bQ Emergent Care M2300s

138 TRF DC M2301 M2301 Emergent Care Identifies whether the patient was seen in a hospital emergency department at the time of or at any time since the most recent SOC/ROC OASIS assessment. Responses to this item include the entire period at or since the last time SOC/ROC OASIS data were collected, including use of hospital emergency department that results in a qualifying hospital admission, necessitating Transfer OASIS data collection. This item includes current events. SOC ROC ER visit w/o admission FU ER visit w admission T R F M2301 Emergent Care M2301 Emergent Care 551 Response 0 No No emergent care in hospital emergency dept since most recent SOC/ROC OR Patient is direct admitted to the hospital Patient was not treated or evaluated in the emergency room Patient had no other emergency department visits since the last SOC/ROC OASIS assessment. 552 Response 1 or 2--Yes Patient went to a hospital emergency department, regardless of whether the patient/caregiver independently made the decision to seek emergency department services or was advised to go the emergency department by the physician, home health agency, or other health care provider 4b-Q179 Response 2 Yes with admission Patient went to a hospital emergency department and was subsequently admitted to the hospital An OASIS transfer assessment is required (assuming the patient stay was for 24 hours or more for reasons other than diagnostic testing).

139 M2301 Emergent Care Dies in the ER 553 What if a patient went to a hospital emergency department, was held at the hospital for observation, then released? The patient did receive emergent care. The time period that a patient can be "held" without admission can vary An OASIS transfer assessment is not required if the patient was never actually admitted to an inpatient facility. 554 A patient who dies in a hospital emergency department is considered to have been under the care of the emergency department, not the home health agency. In this situation, a Transfer assessment, not an assessment for "Death at Home," should be completed. For M2300, select Response 1 - Yes, used hospital emergency department WITHOUT hospital admission. TRF DC M2310 Reason for Emergent Care M2310 Reason for Emergent Care = injury caused by a fall only 19 = New wound not caused by fall 556 Emergency Room only If more than one reason contributed to the hospital emergency department visit, mark all appropriate responses (include why even though not diagnosed) If a patient received care for a fall at home and was found to have medication side effects, mark both responses. Improper medication administration, regardless of who (patient, caregiver, or medical staff) administered the med improperly. 4b-Q181.5

")
140 557 M2310 Reason for Emergent Care If the reason is not included in the choices, mark Response 19 - Other than above reasons. If Pt received emergent care in a hospital ED multiple times since the last time OASIS data were collected, include the reasons for all visits. Include both the reasons care was sought and care received. 4b-Q Not counted in ACH statistics M2430 The clinician is to use his/her clinical judgment to determine if the patient's condition (for instance; "hypertension", or "change in mental status") resulting in hospitalization, fits into the categories/conditions reflected in the various M2430 responses (for instance; "Other heart disease", or "Acute mental/behavorial health problem"). If the clinician finds that none of the categories represent the reason(s) why the patient was hospitalized, then "Other" is the correct response. The clinician could provide more information for agency use in a narrative within the comprehensive assessment. Questions?? Send to Lisa@selmanholman.com Teresa@selmanholman.com Sign up for Lisa s blog at Selman-Holman & Associates, LLC Home Health Insight CoDR Coding Done Right CodeProUniversity Med-PASS.com Like us on Facebook Selman-Holman & Associates, LLC Code Pro University You re invited to join the groups: Homecare Coders ICD-10-CM For Coders
Basic Training: Home Health Edition. OASIS and Outcomes. April 2, 2013
 Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
Care Coordination in the New CoP s. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Climb Every Mountain: Improve Every OASIS Outcome
 KHCA Annual Meeting C3 Climb Every Mountain: Improve Every OASIS Outcome Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus September 21, 2017 Climb Every Mountain: Improve
KHCA Annual Meeting C3 Climb Every Mountain: Improve Every OASIS Outcome Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus September 21, 2017 Climb Every Mountain: Improve
CASPER Reports. Objectives: What is Casper? 4/27/2012. Certification And Survey Provider Enhanced Reports
 CASPER Reports By Cindy Skogen, RN Oasis Education Coordinator at MDH Contact #: 651-201-4314 E-mail: Health.OASIS@state.mn.us Source: Center for Medicare/Medicaid Services (CMS). Objectives: Following
CASPER Reports By Cindy Skogen, RN Oasis Education Coordinator at MDH Contact #: 651-201-4314 E-mail: Health.OASIS@state.mn.us Source: Center for Medicare/Medicaid Services (CMS). Objectives: Following
OASIS-C Home Health Outcome Measures
 OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
OASIS ITEM ITEM INTENT TIME POINTS ITEM(S) COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES
 COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES") (M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Part 2: OASIS C2 Accuracy
 Part 2: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy Patient Tracking Items M0010 M0150 Completed at SOC and updated when a change occurs in the episode. 1
Part 2: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy Patient Tracking Items M0010 M0150 Completed at SOC and updated when a change occurs in the episode. 1
CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. Are OASIS data collected on patients that are recertified or only on patients that are transferred or discharged? A1. The condition of participation (CoP) published
CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. Are OASIS data collected on patients that are recertified or only on patients that are transferred or discharged? A1. The condition of participation (CoP) published
A Tool for Maximizing Quality in Your Organization
 OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q1. [Q&A RETIRED 09/09; Outdated] Q2. When integrating the OASIS data items into an HHA's assessment
CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q1. [Q&A RETIRED 09/09; Outdated] Q2. When integrating the OASIS data items into an HHA's assessment
October 2011 Quarterly CMS OCCB Q&As
 October 2011 Quarterly CMS OCCB Q&As Category 2; Category 3; M0100 Question 1: A patient is seen monthly. On a monthly visit, which falls within the last five days of the certification period, the assessing
October 2011 Quarterly CMS OCCB Q&As Category 2; Category 3; M0100 Question 1: A patient is seen monthly. On a monthly visit, which falls within the last five days of the certification period, the assessing
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
HHVBP Sessions. HHVBP Overview 6/7/2016. Home Health Value Based Purchasing. Session 1: Overview
 Home Health Value Based Purchasing Session 1: Overview Session 1: Overview HHVBP Sessions Future session topics: New Measures Form & KAHL Courses Total Performance Score & State Benchmarks / Achievement
Home Health Value Based Purchasing Session 1: Overview Session 1: Overview HHVBP Sessions Future session topics: New Measures Form & KAHL Courses Total Performance Score & State Benchmarks / Achievement
HOW PROCESS MEASURES ARE CALCULATED
 HOW PROCESS MEASURES ARE CALCULATED 1) Timely initiation in care (check at SOC and ROC) (5-star) Percentage of home health episodes of care in which the start or resumption of care date was either on the
HOW PROCESS MEASURES ARE CALCULATED 1) Timely initiation in care (check at SOC and ROC) (5-star) Percentage of home health episodes of care in which the start or resumption of care date was either on the
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING
 January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the
Outcome Based Case Conference
 Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
Final Rule Summary. Medicare Home Health Prospective Payment System Calendar Year 2016
 Final Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2016 November 2015 Table of Contents Overview and Resources... 1 HHPPS Payment Rates... 1 National Per Visit Amounts...
Final Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2016 November 2015 Table of Contents Overview and Resources... 1 HHPPS Payment Rates... 1 National Per Visit Amounts...
QAPI Quality Assurance Process Improvement
 QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
Selman Holman & Associates, LLC PATIENT RIGHTS: Four New CoP s. Objectives
 PATIENT RIGHTS: MEETING THE PROPOSED CONDITIONS OF PARTICIPATION JUNE 2016 2 Selman Holman & Associates, LLC Home Health Insight Consulting, Education and Products CoDR Coding Done Right CodeProUniversity
PATIENT RIGHTS: MEETING THE PROPOSED CONDITIONS OF PARTICIPATION JUNE 2016 2 Selman Holman & Associates, LLC Home Health Insight Consulting, Education and Products CoDR Coding Done Right CodeProUniversity
CY2019 Proposed Medicare Home Health Rate Rule and Much More
 Medicare Home Health Proposed Rule July 13, 2018 William A. Dombi President wad@nahc.org Mary K. Carr Vice President mkc@nahc.org CY2019 Proposed Medicare Home Health Rate Rule and Much More Published
Medicare Home Health Proposed Rule July 13, 2018 William A. Dombi President wad@nahc.org Mary K. Carr Vice President mkc@nahc.org CY2019 Proposed Medicare Home Health Rate Rule and Much More Published
Home Health Value-Based Purchasing Series: HHVBP Model 101. Wednesday, February 3, 2016
 Home Health Value-Based Purchasing Series: HHVBP Model 101 Wednesday, February 3, 2016 About the Alliance 501(c)(3) non-profit research foundation Mission: To support research and education on the value
Home Health Value-Based Purchasing Series: HHVBP Model 101 Wednesday, February 3, 2016 About the Alliance 501(c)(3) non-profit research foundation Mission: To support research and education on the value
LET S SEE HOW IT MIGHT HAVE WENT..
 George Jetson, OASIS, and the survey process Hooba doobadooba! Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative Standards Fern.Dewert@health.mo.gov
George Jetson, OASIS, and the survey process Hooba doobadooba! Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative Standards Fern.Dewert@health.mo.gov
HOME HEALTH VALUE BASED PURCHASING FREQUENTLY ASKED QUESTIONS Updates in Red
 1. What is the contact information of the Home Health Value-Based Purchasing (HHVBP) Helpdesk? General HHVBP The HHVBP Helpdesk can be reached by email at HHVBPquestions@cms.hhs.gov). The Helpdesk number
1. What is the contact information of the Home Health Value-Based Purchasing (HHVBP) Helpdesk? General HHVBP The HHVBP Helpdesk can be reached by email at HHVBPquestions@cms.hhs.gov). The Helpdesk number
July 2011 Quarterly CMS OCCB Q&As
 July 2011 Quarterly CMS OCCB Q&As Category 1 - Applicability Face-to-Face Question 1: If the F2F does not occur within 30 days, but it does occur, for example, on the 35th day, does the agency have to
July 2011 Quarterly CMS OCCB Q&As Category 1 - Applicability Face-to-Face Question 1: If the F2F does not occur within 30 days, but it does occur, for example, on the 35th day, does the agency have to
Basics of Care Planning for Home Health Patients. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Basics of Care Planning for Home Health Patients Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight
Basics of Care Planning for Home Health Patients Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight
CY 2018 Home Health PPS Proposed Rule
 CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
Medicare Home Health Prospective Payment System
 Medicare Home Health Prospective Payment System Payment Rule Summary PROPOSED CY 2017 Overview and Resources On July 5, 2016, the Centers for Medicare and Medicaid Services (CMS) published its proposed
Medicare Home Health Prospective Payment System Payment Rule Summary PROPOSED CY 2017 Overview and Resources On July 5, 2016, the Centers for Medicare and Medicaid Services (CMS) published its proposed
2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE
 2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com FINAL 2017 PAYMENT RATES HOME HEALTH Outlier
2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com FINAL 2017 PAYMENT RATES HOME HEALTH Outlier
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey & Certification Group July 10, 2014 Linda
DEPARTMENT OF HEALTH & HUMAN SERVICES 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey & Certification Group July 10, 2014 Linda
Home Health Value Based Purchasing. Today s Session
 Home Health Value Based Purchasing Session 7: Managing Your HHVBP Quality Today s Session Prior to this session, you should have: Access to the HHVBP Secure Portal Your agency s Interim Performance Report
Home Health Value Based Purchasing Session 7: Managing Your HHVBP Quality Today s Session Prior to this session, you should have: Access to the HHVBP Secure Portal Your agency s Interim Performance Report
HOW HOME HEALTH COMPARE ITEMS ARE CALCULATED
 HOW HOME HEALTH COMPARE ITEMS ARE CALCULATED PERIOD OF STUDY: Home Health Compare and Process Measures will be calculated based upon your Dashboard selections including Payer Sources, Teams, Case-Managers,
HOW HOME HEALTH COMPARE ITEMS ARE CALCULATED PERIOD OF STUDY: Home Health Compare and Process Measures will be calculated based upon your Dashboard selections including Payer Sources, Teams, Case-Managers,
Key points. Home Care agency structures. Introduction to Physical Therapy in the Home Care Setting. Home care industry
 Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
Proposed fy17 LTCH PPS: New rules for Quality & Referrals
 Proposed fy17 LTCH PPS: New rules for Quality & Referrals Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives Describe updates to the LTCH
Proposed fy17 LTCH PPS: New rules for Quality & Referrals Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives Describe updates to the LTCH
Medications: Defining the Role and Responsibility of Physical Therapy Practice
 This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
OASIS-C2 FIELD GUIDE TO DATA COLLECTION
 OASIS-C2 FIELD GUIDE TO DATA COLLECTION Outcome and Assessment Information Set OASIS-C2 Guidance Manual Effective January 1, 2018 Manual: Effective January 1, 2018 Q&A from November 2016 Categories 1 through
OASIS-C2 FIELD GUIDE TO DATA COLLECTION Outcome and Assessment Information Set OASIS-C2 Guidance Manual Effective January 1, 2018 Manual: Effective January 1, 2018 Q&A from November 2016 Categories 1 through
Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC. Month Day Year / / Month Day Year
 / / UHHC. Month Day Year / / Month Day Year") Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
PPS Therapy. Medicare 2/28/ year Home Health clinician/contractor. 30 years Geriatric Rehab. Home Health consultant, author, speaker
 PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality
 Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services President Home Health Section APTA August
Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services President Home Health Section APTA August
Medicare Home Health Prospective Payment System
 Medicare Home Health Prospective Payment System Payment Rule Summary PROPOSED CY 2018 Overview and Resources On July 28, 2017, the Centers for Medicare and Medicaid Services (CMS) published its proposed
Medicare Home Health Prospective Payment System Payment Rule Summary PROPOSED CY 2018 Overview and Resources On July 28, 2017, the Centers for Medicare and Medicaid Services (CMS) published its proposed
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
Quality Improvement: Utilization Measures
 Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
(M1025) Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition
 Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition") HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
Using Benchmarks to Drive Home health Success
 Introductory announcements: This provider-directed continuing nursing education activity was approved by the Maryland Nurses Association (MNA) to award contact hours. The MNA is accredited as an approver
Introductory announcements: This provider-directed continuing nursing education activity was approved by the Maryland Nurses Association (MNA) to award contact hours. The MNA is accredited as an approver
Therapies (e.g., physical, occupational and speech) Medical social worker (MSW) 3328ALL0118-F 1
 Medical social worker (MSW) 3328ALL0118-F 1") 1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know
 New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
HHGM is Alive and Kicking: How Can You Prepare for What s Next?
 HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
DEPARTMENT OF HEALTH & HUMAN SERVICES Survey and Certification Group 7500 Security Boulevard Baltimore, Maryland
 DEPARTMENT OF HEALTH & HUMAN SERVICES Survey and Certification Group 7500 Security Boulevard Baltimore, Maryland 21244-1850 Survey and Certification Group April 20, 2010 Linda Krulish, PT, MHS, COS-C President
DEPARTMENT OF HEALTH & HUMAN SERVICES Survey and Certification Group 7500 Security Boulevard Baltimore, Maryland 21244-1850 Survey and Certification Group April 20, 2010 Linda Krulish, PT, MHS, COS-C President
Proposed Rule Summary. Medicare Home Health Prospective Payment System Program Year: CY2019
 Proposed Rule Summary Medicare Home Health Prospective Payment System Program Year: CY2019 July 2018 TABLE OF CONTENTS Overview and Resources... 2 HHPPS Payment Rates... 2 National Per Visit Amounts...
Proposed Rule Summary Medicare Home Health Prospective Payment System Program Year: CY2019 July 2018 TABLE OF CONTENTS Overview and Resources... 2 HHPPS Payment Rates... 2 National Per Visit Amounts...
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
OASIS-C Guidance Manual Errata
 Errata Updated January 2011 Page F-18 M1340 CORRECTED the last sentence of the 9 th bullet under Response- Specific Instructions, to read as follows: These may be reported in M1350 if the home health agency
Errata Updated January 2011 Page F-18 M1340 CORRECTED the last sentence of the 9 th bullet under Response- Specific Instructions, to read as follows: These may be reported in M1350 if the home health agency
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Home Health Coverage 101. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Home Health Coverage 101 Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting, Education
Home Health Coverage 101 Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting, Education
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
LET S SEE HOW IT MIGHT HAVE GONE..
 Would watching the Jetson s have given you any prediction on the future for OASIS? Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative
Would watching the Jetson s have given you any prediction on the future for OASIS? Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative
An Initial Review of the CY Medicare Home Health Rule. CY2018 Proposed Medicare Home Health Rate Rule and Much More
 An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
Home Health Eligibility Requirements
 Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
7/27/2016. HHVBP Sessions. General HHVBP Questions. Home Health Value Based Purchasing. Session 5: Frequently Asked Questions
 Home Health Value Based Purchasing Session 5: Frequently Asked Questions HHVBP Sessions Session 5: Frequently Asked Questions Previous session topics: Overview New Measures & KAHL Modules Total Performance
Home Health Value Based Purchasing Session 5: Frequently Asked Questions HHVBP Sessions Session 5: Frequently Asked Questions Previous session topics: Overview New Measures & KAHL Modules Total Performance
OASIS, OUTCOMES & YOUR AGENCY S STAR RATINGS
 OASIS, OUTCOMES & YOUR AGENCY S STAR RATINGS SHARON M. LITWIN, RN, BSHS, MHA, HCS-D SENIOR MANAGING PARTNER 5 STAR CONSULTANTS, LLC OBJECTIVES Review CASPER Reports so that participants can understand
OASIS, OUTCOMES & YOUR AGENCY S STAR RATINGS SHARON M. LITWIN, RN, BSHS, MHA, HCS-D SENIOR MANAGING PARTNER 5 STAR CONSULTANTS, LLC OBJECTIVES Review CASPER Reports so that participants can understand
Is your Home Health Agency ready for the Final Rule to the Conditions of Participation?
 Is your Home Health Agency ready for the Final Rule to the Conditions of Participation? Medicare-certified home health agencies have almost doubled from 6,461 in 1990 to 12,268 in 2014 due to longer life
Is your Home Health Agency ready for the Final Rule to the Conditions of Participation? Medicare-certified home health agencies have almost doubled from 6,461 in 1990 to 12,268 in 2014 due to longer life
Objectives. Home Health Benefits. Pretest 1. True or False. Pretest 2. Multiple choice. Pretest 4. Multiple choice. Pretest 3.
 Home Health Benefits Objectives Coleen M. Schmidt, VP Clinical Services, COO June 2015 Wisconsin Association for Home Care (WiAHC) 1. List the type of home health providers/services within the home care
Home Health Benefits Objectives Coleen M. Schmidt, VP Clinical Services, COO June 2015 Wisconsin Association for Home Care (WiAHC) 1. List the type of home health providers/services within the home care
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Linking the Coding Process, the OASIS & the POC to Make Them All Work Together
 Linking the Coding Process, the OASIS & the POC to Make Them All Work Together Presented by Jennifer Warfield, RN, BSN, HCS-D, COS-C Education Director PPS Plus Software Linking the Coding Process, the
Linking the Coding Process, the OASIS & the POC to Make Them All Work Together Presented by Jennifer Warfield, RN, BSN, HCS-D, COS-C Education Director PPS Plus Software Linking the Coding Process, the
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
5/1/2017 THE BEST DEFENSE IS A GOOD OFFENSE OBJECTIVES. Preparing for a Home Health Medicare Recertification Survey
 THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
Overview of Home Health Star Ratings
 Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Medication Management: Therapy Scope Versus Comfort Level
 Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
OASIS Complete Webinar Series
 OASIS Complete Webinar Series Selecting Clinically Relevant and Fiscally Appropriate Diagnoses Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C October 1, 2010 243 King Street, Suite 246 Northampton,
OASIS Complete Webinar Series Selecting Clinically Relevant and Fiscally Appropriate Diagnoses Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C October 1, 2010 243 King Street, Suite 246 Northampton,
Dazed and Confused: Initial Results from the IRF QRP Data
 Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
5-Star Ratings and How to Position Your Agency
 2017 Annual Conference 5-Star Ratings and How to Position Your Agency Educational Objectives 1. Define the 5 Star Ratings programs and understand the differences and requirements for participation 2. Describe
2017 Annual Conference 5-Star Ratings and How to Position Your Agency Educational Objectives 1. Define the 5 Star Ratings programs and understand the differences and requirements for participation 2. Describe
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
OASIS - The Basics & Beyond 2 Day Workshop OASIS Workshop June 12 13, 2018
 OASIS - The Basics & Beyond 2 Day Workshop OASIS Workshop June 12 13, 2018 Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC Melissa Abbott RN, MSN, MHA,
OASIS - The Basics & Beyond 2 Day Workshop OASIS Workshop June 12 13, 2018 Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC Melissa Abbott RN, MSN, MHA,
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
ICD-10 for Beginners Four-Part Series JLU Health Records Systems 1. ICD-10-CM Coding. & Its Impact on Reimbursement
 ICD-10 for Beginners Four-Part Series www. 1 ICD-10-CM Coding & Its Impact on Reimbursement PRESENTER: Joan L. Usher, BS, RHIA, ACE AHIMA Approved ICD-10-CM Trainer JLU HEALTH RECORD SYSTEMS TEL: (781)
ICD-10 for Beginners Four-Part Series www. 1 ICD-10-CM Coding & Its Impact on Reimbursement PRESENTER: Joan L. Usher, BS, RHIA, ACE AHIMA Approved ICD-10-CM Trainer JLU HEALTH RECORD SYSTEMS TEL: (781)
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Home Health Guide to OASIS-C2
 Home Health Guide to OASIS-C2 A Reference For Field Staff Melinda A. Gaboury, COS-C Home Health Guide to OASIS-C2 A Reference For Field Staff MELINDA A. GABOURY, COS-C : A Reference for Field Staff is
Home Health Guide to OASIS-C2 A Reference For Field Staff Melinda A. Gaboury, COS-C Home Health Guide to OASIS-C2 A Reference For Field Staff MELINDA A. GABOURY, COS-C : A Reference for Field Staff is
COPs 2018 Now is the Time. HCAC 2017 Conference PreConference 2017 The Crag Business Group, Inc.
 COPs 2018 Now is the Time HCAC 2017 Conference PreConference 2017 The Crag Business Group, Inc. FOCUS & THEMES Revisions of the Home Health Agency provider requirements..focus on a patient-centered, data-driven,
COPs 2018 Now is the Time HCAC 2017 Conference PreConference 2017 The Crag Business Group, Inc. FOCUS & THEMES Revisions of the Home Health Agency provider requirements..focus on a patient-centered, data-driven,
Home Health Quality Measures
 Home Health Quality Measures Staying Current with a Moving Target Presenters J non Griffin, RN, MHA, WCC, HCS-D, COS-C, HCS-C, HCS-H Home Health Solutions, LLC www.homehealthsolutionsllc.com Objectives
Home Health Quality Measures Staying Current with a Moving Target Presenters J non Griffin, RN, MHA, WCC, HCS-D, COS-C, HCS-C, HCS-H Home Health Solutions, LLC www.homehealthsolutionsllc.com Objectives
Navigating the New CMS Quality Measures
 Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SKILLED NURSING SERVICES
 DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
QIES Help Desk. Objectives. Nursing Home Quality Initiatives and Five-Star Quality Rating System
 Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Overview. Case Management Role 6/11/2018. What It Takes To Be The Best Case Manager
 What It Takes To Be The Best Case Manager Overview Identify Case Manager Role and Responsibilities Identify Differences Between Good Case Manager and Great Case Manager Identify How to Appropriately Schedule
What It Takes To Be The Best Case Manager Overview Identify Case Manager Role and Responsibilities Identify Differences Between Good Case Manager and Great Case Manager Identify How to Appropriately Schedule
Work In Progress August 24, 2015
 Presenter Sarah Wilson MSOTR/L, CHT, CLT 4 th year PhD student at NOVA Southeastern University Practicing OT for 14 years Have worked for Washington Orthopedics and Sports Medicine for the last 8 years
Presenter Sarah Wilson MSOTR/L, CHT, CLT 4 th year PhD student at NOVA Southeastern University Practicing OT for 14 years Have worked for Washington Orthopedics and Sports Medicine for the last 8 years
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Outcome and ASsessment Information Set OASIS-C1/ICD-10 Guidance Manual Revised: October 2015 Centers for Medicare & Medicaid Services
 Outcome and ASsessment Information Set OASIS-C1/ICD-10 Guidance Manual Revised: Table of Contents Page CHAPTER 1 INTRODUCTION... 1-1 A. Manual Overview... 1-1 B. Why is OASIS Being Revised Now?... 1-1
Outcome and ASsessment Information Set OASIS-C1/ICD-10 Guidance Manual Revised: Table of Contents Page CHAPTER 1 INTRODUCTION... 1-1 A. Manual Overview... 1-1 B. Why is OASIS Being Revised Now?... 1-1
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Comments for CMS Draft Conditions of Participation (CoPs) Interpretive Guidelines (IG)
 Interpretive Guidelines (IG)") Comments for CMS Draft Conditions of Participation (CoPs) Interpretive Guidelines (IG) Overarching concerns: State Operating Manual Without knowing how CMS will update the State Operations Manual (SOM),
Comments for CMS Draft Conditions of Participation (CoPs) Interpretive Guidelines (IG) Overarching concerns: State Operating Manual Without knowing how CMS will update the State Operations Manual (SOM),
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...