Kenny Barajas DNP, RN, CEN
|
|
|
- Kelly Shields
- 6 years ago
- Views:
Transcription
1 Advanced Disease-Specific Care Certification Requirements for Comprehensive Stroke Center Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer The Joint Commission
2 Presenter Disclosure Statement ASRH, PSC and CSC Reviewer for The Joint Commission No Financial Disclosure
3 Mission The mission of The Joint Commission is to continuously improve healthcare for the public, in collaboration with other stakeholders, by evaluating healthcare organizations and inspiring them to excel in providing safe and effective care of the highest quality and value.
4 Objectives Inspire your journey for ongoing development of your Comprehensive Stroke Program Provide you with strategies on how to prepare for your next onsite review Identify challenging standards and leading practices to ensure delivery of high quality care
5 Disease-Specific Care Certification The Joint Commission s Disease-Specific Care (DSC) Certification Program provides an evaluation of a clinical program that delivers care to a defined patient population. Certification is designed to evaluate clinical care in disease management programs provided in all types of settings, including hospitals, ambulatory care, homecare, free standing emergency centers, and nursing care centers, as well as physician offices.
6 Disease-Specific Care Certification Certification is not connected to an organization s accreditation status, although the organization, if eligible for accreditation, must achieve accreditation by The Joint Commission to be eligible for DSC certification.
7 Disease Specific Advanced Certifications Acute stroke ready hospital(asrh) Chronic kidney disease(ckd) Chronic obstructive pulmonary disease(copd) Comprehensive stroke center(csc) Heart failure(achf) Inpatient diabetes care(idc) Lung volume reduction surgery(lvrs) Primary stroke center(psc) Total hip and total knee replacement(thkr) Ventricular assist device destination therapy(vad) Palliative Care

8 Tools for Success

9 Other Resources




10 Clinical Practice Guidelines Purpose: To describe appropriate care based on the best available scientific evidence and broad consensus; To reduce inappropriate variation in practice Where to locate Clinical Practice Guidelines:

11 Clinical Practice Guidelines
12 The Joint Commission Resources Access your Joint Commission Connect extranet site at Obtain a site license for the E-dition Call Customer Service at (between 8:00 A.M. and 5:00 P.M. central time, Monday through Friday Programs not yet certified can contact Business Development at or certification@jointcommission.org The Standards Interpretation Group (SIG) provides answers to frequently asked questions online at spx. The Joint Commission s Performance Measurement page at spx
13 Facts Acute Stroke Ready- 26 Primary Stroke Centers 1107 Comprehensive Stroke Centers 123
14 Requirements Assessed at Application 1. Volume of cases 2. Advanced imaging capabilities 3. Post-hospital care coordination for patients 4. Dedicated neuro-intensive care unit (ICU) beds for complex stroke patients 5. Peer review process 6. Participation in stroke research
15
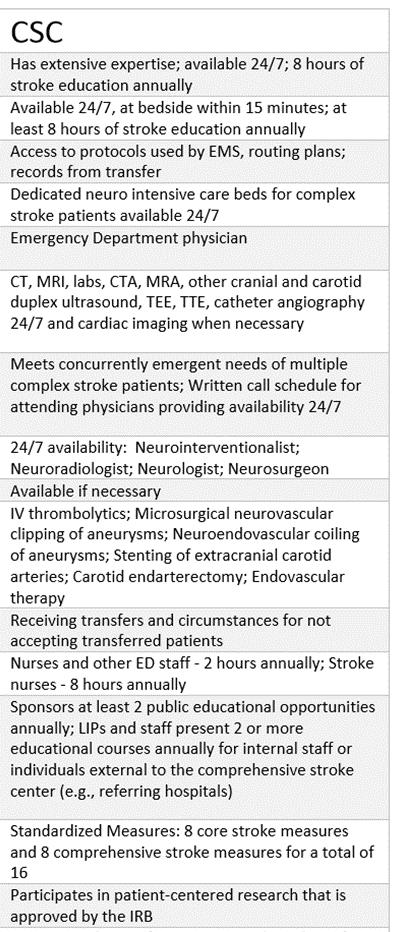
16 CSC Volume of Cases/Requirements Demonstrates that care is provided to 40 or more patients in a two year period with a diagnosis of subarachnoid hemorrhage caused by an aneurysm. Demonstrates that it is capable of treating aneurysms by performing 30 or more endovascular coiling or microsurgical clipping procedures in a two year period. Demonstrates that intravenous (IV) tissue plasminogen activator(tpa, Alteplase) is administered 25 or more times per year for eligible patients. Note 1: Providing IV tpa to a total of 50 eligible patients over a two-year period is acceptable. Note 2: IV tpa administered in the following situations can be counted in the requirement of 25 administrations per year. IV tpa ordered and monitored by the CSC via telemedicine with administration occurring at another hospital IV tpa administered by another hospital, which then transferred the patient within 24 hours to the CSC.
17 CSC Volume of Cases/Requirements Advanced imaging capabilities: The CSC will be able to provide advanced imaging with multimodal imaging capabilities 24 hours a day, 7 days a week for the following: Catheter angiography Computed tomography angiography (CTA) Magnetic resonance angiography (MRA) Magnetic resonance imaging(mri), including diffusion-weighted MRI
18 CSC Volume of Cases/Requirements The CSC performs advanced imaging with multimodal imaging capabilities for the following when indicated by patient need: Carotid duplex ultrasound Extracranial ultrasonography Transcranial Doppler Transesophageal echocardiography (TEE) Transthoracic echocardiography (TTE)
19 CSC Volume of Cases/Requirements Dedicated neuro-intensive care unit (ICU) beds for complex stroke patients The hospital will have dedicated neuro-intensive care unit (ICU) beds for complex stroke patients, including licensed independent practitioners and staff with the expertise and experience to provide on-site, neuro-critical care 24 hours a day, 7 days a week.
20 CSC Volume of Cases/Requirements The CSC has an interdisciplinary program-level review, including a peer review process that is as follows: Part of the CSC s quality improvement process A performance improvement plan when needed Note: An interdisciplinary program-level review is defined as a review at the program level to assess causes of patient adverse outcomes with the aim of decreasing the incidence of such outcomes.
21 Peer Review Criteria for selection of complex stroke patients reviewed at meeting Both ischemic and hemorrhagic strokes Method for referring case for review Multi-level process Protected peer review Monitoring and comparing complication rates Process improvement Highlight successes for team to learn from
22 Peer Review Membership Inter-specialty Emergency Medicine Neurology Neurosurgery Interventional Provider Radiologist Intensivist Hospitalists Vascular Surgery Cardiology Inter-disciplinary Physicians Nurse Practitioner Physician Assistants Nurses Quality Technologists Administration
23 CSC Volume of Cases/Requirements Participation in stroke research: The comprehensive stroke center currently participates in patient-centered stroke research that is approved by the Institutional Review Board.
24 Core Standards versus Advanced Standards Organizations must meet all Core Standards for Disease Specific Certification IN ADDITION to advanced standards for the program
25 Core Standards Certification Participation Requirements (CPR) Program Management (DSPR) Delivering or Facilitating Clinical Care (DSDF) Supporting Self-Management (DSSE) Clinical Information Management (DSCT) Performance Measurement (DSPM)
26
27
28 Endovascular Care Staffing model for 24/7 Roles and Responsibilities Staffing model for more than one case Who calls you in? Time frame for response if on-call Inclusion/exclusion criteria When does consenting occur? By whom? Anesthesia involved in care? How are they notified? Moderate sedation? Who monitors? Competency in place? Who documents? Where?
29 Endovascular Care Orientation and competency Educational requirements in care of cerebrovascular patients Do you give Alteplase? Do you mix? Do you have competency? Do you recover patients there? Remove sheaths? Who performs neurological assessments during time in department? What does hand-off look like between departments? Standardized orders for assessments and monitoring Process improvement activities
30 Preparing for Your Site Visit Request assistance from your accreditation/quality department Utilize your resources Mirror tracer experience Increases staff comfort level in presenting patient case Inter-professional team discussion Individual role and communication as a team
31 CSC Review Schedule 2 Reviewers Day 1 Day Opening session Planning session Emergency Department Tracers Lunch Tracers Issue Resolution/Closing Daily briefing Tracers System tracer/data session/pi Lunch HR/Education/Credentialing Prepare report Issue resolution report to admin Closing conference

32 Opening Session Your program s time to shine! Engage team members across continuum 90 minutes If a provider has a restricted schedule, please share with reviewer so schedule can be accommodated to speak with them
33 Opening Session Highlights Program mission, goals, and objectives Program structure, Program leadership and management Program design, Stroke team composition: including core members, and extended members Developing, implementing, and evaluating the program Target population for the program: Complex stroke patients who have the need for emergent care, advanced imaging, and a surgical intervention such as clipping for aneurysm, coiling for aneurysms, and stenting of the extracranial carotid. The target population also includes complex stroke patients who received IV tpa or IA tpa.
34 Opening Session Highlights Identified needs of the program population The selection, implementation, and evaluation of clinical practice guidelines Model of neuro-icu care Evaluation of clinical practice guidelines use and appropriateness to the target population Performance improvement process, including evaluation of the disease management program s efficacy Community relationships, Use of telemedicine
35 Opening Session Highlights What does stroke team look like? Time frame for initiating stroke alert processes Is there a stroke system designation at state level for EMS? Transfer center? Transfer agreements? Formal or informal processes Telemedicine acute care or follow-up process Management of two or more stroke alerts at one time and/or shared responsibility for telestroke Your community/patient population
36 Opening Session Highlights Location and number of interventional suites (Radiology, Cath Lab, Surgery) Neuro Critical Care Unit/beds location, numbers Stroke Unit or designated unit Key transitional care processes: EMS to ED, ED to Stroke Unit, Stroke Unit to home, rehabilitation, skilled facility Research - types of opportunities for patients to participate. Who coordinates, when is this offered?
37 Opening Session Highlights Medical staff model Primary care Hospitalists Intensivists Neurologists Neurosurgeons Admitting/attending physician? Consultation?

38 Planning Session
39 Schedules and call-schedules for specialties covering 24/7 Neurologist Interventionalist Intensivist Neurosurgeon IR Suite staff Residents APN s or PA s Anesthesia
40 Planning Session Protocols to understand process flows ED Imaging In-house stroke alerts Order sets Dated documents: Last reviewed or revised Roles and responsibilities defined Anything we could find on paper provide reviewer up front Schedules and callschedules for specialties covering 24/7 Neurologist Interventionalist Intensivist Neurosurgeon IR Suite staff Residents APN s or PA s Anesthesia
41 Planning Session Preparation of documents: List of last 4/12 months What reviewers like to have available for open medical records Stroke Log Date of admission Age Provider and/or specialty Type of stroke Any stroke intervention procedure completed: IV Alteplase Thrombectomy Coiling, Clipping, CAS, CEA (All services) Ventriculostomy Decompression (evacuation/craniectomy)
42 Planning Session Preparation of documents: What reviewers like to have available for closed medical records Date of admission Length of stay Age Disposition Provider and/or specialty Electronic Health Record navigator
43 Emergency Department Session Describe unit-beds, staffing, resources Stroke protocols-ems arrival, walk-in, 2 or more stroke alerts Tools used by staff to identify stroke patients Stroke response activation, team activities (CT, lab, RX, RAD, Neuro) Who initiates orders, Who admits or consults Off hour process EMS protocols-state legislation for transport of stroke patients How many systems feed into your ED Education: ED staff, EMS (feedback) Bypass or diversion minutes

44 Tracer Locations Locations touching complex stroke patients Emergency Department Radiology Lab POCT Pharmacy Interventional Radiology / Cath Lab Operating Room Post-Anesthesia Recovery Room
45 System Tracer/Data Session/PI Data-how abstracted, validated, analyzed, used for process improvement Performance improvement plan Meeting minutes How data is reported up and down the organization PSC and CSC measures Stroke alert data Patients perception of care Complication rates, peer review process Patient call back process including Modified Rankin scoring Public reporting of interventions 120 minutes
46 Credentialing and Competencies Allied Health Onboarding-Human resources Orientation-Organization and unit specific Performance evaluation Initial/Ongoing competencies Continuing education Medical Staff Med staff appointment Provider privileges CME FPPE OPPE 120 minutes
47 Issue Resolution Resolve issues identified during review Submit last minute IOU s *The goal of The Joint Commission is to be transparent throughout the review process and nothing should be a surprise 30 minutes
48 Closing Session Core group session Organization session *Report is preliminary: Summary of findings
49 Standards and Pitfalls Certification Participation Requirements (CPR) Program Management (DSPR) Delivering or Facilitating Clinical Care (DSDF) Supporting Self-Management (DSSE) Clinical Information Management (DSCT) Performance Measurement (DSPM)
50 The Joint Commission s Survey Analysis for Evaluating Risk (SAFER) Matrix Immediate Threat to Life (a threat that represents immediate risk or may potentially have serious adverse effects on the health of the patient, resident, or individual served) Likelihood to Harm a Patient/Staff/Visitor HIGH MODERATE LOW LIMITED PATTERN WIDESPREAD Scope
51 Why are findings Scored in Different Standards? Dysphagia Screen Do you have an evidenced based tool? Did you perform the task prior to PO meds? Order Sets Do you have a current CPG derived order set? Did your provider use the correct order set? Did your provider use an order set? Consents Did the patient receive the information needed for informed consent? Was the consent dated and signed? Did you follow your incapacity/emergency consent procedures?
52 Certification Participation Requirements (CPRs) Address specific requirements for participation in the certification program and for maintaining a certification award Do you meet the requirements?
53 Program Management (DSPR) Designing and implementing the program Evaluating the program Offering a relevant program for patients Providing safe and adequate access to care Conducting the program in an ethical manner Supplying reference resources to practitioners Offering the program in safe and accessible facilities
54 Program Management (DSPR) DSPR.1-The program defines its leadership roles EP 4-The CSC documents the roles and responsibilities for member of the core stroke team EP 6-Providers use order sets: derived from CPG s EP 6-Variation in practice between specialist for same procedure EP 7-Providers practice within scope of practice (licensure, certification, training and competency) DSPR.2 The program is collaboratively designed, implemented, and evaluated DSPR.3 The program meets the needs of the target population EP 3-Identify target population EP 4-EMS: Partnership/Guidelines
55 Program Management (DSPR) DSPR.5 The program determines the care, treatment, and services it provides EP 1-Participates in patient-centered research approved by IRB EP 4-Informed consent: procedures, date, time and signatures. DSSE.1 EP 1 Lack of risks, benefits and alternatives EP 6-Detailed plan to meet the needs of two complex patients at the same time: Bedside or telemedicine EP 7-Neurosurgeon cannot be on call at any other hospital: Documents back up if covering two services Fellows: neurocritical care & cerebrovascular experience Residents: neurocritical care & cerebrovascular experience: training in residency program NP/PA: Documented neurocritical care & cerebrovascular experience/competency (ENLS etc.) DSPR.6 The program has current reference and resource materials EP 1-Practitioners have access to reference materials (CPG s): Acute assessment of IS and hemorrhagic stroke
56 Delivering or Facilitating Clinical Care (DSDF) Using qualified, competent practitioners Delivering or facilitating the delivery of care using evidence-based clinical practice guidelines Individualizing care to meet patients needs Managing comorbidities and concurrently occurring conditions Initiating discharge planning and facilitating subsequent care, treatment, and services
57 Delivering or Facilitating Clinical Care (DSDF) DSDF.1 Practitioners are qualified and competent (document competency) DSDF.2 The program develops a standard process originating in CPG s or evidenced based practice to deliver or facilitate the delivery of clinical care DSDF.3 The program is implemented through the use of clinical practice guidelines selected to meet the patient s needs. EP 2-The assessment(s) and reassessments(s) are completed according to the patient s needs and clinical practice guidelines EP 2-Documentation tools/abbreviated assessment tools do not allow for ongoing assessment of patient specific deficits EP 2-Vital signs, distal pulse checks, groin checks, neuro checks, wounds/incision, dressing etc.
58 Delivering or Facilitating Clinical Care (DSDF) DSDF.3 The program is implemented through the use of clinical practice guidelines selected to meet the patient s needs. EP 3-Laboratory results should not delay stroke intervention Physical, Occupational, Speech therapy or social work/case management needs are assessed in a timely manner according to the organizations/programs requirement Timely management of blood pressure in ICH Timely management of hyperglycemia
59 Delivering or Facilitating Clinical Care (DSDF) DSDF.4 The plan of care is developed using an interdisciplinary approach and patient participation. EP 2-Assessed for cognitive decline, depression and other social issues Depression screening consistency of when and who performs it Illicit drug or alcohol abuse appropriate referral process in place EP 3-Individualized plan of care is based on patient s goals and the time frames to meet those goals Engagement of patient and family in goal setting
60 Delivering or Facilitating Clinical Care (DSDF) DSDF.5 The program manages co-morbidities and concurrently occurring conditions and/or communicates the necessary information to manage these conditions to other practitioners. EP 1-Process to receive transfers including time frames EP 3-Depression screening positive no protocol to address positive screen DSDF.6 The program initiates discharge planning and facilitate arrangements for subsequent care, treatment, and services to achieve mutually agreed upon patient goals. EP 1-SNF, rehab, outpatient services, home care, palliative care
61 Supporting Self-Management (DSSE) Assessing patients self-management capabilities Providing support for patients in self-management activities Involving patients in developing the plan of care Educating patients in the theory and skills necessary to manage their disease(s) Recognizing and supporting self-management effort
62 Supporting Self-Management (DSSE) DSSE.1 The program involves patients in making decisions about their care, treatment, and services EP 1- Informed consent Potential benefits, risks, side effects of patient's proposed stroke interventions and care Likelihood of the patient achieving his or her goals Any potential problems that might occur as a result of the intervention Reasonable alternatives
63 Supporting Self-Management (DSSE) DSSE.1 The program involves patients in making decisions about managing their disease or condition EP 2-The program assesses the patient s readiness, willingness, and ability to engage in self-management activities EP 3-The program assesses the family and/or caregiver s readiness, willingness, and ability to provide or support selfmanagement activities when needed EP 5-Patients and practitioners mutually agree upon goals Templated documents, used to document
64 Supporting Self-Management (DSSE) DSSE.2 The program addresses the patient s self-management plan EP 1 The program promotes lifestyle changes that support selfmanagement activities EP 2 The program evaluates barriers to lifestyle changes EP 4 The program assesses and documents the patient s response to recommended lifestyle changes EP 5 The program addresses the education needs of the patient regarding disease progression and health promotion
65 Supporting Self-Management (DSSE) DSSE.3 The program addresses the patient s educational needs EP 1-The program s education material comply with recommended elements of care, treatment, and services EP 3-The program presents content in an understandable manner according to the patient s level of literacy EP 5-The program addresses the education needs of the patient regarding his or her disease or condition and care, treatment, and services
66 Clinical Information Management (DSCT) Proactively gathering and sharing information across the continuum to coordinate care across settings and overtime Providing easy access to patient-related information Preserving confidentiality of patient information Maintaining data quality and integrity Integrating and interpreting data from various sources Using aggregate data to support the program s information needs and direction setting
67 Clinical Information Management (DSCT) DSCT.4 The program shares information with relevant practitioners and/or healthcare organizations about the patient s disease or condition across the continuum. EP 2-The program shares information with relevant practitioners and/or healthcare organizations to facilitate continuation of patient care Summary of events at transferring facility in medical record Orders and treatment reflected in medical record Nurse Case Management document in the same electronic health record
68 Clinical Information Management (DSCT) DSCT.5 The program initiates, maintains, and makes accessible a medical record for every patient. EP 4-The medical record contains sufficient information to justify the care, treatment, and services provided. Does it tell the story EP 4-Documentation indicates the reason eligible ischemic stroke patients did not receive IV thrombolytic therapy EP 5-The medical record contains sufficient information to document the course and results of care, treatment, and services *Documentation of care during transport, procedures (MRI) or transfers
69 Performance Measurement (DSPM) Having an organized, comprehensive approach to performance improvement Developing a performance improvement plan Trending and comparing data to evaluate processes and outcomes Using information garnered from measurement data to improve or validate clinical practice Using participant-specific, care-related data Evaluating the participants perception of the quality of care Maintaining data quality and integrity
70 Performance Measurement (DSPM) DSPM.1 The program has an organized, comprehensive approach to performance improvement EP 1-Identify goals and set priorities for improvements in a performance improvement plan EP 2-Peer review process EP 6-Monitoring complications and identify area of opportunity DSPM.2 The program maintains data quality and integrity EP 2-The program monitors data reliability and validity
71 Performance Measurement (DSPM) DSPM.3 The program collects measurement data to evaluate processes and outcomes EP 3-The program collects patient satisfaction data relevant to its target population EP 4-Phone call within 7 days from member the stroke team EP 6-Public reporting of interventional outcomes (CEA and CAS on website) DSPM.4 The program collects and analyzes data to determine variance from the clinical practice guidelines EP 1-The program tracks data variances at the patient level
72 Follow-up Phone Call Define intent of phone call Make it meaningful to patient and program Readmission prevention (appointment, transportation, medication, equipment) Satisfaction of comprehensive stroke care Reinforce education Successful in reaching? Get alternate phone numbers Share with patient/family that you will be calling and for what reason Have them call you back
73 Questions? Thank you for you commitment to each other, communities, families and the patients you serve Without you, stroke would not have dropped to the 5 th leading cause of death in the United States
74 The Joint Commission Disclaimer These slides are current as of 4/27/2017. The Joint Commission reserves the right to change the content of the information, as appropriate. These slides are only meant to be cue points, which were expounded upon verbally by the original presenter and are not meant to be comprehensive statements of standards interpretation or represent all the content of the presentation. Thus, care should be exercised in interpreting Joint Commission requirements based solely on the content of these slides. These slides are copyrighted and may not be further used, shared or distributed without permission of the original presenter or The Joint Commission.
Element(s) of Performance for DSPR.1
 of Performance for DSPR.1") Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix
 Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix David Eickemeyer, MBA Associate Director, Certification April 20, 2017 Today s Agenda Three Levels of Stroke Certification
Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix David Eickemeyer, MBA Associate Director, Certification April 20, 2017 Today s Agenda Three Levels of Stroke Certification
Proposed Requirements for Comprehensive Stroke Center
 Proposed Requirements for Comprehensive Stroke Center Please Note: The current requirements for Disease-Specific Care Advanced Certification Program for Primary Stroke are included in this document. Proposed
Proposed Requirements for Comprehensive Stroke Center Please Note: The current requirements for Disease-Specific Care Advanced Certification Program for Primary Stroke are included in this document. Proposed
Acute Stroke Ready Hospital Certification Program
 Ready-or-Not? Acute Stroke Ready Here We Come! Acute Stroke Ready Hospital Certification Program Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer-The Joint Commission April 28, 2017 Presenter
Ready-or-Not? Acute Stroke Ready Here We Come! Acute Stroke Ready Hospital Certification Program Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer-The Joint Commission April 28, 2017 Presenter
PSC Certification: What really happens
 PSC Certification: What really happens Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN, SCRN Christy Franklin, MS, RN, CNRN Julie Fussner, BSN, RN, CPHQ, SCRN Disclosures Wendy J. Smith- I have no actual
PSC Certification: What really happens Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN, SCRN Christy Franklin, MS, RN, CNRN Julie Fussner, BSN, RN, CPHQ, SCRN Disclosures Wendy J. Smith- I have no actual
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
The Basics: Getting Started on Disease- Specific Care Certification
 The Basics: Getting Started on Disease- Specific Care Certification May 4, 2017 David Eickemeyer, MBA Associate Director, Certification Today s Objectives Define the main components of Disease- Specific
The Basics: Getting Started on Disease- Specific Care Certification May 4, 2017 David Eickemeyer, MBA Associate Director, Certification Today s Objectives Define the main components of Disease- Specific
DNV GL - Healthcare Advisory Notice Notice No:
 DNV GL - Healthcare Advisory Notice Notice No: 2015-06 DATE: September 3, 2015 SUBJECT: New Version Comprehensive Stroke Center Standards 2.0 DISTRIBUTION: All DNV GL - Healthcare Customers, Employees
DNV GL - Healthcare Advisory Notice Notice No: 2015-06 DATE: September 3, 2015 SUBJECT: New Version Comprehensive Stroke Center Standards 2.0 DISTRIBUTION: All DNV GL - Healthcare Customers, Employees
Disease Specific Care. Certification Review Process Guide
 Disease Specific Care Certification Review Process Guide 2018 Disease Specific Care Certification Review Process Guide 2018 Copyright: 2018 The Joint Commission Disease Specific Care Certification Review
Disease Specific Care Certification Review Process Guide 2018 Disease Specific Care Certification Review Process Guide 2018 Copyright: 2018 The Joint Commission Disease Specific Care Certification Review
Core Elements of Delivery of Stroke Prevention Services
 Core Elements of Delivery of A critical component of secondary stroke prevention is access to specialized stroke prevention services (SPS), ideally provided by dedicated stroke prevention clinics. Stroke
Core Elements of Delivery of A critical component of secondary stroke prevention is access to specialized stroke prevention services (SPS), ideally provided by dedicated stroke prevention clinics. Stroke
HFAP Stroke Survey. Overview of the Survey Process 8/17/2011
 HFAP Stroke Survey Surveyors Viewpoint Bernard C. McDonnell, D.O. Stroke Center Accreditation from the Surveyors Viewpoint 01.00.01 Primary stroke Center Facility Commitment. The leadership of the facility
HFAP Stroke Survey Surveyors Viewpoint Bernard C. McDonnell, D.O. Stroke Center Accreditation from the Surveyors Viewpoint 01.00.01 Primary stroke Center Facility Commitment. The leadership of the facility
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Neurocritical Care Fellowship Program Requirements
 Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R)
") East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R) RAC-R proudly supports and serves Jasper, Newton, Hardin, Orange, Liberty, Jefferson, Chambers, Galveston and
East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R) RAC-R proudly supports and serves Jasper, Newton, Hardin, Orange, Liberty, Jefferson, Chambers, Galveston and
Joint Commission Update National Credentialing Forum
 Joint Commission Update National Credentialing Forum San Diego, California March 2, 2017 Paul Ziaya MD Senior Director, Field Operations Accreditation and Certification Operations The Joint Commission
Joint Commission Update National Credentialing Forum San Diego, California March 2, 2017 Paul Ziaya MD Senior Director, Field Operations Accreditation and Certification Operations The Joint Commission
HRSA/Bureau of Primary Health Care (BPHC) Presentation
 Presentation") HRSA/Bureau of Primary Health Care (BPHC) Presentation Educational Webinar September 14, 2017 Valerie Henriques, MA, M.Ed., RN Joint Commission Clinical Surveyor 1 Webinar Objectives: Discuss the theory
HRSA/Bureau of Primary Health Care (BPHC) Presentation Educational Webinar September 14, 2017 Valerie Henriques, MA, M.Ed., RN Joint Commission Clinical Surveyor 1 Webinar Objectives: Discuss the theory
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures
 The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
2012 Medical Staff Update 2011 CHALLENGING STANDARDS/NPSGS
 2012 Medical Staff Update Laurel McCourt, M.D. TJC Surveyor: Hospital and Office-Based Surgery Programs, and Special Survey Unit 2011 CHALLENGING STANDARDS/NPSGS 2 Standard/NPSG 2010 Non Compliance 3 2011
2012 Medical Staff Update Laurel McCourt, M.D. TJC Surveyor: Hospital and Office-Based Surgery Programs, and Special Survey Unit 2011 CHALLENGING STANDARDS/NPSGS 2 Standard/NPSG 2010 Non Compliance 3 2011
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
Stroke System-of- Care Plan. Mississippi State Department of Health
 Stroke System-of- Care Plan Mississippi State Department of Health Bureau of Acute Care Systems MSDH Board of Health Approved: October 14, 2015 Revised July 6, 2015 Stroke System-of-Care Plan Table of
Stroke System-of- Care Plan Mississippi State Department of Health Bureau of Acute Care Systems MSDH Board of Health Approved: October 14, 2015 Revised July 6, 2015 Stroke System-of-Care Plan Table of
Cardiac Certification. Achieving excellence beyond accreditation
 Cardiac Certification Achieving excellence beyond accreditation Accreditation is just the beginning. 2 When it comes to accreditation, no organization can match The Joint Commission s experience and knowledge.
Cardiac Certification Achieving excellence beyond accreditation Accreditation is just the beginning. 2 When it comes to accreditation, no organization can match The Joint Commission s experience and knowledge.
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
STROKE REHAB PROGRAM
 STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
Neuro Labs and Best Practices in Stroke Programs. Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing
 Neuro Labs and Best Practices in Stroke Programs Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing Objectives Discuss the evolving best practices for neuro lab practice
Neuro Labs and Best Practices in Stroke Programs Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing Objectives Discuss the evolving best practices for neuro lab practice
1 st Annual Neurosciences Critical Care Symposium June 5, 2010 Karen Ellmers, RN, MS, CCNS
 What does it mean to be a Primary Stroke Center? 1 st Annual Neurosciences Critical Care Symposium June 5, 2010 Karen Ellmers, RN, MS, CCNS ellmersk@ohsu.edu 1 What are the goals of a Primary Stroke Center?
What does it mean to be a Primary Stroke Center? 1 st Annual Neurosciences Critical Care Symposium June 5, 2010 Karen Ellmers, RN, MS, CCNS ellmersk@ohsu.edu 1 What are the goals of a Primary Stroke Center?
ProviderNews2014 Quarter 3
 TEXAS ProviderNews2014 Quarter 3 Our Quality Improvement program The Amerigroup* Quality Improvement (QI) program is committed to excellence in the quality of service and care our members receive and the
TEXAS ProviderNews2014 Quarter 3 Our Quality Improvement program The Amerigroup* Quality Improvement (QI) program is committed to excellence in the quality of service and care our members receive and the
Alabama Trauma Center Designation Criteria
 2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017
 Insights July 13, 2017") Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017 Caroline Heskett, MPH The Joint Commission, Accreditation & Certification Operations Project Manager, Business Transformation Objectives
Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017 Caroline Heskett, MPH The Joint Commission, Accreditation & Certification Operations Project Manager, Business Transformation Objectives
2016 Medical Staff Standards Update Panel Featuring TJC, NCQA, URAC, DNV, and HFAP (Part 1) THE JOINT COMMISSION. Objectives
 THE JOINT COMMISSION. Objectives") 2016 Medical Staff Standards Update Panel Featuring TJC, NCQA, URAC, DNV, and HFAP (Part 1) Paul Ziaya, MD, Veronica C. Locke, MHSA, Donna Merrick, BNS, MEd, Patrick Horine, MHA, and Karen Beem, MS, RN
2016 Medical Staff Standards Update Panel Featuring TJC, NCQA, URAC, DNV, and HFAP (Part 1) Paul Ziaya, MD, Veronica C. Locke, MHSA, Donna Merrick, BNS, MEd, Patrick Horine, MHA, and Karen Beem, MS, RN
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification
 Certification") Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification Joyce Webb, RN, MBA Project Director, Standards and Survey Methods Program Lead, The Joint Commission s PCMH Initiative
Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification Joyce Webb, RN, MBA Project Director, Standards and Survey Methods Program Lead, The Joint Commission s PCMH Initiative
SAMPLE Bariatric Surgery Program Survey for Facilities and Surgeons
 I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
Achieving Perinatal Care Certification and Lessons learned from 2016
 Achieving Perinatal Care Certification and Lessons learned from 2016 Caroline Isbey RN, MSN, CDE Associate Director Heather Martin RN, MSN, MBA Associate Project Director, Specialist March 29, 2017 The
Achieving Perinatal Care Certification and Lessons learned from 2016 Caroline Isbey RN, MSN, CDE Associate Director Heather Martin RN, MSN, MBA Associate Project Director, Specialist March 29, 2017 The
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
APP PRIVILEGES IN NEUROSURGERY
 APP PRIVILEGES IN NEUROSURGERY Education/Training Licensure (Initial and Reappointment) Required Successful completion of a PA, NP or CNS program Current Licensure as a PA, RN or CNS in the state of CA
APP PRIVILEGES IN NEUROSURGERY Education/Training Licensure (Initial and Reappointment) Required Successful completion of a PA, NP or CNS program Current Licensure as a PA, RN or CNS in the state of CA
Accreditation Standards 2014 Diagnostic Imaging
 DIAGNOSTIC ACCREDITATION PROGRAM Accreditation Standards 2014 Diagnostic Imaging GOVERNANCE AND LEADERSHIP 1 DGL5.1.3 New Criteria There are processes to receive and resolve ethical dilemmas in a timely
DIAGNOSTIC ACCREDITATION PROGRAM Accreditation Standards 2014 Diagnostic Imaging GOVERNANCE AND LEADERSHIP 1 DGL5.1.3 New Criteria There are processes to receive and resolve ethical dilemmas in a timely
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience
 Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Stroke Distinction Report. Lakeridge Health Oshawa. Oshawa, ON. On-site Survey Dates: October 26, October 29, 2015
 Stroke Distinction Report Lakeridge Health Oshawa Oshawa, ON On-site Survey Dates: October 26, 2015 - October 29, 2015 Report Issued: November 12, 2015 About the Distinction Report Lakeridge Health Oshawa
Stroke Distinction Report Lakeridge Health Oshawa Oshawa, ON On-site Survey Dates: October 26, 2015 - October 29, 2015 Report Issued: November 12, 2015 About the Distinction Report Lakeridge Health Oshawa
TORRANCE MEMORIAL MEDICAL STAFF
 BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
Neurovascular Unit Krembil Neuroscience Centre
 Neurovascular Unit Krembil Neuroscience Centre Information for patients and their families Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca 2016 University
Neurovascular Unit Krembil Neuroscience Centre Information for patients and their families Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca 2016 University
Readiness Assessment Document for Acute Telestroke Collaboration (Sample. Checklist from OTN)
") Readiness Assessment Document for Acute Telestroke Collaboration (Sample Checklist from OTN) Telestroke Referring Site Application This application should be completed in conjunction with your Regional/District
Readiness Assessment Document for Acute Telestroke Collaboration (Sample Checklist from OTN) Telestroke Referring Site Application This application should be completed in conjunction with your Regional/District
Getting Started: How to Operationalize Performance Measures for Your Acute Stroke Ready Hospital
 Getting Started: How to Operationalize Performance Measures for Your Acute Stroke Ready Hospital January 17, 2018 11 AM to 1 PM CST Topics For Discussion State the five standardized performance measures
Getting Started: How to Operationalize Performance Measures for Your Acute Stroke Ready Hospital January 17, 2018 11 AM to 1 PM CST Topics For Discussion State the five standardized performance measures
SITE PROFILE CORNER BROOK
 SITE PROFILE CORNER BROOK Western Memorial Regional Hospital 1 Brookfield Avenue P.O. Box 2005 Corner Brook, NL A2H 6J7 709-637-5000 Site Information: Western Memorial Regional Hospital (WMRH), located
SITE PROFILE CORNER BROOK Western Memorial Regional Hospital 1 Brookfield Avenue P.O. Box 2005 Corner Brook, NL A2H 6J7 709-637-5000 Site Information: Western Memorial Regional Hospital (WMRH), located
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Trauma Center Pre-Review Questionnaire Notes Title 22
 This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Surgical Critical Care Sub I
 Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
Neurocritical Care. Does it make a difference?
 Neurocritical Care Does it make a difference? Dr Hilary Madder Neurosciences Intensive Care Unit John Radcliffe Hospital, Oxford ANZCA Neuroanaesthesia SIG July 2013 Neurocritical Care Capacity 32 neurosurgical
Neurocritical Care Does it make a difference? Dr Hilary Madder Neurosciences Intensive Care Unit John Radcliffe Hospital, Oxford ANZCA Neuroanaesthesia SIG July 2013 Neurocritical Care Capacity 32 neurosurgical
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION
 VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
SARASOTA MEMORIAL HOSPITAL POLICY
 smh0076850ps1070 SARASOTA MEMORIAL HOSPITAL POLICY TITLE EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner: Director, Patient Care 12/09/13 08/19/16 Clinical Non-Clinical
smh0076850ps1070 SARASOTA MEMORIAL HOSPITAL POLICY TITLE EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner: Director, Patient Care 12/09/13 08/19/16 Clinical Non-Clinical
UNMH Neurology Clinical Privileges. Name: Effective Dates: From To
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective May 20, 2016: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective May 20, 2016: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
Nurse Practitioner - Outpatient Lung Transplant (1.0 FTE, Days)
") Nurse Practitioner - Outpatient Lung Transplant (1.0 FTE, Days) Category: Nursing Advance Practice Job Type: Full-Time Shift: Days Location: Palo Alto, CA, United States Req: 5609 FTE: 1 Nursing Advance
Nurse Practitioner - Outpatient Lung Transplant (1.0 FTE, Days) Category: Nursing Advance Practice Job Type: Full-Time Shift: Days Location: Palo Alto, CA, United States Req: 5609 FTE: 1 Nursing Advance
ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA
 ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA QUALITY IMPROVEMENT PROGRAM 2010 Overview The Quality
ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA QUALITY IMPROVEMENT PROGRAM 2010 Overview The Quality
Intracerebral Hemorrhage For patients in the Neuro-Intensive Care Unit
 Intracerebral Hemorrhage For patients in the Neuro-Intensive Care Unit What is it? An Intracerebral Hemorrhage, or ICH, happens when a blood vessel deep inside your brain bursts. The blood then leaks into
Intracerebral Hemorrhage For patients in the Neuro-Intensive Care Unit What is it? An Intracerebral Hemorrhage, or ICH, happens when a blood vessel deep inside your brain bursts. The blood then leaks into
Neonatal Rules Webinar
 Neonatal Rules Webinar Today is the Level III Neonatal Intensive Care Unit (NICU) and Level IV Advanced NICU Rules Webinar. Power Point Presentation and Webinar link will be mailed out to participants,
Neonatal Rules Webinar Today is the Level III Neonatal Intensive Care Unit (NICU) and Level IV Advanced NICU Rules Webinar. Power Point Presentation and Webinar link will be mailed out to participants,
Physician Hospital/SNF Collaborative Guidelines
 Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
The Joint Commission 2016 Medical staff Standards Update
 The Joint Commission 2016 Medical staff Standards Update Session Code: WE01 Date: Wednesday, September 21, 2016 Time: 8:30am - 10:00am Total CE Credits: 1.5 Presenter(s): Paul Ziaya, MD Medical Staff Leadership:
The Joint Commission 2016 Medical staff Standards Update Session Code: WE01 Date: Wednesday, September 21, 2016 Time: 8:30am - 10:00am Total CE Credits: 1.5 Presenter(s): Paul Ziaya, MD Medical Staff Leadership:
Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers. Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care
 Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care Conclusions New paradigm has shifted towards team-based
Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care Conclusions New paradigm has shifted towards team-based
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
The Joint Commission 2017 Medical Staff Standards Update
 The Joint Commission 2017 Medical Staff Standards Update Session Code: TU07 Date: Tuesday, October 24 Time: 11:30 a.m. - 1:00 p.m. Total CE Credits: 1.5 Presenter(s): Louis Goolsby, MD The Joint Commission
The Joint Commission 2017 Medical Staff Standards Update Session Code: TU07 Date: Tuesday, October 24 Time: 11:30 a.m. - 1:00 p.m. Total CE Credits: 1.5 Presenter(s): Louis Goolsby, MD The Joint Commission
Evaluation of Telestroke Services
 Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE
 INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE Bacharach Institute for Rehabilitation offers a number of in and outpatient rehabilitation programs and services designed
INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE Bacharach Institute for Rehabilitation offers a number of in and outpatient rehabilitation programs and services designed
Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program
 Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program Hector E. James M.D., FAANS,FAAP,FCCM. Division of Pediatric Neurosurgery and Lucy Gooding Pediatric
Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program Hector E. James M.D., FAANS,FAAP,FCCM. Division of Pediatric Neurosurgery and Lucy Gooding Pediatric
TELNET COURSE T2861 PART 1 (WEBINAR) TELNET COURSE T2864 PART 2 (WEBINAR) TELNET COURSE T2866 PART 3 (WEBINAR) DATE: SEPTEMBER 26, 2013
 TELNET COURSE T2864 PART 2 (WEBINAR) TELNET COURSE T2866 PART 3 (WEBINAR) DATE: SEPTEMBER 26, 2013") CMS Conditions of Participation (CoPs) for Critical Access Hospitals (CAHS): Ensuring Compliance This is a 3-part series; each program can be taken independent of the others. TELNET COURSE T2861 PART 1
CMS Conditions of Participation (CoPs) for Critical Access Hospitals (CAHS): Ensuring Compliance This is a 3-part series; each program can be taken independent of the others. TELNET COURSE T2861 PART 1
Community Health Network, Inc. MEDICAL STAFF POLICIES & PROCEDURES
 Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
APP PRIVILEGES IN RADIATION ONCOLOGY
 APP PRIVILEGES IN RADIATION ONCOLOGY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the
APP PRIVILEGES IN RADIATION ONCOLOGY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the
RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT
 CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
APP PRIVILEGES IN UROLOGY
 APP PRIVILEGES IN UROLOGY Education/Training Licensure Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification as a
APP PRIVILEGES IN UROLOGY Education/Training Licensure Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification as a
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Provider Frequently Asked Questions (FAQs)
") 1 Provider Frequently Asked Questions (FAQs) November 2012 BlueAdvantage Administrators of Arkansas will be working with AIM Specialty HealthSM (AIM) on a new Integrated Imaging Program for outpatient
1 Provider Frequently Asked Questions (FAQs) November 2012 BlueAdvantage Administrators of Arkansas will be working with AIM Specialty HealthSM (AIM) on a new Integrated Imaging Program for outpatient
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Nursing Care for Acute Ischemic Stroke Patients
 Nursing Care for Acute Ischemic Stroke Patients Highlights of lessons learned 2016 Annie Sanford MSN, RN Stroke Program Manager Swedish Medical Center, Seattle, WA 1 Learning Objectives: By attending this
Nursing Care for Acute Ischemic Stroke Patients Highlights of lessons learned 2016 Annie Sanford MSN, RN Stroke Program Manager Swedish Medical Center, Seattle, WA 1 Learning Objectives: By attending this
Information Technology Report to Medical Executive Committee
 March 10, 2015 z Information Technology Report to Medical Executive Committee Contents 1 Physician Training Opportunities for PowerChart Maternity and FetaLink Launch March 24 at Germantown Hospital 2
March 10, 2015 z Information Technology Report to Medical Executive Committee Contents 1 Physician Training Opportunities for PowerChart Maternity and FetaLink Launch March 24 at Germantown Hospital 2
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
IV. Additional UM Requirements/Activities...29
 I. HMO Responsibilities...2 A. HMO Program Structure... 2 B. Physician Involvement... 3 C. HMO UM Staff... 3 D. Program Scope... 3 E. Program Goals... 4 F. Clinical Criteria for UM Decisions... 4 G. Requirements
I. HMO Responsibilities...2 A. HMO Program Structure... 2 B. Physician Involvement... 3 C. HMO UM Staff... 3 D. Program Scope... 3 E. Program Goals... 4 F. Clinical Criteria for UM Decisions... 4 G. Requirements
AMGA 2013 ANNUAL CONFERENCE
 AMGA 2013 ANNUAL CONFERENCE Mercy Medical Group, Inc. Interdependent Multi-specialty group in Sacramento, CA. Hospital Aligned since 1993 (group practice began 1940 s) > 320 Physicians/APC s 6 Departments
AMGA 2013 ANNUAL CONFERENCE Mercy Medical Group, Inc. Interdependent Multi-specialty group in Sacramento, CA. Hospital Aligned since 1993 (group practice began 1940 s) > 320 Physicians/APC s 6 Departments
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service
 WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
Diagnostic Imaging: Surveyor Education, Survey Experience, and Trends
 Compliance with the AAPM CT Clinical Practice and Joint Commission Guidelines Diagnostic Imaging: Surveyor Education, Survey Experience, and Trends On-Site Survey focused on patient care: Patient Tracer
Compliance with the AAPM CT Clinical Practice and Joint Commission Guidelines Diagnostic Imaging: Surveyor Education, Survey Experience, and Trends On-Site Survey focused on patient care: Patient Tracer
Hospital Service Accountability Agreements
 2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
Duke Life Flight. Systems of Care for Time Dependent Emergencies. Disclosures. Disclosures 9/19/2017
 Duke Life Flight Systems of Care for Time Dependent Emergencies Claire M Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center Wilmington, NC Disclosures Clinical
Duke Life Flight Systems of Care for Time Dependent Emergencies Claire M Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center Wilmington, NC Disclosures Clinical
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Penrose-St Francis Hospital
 Advanced Practice Nurse Please check applicable credential [ ] Nurse Practitioner [ ] Clinical Nurse Specialist [ ] Certified Nurse Midwife [ ] Certified Registered Nurse Anesthesist Area of focus _ ***************************************************************
Advanced Practice Nurse Please check applicable credential [ ] Nurse Practitioner [ ] Clinical Nurse Specialist [ ] Certified Nurse Midwife [ ] Certified Registered Nurse Anesthesist Area of focus _ ***************************************************************
ABOUT THE CONE HEALTH NETWORK OF SERVICES
 THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
INSERT ORGANIZATION NAME
 INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
1. PROMOTE PATIENT SAFETY.
 SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
WHAT YOU NEED TO KNOW! CMS (Medicare)! and! The Joint Commission CSC! Updates!
! and! The Joint Commission CSC! Updates!") !!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
!!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
Bethesda Hospital PGY1 Residency Program Learning Experiences
 Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,