GASTROENTEROLOGY TRAINING PROGRAM CURRICULUM AND OBJECTIVES
|
|
|
- Winifred Snow
- 6 years ago
- Views:
Transcription
1 2 GASTROENTEROLOGY TRAINING PROGRAM CURRICULUM AND OBJECTIVES TITLE OF PROGRAM: State University of New York Upstate Medical University, Gastroenterology Fellowship Training Program SPONSOR: State University of New York PARTICIPATING INSTITUTIONS: State University of New York Upstate Medical University, Veteran s Administration Medical Center at Syracuse, Upstate University Hospital Community Campus; Oswego Health system, Oswego, NY. PROGRAM DIRECTOR: Ronald D. Szyjkowski, M.D. Professor of Medicine and Pediatrics Chief, Division of Gastroenterology State University of New York Upstate Medical University 750 East Adams Street Syracuse, New York Phone:(315) Fax: (315) DATE LAST MODIFIED: August 2017 INTRODUCTION: The purpose of this document is to outline the subspecialty education program in gastroenterology fellowship training, sponsored by the State University of New York Upstate Medical University. Fellowship training in gastroenterology is a three-year program, and successful completion of this fellowship training will allow candidates to be eligible for certification examination in the subspecialty of gastroenterology by the American Board of Internal Medicine. The curriculum and objectives in this document are outlined in accordance with program requirements for residency education in gastroenterology, published by the Accreditation Council for Graduate Medical Education (ACGME). A candidate is selected for GI fellowship based on a number of factors. These include, but are
2 not limited to: performance on standardized test; grades and transcripts, letters of recommendation (3); degree of research experience; personal statements; academic interests; ability to speak and understand English; completion of Internal Medicine Residency training and at least Board Eligible status; and interview performance. Our program has been accredited since Twenty-two+ fellows have successfully completed our GI Fellowship during this time. To date, all of our GI fellows have been Board Certified. I. PROGRAM OUTLINE - GENERAL A. Training in the gastroenterology fellowship program will provide opportunities for fellows to develop clinical competence in the field of gastroenterology, including exposure to hepatology, clinical nutrition, gastrointestinal oncology, radiology, and pathology. While this is a subspecialty program, training will emphasize the trainee functioning as a total academic physician, internist and consultant, with interest in the entire person and his/her environment. B. The training program will be three years in duration and will provide the opportunity for the trainee to observe and manage patients with a wide variety of digestive disorders in both the outpatient and inpatient setting. C. The training program will provide access to the basic and clinical sciences necessary to develop the skills necessary to practice sound gastroenterology. D. The training program will be designed to teach critical analysis and reasoning relative to clinical and investigative problems in gastroenterology, and to consider choices in light of current cost/benefit analysis. E. The training program will be designed to teach both cognitive and technical aspects of gastrointestinal endoscopy. F. The training program will offer in-depth interaction with other disciplines such as radiology, pathology, surgery, pediatrics and nutrition. Principles of psychosomatic medicine will also be taught. G. While this is primarily a clinical training program, it is recognized that research training is mandatory for all fellows in training and will receive appropriate emphasis. 3
3 II. TEACHING STAFF All Faculty receive training in work hour rules, moonlighting and general policy regarding Fellows service annually. In conjunction with this training a refresher/review of fatigue recognition and management will be conducted during the annual Fellowship orientation meeting. Strategies for assessing learners for - and helping learners with - fatigue, triage, and stress management will be reviewed at training session. Effective July 1, 2010 a Faculty Attestation form will be completed regarding training documentation. Teaching Attendings are to attend greater than 50% of all required teaching conferences and all appropriate 360 degree evaluations. A. The following are the full-time key academic staff of the State University of New York Upstate Medical University Gastroenterology Fellowship Training Program: BOARD CERTIFIED IM GI Hep Uma Murthy, MD C C Ronald D. Szyjkowski, MD C C Ajoy Roy, MD C C C Savio John, MD C C C Sekou Rawlins, MD C C David Heisig, MD C C Anand Gupta, MD C C Nuri Ozden, MD C C Muhammad Osman Arif, MD C C Divey Manocha, MD C C Bishnu Sapkota, MD C C IM = Internal Medicine GI = Gastroenterology Hep = Hepatology C = Board Certified E =Board Eligible B. The following are non-full-time staff (Academic Emeritus) of the State University of New York Upstate Medical University Gastroenterology Fellowship Training Program: Philip G. Holtzapple, MD 3
4 D. The following are Research mentor staff of the State University of New York Upstate Medical University Gastroenterology Fellowship Training Program: currently none. III. CONSULTANTS Scholarly input from outside consultants the advent of recorded talks, societal programs such as the ACG universe and didactic material from major scholarly meetings have allowed this function to now include prepared teaching programs. These consultants are of the highest caliber and enjoy a national and often international reputation and may at time be virtual. When possible, interaction will be structured to provide a close, intense, small group experience in which clinical problems are discussed in detail and questions are encouraged to maximize the learning experience. IV. RESOURCES A. General and Patient Population - The participating institutions and facilities for the State University of New York Upstate Medical University are the Upstate Medical University, including the Veteran s Administration Medical Center at Syracuse and the Oswego Health System, Oswego N.Y. Both Syracuse facilities are tertiary care referral centers which provide staff support and material consistent with tertiary care referral hospitals. The OHS, including affiliated out-patient clinics, is a local, regional leader in community level health care. The general medical patient population is diverse and is derived from the population base living in and around the immediate Syracuse area. Additionally, Upstate Medical University is the major referral center for central New York servicing outlying facilities from the Canadian border to Pennsylvania and Veteran s Administration Medical Center at Syracuse serves as the primary referral hospital for a variety of outlying hospitals and clinics. It is the major source for veteran s inpatient care in central New York. Additionally, patients are also referred from local military bases. B. Physical Plant - The Gastroenterology Services at all three hospitals have very modern physical facilities that provide adequate office space, as well as individual areas for each 4
5 type of diagnostic and therapeutic procedures and modalities. Both hospitals share the medical school s library facility which provides an excellent selection of current gastroenterology and internal medicine textbooks and journals. C. Inpatient Facilities - The Gastroenterology Service provides consultative services to patients who are admitted to each facility. D. Endoscopic Facilities and Equipment - The Gastroenterology Services of both hospitals enjoy state-of-the art equipment, which permits safe and skillful performance of the latest diagnostic and therapeutic endoscopic procedures. The faculty at both institutions possesses the technical expertise and access to the equipment to perform the following procedures: 5 HSC VAMC OHS Upper endoscopy Y Y Y Colonoscopy Y Y Y Flexible sigmoidoscopy Y Y Y Percutaneous liver biopsy Y Y Y Percutaneous endoscopic gastrostomy Y Y Y ERCP: Diagnostic Y Y Y Sphincterotomy Y Y Y Balloon cholangioplasty & pacreatoplasty Y Y Y Insertion of biliary and pancreatic stents Y Y Y Endoscopic lithotripsy Y Y Y Biliary manometry Y N N Choledochoscopy Y Y N Endoscopic laser therapy Y N N Endoscopic therapeutic Hemostasis: Laser Y N N Bicap Y Y Y Heater probe Y Y N Injection sclerotherapy Y Y Y Variceal band ligation Y Y Y Argon plasma coagulator Y Y N Endoscopic ultrasound - diagnostic Y Y N
6 Endoscopic ultrasound - therapeutic Y Y N Esophageal manometry Y Y N Esophageal ph studies Y Y N Anal rectal manometry Y N N Photodynamic Therapy Y N N Capsule Endoscopy Y Y Y Radio Frequency Ablation Y Y N All institutions have state-of-the art fluoroscopy and x-ray equipment available for performing endoscopic procedures requiring the assistance of fluoroscopy. Endoscopic equipment is also available for performing endoscopic procedures outside the endoscopy suites, to include those performed in various intensive care units throughout the hospitals. All facilities have endoscopic equipment which is completely computerized and utilizing video endoscopy. V. ROTATIONS A. GENERAL - The fellows in gastroenterology program will all receive training at all three facilities. Rotations at other facilities, which offer specialty training or expertise not available from either institution, will be allowed and encouraged based on the fellows interest. The three year fellowship is divided into 39 fourweek blocks or 13 blocks per year. At least 18 months will be devoted entirely to clinical gastroenterology, of which approximately 35% of which will be related to diseases of the liver. The third year of gastroenterology fellowship training will stress research, advance therapeutics to include ERCP and endoscopic ultrasound, and motility training. Training in hepatic transplantation, clinical nutrition, and pediatric gastroenterology will also be encouraged. The fellows will also be exposed to approximately 1-2 months of inpatient consultative rotations during the third year of fellowship. The specific details of the rotations follow. B. GENERAL OUTPATIENT CLINIC ROTATION (1 st and 2 nd YEAR FELLOWS 9-11 BLOCKS TOTAL) - Examines and treats scheduled and unscheduled patients with a wide variety of common gastrointestinal conditions. Fellows will also see more acute emergency patients with more complex problems, requiring interaction with surgical and radiology departments at all three facilities. By their nature each facility will have different patient populations and consultative experiences, allowing the fellow to learn how to manage inpatients in various settings/practice patterns, which is our goal. Patients are followed for their 6
7 active problems or referred back to the primary physician. When appropriate, long-term follow up will be continued through the fellow s continuity clinic. Fellows will perform GI endoscopic procedures on such patients after a determination is made that such procedures are required. The second year fellow will begin to be exposed to motility as well as some advanced diagnostic and therapeutic procedures during this rotation. GOALS: The outpatient rotation is designed to allow the trainee to gain expertise in handling a multitude of common gastrointestinal problems, not only from a scientific standpoint, but also to include psychosocial considerations. Experience at determining appropriate follow-up intervals and scheduling is also gained, thus develop clinical competence in the field of gastroenterology. All fellows will be assessed for the six competencies as outlined on the Internal medicine Resident evaluation Form, including patient care, medical knowledge base, practice based learning, interpersonal and communication skills, professionalism and systems based learning. Overall all clinical acumen and competence will also be assessed. On going assessment of progress will be included in the evaluation process at all levels. The first year fellow will be evaluated based on ability to develop a pertinent and coherent differential diagnosis based on a history and physical. The fellow s knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be assessed for competency and to ensure adequate progression and maturation. The second year fellow will be expected to have mastered the basic ability to develop a pertinent and coherent differential diagnosis based on a history and physical and will be evaluated on being able to appropriately focus that evaluation on the gastrointestinal tract. The fellow s knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be assessed for competency and to ensure adequate progression and maturation. The fellow should be beginning to master integration of data to form a coherent assessment and plan. C. INPATIENT CONSULTATIONS (ALL FELLOWS BLOCKS TOTAL) - During those rotations the fellows consult on patients with gastrointestinal problems at all three sites, depending upon assignment, hospitalized on various inpatient wards including general medicine, surgical, pediatric wards, and various intensive care units throughout both institutions. The fellow evaluates patients and advises primary care and specialty services physicians of his diagnostic impressions, recommended diagnostic tests and appropriate therapy. The trainee also performs endoscopic procedures or other GI procedures generated by such patient contacts, under the direct supervision of the attending staff. 7
8 GOALS: To evaluate patients who are generally sicker than those seen in the outpatient setting at an academic center, a mixed academic and closed population center and a community practice depending upon assignment. Complex co-morbid inpatient problems are seen more commonly at the university and the VA Medical Center while generally lower acuity patients are seen at the Oswego site. This mix aids in the development of factual knowledge, reasoning ability and problem solving. In addition, the trainee learns the art of consultative medicine in different clinical settings, which requires interaction with the primary and specialty physicians to influence the final diagnostic and therapeutic decisions. This activity develops experience with differing levels of like it assertiveness and diplomacy. All fellows will be assessed for the six competencies as outlined on the Internal medicine Resident evaluation Form, including patient care, medical knowledge base, practice based learning, interpersonal and communication skills, professionalism and systems based learning. Overall all clinical acumen and competence will also be assessed. On going assessment of progress will be included in the evaluation process at all levels and at each site. The first year fellow will be evaluated based on ability to develop a pertinent and coherent differential diagnosis based on a history and physical. The fellow will also be evaluated on their ability to adequately triaging of consults. Instruction and assessment will be geared toward allowing the fellow to develop his / her knowledge base and clinical experience to that end, and therefore the greater percentage of this experience will be at University Hospital and the VA Medical Center. The fellow s knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be assessed for competency and to ensure adequate progression and maturation. The second year fellow will be expected to have mastered the basic ability to develop a pertinent and coherent differential diagnosis based on a history and physical and will be evaluated on being able to appropriately focus that evaluation on the gastrointestinal tract and therefore will have a greater presence at the Oswego center in the latter part of the year. The fellow will be assessed for their ability to appropriately triage consults and will be expected to be significantly more proficient than during the first year. The fellow s knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be assessed for competency and to ensure adequate progression and maturation. The fellow should be beginning to master integration of data to form a coherent assessment and plan and will be expected to be beginning to transition toward independent inpatient consultation. The third year fellow will be expected to not only have mastered the basic ability to develop a pertinent and coherent differential diagnosis based on a history and physical but also to be able to 8
9 appropriately focus that evaluation on the gastrointestinal tract. The fellow should be able to consistently make appropriate triage decisions. The fellow should be virtually competent in his / her knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be expected to continue to progress toward being able to practice independently and therefore they will be afforded the opportunity to have the bulk of activity at the Oswego Center. The inpatient staff will specifically assess the fellow s ability to integrate of data to form a coherent assessment and plan. This plan should include appropriate use of ancillary services and assessment of the most medically appropriate venue (i.e. outpatient versus inpatient.) The fellow will be specifically assessed for the ability to transition to independent inpatient consultation. D. ADVANCED OUTPATIENT CLINIC ROTATION (3rd YEAR FELLOW 6-8 BLOCKS TOTAL) As with the general outpatient clinic rotation (B. above) the fellow examines and treats scheduled and unscheduled patients with a wide variety of unusual gastrointestinal conditions. The fellows see more acute emergency patients with more complex problems, requiring therapeutic intervention such as with ERCP. The fellow will be allowed to assess patients sent for and to perform the majority of motility and ph studies in conjunction with the attending staff. Patients are followed for their active problems or referred back to the primary physician or gastroenterologist. When appropriate, long term follow up will be continued through the fellow s continuity clinic. The fellow s clinic schedule will be structured so that they can participate in didactic discussions about these cases and so that they can perform or assist in performing all therapeutic and advanced diagnostic at both facilities. GOALS: To allow a truly didactic setting in which the fellow can be exposed to and learn from complicated cases requiring advanced diagnostic and therapeutic modalities. To give the fellow greater responsibility in determining the best overall care plan for the patients they are consulted on. It is not the goal of this rotation to ensure sufficient skill is developed to recommend independent practice in these procedures after graduation. The third year fellow will be expected to not only have mastered the basic ability to develop a pertinent and coherent differential diagnosis based on a history and physical but also to be able to appropriately focus that evaluation on the gastrointestinal tract. The fellow should be virtually competent in his / her knowledge of indications and contraindications to medicines, therapeutic plans and endoscopy will be expected to continue to progress toward being able to practice independently. The fellow should be able to integrate of data to form a coherent assessment and plan. The fellow will be specifically assessed for the ability to transition to independent practice. 9
10 At the same time the fellow will be assessed for the six competencies as outlined on the Internal medicine Resident evaluation Form, including patient care, medical knowledge base, practice based learning, interpersonal and communication skills, professionalism and systems based learning. E. RESEARCH AND SCHOLARLY ACTIVITIES (FIRST YEAR FELLOW 2 MONTHS, SECOND YEAR FELLOW 2 MONTHS, THIRD YEAR FELLOW 3 MONTHS) - The research rotation will be conducted under through the Graduate Medical Education Office under the auspices of Clinical Investigation Divisions at the Upstate Medical University and Veterans Administration Medical Center. Fellows will be exposed to research activities by designing a clinical or basic science research protocol, which would then be submitted for approval by the Institutional Review Board and Human Use Committee of the respective institutions. Once the protocols have been approved, fellows will then conduct the study under the supervision of a staff gastroenterologist, in cooperation with other members of facilities where appropriate. Fellows will be taught how to analyze data and apply statistical techniques to interpret such data. A manuscript will then be prepared which will be submitted to satisfy fellowship program graduation requirements. Preparation of a publishable piece of investigation, either clinical or basic science, is required for graduation. GOALS: To acquaint the trainee with the scientific method by asking and attempting to answer a question of biomedical important. It is expected that the research performed will eventually lead to a scientific presentation at a national meeting and a published manuscript. First year fellows will be expected to develop a hypothesis and complete a research proposal and have it evaluated by the appropriate reviewing board. This will be in conjunction with a staff of the fellow s choice who agrees to support the project. The second year will be expected to complete virtually all of his / her data collection in conjunction with their staff and in preparation for manuscript preparation, presentation, etc. The third year fellow will be expected to prepare a manuscript in publishable format in conjunction with their staff. This will be reviewed by the collective teaching faculty for adequacy and will be reviewed during a monthly research meeting or journal club. F. Pregnancy in Gastrointestinal disorders 10
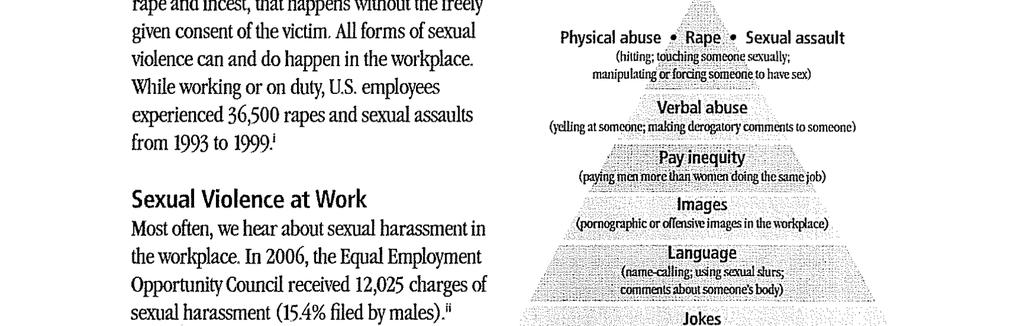
11 This monograph is available in our curriculum library both in print form (which will be stored in the fellow's library at the CWB) and virtually. (To view virtually, please request from Division Secretary ) The structure of our educational system is such that fellows have less than average exposure to pregnant patients, therefore reading of this document will be required. Each fellow will sign an attestation form documenting this once during their fellowship. As a part of their duties regarding conference scheduling, the third year fellow will insure that at least one Tuesday lecture each quarter will be devoted to topics in this document. G. Monograph on IBS, Constipation and Acid-Related Disorders This monograph is available in our curriculum library virtually. (To view virtually, please request from Division Secretary krauseb@upstate.edu ) Reading of this document will be required. Each fellow will sign an attestation form documenting this once during their fellowship. H. Module on Nutrition Each fellow will sign an attestation form documenting this once during their fellowship. I. To report patient safety events, click on link occurrence reporting J. Sexual violence Copy of Workplace Sexual Violence flyer below. Each fellow will sign an attestation form documenting this once during their fellowship. Each attending, NP, PA will sign an attestation form documenting the review of this flyer at beginning of their employment. 11
12 12
13 13
14 K. IHI Quality/Safety Modules-Basic Certificate Requirement to be completed by All Fellows in their First Year. Please reference the attached instruction page for accessing education module. Milestones First Year: a. Esophagogastroduodenoscopy - Minimum of 25 supervised studies b. Esophageal dilations - Minimum 5 supervised studies c. Colonoscopy with polypectomy - Minimum of 25 supervised colonoscopies and 5 supervised polypectomies d. Percutaneous endoscopic gastrostomy - Minimum of 3 supervised studies and completion of didactic training in complications and anatomy and physiology of replacement relative to time of placement e. Biopsy of the mucosa of the esophagus, stomach, small bowel and colon - Minimum 5 supervised studies any site f. Moderate sedation Completion to competence g. Summary of evaluations showing adequate performance in each of the six core competencies Second Year: a. Esophagogastroduodenoscopy - Minimum of 50 supervised studies b. Esophageal dilations - Minimum 10 supervised studies c. Colonoscopy with polypectomy - Minimum of 50 supervised colonoscopies and 10 supervised polypectomies d. Percutaneous endoscopic gastrostomy - Minimum of 6 supervised studies e. Biopsy of the mucosa of the esophagus, stomach, small bowel and colon - Minimum 5 supervised studies each site f. Other diagnostic and therapeutic procedures utilizing enteral intubation and bouginage - Minimum 5 supervised studies g. Non-variceal hemostasis - Minimum 5 supervised studies h. Variceal hemostasis - Minimum 5 supervised studies i. Summary of evaluations showing adequate performance in each of 14
15 the six core competencies 15 Third Year: a. Esophagogastroduodenoscopy - Minimum number to be performed supervised studies and demonstrate competence b. Esophageal dilations - Minimum 50 supervised studies studies and demonstrate competence c. Colonoscopy with polypectomy - Minimum of 140 supervised colonoscopies and 30 supervised polypectomies studies and demonstrate competence d. Percutaneous endoscopic gastrostomy - Minimum of 15 supervised studies studies and demonstrate competence e. Biopsy of the mucosa of the esophagus, stomach, small bowel and colon - demonstrate competence f. Other diagnostic and therapeutic procedures utilizing enteral intubation and bouginage - demonstrate competence g. Gastrointestinal motility studies - minimum of 20 each of ph and esophageal motility studies and demonstrate competence h. Non-variceal hemostasis - Fellows will perform 25 supervised cases including 10 active bleeders studies and demonstrate competence i. Variceal hemostasis - 20 supervised cases, including 5 active bleeders studies and demonstrate competence j. Moderate sedation studies and demonstrate competence k. Small bowel capsule endoscopy studies and demonstrate competence l. Complete original research report in publishable form m. Summary of evaluations showing adequate performance in each of the six core competencies The major advancement milestones in the area of gastroenterology for the general internist in training are divided into three general areas: Inpatient Urgent, Routine Inpatient and Outpatient. It is important that all members of the team (including our fellows) be aware of these and that they also recognize they are a major part of the process. These are listed here.
16 INPATIENT URGENT By the end of the first year the R1 will be able to rapidly assess and triage the inpatient presenting with symptom and sign complexes typical of common urgent diagnoses including but not limited to GI bleeding, cholangitis, appendicitis, perforation, bowel obstruction, SBP, etc. The learner will have the ability to perform a full abdominal exam to facilitate the evaluation of their patient. The needs for routine stabilization will be easily identified. By the end of the second year the R2 will be able to identify and prioritize the appropriate testing to guide initial therapy decisions for common urgent diagnoses including but not limited to GI bleeding, cholangitis, appendicitis, perforation, bowel obstruction, SBP, etc. The learner will be able to initiation measures for routine stabilization and resuscitation. By the end of the third year the R3 will be able to initiate therapy for common and more unusual urgent diagnoses including but not limited to GI bleeding, cholangitis, appendicitis, perforation, bowel obstruction, SBP, IBD, ischemia, etc. After assessing and understanding the likelihood of response to standard medical therapy the R3 will be able to determine when subspecialty consultation is appropriate, thereby being able to fully practice independently. INPATIENT ROUTINE By the end of the first year the R1 will be able to assess and triage the inpatient presenting with typical routine internal medicine symptoms and conditions related to the gastrointestinal tract including but not limited to loose stools, nausea, vomiting, pain and abnormal labs / x-rays etc. The learner will have the ability to perform a full abdominal exam to facilitate the evaluation of their patient. The learner will be facile in routine initiation of assessment and directed therapy will be easily identified. By the end of the second year the R2 will be able to synthesize and work through the differential diagnosis selecting appropriate testing and initial therapy for typical routine internal medicine symptoms and conditions related to the gastrointestinal tract including but not limited to loose stools, nausea, vomiting, pain and abnormal labs / x-rays etc. The learner will demonstrate the ability to integrate patient information from multiple internal and external sources. The learner will also be able to work with the available systems to initiated disposition plans and will begin to apply these skills at the Oswego Center. 16
17 By the end of the third year the R3 will be able to independently chose therapy and testing for typical routine internal medicine symptoms and conditions related to the gastrointestinal tract including but not limited to loose stools, nausea, vomiting, pain and abnormal labs / x-rays etc. in an academic, VA or community setting. After assessing and integrating all available data and understanding the likelihood of response to standard medical therapy the R3 will be able to determine when subspecialty consultation is appropriate based upon available skill sets at any level, thereby being able to fully practice independently. OUTPATIENT By the end of the first year the R1 will be able to assess and triage the clinic patient presenting with typical routine internal medicine symptoms and conditions including such conditions as reflux, abnormal liver functions while understanding the standard preventative measures such as colorectal cancer screening and vaccinations. The learner will have the ability to perform a full abdominal exam to facilitate the evaluation of their patient. The learner will be facile in routine initiation of symptom directed assessment and understand the pharmacology of typical gastrointestinal medications. By the end of the second year the R2 will be able to synthesize and work through the differential diagnosis selecting appropriate testing and initial therapy for the clinic patient presenting with typical routine internal medicine symptoms and conditions including such conditions as reflux, abnormal liver functions while understanding the standard preventative measures such as colorectal cancer screening and vaccinations, enacting and making future follow up plans including subspecialty consultation The learner will demonstrate the ability to integrate patient information from multiple internal and external sources and determining the pharmacologic interactions of existing medications with planned gastroenterological therapeutics. The learner will also be able to work with the available systems to initiated disposition plans. By the end of the third year the R3 will be able to independently choose therapy and testing for typical routine and more esoteric condition more complicated than conditions such as reflux, abnormal liver functions while understanding the standard preventative measures such as colorectal cancer screening and vaccinations. The learner will be able to integrate and coordinate the care of these conditions themselves as well as in interaction with other medical problems and therapeutics. After assessing and integrating all available data and understanding the likelihood of response to standard medical therapy using multiple sources (including when 17
18 appropriate outside information) the graduating R3 will be able to follow through on and coordinate subspecialty consultation recommendations, thereby being able to fully practice independently, guiding and orchestrating their care so as to avoid polypharmacy, drug / drug interactions etc. VI. CONFERENCE SCHEDULE A. GENERAL: Fellows will attend at least ninety percent of gastroenterology conferences. An attendance record will be maintained. Some conferences will be combined with other functions at either institution and/or the medical school. Other services, students, residents and the gastroenterology community are encouraged to attend all fellowship conferences. B. CONFERENCES FOR FELLOWSHIP TRAINING: 1. Pathology Conference (Bi-Weekly) - Recognizing that changes in department of pathology faculty availability and service constraints, as well as changes in technology, teaching material / methods we are presented with an opportunity to improve how our didactic pathology teaching. These organ systems and pathophysiologically based bi weekly didactics which are integrated with our board review schedule are staffed by Upstate Department of Pathology faculty. On alternate weeks recent cases of teaching interest are reviewed with the staff pathologist. This allows correlation of endoscopic findings with histopathology. In addition, specific areas of interest are targeted for discussion with appropriate histologic material for review. At the midway point of academic year 2017/2018 we will reassess if our goal of increasing pathologic information into the day to day practice and education is working. 2. GI Radiology Conference (Monthly October - June) - Cases are selected either by the Gastroenterology Service or by the Radiology staff presenting the conference. Common and uncommon radiologic features are reviewed. This may be on a selected interesting case or targeted topic basis. Normal anatomy as well as imaging techniques and general principles of radiology will also be covered (and will also be addressed in Clinical and Basic Science Conferences 4 and 5 below). 3. Case Conference (Weekly) - The entire staff including house staff and fellow physicians meet to discuss either perplexing diagnostic cases or management problems so that all may be allowed to participate and contribute their knowledge and experience. The fellow 18
19 presenting the case also reviews and formally presents the most recent and/or pertinent literature concerning the case. Specific attention to the nutritional aspects of ongoing patient care will be explored when appropriate. At least once a month on average a case specifically focusing on nutrition will be discussed. 4. Clinical Conference Series (Biweekly) - A series of lectures, usually of didactic nature, on common clinical problems, diagnostic techniques or therapeutic modalities, are presented by both staff and trainees on a rotating basis. The topics are spread out over a three year period, so that during the entire fellowship training the fellows are exposed to each lecture only once during their training. The only exception is those topics that the staff feels the fellows (especially the incoming first year fellow) must be exposed to on a yearly basis. For this conference, slides are prepared utilizing a variety of slide making software such as Harvard Graphics or Power Point, both of which are readily available within the department. Handouts or lecture outlines are also highly encouraged. Feedback via form will be given to both staff and fellows. The fellow s performance and progression will be included as a part of their training recorded. 5. Basic Science Conference (Biweekly) - A series of lectures by both staff and fellow physicians, covering basic science and physiology topics. These topics are spread over the entire three year fellowship training, so that fellows are exposed to each topic once during their fellowship. For this conference, slides are prepared utilizing a variety of slide making software such as Harvard Graphics or Power Point, both of which are readily available within the department. Handouts or lecture outlines are also highly encouraged. Feedback via form will be given to both staff and fellows. The fellow s performance and progression will be included as a part of their training recorded. 6. Journal Club (Monthly) - Articles from the general medical literature, as well as gastroenterology journals, are reviewed by the entire Service. Critical review of scientific articles is emphasized. Important articles and reviews are Xeroxed for lateral review and permanent files. 7. Research Conference (Monthly) The status of on-going fellow research projects will be tracked and reviewed on a monthly basis. This will include independent projects for graduation requirements as well as other projects on which fellows are assistant investigators. This forum, often in conjunction with Journal Club, will also be used to develop research ideas. Staff will be serving as a sounding board for these ideas, shepherding and mentoring the fellows in the development of these hypotheses. Research design principles, ethics of research, informed 19
20 consent standards, human subject use, etc. will be an a priori part of these sessions. 8. Internal Medicine Grand Rounds AKA Chairman s Rounds (Monthly) - Topics of general medicine interest are presented by UMU and VAMC staff or by distinguished visiting professors. Participation is hospital wide. 9. GI / Surgery Conference (weekly) - Cases are selected by both the Gastroenterology Service and the Surgery staff for presentation at the conference. Common and uncommon cases are reviewed with emphasis on interaction between the specialties, thereby promoting system integration, professional relations and teamwork. This may be on a selected interesting case or targeted topic basis. Surgical technique and approach will be discussed for the benefit of the medical trainees, and medical approaches will be discussed for the benefit of the surgical trainees. Radiological and pathologic input will be solicited when appropriate. 10. Pregnancy in Gastrointestinal disorders (Quarterly) As a part of their duties regarding conference scheduling, the third year fellow will insure that at least one Tuesday lecture each quarter will be devoted to topics in this document. 11. VA GI Tumor Multi-Disciplinary Conference (Monthly) All UH GI Fellows will attend/participate in this GI conference. Cases may be assigned to an individual Fellow discussion will follow presentation. 12. Nutrition (Quarterly) As a part of their duties regarding conference scheduling, the third year fellow will insure that at least one Tuesday lecture each quarter will be devoted to this topic. In addition to lecture, below link will be reviewed. An outpatient fellow will prepare weekly case conference based on the published and equally distributed schedule in conjunction with their supervising attending mentor. First year fellows will be assigned a minimum of one clinical and one basic science lecture per year. During subsequent years fellows will be expected to select a minimum of two topics based on the core curriculum cycle and trainee interest. Fellows are expected to select cases for pathology, radiology and gastrointestinal / Surgery conference, as well as articles for review during journal club. The third year fellow will be the point of contact for coordination of these cases. The attending staff will evaluate the lecture and feedback will be provided to the trainee informally and formally at the bi-annual assessment. 20
21 ACP High Value Curriculum(reference) VII. CORE CURRICULUM A. CLINICAL EXPERIENCE, CONCEPTS AND FACTS - This will include an opportunity to observe and manage a sufficient number of new and follow-up inpatients and outpatients of appropriate age, including adolescent and geriatric age groups, with a wide variety of common and uncommon digestive orders. Fellows will be given opportunities to assume continuing responsibility for both acute and chronically ill patients, to learn the natural history of gastroenterologic disorders, as well as effectiveness of therapeutic programs. Specifically, the fellows will receive formal instruction, clinical experience, and opportunities to acquire expertise in the evaluation and management of the following disorders: Diseases of the esophagus 2. Acid peptic disorders of the gastrointestinal tract 3. Motor disorders of the gastrointestinal tract 4. Irritable bowel syndrome 5. Disorders of nutrient assimilation 6. Inflammatory bowel diseases 7. Vascular disorders of the gastrointestinal tract 8. Gastrointestinal infections including viral, bacterial, mycotic and parasitic diseases 9. Gastrointestinal pancreatic neoplasms 10. Gastrointestinal diseases with an immune basis 11. Pancreatitis 12. Gallstones and cholecystitis 13. Alcoholic liver diseases 14. Viral and immune hepatitis 15. Cholestatic syndromes 16. Drug-induced liver injury 17. Hepatobiliary neoplasms 18. Chronic liver disease 19. Gastrointestinal manifestations of HIV infections
22 20. Gastrointestinal neoplastic disease 21. Acute and chronic hepatitis 22. Biliary and pancreatic diseases 23. Women s health issues in digestive diseases 24. Geriatric gastroenterology 25. Gastrointestinal bleeding 26. Cirrhosis and portal hypertention 27. Genetic/inherited disorders 28. Medical management of patients under surgical care for gastrointestinal disorders 29. Management of GI emergencies in the acutely ill patient 2. Fellows will also receive formal instruction, clinical experience, and opportunities to acquire expertise in the evaluation and management of the patients with the following clinical problems: a. Dysphagia b. Abdominal pain c. Acute abdomen d. Nausea and vomiting e. Diarrhea f. Constipation g. Gastrointestinal bleeding h. Jaundice i. Abnormal liver chemistries j. Cirrhosis and portal hypertension k. Malnutrition l. Genetic/inherited disorders m. Depression, neurosis and somatization syndromes pertaining to the gastrointestinal tract n. Surgical care of gastrointestinal disorders B. ENDOSCOPIC PROCEDURES, TECHNICAL AND OTHER SKILLS - 1. The program will provide for instruction in the indications, contraindications, complications, limitations, and where applicable, interpretation of the 22
23 following diagnostic and therapeutic techniques and procedures. a. Imaging of the digestive system including: (1) Ultrasound procedures, including endoscopic ultrasound (2) Computed tomography (3) Magnetic resonance imaging (4) Vascular radiology procedures (5) Contrast radiography (6) Nuclear medicine procedures (7) Percutaneous cholangiography b. Endoscopic procedures. c. Specialized dilation procedures d. Percutaneous cholangiography e. Percutaneous endoscopic gastrostomy (1) placement (2) appropriate replacement f. Liver and mucosal biopsies g. Gastric, pancreatic and biliary secretory tests h. Other diagnostic and therapeutic procedures utilizing enteral intubation and bouginage i. Gastrointestinal motility studies j. Sclerotherapy k. Enteral and parenteral alimentation l. Liver transplantation m. Pancreatic needle biopsy n. ERCP including papillotomy and biliary stent placement 2. Opportunities will be provided for fellows to gain competence in the following procedures and a skill endoscopic preceptor will be available to teach and supervise the procedures. The performance of these procedures will be documented in the fellow s record, providing indications, outcomes, diagnosis, and supervisor(s). 23 a. Esophagogastroduodenoscopy - Minimum number to be performed supervised studies b. Esophageal dilations - Minimum 50 supervised studies c. Flexible sigmoidoscopy - Minimum 30 supervised studies d. Colonoscopy with polypectomy - Minimum of 140 supervised
24 colonoscopies and 30 supervised polypectomies e. Percutaneous endoscopic gastrostomy - Minimum of 15 supervised studies and completion of didactic training in complications and anatomy and physiology of replacement relative to time of placement f. Biopsy of the mucosa of the esophagus, stomach, small bowel and colon g. Other diagnostic and therapeutic procedures utilizing enteral intubation and bouginage h. Non-variceal hemostasis - Fellows will perform 25 supervised cases including 10 active bleeders i. Variceal hemostasis - 20 supervised cases, including 5 active bleeders j. Enteral and parenteral alimentation k. Moderate sedation l. Small bowel capsule endoscopy m. Esophageal capsule endoscopy 3. While fellows may not directly perform them, exposure to the following diagnostic and therapeutic procedures will be provided: a. Laser treatment of gastrointestinal tract b. Endoscopic ultrasound c. Biliary manometry d. ERCP e. Endoluminal Reflux Therapy f. Radio frequency Ablation g. Percutaneous liver biopsy - Minimum of 20 supervised studies h. Gastrointestinal motility studies As a part of the fellow s orientation and prior to initially performing any endoscopic procedure, the trainee will review available introductory literature through books, videotapes, and slide films. Subsequently, throughout training, the supervising staff member will review the indications for each procedure, as well as complications and treatment, along with the clinical utility and limitations of each procedure on a case by case basis, as well as in a didactic fashion during our conference/lecture series. Knowledge of the operational and maintenance aspects of endoscopic instruments is also considered
25 essential, and is therefore included in the fellow s initial orientation. 5. A qualified staff physician will provide daily, close and immediate supervision of scheduled and emergent cases. After the trainee has reached a competent level of endoscopic technique and interpretation, the fellows may be allowed to perform some elective procedures such as flexible sigmoidoscopy independently. All endoscopic procedures requiring conscious sedation with intravenous medications will be supervised at all institutions through which the fellows rotate. Additionally, competence with endoscopic biopsy, cytology and photographic documentation is also essential. C. Pregnancy in Gastrointestinal disorders The structure of our educational system is such that fellows have less than average exposure to pregnant patients, therefore reading of this document will be required. Each fellow will sign an attestation form documenting this once during their fellowship. The monograph is available in our curriculum library both in print form (which will be stored in the fellow's library at the CWB) and virtually. As a part of their duties regarding conference scheduling, the third year fellow will insure that at least one Tuesday lecture each quarter will be devoted to topics in this document. VIII. SUPERVISION: The ultimate responsibility for the care of the patient and instruction and supervision of the fellow lies with the attending staff physician. As such it is the fellow s responsibility to always obtain staff review of all their patient care activity as outlined below. The master rotation schedule, which is distributed in July and with each change lists fellow and staff assignments by clinic in all ambulatory settings. This schedule also lists inpatient fellow assignments. The inpatient attending schedule, distributed in July and with each change settings, lists staff inpatient attending for the entire year. If the fellow feels the number of patients or complexity of the patient load exceeds his or her ability to manage / triage they are instructed to seek the assistance of the appropriate staff. Circumstance or Events Requiring Attending Physician Approval Accepting for transfer patients from another institution. 25
26 Accepting a patient transferred from another service. Scheduling an endoscopic procedure. Initial antibiotic treatment of a wound infection. Undertaking any invasive diagnostic study. Circumstance or Events Requiring Attending Physician Notification Resident/fellow believes decisions can best be accomplished after communication with an attending. Concern of anyone, including nurses, that a situation is more complicated than a resident or fellow can manage effectively. Patient, a family member, nurse, allied professional, or a physician suggests that an attending be notified. Decision to admit patient to the hospital. Transfer to locus for a higher level of care or to ICU. Significant arrhythmia, cardiac arrest, unplanned intubation or need for ventilatory support, critical results of lab, radiology, or cardiac diagnostic tests, medication or treatment errors requiring intervention related to GI prognosis and procedure. Any issue prompting a significant change in a previously agreed upon treatment plan. Patient leaving hospital against medical advice. Changes in code status. Patient death. IX. FITNESS FOR DUTY/Fellow Back-Up Plan Policy The program director and institution must ensure a culture of professionalism that supports patient safety and personal responsibility. Residents and faculty members must demonstrate (Common Program Requirements VI A 5) V1 A 5 a.) Assurance of the safety and welfare of patients entrusted to their care, V1A 5 b.) provision of patient and family centered care, V1A 5 c.) assurance of their fitness for duty, V1A 5 d.) management of their time before, during and after clinical assignments, V1A 5 e.) recognition of impairment, including illness and fatigue, in themselves and in their peers. 26
27 27 Residents and Fellows must be educated about their self reflection on Fitness for Duty. It is clear that current alcohol or illicit substance use is incompatible with fitness to provide medical care to others. Excess fatigue, medical or psychiatric illness may also preclude participation in the workplace. This suicide prevention training video ( ) created by Mayo Clinic and the American Foundation for Suicide Prevention provides information on prevention, treatment, and emergency support services for mental health and medical issues. Fellows will be required to attest to viewing this training exercise at the start of each academic year and prior to the October meeting with the program director for First Years. This tool will remain available to Fellows at all times, and it is encourage that it be reviewed frequently during the July through September timeframe. Examples of additional situations in which a resident or fellow may not be fit for duty include but are not limited to the use of medications that impair dexterity significantly, grief that precludes concentration or acute illness that would make the physician a risk to others (ex. infectious illness) This policy is designed to: a. Provide guidance to both residents/fellows and supervisors when a fellow is unfit for duty b. Provide coverage for clinical duties if another fellow is ill or has a family emergency. c. Ensure the availability of coverage for fellow who calls in ill. d. Delineate the fellow s responsibility for coverage. FITNESS FOR DUTY: A resident or fellow who does not feel fit for duty should consult with their current program director or Employee health. Additionally, a supervisor who has concerns regarding a resident or fellow s fitness for duty should also consult with the Associate Dean for Graduate medical Education. BACK-UP SUPPORT: Appropriate use of sick call includes unexpected illness, death in the family or other personal emergency. Sick call is not to be used for scheduled absences, e.g., doctor s visits, family responsibilities, interviews, etc. for such scheduled absences, the resident/fellow will complete
Overview: Principal Teaching/Learning Activities:
 B. Endoscopy Overview: During the first year, the fellows will blend Consult Service with Endoscopy. In addition, there will be three months set aside for dedicated protected time on Endoscopy rotation
B. Endoscopy Overview: During the first year, the fellows will blend Consult Service with Endoscopy. In addition, there will be three months set aside for dedicated protected time on Endoscopy rotation
Division of Gastroenterology GI FELLOWSHIP PROGRAM
 Division of Gastroenterology GI FELLOWSHIP PROGRAM Training Program Manual Revised January 2009 University of California, San Diego http://gastro.ucsd.edu Fellowship Year Commencing July 2009 Table of
Division of Gastroenterology GI FELLOWSHIP PROGRAM Training Program Manual Revised January 2009 University of California, San Diego http://gastro.ucsd.edu Fellowship Year Commencing July 2009 Table of
Division of Gastroenterology, Hepatology and Nutrition
 Jewish Hospital Goals: 1. Consultative and management prevalence in hepatology, pre- and post-liver transplantation. 2. Offer diagnostic and therapeutic procedure experience. Learning Objectives: Patient
Jewish Hospital Goals: 1. Consultative and management prevalence in hepatology, pre- and post-liver transplantation. 2. Offer diagnostic and therapeutic procedure experience. Learning Objectives: Patient
Internal Medicine Curriculum Gastroenterology/Hepatology Rotation
 Internal Medicine Curriculum Gastroenterology/Hepatology Rotation Contact Person: Educational Purpose Gastrointestinal and hepatic disorders frequently cause patients to seek medical attention. Abdominal
Internal Medicine Curriculum Gastroenterology/Hepatology Rotation Contact Person: Educational Purpose Gastrointestinal and hepatic disorders frequently cause patients to seek medical attention. Abdominal
Internal Medicine Residency Program Rotation Curriculum
 University of California, Irvine Department of Medicine Internal Medicine Residency Program Rotation Curriculum I. Rotation Sites and Supervision Rotation Name: GASTROENTEROLOGY CONSULT Site Faculty Supervisor
University of California, Irvine Department of Medicine Internal Medicine Residency Program Rotation Curriculum I. Rotation Sites and Supervision Rotation Name: GASTROENTEROLOGY CONSULT Site Faculty Supervisor
UNMH Gastroenterology Clinical Privileges
 o Initial privileges (initial appointment) o Renewal of privileges (reappointment) o Expansion of privileges (modification) All new applicants must meet the following requirements as approved by the UNMH
o Initial privileges (initial appointment) o Renewal of privileges (reappointment) o Expansion of privileges (modification) All new applicants must meet the following requirements as approved by the UNMH
Fellowship Training Program in Digestive Diseases and Hepatology Stony Brook University Medical Center Northport Veterans Affairs Medical Center
 Fellowship Training Program in Digestive Diseases and Hepatology Stony Brook University Medical Center Northport Veterans Affairs Medical Center Inpatient GI Curriculum Goals and Objectives Revised December
Fellowship Training Program in Digestive Diseases and Hepatology Stony Brook University Medical Center Northport Veterans Affairs Medical Center Inpatient GI Curriculum Goals and Objectives Revised December
Inpatient GI Consult Service LBJ General Hospital Curriculum for Year I, II & III Fellows
 Inpatient GI Consult Service LBJ General Hospital Curriculum for Year I, II & III Fellows Educational Purpose: The LBJ rotation comprises several aspects of clinical gastroenterology: consultation on inpatients
Inpatient GI Consult Service LBJ General Hospital Curriculum for Year I, II & III Fellows Educational Purpose: The LBJ rotation comprises several aspects of clinical gastroenterology: consultation on inpatients
DUKE INTERNAL MEDICINE RESIDENCY PROGRAM. GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
 ROTATION DESCRIPTION Biliary, General GI and Hepatology") Department of Medicine Internal Medicine Residency Program DUKE INTERNAL MEDICINE RESIDENCY PROGRAM GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
Department of Medicine Internal Medicine Residency Program DUKE INTERNAL MEDICINE RESIDENCY PROGRAM GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
Entrustable Professional Activity
 Entrustable Professional Activity 1. EPA Title: Perform medical procedures related to gastrointestinal and liver disease for screening, diagnosis, and intervention 2. Description of Activity Endoscopy
Entrustable Professional Activity 1. EPA Title: Perform medical procedures related to gastrointestinal and liver disease for screening, diagnosis, and intervention 2. Description of Activity Endoscopy
GASTROENTEROLOGY. Department of Medicine
 GASTROENTEROLOGY Department of Medicine Overview The Division of Gastroenterology at Queen s University offers a nationally recognized two-year residency program that prepares graduates for stimulating
GASTROENTEROLOGY Department of Medicine Overview The Division of Gastroenterology at Queen s University offers a nationally recognized two-year residency program that prepares graduates for stimulating
Department of Surgery Surgical Endoscopy Goals and Objectives
 Department of Surgery Surgical Endoscopy Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate understanding of anatomy and physiology of the gastrointestinal tract, with
Department of Surgery Surgical Endoscopy Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate understanding of anatomy and physiology of the gastrointestinal tract, with
American College of Rheumatology Fellowship Curriculum
 American College of Rheumatology Fellowship Curriculum Mission: The mission of all rheumatology fellowship training programs is to produce physicians that 1) are clinically competent in the field of rheumatology,
American College of Rheumatology Fellowship Curriculum Mission: The mission of all rheumatology fellowship training programs is to produce physicians that 1) are clinically competent in the field of rheumatology,
Fellowship Training Program in Digestive Diseases. Yale University School of Medicine. Curriculum. Goals and Objectives. Policies and Procedures
 Fellowship Training Program in Digestive Diseases Yale University School of Medicine Curriculum Goals and Objectives Policies and Procedures Revised March 2017 (A. Imaeda and PEC) Avlin Imaeda, M.D., Ph.D
Fellowship Training Program in Digestive Diseases Yale University School of Medicine Curriculum Goals and Objectives Policies and Procedures Revised March 2017 (A. Imaeda and PEC) Avlin Imaeda, M.D., Ph.D
Gastroenterology Fellowship Program
 Roles, Responsibilities and Patient Care Activities of Residents and Fellows Gastroenterology Fellowship Program Definitions University of Washington Medical Center Harborview Medical Center Seattle Cancer
Roles, Responsibilities and Patient Care Activities of Residents and Fellows Gastroenterology Fellowship Program Definitions University of Washington Medical Center Harborview Medical Center Seattle Cancer
Gastroenterology Elective Residency Rotation Presbyterian/St. Luke s Hospital
 Preceptor: Dr. Kevin Seija 2005 Franklin St., Suite 210 Denver, CO 80218 303-861-4500 Gastroenterology Elective Residency Rotation Presbyterian/St. Luke s Hospital Specific Goals: 1. To gain knowledge
Preceptor: Dr. Kevin Seija 2005 Franklin St., Suite 210 Denver, CO 80218 303-861-4500 Gastroenterology Elective Residency Rotation Presbyterian/St. Luke s Hospital Specific Goals: 1. To gain knowledge
PEDIATRIC GASTROENTEROLGY PROGRAM MANUAL. Division of Pediatric Gastroenterology Louisiana State University
 PEDIATRIC GASTROENTEROLGY PROGRAM MANUAL Division of Pediatric Gastroenterology Louisiana State University STAFF Paul Hyman, MD Professor of Pediatrics Division Head of Pediatric Gastroenterology Allan
PEDIATRIC GASTROENTEROLGY PROGRAM MANUAL Division of Pediatric Gastroenterology Louisiana State University STAFF Paul Hyman, MD Professor of Pediatrics Division Head of Pediatric Gastroenterology Allan
University of Michigan Health System Internal Medicine Residency. Hepatology Curriculum: Consultation Service
 University of Michigan Health System Internal Medicine Residency Hepatology Curriculum: Consultation Service Version date: June 1, 2012 Fellow curriculum author: Reena Salgia, M.D. Faculty curriculum editor:
University of Michigan Health System Internal Medicine Residency Hepatology Curriculum: Consultation Service Version date: June 1, 2012 Fellow curriculum author: Reena Salgia, M.D. Faculty curriculum editor:
OUTPATIENT LIVER INTRODUCTION:
 OUTPATIENT LIVER INTRODUCTION: The purpose of the Liver rotation is to expose residents in internal medicine to acute and chronic liver diseases. Emphasis is on diagnosis of liver diseases by taking a
OUTPATIENT LIVER INTRODUCTION: The purpose of the Liver rotation is to expose residents in internal medicine to acute and chronic liver diseases. Emphasis is on diagnosis of liver diseases by taking a
Colorectal PGY3 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Colon and Rectal Surgery Service Goals and Objectives for Residents: R-3 Rotation Director: Andrew Shelton, MD Description The Colon and Rectal Surgery
Stanford University General Surgery Residency Program Colon and Rectal Surgery Service Goals and Objectives for Residents: R-3 Rotation Director: Andrew Shelton, MD Description The Colon and Rectal Surgery
University of Michigan Health System Internal Medicine Residency. Outpatient Liver Curriculum
 Version date: April 14, 2009 University of Michigan Health System Internal Medicine Residency Outpatient Liver Curriculum Subspecialty Education Coordinator: Anna Lok, M.D. Resident curriculum author:
Version date: April 14, 2009 University of Michigan Health System Internal Medicine Residency Outpatient Liver Curriculum Subspecialty Education Coordinator: Anna Lok, M.D. Resident curriculum author:
UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES
 January 2007 UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES This paragraph only applies if you are rotating at the University of Colorado
January 2007 UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES This paragraph only applies if you are rotating at the University of Colorado
Hematology and Oncology Curriculum
 Hematology and Oncology Curriculum Program overview The University of Texas Southwestern Medical Center provides a three year combined Hematology/Oncology fellowship training program in which is administered
Hematology and Oncology Curriculum Program overview The University of Texas Southwestern Medical Center provides a three year combined Hematology/Oncology fellowship training program in which is administered
Neurocritical Care Fellowship Program Requirements
 Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Administration ~ Education and Training (919)
") The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
Privileges for San Francisco General Hospital
 Applicant: Please initial the privileges you are requesting in the Requested column. Service Chief: Please initial the privileges you are approving in the Approved column. MedGI GASTROENTEROLOGY 2008 (0808
Applicant: Please initial the privileges you are requesting in the Requested column. Service Chief: Please initial the privileges you are approving in the Approved column. MedGI GASTROENTEROLOGY 2008 (0808
Administration ~ Education and Training (919)
") The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
Stanford Multiorgan Transplant Surgery: R-1 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Abdominal Transplant Surgery Goals and Objectives for Residents: R-1 Rotation Director: Carlos Esquivel, M.D., Ph.D. Description The Abdominal Transplant
Stanford University General Surgery Residency Program Abdominal Transplant Surgery Goals and Objectives for Residents: R-1 Rotation Director: Carlos Esquivel, M.D., Ph.D. Description The Abdominal Transplant
SURGICAL ONCOLOGY MCVH
 SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
Surgical Residency Curriculum
 Community Memorial Hospital Surgical Residency Curriculum Program Director: G. W. Iwasiuk MD FACS 2016 Educational Goals & Objectives Surgeons provide continuing care for patients with a myriad of surgical
Community Memorial Hospital Surgical Residency Curriculum Program Director: G. W. Iwasiuk MD FACS 2016 Educational Goals & Objectives Surgeons provide continuing care for patients with a myriad of surgical
CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM
 CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM Faculty representative: Venu Chennamaneni, MD Original document by: Davoren Chick, MD, Kelly Morgan, MD Resident Representative: None
CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM Faculty representative: Venu Chennamaneni, MD Original document by: Davoren Chick, MD, Kelly Morgan, MD Resident Representative: None
COMBINED INTERNAL MEDICINE & PEDIATRICS Department of Medicine, Department of Pediatrics SCOPE OF PRACTICE PGY-1 PGY-4
 Definition and Scope of Specialty The Internal Medicine/Pediatrics residency program is a voluntary component in the continuum of the educational process of physician training; such training may take place
Definition and Scope of Specialty The Internal Medicine/Pediatrics residency program is a voluntary component in the continuum of the educational process of physician training; such training may take place
SCOPE OF PRACTICE PGY-4 PGY-6
 The Fellowship in Pediatric Gastroenterology, Hepatology and Nutrition is a three-year specialized training program designed to provide and refine knowledge and skills regarding the care of children with
The Fellowship in Pediatric Gastroenterology, Hepatology and Nutrition is a three-year specialized training program designed to provide and refine knowledge and skills regarding the care of children with
1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants.
 Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants.") Clinical curriculum: Transplant 1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants. 2) Objectives Detailed objectives
Clinical curriculum: Transplant 1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants. 2) Objectives Detailed objectives
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
Resident Core Curriculum Vascular and Interventional Radiology
 Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
Pediatric Surgery Curriculum Clinical Base Year
 Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Members of the Section will decide on the desirability of an ER On-Call Schedule and will determine criteria for inclusion in such a roster.
 SHADY GROVE ADVENTIST HOSPITAL DEPARTMENT OF MEDICINE GASTROENTEROLOGY SECTION RULES AND REGULATIONS I. Purpose A Section of Gastroenterology within the Department of Medicine will be established pursuant
SHADY GROVE ADVENTIST HOSPITAL DEPARTMENT OF MEDICINE GASTROENTEROLOGY SECTION RULES AND REGULATIONS I. Purpose A Section of Gastroenterology within the Department of Medicine will be established pursuant
Curriculum for Year II & III Fellows
 Gastroenterology PancreaticoBiliary Consultation Service (PBS) Memorial Hermann Hospital Texas Medical Center & HCHD: Lyndon B. Johnson General Hospital Curriculum for PGY 4, 5 and 6 Curriculum for Year
Gastroenterology PancreaticoBiliary Consultation Service (PBS) Memorial Hermann Hospital Texas Medical Center & HCHD: Lyndon B. Johnson General Hospital Curriculum for PGY 4, 5 and 6 Curriculum for Year
GASTROENTEROLOGY CLERKSHIP
 College of Osteopathic Medicine GASTROENTEROLOGY CLERKSHIP Alan Hilgerson, D.O., FACP, FACOI Office for Clinical Affairs Assistant Professor of Medicine 515-271-1629 515-271-1490 FAX 515-271-1727 Elective
College of Osteopathic Medicine GASTROENTEROLOGY CLERKSHIP Alan Hilgerson, D.O., FACP, FACOI Office for Clinical Affairs Assistant Professor of Medicine 515-271-1629 515-271-1490 FAX 515-271-1727 Elective
MINIMALLY INVASIVE AND DIGESTIVE DISEASES SURGERY SECTION
 MINIMALLY INVASIVE AND DIGESTIVE DISEASES SURGERY SECTION Faculty Dr. Michael Edwards 1-4686 pager 8015 Dr. Bruce MacFadyen 1-4687 pager 6528 Dr. Jeremy Warren 1-4687 pager 1300 Dietitian Dr. Emily Van
MINIMALLY INVASIVE AND DIGESTIVE DISEASES SURGERY SECTION Faculty Dr. Michael Edwards 1-4686 pager 8015 Dr. Bruce MacFadyen 1-4687 pager 6528 Dr. Jeremy Warren 1-4687 pager 1300 Dietitian Dr. Emily Van
LOYOLA UNIVERSITY MEDICAL CENTER RESIDENCY PROGRAM IN GENERAL SURGERY CLINICAL ROTATION DESCRIPTION
 LOYOLA UNIVERSITY MEDICAL CENTER RESIDENCY PROGRAM IN GENERAL SURGERY CLINICAL ROTATION DESCRIPTION Loyola University Medical Center Department of Surgery Colorectal Surgery RESIDENT COMPLEMENT: ROTATION
LOYOLA UNIVERSITY MEDICAL CENTER RESIDENCY PROGRAM IN GENERAL SURGERY CLINICAL ROTATION DESCRIPTION Loyola University Medical Center Department of Surgery Colorectal Surgery RESIDENT COMPLEMENT: ROTATION
SERVICE: GI/Endoscopy, PGY 3 or 4 Sinai
 SERVICE: GI/Endoscopy, PGY 3 or 4 Sinai General description: The Sinai surgical residents will rotate in the Division of Gastroenterology at Sinai Hospital during their 3 rd or 4 th clinical year. The
SERVICE: GI/Endoscopy, PGY 3 or 4 Sinai General description: The Sinai surgical residents will rotate in the Division of Gastroenterology at Sinai Hospital during their 3 rd or 4 th clinical year. The
Course Descriptions. CLSC 5227: Clinical Laboratory Methods [1-3]
![Course Descriptions. CLSC 5227: Clinical Laboratory Methods [1-3]](/thumbs/77/75853296.jpg "Course Descriptions. CLSC 5227: Clinical Laboratory Methods [1-3]") Didactic Year Courses (YEAR 1) Course Descriptions CLSC 5227: Clinical Laboratory Methods [1-3] Lecture and laboratory course that introduces the student to the medical laboratory. Emphasizes appropriate
Didactic Year Courses (YEAR 1) Course Descriptions CLSC 5227: Clinical Laboratory Methods [1-3] Lecture and laboratory course that introduces the student to the medical laboratory. Emphasizes appropriate
Administration ~ Education and Training (919)
") The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
Course Title FUNCTIONAL ASSESSMENT OF PATIENTS WITH CARDIOVASCULAR DISEASES
 Course Title FUNCTIONAL ASSESSMENT OF PATIENTS WITH CARDIOVASCULAR DISEASES Director Judith Regensteiner, Ph.D., Professor of Medicine Director, Clinical Treadmill Laboratory, UCHSC Background & Objectives
Course Title FUNCTIONAL ASSESSMENT OF PATIENTS WITH CARDIOVASCULAR DISEASES Director Judith Regensteiner, Ph.D., Professor of Medicine Director, Clinical Treadmill Laboratory, UCHSC Background & Objectives
Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency
 DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
Family Medicine Residency Surgery Rotation
 Family Medicine Residency Surgery Rotation Rotation Goal The overall goal for the educational experience provided in the areas of general surgery, trauma surgery, office orthopedic surgery and sports medicine,
Family Medicine Residency Surgery Rotation Rotation Goal The overall goal for the educational experience provided in the areas of general surgery, trauma surgery, office orthopedic surgery and sports medicine,
Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017
 Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017 PHRD 510 - Pharmacy Seminar I Credit: 0.0 hours PHRD 511 Biomedical Foundations Credit: 4.0 hours This course is designed
Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017 PHRD 510 - Pharmacy Seminar I Credit: 0.0 hours PHRD 511 Biomedical Foundations Credit: 4.0 hours This course is designed
I. Overall Goals and Objectives . Competencies
 Page 1 Goals and Objectives Pediatric Endocrinology Fellowship Andrew Lane, MD Program Director Pediatric Endocrinology Department of Pediatrics Stony Brook University Children s Hospital Stony Brook,
Page 1 Goals and Objectives Pediatric Endocrinology Fellowship Andrew Lane, MD Program Director Pediatric Endocrinology Department of Pediatrics Stony Brook University Children s Hospital Stony Brook,
Basic Standards for Residency Training in Pediatrics. American Osteopathic Association and the American College of Osteopathic Pediatricians
 Basic Standards for Residency Training in Pediatrics American Osteopathic Association and the American College of Osteopathic Pediatricians Revised, BOT 7/1991 Revised, BOT 2/1997 Revised, BOT 3/1999 Revised,
Basic Standards for Residency Training in Pediatrics American Osteopathic Association and the American College of Osteopathic Pediatricians Revised, BOT 7/1991 Revised, BOT 2/1997 Revised, BOT 3/1999 Revised,
RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised )
") RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised 12-31-2011) Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC. A link to the
RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised 12-31-2011) Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC. A link to the
Family Medicine Residency Behavior Medicine Rotation Elly Riley, DO
 Family Medicine Residency Behavior Medicine Rotation Elly Riley, DO Rotation Goal The teaching of Human Behavior and Psychiatry at the UT Family Medicine Center (UTFPC) is divided into several discreet
Family Medicine Residency Behavior Medicine Rotation Elly Riley, DO Rotation Goal The teaching of Human Behavior and Psychiatry at the UT Family Medicine Center (UTFPC) is divided into several discreet
POLICY - RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (2008) - Approved UTHSCSA GME 2009
 - Approved UTHSCSA GME 2009") POLICY - RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (2008) - Approved UTHSCSA GME 2009 Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC.
POLICY - RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (2008) - Approved UTHSCSA GME 2009 Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC.
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
Basic Standards for Community Based Residency Training in Pediatrics
 Basic Standards for Community Based Residency Training in Pediatrics American Osteopathic Association and the American College of Osteopathic Pediatricians Table of Contents SECTION - Introduction... 3
Basic Standards for Community Based Residency Training in Pediatrics American Osteopathic Association and the American College of Osteopathic Pediatricians Table of Contents SECTION - Introduction... 3
September 24, Dear Administrator Verma:
 Seema Verma, MD Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: P.O. Box 8013 Baltimore, MD 21244-1850 RE: [] Medicare Program: Proposed Changes to Hospital
Seema Verma, MD Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: P.O. Box 8013 Baltimore, MD 21244-1850 RE: [] Medicare Program: Proposed Changes to Hospital
Neurocritical Care Program Requirements
 Neurocritical Care Program Requirements Approved October 17, 2014 Page 1 Table of Contents I. Introduction 3 II. Institutional Support 3 A. Sponsoring Institution 4 B. Primary Institution 4 C. Participating
Neurocritical Care Program Requirements Approved October 17, 2014 Page 1 Table of Contents I. Introduction 3 II. Institutional Support 3 A. Sponsoring Institution 4 B. Primary Institution 4 C. Participating
By the final rotation in Nuclear Medicine as a first year Radiology Resident, the resident will demonstrate:
 Goals and Objectives Nuclear Medicine Rotation First Year Residents Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health
Goals and Objectives Nuclear Medicine Rotation First Year Residents Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health
HEMATOLOGY / ONCOLOGY
 HEMATOLOGY / ONCOLOGY INTRODUCTION: Residents are required to take a minimum of a one month rotation through the Hematology/Oncology service at Huntington Hospital. Residents will also spend a month rotating
HEMATOLOGY / ONCOLOGY INTRODUCTION: Residents are required to take a minimum of a one month rotation through the Hematology/Oncology service at Huntington Hospital. Residents will also spend a month rotating
BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE
 BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE American Osteopathic Association and American College of Osteopathic Pediatricians TABLE OF CONTENTS 1 Article I. Introduction...
BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE American Osteopathic Association and American College of Osteopathic Pediatricians TABLE OF CONTENTS 1 Article I. Introduction...
Competencies, Milestones and EAPs. Program Director Series October 20, 2015
 Competencies, Milestones and EAPs Program Director Series October 20, 2015 Objectives Review the history of new approach to evaluation by the ACGME Show the differences between standard Likert scale evaluations
Competencies, Milestones and EAPs Program Director Series October 20, 2015 Objectives Review the history of new approach to evaluation by the ACGME Show the differences between standard Likert scale evaluations
Basic Standards for Residency Training in Anesthesiology
 Basic Standards for Residency Training in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists Adopted BOT 7/2011, Effective 7/2012 Revised, BOT 6/2012,
Basic Standards for Residency Training in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists Adopted BOT 7/2011, Effective 7/2012 Revised, BOT 6/2012,
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
DEPARTMENT OF SURGERY SECTION OF PEDIATRIC SURGERY PEDIATRIC SURGERY ROTATION (DSP)
") DEPARTMENT OF SURGERY SECTION OF PEDIATRIC SURGERY PEDIATRIC SURGERY ROTATION (DSP) C.S. Mott Children s Hospital Von Voigtlander Women s Hospital House Officer I House Officer II House Officer III Curriculum/Rotation
DEPARTMENT OF SURGERY SECTION OF PEDIATRIC SURGERY PEDIATRIC SURGERY ROTATION (DSP) C.S. Mott Children s Hospital Von Voigtlander Women s Hospital House Officer I House Officer II House Officer III Curriculum/Rotation
San Antonio Uniformed Services Health Education Consortium San Antonio, Texas
 Musculoskeletal Radiology Fellowship San Antonio Uniformed Services Health Education Consortium San Antonio, Texas I. Applicability Supervision Policies The SAUSHEC Command Council [Commanders of Brooke
Musculoskeletal Radiology Fellowship San Antonio Uniformed Services Health Education Consortium San Antonio, Texas I. Applicability Supervision Policies The SAUSHEC Command Council [Commanders of Brooke
COPIC Objectives and Expectations
 COPIC Objectives and Expectations Goals: 1. Familiarize residents with how the state s medical malpractice insurer functions 2. Gain knowledge of process of malpractice claims work 3. Understand the most
COPIC Objectives and Expectations Goals: 1. Familiarize residents with how the state s medical malpractice insurer functions 2. Gain knowledge of process of malpractice claims work 3. Understand the most
INTRODUCTION AND OVERVIEW
 INTRODUCTION AND OVERVIEW GOALS: Provide the educational and academic environment, formal and informal instruction, and clinical material necessary to train physicians for the practice of internal medicine
INTRODUCTION AND OVERVIEW GOALS: Provide the educational and academic environment, formal and informal instruction, and clinical material necessary to train physicians for the practice of internal medicine
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
PART IIIB DIPLOMA AND CERTIFICATE PROGRAMS CURRICULA
 PART IIIB DIPLOMA AND CERTIFICATE PROGRAMS CURRICULA NURSE EDUCATION DEPARTMENT Practical Nurse Education Program (Diploma Program) Objective This professional education program is designed to provide
PART IIIB DIPLOMA AND CERTIFICATE PROGRAMS CURRICULA NURSE EDUCATION DEPARTMENT Practical Nurse Education Program (Diploma Program) Objective This professional education program is designed to provide
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
COURSE TITLES, PRE-REQUISITES, COURSE DESCRIPTIONS AND LEARNING OBJECTIVES
 COURSE TITLES, PRE-REQUISITES, COURSE DESCRIPTIONS AND LEARNING OBJECTIVES NA640 Chemistry and Physics for Nurse Anesthesia - 3 Credits This course examines the principles of inorganic chemistry, organic
COURSE TITLES, PRE-REQUISITES, COURSE DESCRIPTIONS AND LEARNING OBJECTIVES NA640 Chemistry and Physics for Nurse Anesthesia - 3 Credits This course examines the principles of inorganic chemistry, organic
Surgical Oncology II: R5 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Surgical Oncology II Goals and Objectives for Residents: R-5 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation at Stanford
Stanford University General Surgery Residency Program Surgical Oncology II Goals and Objectives for Residents: R-5 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation at Stanford
Pathophysiology Curriculum
 Pathophysiology Curriculum Educational Purpose and Goals It is crucial for practicing Infectious Disease physicians to stay abreast of new developments in the field. Understanding how to critically read
Pathophysiology Curriculum Educational Purpose and Goals It is crucial for practicing Infectious Disease physicians to stay abreast of new developments in the field. Understanding how to critically read
Gastrointestinal endoscopy
 Procedure 23 Clinical PRIVILEGE WHITE PAPER Background Gastrointestinal endoscopy Gastrointestinal (GI) endoscopy is a minimally invasive procedure in which the physician uses an endoscope that has a light
Procedure 23 Clinical PRIVILEGE WHITE PAPER Background Gastrointestinal endoscopy Gastrointestinal (GI) endoscopy is a minimally invasive procedure in which the physician uses an endoscope that has a light
SPECIALTY SPECIFIC OBJECTIVES
 Family Medicine Residency Internal Medicine In-house II Rotation Rotation Goal Admission, evaluation, treatment and appropriate specialty consultation of adult hospitalized patients from either the ER,
Family Medicine Residency Internal Medicine In-house II Rotation Rotation Goal Admission, evaluation, treatment and appropriate specialty consultation of adult hospitalized patients from either the ER,
INTRODUCTION. LEARNING OBJECTIVES (CanMEDS)
") OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
Pediatric ICU Rotation
 Pediatric Anesthesia Fellowship Program Department of Anesthesiology 800 Washington Street, Box 298 Boston, MA 02111 Tel: 617 636 6044 Fax: 617 636 8384 Pediatric ICU Rotation ROTATION DIRECTOR: RASHED
Pediatric Anesthesia Fellowship Program Department of Anesthesiology 800 Washington Street, Box 298 Boston, MA 02111 Tel: 617 636 6044 Fax: 617 636 8384 Pediatric ICU Rotation ROTATION DIRECTOR: RASHED
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Goals and Objectives GI/GU Radiology (First year)
") Goals and Objectives GI/GU Radiology (First year) I. Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and
Goals and Objectives GI/GU Radiology (First year) I. Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and
Clinical Cardiology Adult Congenital Heart Disease Clinical Service (1 month)
") Clinical Cardiology Adult Congenital Heart Disease Clinical Service (1 month) During this rotation, the Cardiovascular Diseases (CD) fellow functions as an independent Cardiologist. The subspecialty trainee
Clinical Cardiology Adult Congenital Heart Disease Clinical Service (1 month) During this rotation, the Cardiovascular Diseases (CD) fellow functions as an independent Cardiologist. The subspecialty trainee
WRNMMC Nephrology Rotation 2013
 WRNMMC Nephrology Rotation 2013 Educational Purpose The WRNMMC nephrology rotation provides in-depth exposure and education for interested housestaff and medical students in areas of acid-base and electrolyte
WRNMMC Nephrology Rotation 2013 Educational Purpose The WRNMMC nephrology rotation provides in-depth exposure and education for interested housestaff and medical students in areas of acid-base and electrolyte
Teaching Methods. Responsibilities
 Avera McKennan Critical Care Medicine Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Written: May 2011 I) Rotation Goals A) To manage
Avera McKennan Critical Care Medicine Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Written: May 2011 I) Rotation Goals A) To manage
Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty:
 Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty: Goals: develop and refine the necessary knowledge base, medical interviewing skills, and
Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty: Goals: develop and refine the necessary knowledge base, medical interviewing skills, and
San Antonio Uniformed Services Health Education Consortium San Antonio, Texas. Nuclear Medicine Fellowship Supervision Policies
 San Antonio Uniformed Services Health Education Consortium San Antonio, Texas Nuclear Medicine Fellowship Nuclear Medicine Fellowship Supervision Policies I. Applicability The SAUSHEC Command Council [Commanders
San Antonio Uniformed Services Health Education Consortium San Antonio, Texas Nuclear Medicine Fellowship Nuclear Medicine Fellowship Supervision Policies I. Applicability The SAUSHEC Command Council [Commanders
SCOPE OF PRACTICE PGY-2 PGY-5
 The Residency Review Commission on Urology requires demonstrated progressive responsibility in cognitive and procedural patient management. A concrete list of procedures limiting the progression of gifted
The Residency Review Commission on Urology requires demonstrated progressive responsibility in cognitive and procedural patient management. A concrete list of procedures limiting the progression of gifted
Internal Medicine Residency Program Rotation Curriculum
 University of California, Irvine Department of Medicine Internal Medicine Residency Program Rotation Curriculum DIVISION: PULMONARY AND CRITICAL CARE MEDICINE I. Rotation Sites Rotation Name: Pulmonary
University of California, Irvine Department of Medicine Internal Medicine Residency Program Rotation Curriculum DIVISION: PULMONARY AND CRITICAL CARE MEDICINE I. Rotation Sites Rotation Name: Pulmonary
UNDERSTANDING THE CONTENT OUTLINE/CLASSIFICATION SYSTEM
 BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
PHYSICIAN ASSISTANT PROGRAM
 Physician Assistant Program PHYSICIAN ASSISTANT PROGRAM Master of Science in Physician Assistant Studies Cynthia Booth Lord, MHS, PA-C PA Program Director David Shafran, MD, MA Director of Admissions PAProgram@case.edu
Physician Assistant Program PHYSICIAN ASSISTANT PROGRAM Master of Science in Physician Assistant Studies Cynthia Booth Lord, MHS, PA-C PA Program Director David Shafran, MD, MA Director of Admissions PAProgram@case.edu
MISSION, VISION AND GUIDING PRINCIPLES
 MISSION, VISION AND GUIDING PRINCIPLES MISSION STATEMENT: The mission of the University of Wisconsin-Madison Physician Assistant Program is to educate primary health care professionals committed to the
MISSION, VISION AND GUIDING PRINCIPLES MISSION STATEMENT: The mission of the University of Wisconsin-Madison Physician Assistant Program is to educate primary health care professionals committed to the
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
Curricular area: Specific Rotations: Responsible faculty: Goals: Setting: Key to Competencies Teaching activities: Level of supervision:
 Curricular area: Endocrinology Specific Rotations: Endocrinology Consult Elective Responsible faculty: Michelle Cordoba Kissee, MD Reviewed and revised by Dr. Amer Malas, Program Director, on 12/1/2013
Curricular area: Endocrinology Specific Rotations: Endocrinology Consult Elective Responsible faculty: Michelle Cordoba Kissee, MD Reviewed and revised by Dr. Amer Malas, Program Director, on 12/1/2013
Nephrology Transplant Training Program
 Nephrology Transplant Training Program Goals At the present time, our program is ASTS certified for surgical aspects of renal transplantation, which has requirements similar to those required for AST certification.
Nephrology Transplant Training Program Goals At the present time, our program is ASTS certified for surgical aspects of renal transplantation, which has requirements similar to those required for AST certification.
University of Toronto Physician Assistant Professional Degree Program YEAR 1 & 2 COURSE DESCRIPTIONS
 University of Toronto Physician Assistant Professional Degree Program YEAR 1 & 2 COURSE DESCRIPTIONS PAP 111H1 - Introduction to the Physician Assistant Role This course will describe the PA profession
University of Toronto Physician Assistant Professional Degree Program YEAR 1 & 2 COURSE DESCRIPTIONS PAP 111H1 - Introduction to the Physician Assistant Role This course will describe the PA profession
Pediatric Intensive Care Unit Rotation PL-2 Residents
 PL-2 Residents Residents are required to have sufficient knowledge of their patients in order to present them to the team on rounds, and to construct a differential diagnosis and treatment plan. They are
PL-2 Residents Residents are required to have sufficient knowledge of their patients in order to present them to the team on rounds, and to construct a differential diagnosis and treatment plan. They are
Stanford Surgical Oncology II: R1 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Surgical Oncology II Surgery goals and objectives for residents: R-1 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation
Stanford University General Surgery Residency Program Surgical Oncology II Surgery goals and objectives for residents: R-1 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation
Department of Pharmacy Services PGY1 Residency Program. Residency Manual
 Department of Pharmacy Services PGY1 Residency Program Residency Manual 1 TABLE OF CONTENTS I. Introduction II. General Program Goals III. Residency Program Purpose Statement IV. Program s Goals V. Residency
Department of Pharmacy Services PGY1 Residency Program Residency Manual 1 TABLE OF CONTENTS I. Introduction II. General Program Goals III. Residency Program Purpose Statement IV. Program s Goals V. Residency
University of Michigan Health System Internal Medicine Residency. Infectious Diseases Curriculum: Ambulatory ID
 University of Michigan Health System Internal Medicine Residency Infectious Diseases Curriculum: Ambulatory ID Version date: 2/2011 Subspecialty Education Coordinator: Daniel Kaul, MD Faculty curriculum
University of Michigan Health System Internal Medicine Residency Infectious Diseases Curriculum: Ambulatory ID Version date: 2/2011 Subspecialty Education Coordinator: Daniel Kaul, MD Faculty curriculum