An Assessment of Personal Assistance Services in Indiana
|
|
|
- Jemima Carpenter
- 6 years ago
- Views:
Transcription
1 An Assessment of Personal Assistance Services in Indiana Submitted to: Indiana Office of Medicaid Policy and Planning Family and Social Services Administration 402 West Washington Street Room W382 Indianapolis, Indiana Prepared by: Center on Community Living and Careers Indiana Institute on Disability and Community Indiana s University Center for Excellence on Disabilities Indiana University 2853 East Tenth Street Bloomington, Indiana (812) Fax: (812) For information, contact: Becky Banks, M.A., L.S.W. or Teresa Grossi, Ph.D. July 1, 2005
2 TABLE OF CONTENTS ACKNOWLEDGEMENTS EXECUTIVE SUMMARY iii v I. INTRODUCTION 1 A. Purpose of the Personal Assistance Services Assessment 6 B. Methodology for the Personal Assistance Services Assessment 6 C. Limitations of this Assessment 9 II. MEDICAID INFRASTRUCTURE GRANT FUNDING AND PERSONAL ASSISTANCE SERVICES 9 A. Centers for Medicare and Medicaid Services Criteria for Personal Assistance Services within Medicaid Infrastructure Grant Funding 10 B. Indiana s Progress toward Removing Medicaid Barriers to Employment 13 C. Indiana s Accomplishments with Medicaid Infrastructure Grant Funding 16 II. PERSONAL ASSISTANCE SERVICES IN INDIANA 18 A. Overview of Indiana s Medicaid Waiver Programs Eligibility for Medicaid Waivers Cost Sharing Mechanisms for Medicaid Waiver Participants Services Provided through Indiana s Waivers Cost-containment within Indiana s Waivers 34 B. Medicaid Waiver Services Providing Personal Assistance 36 C. Other Indiana Programs Funding Personal Assistance Services 39 D. Adequacy of Personal Assistance Services to Support the Employment of People with Disabilities in the Workforce 41 i
3 1. Adequacy of Home and Community-Based (HCBS) Waiver Services Adequacy of Personal Assistance Services Providers 44 E. Policy Development and Performance Monitoring 49 III. SURVEY OF OTHER STATE S SRATEGIES TO MEET MEDICAID INFRASTRUCTURE GRANT FULL ELIGIBILITY CRITERIA 52 A. State Programs Providing Personal Assistance Services Options to Support Employment 53 B. Other Options for Increasing Community-Based Services 57 IV. RECOMMENDATIONS FOR INDIANA S SUPPORT OF PEOPLE WITH DISABILITIES IN THE WORKFORCE 60 A. Recommendations Relative to Home and Community Based Services and Personal Assistance Services 60 B. Recommendations Relative to Service Improvement and Service Initiatives 64 C. Recommendations Relative to Employment Barriers 65 V. CONCLUSION 72 REFERENCES 74 APPENDICES ii
4 ACKNOWLEDGEMENTS We appreciate the support and cooperation of the National Consortium for Health Systems Development (NCHSD) who developed a Personal Assistance Assessment Tool tailored for Indiana to use as a framework for building a state level Personal Assistance Services (PAS) infrastructure. NCHSD facilitates state-to-state information sharing to develop comprehensive health and service systems to support people with disabilities in the workforce. Through information sharing, Indiana has access to information and can collaborate with state and federal experts to address service systems change and improvement. We appreciate the flexible technical assistance of Melissa Wittman and Sara Salley of NCHSD, who provided guidance to the Office of Medicaid Policy and Planning s Medicaid Infrastructure Grant activities, and offered support on the Assessment of Personal Assistance Services in Indiana. We wish to acknowledge the excellent cooperation and leadership of Indiana s Medicaid Infrastructure Grant Director, Andrea Vermeulen and the data provided by the Family and Social Services Administration. Other organizations and individuals who provided valuable information include: Bitta DeWees of Stone Belt; Kay Boas, Developmental Services, Inc.; Melissa Durr of the Indiana Association for the Area Agencies on Aging; Gwen Chesterfield, Case Manager and private consultant; Christine Jones, Director of IRL Development, Inc.; Gwen Kilmer, Bureau of Aging and In-Home Services; Albert Tolbert, Director of Southern Independent Living Center of Central Indiana; Sheri Caveda, Fifth Freedom, Inc.; Nanette Whightsel, The ARC of Indiana Incorporated; Holly Fuller, Board of Directors, Indiana Chapter of Professional Case Managers; Jean MacDonald, Indiana Association for Home and Hospice Care; Juman Bruce, Family and Social Services Administration; and Pat Cassanova, Family and Social Services Administration. iii
5 The Office of Medicaid Policy and Planning is awarded Medicaid Infrastructure Funding from the Centers for Medicare and Medicaid Services, available under the provisions of the Ticket to Work and Work Incentives Improvement Act of Funding for this assessment was provided pursuant to a contract between the Office of Medicaid Policy and Planning, Medicaid Infrastructure Grant and the Indiana Institute on Disability and Community, Center on Community Living and Careers. The Center on Community Living and Careers is one of seven centers located at the Indiana Institute on Disability and Community, Indiana University, Bloomington. The work of the Indiana Institute encompasses the entire life span, from birth through older adulthood, and addresses topical areas that include: Young children and families School inclusion Transition from school to work Employment Community living Aging Autism Information and referral Planning and policy studies Technology and technological adaptations Individual and family perspectives The Indiana Institute on Disability and Community pursues its mission with support from Indiana University and funding from federal and state agencies, and foundations. The Center on Community Living and Careers promotes partnerships with people with disabilities, their families and communities to affect systems and organizational change through research, evaluation, training, and technical assistance. The Center focuses on improving transition and adult services through person-directed planning, career development, community living, affordable housing and home ownership, community membership, and organizational change. iv
6 AN ASSESSMENT OF PERSONAL ASSISTANCE SERVICES IN INDIANA EXECUTIVE SUMMARY The purpose of this project was to assess Indiana s Medicaid-funded Personal Assistance Services (PAS), and determine if these services are adequate to support individuals with disabilities who work. This assessment is one of the benchmarks set forth by Indiana s Medicaid Infrastructure Grant (MIG) funded by the Centers for Medicare and Medicaid Services (CMS). It is designed to assist state officials, advocates, provider agencies, individuals with disabilities and their family members to understand how PAS is provided, what limitations exist, and what approaches may be used to support competitive employment of people with disabilities. Centers for Medicare and Medicaid Requirements for Medicaid Infrastructure Grant Funding Beginning in 2000, (CMS) began soliciting proposals from states to develop the infrastructure to support competitive employment for people with disabilities through Medicaid Infrastructure Grant funding. This funding was created by the Ticket to Work and Work Incentives Improvement Act of 1999 (TWWIIA) and allows states to develop strategies to remove barriers to employment for people with disabilities. CMS is the federal agency that administers MIG funding, and has established two levels of funding eligibility for states. These levels are categorized as fully eligible and conditionally eligible, and are tiered in a way that enables states to qualify for funding while making incremental changes to their Medicaid Infrastructure and improving the delivery of Personal Assistance Services (PAS) to support employment for people with disabilities. Fully eligible states must offer PAS inside and outside the home (including the workplace) 40 hours per week sufficient to support an individual in full-time v
7 employment. Conditionally eligible states are those which offer personal assistance services inside and outside the home through their Medicaid programs in a sufficient manner to support an individual who is working 40 hours per month. For either level of MIG funding, CMS requires PAS services to be available statewide. In Indiana, PAS is available to some extent under the Home and Community- Based Services (HCBS) Waivers but not under Indiana s State Plan Option. CMS requires that if PAS is only available through the HCBS Waivers, these Waivers must allow recipients to be eligible for Medicaid Buy-In (known as M.E.D. Works in Indiana). In addition, the services must be available in the workplace and the Waivers must serve more than 50% of individuals estimated to need services. Because of this requirement, Indiana s Office of Medicaid Policy and Planning (OMPP) requested an assessment of Personal Assistance Services to understand how, where and to what extent PAS services are provided; and, if these services meet CMS criteria for full eligibility for MIG funding. Indiana applied for and received Medicaid Infrastructure Grant (MIG) funding beginning in 2003 as a requirement of House Enrolled Act 1950, the Medicaid Buy- In legislation, which was passed in the Indiana General Assembly in The Office of Medicaid Policy and Planning receives MIG funding as a conditionally eligible state. To become fully eligible for MIG funding through the year 2011, Indiana must meet certain criteria set forth by CMS. These criteria outline expectations for Medicaid PAS services: Services must be provided inside or outside the home including the workplace; The population served are those who are most likely to be competitively employed; The services are available statewide; and There are sufficient amounts of hours of PAS services available for people who need services to be employed full time. vi
8 If Indiana does not reach full eligibility status, MIG funding will end in If Indiana meets CMS criteria for PAS availability to support competitive employment of people with disabilities, it will be eligible for continued funding, and will become what CMS calls a Comprehensive Employment State. Funding will then be available to form linkages between Medicaid services and non-medicaid services to continue addressing employment barriers and build Indiana s infrastructure to support the employment of people with disabilities. Indiana s Accomplishments through Medicaid Infrastructure Grant Funding Since first receiving funds in 2003, the MIG program has pursued activities that enhance employment supports for people with disabilities. These activities include: Operating a Medicaid Buy-In program, known as M.E.D. Works; Convening an Employment Leadership Group through collaborative efforts between the Office of Medicaid Policy and Planning MIG grant and Vocational Rehabilitation Services; Pursuing employer involvement through a statewide Business Leadership Network; Conducting a needs assessment on education and outreach to people with disabilities on M.E.D. Works and other state and federal benefits; Providing user-friendly educational resources on M.E.D Works federal benefit programs and other resources for people with disabilities; Establishing a comprehensive work supports website for people with disabilities; Surveying community and state resources to map out those offered to people with disabilities in Indiana through local, state and federal venues; Establishing a Benefits Information Network to increase capacity of benefits counseling; vii
9 Creating orientation materials on work incentives and employment information for the Medicaid Work Incentives Council and other policy advisors; Increasing consumer involvement in systems change activities under the MIG funding; Improving data analysis on outcomes of people with disabilities and employment; and Spearheading the establishment of an Employment Network Consortium. These efforts have had a remarkable impact on employment supports for people with disabilities, and to continue progress Indiana would benefit by becoming fully eligible for Medicaid Infrastructure Grant Funds. Personal Assistance Services and Indiana s Home and Community-Based Waivers Indiana offers a comprehensive array of Medicaid services. It provides funding for long-term care in facilities as well as funding for Home and Community- Based (HCBS) Waiver services in the community. Because PAS is not available under Indiana s Medicaid State Plan Option, this assessment evaluated Personal Assistance Services provided in the community under the HCBS Waiver services and explored the following areas: Eligibility for PAS and Waiver services, Access to PAS under Waiver Services Adequacy of PAS to support employment, and Policy development and performance monitoring. Eligibility: Because Waiver services are intended to support individuals in the community rather than in institutions or facilities, individuals must meet the level of viii
10 care criteria of the Waivers for which they apply. Individuals may apply for Waivers at the local Bureau of Developmental Disabilities Office or the Area Agencies on Aging. It is important to know which location is the appropriate place to apply for particular Waivers. Individuals applying for Waivers must also meet financial criteria, including income and resource limits. The financial determination is handled by the local Division of Family Resources. Because there are different entry points and numerous steps to undergo to qualify for Waivers, this process may be somewhat daunting for individuals with disabilities and their families, advocates, providers and school personnel who are supporting them. Access: Once eligible for a Waiver, individuals have an Individual Support Plan developed through a Person-Centered Planning process to determine the quantity and the nature of supports an individual will receive. Accessing services based on the Person-Centered Plan must be negotiated within services offered and costcontainment policies under particular Waiver services. The services available to an individual will vary depending on the type of Waiver for which he or she qualifies and may include: Community Habilitation and Participation; Independence Assistance Services; Residential Habilitation and Support; Respite; and, Supported Employment Services. Personal Assistance Services are currently embedded within these service definitions, and each service definition has specific rates and cost caps. Because of this, it may be difficult for CMS to determine if PAS is clearly available inside and outside the home (including the workplace) for 40 hours per week for the individuals who need this support through the Waivers. Adequacy: The ARC of Indiana (2005) reports an unduplicated count of approximately 15,500 Hoosiers with disabilities waiting for Waiver services. Many individuals are ix
11 told to apply for more than one Waiver so that they may access funding when a slot under a particular Waiver becomes available. Individuals needing PAS funded through Medicaid must meet the level of care for Waivers; meet income and resource requirements, and wait until a Waiver slot is available to provide funding for them. Indiana clearly needs more Waiver slots to adequately serve individuals who require services. As Indiana transitions individuals with disabilities out of state developmental centers, nursing facilities and Intermediate Care Facilities for the Mentally Retarded, Indiana needs to address how funds are allocated to follow these individuals to support their needs in the community. There is a steady effort to add 450 Waiver slots for people transitioning from nursing facilities as a result of litigation (Krauss vs. Hamilton, 2004). This is only a small effort compared to the number of individuals waiting for Waiver services in the community. Recently, the Indiana Family and Social Services Administration reported its intent to add up to 1,000 additional Waiver slots by 2006 and revamp the current Waiver system. In so doing, Indiana should consider recommendations outlined in this report to ensure individuals with disabilities are served effectively. In addition to the inadequate number of Waiver slots, Indiana also reflects the deficit nationally in availability of direct support professionals. Further, there remains inadequate training and professional development opportunities for these personnel. Indiana has training requirements for provider agencies, case managers, and direct support professionals to ensure Waiver recipients are adequately served. Training initiatives such as the Indiana Statewide Education Training and Planning Group are available to ensure direct support professionals will have adequate skills to competently support individuals in the community. At the current time, most personal care attendants are accessed through a provider agency. Individuals have input regarding the choice of their provider agency and attendants. Individuals participating in the Consumer-Directed Control Pilot Program under the Aged and Disabled Waiver may hire and train their own x
12 attendants. A fiscal intermediary is available for these individuals to support the budgeting and payment of services for their care. The Consumer-Directed Control Pilot is one initiative that allows more flexibility for PAS services to support individuals needs. Policy Development and Performance Monitoring: Indiana has developed numerous mechanisms to ensure Waiver services are provided with quality. These mechanisms include, but are not limited to, reporting requirements such as provider surveys; individual visits; satisfaction surveys; progress reports; ombudsman functions; hearings and appeals; and, audits. While quality assurance mechanisms are important, having a variety of mechanisms that measure very similar indicators may not be cost-effective. Strategies to Meet the Centers for Medicare and Medicaid Criteria for Personal Assistance Services For Indiana to become eligible for full Medicaid Infrastructure Grant funding it must have PAS services that are clearly identifiable in the Medicaid State Plan, or through Home and Community-Based Waivers, or a combination of both. States that have initiatives to provide PAS related to employment are described below: Maine implemented a Consumer-Directed care program under the HCBS Waiver program; Utah added Employment-Related Personal Assistance to their State Plan for individuals working in integrated settings; Kansas is applying for an Independence Plus demonstration Waiver to support individuals who are on waiting lists for Waivers and are employed in competitive, integrated settings; and Minnesota provides Personal Care Assistance under the HCBS Waiver Programs and the State plan. Personal care is designed with flexibility to the needs of individuals based on their individualized assessment. xi
13 Although Indiana can learn from other states, it will gain more from evaluating its current HCBS system and exploring how to address issues in eligibility, access, adequacy, policy development and performance monitoring. For example, currently a number of initiatives are being undertaken to do just this. The MATRIX Task Force through the Division of Disability and Rehabilitative Services is exploring how to implement a program for personal and flexible budgets. The Community- Integrated Personal Assistance Services and Supports (C-PASS) Task force through the Division on Aging recommends implementing consumer-directed care under the current Waivers, beginning with the Aged and Disabled Waiver and then eventually adding consumer-directed care to other HCBS Waivers. These initiatives will be useful, and coupled with changes to eligibility, access, adequacy, policy development and performance monitoring of the Waiver services, Indiana s HCBS Waivers will become more effective in serving individuals with disabilities who need PAS services. Other Assessment Findings Indiana has achieved some progress on policy directions outlined in Indiana s Olmstead Comprehensive Plan in relation to Home and Community-Based Services. Some of the steps identified in the Plan are comparable to the issues explored in this assessment. These issues include: adding more Waiver slots to support individuals with disabilities in the community; addressing waiting lists for Medicaid Waivers; piloting consumer-directed personal assistance; increasing training options for providers; expanding an ombudsman program; and, developing quality improvement systems for services provided to individuals with developmental disabilities. One Olmstead action step incorporated changes to the Developmental Disabilities Waiver to broaden categories for reporting and rate structuring (consolidating PAS into Community Habilitation and Participation and Residential Habilitation Services). While this action step may have alleviated reporting and rate structuring for separate services provided under the Waiver, it reduced the ability to xii
14 clearly identify PAS as a separate service and quantify how much PAS is available to individuals. While conducting this assessment, other areas were explored that would address employment barriers. These areas included improvements for the M.E.D. Works program and allowing a Social Security Work incentive called Plan to Achieve Self-Sufficiency (PASS) which is currently not available for many individuals with disabilities who are pursuing employment. These are issues not directly related to PAS; however they are worth mentioning in this assessment as recommended changes in state policy. Assessment Recommendations This project identified the following 12 specific recommendations for the state of Indiana to ensure it meets the CMS criteria for Personal Assistance Services: Home and Community-Based Waiver Services and Personal Assistance: Reduce administrative costs of Waiver Services by having one centralized, local access point at which application and eligibility determination is done for all Waivers services. Simplify Indiana s current Waiver rates and service definitions. Ensure that services and funding are tailored to individual support needs and are flexible as the individual s needs change. Add a Consumer-Directed Home Care Option to the Waivers as recommended by the Community-Integrated Personal Assistance Services and Supports Task Force. Reduce the number of individuals on waiting lists for HCBS Waivers. Encourage legislators to implement rebalancing of funds allocated to nursing facilities and re-direct funds into community-based services. xiii
15 Proceed with plans to add HCBS Waiver slots in to ensure that more individuals with disabilities living in the community have access to services. Develop a clear definition of PAS under the HCBS Waiver programs or under the Medicaid State Plan, or a combination of both options. Identify PAS as a service offered to individuals in the home, community or workplace as needed for a minimum of 40 hours per week. Service Improvement and Service Initiatives: Work with entities to evaluate the training needs of PAS attendants and other direct-care staff based on quality improvement recommendations. Develop a formal process for grants collaboration among the various CMS grants funding initiatives in Indiana, so that a unified system of communitybased supports and planning is coordinated. Continue exploring Money Follows the Person initiatives through the MATRIX Task Force. Study the concepts of flexible funding and personal budgets to support individuals with disabilities in their communities and employment. Consider accessing funding for this initiative through applying for a Money Follows the Person Grant from CMS. Address Employment Barriers: Implement changes to the Medicaid Buy-In program as recommended by the Work Incentives Council in August Explore how Social Security s PASS program changes can be beneficial for Medicaid recipients. Explore and implement policies to allow eligible individuals in the Medicaid Assistance for the Disabled (MA D) category to set aside resources under the federal PASS program in excess of Indiana s xiv
16 Medicaid resource limit. Clearly state policies that allow individuals with approved PASS programs to participate in M.E.D. Works. Develop a unified state government policy on how to support people with disabilities in employment that does not define individual needs based on a specific disability eligibility category. The full report is a detailed assessment that addresses Indiana s status for meeting the Centers for Medicare and Medicaid Services criteria for full eligibility for Medicaid Infrastructure Grant funding. It also serves as a basis for the above recommendations. xv
17 I. INTRODUCTION Since the passage of the Ticket to Work and Work Incentives Improvement Act (TWWIIA) in 1999, several Federal initiatives have been underway to improve the choices and opportunities for people with disabilities to obtain and maintain community employment and self-sufficiency. One critical element of TWWIIA is to increase the availability of supports that individuals with disabilities may need to be successful in employment ventures. One of these supports is Personal Assistance Services (PAS), a support offered in both the home and workplace to improve the employment outcomes of individuals who require it. The definition of PAS in TWWIIA is: A range of services, provided by one or more persons designed to assist an individual with a disability to perform daily activities on and off the job that the individual would typically perform if the individual did not have a disability. Such services shall be designed to increase the individual s control in life and the individual s ability to perform activities on and off the job. 1 PAS is also defined as devices or hands-on support and assistance that encompass two categories of assistance, namely Activities of Daily Living (ADL s) and Instrumental Activities of Daily Living (IADL s). Assistance with ADL s includes bathing, dressing, transferring from bed or chair, walking, eating, toilet use and grooming. IADL s may include use of the telephone or computer, traveling via automobile or public transportation, shopping for food or clothing, meal preparation, 1 Public Law also known as the Ticket to Work and Work Incentives Improvement Act of 1999, consists of five titles including Ticket to Work and Self Sufficiency Provisions, Expanded Availability of Healthcare Provisions, Demonstration Projects and Studies, Miscellaneous and Technical Amendments, and the Tax Relief Extension Act. Pub. L. No , 203 (b)(2)(b)(ii) provides grants to develop and establish state infrastructures to support working individuals with disabilities. An eligibility requirement of infrastructure grants is to ensure Personal Assistance Services are available to individuals on and off the job
18 housework, medication use and management of money. Without personal assistance services, individuals would not be able to live independently, pursue employment, obtain an education or participate fully in community living (Wittman & Bezanson, 2004). Personal assistance is often as important in the workplace as it is in the home. Individuals with disabilities may need PAS to prepare for work; and while at work, may need assistance to perform some activities of daily living (such as eating or toileting). Employers are not required to provide these types of activities of daily living, though they may allow Personal Assistance Services in the work setting as reasonable accommodations. Other workplace accommodations that an employer may provide include but are not limited to: arranging workplace supports, making existing facilities used by employees with disabilities accessible, modifying jobs or work schedules, restructuring tasks, acquiring equipment or devices, providing travel assistance for an employee with a mobility impairment, helping an individual with a cognitive impairment with planning or decision making, or arranging for or facilitating communication for individuals with sensory impairments. Each individual with a disability has different needs and may require different combinations of assistance within reasonable parameters. Employers are encouraged to provide these workplace accommodations according to the Americans with Disabilities Act. 2 However, according to Title 1 of the Equal 2 United State Department of Labor, Office of Disability and Employment Policy describes Personal Assistance Services (PAS) in the workplace and provides examples of reasonable accommodations provided by employers to ensure workers with disabilities have access to assistance in the workplace
19 Employment Opportunity Commission (EEOC), employers are not required to provide accommodations primarily related to medical care or personal use items (such as eyeglasses or hearing aids). 3 Hoosiers with disabilities have access to different degrees of personal assistance through various means including a combination of Medicaid or Medicare funded services, family assistance, natural workplace supports, private-pay or selfpay. While several options exist, individuals with disabilities who need PAS-related services to support their employment goals realize that access to (and funding for) PAS is complex and difficult to obtain. The Federal government has provided opportunities for states to address access to PAS with several initiatives including Medicaid Infrastructure Grants (MIG); counseling on Social Security Work Incentives that addresses ways to fund PAS through Benefits Planning, Assistance & Outreach (BPAO); Community Integrated Personal Assistance Services (CPAS); Real Choice (RC) systems change grants; and, Direct Service Worker (DSW) grants. Indiana s Family and Social Services Administration accessed several of these Federal grant funding opportunities. These include the Community-Integrated Personal Assistance Services and Supports; Nursing Facility Transitions Grant; Quality Assurance and Quality Improvement System for Home and Community- Based Services; Real Choice Systems Change Grant; and, the Medicaid Infrastructure Grant. These Federal grants have an impact on community-based services and community living and are intended to achieve permanent and sustainable changes to the Medicaid funded services for long-term care in Indiana. This will allow individuals with disabilities return to work, remain employed and enhance their employment opportunities. References to systems change activities within these grant activities will be addressed in further detail in this document. 3 The Americans With Disabilities Act of 1990: Titles I & V outline reasonable accommodations and prohibits private employers, state and local governments, employment agencies and labor unions from discriminating against qualified individuals with disabilities in job application procedures, hiring, firing, advancement, compensation, job training, and other terms, conditions, and privileges of employment
20 In addition to accessing the aforementioned grants, Indiana University, Indiana Institute on Disability and Community, Center on Community Living and Careers and the Center for Mental Health in Anderson are awarded Federal funding from the Social Security Administration for Benefits Planning Assistance and Outreach. A summary of these grants and their activities is provided below. Table 1 Employment and Community-Based Services Grants in Indiana * Indicates CMS Systems Change Grants Type of Grant Purpose Grantee Activities * Medicaid Infrastructure Grant To design and implement an infrastructure to support competitive employment for people with disabilities. Family and Social Services Administration, Office of Medicaid Policy and Planning -Increase proper utilization of the Medicaid Buy-In program and other work incentives -Evaluate the feasibility of PAS services to meet CMS criteria for PAS available to workers with disabilities -Develop an employment leadership group for collaboration among state partners -Develop training program for Medicaid caseworkers to improve customer service on Medicaid Buy-In -Implement a data plan to evaluate the Medicaid Buy-in program -Develop web trainings, Business Leadership Network, Benefits Information Network, Employment Network Consortium *Community Personal Assistance and Supports *Nursing Facility Transition Grant To support states' efforts to improve personal assistance services that are consumerdirected or offer maximum individual control. To transition eligible individuals from nursing facilities to the community through two types of grants: State program grants to support state program initiatives and "Independent Living Partnership" to selected Independent Living Centers to promote partnerships for nursing facility transitions. Family and Social Services Administration Family and Social Services Administration -Outreach to increase awareness of consumer-directed personal attendant care services -Develop consumer-directed personal assistance services model and the infrastructure needed to support it -Establish a fiscal agent process to ensure accurate and timely claims payment and/or systems changes to the Medicaid contractor system -Provide enhanced training for state staff and local providers. Case managers will receive additional training on the newly designed consumer-directed attendant care model -Provide funding to four Area Agencies on Aging with successful models for diverting individuals to assist in transition and diversion efforts -Complete analysis of Senate Enrolled Act 493 to determine the fiscal impacts of increasing the eligibility for Medicaid Waiver services from 100% to 300% of SSI - 4 -
21 Type of Grant Purpose Grantee Activities *Quality Assurance and Quality Improvement in Home and Community- Based Services To design a quality assurance/quality improvement program to fulfill a commitment to assuring the health and welfare for HCBS Waiver participants. Family and Social Services Administration, Division of Aging and Rehabilitative Services -Design and implement an annual survey of at least 20% of beneficiaries and conduct annual focus groups to obtain feedback on service system -Establish and implement an ongoing review process to ensure that emergency backup systems are in place and effective -Develop and implement a standardized and effective system of incident reporting and response -Develop, monitor and enforce standards for service providers -Develop and implement effective and automated client incident reporting and complaint systems -Develop and implement automated systems to collect and analyze operational data from *Real Choice Systems Change Grant Benefits Planning Assistance and Outreach To design and implement effective and enduring improvements in community long term support systems to enable children and adults of any age who have disabilities or long term illnesses to live and participate in their communities. To hire benefits specialists and conduct outreach to better enable Social Security Administration beneficiaries with disabilities to make informed choices about work. Family and Social Services Administration Indiana Institute on Disability and Community, Indiana University; Center for Mental Health, Anderson the QA/QI system -Create the Governor s Commission on Home and Community-Based Services to develop short and long term strategies to create or expand community capacity for persons at risk of being institutionalized, or for those currently in an institution or nursing home -Have task forces of the commission address current system barriers and best practices, incentives for change, partnership recommendations for systems change, recommendations for strategies on community capacity building, process for implementing short-term strategies, and evaluation criteria to measure effectiveness of change -Issue mini-grants to create community partnerships to provide incentives for public/private partnerships, and to encourage innovation at the community level between community stakeholders -Provide individualized benefits counseling to beneficiaries of Federal and state programs on the impact of employment on their state and Federal benefits -Collaborate with the Social Security Administration, state partners, provider agencies, beneficiaries to provide education and outreach on work incentives -Collaborate with the MIG grant to develop education and outreach materials on M.E.D. Works and other state and Federal benefits -Collaborate with MIG and other state and Federal partners to develop a Benefits Information Network to build capacity of work incentives and outreach Source: Clearing House for the Community Living Information Exchange,
22 A. Purpose of the Personal Assistance Services Assessment The purpose of the Assessment of Personal Assistance Services in Indiana is to explore the need for enhancing Medicaid-funded Personal Assistance Services (PAS) to support individuals with disabilities who work. This document also assesses how Indiana s PAS services compare to the PAS eligibility criteria set forth by the Centers for Medicare and Medicaid Services (CMS) in its Medicaid Infrastructure Grant Program to assure that there are adequate PAS services for people with disabilities in the workplace. The assessment provides detailed information about the PAS programs currently available in Indiana. Recommendations are proposed for changes in Indiana s PAS programs pertaining to adding a State Plan PAS option, amending Waivers, developing a specific Waiver for PAS and employment or a combination of these strategies. B. Methodology for Personal Assistance Services Assessment The Office of Medicaid Policy and Planning (OMPP) used Medicaid Infrastructure Grant (MIG) funds to contract with the Indiana Institute on Disability and Community, Center on Community Living and Careers, to conduct a feasibility assessment of Personal Assistance Services (PAS) across the state. The assessment spanned a nine-month period of time, beginning in September of 2004 and continuing through June This assessment encompasses: a) Developing an understanding of the Federal policies and directives regarding PAS and employment of people with disabilities; b) Conducting a comprehensive overview and understanding of the current status of Personal Assistance Services (PAS) in Indiana; c) Evaluating the needs for PAS for people with disabilities who are employed; d) Identifying gaps in services and funding for these services; - 6 -
23 e) Suggesting options and recommendations to enhance PAS to meet the needs of people with disabilities who are employed; and f) Addressing the Federal recommendations related to PAS in Indiana s current Medicaid Infrastructure Grant. Modalities for gathering information included conducting interviews with numerous stakeholders such as individuals with disabilities requiring PAS and their family members; Medicaid Waiver case managers; providers of PAS services; consultation with the Community Personal Assistance Services and Supports (CPASS) task force; the Arc of Indiana; Indiana Association for the Area Agencies on Aging (IAAA) and other non-profit organizations. Regular monthly telephone consultations between the Indiana Institute on Disability and Community (IIDC), the Office of Medicaid Policy and Planning (OMPP) and the National Consortium for Health Systems Development (NCHSD) occurred to obtain resources and information. This assessment included an extensive review of state documents, memorandums, information bulletins and manuals (including the Bureau of Developmental Disabilities Services, Service Definitions and Standards Manual). Statistical data was collected from the Office of Medicaid Policy and Planning and the Office of Vocational Rehabilitation, Indiana Association for Area Agencies on Aging, the Centers for Medicare and Medicaid Services and reports of Indiana data posted on the Center for Personal Assistance Services website (2005). This assessment addressed the following topics: 4 Access to PAS services: Identifying the locations where PAS services are provided; exploring cost sharing mechanisms; identifying entry points to services; and, maximizing community inclusion and natural supports. 4 This format was adapted from the Personal Assistance Assessment Tool for Indiana, developed by the National Consortium for Health Systems Development
24 Eligibility for PAS services: Identifying the Waivers that cover PAS; identifying Medicaid Buy-In as being available to Waiver participants; evaluating the criteria to identify PAS services needed by individuals on Waivers; and, identifying how individuals access appropriate Waiver programs for their needs. Adequacy of PAS to support employment goals: Identifying the amount of hours PAS is available; exploring the cost containment measures that may limit PAS, or what measures are in place to ensure there is enough funding for sufficiency of services; identifying whether consumers have control and self-direction over their services; identifying the qualifications and adequacy of the PAS providers; exploring workers compensation for PAS providers; describing attempts to ensure the employer community is complying with the Americans with Disabilities Act guidelines for reasonable accommodations; exploring whether services are appropriate to meet individual needs of people needing services including type and amount of services to meet employment goals; and, identifying other services that maximize earnings and assets of individuals with disabilities. Policy development and performance monitoring: Exploring how policy decisions are made and what advocacy efforts are in place to address policy issues; identifying partnerships between and among state agencies; and, exploring the current system for gathering and monitoring data including statistical data, quality assurance, and consumer satisfaction. In addition to a comprehensive assessment of Indiana s PAS system, PAS services in states that are eligible to receive full Medicaid Infrastructure Grant funding were reviewed to determine options that may be beneficial for Indiana. This - 8 -
25 assessment summarizes the gathered information and provides a compilation of recommendations and options for Indiana to pursue PAS and implement inclusive employment policies. C. Limitations of This Assessment Because Indiana does not provide Personal Assistance Services (PAS) as a State Plan option, this assessment involves a review of Indiana s HCBS services and the accessibility and inclusiveness of PAS within those Waiver services. In Indiana, there is no clear definition of PAS under Waivers, as each Waiver has its own service definitions and categories. These definitions and service categories vary within Waivers, and alternatively are called Community Habilitation and Participation, Independence Assistance Services, Residential Habilitation and Support, Respite, and Supported Employment Services. Each service has different rates for reimbursement and capitations on numbers of hours of service available each month. With this complexity, it is difficult to ascertain if services are provided based on consumer need and choice or on limitations imposed by rates and cost containment measures. Accordingly, the previous broad definition of PAS is used in exploring the access, eligibility, and adequacy of services. Additionally, while this assessment progressed, Indiana imposed several changes to Waiver programs pertaining to cost-containment, reimbursement rates and other policies. Therefore, a general overview of PAS services and other issues related to removing barriers to employment for people with disabilities is addressed in this document. II. MEDICAID INFRASTRUCTURE GRANT FUNDING AND PERSONAL ASSISTANCE SERVICES The Medicaid Infrastructure Grant (MIG) program was authorized by The Ticket to Work and Work Incentives Improvement Act of 1999 (TWWIIA). Funding - 9 -
26 for this grant program is administered by the Centers for Medicare and Medicaid Services (CMS) and expires in The Federal Government has authorized a total of $30 million to be distributed among states who meet criteria outlined by CMS. MIG funds are available to encourage states to make lasting changes to their infrastructure and service delivery systems to enhance employment options for working individuals with disabilities. Many states use this funding to develop Medicaid Buy-In programs for working people with disabilities, increase the availability of Personal Assistance Services or access state-to state technical assistance and support. States may use the funding to remove barriers to employment through changes in the public health system and bridge Medicaid services with other key supports and programs used by employed people with disabilities. The two most important elements of MIG activities encouraged by CMS are Medicaid Buy-In and Personal Assistance Services. Indiana developed a Medicaid Buy-in program in 2001 known as Medicaid for Employees with Disabilities or M.E.D. Works. Indiana has yet to meet the MIG-related criteria for developing adequate Personal Assistance Services to support the employment of people with disabilities. This section describes the specific criteria outlined by CMS and Indiana s efforts toward meeting the criteria. A. Centers for Medicare and Medicaid Services Criteria for Personal Assistance Services within Medicaid Infrastructure Grant Funding In addition to developing Medicaid Buy-In, CMS is encouraging states to take steps to provide funding for PAS that meet the objectives of the TWWIIA provisions. Section 203(A)(1) of TWWIIA provides that states are eligible for MIG funding if they make PAS available under the state plan... to the extent necessary to enable persons with disabilities to remain employed. Beginning in 2001, CMS established eligibility criteria to implement this legislative directive and allow states to participate in the MIG program. In 2003, CMS issued new guidelines for determining a state s eligibility status for MIG funding. Two levels of eligibility were established:
27 conditional eligibility and full eligibility. Fully eligible states receive a four year award of funding. States that are conditionally eligible receive a two year award, and must achieve annual benchmarks related to improving their PAS systems. 5 Appendix A provides the CMS PAS scoring tool used to determine MIG funding eligibility (Centers for Medicare and Medicaid Services, 2005). After 2006, CMS will no longer make MIG funding available to states that are not fully eligible. CMS evaluates states eligibility for full MIG funding by examining how, where, and to what extent PAS services are provided. There is some flexibility on how states can meet CMS criteria for PAS services under the scoring tool. The criteria address whether PAS is offered through the optional Medicaid personal care services under the State Medicaid plan or through a selection of , 1915(c) 7 or 1915(b) 8 Waivers, and whether Waivers are sufficient in the number of slots and not 5 Effective October 2001, the Secretary of Health and Human Services began awarding grants effective states to design, establish, and operate infrastructures which provide items and services to support working individuals with disabilities. CMS is authorized to distribute infrastructure funds up to $20 million, $25 million, $30 million, $35 million, and $40 million for fiscal years , respectively. Beginning in fiscal years , CMS will authorize the prior year's amount adjusted for inflation. 6 Section 1115 of the Social Security Act provides opportunities for research and demonstration through Medicaid Waivers. States have used 1115 Waivers to make programmatic changes to their Medicaid program or alter the way they provide coverage and for services to the low-income population outside of the Federal standards and options. 7 Section 1915 (c) of the Social Security Act allows states to develop Home and Community Based Service Waivers (HCBS) to creative alternatives to placing Medicaid-eligible individuals in hospitals, nursing facilities or intermediate care facilities for persons with mental retardation. Under section 1915 (c) of the Social Security Act, states may request Waivers of certain Federal requirements in order to develop of Medicaid-financed community-based treatment alternatives. Services which may be provided in HCBS Waiver programs include: case management, homemaker/home health aide services, personal care services, adult day health, habilitation, and respite care. HCBS Waiver programs are initially approved for 3 years and may be renewed at 5-year intervals. 8 Section 1915 (b) of the Social Security Act allows states to create Freedom of Choice Waivers, which are generally used to enroll beneficiaries into managed care programs; create a "carve out" delivery system for specialty care; create programs that are not available statewide and provide an enhanced service package. This allows the State to provide additional services to Medicaid beneficiaries via savings from managed care programs. The 1915(b) Waivers are limited in that they apply to existing Medicaid eligible beneficiaries, and authority under this Waiver cannot be used for eligibility expansions
28 limited by a high level of care criteria. For states pursuing eligibility for MIG funding through Waivers, CMS must also be able to determine the Waivers have the capacity to serve at least 51% of the number of individuals who would be expected to participate in employment. At a minimum, PAS services must meet these key criteria: Services must be provided inside or outside the home including the workplace; The population served are those who are most likely to be competitively employed; The services are available statewide; and There are sufficient amounts of hours of PAS services available for people who need services to be employed full-time. In addition to the criteria listed above, Medicaid Waivers must serve a sufficient number of individuals relative to the estimated need for services and those Waivers must allow participation in the state s Medicaid Buy-In program. In the 2006 grant year solicitation, conditional eligibility for MIG funding will be offered a final time. States must reach full eligibility by 2008 or be ineligible for continued MIG funding. Indiana is currently receiving MIG funding as a conditionally eligible state, meaning Indiana offers PAS sufficient to support a person with disabilities to work 40 hours per month or sufficient enough to support part-time employment. States that are fully eligible for MIG funding offer PAS to individuals for a minimum of 40 hours per week or sufficient enough to support full-time employment. Per the objectives of TWWIIA, states need to offer PAS to support fulltime employment and produce desired outcomes resulting in self-sufficiency. To meet the criteria to be fully eligible for MIG funding, Indiana must ensure PAS services are available inside and outside the home, including the workplace, to support individuals in full-time employment. Indiana does not currently offer PAS
29 under the state plan. It does offer PAS statewide to persons with developmental disabilities and physical disabilities under the various Waiver services inside and outside the home on a limited basis. Indiana s Waivers also allow individuals to participate in M.E.D. Works (Indiana s Medicaid Buy-In program). According to the Centers for Medicare and Medicaid Services MIG Grant Project Officer, to meet sufficiency of CMS criteria under the Home and Community- Based Waivers, Indiana is required to have enough Waiver slots to serve 3,692 individuals with physical disabilities and 5,672 individuals with mental retardation/developmental disabilities. 9 This figure is equal to or greater than 51% of the number of individuals estimated to qualify for the Waiver in the state. B. Indiana s Progress toward Removing Medicaid Barriers to Employment In 2000, a group of citizen advocates convened to address Indiana s Medicaid barriers to employment. This group was comprised of people with disabilities, family members, advocates, employers of people with disabilities and professionals. They named themselves the Indiana Medicaid Action Coalition (IMAC) and worked for approximately 18 months to develop legislation to create an optional Medicaid service allowed under TWWIIA. 10 Under the Ticket to Work provisions, states were granted more flexibility to provide Medicaid coverage for people with disabilities who work. 9 Phil Otto, Project Officer for Medicaid Infrastructure Grants, Center for Medicare and Medicaid Services provided Indiana s requirements for sufficiency of Waivers in an dated June The estimates of 3,692 individuals with physical disabilities and 5,672 individuals with mental retardation/developmental disabilities estimated to qualify for the Waiver in Indiana is derived from the Home and Community-Based Services State by State Population Tool, a tool developed for CMS by the Lewin Consulting Group. 10 Section 201 of the Ticket to Work and Work Incentives Improvement Act P.L , 42 U.S.C et. seq. allowed states to create Medicaid-Buy-In coverage for eligible working individuals with disabilities. In Indiana, the Medicaid buy-in program was established in July 1, 2002 and is called M.E.D. Works- Medicaid for Employees with Disabilities
30 After collecting data and studying the Federal Medicaid provisions, IMAC proposed that Indiana develop a state Medicaid Buy-In program for working people with disabilities. In 2001 of the first regular session of the General Assembly, House Enrolled Act (HEA) provided the opportunity to allow Medicaid coverage for working individuals with disabilities who would either (1) find themselves ineligible for Medicaid; or who would (2) experience increased out of pocket costs (spend-down) each month before becoming eligible for Medicaid when they worked. The program, beginning in July 1, 2002 resolved the barrier to work for Hoosiers with disabilities who previously had to choose between employment and healthcare. This program, called M.E.D. Works - Medicaid for Employees with Disabilities, allows working individuals whose incomes are too high for Medicaid Assistance for the Disabled (MA D) to be eligible for health care coverage. A summary of HEA 1950 is described below: Includes language of Section 1619 of the Social Security Act in the Indiana code. Adds a new chapter to the Indiana code (Chapter 41) to develop a Medicaid Buy- In program for working individuals with disabilities by January 1, Allows for resource disregards, including all resources currently not counted by Medicaid, retirement savings held by the individual or their spouse, and savings for independence and employability (up to $20,000 for goods or services not covered by any other public funding through a special account called savings for Independence and Self-Sufficiency). Requires applicants to meet Indiana s durational requirement of a disability as defined with some important exceptions for enrollees in Medicaid Buy-In, including: individuals must have a severe medically determinable impairment without regard to their ability to work; individuals must be between ages16-64; individuals must be engaged in a substantial or reasonable work effort as allowed by Federal law and defined by the Office of Medicaid Policy and Planning; individual s gross income must not exceed 350% of the Federal poverty level; 11 House Enrolled Act 1950 is the 2001 legislation that allows Indiana to provide Medicaid Buy-In under a state plan option as allowed under the Ticket to Work and Work Incentives Improvement Act provisions
31 income of the individual s spouse is disregarded in determining eligibility for the program; and, individuals may disregard Impairment-Related Work Expenses as defined by Medicaid and the Social Security Administration. Provides coverage for medical improvement as defined by Federal law, meaning the loss of eligibility for Social Security Disability Insurance cash benefits due to earnings. These individuals may still be eligible for Medicaid coverage if: they continue to have a medically determinable impairment; they are employed and are earning a monthly wage that is not less than the Federal minimum hourly wage times 40; they pay cost sharing premiums; and, they meet all other eligibility requirements of the Medicaid Buy-In program. Provides continued coverage for involuntary loss of employment. Individuals who are unable to maintain employment involuntarily (due to health conditions or involuntary termination), may continue Medicaid coverage if they: request a continuance within 60 days of termination; maintain connection to the workforce (such as participation with Vocational Rehabilitation, Workforce Development, a school to work program); have documentation from the employer regarding a temporary leave from work; pay premiums if required; and, continue to meet eligibility requirements for Buy-In. This coverage can continue for up to 12 months. After 12 months, an individual must meet the requirements for Medicaid assistance to individuals who are disabled. Allows premium sliding fee scales for participation in Buy-In. These are based on the annual gross income of the individual (and spouse if married); ranging between a minimum of 25 dollars and a maximum of 275 dollars for income between 150% and 350% of the Federal poverty level; the premium may not be over 7 and 1/2 percent of the gross annual income of the individual and their spouse divided by 12; and, deductions in the premiums are made for any other health insurance premium paid by the individual or individual s spouse for healthcare that covers the individual. Requires re-determination of disability based on the individual s medical evidence rather than based on participation in employment, earned income and/or income from self-employment
32 Allows individuals in Medicaid Buy-In to receive the same benefits and be subject to the same requirements as other Medicaid recipients including personal care and home health care services. Requires the Office of Medicaid Policy and Planning to determine the effectiveness of the program and report data collection. Establishes a Medicaid Work Incentives Council to oversee and advise on the program. Requires the Office of Medicaid Policy and Planning to amend the Medicaid State Plan to include Medicaid Buy-In, apply for a Medicaid Infrastructure Grant, and include all Medicaid Waivers for eligibility for Medicaid Buy-In (effective September 1, 2002, the M.E.D. Works categories of assistance included coverage for all of Indiana s Medicaid Waivers). The M.E.D. Works program includes Personal assistance-related services in the definition of Impairment-Related Work Expenses (IRWE). 12 This provision of M.E.D. Works allows individuals to pay for PAS-related services out of pocket and offset these expenses against earnings counted by the Social Security Administration (SSA) under the Substantial Gainful Activity level (currently $840 in 2005). By including IRWE deductions in the M.E.D. Works program, individuals may continue to receive a Social Security Disability Insurance (SSDI) benefit for a longer period of time as they work toward self-sufficiency and independence. The IRWE deduction for PAS allows individuals to supplement their PAS in the workplace once the maximum allotted hours of Medicaid-funded services are reached. C. Indiana s Accomplishments with Medicaid Infrastructure Grant Funding The Indiana OMPP received MIG funding beginning in 2003 for four years (through 2006). Currently, based on its availability of PAS, Indiana is conditionally 12 Impairment Related Work Expenses are a Social Security work incentive that allows individuals to deduct certain items or services they need in order to work from their gross earnings, even if those items are needed for non-work activities. IRWE s are defined in the Indiana code, section 405 IAC Income of Applicant or Recipient Sec. 2 (b) (4)
33 eligible for MIG funding. 13 To be determined fully eligible for MIG funding, Indiana must achieve benchmarks recommended by CMS (including providing Medicaid coverage for PAS services that are sufficient to support individuals in full-time employment). If Indiana is determined fully eligible, the state may receive funding in excess of $500,000 through year 2011 to address infrastructure issues related to employment for people with disabilities. In addition, Indiana would be able to apply for a Comprehensive Employment Systems Medicaid Infrastructure Grant, which would allow grant activities to address employment infrastructure needs beyond Medicaid services. Already through the past two years, Indiana has made remarkable strides to improve the state s employment infrastructure for people with disabilities. This progress includes: Operating a Medicaid Buy-In program, known as M.E.D. Works; Convening an Employment Leadership Group through collaborative efforts between the Office of Medicaid Policy and Planning MIG grant and Vocational Rehabilitation Services; Pursuing employer involvement through a statewide Business Leadership Network; Conducting a needs assessment on education and outreach to people with disabilities on M.E.D. Works and other state and Federal benefits; Providing user-friendly educational resources on M.E.D. Works, Federal benefit programs and other resources for people with disabilities; Establishing a comprehensive work supports website for people with disabilities; Surveying community and state resources to map out resources offered to people with disabilities in Indiana through local, state and Federal venues; 13 In 2003, CMS permitted conditionally eligible states up to four years of funding. For the 2005 and 2006 funding years, CMS will only provide new conditionally eligible grantees with two years of funding
34 Establishing a Benefits Information Network to increase capacity of benefits counseling; Creating orientation materials on work incentives and employment information for the Medicaid Work Incentives Council and other policy advisors; Increasing consumer involvement in systems change activities under the MIG funding; Improving data analysis on outcomes of people with disabilities and employment; and Spearheading an Employment Network Consortium. Indiana continues making progress in promoting employment for people with disabilities through the MIG funding and is committed to improving its employment infrastructure for people with disabilities. A critical benchmark that Indiana must achieve to receive MIG funds as a fully eligible, comprehensive employment state is to satisfy CMS s requirements for providing Personal Assistance Services. While Indiana offers PAS-related services through the Home and Community-Based (HCBS) Waiver services, the services offered may not be sufficient as outlined by CMS requirements for workplace personal assistance. II. PERSONAL ASSISTANCE SERVICES IN INDIANA Because Personal Assistance Services (PAS) are not offered under Indiana s Medicaid State Plan, this section will review Indiana s Waiver system and how PAS is currently offered under the Home and Community-Based (HCBS) Waivers. A detailed description of the available Waiver services, including reimbursement rates for hours/units of services are provided
35 A. Overview of Indiana s Medicaid Waiver Programs Indiana Medicaid is a needs-based health insurance program that helps to pay for the medical expenses and disability-related services and supports of individuals and families with limited incomes. As a Federal/state public health insurance program providing coverage to families with children, pregnant women and children, aged, blind and disabled individuals with low incomes, Medicaid has several different categories of coverage. It is important to understand which category of Medicaid applies to different individuals for their particular needs. Medicaid assistance for people with disabilities or people who are blind covers a wide variety of services and supports. For eligibility purposes, individuals must belong to one of the aforementioned groups and meet financial criteria for that group. To qualify for Medicaid Assistance for the Disabled (MA D) a person must have a physical or mental impairment, disease or loss (verified by a physician) that will result in death or that has lasted or appears reasonably certain to last for a continuous period of at least 12 months. Indiana provides a comprehensive package for Medicaid services; a number of which are mandated by CMS to receive Federal matching funds. These include: Outpatient hospital services, Inpatient hospital services, Laboratory and X-ray services, Nursing facility and home health services, Nurse midwife services, Family planning services and supplies, Physician services and surgical services of a dentist, Early periodic screening diagnosis and treatment for people under age 21, Rural health clinic services, and Nurse Practitioner services
36 In addition, Indiana funds an extensive list of optional Medicaid services, including: Dental services, Emergency hospital services, Hospice care, Inpatient psychiatric services for those under age 21, Home health services provided by home health agency (under age 21), including intermittent/part-time nursing services, home health aide services, medical supplies, equipment, appliances for use in home, physical, occupational or speech pathology/audiology, Transportation services, Nurse anesthesia services, Occupational therapy, Physical therapy, Prescription drugs, Private duty nursing services, Psychological services, Respiratory care services, Speech, hearing, and language disorder services, Extended services for pregnant women (including pregnancy-related & postpartum services for 60 days, additional services provided to pregnant women only (care coordination/targeted case management), and services for condition that may complicate pregnancy, Clinic services, Diagnosis services, Eyeglasses, Inpatient hospital services for those over age 65 in institutions for mental diseases, Intermediate Care for the Mentally Retarded (group homes and large facilities),
37 Nursing facility services for those under age 21, Optometry services, Podiatry services, Preventive services, Prosthetic devices, Rehabilitative services, Screening services, and Durable medical equipment. Indiana Medicaid also provides funding for long-term care in licensed nursing facilities, intermediate care facilities, group homes, state operated institutions and developmental centers (Indiana Family and Social Services Administration, People with Disabilities Medicaid, 2004). Indiana s funding for Home and Community-Based Waivers allow individuals with disabilities to divert from state operated institutions, nursing facilities, long-term care facilities such as Intermediate Care Facilities for the Mentally Retarded (ICFMR s) and group homes, and live in either the community with their families or independently with supports. These Waivers are intended to ease the fiscal burden and high cost of services for individuals living in facility-based Medicaid funded institutions (Arc of Indiana, Guide to Medicaid and Medicaid Waivers, 2005). Eight different Medicaid Home and Community Based Waivers are available for individuals with disabilities in Indiana. Seven of these Waivers are available statewide, without geographic restrictions. The exception is the Waiver for Youth with Serious Emotional Disturbance (SED). Indiana s current Waivers include: Developmental Disabilities (DD) Waiver Autism Waiver Support Services for People with Developmental Disabilities Waiver Medically Fragile Children's Waiver Traumatic Brain Injury Waiver
38 Assisted Living Waiver Aged and Disabled Waiver Serious Emotional Disturbed Youth Waiver Eligibility for Medicaid Waivers Individuals must meet the financial eligibility guidelines for Indiana Medicaid in order to qualify for a Medicaid Waiver (for children and youth under 18, parental income and resources are not counted). In addition, an applicant must also meet the criteria for level of care required for admission into a group home, long-term care facility or state institution. The Level of Care System is a key component of the eligibility determination process for Medicaid Waivers. Each Waiver has different requirements for the amount or level of care required. For example, individuals eligible for the Developmental Disability, Autism, or Support Services Waivers must need the level of care provided in an Intermediate Care Facility for the Mentally Retarded (ICFMR), nursing facility or state operated facility. Individuals eligible for the Traumatic Brain Injury Waiver, Assisted Living and Aged and Disabled Waivers must need the level of care provided in a nursing facility. To be eligible for the Medically Fragile Children s Waiver, individuals must need the level of care provided in a skilled nursing facility or hospital. To qualify for a Medicaid Waiver a person needs to be eligible for care in a nursing facility or a hospital; or if the person has a developmental disability, he or she must qualify for services through an Intermediate Care Facility for the Mentally Retarded (ICFMR) or a group home. Depending on the Waiver for which a person is applying, the Area Agency on Aging, Bureau of Developmental Disabilities Services 14 For this assessment, the Serious Emotional Disturbed Youth (or SED Waiver) for children and youth ages 4 through 21 years is not included in evaluating Personal Assistance Services for Medicaid Infrastructure Grant eligibility. This Waiver is not required to be offered statewide at the current time. The SED Waiver became available in February 2004 for up to 50 people in 10 counties (Daviess, Elkhart, Knox, Lake, Marion, Martin, Pike, Randolph, St. Joseph, and Vigo) for the first year. For years two and three, CMS approved a maximum of 200 additional Waiver slots for the SED Waiver depending on the availability of the required state match. The SED Waiver program will eventually be implemented state-wide. Source: Medicaid Home and Communitybased Waiver for Children with SED last revised July,
39 or the Department of Mental Health and Addictions will coordinate the assessment process to determine if the person needs the level of care provided in an ICFMR group home, nursing facility or hospital. The total Medicaid cost of serving the person on the Waiver (Waiver cost plus other Medicaid services) cannot exceed the total cost to Medicaid for serving the person in an institutional setting. Appendix B provides a summary of Indiana Medicaid Waivers, where to apply for Waiver services, the waiting lists, state expenditures for each Waiver and who the Waivers serve. Individuals must also meet income eligibility provisions for Waivers. These provisions are explained in detail in the Indiana Client Eligibility System Program Policy Manual. 15 Understanding where to apply for Waivers can be confusing for individuals with disabilities, family members, advocates, school personnel and providers. There are two main entry points for Waivers. Individuals must apply at the local Bureau of Developmental Disabilities Services (BDDS) office for the Autism, Support Services and Developmental Disability Waivers, but they must go to the Area Agency on Aging (AAA) to apply for the Aged and Disabled, Traumatic Brain Injury, Assisted Living and Medically Fragile Children s Waivers. Some local AAA offices accept applications for all Waivers. To add to the complexity of where to apply for Waivers, individuals may receive services under one Waiver (such as the Support Services Waiver) and be on the waiting list for another Waiver (such as the DD Waiver). Individuals with disabilities who want to access Waivers and those advocating for them need to understand level of care criteria and the various services offered through each of these Waivers in order to navigate the system. In addition, applications for Social Security cash benefits, Medicaid Assistance for the Disabled 15 The Indiana Client Eligibility System Program Policy Manual Chapter 3300 outlines income and resource requirements. There may be two different ways in which a person can be eligible for Medicaid under a waiver: regular Medicaid eligibility rules and special waiver rules. There are variances in resource limits among the different waivers. In general, the resource limit is $1500 for an individual and $2250 for a married couple. For income eligibility, a Special Income Level (SIL) is used depending on the type of waiver and whether the applicant is a child or an adult, single or married. The SIL is 300% of the maximum benefit payable under the SSI program. The standard increases annually when SSI increases in January. The SIL effective 1/1/05 is $
40 (MA D) and other services such as Vocational Rehabilitation Services (VRS) may need to be addressed. Many individuals receiving Vocational Rehabilitation may need funding for supported employment follow-along services to ensure an individual s continued success on the job. Determining how to fund follow-along when individuals are on waiting lists for Waivers can be challenging for providers who are required to ensure follow-along is available. 2. Cost Sharing Mechanisms for Medicaid Waiver Participants For the purpose of financial eligibility, Indiana has a spend-down program for individuals with income or resources too high to qualify for Medicaid assistance. Participants in the spend-down category must pay for some of their medical costs each month before they are eligible for Medicaid in that month. This situation occurs any month their income exceeds the Federal benefit rate (currently $579 in 2005). The exception to this policy is for individuals who participate in the DD, Autism, and Support Services Waivers, as the monthly income limit for these Waivers is $1,737 per month (in 2005). Spend-down in these cases occurs if a person's income exceeds $1,737 a month. Individuals must also spend down excess resources if their resources exceed Indiana s resource limit of $1,500. Working Medicaid recipients with disabilities (including Waiver participants) may participate in M.E.D. Works, Indiana s Medicaid work incentive. This work incentive is particularly useful for those individuals who are not eligible for Social Security s Supplemental Security Income (SSI) Program. For those individuals who are SSI recipients, Section 1619 of the Social Security Act protects their eligibility for Medicaid when they are working and earning income above the Federal benefit rate. 16 Those individuals who are not eligible for 1619 Medicaid protection have 16 The Social Security Act 42 U.S.C. 1382h provides continued protection for Supplemental Security Income (SSI) and Medicaid for SSI recipients who work. These individuals can continue to be eligible to receive SSI checks and Medicaid when working if they still have a disability and meet other requirements (such as income and resource limits). Section 1619b allows individuals who are eligible for SSI to continue to be eligible for Medicaid coverage when their earnings are too high to continue to receive SSI. This work incentive applies to individuals whose earnings are below Indiana s threshold (currently $29,194 in 2005)
41 access to Indiana s M.E.D. Works program and may be subject to paying premiums on a sliding fee scale based on their income. In addition, M.E.D. Works allows a Savings for Independence and Self- Sufficiency of up to $20,000 that may be established for the participant to purchase specified services or items needed to maintain employment and/or improve his or her employability and independence. Examples of Savings for Independence and Self-Sufficiency include saving to purchase a modified vehicle for transportation to and from work or saving for educational expenses to increase employment income. Medicaid does not cover the out of pocket costs that individuals may require for non-prescription health related items (e.g., suppositories or latex gloves). The non-covered costs of health related items combined with the costs of a Medicaid spend-down can result in a substantial portion of a person s income being directed towards health related costs. 3. Services Provided through Indiana s Waivers There is an array of services that may be provided on particular Waivers. The type of services available to a person will vary depending on the Medicaid Waiver program in which the person is participating, the individual s needs and his or her personal preferences and priorities. The following services are available under each of the Waivers: Adult Day Services, Behavior Support Services, Case Management, Community Habilitation and Participation, Enhanced Dental Services, Rent and Food for an Unrelated Live-In Caregiver, Family and Caregiver Training, Health Care Coordination,
42 Music Therapy, Nutritional Counseling, Occupational Therapy, Person Centered Planning/Individual Support Planning Facilitation, Personal Emergency Response System, Physical Therapy, Pre-Vocational Services, Psychological Therapy, Recreational Therapy, Respite Care, Specialized Medical Equipment and Supplies, Speech/Language Therapy, Supported Employment Follow-Along, and Transportation. Additional services that are available under each of the Waivers (with the exception of the Support Services Waiver) include: Community Transition (one time set-up expenses for people moving from institutions); Environmental Modifications; Residential Habilitation and Support; and, Adult Foster Care. The Support Services Waiver is limited to $13,500 per year, which may include up to $2,000 in respite care. The Autism Waiver covers Applied Behavior Analysis in addition to the services listed above. Different Waivers may have different names for services that are very similar (or essentially the same). For example although the DD Waiver, Support Services Waiver and Autism Waiver do not specify attendant care as a separate service, attendant care may be provided within the context of the services identified as Community Habilitation and Participation, Residential Habilitation and Support or Respite Care. Each Waiver has a different service definition (Bureau of Developmental Disabilities Services, Service Definitions and Standards Manual
43 2004). Services allowed under the Home and Community-Based Waivers are summarized below. Community Habilitation and Participation (CHP) Services Community Habilitation and Participation (CHP) Services are available under the Developmental Disability, Support Services and Autism Waivers. These are supports provided outside of an individual s home that support learning and assistance in any of the following areas: Self-care, Sensory motor development, Socialization, Daily living skills, Communication, or Social skills. CHP services can be delivered to an individual one-on-one or in a group setting (see group size below); in the community, or in a facility. CHP services are provided within the following categories: Community Based Individual CHP-I Community Based Group CHP-G Facility Based Individual CHP-F Facility Based Group CHP-R In general, the CHP services include: supervision, monitoring, training, education, demonstration or support to assist with the acquisition and retention of skills; and, training and education in self-determination. Each person receiving CHP services works toward acquiring the skills to become an active member of the community. CHP services for the individual (CHP-I) are intended to help build non
44 paid relationships or natural supports between the person with a disability and people without disabilities. Examples of CHP services include but are not limited to: Unpaid work experience (e.g., volunteerism); Educational activities; Leisure activities and community events related to desired outcomes reflected in the Individualized Support Plan (ISP) required by the state; Training and education in self-determination designed to help individuals achieve one or more of the following outcomes: - Development of self-advocacy skills, exercise civil rights, - Acquisition of skills that enable the ability to exercise control and responsibility over services and supports received or needed, and - Obtainment of skills that enable the person to become more independent, integrated or productive in the community. Location of Services: Services are to be furnished outside of the person s home (including residential settings) and are not available to support a person in paid employment. Number of Allowable Hours of Service per Month: For people on the DD or Autism Waivers up to 25 hours per month of CHP-I and CHP-F are available. For people on the Support Services Waiver, CHP-I hours may be used as needed, taking into account the other needs of the person and the $13,500 annual fiscal cap of this Waiver. Medicaid Waiver Rate: CHP-I and CHP-F allows 1:1 support for volunteer work or participation in integrated classes at a rate of $6.90 for a.25 hour unit (or $27.60/hour). These services are capped at 25 hours per month
45 Independence Assistance Services Independence Assistance Services (IAS) are allowed under the Developmental Disability and Autism Waivers. IAS provides supports needed for a person to live successfully in his or her own home. Allowable activities include the provision of monitoring and supervision to assure the following: Acceptable personal care and grooming, Appropriate handling of personal finances, bill payment, bank accounts, etc., Proper administration of medications, access to medical care and attention to health care needs, Maintenance of household care and responsibility, Sustaining dietary plans and grocery needs, or Demonstration of appropriate self-direction and decision making skills. Locations of Services: A minimum of 50% of the time delivered by a paid support person must be a direct face-to-face contact with the person with a disability in the person s home or community. Number of Allowable Hours of Service per Month: Independence Assistance Services allow up to a maximum of 30 hours of support per month for persons on the DD and Autism Waivers, as well as for those who have an Individual Community Living Budget (ICLB), a state funded service. IAS services may not be combined with the Medicaid Waiver service category of Residential Habilitation and Support Services (RHS). Medicaid Waiver Rate: This service allows $24.52 per hour for up to 30 hours per month
46 Residential Habilitation and Support Services Residential Habilitation and Support Services (RHS1, RHS2, and RHS3) are available through the Developmental Disability and Autism Waivers and allow supports up to 24 hrs per day which are intended to ensure the health, safety and welfare of the person. Services provided must be outlined in the Individual Support Plan. In addition, RHS services are designed to assist with the acquisition, improvement, and retention of skills needed for the person to live in his or her own home. Allowable activities include direct supervision, monitoring, training, education, demonstration or support to assist with: Meals, Household care/chores, Acquisition, improvement and retention of life skills, Behavioral Support Plan implementation, Shopping, Medical appointments, or Community exploration and leisure activities. Number of Allowable Hours of Service per Day/ Week/ Month: Up to 24 hours per day of services may be provided as needed. There are several categories of service provision. These are reflected as follows: RHS1 35 hours or less per week if needed by the individual; RHS2 Support provided by a Qualified Mental Retardation Professional, 10 hours per month or less, and may be used only with RHS1; and RHS3 More than 35 hours per week if needed by the individual. Guidelines are included in the BDDS Service Definitions and Standards Manual for determining the staffing needs and/or RHS service needs of individuals receiving services. In general, the guidelines suggest the following provision of
47 RHS services per day based on the number of people with disabilities or service recipients within a household: 1 person setting average of 18 hours RHS per day 2 person setting average of 30 hours RHS per day 3 person setting average of 40 hours RHS per day 4 person setting average of 50 hours RHS per day Fluctuation in the total daily hours of services is noted as acceptable as long as the daily average for the week is within the guidelines. It should be noted that within the guidelines for RHS it is also reflected that in some instances a person in need of services and supports cannot live with another person and must live in his or her own place with 1:1 staffing. In these instances up to 24 hours of RHS may be available. Parents/Guardians Provision of RHS: RHS may be furnished to an adult with disabilities by the person s parent or guardian for up to 40 hours per week. RHS may not be provided by a parent or stepparent for minors. Location of RHS: RHS may be provided in the person s home, place of employment when approved by the Waiver Specialist for workplace assistance and in the community. Medicaid Waiver RHS Rate: RHS1 = $4.88 /.25 hour unit (or $19.52/hour) - when RHS hours are 35 hours or less per week. RHS2 = $6.13 /.25 hour unit (or $24.52/hour) - only available with RHS1 services, 10 hours per month or less of QMRP time. RHS3 = $4.40 /.25 hour unit (or $17.60/hour) - when RHS hours are more than 35 hours per week
48 Respite Respite services are provided to individuals unable to care for themselves that are furnished on a short term basis due to the absence of others who typically provide supports and care. Respite is allowed under the Developmental Disability, Support Services, Autism, Aged and Disabled, Medically Fragile Children s, Traumatic Brain Injury and Serious Emotionally Disturbed Youth Waivers. Respite is a support allowed for temporary relief from care for family members and may include the following activities: Assistance with grooming, toileting and personal hygiene, Assistance with mealtime preparation and eating, Assistance with daily living skills, including assistance with accessing the community and community activities, or Administration of medications. Location of Services: Services may be provided in the person s home, the caregiver s home, or in a nonprofit residential facility (i.e., respite home). Services may include supporting the person to access community activities as well. Medicaid Respite Rates: RATT (respite) services allow $3.97 per.25 hour unit (or $15.88 per hour) or a cap of up to 10 hours per month. Respite rates may not exceed $2,000 per year per person unless approved by a State Exception Review Team. Bureau of Developmental Disabilities Services Supported Employment Follow- Along Services Supported Employment Follow-Along Services (coded as HSE) are services that enable a person to maintain paid employment if the person is paid at or above the Federal minimum wage. Activities allowed include:
49 Employment services in an integrated work setting. Integrated is defined as a setting where at least 51% of the workers are people without disabilities; Support provided at the work place by paid personnel who may observe and supervise the individual, teach job tasks as needed and monitor the workplace at least twice a month to help maintain employment; Off site or work place monitoring at the request of the person receiving services (including staff travel, plan development, client advocacy client transportation, client training, coworker supports and documentation); or Facilitation of natural supports at the workplace. Annual rate/cap for service: HSE (Supported Employment Follow-Along) allows $9.17 per.25 hour unit (or $36.68 per hour). There are several caps outlined in the Supported Employment Follow-Along service definitions. For example, individuals working more than 5 hours a week may receive up to $4500 annually in follow-along services. Individuals working less than 5 hours a week may receive up to $2500 annually in follow-along services. Other Service Standards: The person receiving services must have: 1. Made the transition from Vocational Rehabilitation Services (VRS), 2. Been found ineligible for VRS, or 3. Lost his/her job and requires less than 10 hours of job development Providers interviewed for this report have indicated that as of March 2004, job development is no longer an allowable service under Supported Employment Follow-Along. If individuals need job development and funding for this service, they must be referred to Vocational Rehabilitation Services for this activity
50 4. Cost-containment within Indiana s Waivers Indiana has developed a system for managing the expenses and the services provided under the Medicaid Waiver programs. Individuals and their families must work with a Medicaid Waiver case manager to develop an "Individualized Support Plan" (ISP) using a "Person-Centered Planning Process" (PCP) to determine what services available under the Waiver are most appropriate for the individual and how those services will be used from month to month. Indiana is committed to ensuring that the costs of providing services under a Medicaid Waiver are less than the cost of services provided in a Medicaid funded institution. Because of this, case managers and individuals must ensure that services are appropriate, and of a level of need to maintain community living. Success in accessing the appropriate services and hours tailored to the individual s Person-Centered Plan is dependent on the skill of Waiver case managers in balancing the services that the individual needs within rates and caps of services. 18 The Department of Justice has been reviewing Indiana s community-based services and providing recommendations for services offered to individuals who have been transitioned out of State Developmental Centers. These recommendations noted continued growth and improvement in community-based services. Additionally, they suggested further improvements in the transition process, case management services; interdisciplinary team processes and support planning, documentation, quality assurance and quality improvement, communication, training and vocational supports, behavior management and other health and medical concerns. Indiana is required to carefully consider these recommendations when evaluating funding, policy implementation, and program 18 Waiver case managers interviewed for this assessment indicate that caps on services (such as Supported Employment Follow-Along) may at times prohibit supports and interventions when required by individuals on their jobs. Individuals receiving follow-along services must be stable on their jobs before Vocational Rehabilitation Services cease. However, over time, changes in the job environment or the individual s situation after successful Vocational Rehabilitation case closure may require intervention that is not funded because of service caps. This may cause risks to employment stability and potentially perpetuates recidivism in job loss for some individuals
51 changes for Home and Community-Based Services (Family and Social Services Administration, 2005). In 2001, Indiana developed an Olmstead Comprehensive Plan, and has achieved some progress on policy directions related to Home and Community- Based Services. Some of the steps identified in the Plan are comparable to the issues explored in this assessment. These issues include: adding additional Waiver slots to support individuals with disabilities in the community; addressing waiting lists for Medicaid Waivers; piloting consumer-directed personal assistance; increasing training options for providers; expanding an ombudsman program; and, developing quality improvement systems for services provided to individuals with developmental disabilities. One Olmstead action step incorporated changes to the Developmental Disabilities Waiver to broaden categories for reporting and rate structuring (consolidating PAS into Community Habilitation and Participation and Residential Habilitation Services). While this action step may have alleviated reporting and rate structuring for separate services provided under the Waiver, it reduced the ability to clearly identify PAS as a separate service and quantify how much PAS is available to individuals. Indiana is exploring the service needs and costs of Medicaid Home and Community-Based Waiver Services as individuals have transitioned out of institutions. In 2005, FSSA s Division of Disability and Rehabilitative Services contracted with the Indiana Institute on Disability and Community to evaluate the high cost of Medicaid Waiver services for 200 individuals. The two primary questions asked: 1) Are unnecessary costs occurring? 2) If so, what are the unnecessary costs? Preliminary findings from this evaluation indicate the lack of capacity across the state as well as the impact of staff turnover, influences the quality of services
52 B. Medicaid Waiver Services Providing Personal Assistance Because each Waiver has different names for services that are very similar or essentially the same, and the services offered through most Waivers may be provided both inside the person s home and in the community, Waiver case managers and individuals must choose to balance the rates and services for support on the job against a full array of non-employment related activities. To some extent, PAS are offered under home health services through Waivers. However, home health is not a service that is considered by CMS as meeting the criteria of PAS services for the purposes of MIG eligibility. PAS should be clearly identifiable in Waivers to count towards Indiana s MIG eligibility. Currently, it is disguised in other service definitions (such as Residential Habilitation and Supports). Indiana has five Waivers that include PAS related services under other service definitions; however, these services are not specified as PAS in each of the Waivers. The following table describes how PAS is provided under various service definitions through each of the Waivers
53 HCBS Waivers Developmental Disabilities Waiver established 2001 (formerly ICF/MR Waiver) -- established in 1992 Support Services for People with Developmental Disabilities Waiver -- established in 2002 Autism Waiver -- established in 1990 Table 2 Personal Assistance Service and Indiana HCBS Waivers Aged & Disabled Waiver -- established in 1990 Assisted Living Waiver -- established in 2000 Medically Fragile Children (under 18 years of age) Waiver -- established in 1992 Traumatic Brain Injury Waiver -- established in 2000 Serious Emotional Disturbance Waiver -- established in 2004 Personal Assistant Services in Any Community Setting Not specified in service listing Not specified in service listing Not specified in service listing Attendant services are specified By Definition, May Include Personal Assistance Services in Specified Settings Community Habilitation and Participation; Independence Assistance Services; Residential Habilitation and Support; Respite; Supported Employment Services Community Habilitation and Participation; Respite; Supported Employment Services Community Habilitation and Participation; Independence Assistance Services; Residential Habilitation and Support Services; Respite; Supported Employment Services Respite No listing of service No listing of service Attendant care is specified Personal care Is specified Not specified in service listing Respite Respite Respite Source: Bureau of Developmental Disabilities: Service Definitions and Standards Manual 2/22/
54 Prior to 2002 the Developmental Disabilities and Autism Waivers each listed Personal Assistance as an individual service. In 2002 FSSA consolidated the two distinct services of Personal Assistance and Residential-Based Habilitation into one service now called Residential Habilitation and Support Services. Through this consolidation of service types, providers were no longer required to differentiate between instruction/teaching and assisting a person with an activity. Beginning in 2002, providers that were approved to offer Personal Assistance and Residential Based Habilitation services were automatically approved to offer Residential Habilitation and Support Services. The Support Services Waiver though, has no such definition for Personal Assistance Services. This complex system of Waiver definitions presents challenges for case managers in ensuring they are accessing the supports individuals require for their particular needs. In 2002 FSSA also replaced the services identified as Day Individual Habilitation and Day Group Habilitation. Community Habilitation and Participation replaced these two services. Providers must still differentiate between teaching and assisting an individual with habilitation services. In addition, FSSA provides an enhanced rate for community services that are provided for the individual outside of the traditional congregate day services paradigm. This rate, however, is still lower than the rate that providers can reap from providing facility-based services. 19 The consolidation of personal assistance services with other services that include instruction was intended to ensure individuals have access to personal assistance services. However, it has likewise resulted in the inability to distinguish between these different types of services in the Medicaid Waiver data on service usage and associated expenditures. 19 The DD Waiver Bulletin 18 explains the enhanced rate structure effective June 27, 2002 and can be found on the FSSA website at The community staff to client ratio is 1:4 and the facility staff to client ratio is 1:
55 The three Waivers that are available to serve people with developmental disabilities (Developmental Disabilities, Autism, and Support Services Waivers) do not include personal assistance services individually. Further, the Support Services Waiver has no service definitions that allow assistance on a job. Although FSSA consolidated the provision of personal assistance services with instructional services for the Waivers serving people with developmental disabilities, the Aged and Disabled, Medically Fragile Children and Traumatic Brain Injury Waivers have maintained personal assistance services or attendant care as a specified service. These changes have implications for Indiana s full eligibility for Medicaid Infrastructure Grant funds if Indiana chooses to continue offering Personal Assistance Services (PAS) only through its Waivers and does not consider offering PAS under a State Plan Amendment. The CMS Eligibility Pre-Determination Checklist, for the Medicaid Infrastructure Grant notes that if PAS is offered under home health or through other names such as day habilitation rather than as an individual service, the Waiver is not counted in an eligibility assessment. Personal assistance services must be included individually in the service definitions and only those Waivers that serve people with disabilities who are non-elderly adults (ages years old) are able to be counted within the eligibility assessment. Waivers that serve only children or the elderly are also excluded in the assessment for MIG eligibility (Salley, 2005). It appears that under the Waivers as currently defined, there is an absence of clearly identifiable PAS services available in the home, community or workplace. C. Other Indiana Programs Funding Personal Assistance Services While at the current time it appears that PAS is not clearly identifiable in the Waivers (although they may be provided in limited ways under other service definitions) there are some opportunities to access PAS services through other avenues and programs. Two areas explored include the Community and Home
56 Options to Institutional Care for the Elderly and Disabled (CHOICE) Program and the PAS services offered through Indiana s Vocational Rehabilitation Services. 20 CHOICE is a state funded program within the Division of Aging (formerly known as the Bureau of Aging and In-Home Services) that provides support to both people with disabilities across the lifespan and the elderly. Services such as personal assistance and respite are offered and may be provided outside of the home. There is a waiting list for services. This program is housed within regional Area Agencies on Aging. Beginning in July of 2003, Indiana was mandated by the state legislature to provide Personal Assistance Services under the CHOICE programs through Senate Enrolled Act A concept that would enhance the provision of SEA 493 to shift Medicaid funding from institutions to community-based care is known as Money Follows the Person (MFP), and is intended to rebalance Medicaid funds. Funding follows the person from the institution to the most appropriate and preferred community setting. Through MFP initiatives, people receiving services determine how resources are allocated as they move through service systems (Crisp, Eiken, Gerst & Justice, 2003). The Indiana Office of Vocational Rehabilitation Services (VRS) provides PAS services as needed to individuals as they are participating in a vocational rehabilitation program, according to services identified in the Individual Employment Plan. These services may be used inside and outside the home for employment-related supports. In 2003 PAS services equaled 1.15% of the total 20 Vocational Rehabilitation Services (VRS) are time-limited and require providers to identify funding for follow-along or ongoing support services after job stabilization and successful rehabilitation (case closure of VRS). The Office of Vocational Rehabilitation is developing a white paper as of June 2005 to address the capping of follow-along services at 10 hours per month under HCBS Waivers. The Office of Vocational Rehabilitation is drafting recommendations to address the inadequacy of limiting follow-along funding under the HCBS Waiver system. 21 Senate Enrolled Act 493 was passed by the Indiana General Assembly in 2003 to ensure that Medicaid funds follow an individual who is transferring from institutional care to home and community-based care
57 VRS expenditures; and in 2004, PAS services equaled 1.01% of the total VRS expenditures. This information may be useful in determining if adding PAS services under the Waiver for employment services or through a Medicaid State Plan Amendment is financially feasible. D. Adequacy of Personal Assistance Services to Support Employment of People with Disabilities in the Workforce Since 1998, Indiana has gradually diverted individuals from institutional care into community-based services and has used Waiver funding to simultaneously expand the availability of community services and related supports. In two state developmental centers were closed (New Castle and Northern Indiana State Developmental Center). Since that time, there have been reductions in the number of people living in the two remaining state developmental centers, and in April 2005, one of those facilities (Muscatatuck State Developmental Center) closed. Fort Wayne Developmental Center, the one remaining center for people with developmental disabilities, is continuing to steadily reduce the number of people who live in the facility. In addition to the closure of the state developmental centers, two units for people with developmental disabilities in state mental health hospitals, and three large private Intermediate Care Facilities for the Mentally Retarded closed. Braddock and Hemp (2004) reported that between 2000 and 2004 the combined public and private institutional census dropped by 28%. In fiscal year 2004 the Indiana institutional utilization rate of 9 per 100,000 of the general population fell below the projected U.S. rate of 10 per 100,000. While these developments in transition to home and community-based services are remarkable, Indiana continues to have waiting lists for individuals seeking funding for home and community-based services. The lack of funding for
58 community-based services may consequently lead to a crisis situation for Indiana in supporting individuals living in the community. 1. Adequacy of Home and Community-Based Waiver Services According to the Family and Social Services Administration Indiana serves over 14,000 individuals through the Aged and Disabled, Assisted Living, Autism, Medically Fragile Children, Traumatic Brain Injury, Developmental Disability and Support Services Waivers. It is estimated 20,000 applicants are waiting for Home and Community-based Waivers in State Fiscal Year Appendix B outlines the number of individuals served by Indiana s Medicaid Waivers and expenditures through In September 2004 a settlement was reached on a lawsuit that alleged that the Indiana Family and Social Services Administration had violated Title II of the Americans with Disabilities Act and Section 504 of the Rehabilitation Act by failing to serve individuals in the most integrated setting ; violated the Medicaid Act by failing to provide nursing facility residents with developmental disabilities a choice between living in a facility and living in the community with HCBS Waiver supports; and, failing to provide Home and Community-Based Services within a reasonable amount of time. As a result of the settlement, Indiana is to expand its capacity to provide Waiver services; designate Waiver slots based on the number of Medicaid recipients in nursing facilities within the eight Bureau of Developmental Disabilities Services districts; and, reduce (and if possible eliminate) waiting time for HCBS services for people with developmental disabilities residing in nursing facilities. 22 The estimate is provided in the Division of Disability, Aging and Rehabilitative Services monthly management report, for the Indiana Fact Sheet, for State Fiscal Year The estimate represents a duplicated count of Waiver recipients on waiting lists, as some individuals may be on more than one waiting list. The ARC of Indiana reports an unduplicated count of over 15,500 individuals on Waiver waiting lists
59 More specifically, Krauss v. Hamilton resulted in the state agreeing to fund 450 additional Waiver slots, by The timeline for the expansion of Waivers is listed below: 50 Waiver slots by end of State Fiscal Year 2003; 50 Waiver slots by end of State Fiscal Year 2004; 50 Waiver slots by end of State fiscal Year 2005; 100 Waiver slots by end of State Fiscal Year 2006; 100 Waiver slots by end of State Fiscal Year 2007; and 100 Waiver slots by end of State Fiscal Year 2008 (Bureau of Developmental Disabilities Services, 2004). While the above settlement adds 450 Waiver slots, for Indiana to be eligible for full MIG funding the Centers for Medicare and Medicaid Services (CMS) requires reasonable evidence that Waivers have the capacity to serve at least 51% of the population of individuals with disabilities who wish to be employed. Additionally, to be fully eligible for Medicaid Infrastructure Grant Funding, a state must have criteria for reviewing and responding to requests from qualified employed individuals who use Personal Assistance Services (PAS) and are competitively employed. CMS encourages states to provide enough PAS services to workers both during the day and night, seven days per week, based on their need. A third criteria of CMS is that unless an individual needs only assistance with Activities of Daily Living (ADL s), medical necessity must not preclude the availability of PAS for Instrumental Activities of Daily Living (IADL s) if this assistance is required for individuals to be employed. In reviewing how PAS is provided under Indiana s Waiver service definitions, it is not clear as to how PAS is available to support the employment goals of people with disabilities. To access full eligibility for MIG funding, Indiana should develop a mechanism to review the access to PAS services and how much PAS is used to support employment goals
60 2. Adequacy of Personal Assistance Services Providers Providers of HCBS are approved through the Bureau of Aging and In-Home services. Title 460 of the Division of Disability, Aging and Rehabilitation Services Final Rule, Legislative Services Agency Document #03-245(F) requires agencies to acquire approval to provide attendant care. This rule appears to apply generally to qualifications for providers of HCBS services. Indiana has specific training or certification requirements for Personal Care Attendants, as outlined in Title 460 IAC which pertains to training requirements. These requirements include protection of the individual s rights; training on how to carry out individual s goals; and, providing a healthy and safe environment, including diet and nutrition, behavior management, seizure management, crisis management and medication assistance, first aid, cardiopulmonary resuscitation, infection control, universal precautions, and health concerns. The requirements as outlined in Title 460 IAC are listed below: For providers of PAS services, attendants must: (1) Be at least eighteen (18) years of age. (2) Demonstrate the ability to communicate adequately in order to: (A) complete required forms and reports of visits; and (B) follow oral or written instructions. (3) Demonstrate the ability to provide services according to the individual s Individualized Support Plan (ISP). (4) Demonstrate willingness to accept supervision. (5) Demonstrate an interest in and empathy for individuals. There are stringent competency and skill requirements for Personal Care Attendants as well as Home Health Service aids. While a registry of Indiana Home Health Aids is available through the Indiana State Department of Health, there is no official registry for Personal Care Attendants, even though PAS services are often similar and require the same types of services as Home Health Services. Title
61 indicates direct support professionals must be compassionate, ethical people who understand the support needs of individuals with disabilities and/or their family members. Indiana currently requires minimal formal education for attendants other than meeting the training requirements described above. To improve the quality of direct support professionals providing support to individuals with disabilities, the Division of Disability Aging and Rehabilitative Services (DDARS) has collaborated with state partners and the Indiana Institute on Disability and Community to develop the Indiana Statewide Training and Education Planning Group (ISETPG). ISETPG is a collaboration of disability related state and local service and advocacy organizations working with DDARS, the Department of Workforce Development, Ivy Tech Community Colleges and the Indiana Institute on Disability and Community to develop the statewide availability of innovative, best practices educational opportunities for the workforce supporting people with disabilities to live and work in the community. Through ISETPG Indiana hopes to build the capacity of direct service providers, reduce turnover and build professionalism in direct support professionals (DD InfoSOURCE, 2005). ISETPG is another option to ensure Personal Care Attendants have adequate training on supporting individuals with disabilities. Providers of HCBS services are responsible for hiring, training and managing staff that provide direct care services to individuals. The only exception to this process is through the Consumer-Directed Control Pilot program within the Aged and Disabled Waiver that is available to Choice participants. In this case, individuals may hire and manage their own attendants. Under these programs, individuals have a fiscal intermediary to assist with directing the fiscal process of their care. At the current time, individuals are given a choice of provider agencies that are approved to provide PAS services. Individuals on Waivers are required to have a Person Centered Plan developed, a Developmental Disability Profile (if applicable), a Plan of Care/Individual Service Plan and a Cost Comparison Budget
62 Indiana has made extensive efforts to ensure that case managers and providers are trained in Person Centered-Planning processes and other aspects of providing quality services (e.g., initiating services in a prompt and timely manner, providing services that are responsive to individuals changing needs, and gathering input from consumers pertaining to satisfaction with services and effectiveness of services). Although Person-Centered Planning is to guide the services, often the structure of rates and cost containment measures make it challenging to fulfill the elements of the Person-Centered Plan. Case managers interviewed for this assessment indicated a number of concerns with the current structure of Indiana s HCBS Waivers and they report they have presented their concerns and recommendations to the Family and Social Services Administration. 23 In addition to training issues mentioned above, providers and organizations have noted that since reimbursement rates for PAS-related services are low, attendants are paid lower wages than other workers. Keeping experienced attendants is difficult as many attendants leave to work at jobs that provide benefits and better wages per hour such as fast food restaurants and factories. Larson & Hewitt (2005) indicate turnover rates in residential and vocational organizations average 52% nationally. High staff turnover is also reported in Indiana by the providers interviewed for this assessment. Often attendants leave agencies to find jobs with adequate health insurance benefits. While some provider agencies provide shift differentials for individuals needing attendant care, there is generally a 23 In a briefing paper developed by the Indiana Chapter of Professional Case managers, several concerns were indicated that affect the quality of the Waiver case management system: Frequent changes in leadership at both DDARS and BDDS has resulted in continual changes in policies, and procedures, and lack of vision ; Policy changes have been made based on hearsay versus data and fact; No centralized location exists where a case manager can find the answers to procedural questions; Certification guidelines to become a case manager are much too broad; Communication from state personnel to case managers is inconsistent; Emphasis is on process and procedural compliance versus quality of life; and Pertinent, up-to-date training is sorely lacking. The briefing paper was developed and updated in February 2004 and presented to the Family and Social Services Administration
63 lack of attendant care when needed (such as early morning hours or late in the evening). Turnover results in barriers to continuity of support in individuals lives, including community living and employment supports. At the current time, personal care attendants are most likely employed by a provider agency approved by the state. Some questions arise as to how Indiana law addresses worker s compensation for attendants who are not employed by an agency. Worker s Compensation is, in general, a strict-liability, fixed recovery system that is the exclusive recovery mechanism for an individual hurt during the course of, and in the scope of, employment. The benefits of the system are that the costs of litigation are relatively low and the financial implication of an injury is relatively easy to determine because the recovery ability of an injured employee is limited by statute. Indiana is like a large number of other states in that it is unclear who if anyone, is responsible for workers compensation coverage for a worker providing services in the home of an individual (Indiana Code sections through section ). Like many states, Indiana lacks a clear definition regarding which job duties or classifications require an individual to be classified as a household employee for Worker s Compensation purposes (Flannigan 2004). Given the lack of definitions in the Indiana code, it is extremely difficult to determine if a Personal Assistance Service (PAS) worker would be considered an employee who was required to be covered under the Indiana Worker s Compensation Act. In the 2005 General Assembly, Senate Enrolled Act 206 addresses workers compensation by requiring provider agencies that employ personal care attendants to furnish liability insurance for those attendants. This law is pertinent if attendants providing services are not considered to be employees of the individual, but are considered employed by an agency providing services. In general, responsibility for providing worker s compensation is determined by who has the most control in
64 directing the care for the individual. Individuals might be considered an employer of the attendant if: They have a high amount of control over the services provided by the attendant; and The PAS attendant works 40 hours a week for the individual; the individual sets the hours of work; the individual has the ability to completely discharge the worker; the individual writes a paycheck to the worker; and the PAS attendant is placed in individual s home for extended period of time. Agencies would most likely to be considered the employer of the attendant for worker s compensation purposes if: The PAS worker works in multiple people s homes in a work week; The PAS worker s conduct and work location is prescribed by an agreement with the agency; The PAS worker receives a paycheck/fringe benefits from the agency, If a disagreement occurs between an individual and the PAS worker, the agency has the ability to ensure the PAS worker of continued employment; and A third party provides supplies for PAS workers to complete their duties. In regards to consumer-directed care, if the consumer is given the funds directly by Medicaid to pay the salary of the PAS attendant and the consumer (or a representative of the consumer) hired a PAS attendant and paid the worker s weekly wages, it is likely that the PAS attendant would be considered an employee of the consumer. The consumer would then be responsible for payment of worker s compensation insurance coverage for the PAS worker. Whether this has been addressed in Indiana s Consumer-Directed Services pilot is unknown. To protect the needs of individuals receiving PAS, Indiana should carefully address issues with workers compensation for PAS attendants who may be employed by an individual
65 needing attendant care, or individuals who may use attendants for employmentrelated services outside the home and at the workplace. One final area that addresses the adequacy of PAS in the workplace is employer accommodations. Through the MIG grant activities, Indiana has collaborated with the Indiana Department of Workforce Development, Division of Mental Health and Addictions and the Office of Vocational Rehabilitation Services to find ways to engage the business community in supporting employment efforts of individuals with disabilities. Though this endeavor, Indiana will continue to address barriers to employment, opportunities for people with disabilities to work with reasonable accommodations and employer supports. E. Policy Development and Performance Monitoring Many of Indiana s current initiatives and policies are a reflection of the six policy directives outlined in Indiana s Olmstead Comprehensive Plan. The six policy directives include: Emphasize consumer choice; Provide information, assistance and access to consumers to increase their opportunities for informed choice; Support the informal network of families, friends, neighbors, and communities Strengthen quality assurance, monitoring systems, complaint system, and advocacy efforts; Increase the system capacity for provision of high quality care; Create a coordinated workforce development system that recruits and supports a stable resource of direct support staff. Progress toward action items in the Olmstead Plan has been evaluated in this assessment. These issues include: adding additional Waiver slots to support individuals with disabilities in the community; addressing waiting lists for Medicaid Waivers; piloting consumer-directed personal assistance; increasing training options
66 for providers; expanding an ombudsman program; and developing quality improvement systems for services provided to individuals with developmental disabilities. One of the recommendations of Indiana s Olmstead Comprehensive Plan was to strengthen quality assurance and improvement systems. The Division of Disability and Rehabilitative Services (DDRS) has a number of ways to assure that individuals are receiving quality services. Quality assurance is measured through mechanisms established within the Bureaus of Developmental Disabilities Services, Aging and In-Home Services and Quality Improvement Services. A variety of quality assurance activities are used within the Medicaid Waiver system. Indiana s key Waiver quality approaches are administered by Bureau of Quality Improvement Services (BQIS) and the Area Agencies on Aging (AAA) as part of their contract with the state. These include the following: An Electronic Data Systems (EDS) review of providers of Waiver services. EDS serves as the fiscal agent for the Medicaid Waivers. EDS submits any issues identified to BQIS for follow up. Case managers are required to meet with individuals every 90 days. Some of these visits are to be in an individual s home and some may be an unannounced visit. The AAA s are responsible for the administration of Waiver programs and are required to monitor program performance and quality. Specifically, AAA s are required to conduct client satisfaction surveys for 5-10 percent of all Waiver participants. BQIS manages the Waiver complaints and conducts regular surveys of all services and standards pertaining to the Waivers. The Developmental Disabilities Waiver includes an Ombudsman who is charged with receiving and investigating complaints and charged with resolving complaints and concerns on behalf of individuals served
67 The Waiver Services Unit receives monthly reports on diversion of individuals from facility based care and the progress of individuals transitioned from facilities and institutions. As the Indiana Medicaid agency, the Office of Medicaid Policy & Planning (OMPP) is responsible for administering the hearings and appeals processes for Medicaid participants, including those who have access to Waiver services. Provider agencies are required to participate in surveys provided by the Commission on Accreditation for Rehabilitation Facilities (CARF) or a similar national accrediting organization that review quality services for people with disabilities. To augment quality improvement, Indiana has engaged in developing processes for quality assurance and improvement that involve the active participation of individuals with disabilities in the design and implementation of these programs. Two recent initiatives are described below. The Bureau of Quality Improvement Services (BQIS) has established numerous mechanisms for ensuring quality services are in place. These include: Guides for Developmental Disability Services; and Policies and processes on safety, incident reporting, individualized support planning, performance and outcome indicators, person-centered planning guidelines, provider standards, policies and procedures for transition to community services, and other reporting processes, and a variety of surveys to assess quality of the HCBS services. Through funding from the Robert Wood Johnson Foundation, Indiana has initiated a Quality Improvement Process (QIP) to ensure the health and welfare of HCBS Waiver participants who have disabilities or are elderly. This process includes an automated program participant feedback survey that is administered in person to program participants and measures satisfaction with services provided
68 under the Waivers, case management supports, and provider agency supports. Development of the Quality Improvement Process involved participation from individuals with disabilities, state agency officials, Area Agencies on Aging, case managers and service providers. The information from the QIP provides data participant responses that are useful for the Bureau of Aging and In-Home Services as well as providers and program participants (Indiana s Quality Improvement Process, 2003). Indiana also has funding from CMS to design a Quality Assurance/Quality Improvement system (QA/QI) for HCBS Waivers. This program is developing mechanisms to obtain participant input on the quality of services; creating consistent standards for service providers to abide; by instituting uniform policies and procedures for state agencies and contractors who provide services; and, developing information technology and data collection tools to review trends, make recommendations, implement processes, and reevaluate the effectiveness of systems. Individuals with disabilities are involved with this initiative along with the Indiana Home Care Task Force. III. SURVEY OF OTHER STATE S STRATEGIES TO MEET MEDICAID INFRASTRUCTURE GRANT FULL ELIGIBILITY CRITERIA To obtain full eligibility for Medicaid Infrastructure Grant funding a state must have Personal Assistance Services (PAS) that are clearly identifiable in their Medicaid State Plan, or through Home and Community-Based Services Waivers, or a combination of both a State Plan Amendment and Waiver amendments. Indiana, like other states, must address how to achieve these MIG criteria in a cost-effective manner. Some states have developed or enhanced existing PAS programs through a State Plan Service. Other states have instead developed new Waivers or made changes to their existing Waivers. Federal Waiver programs that provide PAS
69 include the 1915(c) Waivers, which cover personal attendant care services; the 1915(b) Freedom of Choice Waivers, and the 1115 Research and Demonstration Waivers to develop pilot or demonstration projects. A. State Programs Providing Personal Assistance Services Options to Support Employment Several states have various initiatives to address limitations in their PAS programs. PAS program descriptions for the states of Maine, Utah, Kansas and Minnesota are described in this section. The information pertains to the eligibility criteria for consumers as well as definitions of covered services under the PAS program (or similar services). Maine s Consumer-Directed Personal Care Attendant Program Maine s Medicaid program is called Maine Care. In 2000, Maine s Medicaid Infrastructure Grant called Maine CHOICES (Continued Health Options and Incentives via Coordinated Employment Supports) conducted a qualitative study to assess Medicaid participant preferences in consumer-directed independent living and the home health medical model of services. Overall, participants preferred the consumer-directed personal care program which allows PAS services in the home, away from the home and at the workplace (Gray & Glantz, 2003). Maine offers a Waiver program for current Medicaid recipients who want to access Consumer-Directed Personal Care Assistance. The consumer applying must have a valid Community Medicaid card and be deemed medically eligible for nursing facility services and cognitively capable of hiring, directing, training, supervising and firing their Personal Care Attendant (PCA). Through this program, consumers have control and responsibility in employing their PCA including arranging schedules. Additionally, under this program consumers have responsibility for:
70 (a) Hiring, training, supervision, and termination of the PCA or directing the Authorized Agent in selection, supervision and termination of a PCA; (b) Establishing work schedules; (c) Carrying out the plan of service as it relates to the PCA and using the PCA responsibly; (d) Unemployment and workers compensation insurance, unless the consumer has chosen to have this carried out by an Authorized Agent (AA); and (e) Maintaining records, which comply with Maine State employment laws. The Authorized Agent who administers the consumer directed programs completes an assessment and the authorized plan of care. Services cannot begin until the consumer has successfully completed skills training and hired a personal care attendant. The assessment will then be converted and plan of care authorized, giving 90-day eligibility from date of original assessment. Covered services include Activities of Daily Living (ADL s) and Instrumental Activities of Daily Living (IADL s) and/or health maintenance activities, which are directly related to the consumer s plan of care. These tasks must be performed in conjunction with direct care to the consumer. IADL's and health maintenance activities are those activities that would otherwise be normally performed by the consumer if he or she were physically able to do so. It must also be established that there is no family member or other person available to assist with these tasks. These services must be authorized and specified in an individual s plan of care. IADL s have limits per level of eligibility, based on hours of services and level of care. These hours of services range from two hours of PAS to four hours of PAS to per week. Utah s Employment-Related Personal Assistance Program Under Utah s Medicaid State Plan, Employment-Related Personal Assistance (E-PAS) is personal assistance for people with disabilities on Medicaid who are working and, because of their disability, need personal assistance to work. E-PAS
71 services are covered benefits provided to support integrated and competitive employment opportunities for individuals with moderate to severe levels of disabilities. The E-PAS Program is designed to provide personal assistance for people who may have physical, mental, cognitive, and/or developmental disabilities and are working in integrated employment settings. The assistance provided is for tasks directly related to maintaining employment. The EPAS Program strives for a consumer-directed system that allows for a person to have a range of provider options. An individual may choose between a licensed Home Health Agency from a state list of approved providers, or a qualified person hired by the E-PAS Participant. Under this model, E-PAS participants can choose to take on the responsibility of being an Employer. They have the opportunity to find their own employees, screen applicants, check references and select someone to hire. As an employer, they can choose what to pay their employee as long as it is in the range determined by the E-PAS Program. Under this model they will choose a fiscal employer agent that will complete the usual Federal and state tax forms and collect and disburse employment taxes and payroll on their behalf. Under the E-PAS Option, an individual with disabilities must meet the following requirements: 1. Have a job, or job offer; 2. Be working at least 40 hours a month, or 10 hours a week; 3. Have a disability, as defined by the Social Security Administration or by the Utah Medicaid Office; 4. Be or become a Medicaid recipient; and 5. Need assistance with daily living activities to maintain a job. Activities of Daily Living (ADL s) and Instrumental Activities of Daily Living (IADL s) are covered under the E-PAS model. E-PAS may not be used for assistance related to completing job tasks including job coaching, job training, or as a reasonable accommodation that an employer is required to provided under the
72 Americans with Disabilities Act (Utah Employment-Related Personal Assistance Program, 2005). Kansas Independence Plus Waiver Initiative The state of Kansas is submitting an 1115 Independence Plus demonstration Waiver entitled WORK (Work Opportunities Rewards Kansas). This demonstration Waiver is for individuals eligible or on waiting lists for the Developmental Disability, Head Injury, Physical Disability or Serious Emotionally Disturbed Waivers who are employed 40 hours per month in a competitive, integrated setting. Services include Personal Attendant Services, Assistive Services and Supports Brokerage. Minnesota s Personal Care Assistance Available under the State Plan and through Waivers Minnesota s Personal Care Assistance (PCA) services are available in four broad categories, including Activities of Daily Living, Instrumental Activities of Daily Living, Health-Related Functions and Redirection and intervention for Behavior. Individuals have flexibility to use allocated authorized units of service to meet their needs and schedules for medically necessary covered services as specified in their individualized assessment. There are clear definitions of flexible use of services, namely: Flexible use does not increase the total amount of authorized units available; The person or responsible party, together with the provider, must work to monitor and document the use of authorized units and ensure that a person is able to manage services effectively throughout the authorized period; When requested by the person or responsible party, the provider must furnish regular updates on the amount of PCA units used; Additional PCA units will not be authorized to supplement a service authorization exhausted before the end date, unless the county public health
73 nurse determines a change in condition and establishes a need for increased services. Individuals may use their PCA services anywhere including work, shopping, medical appointments, worship services, school or any place in the community. A person may be accompanied by their PCA to community activities if the community activities are documented in the service plan. PCA reimbursement is the authorized units of time as per the assessment process. PCA s may provide assistance to individuals at their work site. They may provide any assistance identified in the care plan. Individuals have the following choices for getting personal care assistance at work: Individuals may schedule a PCA to come in to their workplace at the times they need help, or Individuals may find someone employed at their workplace that is willing to be hired as a PCA for them. This program clearly delineates what is PCA and what is an employer s responsibility under the ADA to provide accommodations to individuals in the workplace. B. Other Options for Increasing Community-Based Services Many states have made great strides in downsizing institutional services and increasing community-based services. Indiana is one of those states, and continues to transition individuals to the community. However, Medicaid spending on nursing facilities and Intermediate Care Facilities for the Mentally Retarded (ICF/MR) facilities remains high in Indiana compared to other states. Likewise, spending on home and community-based services is lower than other states in the nation (Gibson, Gregory, Houser & Fox-Grage 2004). The Lewin Group (2004) reports that Indiana s proportion of long-term care expenditures in the community was
74 significantly lower than other states, with Indiana spending only 16% of it s funds for long-term care on HCBS services and 84% on institutional care. Indiana could concurrently reduce its nursing home capacity and simultaneously increase its Home and Community-Based Services capacity. This process is known as rebalancing, and could result in significant savings over the upcoming years. Strategies for rebalancing may include: Legislative actions to mandate reducing the growth in nursing facility expenditures; downsizing facilities and diverting savings to the HCBS services; Implementing self-directed services, more consumer supports, timely information and involvement of individuals with disabilities and their families and participating in Independence Plus initiatives and; Building connections between funding streams, such as establishing local access points for all long-term supports or merging administrative and regulatory responsibilities at the state and local levels. (Crisp, Eiken, Gerst, & Justice, 2003). The Centers for Medicare and Medicaid Services (CMS) offers Money Follows the Person (MFP) grants to help states reform the financing of long-term care systems. Through a system of money following the person, a package of State Plan and HCBS Waiver services is available to individuals to allow funding to be tailored to the individual s needs and preferences in the most appropriate setting. As the individual s needs and preferences change, funds move and shift to support his or her needs. For example, an individual who moves from a day program into community-based employment needs fewer services to support day activities and more services to support employment-related activities. Through MFP and a flexible budget, resources are allocated for that individual to easily flex to support the individual in his or her job without restrictions on hourly caps and other rate limitations. Through this method, the funding is truly paying for services identified in
75 the Person-Centered Plan. States currently participating in MFP grants from CMS include California, Idaho, Maine, Michigan, Nevada, Pennsylvania, Texas, West Virginia, and Wyoming. Indiana currently does not have a system in place known as Money Follows the Person; however, an Indiana task force known as MATRIX is evaluating how funding is allocated and managed for Waiver recipients to support individuals in a flexible manner outside of rates and cost caps. The MATRIX Task Force through the Division of Disability and Rehabilitative Services is discussing the idea of individuals on HCBS Waivers having a needs assessment using a standard scoring tool. Based on the needs assessment, individuals will be allocated personal budgets or funding levels depending on their community-based needs. In exploring flexible funding and individual resource allocation, it is essential to consider some important issues such as: individuals conducting individual assessments need extensive training on using a scoring tool; assessments should consider the environment and other external factors that will affect an individual s functioning in the community; individuals needs change over time, so funding should adjust to their needs; individual budgets should be flexible because an individual s use of services may fluctuate, requiring extra services in some months and not as much in other months. Funding should support the changing needs of individuals in a flexible manner. IV. RECOMMENDATIONS FOR INDIANA S SUPPORT OF PEOPLE WITH DISABILITIES IN THE WORKFORCE Indiana s Family and Social Services Administration must assess its strengths and weaknesses in providing community-based services and employment services for people with disabilities. It must also explore Federal opportunities that will help to change the service system and promote community living and employment. Lack of
76 clearly identifiable Personal Assistance Services in the Home and Community- Based Waivers are only one of the barriers to employment for people with disabilities. Indiana s Family and Social Services Administration needs to survey all of its agencies to identify strengths and where barriers to effectiveness exist. A. Recommendations Relative to Home and Community Based Services and Personal Assistance Services Indiana s Home and Community-Based Waiver services are extremely complex, with various allowable services, rates of services, cost-containment, and policies that appear to change frequently. Adding to this complexity is the existence of different entry points for Waiver services (either through the Bureau of Developmental Disability Services or the Area Agency on Aging), and a separate Medicaid financial eligibility determination through the Division of Family Resources. It is difficult to ascertain how many individuals are actually waiting for Waiver services, as state data shows duplicated counts and individuals are encouraged to apply for more than one Waiver. Individuals and family members interviewed for this assessment indicated the current system is not customer-friendly in that once eligible for Waiver services, the funding system is not flexible to meet their unique needs, and individuals and families are subject to regular audits from a number of entities concerned with quality assurance issues. While Person-Centered Planning is identified as a priority in the state s waiver programs, carrying out the Person-Centered Plan is difficult because of numerous restrictions on allowable services and units of care. There appears to be little flexibility to account for changes in support needs and budgeting for these needs from month to month (such as carrying over unused units of service for future months if needed). Caps on specific services (for example Supported Employment Follow-Along) do not allow for flexibility in individual supports
77 Indiana and most states are experiencing difficulties in providing sufficient Home and Community-Based Services that do not burden the state Medicaid system. CMS is shifting from a medical model of supports toward community-based rehabilitation models, and is offering several initiatives for states to provide services in a flexible, yet cost-effective manner (such as Consumer-Directed Care or Money Follows the Person initiatives). To address the shifts in CMS policies, state Medicaid budgets must be rebalanced to move from a medical model to communitybased supports and services. Discussions are occurring within FSSA and other groups (such as the Community Personal Assistance Services and Supports (C-PASS) Task Force) about initiatives such as Consumer-Directed Care. Indiana is exploring whether to apply for a Waiver to provide Consumer-Directed Home Care or to amend existing Waivers to add this service. 24 Per CMS requirements for Medicaid Infrastructure Grant Funding, Indiana must have Personal Assistance Services available for working individuals inside and outside the home at least 40 hours per week, and CMS must be able to clearly identify PAS in the Medicaid State Plan or Waivers. Personal Assistance Services are currently couched under other service definitions under the HCBS Waivers, and are not available as a State Plan option. According to data provided by the Office of Medicaid Policy and Planning Data Management Analysis, the state expenditures for PAS for waiver enrollees were relatively low compared to the total Medicaid expenditures and Waiver expenditures for waiver enrollees. In the calendar year 2002, there were a total of 7,036 individuals enrolled in the Home and Community-Based Waiver programs who were between the ages of Of those individuals, 7,005 individuals received some kind of Medicaid services and 6,760 individuals received Waiver services. For 24 C-PASS is a Task Force working with the Consumer Personal Assistance and Supports Services Grant from CMS. This group met on June 14, 2005 and is taking steps to achieve implementation of the Consumer- Directed Home Care Option for Medicaid Waivers
78 these individuals their total Medicaid expenditures in calendar year 2002 were $250.9 million. The Waiver expenditures for this group were $190.9 million. Of these Waiver expenditures, 16.4% of the expenditures were for Personal Assistance Services, or a total of $31.4 million. Just 37.4% of the Waiver recipients actually received PAS services. Of those that did receive PAS, the average expenditure per enrollee per year was $12,410. In calendar years 2003 and 2004, Personal Assistance Expenditures were 3.2% each year. This may be explained by the rate structure change that occurred after The individual PAS rate was consolidated with other services, to ensure that individuals have access to PAS and providers would not have to differentiate between teaching someone and assisting someone with an activity. While this change was approved by CMS it is questionable whether PAS is clearly identifiable as defined at the current time. Appendix C illustrates the expenditures for PAS services for waiver recipients ages for calendar years 2002, 2003 and There are a number of alternatives available to Indiana in addressing the issues with the Waiver system as it currently exists. There are several options to strengthen the availability of Personal Assistance Services to support people with disabilities in the workplace, and provide this in a cost effective manner. Recommendations: The state should explore how to reduce administrative costs of services. This may be achieved by having one centralized access point for Waivers in local communities, and one centralized state management point for the various Waivers. Indiana s current Waiver rates and services should be simplified. Indiana should research best practices of other states in funding person-centered, community-based services and evaluate what practices would be practical and fiscally possible in Indiana. These practices may include adjustments for
79 flexible hours of service or changes in services and rate structures that allow services to follow the Person-Centered Plan. For example, Indiana could collapse rates and allocate a personal budget per individual Waiver recipient. Services and funding should be tailored to individual s support needs and should evolve along with individuals needs. Indiana should support moving ahead with efforts of the C-PASS task force and amend Waivers to add a Consumer-Directed Home Care Option. Indiana should reduce the number of individuals on waiting lists for HCBS Waivers. Indiana should encourage legislators to implement rebalancing of funds allocated to nursing facilities and re-direct funds into community-based services. Indiana should proceed with plans to add HCBS Waiver slots in to ensure that individuals with disabilities living in the community have access to services. 25 To achieve full Medicaid Infrastructure Grant eligibility and achieve CMS criteria for community-based employment services, Indiana must clearly identify PAS as a service offered to individuals in the home, community, or workplace as needed for a minimum of 40 hours per week. To achieve this, Indiana could do one or both of the following: 1. Add Personal Assistance Services to Indiana s State Medicaid Plan: Indiana can elect to provide PAS services under the Medicaid State Plan and add an enhanced PAS option to support employment (similar to Utah s Employment-Related Personal Assistance Program) and authorize hours and types of services for employment-related personal assistance. Through a state plan amendment individuals will have access to the needed personal assistance supports. Individuals who are working could access an enhanced Personal Assistance option for supports in the workplace as well as in their homes and communities. 25 According to an interview with Pat Cassanova of the Family and Social Services Administration, Indiana is planning on adding up to 1,000 Aged and Disabled Waiver slots in and revamping the Waiver system beginning in July
80 2. Modify the HCBS Waivers to include Personal Assistance Services as an individual service, as needed: Indiana can elect to offer PAS under a variety of Home and Community Based Waivers. This is not clearly indicated in the Waiver service definitions at the current time. A definition for PAS as an allowable service should be included in all Waivers. Indiana may want to add a workplace assistance PAS service definition. If so, Indiana should phase this service in under specific waivers (such as the Aged and Disabled Waiver, the Developmental Disability Waiver, and the Autism Waiver. Given the current service definitions under the Waivers it is difficult to ascertain how much PAS is actually provided. Indiana should ensure that PAS provided under the Waivers meets the CMS criteria for full eligibility (available 40 hours per week inside and outside the home) for Medicaid Infrastructure Grant funding. B. Recommendations Relative to Service Improvement and Service Initiatives Indiana now engages in an extensive process of quality assurance and quality improvement for individuals served through HCBS Waivers. However, training for PAS attendants to support individuals who are working would augment the quality of supports to those who need PAS. Under the New Freedom Initiative, CMS offers demonstration grants for improving the training for direct support professionals who provide PAS to people with disabilities. These grants are called Demonstration to Improve Direct Service Community Workforce and may be an opportunity for Indiana to implement a formal training program. Indiana has several CMS systems change grants (as outlined in Table 1) that improve the quality and availability of HCBS Waiver services and address capacity building for community based services and employment. While these grants have existed in Indiana for more than a year, there does not appear to be a formal coordinated effort among these CMS grants. Many of the goals and objectives of
81 the grants may intersect in improving community-based services. It may behoove state leaders to strategize between and among these funding opportunities and collaborate in their goals and objectives to address the waiting lists and develop options that promote continued diversion into community and employment opportunities. Indiana does not have a Money Follows the Person grant, but is exploring options through the MATRIX Task Force to develop flexible funding to support the changing needs of individuals. Recommendations: Work with entities to evaluate the training needs of PAS attendants and other direct-care staff based on quality improvement recommendations. Develop a formal process for grants coordination among the CMS grants to provide a unified system of community-based supports and planning. Continue exploring Money Follows the Person initiatives through the MATRIX Task Force. Explore flexible funding and personal budgets for individuals through applying for a Money Follows the Person Grant from CMS. C. Recommendations Relative to Employment Barriers In 2002, landmark legislation eliminated a significant Medicaid barrier to employment for people with disabilities and created the M.E.D. Works program. While M.E.D. Works has seen a steady increase in enrollment, it has also shown benefits in allowing individuals with disabilities, including those on Medicaid Waivers, to work. Because of the increase in M.E.D. Works recipients, the Indiana Office of Medicaid Policy and Planning began to explore ways to curtail the rapid growth of MED Works enrollees and the high Medicaid expenditures without causing detriment to individuals who were engaged in a reasonable and substantial work effort
82 According to a report developed by Mathematica Policy Research, Inc., (Ireys, White & Thornton 2003) in 2002 Indiana spent an average of $2,260 per month per Buy-In Participant. The average monthly earnings for these participants was $713, which was lower than Social Security s Substantial Gainful Activity level in MED Works participants are more likely to have developmental disabilities and this population has higher Medicaid expenditures and lower earnings (individuals earnings were less than the national average). Conversely, individuals with higher earnings had lower per member per month expenditures. 26 In a report developed by the Lewin Consulting Group in 2004), recommendations were made to implement an enhanced test to the M.E.D. Works program to tighten eligibility standards for members who were earning below $150% of the Federal poverty level. Because of the phenomenon of earnings compared to expenditures, OMPP proposed changes which were approved by the M.E.D. Works Advisory Council on August 18 th These changes include adding additional criteria for earned income in the countable income formula by fall of 2005, and proposing legislation to add premiums on a sliding fee scale for all M.E.D. Works members, including those below 150% of the Federal poverty level. These changes are predicted to enhance the incentive for participants to increase their earnings and level of self sufficiency. The Restrictions on Plan to Achieve Self Support in Indiana While the M.E.D. Works program continues to increase employment options for individuals with disabilities, (particularly those individuals who are beneficiaries of SSDI, or do not receive SSI), Indiana continues to impose barriers to employment through one of its policies that may be outdated since the implementation of the Ticket to Work and Work Incentives Improvement Act. This policy pertains to Indiana s disallowance for SSI recipients who are eligible for Medicaid Assistance for Disabilities (MA D) to access the Social Security Administration s Plan to Achieve 26 Presentation by the Office of Medicaid Policy and Planning to the M.E.D. Works Advisory Council August,
83 Self Support (PASS). This policy is also important to consider as a barrier for individuals needing Personal Assistance Services as it does not allow individuals to set aside excess resources to pay for personal care. The Social Security Administration (SSA) has a Federal provision in place to protect Medicaid for low income, disabled individuals who are Supplemental Security Income (SSI) recipients who are working. For the SSI program, individuals who are age 65 or older or are blind and have a disability that is expected to last for 12 months or result in death, who have countable resources below $2000 and have countable income below the Federal Benefit Rate ($ per month in 2005) are determined eligible for SSI. SSI s Medicaid work incentive, entitled Section 1619 (b)(3) of the Federal Social Security Act mandates states provide Medicaid coverage for working individuals who receive cash benefits through Supplemental Security Income and are no longer eligible for an SSI cash payment due to earnings. 27 Because of this provision, SSI recipients do not participate in the M.E.D. Works program, as Medicaid is available without having to pay a premium to continue Medicaid Coverage (as in M.E.D. Works). Indiana does not recognize PASS plans for Medicaid recipients in the MA D eligibility category. The PASS program is an SSI work incentive that allows people with disabilities to set aside income and/or resources to be used to achieve specific work goals, including covering the costs of obtaining an education, receiving vocational training, starting a business or purchasing support services. The Social Security Act authorizes income and resource exclusions that a recipient of cash benefits may have if he or she is blind or has a disability, when the income or resources are used to fulfill an approved PASS. The purpose of this work incentive is to enable individuals to work and thereby reduce or terminate cash benefits. For Supplemental Security Income, the excess income and resources an individual sets 27 According to the Social Security Act 42 U.S.C. 1382h The 1619(b), this provision allows SSI beneficiaries to work and continue Medicaid coverage even after their earned income makes them ineligible for SSI cash benefits until their income reaches a threshold. In Indiana, the 2005 Medicaid threshold for working recipients of SSI is $29,194 as indicated in the Social Security Administration s Policy Operations Manual System Section SI
84 aside in a PASS Plan will not be counted in determining the individual s eligibility or SSI payment amount. As noted, this Federal provision applies to individuals who are blind or have a disability. 28 Until 1996, the Federal guidelines for establishing a PASS plan were lenient. Unfortunately, the intent of the PASS in reducing or ceasing cash benefits was not the resulted goal. In April 1996, SSA revised guidelines for handling PASS applications and reviews to ensure proper use of the PASS work incentive. Effective December 1, 1997 PASS procedures were revised and clarified and policy changes were implemented, including: a thorough application for PASS plans; approval requirements; occupational goal requirements; milestones and interval steps; and, definable timeframes and accounting procedures to ensure that funds set aside were used to achieve vocational goals. These changes ultimately result in a reduction or cessation of public assistance. With the 1997 policy changes, the Social Security Administration developed a PASS cadre (experts for the program) to oversee the development of the PASS directly with the PASS applicant. The PASS cadre conducts progress checks and reviews PASS plans with beneficiaries who are using this work incentive. While the Social Security Administration made substantial changes to the program to ensure proper use of PASS and alleviate the detrimental consequence of added fiscal burdens to Federal and state assistance programs resulting from PASS misuse, Indiana Medicaid did not change its state policies to reflect the Federal improvements with the use of this work incentive. Indiana is a 209(b) state, meaning Indiana does not use the SSI standard for Medicaid Eligibility for SSI recipients (including counting income, disregarding income and establishing resource limits) The PASS program is legislated from the Social Security (Act as Amended in Section 1612(b)(4)(A) and (B), Section 1613(a)(4); Social Security Independence and Program Improvements Act of 1994 (Public Law )-Section 203). 29 The Social Security Act 42 U.S.C. sec. 1396a(f) allows 209(b) states to set standards that differ from Social Security s eligibility and determination of disability requirements. All states are required to provide protections against loss of Medicaid for persons who are eligible for Medicaid under their Medicaid eligibility criteria and when individuals begin work
85 For example, the Federal resource limit for the SSI program is $2000; Indiana s resource limit is $1500. Indiana s policies appear to interpret PASS plans and exemption of excess resources and income based on an interpretation that differs from Federal law, in that individuals who are eligible for Medicaid under certain categories of assistance qualify for PASS including Blind (MA B), Qualified Disabled worker (MA G), Qualified Medicare Beneficiaries (MA L), Specified Low Income Medicare Beneficiaries (MA J), and Qualified Individuals (MA I, MA K) categories of assistance. However, individuals who would most benefit from the Federal work incentive, those individuals who are eligible for Medicaid Assistance for the Disabled (MA D) category and SSI recipients (MA U) category of assistance are not eligible for the Federal PASS work incentive once their resources exceed Indiana s $1500 resource limit (Indiana Client Eligibility System ; Indiana Client Eligibility System Plan for Achieving Self-Support). Because of Indiana s rigid interpretation of the PASS program, Indiana has few PASS plans approved through the Social Security Administration in comparison to other states. Even with the Federal changes to the PASS program to ensure that it is used more appropriately and decreases or ceases reliance on public assistance, Indiana has not explored how this Social Security work incentive and thorough requirements for PASS development and process can benefit the state s Medicaid program. In comparison to states in the Social Security Region V (including Ohio, Illinois, Minnesota, Michigan, and Wisconsin), Indiana has substantially fewer PASS Plans applied for and approved than other sates. Indiana has 21 PASS Plans other states have between PASS plans approved as of June Indiana s policies on PASS programs were challenged in a class action lawsuit filed in the Southern District Court of Indiana. In Vaughn v. Sullivan, (83 F.3d 30 The Social Security PASS specialist for Region V provided information on status of PASS plans for Indiana, Illinois, Michigan, Minnesota, Ohio, and Wisconsin
86 907; 7 th Cir., 1996) the United States Court of Appeals for the Seventh Circuit Court affirmed the holding of the district court which upheld Indiana s Medicaid treatment of PASS plans. The plaintiffs in Vaughn alleged that while PASS plans were allowed for individuals who were blind, they were not allowed for individuals with disabilities, and that disallowing PASS plans for some groups of Medicaid eligibility, yet allowing it for others, violates the comparability of Medicaid services. In the Vaughn lawsuit, the State of Indiana argued they have the option to choose which groups are eligible for the Federal work incentive because of their 209(b) status, and there is no way to guarantee that PASS Plans would lead to self-sufficiency. Both the district court and panel of the Seventh Circuit agreed with the state, partially because evidence was not available to show the improvements in the PASS program process and policies (as the PASS program was not revamped at the time of the lawsuit). In December 1997, SSA had improved the work incentive to ensure self-sufficiency outcomes. Since this lawsuit in 1996, there have been substantial changes in Federal and state work incentives. Ironically, since the passage of the Medicaid Buy-In legislation in 2001 and the implementation of M.E.D. Works policies in 2002, individuals in the MA G, MA L, MA J and MA K categories of assistance would most likely be eligible for M.E.D. Works while employed, and subsequently eligible to have excess resources protected through an approved Independence and Self Sufficiency account. Because the PASS plan is primarily an SSI work incentive, individuals who are SSI recipients would be most likely eligible for the MA D category of assistance, have continued Medicaid protection under section 1619(b) of the Social Security Act, and would most likely benefit from the PASS work incentive. This is not possible unless Indiana s Medicaid eligibility policies are amended to allow PASS plans as approved by the Social Security Administration. The Federal Social Security Act provisions regarding PASS (SEC [42 U.S.C. 1382) outlines that states must have a Medicaid State Plan that addresses the following:
87 (14) provide that the State agency shall, in determining need for aid to the aged, blind, or disabled, take into consideration any other income and resources of an individual claiming such aid, as well as any expenses reasonably attributable to the earning of any such income; except that, in making such determination with respect to any individual (A) if such individual is blind, the State agency (i) shall disregard the first $85 per month of earned income plus one-half of earned income in excess of $85 per month, and (ii) shall, for a period not in excess of 12 months, and may, for a period not in excess of 36 months, disregard such additional amounts of other income and resources, in the case of any such individual who has a plan for achieving self-support approved by the State agency, as may be necessary for the fulfillment of such plan, (B) if such individual is not blind but is permanently and totally disabled, (i) of the first $80 per month of earned income, the State agency may disregard not more than the first $20 thereof plus one-half of the remainder, and (ii) the State agency may, for a period not in excess of 36 months, disregard such additional amounts of other income and resources, in the case of any such individual who has a plan for achieving self-support approved by the State agency, as may be necessary for the fulfillment of such plan, but only with respect to the part or parts of such period during substantially all of which he is actually undergoing vocational rehabilitation. It appears that Indiana s policies on PASS Plans are outdated. The arguments offered by the State of Indiana in the Vaughn vs. Sullivan lawsuit are no longer pertinent, as SSA has revamped the PASS Program since that time. Also, the M.E.D. Works program allows Savings for Independence and Self-Sufficiency for individuals eligible for M.E.D. Works. This application requires less oversight than the application, approval and monitoring process provided by SSA for PASS plans. Additionally, PASS is allowed for individuals who are Medicare beneficiaries who would not benefit from the program; rather these individuals would benefit from Savings for Independence and Self-Sufficiency through M.E.D. Works. Advocates
88 are beginning to recognize these issues and are taking steps to propose policy changes. Recommendations: Implement changes to the Medicaid Buy-In program as recommended by the Work Incentives Council in August Conduct a study to explore how Social Security s PASS program changes can be beneficial for Medicaid recipients. Explore and implement policies to allow eligible individuals in the Medicaid Assistance for Disabled to set aside resources under the Federal PASS program in excess of Indiana Medicaid s resource limit, or clearly state policies that allow individuals with approved PASS programs to participate in M.E.D Works. Develop a unified state government policy on how to support people with disabilities in employment that does not define individual needs based on a specific disability eligibility category. V. CONCLUSION This assessment addressed Indiana s Medicaid system of care for people with disabilities in relation to how and where Personal Assistance Services are offered to individuals with disabilities who are employed or wish to be employed. This study explored Indiana s Home and Community-Based Waiver Services and how PAS is offered in the community and workplace. CMS outlines specific criteria for states to achieve full eligibility for Medicaid Infrastructure Grant (MIG) funds. At the current time, Indiana s Personal Assistance Services appear to fall short of meeting CMS criteria. However there are opportunities to address these limitations in the next year and promote systems change within the Medicaid State Plan and the HCBS Waivers
89 As these opportunities are pursued, further assessments of both process and progress of systems change in community-based services should be conducted to evaluate the impact of these systems changes on individuals and family members, as well as provider capacity to serve individuals effectively, efficiently and satisfactorily. Finally, the fiscal impact of systems changes should be assessed as services are revamped to include more options for community-based employment. The Medicaid Infrastructure Grant is a valuable tool to address these changes and should be used not only to achieve the outcomes it has already achieved, but to also be a companion to other state grants working toward systems change
90 REFERENCES Americans with Disabilities Act, Titles I & V retrieved June 1, 2005 from ARC of Indiana (n.d.). A Guide to Medicaid and Medicaid Waivers. Retrieved May 20, 2005 from ARC of Indiana (2005). Indiana s 317 Plan Update February Retrieved June 3, 2005 from Braddock, D., & Hemp, R. (2004). Developmental Disabilities Services in Indiana: 2004 Progress Report. Indianapolis: Association of Rehabilitation Facilities of Indiana. Clearing House for the Community Living Information Exchange Collaborative Compendia (2005). Retrieved June 2, 2005 from Center for Personal Assistance Services (n.d.). Retrieved May 20, 2005 from Centers for Medicare and Medicaid Services (2004). Home and Community- Based Services Waiver Program. Retrieved June 2, 2005 from Centers for Medicare and Medicaid Services PAS Scoring Tool (2003). Available at: [ Crisp, S., Eiken, S., Gerst, K., & Justice, D. (2003). Money Follows the Person and Balancing Long-Term Care Systems: State Examples. Washington, D.C.: U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Disabled and Elderly Health Programs Division
91 Department of Health and Human Services, Centers for Medicare and Medicaid Services, 2006 Edition-Announcement Medicaid Infrastructure Grant. Retrieved June 2, 2005 from Flannigan, S. (2004). Accessing workers compensation insurance for consumeremployed personal assistance service workers: Issues, challenges and promising practices, Final Report. Boston: Boston College Graduate School of Social Work. Gibson, M., Gregory, S., Houser, A., & Fox-Grage, W. (2004), Across the states: Profiles of long-term care: Indiana: AARP Public Policy Institute. Gray, C., & Glantz, L. (2003). MaineCare and other Supports for Workers with Disabilities: A Summary Report of Focus Group Findings. Augusta: CHOICES: Maine s Medicaid Infrastructure Grant. Indiana s Quality Improvement Process. Author, (2003). HCBS Quality 1 (5). Indiana Family and Social Services Administration, Bureau of Developmental Disabilities. Service Definitions and Standards Manual (2004). Indianapolis. Indiana Family and Social Services Administration, (June, 2001). Comprehensive Plan for Community Integration and Support of Persons with Disabilities. Indianapolis. Indiana Family and Social Services Administration, Division of Disability and Rehabilitative Services Information Bulletin, (April 1, 2005). Department of Justice (DOJ) Recommendations, Indianapolis. Indiana Family and Social Services Administration, (n.d.). People with Disabilities- Medicaid Retrieved May 20, 2005 from Indiana Legislative Services Agency, Document #03-245F Title 460 Final Rule Indiana Code sections through ) Indianapolis, Author
92 Ireys, H., White, J., & Thornton, C. (2003). The Medicaid Buy-In program: quantitative measures of enrollment trends and participant characteristics in 2002, preliminary report. Baltimore: Centers for Medicare and Medicaid Services. Krauss v. Hamilton No. 71 DO CT 002 (Saint Joseph Superior Court, 2004). Larson, S. A., & Hewitt, A. S. ( 2005). Staff Recruitment, Retention, and Training Strategies. Paul H. Brookes Publishing Co.: Baltimore, MD. Minnesota Department of Human Services. Disability Services Program Manual, Personal Care Assistance Overview. Retrieved April 1, 2005 from _id_ hcsp. Personal Assistance Services in the Workplace. Retrieved May 31, 2005 from O Brien-Wright, M.E. (2003). Personal Assistance Services for working healthy in progress. Working Healthy: Making healthcare work. 2 (4). Kansas University Department of Health Policy and Management. The Lewin Group (2004). Opportunities and obstacles for Indiana Medicaid. Indianapolis: Indiana Government Efficiency Commission, Subcommittee on Medicaid and Human Services. Salley, S. (2005). National Consortium on Health Systems Development Memorandum dated May 4, 2005 regarding Medicaid Infrastructure Grants and Personal Assistance Services Eligibility Status. Ticket to Work and Work Incentives Improvement Act (TWWIIA) of 1999, PL , 42, U.S.C. 1305, et seq. United States Department of Labor, Office of Disability and Employment Policy. Reasonable Accommodations. Retrieved June from
93 Vaughn v. Sullivan No (United States Court of Appeals for the Seventh Circuit, 1996). Wittman and Bezanson (2004). Framework for building state level personal assistance services infrastructure. Community Living Briefs 2, 3. Work Ability: Employment-Related Personal Assistance Services (E-PAS) Retrieved March 30, 2005 from
94 APPENDIX A Personal Assistance Services Scoring Tool
95 - 79 -
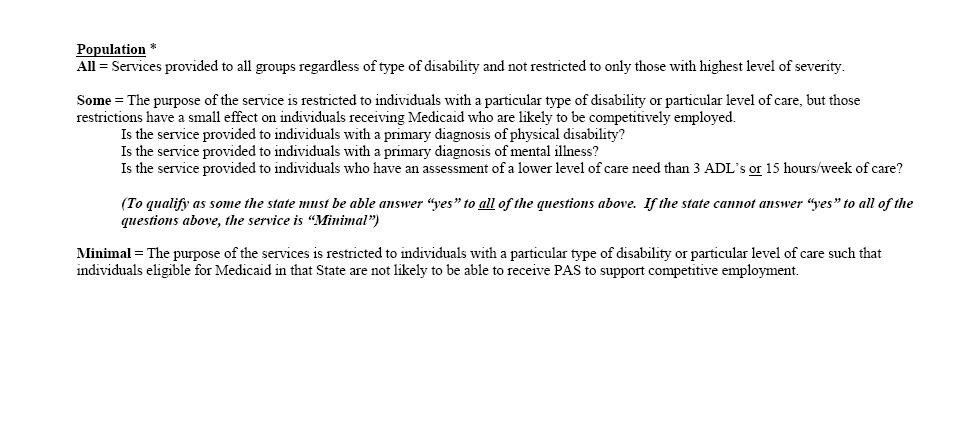
96 - 80 -
Long-Term Care Glossary
 Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
Medicaid Home- and Community-Based Waiver Programs
 INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: October 2016 Medicaid Home-
INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: October 2016 Medicaid Home-
Older Adult Services. Submitted as: Illinois Public Act Status: Enacted into law in Suggested State Legislation
 Older Adult Services This Act is designed to transform the state older adult services system into a primarily home and community-based system, taking into account the continuing need for 24-hour skilled
Older Adult Services This Act is designed to transform the state older adult services system into a primarily home and community-based system, taking into account the continuing need for 24-hour skilled
New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence
 New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence The Centers for Medicare and Medicaid Services (CMS) has published a Final Rule
New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence The Centers for Medicare and Medicaid Services (CMS) has published a Final Rule
Request for an Amendment to a 1915(c) Home and Community-Based Services Waiver
 Home and Community-Based Services Waiver") Page 1 of 11 Request for an Amendment to a 1915(c) Home and Community-Based Services Waiver 1. Request Information A. The State of North Carolina requests approval for an amendment to the following Medicaid
Page 1 of 11 Request for an Amendment to a 1915(c) Home and Community-Based Services Waiver 1. Request Information A. The State of North Carolina requests approval for an amendment to the following Medicaid
NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL
 NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL POLICY GUIDELINES Table of Contents SECTION I - DESCRIPTION OF
NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL POLICY GUIDELINES Table of Contents SECTION I - DESCRIPTION OF
S 2734 S T A T E O F R H O D E I S L A N D
 LC00 01 -- S S T A T E O F R H O D E I S L A N D IN GENERAL ASSEMBLY JANUARY SESSION, A.D. 01 A N A C T RELATING TO HUMAN SERVICES -- QUALITY SELF-DIRECTED SERVICES -- PUBLIC OFFICERS AND EMPLOYEES --
LC00 01 -- S S T A T E O F R H O D E I S L A N D IN GENERAL ASSEMBLY JANUARY SESSION, A.D. 01 A N A C T RELATING TO HUMAN SERVICES -- QUALITY SELF-DIRECTED SERVICES -- PUBLIC OFFICERS AND EMPLOYEES --
EMS Systems Act of 1973
 EMS Systems Act of 1973 Public Law 93-154 93rd Congress, S. 2410 November 16, 1973 An Act To amend the Public Health Service Act to provide assistance and encouragement for the development of comprehensive
EMS Systems Act of 1973 Public Law 93-154 93rd Congress, S. 2410 November 16, 1973 An Act To amend the Public Health Service Act to provide assistance and encouragement for the development of comprehensive
Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule
 January 16, 2014 Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule On January 10, 2014, the Centers for Medicare and Medicaid
January 16, 2014 Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule On January 10, 2014, the Centers for Medicare and Medicaid
November 14, Chief Clinical Operating Officer Division of Medical Assistance Department of Health and Human Services
 Department of Health and Human Services Division of Medical Assistance Response To Questions from the Adult Care Home Transition Subcommittee of the Blue Ribbon Commission November 14, 2012 Presenter:
Department of Health and Human Services Division of Medical Assistance Response To Questions from the Adult Care Home Transition Subcommittee of the Blue Ribbon Commission November 14, 2012 Presenter:
medicaid Case Study: Georgia s Money Follows the Person Demonstration
 I S S U E kaiser commission o n medicaid a n d t h e uninsured December 2011 P A P E R Case Study: Georgia s Money Follows the Person Demonstration Introduction The Georgia Department of Community Health
I S S U E kaiser commission o n medicaid a n d t h e uninsured December 2011 P A P E R Case Study: Georgia s Money Follows the Person Demonstration Introduction The Georgia Department of Community Health
Transforming Louisiana s Long Term Care Supports and Services System. Initial Program Concept
 Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Long Term Care. Lecture for HS200 Nov 14, 2006
 Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
Provider Certification Standards Adult Day Care
 Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
 Page 1 of 7 Social Services 365-f. Consumer directed personal assistance program. 1. Purpose and intent. The consumer directed personal assistance program is intended to permit chronically ill and/or physically
Page 1 of 7 Social Services 365-f. Consumer directed personal assistance program. 1. Purpose and intent. The consumer directed personal assistance program is intended to permit chronically ill and/or physically
Money Follows the Person Getting it Done in Nevada TABLE OF CONTENTS
 Money Follows the Person Getting it Done in Nevada May 30, 2006 TABLE OF CONTENTS Introduction 2 Report Methodology 3 Impact of Olmstead Decision 3 Current Institutional Bias 4 Recommendations 1. Development
Money Follows the Person Getting it Done in Nevada May 30, 2006 TABLE OF CONTENTS Introduction 2 Report Methodology 3 Impact of Olmstead Decision 3 Current Institutional Bias 4 Recommendations 1. Development
Application for a 1915(c) Home and Community-Based Services Waiver
 Home and Community-Based Services Waiver") Page 1 of 76 Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Page 1 of 76 Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
KENTUCKY DECEMBER 7, Cabinet for Health and Family Services HOME AND COMMUNITY BASED SERVICES (HCBS) WAIVER REDESIGN
 WAIVER REDESIGN") KENTUCKY Cabinet for Health and Family HOME AND COMMUNITY BASED SERVICES (HCBS) WAIVER REDESIGN DECEMBER 7, 2016 Session Timeline Time Topic 9:30 9:45 AM Welcome: Introductions & Agenda Review 9:45 10:15
KENTUCKY Cabinet for Health and Family HOME AND COMMUNITY BASED SERVICES (HCBS) WAIVER REDESIGN DECEMBER 7, 2016 Session Timeline Time Topic 9:30 9:45 AM Welcome: Introductions & Agenda Review 9:45 10:15
SERVICES. The following figures reflect total waiver numbers as of September 12, 2017: Total # Slots Allocated
 Office for Citizens with Developmental Disabilities (OCDD) QUARTERLY DEVELOPMENTAL DISABILITIES (DD) COUNCIL REPORT (Submitted for 3rd Quarter 2017) September 27, 2017 SERVICES Developmental Disability
Office for Citizens with Developmental Disabilities (OCDD) QUARTERLY DEVELOPMENTAL DISABILITIES (DD) COUNCIL REPORT (Submitted for 3rd Quarter 2017) September 27, 2017 SERVICES Developmental Disability
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10
 Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Revised: November 2005 Regulation of Health and Human Services Facilities
 Revised: November 2005 Regulation of Health and Human Services Facilities This guidebook provides an overview of state regulation of residential facilities that provide support services for their residents.
Revised: November 2005 Regulation of Health and Human Services Facilities This guidebook provides an overview of state regulation of residential facilities that provide support services for their residents.
DIVISION CIRCULAR #8 (N.J.A.C. 10:46C) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES
 DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES") DIVISION CIRCULAR #8 (N.J.A.C. 10:46C) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES EFFECTIVE DATE: September 17, 2012 DATE ISSUED: September 17, 2012 (Rescinds DC #8 Waiting List
DIVISION CIRCULAR #8 (N.J.A.C. 10:46C) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES EFFECTIVE DATE: September 17, 2012 DATE ISSUED: September 17, 2012 (Rescinds DC #8 Waiting List
Authorized By: Elizabeth Connolly, Acting Commissioner, Department of Human Services.
 HUMAN SERVICES 49 NJR 1(2) January 17, 2017 Filed December 22, 2016 DIVISION OF AGING SERVICES AREA AGENCY ON AGING ADMINISTRATION Statewide Respite Care Program Proposed Readoption with Amendments: N.J.A.C.
HUMAN SERVICES 49 NJR 1(2) January 17, 2017 Filed December 22, 2016 DIVISION OF AGING SERVICES AREA AGENCY ON AGING ADMINISTRATION Statewide Respite Care Program Proposed Readoption with Amendments: N.J.A.C.
Integrated Licensure Background and Recommendations
 Integrated Licensure Background and Recommendations Minnesota Department of Health and Minnesota Department of Human Services Report to the Minnesota Legislature 2014 February 2014 Minnesota Department
Integrated Licensure Background and Recommendations Minnesota Department of Health and Minnesota Department of Human Services Report to the Minnesota Legislature 2014 February 2014 Minnesota Department
OHIO DEPARTMENT OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES NEW FUTURES WAIVER
 OHIO DEPARTMENT OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES NEW FUTURES WAIVER CONCEPT PAPER SUBMITTED TO CMS Brief Waiver Description Ohio intends to create a 1915c Home and Community-Based Services
OHIO DEPARTMENT OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES NEW FUTURES WAIVER CONCEPT PAPER SUBMITTED TO CMS Brief Waiver Description Ohio intends to create a 1915c Home and Community-Based Services
Appendix A. Laws & Statutory Regulations. K-PASS Self-Direction Toolkit 173
 Appendix A Laws & Statutory Regulations K-PASS Self-Direction Toolkit 173 174 K-PASS Self-Direction Toolkit SELF-DIRECTED PERSONAL ASSISTANCE SERVICES 1. 1989 Session of Kansas Legislature Passed H.B.
Appendix A Laws & Statutory Regulations K-PASS Self-Direction Toolkit 173 174 K-PASS Self-Direction Toolkit SELF-DIRECTED PERSONAL ASSISTANCE SERVICES 1. 1989 Session of Kansas Legislature Passed H.B.
79th OREGON LEGISLATIVE ASSEMBLY Regular Session. Enrolled. Senate Bill 58
 79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled Senate Bill 58 Printed pursuant to Senate Interim Rule 213.28 by order of the President of the Senate in conformance with presession filing
79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled Senate Bill 58 Printed pursuant to Senate Interim Rule 213.28 by order of the President of the Senate in conformance with presession filing
1915(k) Community First Choice Option in New York State
 Community First Choice Option in New York State") 1915(k) Community First Choice Option in New York State BACKGROUND Key Questions and Issues for Implementing the Community First Choice Option in New York State Prepared by New York State ADAPT February
1915(k) Community First Choice Option in New York State BACKGROUND Key Questions and Issues for Implementing the Community First Choice Option in New York State Prepared by New York State ADAPT February
Office of Long-Term Living Waiver Programs - Service Descriptions
 Adult Daily Living Office of Long-Term Living Waiver Programs - Descriptions *The service descriptions below do not represent the comprehensive Definition as listed in each of the Waivers. Please refer
Adult Daily Living Office of Long-Term Living Waiver Programs - Descriptions *The service descriptions below do not represent the comprehensive Definition as listed in each of the Waivers. Please refer
Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions
 Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions Webinar Website: http://gucchdtacenter.georgetown.edu/resources/tawebinars.html Coverage
Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions Webinar Website: http://gucchdtacenter.georgetown.edu/resources/tawebinars.html Coverage
Georgia Department of Behavioral Health & Developmental Disabilities FOR. Effective Date: January 1, 2018 (Posted: December 1, 2017)
") Georgia Department of Behavioral Health & Developmental Disabilities PROVIDER MANUAL FOR COMMUNITY DEVELOPMENTAL DISABILITY PROVIDERS OF STATE-FUNDED DEVELOPMENTAL DISABILITY SERVICES FISCAL YEAR 2018
Georgia Department of Behavioral Health & Developmental Disabilities PROVIDER MANUAL FOR COMMUNITY DEVELOPMENTAL DISABILITY PROVIDERS OF STATE-FUNDED DEVELOPMENTAL DISABILITY SERVICES FISCAL YEAR 2018
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
term does not include services provided by a religious organization for the purpose of providing services exclusively to clergymen or consumers in a
 HEALTH CARE FACILITIES ACT - LICENSURE OF HOME CARE AGENCIES AND HOME CARE REGISTRIES, CONSUMER PROTECTIONS, INSPECTIONS AND PLANS OF CORRECTION AND APPLICABILITY OF ACT Act of Jul. 7, 2006, P.L. 334,
HEALTH CARE FACILITIES ACT - LICENSURE OF HOME CARE AGENCIES AND HOME CARE REGISTRIES, CONSUMER PROTECTIONS, INSPECTIONS AND PLANS OF CORRECTION AND APPLICABILITY OF ACT Act of Jul. 7, 2006, P.L. 334,
Medicaid 201: Home and Community Based Services
 Medicaid 201: Home and Community Based Services Kathy Poisal Division of Long Term Services and Supports Disabled and Elderly Health Programs Group Center for Medicaid and CHIP Services Centers for Medicare
Medicaid 201: Home and Community Based Services Kathy Poisal Division of Long Term Services and Supports Disabled and Elderly Health Programs Group Center for Medicaid and CHIP Services Centers for Medicare
Medicaid Interpreter Services Pilot: Report on Program Effectiveness and Feasibility of Statewide Expansion
 Report on Program Effectiveness and Feasibility of Statewide Expansion Pursuant to S.B. 376, 79th Legislature, Regular Session, 2005 Submitted by the Health and Human Services Commission January 2007 Table
Report on Program Effectiveness and Feasibility of Statewide Expansion Pursuant to S.B. 376, 79th Legislature, Regular Session, 2005 Submitted by the Health and Human Services Commission January 2007 Table
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY
 MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY Public Act 280 of 1939, as amended, and consultation guidelines for Medicaid policy provide an opportunity to review proposed
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY Public Act 280 of 1939, as amended, and consultation guidelines for Medicaid policy provide an opportunity to review proposed
COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN. Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013
 COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN I. INTRODUCTION Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013 In 1981, with the creation of the Community Options Program, the state
COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN I. INTRODUCTION Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013 In 1981, with the creation of the Community Options Program, the state
Application for a 1915(c) Home and Community-Based Services Waiver
 Home and Community-Based Services Waiver") Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM Page 1 of 117 The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM Page 1 of 117 The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
THE REHABILITATION ACT OF 1973, AS AMENDED (by WIOA in 2014) Title VII - Independent Living Services and Centers for Independent Living
 Title VII - Independent Living Services and Centers for Independent Living") THE REHABILITATION ACT OF 1973, AS AMENDED (by WIOA in 2014) Title VII - Independent Living Services and Centers for Independent Living Chapter 1 - INDIVIDUALS WITH SIGNIFICANT DISABILITIES Subchapter
THE REHABILITATION ACT OF 1973, AS AMENDED (by WIOA in 2014) Title VII - Independent Living Services and Centers for Independent Living Chapter 1 - INDIVIDUALS WITH SIGNIFICANT DISABILITIES Subchapter
DEVELOPMENTAL DISABILITIES INDIVIDUAL BUDGETING MEDICAID WAIVER COVERAGE AND LIMITATIONS HANDBOOK
 Florida Medicaid DEVELOPMENTAL DISABILITIES INDIVIDUAL BUDGETING MEDICAID WAIVER COVERAGE AND LIMITATIONS HANDBOOK Agency for Health Care Administration UPDATE LOG DEVELOPMENTAL DISABILITIES INDIVIDUAL
Florida Medicaid DEVELOPMENTAL DISABILITIES INDIVIDUAL BUDGETING MEDICAID WAIVER COVERAGE AND LIMITATIONS HANDBOOK Agency for Health Care Administration UPDATE LOG DEVELOPMENTAL DISABILITIES INDIVIDUAL
A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports
 A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports California Department of Health Care Services, Home and Community Based Services Universal Assessment Workgroup February
A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports California Department of Health Care Services, Home and Community Based Services Universal Assessment Workgroup February
Department of Elder Affairs Programs and Services Handbook Chapter 3: Description of DOEA Coordination with Other State/Federal Programs CHAPTER 3
 CHAPTER 3 Description of DOEA Coordination with Other State/Federal Programs 3-1 Table of Contents TABLE OF CONTENTS Section: Topic Page I. Overview and Specific Legal Authority 3-4 II. 3-7 A. Adult Care
CHAPTER 3 Description of DOEA Coordination with Other State/Federal Programs 3-1 Table of Contents TABLE OF CONTENTS Section: Topic Page I. Overview and Specific Legal Authority 3-4 II. 3-7 A. Adult Care
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS DIRECTOR EDMUND G. BROWN JR. GOVERNOR DATE: September 15, 2014 All Plan Letter 14-011 TO: ALL MEDI-CAL
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS DIRECTOR EDMUND G. BROWN JR. GOVERNOR DATE: September 15, 2014 All Plan Letter 14-011 TO: ALL MEDI-CAL
Application for a 1915(c) Home and Community-Based Services Waiver
 Home and Community-Based Services Waiver") Application for 1915(c) HCBS Waiver: PA.0147.R04.03 - Jul 01, 2009 (as of Jul 01, 2009)Page 1 of 271 https://www.hcbswaivers.net/cms/faces/protected/35/print/printselector.jsp 5/4/2011 Application for
Application for 1915(c) HCBS Waiver: PA.0147.R04.03 - Jul 01, 2009 (as of Jul 01, 2009)Page 1 of 271 https://www.hcbswaivers.net/cms/faces/protected/35/print/printselector.jsp 5/4/2011 Application for
Home and Community Based Services Mental Retardation/Developmental Disabilities Providers
 May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental
May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental
Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE. Effective Date:
 Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE Date of Issue: July 30, 1993 Effective Date: April 1, 1993 Number: OMH-93-09 Subject By Resource
Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE Date of Issue: July 30, 1993 Effective Date: April 1, 1993 Number: OMH-93-09 Subject By Resource
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE
 Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 09 MEDICAL CARE PROGRAMS Chapter 07 Medical Day Care Services Authority: Health-General Article, 2-104(b), 15-103, 15-105, and 15-111, Annotated
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 09 MEDICAL CARE PROGRAMS Chapter 07 Medical Day Care Services Authority: Health-General Article, 2-104(b), 15-103, 15-105, and 15-111, Annotated
The Patient Protection and Affordable Care Act (Public Law )
") Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Using Medicaid Home and Community Based Services or ICF/MR Funding to Pay for Direct Support Staff Training and Credentialing Programs
 Using Medicaid Home and Community Based Services or ICF/MR Funding to Pay for Direct Support Staff Training and Credentialing Programs Purpose and Background Many states are facing significant challenges
Using Medicaid Home and Community Based Services or ICF/MR Funding to Pay for Direct Support Staff Training and Credentialing Programs Purpose and Background Many states are facing significant challenges
DEPARTMENT OF ELDER AFFAIRS PROGRAMS AND SERVICES HANDBOOK Chapter 5: Community Care for the Elderly Program CHAPTER 5
 CHAPTER 5 Administration of the Community Care for the Elderly (CCE) Program July 2011 5-1 Table of Contents TABLE OF CONTENTS Section: Topic Page I. Purpose of the CCE Program 5-3 II. Legal Basis and
CHAPTER 5 Administration of the Community Care for the Elderly (CCE) Program July 2011 5-1 Table of Contents TABLE OF CONTENTS Section: Topic Page I. Purpose of the CCE Program 5-3 II. Legal Basis and
Application for a 1915(c) Home and Community- Based Services Waiver
 Home and Community- Based Services Waiver") Page 1 of 216 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Page 1 of 216 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Medicaid and CHIP Managed Care Final Rule MLTSS
 Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
Application for a 1915 (c) HCBS Waiver
 HCBS Waiver") Application for a 1915 (c) HCBS Waiver HCBS Waiver Application Version 3.3 Submitted by: Connecticut Department of Social Services Patricia A. Wilson Coker, JD, MSW Commissioner Submission Date: October
Application for a 1915 (c) HCBS Waiver HCBS Waiver Application Version 3.3 Submitted by: Connecticut Department of Social Services Patricia A. Wilson Coker, JD, MSW Commissioner Submission Date: October
Exhibit A. Part 1 Statement of Work
 Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
CHAPTER House Bill No. 5303
 CHAPTER 2010-157 House Bill No. 5303 An act relating to the Agency for Persons with Disabilities; amending s. 393.0661, F.S.; specifying assessment instruments to be used for the delivery of home and community-based
CHAPTER 2010-157 House Bill No. 5303 An act relating to the Agency for Persons with Disabilities; amending s. 393.0661, F.S.; specifying assessment instruments to be used for the delivery of home and community-based
Day 2, Morning Plenary 1 CMS and OIG Joint Briefing: Importance and Progress of Improved Background Screenings for Long Term Care
 Day 2, Morning Plenary 1 CMS and OIG Joint Briefing: Importance and Progress of Improved Background Screenings for Long Term Care Don Howard, CMS Ernie Baumann, CNA Tricia Fields, OIG Michala Walker, OIG
Day 2, Morning Plenary 1 CMS and OIG Joint Briefing: Importance and Progress of Improved Background Screenings for Long Term Care Don Howard, CMS Ernie Baumann, CNA Tricia Fields, OIG Michala Walker, OIG
5/30/2012
 The Affordable Care Act Background Coverage Long-term Care Home and Community Based Services Payment Delivery Care Transitions Assuring Quality Supreme Court 5/30/2012 www.nasuad.org BACKGROUND Health
The Affordable Care Act Background Coverage Long-term Care Home and Community Based Services Payment Delivery Care Transitions Assuring Quality Supreme Court 5/30/2012 www.nasuad.org BACKGROUND Health
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage
 Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Infant Toddler Early Intervention Services - Infant/Toddler/Family (ITF) Waiver
 Waiver") II-G Waiver Services Infant Toddler Early Intervention Services - Infant/Toddler/Family (ITF) Waiver The Infant, Toddler and Family (ITF) Waiver applies to children from birth to their third birthday.
II-G Waiver Services Infant Toddler Early Intervention Services - Infant/Toddler/Family (ITF) Waiver The Infant, Toddler and Family (ITF) Waiver applies to children from birth to their third birthday.
Program of All-inclusive Care for the Elderly (PACE) Summary and Recommendations
 Summary and Recommendations") Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
A Snapshot of the Connecticut LTSS Rebalancing Agenda
 A Snapshot of the Connecticut LTSS Rebalancing Agenda Agenda Medicaid context and vision State Rebalancing Plan Major elements of rebalancing agenda Money Follows the Person, Nursing Home Rightsizing,
A Snapshot of the Connecticut LTSS Rebalancing Agenda Agenda Medicaid context and vision State Rebalancing Plan Major elements of rebalancing agenda Money Follows the Person, Nursing Home Rightsizing,
Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model
 Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model In 2011, Tennessee was awarded a federal Money Follows the Person (MFP) grant,
Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model In 2011, Tennessee was awarded a federal Money Follows the Person (MFP) grant,
Medicare and Medicaid
 Medicare and Medicaid Medicare Medicare is a multi-part federal health insurance program managed by the federal government. A person applies for Medicare through the Social Security Administration, but
Medicare and Medicaid Medicare Medicare is a multi-part federal health insurance program managed by the federal government. A person applies for Medicare through the Social Security Administration, but
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. HCBS Autism Waiver
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS Autism Waiver Introduction Section 7000 7010 8100 8300 8400 BILLING INSTRUCTIONS HCBS Autism Waiver Billing Instructions... Submission of Claim...
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS Autism Waiver Introduction Section 7000 7010 8100 8300 8400 BILLING INSTRUCTIONS HCBS Autism Waiver Billing Instructions... Submission of Claim...
LONG TERM CARE SETTINGS
 LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
REQUEST FOR PROPOSALS: IMMIGRANT ASSISTANCE PROGRAMS GRANTS
 CITY AND COUNTY OF SAN FRANCISCO OFFICE OF CIVIC ENGAGEMENT & IMMIGRANT AFFAIRS REQUEST FOR PROPOSALS: IMMIGRANT ASSISTANCE PROGRAMS GRANTS I N F O R M A T I O N P A C K E T # 2 0 1 6-0 1 Date Issued:
CITY AND COUNTY OF SAN FRANCISCO OFFICE OF CIVIC ENGAGEMENT & IMMIGRANT AFFAIRS REQUEST FOR PROPOSALS: IMMIGRANT ASSISTANCE PROGRAMS GRANTS I N F O R M A T I O N P A C K E T # 2 0 1 6-0 1 Date Issued:
DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE
 DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE DATE OF ISSUE January 30, 2008 EFFECTIVE DATE January 1, 2008 NUMBER 00-08-03 SUBJECT: Procedures for Service Delivery
DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE DATE OF ISSUE January 30, 2008 EFFECTIVE DATE January 1, 2008 NUMBER 00-08-03 SUBJECT: Procedures for Service Delivery
Initial Needs Determination Report for Disability Waiver Residential and Support Services. Disability Services Division
 DHS-6674-ENG This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Initial
DHS-6674-ENG This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Initial
Disability Rights California
 Disability Rights California California s protection and advocacy system BAY AREA REGIONAL OFFICE 1330 Broadway, Suite 500 Oakland, CA 94612 Tel: (510) 267-1200 TTY: (800) 719-5798 Toll Free: (800) 776-5746
Disability Rights California California s protection and advocacy system BAY AREA REGIONAL OFFICE 1330 Broadway, Suite 500 Oakland, CA 94612 Tel: (510) 267-1200 TTY: (800) 719-5798 Toll Free: (800) 776-5746
Medicaid Efficiency and Cost-Containment Strategies
 Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Application for a 1915(c) Home and Community- Based Services Waiver
 Home and Community- Based Services Waiver") Page 1 of 222 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Page 1 of 222 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Long-Term Care Improvements under the Affordable Care Act (ACA)
") Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
FEB DEPARTMENT OF HEALTH & HUMAN SERVICES
 DEPARTMENT OF HEALTH & HUMAN SERVICES FEB - 2 2016 Centers for Medicare & Medicaid Services Administrator Washington, DC 20201 Mr. Darin Gordon Director Bureau of Tenn Care Tennessee Department of Finance
DEPARTMENT OF HEALTH & HUMAN SERVICES FEB - 2 2016 Centers for Medicare & Medicaid Services Administrator Washington, DC 20201 Mr. Darin Gordon Director Bureau of Tenn Care Tennessee Department of Finance
Determining Need for Medicaid Personal Care Services
 Spring 2011 No. 6 Determining Need for Medicaid Personal Care Services By Susan M. Tucker and Marshall E. Kelley The Community Living Assistance Services and Supports (CLASS) Plan a groundbreaking component
Spring 2011 No. 6 Determining Need for Medicaid Personal Care Services By Susan M. Tucker and Marshall E. Kelley The Community Living Assistance Services and Supports (CLASS) Plan a groundbreaking component
Health Care Reform Laws And Their Impact On Individuals With Disabilities (Part 2)
") Health Care Reform Laws And Their Impact On Individuals With Disabilities (Part 2) ONE STRONG VOICE: Disabilities Leadership Coalition Of Alabama Montgomery, Alabama December 8, 2010 Allan I. Bergman PATIENT
Health Care Reform Laws And Their Impact On Individuals With Disabilities (Part 2) ONE STRONG VOICE: Disabilities Leadership Coalition Of Alabama Montgomery, Alabama December 8, 2010 Allan I. Bergman PATIENT
The Commission on Long-Term Care: Background Behind the Mission
 THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
Medicaid Fundamentals. John O Brien Senior Advisor SAMHSA
 Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
Long-Term Care Community Diversion Pilot Project
 Long-Term Care Community Diversion Pilot Project 2010-2011 Legislative Report Rick Scott, Governor Charles T. Corley, Secretary Table of Contents Executive Summary 1 Chart 1 Comparative Cost Trends, FY2006
Long-Term Care Community Diversion Pilot Project 2010-2011 Legislative Report Rick Scott, Governor Charles T. Corley, Secretary Table of Contents Executive Summary 1 Chart 1 Comparative Cost Trends, FY2006
Community Outreach, Engagement, and Volunteerism
 Community Outreach, Engagement, and Volunteerism Overview To address demographic shifts in the Texas population, DADS provides additional supports to state government, local communities, and individuals
Community Outreach, Engagement, and Volunteerism Overview To address demographic shifts in the Texas population, DADS provides additional supports to state government, local communities, and individuals
Home Care Ombudsman Programs Status Report: 2007
 Prepared by the National Association of State Units on Aging National Long-Term Care Ombudsman Resource Center National Citizens' Coalition for Nursing Home Reform 1828 L Street, NW, Suite 801 Washington,
Prepared by the National Association of State Units on Aging National Long-Term Care Ombudsman Resource Center National Citizens' Coalition for Nursing Home Reform 1828 L Street, NW, Suite 801 Washington,
North Carolina Innovations Technical Guide Version 1.0 June 2012
 North Carolina Innovations Technical Guide Version 1.0 June 2012 TABLE OF CONTENTS NORTH CAROLINA INNOVATIONS WAIVER 1. OVERVIEW AND PURPOSE 5 2. NORTH CAROLINA INNOVATIONS 13 3. ASSESSMENT OF NEEDS 15
North Carolina Innovations Technical Guide Version 1.0 June 2012 TABLE OF CONTENTS NORTH CAROLINA INNOVATIONS WAIVER 1. OVERVIEW AND PURPOSE 5 2. NORTH CAROLINA INNOVATIONS 13 3. ASSESSMENT OF NEEDS 15
programs and briefly describes North Carolina Medicaid s preliminary
 State Experiences with Managed Long-term Care in Medicaid* Brian Burwell Vice President, Chronic Care and Disability Medstat Abstract: Across the country, state Medicaid programs are expressing renewed
State Experiences with Managed Long-term Care in Medicaid* Brian Burwell Vice President, Chronic Care and Disability Medstat Abstract: Across the country, state Medicaid programs are expressing renewed
ID/DD Waiver Redesign Update
 ID/DD Waiver Redesign Update Virginia General Assembly House Appropriations Committee Health and Human Resources Subcommittee June 15, 2015 Debra Ferguson, Ph.D. Commissioner Virginia Department of Behavioral
ID/DD Waiver Redesign Update Virginia General Assembly House Appropriations Committee Health and Human Resources Subcommittee June 15, 2015 Debra Ferguson, Ph.D. Commissioner Virginia Department of Behavioral
1915(k) Community First Choice Overview
 Community First Choice Overview") 1915(k) Community First Choice Overview 1 Today s Objectives 1. Brief overview of Community First Choice (CFC) Program & Key Features Other materials available: http://www.medicaid.gov/medicaid-chip-program-information/by-topics/longterm-services-and-supports/home-and-community-based-services/communityfirst-choice-1915-k.html\
1915(k) Community First Choice Overview 1 Today s Objectives 1. Brief overview of Community First Choice (CFC) Program & Key Features Other materials available: http://www.medicaid.gov/medicaid-chip-program-information/by-topics/longterm-services-and-supports/home-and-community-based-services/communityfirst-choice-1915-k.html\
Workforce Arizona Council Job Center Structure of One Stop Service Delivery System Policy
 03-2016 ARIZONA@WORK Job Center Structure of One Stop Delivery System ISSUING AGENCY: SCOPE: State Workforce Development Board State Workforce Development Board, Arizona Department of Economic Security,
03-2016 ARIZONA@WORK Job Center Structure of One Stop Delivery System ISSUING AGENCY: SCOPE: State Workforce Development Board State Workforce Development Board, Arizona Department of Economic Security,
FLORIDA MEDICAID DEVELOPMENTAL DISABILITIES WAIVER SERVICES COVERAGE AND LIMITATIONS HANDBOOK. Agency for Health Care Administration
 FLORIDA MEDICAID DEVELOPMENTAL DISABILITIES WAIVER SERVICES COVERAGE AND LIMITATIONS HANDBOOK Agency for Health Care Administration May 2010 Developmental Disabilities Waiver Services Coverage and Limitations
FLORIDA MEDICAID DEVELOPMENTAL DISABILITIES WAIVER SERVICES COVERAGE AND LIMITATIONS HANDBOOK Agency for Health Care Administration May 2010 Developmental Disabilities Waiver Services Coverage and Limitations
Medicaid Simplification
 Medicaid Simplification This Act authorizes the director of the state department of health and welfare to restructure the state Medicaid program in order to achieve improved health outcomes for Medicaid
Medicaid Simplification This Act authorizes the director of the state department of health and welfare to restructure the state Medicaid program in order to achieve improved health outcomes for Medicaid
Application for a 1915(c) Home and Community- Based Services Waiver PROPOSED
 Home and Community- Based Services Waiver PROPOSED") Page 1 of 165 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Page 1 of 165 Application for a 1915(c) Home and Community- Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home and Community-Based Services (HCBS) waiver program is authorized in
Letters in the Medicaid Alphabet:
 Letters in the Medicaid Alphabet: OPTIONS FOR FINANCING HOME AND COMMUNITY- BASED SERVICES P R E S E N T E D B Y : R O B I N E. C O O P E R D I R E C T O R O F T E C H N I C A L A S S I S T A N C E N A
Letters in the Medicaid Alphabet: OPTIONS FOR FINANCING HOME AND COMMUNITY- BASED SERVICES P R E S E N T E D B Y : R O B I N E. C O O P E R D I R E C T O R O F T E C H N I C A L A S S I S T A N C E N A
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Rhode Island Real Choices Long-Term Services and Supports Resource Mapping. April 14, Ian Stockwell
 Rhode Island Real Choices Long-Term Services and Supports Resource Mapping April 14, 2010 Cynthia Woodcock Ian Stockwell Aaron Tripp Overview of Presentation Resource Mapping Objectives Interviews with
Rhode Island Real Choices Long-Term Services and Supports Resource Mapping April 14, 2010 Cynthia Woodcock Ian Stockwell Aaron Tripp Overview of Presentation Resource Mapping Objectives Interviews with
DIVISION CIRCULAR #3 (N.J.A.C. 10:46) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES
 DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES") DIVISION CIRCULAR #3 (N.J.A.C. 10:46) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES EFFECTIVE DATE: March 24, 2011 DATE ISSUED: April 27, 2011 (Rescinds Division Circular #3, Determination
DIVISION CIRCULAR #3 (N.J.A.C. 10:46) DEPARTMENT OF HUMAN SERVICES DIVISION OF DEVELOPMENTAL DISABILITIES EFFECTIVE DATE: March 24, 2011 DATE ISSUED: April 27, 2011 (Rescinds Division Circular #3, Determination
Estimated Decrease in Expenditure by Service Category
 Public Notice for June 2009 Release PUBLIC NOTICE COLORADO MEDICAID Department of Health Care Policy and Financing Fee-for-Service Provider Payments Effective July 1, 2009, in an effort to reduce expenditures
Public Notice for June 2009 Release PUBLIC NOTICE COLORADO MEDICAID Department of Health Care Policy and Financing Fee-for-Service Provider Payments Effective July 1, 2009, in an effort to reduce expenditures
Attachment F STC Compliance
 Section I Preface Section II Historical Description of the Demonstration Section III General Program Requirements 1 Federal Non-Discrimination Statutes 2 Medicaid and CHIP Law 3 Changes in Medicaid and
Section I Preface Section II Historical Description of the Demonstration Section III General Program Requirements 1 Federal Non-Discrimination Statutes 2 Medicaid and CHIP Law 3 Changes in Medicaid and
Medicaid Managed Specialty Supports and Services Concurrent 1915(b)/(c) Waiver Program FY 17 Attachment P7.9.1
/(c) Waiver Program FY 17 Attachment P7.9.1") QUALITY ASSESSMENT AND PERFORMANCE IMPROVEMENT PROGRAMS FOR SPECIALTY PRE-PAID INPATIENT HEALTH PLANS FY 2017 The State requires that each specialty Prepaid Inpatient Health Plan (PIHP) have a quality
QUALITY ASSESSMENT AND PERFORMANCE IMPROVEMENT PROGRAMS FOR SPECIALTY PRE-PAID INPATIENT HEALTH PLANS FY 2017 The State requires that each specialty Prepaid Inpatient Health Plan (PIHP) have a quality
Application for a 1915(c) Home and Community-Based Services Waiver
 Home and Community-Based Services Waiver") Application for 1915(c) HCBS Waiver: PA.0279.R04.00 - Jul 01, 2013 Page 1 of 209 Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home
Application for 1915(c) HCBS Waiver: PA.0279.R04.00 - Jul 01, 2013 Page 1 of 209 Application for a 1915(c) Home and Community-Based Services Waiver PURPOSE OF THE HCBS WAIVER PROGRAM The Medicaid Home
The Olmstead Decision: Consumer Rights to and Opportunities for Nursing Home Alternatives. Prepared by Hollis Turnham, Esquire Center Consultant
 The : Consumer Rights to and Opportunities for Nursing Home Alternatives Prepared by Hollis Turnham, Esquire Center Consultant National Long Term Care Ombudsman Resource Center National Citizens' Coalition
The : Consumer Rights to and Opportunities for Nursing Home Alternatives Prepared by Hollis Turnham, Esquire Center Consultant National Long Term Care Ombudsman Resource Center National Citizens' Coalition
Waiver Covered Services Billing Manual
 Covered Services Waiver Covered Services Billing Manual Section 1 - Long Term Care Home and Community Based Waiver Services....2 Section 2 - Assisted Living Facility Waiver Services... 6 Section 3 - Children
Covered Services Waiver Covered Services Billing Manual Section 1 - Long Term Care Home and Community Based Waiver Services....2 Section 2 - Assisted Living Facility Waiver Services... 6 Section 3 - Children
Cooper, NASDDDS 11/15. Start-up Costs
 Start-up Costs Under CSMS guidance, startup costs for services and training are allowable once the person enrolls in the waiver. For example, direct support staff, prior to the person's enrolling on the
Start-up Costs Under CSMS guidance, startup costs for services and training are allowable once the person enrolls in the waiver. For example, direct support staff, prior to the person's enrolling on the
Habilitation Supports Waiver(HSW) Focus on Quality and Compliance
 Focus on Quality and Compliance") Habilitation Supports Waiver(HSW) Focus on Quality and Compliance Home and Community Based Waiver Conference November 2017 Belinda Hawks Yingxu Zhang Agenda Welcome & Introductions Target Audience: HSW
Habilitation Supports Waiver(HSW) Focus on Quality and Compliance Home and Community Based Waiver Conference November 2017 Belinda Hawks Yingxu Zhang Agenda Welcome & Introductions Target Audience: HSW