Proposals to Improve the Internal Medicine Discharge Process
|
|
|
- Kristian Allison
- 6 years ago
- Views:
Transcription
1 Proposals to Improve the Internal Medicine Discharge Process William Archibald MD Candidate 2018 University of Rochester Daniel Ayala MD Candidate 2017 University of Texas, San Antonio Khloe Frank MD Candidate 2018 University of Washington Ryan Gamlin MD Candidate 2018 University of Cincinnati Alazar Haregu MD Candidate 2018 University of Virginia Natalie Hartman MD Candidate 2018 University of Southern California Katia Johnston MD Candidate 2018 University of Colorado Kelly O Connor MD Candidate 2018 Tulane University
2 Table of Contents: Project Overview... 3 Needs & Current State Assessment... 3 PSDA Cycles & Key Lessons... 5 Next Step Recommendations
3 Summary This executive summary, describing the quality improvement project work undertaken by students in the 2015 Health Innovations Scholars Program (HISP) at University of Colorado, provides an at-aglance overview of the teams work and recommendations (page 1), as well as detailed descriptions in the following pages of systems analysis, insights, small tests of change, lessons learned, recommendations for data collection, and suggestions for next steps in implementing sustainable change. Questions about this summary or the project work described below should be directed to Read Pierce, MD, Director of the Young Hospitalist Academy, and Emily Gottenborg, MD, Director of the Health Innovations Scholars Program. Project Charge The HISP 2015 cohort was charged with streamlining discharge from the University of Colorado Hospital (UCH) internal medicine unit. Building upon work already initiated by an inter-professional team based on the AIP-1 9 th floor, we sought to target patient and provider dissatisfaction with the discharge process, suboptimal multidisciplinary communication, and lack of a standard approach for facilitating discharge. Overview: Insights from Needs Assessment Work by the existing inter-professional team and additional current state analysis led by our HISP cohort revealed the following gaps in system and human performance related to patient discharge: Fragmented communication among members of the medical team, leading to provider and patient confusion about and dissatisfaction with the discharge process. On the 9 th floor of AIP-1, HCAHPS Patient Experience scores from February 2015 ranked UCH in the 4 th percentile for communication with physicians, and 10 th percentile for communication with nurses Rushed patient education often occurring at the time of discharge, which leaves the patient confused about the next steps in his/her recovery. Delays in sending patients home: only 11.2% of discharges occur before noon; UCH s average time of discharge is 3:07 pm. Current State Analysis: To understand the current state of the discharge process, we started by interviewing stakeholders including patients, providers, nurses, case managers, and social workers, and by observing existing discharge rounds. These observations resulted in a rich set of insights, derived from qualitative comments and from a detailed process map of steps required to plan for and execute patient discharge from the hospital [A1.1, A1.2]. Based on frequency of observed challenges and/or severity (impact of the challenge on patient care), we identified several areas to explore more deeply, outlined below. 3
4 MD-RN communication Stakeholders unanimously expressed that MD-RN communication was splintered. To gain insight into communication challenges, we rotated through the unit with medical teams and attended rounds focused on discharge planning. Based on our observations, fragmented communication arises from several causes. Both doctors and nurses are exceptionally busy and have distinct workflows; they often work on their respective tasks without much interaction. In addition, cultural hierarchy often impedes open MD-RN dialogue, preventing effective exchange of information. This leads to reduced transparency with regard to patient treatment plans and related discharge planning. Discharge Rounding Structure To better understand the discharge process, we observed multidisciplinary discharge rounds to pinpoint where communication may break down. We were interested in how common discharge barriers were identified, communicated, and addressed through proactive planning. This focus on barriers that can delay discharge arose after we spent time with patients, and observed common themes, captured in the following experience: We sat with a patient from the time her discharge order was placed at 9:50 am until she physically left the hospital at 1:24 pm. The nearly four-hour delay was caused purely by logistical missteps. Pharmacy orders were at odds with her insurance coverage, initially there were no follow-up appointments scheduled, and no wheelchair was arranged though limited mobility was not a new challenge for her. We noted that discharge rounds could address these barriers, but typically fail to do so without standardized structure for effective communication. During these rounds, case managers, social workers, and a charge nurse are seated in a conference room, while provider teams file in and out, briefly reporting on their patients. There is no clear leader of the meeting or specific agenda. As a result, the conversation may fail to cover issues related to discharge planning. Common barriers, such as nursing home placement, home oxygen therapy evaluations, and physical therapy consult recommendations can go undiscussed. The subsequent lack of clarity about next steps in discharge planning can lead to surprises and delays later in the process. Resistance to Change/Change Fatigue Hospital medicine is both hectic and steeped in tradition regarding roles, a combination that makes implementing new changes difficult. Physicians and nurses manage myriad tasks each day, often facing a relatively high degree of unpredictability about when and where key work steps will occur. Each stakeholder group also experiences a number of existing demands for compliance with workflow requirements and quality improvement initiatives, many of which are perceived to originate outside individual nurses or physicians scope of daily practice. As a result, many nurses and physicians with whom we spoke seemed weary at the suggestion of more change, even if that change could have relatively immediate benefit for their daily work. 4
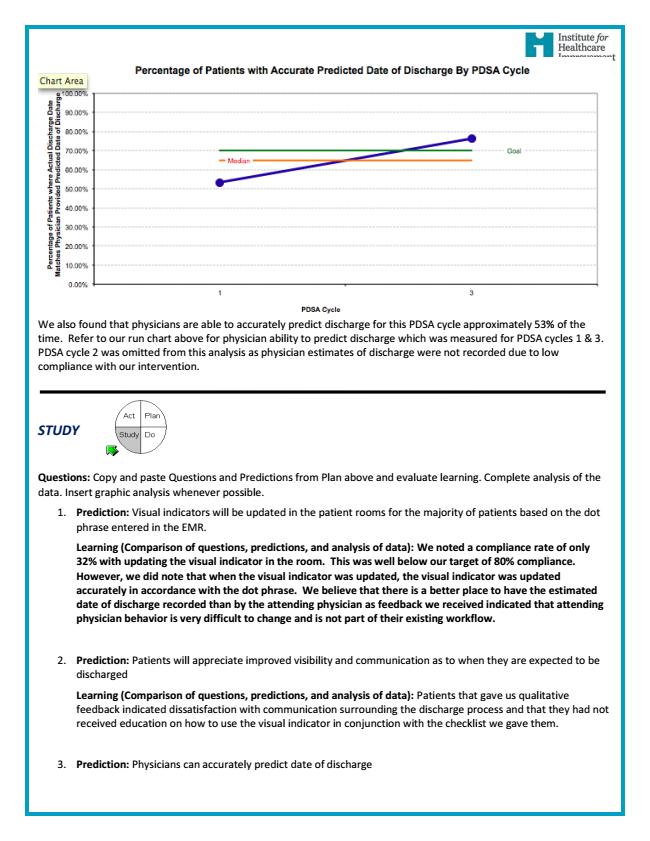
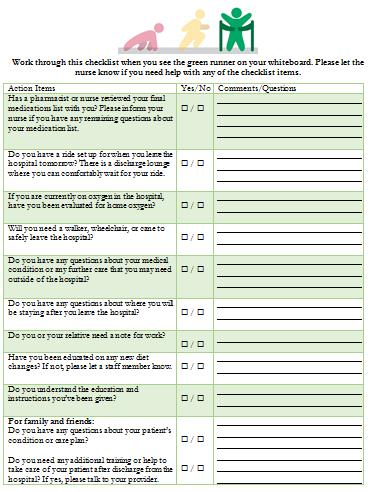
5 Estimating Date of Discharge Improving the planning process for discharge requires providers to correctly estimate a patient s date of discharge, so that other care team members can anticipate when certain tasks must be completed. Multiple clinicians we interviewed expressed concern that the uncertain nature of disease and complexity of multi-organ pathophysiology prohibited accurate predictions. Observations from Addressing Root Causes: PDSA Cycles and Key Lessons We developed ideas to address root causes identified via current state analysis, and implemented several of these ideas in 3 PDSA cycles. These trials aimed to elucidate which ideas were most sound and which workflow process changes would be necessary to sustain broad implementation. PDSA #1 Our first intervention [A2.1] asked physicians from Medicine 2 and Medicine 3 inpatient teams to 1) classify patients as being >2 days, about 2 days, or 1 day away from discharge and 2) then record this estimated discharge date in their daily progress notes using a dot phrase [A2.3] in Epic. The night nurse for a given patient would read the estimated date of discharge in the chart and update a visual indicator [A2.2] hanging in the patient s room, with the same 3 categories (>2, ~2, ~1 day to discharge). The daytime nurse would then give the patient a packet containing three checklists [A2.4]. Each checklist corresponded to a color on the visual indicator (>2 days being red, ~2 days being yellow, ~1 day being green). The checklist contained conversation prompts for each category to help the patient discuss barriers to discharge. There was also a provider checklist [A4.4] organized into the same three categories, which listed items that needed to be addressed in order for patients to be discharged efficiently. PDSA #2 This intervention [A3.1] relied upon the patient s primary nurse being called to the bedside during providers work rounds. We posted a tool called the Daily Conversation Starter [A3.2] on the wall in each patient room, which included a simplified list of 5-6 common barriers to discharge that the patient and nurse could discuss briefly before rounds. The tool included a script for the nurse to summarize any identified concerns during bedside rounds, and to prompt the provider to estimate the patient s discharge date (still using the >2 days, ~2 days, or ~1 day until discharge categories). The nurse would then record the stated prediction in the Epic sticky note using a dot phrase. PDSA #3 Our final PDSA [A4.1] moved the process of identifying, discussing, and documenting estimated date of discharge to multidisciplinary discharge rounds for Medicine team 2 and Medicine team 3 on the AIP-1 9 th floor. The case manager, who organized and led multidisciplinary discharge rounds, would prompt the provider for a given patient to identify readiness for discharge in >2 days, ~2 days, or <24 hours. 5
6 The Patient Resident Liaison (PRL), who was already stationed at a computer during rounds, would use the appropriate Epic dot phrase [A2.3] to document the provider s prediction in the Epic sticky note. Following rounds, the PRL would update the visual indicator [A4.3] in each patient room to reflect the estimated date of discharge. The PRL would also explain the meaning of the indicator to each patient. Key Lessons: Root Cause MD-RN communication Prior improvement work on the unit had already sought to address this challenge. Specifically, an initiative was in place in which signs are placed daily on patient rooms, asking clinical teams to call the primary nurse to the patient s room during bedside rounds with the providers. We anticipated that a more structured conversation at the bedside, focused on discharge planning, could eliminate communicate failures. We designed a PDSA cycle (#2), involving two medicine teams. For those teams, the patient s nurse would visit the patient prior to bedside rounds each morning, record patient concerns/barriers to discharge based on a 6-element checklist containing the most common barriers, and later report these concerns to provider team on rounds. We quickly learned that medical teams frequently fail to call the nurse to bedside rounds, despite the existing communication initiative and signs on the doors [A3.3]. While prior analysis of compliance with the call for rounds initiative suggested teams contacted the primary nurse as much as 60% of the time, during our PDSA cycle teams called the primary nurse approximately 50% of the time. Our PDSA cycle therefore had little impact on bedside conversations related to discharge planning, given that relatively few conversations were occurring. We interviewed resident physicians about barriers to calling nurses to rounds, and identified the following reasons for the poor initiative compliance: I forgot or did not have anything to tell them. It is not helpful when they do come. It interrupts workflow. It s not in my routine. In addition, our observations revealed that, on occasions when nurses were called to join rounds, the prevailing culture and lack of role clarity hampered communication. Nurses often did not want to interject during medical team conversations, and the medical team, trying to work efficiently through rounds, often did not ask the nurse for input. As a result, our checklist was not routinely used to prompt focused conversation about discharge planning. Key Lessons: Root Cause Discharge Rounding Structure and Estimating Date of Discharge Given the significant problems posed by disorganized discharge rounds, we sought to identify positive outliers examples of highly effective discharge rounds on units at UCH and to leverage key elements that address common communication failures during rounds. The Acute Care for the Elderly (ACE) unit is an example of exemplary multidisciplinary discharge rounds. In the ACE model, the charge nurse leads the meeting, calling on the appropriate person to speak in a pre-determined sequence. Each team member s role is clear, and the expectations of 6
7 which questions each individual should ask and what information s/he should provide about a patient is written on a poster board, hanging in the conference room. The components of ACE rounds that we wanted to translate to the 9th floor were: A standardized script for multidisciplinary rounds A designated individual to facilitate rounds On the 9 th floor of AIP-1, a recent initiative had sought to redesign discharge rounds. In this pilot, a single case manager leads the meeting, and specifically inquires about discharge barriers. We designed a PDSA cycle (#3) to complement this work and build upon it. In our PDSA 3 workflow, the case manager prompts the provider to estimate the patient s discharge date (as >2 days, ~2 days, or ~1 day away from discharge). The PRL, already stationed at a computer, then inputs the prediction into the Epic sticky note using a dot phrase. After rounds, the PRL then updates the visual indicators hanging in the patient rooms. Moving the discussion about estimated discharge date to multidisciplinary discharge rounds capitalized on the fact that all major stakeholders- physicians, nurses, case managers, PRL s, social workers- would be in one room at the same time. Furthermore, the point of multidisciplinary discharge rounds is specifically to discuss discharge, so this was a natural time to ask physicians for discharge date predictions. We calculated providers ability to correctly estimate discharge dates by comparing their predictions with dates that patients were actually discharged. In PDSA 1, when providers were estimating discharge in isolation, their accuracy was 54%. In PDSA 3, however, when providers were making their predictions during multidisciplinary rounds and receiving input from nurses, social workers, and case managers, their prediction accuracy rose to 76%. This increased prediction accuracy demonstrates the value of placing this task of estimating discharge date in the multidisciplinary discharge rounds. Key Lessons: Root Cause Resistance to Change/Change Fatigue While we did not seek to directly address this root cause, it manifested repeatedly as a challenge in testing and implementing ideas. For example, during our first PDSA cycle, night nurses displayed and updated the visual indicator 29% of the time (4/14), despite initial 100% physician compliance with documenting discharge date predictions in progress notes. Daytime nurses often did not explain the visual indicator to patients in a way that allowed the patients to tell us what the indicator meant (among patients who did have a visual indicator in their rooms, 0% reported sufficient explanation). Similarly, of the eight patients that we interviewed during PDSA #1, 0% reported that they received the checklist of discharge barriers from their daytime nurse. Doctors utilized the provider checklist 0% of the time as well. One physician reported that she tucked the checklist in her white coat pocket and never looked at it again. 7
8 Similarly limited enthusiasm for testing our tools or new workflows occurred during PDSA #2, when we observed that 0% of nurses recorded patient concerns/barriers to discharge with the simplified checklist and 0% reported this type of information to physicians during bedside rounds, when bedside rounds occurred. Implementing Sustainable Change: Next-Step Recommendations: Quick Wins: We feel the medicine teams can implement the following changes immediately and without large disturbances in the current workflow. Formalize PDSA #3: We recommend continuation of PDSA cycle 3, levering the multidisciplinary discharge rounds structure on the AIP-1 9 th floor to prompt prediction of discharge date, focused discussion of barriers, and recording of predicted discharge date by the PRL. With relatively minimal refinement and practice, we believe this model can be expanded across all inpatient general medicine teams. In addition, we believe that having a visual indicator in patient rooms increases transparency around the discharge process and prompts patients and providers alike to start thinking about discharge earlier in the hospital stay. This intervention creates minimal additional work for providers and nurses. Most workflow changes involve the PRLs, who in the initial PDSA 3 cycle have been open to these new responsibilities and have shown enthusiasm for participating consistently. Use a standard script during discharge rounds: This is a simple measure that we feel will add structure to discharge rounds and increase communication. We observed this model in use during the Acute Care for the Elderly (ACE) discharge rounds. The script ensured that each member of the team had a chance to give input and that any barriers to discharge were discussed. We made a similar poster and displayed it in the conference room on the AIP-1 9 th floor for medicine discharge rounds, where scripting of rounds conversations is underway. As PDSA cycle 3 is spread to other units, following a script will help make multidisciplinary rounds more effective and help identify possible barriers to discharge earlier. Strategic Initiatives: The following recommendations require larger-scope changes that medicine teams and hospital units should work towards to improve hospital discharge, but will require substantial resources and/or time. One designated case manager per team: One of the major issues we identified with existing discharge rounds is that each medicine team works with multiple case managers. This causes confusion, results in redundant work, and wastes 8
9 time. For example, we observed an intern present four patients in rounds before someone told her that the case manager for those patients had stepped out to take a phone call. She then had to figure out which patients were being cared for by the team members in the room, and then re-present the original four patients again once the case manager returned. Having multiple case managers working with each team also makes it easy for information to get lost or never communicated. One case manager told us during discharge rounds that she was supposed to be at a different set of discharge rounds, for a second team, at the same time and could not be in two places at once. This designated case manager model is currently being piloted on Med 2 and Med 3 teams, based on the AIP-1 9 th floor, and all teams have expressed increased satisfaction with this arrangement. Having a designated case manager for every team is not the current hospital standard, due to challenges with geographic cohorting and staffing. Setting up geographic cohorting (see below), restructuring staffing, and/or hiring more case managers will be necessary before this recommendation can be implemented broadly, but we feel this is a worthwhile pursuit. Increase compliance with calling RNs to bedside rounds: The current initiative that asks medicine teams to call nurses to bedside rounds is only being carried out about 25-50% of the time. While the use of a shared visual indicator will likely help keep the entire care team and patient/family aware of the estimated date of discharge, we believe additional work to optimize the discharge process offers a major opportunity to enhance face-to-face communication between physicians and nurses. Nurses often know patients, their active concerns, and possible barriers to discharge better than anyone on the care team. Calling nurses to bedside rounds provides an opportunity for quick information exchange around discharge and other pertinent medical issues. Nurses and nurse managers also expressed a strong desire to be included in bedside rounds so they can be better aware of the care plan. We believe a simple tool, like the Daily Conversation Starter, which focuses on patient needs and utilizes a simple checklist that can be completed in a few minutes each day and reviewed in <60 seconds on bedside rounds, may offer a natural aid to facilitating this new set of behaviors. However, extensive physician and nurse leadership will be necessary to change culture, via consistent action and role modeling particularly for residents, who rotate frequently and expressed numerous perceptions that talking to nurses during bedside rounds is not valuable. We recommend training attendings, residents, and medical students on the importance of having nurses present during bedside rounds to help increase compliance with calling nurses and create a more collaborative dynamic. Move patient education forward in the hospital stay: Currently, the bulk of patient education occurs in one brief episode, immediately prior to discharge. This model doesn t leave time for patients to reflect on what they ve been told, make sure they really understand the instructions, and develop questions. Moving patient education earlier and giving patients multiple exposures to new health information helps to reinforce important discharge 9
10 instructions. Patients will have several opportunities to discuss their conditions and ask questions. We also believe this will better prepare patients to follow their medication and care instructions when they get home, keeping them healthy and decreasing hospital readmissions. We would expect this to improve the low HCAHPs patient satisfaction scores in the communication with nurses, communication with doctors, and communication about medications categories. Moving this work upstream will require careful attention and likely multiple PDSA cycles, with development of new tools/prompts to determine on which pre-discharge days certain topics can and should be covered. Standardized resident training about discharge: During our stakeholder interviews, we talked with residents who described variability in the training they receive on preparing patients for discharge. One resident said that the attending he initially worked with spent the first week training residents on how to efficiently use Epic when discharging a patient. The attending encouraged residents to fill out the discharge tab in each chart as much as possible before the day of discharge. Working through this tab earlier allows the resident to anticipate potential discharge delays and place orders to address them. On the day of discharge, the only thing left to do is place the actual discharge order. Not all residents, however, have been trained under this model of discharge planning. We recommend standardizing the resident training with this model and specifically, focusing on practical knowledge about the discharge process and identification of barriers, rather than extensively and preferentially covering theoretical models about care transition. We feel that training attendings to teach all of their residents with this model should complement any universal, classroom-based didactics. Geographic cohorting: As previously described, the medicine discharge rounds we observed were often disorganized and chaotic. Much of this occurs because each medicine team works with multiple case managers, social workers, etc., for all of their patients. Trying to coordinate care and meetings with all of these different team members is difficult and leads to fragmented communication. Thus, the existing system makes it almost impossible to have an organized team, with clear roles, despite the hard work and good intentions of all team members. It also makes it difficult to have nurses present for discharge rounds. Almost all of the stakeholders we talked to thought mimicking the geographically cohorted ACE unit would be beneficial. Working with the same people consistently on a team can help to clarify roles and speed up the workflow. The major barrier to switching to this model is the lack of geographic cohorting among medicine teams patients. With geographic cohorting, teams spend the vast majority of their time in one unit, instead of having patients on three or more floors at one time. 10
11 Geographic cohorting might not be an immediately achievable goal without changing the admission process, but it is perhaps the most important strategy that we can recommend to increase consistency of team performance. Integration of a provider discharge checklist into Epic: We believe a provider discharge checklist would help anticipate potential barriers to discharge. This checklist could be broken down according to how far a patient is from discharge (one day away, two days away, or greater than two days away, etc.) or by team member (i.e., case manager tasks, nurse tasks, etc.). We have provided an example provider checklist in the appendix [A4.4]. Such a checklist would clarify expectations and roles and help to avoid the day-of-discharge scramble. In order for this checklist to actually be used by providers, it is crucial that it be integrated into Epic. We found that team members were reluctant to carry around an extra sheet of paper as a reference. When we experimented with giving providers printed checklists, we received feedback and observed that people rarely, if ever, used the checklist. Most copies ended up lost or in the trash. Integrating the checklist into Epic avoids the hassle of carrying around additional materials and makes accessing the checklist a seamless part of the existing workflow. A similar system, called the discharge readiness report is used for certain patients at Children s Hospital and has impressively decreased length of stay and hospital readmission rates. We recommend the implementation of a similar tool for the medicine teams at UCH. 11
12 Appendix Discharge Process A1.1: Process Map... Page 13 A1.2: Cause and Effect Diagram... Page 14 PDSA1 A2.1: Details... Page 15 A2.2: Visual Indicator Prototype... Page 20 A2.3: Dot Phrase Card... Page 21 A2.4: Patient Checklist... Page 22 PDSA2 A3.1: Details... Page 24 A3.2: Daily Conversation Starter... Page 29 A3.3: Pareto Diagram Reasons RNs Not Called to Work Rounds... Page 30 PDSA3 A4.1: Details... Page 31 A4.2: Pareto Diagram Reasons Patients Did Not Find Visual Indicator Useful... Page 36 A4.3: Final Visual Indicator... Page 37 A4.4: Provider Checklist... Page 38 A4.5: Discharge Rounds Prompt Poster... Page 39 Data A5.1: Run Chart of Compliance Through PDSAs 1 to 3... Page 40 A5.2: Run Chart of Physician Prediction Accuracy Through PDSAs 1 and 3... Page 41 12
13 A1.1: Process Map 13
14 A1.2: Cause and Effect Diagram 14
15 A2.1: PDSA 1 Details: 15
16 16
17 17
18 18
19 19

20 A2.2: Visual Indicator Prototype 20

21 A2.3: Dot Phrase Card 21


22 A2.4: Patient Checklist 22
23 23

24 A3.1: PDSA 2 Details 24
25 25
26 26
27 27
28 28

29 A3.2: Daily Conversation Starter 29

30 A3.3: Pareto Diagram Reasons RNs Not Called to Work Rounds 30
31 A4.1: PDSA 3 Details 31
32 32
33 33
34 34
35 35
36 Cumulative % A4.2: Pareto Diagram Reasons Patients Did Not Find Visual Indicator Useful 36

37 A4.3: Final Visual Indicator 37

38 A4.4: Provider Checklist 38

39 A4.5: Discharge Rounds Prompt Poster 39
40 A5.1: Run Chart of Compliance Through PDSAs % Compliance with updating visual indicator of discharge in patient rooms % 80.00% Goal 60.00% 40.00% Median 20.00% 0.00% PDSA Cycle 40
41 A5.2: Run Chart of Physician Prediction Accuracy Through PDSAs 1 and 3 41

42 Thank You to Our Supporters! We especially appreciate the mentorship and dedication of YHA staff and faculty. Thank you for your support and enthusiasm! Jeffrey Glasheen, MD Emily Gottenborg, MD Read Pierce, MD Emilie Keeton 42
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Center for Innovation. Enhancing Care Team Communication
 F E B R U A R Y 2 0 1 3 Enhancing Care Team Communication What is the background? Hospital units are dynamic environments in which dozens of care team members must coordinate their efforts to deliver high
F E B R U A R Y 2 0 1 3 Enhancing Care Team Communication What is the background? Hospital units are dynamic environments in which dozens of care team members must coordinate their efforts to deliver high
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
ISAAC. Improving Sickle Cell Care for Adolescents and Adults in Chicago
 ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
A Multi-Phased Approach to Using Clinical Data to Drive Evidence-Based EMR Redesign. Kulik, Carole Marie; Foad, Wendy; Brown, Gretchen
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
A GUIDE TO Understanding & Sharing Your Survey Results. Organizational Development
 A GUIDE TO Understanding & Sharing Your Survey Results al Development Table of Contents The 2018 UVA Health System Survey provides insight and awareness gained through team member feedback, which is used
A GUIDE TO Understanding & Sharing Your Survey Results al Development Table of Contents The 2018 UVA Health System Survey provides insight and awareness gained through team member feedback, which is used
Better care coordination requires streamlined, efficient, secure clinical communication
 Better care coordination requires streamlined, efficient, secure clinical communication May 2015 Contents The current state of clinical communications: Inefficient and error-prone 3 The obstacles to care
Better care coordination requires streamlined, efficient, secure clinical communication May 2015 Contents The current state of clinical communications: Inefficient and error-prone 3 The obstacles to care
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013
 NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
A Publication for Hospital and Health System Professionals
 A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A GUIDE TO Understanding & Sharing Your Survey Results
 A GUIDE TO Understanding & Sharing Your Survey Results Learning & al Development Table of Contents The 2017 UVA Health System Survey provides insight and awareness gained through team member feedback,
A GUIDE TO Understanding & Sharing Your Survey Results Learning & al Development Table of Contents The 2017 UVA Health System Survey provides insight and awareness gained through team member feedback,
A Roadmap for the Journey Home - A Supplemental Tool Guiding Patients from Hospital to Home
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
PFAC as Consultant to Hospital Initiatives
 4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
MnCHOICES Assessment and Support Plan
 MnCHOICES Assessment and Support Plan 11/01/2017 Minnesota Department of Human Services mn.gov/dhs 1 Beyond Assessment: Integration of assessment and support plan application State and federal requirements
MnCHOICES Assessment and Support Plan 11/01/2017 Minnesota Department of Human Services mn.gov/dhs 1 Beyond Assessment: Integration of assessment and support plan application State and federal requirements
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Patient Payment Check-Up
 Patient Payment Check-Up SURVEY REPORT 2017 Attitudes and behavior among those billing for healthcare and those paying for it CONDUCTED BY 2017 Patient Payment Check-Up Report 1 Patient demand is ahead
Patient Payment Check-Up SURVEY REPORT 2017 Attitudes and behavior among those billing for healthcare and those paying for it CONDUCTED BY 2017 Patient Payment Check-Up Report 1 Patient demand is ahead
Analytics in Action. Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY
 Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
The Changing Role CUSTOM MEDIA
 The Changing Role of Paper in healthcare CUSTOM MEDIA Historically, healthcare has always been a document-intensive industry. And despite the widespread adoption of electronic health records (EHRs), it
The Changing Role of Paper in healthcare CUSTOM MEDIA Historically, healthcare has always been a document-intensive industry. And despite the widespread adoption of electronic health records (EHRs), it
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Improving the Patient Experience from Admission to Discharge. Yvonne Chase Section Head Patient Access & Business Services Mayo Clinic Arizona
 Improving the Patient Experience from Admission to Discharge Yvonne Chase Section Head Patient Access & Business Services Mayo Clinic Arizona A Clear Priority SOURCE: A REPORT ON THE BERYL INSTITUTE BENCHMARKING
Improving the Patient Experience from Admission to Discharge Yvonne Chase Section Head Patient Access & Business Services Mayo Clinic Arizona A Clear Priority SOURCE: A REPORT ON THE BERYL INSTITUTE BENCHMARKING
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Pediatric Collaborative Executive Summary
 Pediatric Collaborative Executive Summary Twenty-seven pediatric organizations convened at the NRC Health Pediatric Collaborative at Texas Scottish Rite Hospital for Children in Dallas, Texas. This summary
Pediatric Collaborative Executive Summary Twenty-seven pediatric organizations convened at the NRC Health Pediatric Collaborative at Texas Scottish Rite Hospital for Children in Dallas, Texas. This summary
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
PDSA 2 Change Implemented: Work up room staff will write No on the Face sheet if family doesn t request SWE instead of leaving it blank.
 Improving Efficiency and Patient/Provider Satisfaction Through Standardization of School/Work Excuses in a Pediatric Resident Clinic, a Retrospective Chart Review Michael Tjahjadi, MD, PGY-2 Sara Sterne,
Improving Efficiency and Patient/Provider Satisfaction Through Standardization of School/Work Excuses in a Pediatric Resident Clinic, a Retrospective Chart Review Michael Tjahjadi, MD, PGY-2 Sara Sterne,
NHS Greater Glasgow and Clyde Alison Noonan
 NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
HOW TO CONDUCT GRANT SPRINTS
 HOW TO CONDUCT GRANT SPRINTS A more collaborative, efficient, and fun way to write proposals HOW TO CONDUCT GRANT SPRINTS A more collaborative, efficient, and fun way to write proposals The Grant Sprint
HOW TO CONDUCT GRANT SPRINTS A more collaborative, efficient, and fun way to write proposals HOW TO CONDUCT GRANT SPRINTS A more collaborative, efficient, and fun way to write proposals The Grant Sprint
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1
 EVALUATION Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1 Research Summary No. 9 March 2012 Introduction The current model of primary care in the United States is
EVALUATION Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1 Research Summary No. 9 March 2012 Introduction The current model of primary care in the United States is
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital. Final Report. Submitted To:
 Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes
 Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes Presented by: VIRGINIA FLINTOFT, Manager, Central Measurement Team, Canadian Patient Safety Institute NARDIA BROWN, Clinical
Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes Presented by: VIRGINIA FLINTOFT, Manager, Central Measurement Team, Canadian Patient Safety Institute NARDIA BROWN, Clinical
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond
 Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond Author Marilyn H. Oermann, PhD, RN, ANEF, FAAN Thelma M. Ingles Professor of Nursing, Duke University School of Nursing Editor, Journal
Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond Author Marilyn H. Oermann, PhD, RN, ANEF, FAAN Thelma M. Ingles Professor of Nursing, Duke University School of Nursing Editor, Journal
Service Agreements. Mike Davies, MD FACP
 Service Agreements Mike Davies, MD FACP In flow systems there is delay that is generated not only by the individual clinic both FOR and AT appointments (primary care or specialty care), but also by the
Service Agreements Mike Davies, MD FACP In flow systems there is delay that is generated not only by the individual clinic both FOR and AT appointments (primary care or specialty care), but also by the
A strategy for building a value-based care program
 3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
Supplemental materials for:
 Supplemental materials for: Krist AH, Woolf SH, Bello GA, et al. Engaging primary care patients to use a patient-centered personal health record. Ann Fam Med. 2014;12(5):418-426. ONLINE APPENDIX. Impact
Supplemental materials for: Krist AH, Woolf SH, Bello GA, et al. Engaging primary care patients to use a patient-centered personal health record. Ann Fam Med. 2014;12(5):418-426. ONLINE APPENDIX. Impact
Bluewater Health. Sarnia/Lambton, Ontario, Canada. Case Study
 Sarnia/Lambton, Ontario, Canada When began planning for a major renovation that combined two facilities under one roof and added five floors, they wanted maximum flexibility because they knew change was
Sarnia/Lambton, Ontario, Canada When began planning for a major renovation that combined two facilities under one roof and added five floors, they wanted maximum flexibility because they knew change was
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Increased situational awareness to reduce undetected deterioration
 Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
The Science of Emotion
 The Science of Emotion I PARTNERS I JAN/FEB 2011 27 The Science of Emotion Sentiment Analysis Turns Patients Feelings into Actionable Data to Improve the Quality of Care Faced with patient satisfaction
The Science of Emotion I PARTNERS I JAN/FEB 2011 27 The Science of Emotion Sentiment Analysis Turns Patients Feelings into Actionable Data to Improve the Quality of Care Faced with patient satisfaction
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Michigan Medicine--Frankel Cardiovascular Center. Determining Direct Patient Utilization Costs in the Cardiovascular Clinic.
 Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
A nurse s guide for successful care transition and handoff communication
 A nurse s guide for successful care transition and handoff communication August 2017 Contents A care transition story you may recognize 3 What to communicate and when 4 Pay extra-close attention to medication
A nurse s guide for successful care transition and handoff communication August 2017 Contents A care transition story you may recognize 3 What to communicate and when 4 Pay extra-close attention to medication
Creating Exceptional Physician-Nurse Partnerships
 1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
Best Practices: Access Case Management
 Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Reduction of Time from Admission to Initiation of Chemotherapy on Inpatient Hematology and Bone Marrow Transplant Services Presenter s Name: Ryan J. Mattison,
ASCO s Quality Training Program Project Title: Reduction of Time from Admission to Initiation of Chemotherapy on Inpatient Hematology and Bone Marrow Transplant Services Presenter s Name: Ryan J. Mattison,
Inpatient Flow Real Time Demand Capacity: Building the System
 Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Copyright American Psychological Association INTRODUCTION
 INTRODUCTION No one really wants to go to a nursing home. In fact, as they age, many people will say they don t want to be put away in a nursing home and will actively seek commitments from their loved
INTRODUCTION No one really wants to go to a nursing home. In fact, as they age, many people will say they don t want to be put away in a nursing home and will actively seek commitments from their loved
Value-based Care Report. February How Value-based Care is improving quality and health.
 Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Hospital Clinical Documentation Improvement
 Hospital Clinical Documentation Improvement March 2016 Clinical Documentation Improvement (CDI) is a team approach to improving documentation practices through ongoing education, concurrent chart review
Hospital Clinical Documentation Improvement March 2016 Clinical Documentation Improvement (CDI) is a team approach to improving documentation practices through ongoing education, concurrent chart review
PSAT/NMSQT. Chapter 4. How the PSAT/NMSQT and the SAT Are Linked
 Chapter 4 PSAT/NMSQT The PSAT/NMSQT (Preliminary SAT/National Merit Scholarship Qualifying Test) provides an excellent way to preview the SAT. Like the SAT, the redesigned PSAT/NMSQT will measure the skills
Chapter 4 PSAT/NMSQT The PSAT/NMSQT (Preliminary SAT/National Merit Scholarship Qualifying Test) provides an excellent way to preview the SAT. Like the SAT, the redesigned PSAT/NMSQT will measure the skills
WARNING: Up to 50% of the new patients calling your office may be lost due to the way your team handles that all-important initial phone call!
 TELEPHONE ETIQUETTE WARNING: Up to 50% of the new patients calling your office may be lost due to the way your team handles that all-important initial phone call! At the MasterPlan Alliance we taped new
TELEPHONE ETIQUETTE WARNING: Up to 50% of the new patients calling your office may be lost due to the way your team handles that all-important initial phone call! At the MasterPlan Alliance we taped new
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
Milton Keynes University Hospital NHS Foundation Trust
 Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN
 NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN Wisconsin Organization of Nurse Executives 2017 Annual Convention April 28, 2017 Barbara Pinekenstein DNP, RN-BC, CPHIMS Linsey Steege PhD Presentation
NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN Wisconsin Organization of Nurse Executives 2017 Annual Convention April 28, 2017 Barbara Pinekenstein DNP, RN-BC, CPHIMS Linsey Steege PhD Presentation
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Elderly Simplified Application Project Guidance
 Elderly Simplified Application Project Guidance Program Development Division FY2015-FY2016 What is the Elderly Simplified Application Project (ESAP) Demonstration? The Elderly Simplified Application Project
Elderly Simplified Application Project Guidance Program Development Division FY2015-FY2016 What is the Elderly Simplified Application Project (ESAP) Demonstration? The Elderly Simplified Application Project
13th Annual Meridian Nursing Research and Evidence Based Practice Conference 2017 General Guidelines for Abstract Submission
 Hackensack Meridian Ann May Center for Nursing 13 th Annual Meridian Nursing Research and Evidence Based Practice Conference Instructions for Submission All author information and abstract contents must
Hackensack Meridian Ann May Center for Nursing 13 th Annual Meridian Nursing Research and Evidence Based Practice Conference Instructions for Submission All author information and abstract contents must
Allied Healthcare (Scottish Borders) Housing Support Service Unit 3 Annfield Business Centre Teviot Crescent Hawick TD9 9RE
 Housing Support Service Unit 3 Annfield Business Centre Teviot Crescent Hawick TD9 9RE") Allied Healthcare (Scottish Borders) Housing Support Service Unit 3 Annfield Business Centre Teviot Crescent Hawick TD9 9RE Type of inspection: Unannounced Inspection completed on: 12 June 2014 Contents
Allied Healthcare (Scottish Borders) Housing Support Service Unit 3 Annfield Business Centre Teviot Crescent Hawick TD9 9RE Type of inspection: Unannounced Inspection completed on: 12 June 2014 Contents
Health Quality Ontario: Optimizing provincial feedback programs
 Health Quality Ontario: Optimizing provincial feedback programs Design Process, Challenges, and Lessons Learned Noah Ivers, MD CCFP PhD Family Physician, Women s College Hospital Family Health Team Scientist,
Health Quality Ontario: Optimizing provincial feedback programs Design Process, Challenges, and Lessons Learned Noah Ivers, MD CCFP PhD Family Physician, Women s College Hospital Family Health Team Scientist,
Improving Nurse-patient Communication about New Medicines
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
Project Step 3: Investigate the Process.
 103 Project Step 3:. Program Cycle The Big Picture Project Cycle After defi ning and documenting the aspect of care under review, project team members review the process from which the problem originated
103 Project Step 3:. Program Cycle The Big Picture Project Cycle After defi ning and documenting the aspect of care under review, project team members review the process from which the problem originated
Self-assessment surveys details & definitions
 Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
An Initiative to Improve Patient Discharge Satisfaction
 An Initiative to Improve Patient Discharge Satisfaction Speaker Disclosure Statement Sally Strong, RN, APN-CNS, CNRN, CRRN Clinical Nurse Specialist Marianjoy Rehabilitation Hospital Adjunct Faculty Elmhurst
An Initiative to Improve Patient Discharge Satisfaction Speaker Disclosure Statement Sally Strong, RN, APN-CNS, CNRN, CRRN Clinical Nurse Specialist Marianjoy Rehabilitation Hospital Adjunct Faculty Elmhurst
CMS Quality Program Overview
 CMS Quality Program Overview AMGA/Press Ganey Survey Collaboration September 13, 2012 Presenter Information Incorporated in 1985, Press Ganey was one of the first companies to provide patient satisfaction
CMS Quality Program Overview AMGA/Press Ganey Survey Collaboration September 13, 2012 Presenter Information Incorporated in 1985, Press Ganey was one of the first companies to provide patient satisfaction
Draft Community Outreach Plan for the Climate Action Plan Update
 Draft Community Outreach Plan for the Climate Action Plan Update PREPARED FOR 201 North Broadway Escondido, CA 92025 Project Contact Mike Strong, Assistant Planning Director (760) 839-4556 mstrong@escondido.org
Draft Community Outreach Plan for the Climate Action Plan Update PREPARED FOR 201 North Broadway Escondido, CA 92025 Project Contact Mike Strong, Assistant Planning Director (760) 839-4556 mstrong@escondido.org
Census Based Surveying for Today s Consumer-Driven Industry
 Census Based Surveying for Today s Consumer-Driven Industry Capturing the voice of every patient across the continuum of care provides a competitive advantage in an evolving marketplace. Summary The transformation
Census Based Surveying for Today s Consumer-Driven Industry Capturing the voice of every patient across the continuum of care provides a competitive advantage in an evolving marketplace. Summary The transformation
Getting Started Guide. Created by
 Getting Started Guide Created by December 2, 2016 Table of Contents 1 Getting Started... 2 2 Patient Overview... 2 2.1 Creating Patients... 2 2.2 Patient Information... 2 2.3 Visual Indicators... 3 2.3.1
Getting Started Guide Created by December 2, 2016 Table of Contents 1 Getting Started... 2 2 Patient Overview... 2 2.1 Creating Patients... 2 2.2 Patient Information... 2 2.3 Visual Indicators... 3 2.3.1
Profit = Price - Cost. TAKT Time Map Capacity Tables. Morale. Total Productive Maintenance. Visual Control. Poka-yoke (mistake proofing) Kanban.
 Kanban.") GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
Executive Summary. Leadership Toolkit for Redefining the H: Engaging Trustees and Communities
 Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
University of Michigan Health System
 University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
Pursuing the Triple Aim: CareOregon
 Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Team Building Storyboard Template
 Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient
Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient