A. Service Specifications
|
|
|
- Jessica Morrison
- 6 years ago
- Views:
Transcription
1 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: Service Gender Identity Services for Adults (Surgical Interventions) Commissioner Lead For local completion Provider Lead For local completion 1. Scope 1.1 Prescribed Specialised Service This service specification covers the provision of surgical interventions for individuals on the NHS pathway of care for gender reassignment. This service specification should be read in conjunction with NHS England s service specification for Gender Identity Services for Adults (Non-Surgical Interventions). 1.2 Description Gender Identity Surgical Services include specialist assessment, surgical interventions and immediate associated after care. 1.3 How the Service is Differentiated from Services Falling within the Responsibilities of Other Commissioners NHS England commissions gender identity disorder surgical services from Specialist Gender Identity Surgical Providers. This includes specialist assessment, surgery and immediate associated aftercare. Clinical Commissioning Groups are responsible for commissioning other surgical procedures that are not specialised and that may form the NHS pathway of care for transgender people (as described in this specification). 2. Care Pathway and Clinical Dependencies 2.1 Background The term currently used to describe a discrepancy between birth-assigned sex
2 and gender identity is gender incongruence; this term is preferable to the formerly-used terms of gender identity disorder and transsexualism. Gender incongruence is frequently, but not universally, accompanied by the symptom of gender dysphoria. Gender dysphoria is a cognitive symptom characterised by persistent concerns, uncertainties, and questions about gender identity, which become so intense as to seem to be the most important aspect of the affected individual s life. Affected individuals experience varying degrees of personal distress and dissatisfaction associated with gender that constitute the symptom, gender dysphoria. Since 2002 in the United Kingdom transsexualism has not been regarded as a mental health problem. Its trajectory is similar to the de-pathologisation of homosexuality, which was removed as a mental health diagnosis from the Diagnostic and Statistical Manual of Mental Disorders (DSM-II) in DSM- V, published in 2013, states that gender dysphoria, in itself, is not a mental health problem. The current version of the International Statistical Classification of Diseases and Related Health Problems identifies transsexualism (ICD 10 code F64) as: A disorder characterized by a strong and persistent cross-gender identification (such as stating a desire to be the other sex or frequently passing as the other sex) coupled with persistent discomfort with his or her sex (manifested in adults, for example, as a preoccupation with altering primary and secondary sex characteristics through hormonal manipulation or surgery). 2.2 Principles guiding the development of this service specification All individuals referred to a specialist surgical service may exercise full personal autonomy in respect of their gender identity and presentation; and must have equal access to the range of interventions described in this service specification. Equity of access and quality of care will be provided to all who need it regardless of age, gender expression or ethnicity unless there is evidence that these factors affect the appropriateness or effectiveness of the intervention / treatment. Each individual will receive timely and appropriate treatment, as a minimum in accordance with national waiting time requirements. Interventions will be personalised and based on shared decision making, with service flexibility to match the individual s needs. 2.3 Providers of specialised surgical services for individuals with gender dysphoria will: Provide a high quality service for trans people who may have gender dysphoria; and will observe and promote respect, dignity and equality for trans people. Provide a timely and sustainable service for trans people that meets the needs of the population, and incorporates the views of individuals. Work with specialist Gender Identity Clinics to ensure timely and effective treatments, including post-surgical care needs.
3 Achieve an integrated approach to care with specialist Gender Identity Clinics and ensure close links with other expert centres at national and international levels. Ensure timely and appropriate communications with services who are expected to provide other parts of the individual s pathway. Increase awareness of best practice in the treatment and management of gender dysphoria through active engagement with health professionals; and educate healthcare professionals in the health and support needs of trans people. Collaborate in national and international research projects to increase the evidence base for the commissioning and delivery of specialised services for trans people. Provide support, advice, expertise and training for the local, regional and national network. Collaborate in sharing best practice, peer review, benchmarking, and in the development of research and innovation. Employ consistent and equitable decision-making about the effective use of resources on the NHS pathway of care for trans people. Publicise local and national patient organisations, which can provide invaluable additional information and ongoing support for trans people and their families. 2.4 Staffing, structure and governance Each Provider will have: A nominated Senior Clinical Lead, who has the key leadership role for the service overall. The Senior Clinical Lead must demonstrate evidence of appropriate experience and expertise in specialised gender dysphoria practice (as a minimum this will be at least three years full time or equivalent experience in specialised gender dysphoria practice; significant management experience; and significant evidence of continued professional development). A specialist multi-disciplinary team of professionals. A core multi-disciplinary team will include surgeons with expertise in the procedures described in this service specification; consultant anaesthetists; consultant radiologists; and specialist nurses. The team will also include other clinicians with a mix of skills, experience and expertise that is appropriate to ensure the delivery of effective and high quality services in accordance with the requirements of this service specification. A robust system of clinical governance in place that ensures, inter alia, all clinical staff are trained in meeting the health needs of trans people, and deemed competent to deliver the interventions as per their role. A robust system of corporate governance, including a nominated senior manager, that demonstrates effective management, guidance, oversight and accountability by the host organisation (Board level or equivalent). Arrangements in place to ensure that services deliver culturally appropriate care and support; individuals must be able to access services in a way that ensures their cultural, spiritual, language and communication needs do not
4 prevent them from receiving the same quality of healthcare as others. Sufficient administrative and managerial support that facilitates efficient and timely delivery of services. Information and technology systems that enables the effective submission of data, including the reporting requirements of the national Referral to Treatment waiting time standards. Premises that are appropriate to ensure effective delivery of the services described in this service specification; and in an environment that service users regard as safe and welcoming. Arrangements in place (including ongoing training) to ensure that all staff in public-facing roles have cultural sensitivity towards trans and gender diverse people s health and social care needs. Arrangements in place to ensure that service improvement is shaped by active service user involvement, and be able to demonstrate how this is achieved via means that are accessible, transparent and inclusive. Arrangements in place to ensure that complaints by service users are acknowledged, investigated and responded to promptly; and that the means to complain are publicised and accessible. Systems that demonstrate how providers use audit, data management and analysis, service reviews (including peer reviews) and other intelligence to evaluate effectiveness and drive ongoing service improvement. 2.5 Care Pathway Care pathways for the assessment, diagnosis and treatment of individuals with gender dysphoria related to gender incongruence are described in the Good Practice Guidelines for the Assessment and Treatment of Adults with Gender Dysphoria 1.The model relies on access via primary care, and the principle of multidisciplinary and interdisciplinary teams and networks who work and collaborate in the provision of care. Gender Identity Clinics assess and diagnose individuals; directly provide some interventions and arrange for referrals to other services, including for medical and surgical treatments. Access to surgical intervention is only by referral from the specialist Gender Identity Clinic. Some elements of the NHS care pathway are delivered by nonspecialised services. A diagram of the pathway is at Appendix A. The NHS pathway of care may be summarised as: Referral to a specialist Gender Identity Clinic from primary, secondary or tertiary care Assessment for gender dysphoria, and diagnosis Individuals who meet the criteria for gender dysphoria related to gender incongruence are accepted on to the NHS care pathway and an individualised treatment plan is agreed Therapeutic interventions delivered by the specialist Gender Identity Clinic; and / or referral for interventions with other providers; which may 1 Royal College of Psychiatrists; 2013
5 include recommendations for prescribing hormone treatments, and surgical interventions Ongoing review and monitoring during and after interventions Conclusion of contact: discharge to primary care 2.6 Referral for surgical intervention Referrals for a surgical intervention must be made by a Lead Professional from a specialist Gender Identity Clinic that is commissioned by NHS England, with necessary accompanying clinical opinions as described in this service specification. See Appendix B. 2.7 Role of the specialist surgeon and surgical team The treating surgeon must have insight into each patient s history and the rationale that led to the referral for surgery. To that end, surgeons must demonstrate good communication with patients through multi-source feedback as part of their appraisal; and have close working relationships with NHS England-commissioned specialist, non-surgical gender dysphoria service providers and with other health professionals who have been actively involved in their clinical care. Surgeons must demonstrate evidence of continuing training and mentoring in the relevant techniques, reported through appraisal. Surgeons must perform a minimum of 20 procedures in a year of the general type commissioned from the provider (i.e. 20 masculinising chest surgery procedures and/or 20 masculinising genital reconstruction procedures, and/or 20 feminising genital reconstruction procedures), so that the skills of the entire unit are maintained. Surgeons must engage regularly (at least once a year) with a group of peers (with national or international peers working in another organisation or surgical team), and share and review data on caseload, outcomes and complications experienced in their practice. The group of peers must publish an annual report. Surgical teams must comply with contemporary, authoritative guidance on the management of gender dysphoria and specialised surgery intended to reduce gender dysphoria, including the Standards of Care of the World Professional Association for Transgender Health (version 7, 2011). 2.8 Infrastructure requirements Consultant-led clinical advice available 24 hours a day, 7 days per week Consultant anaesthetists Specialist nurses to support patients throughout the surgical pathway, as both in-patients and out-patients, from referral to discharge. The service will be co-located with the following services: Radiology (including computed tomography (CT) Scanning,
6 Magnetic resonance imaging (MRI), ultrasound and Doppler tests) Transfusion services Infection prevention and control The service will have access to the following services: Pain Service (age appropriate) Pathology services Respiratory physiotherapy service Physiotherapy Occupational Therapy Dietetics Psychological services relevant to surgery Arrangements will be in place for urgent or emergency transfers of in-patients to High Dependency Units and Intensive Care Units. Patients will be assessed and treated in a clinically-appropriate area. This will include giving the option of attending a separate clinic for patients on the gender dysphoria pathway or in a clinic separated in time from patients of a different group. A health professional member of the surgical team will be available during daytime working hours to provide non-urgent advice to patients, and other practitioners providing care to patients who are not currently in-patients of the specialist surgery provider unit, such as urgent and emergency care services, General Practitioners and Gender Identity Clinics. 2.9 Assessment for readiness for surgical interventions The surgeon will offer the patient a pre-operative consultation, and will provide them with information, and agree with them the surgical intervention to be provided, which will be consistent with the patient s gender expression goals, within the limits of what can reasonably be achieved with best surgical practice. See Appendix C Shared decision making Shared Decision Making is a process in which individuals, when they reach a decision point in their health care, can review all the treatment options available to them and participate actively with their healthcare professional in making that decision. The surgeon will provide individuals with the necessary information about all of the options available to them so that they may ask questions, explore the options available, and take a treatment route which best suits their needs and preferences and is clinically appropriate Consent to surgery The process of obtaining informed consent is an important aspect of ethical assessment and intervention, including the emotional, social and factual issues, so as to enable the individual to make informed decisions about the treatment options, benefits, material risks, and the alternatives to the
7 treatments proposed (including the option of having no treatment). Individuals must be given sufficient time to reflect on the clinical advice and the potential treatment options before deciding what is best for them. The Named Clinician and Lead Professional in the specialist Gender Identity Clinic will have previously made all efforts to ensure that individuals are aware of the longer-term consequences of the interventions offered to them. The consequences of treatment decisions can be significant and life-changing. The surgeon will obtain consent for the proposed intervention at a specific preoperative appointment, so as to allow an informed process and give the patient adequate time to consider any relevant options and alternatives. Each patient should receive detailed verbal, written and pictorial information on the following, in the context of the individual s own treatment goals: Different surgical techniques available (with option of referral to colleagues who provide alternative techniques) Advantages and disadvantages of each technique (cosmetic and functional) Limitations of a procedure to achieve ideal results Inherent risks and possible complications of the various techniques Appropriate aftercare 2.12 Nursing team The Provider will have a nursing team that is experienced in meeting the health care needs of trans people. The role of the nursing team should include pre-operative care, whereby contact is made before surgery and information is shared on aftercare including hygiene, risk of infection and general lifestyle considerations. Post-operative care involves wound and physical care, and liaison with community and primary care services around the time of discharge from hospital Surgical interventions that are commissioned by NHS England, and referral criteria The Provider will deliver certain surgical interventions intended to reduce gender dysphoria, and improve health, quality of life and social functioning in people who have gender dysphoria that is a consequence of incongruence between their identity, and their biologically-determined sex characteristics and the social role traditionally expected of people with such biologicallydetermined sex characteristics. Surgery may be combined with other surgical procedures if: the eligibility criteria for each procedure are fulfilled; it is appropriate in the clinical judgment of the surgeon; and this is the patient s preference. If a surgeon recommends a multi-staged reconstructive procedure, the reasons should be explained to the patient and they should be given the option of a single or fewer-staged procedure, either at the same unit or elsewhere. The Provider must offer a range of surgical techniques and must ask the referrer to re-refer the patient to an alternative provider if a technique that is not offered by their unit is in their patient s best interests and is more likely to
8 fulfil the individual s treatment goals. The following specialist surgery and immediate associated after care is commissioned by NHS England: Masculinising chest surgery Masculinising and feminising genital reconstructive surgery Orchidectomy The criteria for initiation of surgical treatments are listed in Appendix D. Masculinising chest surgery Surgeons providing masculinising chest surgery must be trained in oncoplastic breast surgery or be plastic surgeons with expertise in plastic surgery of the breast (undertaking a minimum of 20 similar procedures per annum). The standard practice 2 procedures that are commissioned by NHS England are: Double Incision Technique Peri-Areolar Technique Liposuction for the purpose of masculinising chest surgery Nipple re-positioning techniques, including pedicled flaps Free, full-thickness nipple grafting Modification of the nipple-areolar complex Dermal implant and nipple tattoo Masculinising genital surgery The standard practice 3 procedures commissioned by NHS England are: Phalloplasty (various types) Metoidioplasty (with/without urethroplasty; with/without scrotoplasty) Post-operative training in penile prosthesis use Commissioned only as components of the above procedures: o Hysterectomy o Bilateral Salpingo-oophorectomy o Vaginectomy o Placement of penile prosthesis (various types) 2 If a Provider wishes to implement a new surgical intervention it must a) be determined whether a NICE Interventional Procedure Guidance is in place and b) propose to NHS England s Clinical Reference Group for Gender Identity that a proposition for a clinical commissioning policy be developed. 3 If a Provider wishes to implement a new surgical intervention it must a) be determined whether a NICE Interventional Procedure Guidance is in place and b) propose to NHS England s Clinical Reference Group for Gender Identity that a proposition for a clinical commissioning policy be developed.
9 o Placement of testicular prosthesis (various types) o Glans sculpting Hysterectomy (removal of uterus) and bilateral salpingo-oophorectomy (removal of ovaries and fallopian tubes) are interventions commissioned under this service specification when they are performed by a specialist Gender Identity surgical unit simultaneously with the genital surgical interventions for the purpose of the alleviation of gender dysphoria (described above). They are not commissioned by NHS England when they are performed as stand alone procedures; in such cases commissioning responsibility rests with the individual s Clinical Commissioning Group. Feminising genital surgery The standard practice 4 procedures commissioned by NHS England are feminising genital reconstruction, consisting of some or all of the following: Penectomy Bilateral Orchidectomy Vaginoplasty (various techniques; bowel vaginoplasty should only be performed if other vaginoplasty techniques are not possible because of inadequate donor site skin) Clitoroplasty Vulvoplasty 2.14 Surgical procedures that are not routinely commissioned by NHS England o Phonosurgery o Augmentation Mammoplasty o Facial Feminisation Surgery, including Thyroid Chondroplasty and Rhinoplasty o Lipoplasty / Contouring, Microdermabrasion and other cosmetic procedures o Body hair removal (other than donor site for surgery) o Hair transplantation o Hysterectomy and bilateral salpingo-oophorectomy when they are performed as stand alone procedures o Corrective surgical procedures relating to complications for poor outcomes that are recognised after 18 months of previous surgery o Reversal of a previous gender reassignment surgical intervention (i.e. patients who are satisfied with the surgical outcome at the time of discharge and become dissatisfied with their decision at a later 4 If a Provider wishes to implement a new surgical intervention it must a) be determined whether a NICE Interventional Procedure Guidance is in place and b) propose to NHS England s Clinical Reference Group for Gender Identity that a proposition for a clinical commissioning policy be developed.
10 date) 2.15 Patient dissatisfaction with technical outcome of surgery (all procedures) Readmissions for treatment of complications for poor outcomes that are recognised within 18 months of previous specialised surgery will be provided by the original provider. Should the patient not wish to continue treatment with the surgeon who performed the primary procedure, the surgeon should refer them directly to another surgeon working in an NHS England-commissioned, surgical unit, requesting that they provide a second opinion regarding options for achieving an acceptable outcome. The choice of surgeon who will provide any further treatment or revision procedure must be discussed and agreed with the patient. If a patient reports problems or concerns related to surgery, and if more than 18 months has elapsed since the last specialist surgical procedure or revision, the patient should be referred directly to a relevant non-specialist provider (for example, a gynaecology urology service) for assessment, management and onward referral to another surgeon if appropriate. Subsequent surgical interventions are commissioned by the individual s Clinical Commissioning Group as they are not interventions performed for the alleviation of gender dysphoria related to gender incongruence. NHS England does not have a commissioning policy for the reversal of previous gender reassignment surgical interventions that are requested by the individual (i.e. patients who are satisfied with the surgical outcome at the time of discharge and become dissatisfied with their decision at a later date) Donor Site Skin Epilation Some, but not all patients having genital surgery (masculinising and feminising) require donor site skin epilation. The assessment of need is made by the surgical team. If it is necessary, the surgical team will refer patients requiring donor site skin epilation to a provider of epilation services. Arrangements for epilation should be initiated as soon as the decision is made to offer surgery. Epilation is provided exclusively for the purpose of reducing the risk of poor surgical outcome. Laser epilation will be used for patients with pigmented hair, unless it is demonstrated as ineffective or poorly tolerated by the patient. Electrolysis will only be used for patients who have depigmented or very fair hair, or have not tolerated laser epilation or have found it to be ineffective. The surgical team will collaborate with the epilation provider to assess when treatment is complete; as candidates for surgery are likely to have a typicallymale serum testosterone level, the surgical team will observe the donor site skin for hair re-growth for a period of three months after cessation of epilation treatment, before making a clinical judgment regarding the permanency of epilation Discharge from the surgical provider The Provider will provide and/or arrange any pre-operative assessments or preparatory interventions necessary for a good surgical outcome. The
11 surgeon will provide written reports to the referrer, with copies to the patient and the GP, following assessment, surgery and at discharge; they will provide additional written reports describing any other clinically-significant event or contact with the patient. Information that is relevant to ongoing good health will be given to the individual, such as information on: breast awareness; risk of cancers; and the potential benefits of regular screening. Recommendations for wound care and the use of specialised wound care products will be made by the surgical team, directly to the patient s GP. Patients may be discharged from routine surgical follow up when this is clinically appropriate but Providers will provide open access review at the request of the patient, referrer or the patient s GP for at least one year after surgery Interdependence with other Services Links with other services include: Providers of non-surgical interventions for individuals with gender dysphoria Epilation providers 3. Population Covered and Population Needs 3.1 Population Covered By This Specification The service outlined in this specification is for patients ordinarily resident in England; or otherwise the commissioning responsibility of the NHS in England (as defined in guidance for Establishing the Responsible Commissioner and other Department of Health guidance relating to patients entitled to NHS care or exempt from charges). For the purposes of commissioning health services, this excludes patients who, whilst resident in England, are registered with a GP practice in Wales, but includes patients resident in Wales who are registered with a GP practice in England. The Provider will receive referrals from a specialised Gender Identity Service (that is commissioned by NHS England) of individuals from 17 years of age of individuals who have a diagnosis of gender dysphoria that is a consequence of their gender identity being incongruent with their visible sex characteristics and/or the social role typically associated with those characteristics (gender incongruence). This specification recognises and respects diversity in gender identity and its expression. It recognises that there are other identities than the traditional (binary) identities associated with man and woman, and that gender diverse people with such identities (and who are known by a variety of other names, including non-binary, trans-feminine, trans-masculine, Genderqueer, nongender and others) must have access to treatment and the interventions described in this document that is equitable to the access available to people with binary identities. 3.2 Population needs; and Expected Demographic Changes There is no official data on the number of people in England who present with
12 a degree of gender variance. Difficulties in assessing prevalence are exacerbated by the limited evidence base. There is considerable variation in reported prevalence due to factors such as: variable data reporting by providers; differences in diagnostic thresholds applied and inconsistent terminology; the methodology and diagnostic classification used; and the year and country in which the studies took place. A literature review by Public Health England in provides a prevalence estimate of gender dysphoria in the United Kingdom of between 4.6 and 1200 per 100,000 people; it acknowledges that the lower prevalence estimate must be interpreted with caution as it considers historical data of over fifty years. A Home Office funded study in 2009 suggests prevalence for England of around 20 per 100,000 population 6. Thus there is considerable variation in estimates, and the absence of reliable prevalence data exacerbates the challenges in planning and commissioning gender identity services. What is consistent across the literature is a recognition that the number of people pursuing treatment options the incidence of expressed need - is rising significantly. The number of referrals to adult gender identity services in England increased by 178% between 2011/12 and 2016/17 7. The reasons for the increased numbers are unclear, though often surmised that it is attributable to: increased availability of treatment interventions; changing societal attitudes; a new cohort of non-binary people accessing services; and greater awareness. 4. Outcomes and Applicable Quality Standards NHS Outcomes Framework Domains Domain 1 Domain 2 Domain 3 Domain 4 Domain 5 Preventing people from dying prematurely Enhancing quality of life for people with longterm conditions Helping people to recover from episodes of illhealth or following injury Ensuring people have a positive experience of care Treating and caring for people in safe environment and protecting them from avoidable harm 4.2 Indicators Include: 5 Unpublished 6 Gender Variance in the UK; Gender Identity Research and Education Society; NHS England; April 2017
13 Number Indicator Data Source Outcome Framework Domain CQC Key question Clinical Outcomes 101 For masculinising chest surgery the % of revisions undertaken over a 12 month period. 102 % of planned multistage procedures undertaken for patients receiving masculinising chest surgery. 103 For masculinising genital surgery the % of revisions undertaken over a 12 month period. 104 % of planned multistage procedures undertaken for patients receiving masculinising genital surgery. 105 For feminising genital surgery the % of revisions undertaken over a 12 month period. 106 % of patients referred for second opinion Patient Experience HES 2, 3, 4 Effective, HES 2, 3, 4 Effective, HES 2, 3, 4 Effective, HES 2, 3, 4 Effective, HES 2, 3, 4 Effective, HES 4, 5 Safe, effective, caring, 201 Patient feedback Selfdeclaration 202 Patient information Selfdeclaration 4 Effective, caring, 4 Effective,
14 Structure and Process 301 A patient is cared for in a multi-disciplinary environment, and there is a multidisciplinary support available. 302 Continued professional development 303 Access to a named nurse Selfdeclaration Selfdeclaration Selfdeclaration 304 Patient pathway Selfdeclaration 305 Clinical audit Selfdeclaration 1, 2, 3, 4, 5 Safe, effective, caring,, well-led 1, 2, 3, 4 Safe, effective 1, 2, 3, 4 Safe, effective, caring, 1, 2, 3, 4, 5 Safe, effective, caring, 1, 2, 3, 4 Safe, effective, caring. See Appendix E for more detailed description of the indicators

15 Appendix A
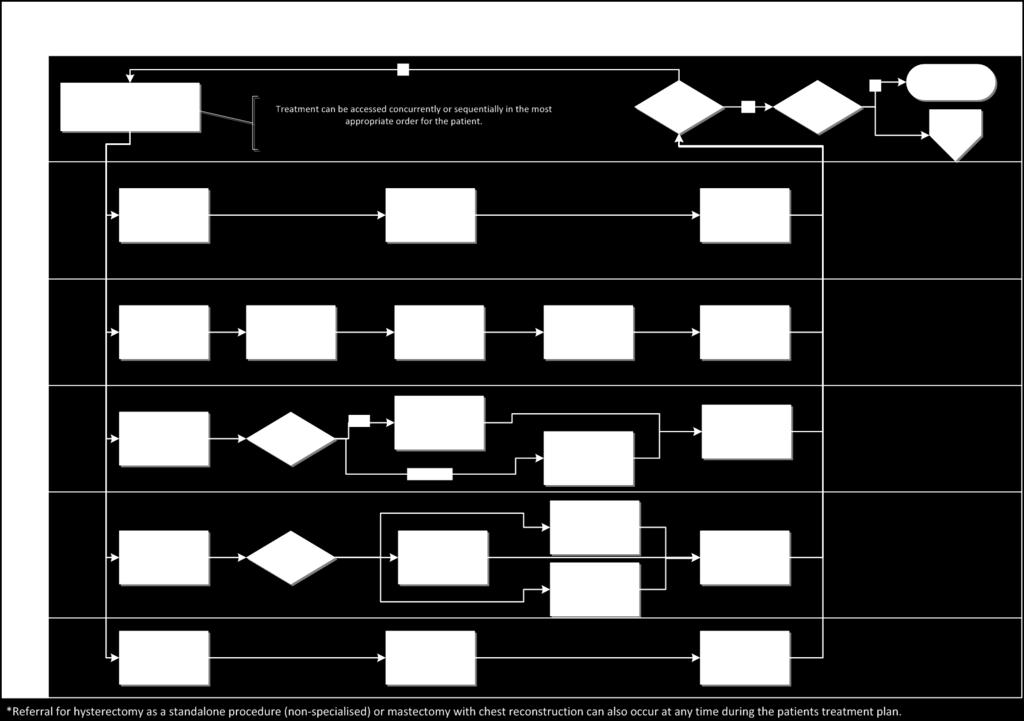
16

17 Corrective surgery after 18 months is a CCG commissioning responsibility
18 Appendix B: Referral for surgical intervention Referrals for a surgical intervention must be made by a Lead Professional from a specialist Gender Identity Clinic that is commissioned by NHS England, with necessary accompanying clinical opinions as described in this service specification. A decision about an individual s suitability for surgical interventions to alleviate gender dysphoria requires careful assessment and support from a specialist multidisciplinary team, taking into account medical, psychological, emotional and social issues in combination. As such, and given the potential range of complexities that may be experienced by individuals on the NHS pathway of care and the potential treatments, referrals to the specialist surgical team will not be accepted from other health professionals or other health services. Before a referral for surgery is made, the Lead Professional in the Gender Identity Clinic will have met with the individual to review current treatment interventions, and to assess the individual s needs and readiness for the surgical intervention, both as described in the criteria below and as an assessment of the individual s physical health generally. The processes of shared decision making and of obtaining consent (as described earlier in this document) will provide the patient with necessary information, and will allow the individual sufficient time to ask questions, and to reflect on the advice of the Lead Professional to enable an informed decision on the treatment options, risks and benefits.
19 Appendix C: Assessment for readiness for surgical interventions The surgeon will offer the patient a pre-operative consultation, and will provide them with information, and agree with them the surgical intervention to be provided, which will be consistent with the patient s gender expression goals, within the limits of what can reasonably be achieved with best surgical practice. It is the surgeon s responsibility to determine that an individual is sufficiently healthy, physically and psychologically, to undergo surgery. If the surgeon has any doubts about the appropriateness of surgery, the surgeon will consult with the referrer before proceeding further. Patients will undergo the relevant pre-op laboratory tests according to local protocol. The patient s GP will normally be asked to arrange these tests locally. Assessment of patients who have been granted a Gender Recognition Certificate The Gender Recognition Act 2004 enables a trans person to apply to the Gender Recognition Panel to receive a Gender Recognition Certificate. Individuals who are granted a full Gender Recognition Certificate are considered in the eyes of the law to be of their acquired gender and they are entitled to all the rights appropriate to a person of their acquired gender. An individual with a Gender Recognition Certificate will already have obtained a clinical diagnosis of gender dysphoria (as that is a requirement for the granting of a Gender Recognition Certificate). As such, the assessment and diagnosis element of the individual s contact with the Provider will be adjusted to reflect the existing diagnosis of gender dysphoria. Possession of a Gender Recognition Certificate does not in itself provide the multidisciplinary team with the clinical information that is necessary to assess an individual s suitability and readiness for the interventions that are available along the NHS pathway of care. As such, individuals with a Gender Recognition Certificate will be assessed for readiness of interventions, including surgical interventions, as otherwise described in this service specification and will include the individual s: Expectations of the interventions and how they will impact upon them socially and psychologically Health history Understanding of the interventions and their potential benefits, risks and limitations Support network and strategies for thriving after the intervention Plans for preparation and aftercare following intervention
20 Appendix D: Criteria for initiation of surgical treatments Criteria for mastectomy and creation of a male chest (requires one letter of referral from a Lead Professional): Persistent, well-documented gender dysphoria Capacity to make a fully informed decision and to consent for treatment Aged 17 years or older If significant medical or mental health concerns are present, they must be reasonably well controlled o Hormone therapy is not a pre-requisite o It is not a requirement for access to masculinising chest surgery to undertake a change in social role Consensus opinion amongst surgeons is that prior treatment with testosterone for a period of six to nine months results in tissue changes that make masculinising chest surgery easier and may improve outcome. This is an expert-opinion based observation and is not supported by research evidence. Patients may wish to take this opinion into consideration when planning their surgery but prior treatment with testosterone is not a requirement and, in some cases, may be inconsistent with patients other goals for gender expression. Criteria for genital surgery (requires two letters of referral: one from a Lead Professional, the other from a similarly-qualified and experienced professional not directly involved in the individual s care and able to form an independent opinion; at least one letter of referral must be from a medical practitioner) Masculinising genital surgery Persistent, well documented gender dysphoria Capacity to make a fully informed decision and to consent for treatment Age 17 years or older If significant medical or mental health concerns are present, they must be well controlled 12 continuous months of hormone therapy as appropriate to the patient s gender goals (unless the patient has a medical contraindication or is otherwise unable or unwilling to take hormones) 12 continuous months of living in a gender role that is congruent with their gender identity; this must not entail a requirement for the individual to conform to externally imposed or arbitrary preconceptions about gender identity and presentation; this requirement is not about qualifying for surgery, but rather preparing and supporting the individual to cope with the profound consequences of surgery; where individuals can demonstrate that they have been living in their gender role before the referral to the Provider, this must be taken into account. Consensus opinion amongst surgeons is that prior treatment with testosterone for a period of two years results in tissue changes, such as clitoral growth, that make masculinising genital surgery easier and may improve outcome. It may also identify
21 the potential for hair growth on donor site skin that might be internalised during surgery. This is an expert-opinion based observation and is not supported by research evidence. Patients may wish to take this opinion into consideration when planning their surgery but prior treatment with testosterone is not a requirement and, in some cases, may be inconsistent with patients other goals for gender expression. Feminising genital surgery Persistent, well documented gender dysphoria Capacity to make a fully informed decision and to consent for treatment Age 17 years or older If significant medical or mental health concerns are present, they must be well controlled 12 continuous months of hormone therapy as appropriate to the patient s gender goals (unless the patient has a medical contraindication or is otherwise unable or unwilling to take hormones); the aim of hormone therapy prior to orchidectomy is primarily to introduce a period of reversible oestrogen or testosterone suppression, before the individual undergoes irreversible surgical intervention 12 continuous months of living in a gender role that is congruent with their gender identity; this must not entail a requirement for the individual to conform to externally imposed or arbitrary preconceptions about gender identity and presentation; this requirement is not about qualifying for surgery, but rather preparing and supporting the individual to cope with the profound consequences of surgery; where individuals can demonstrate that they have been living in their gender role before the referral to the Provider, this must be taken into account Patients who smoke Consensus opinion amongst surgeons is that patients should not smoke for six weeks prior to surgery and for at least six weeks after surgery, particularly if they are having reconstructive surgery that involved the creation of pedicle flaps. Smoking increases risk of perioperative complications but also of major skin and tissue loss. For patients who smoke, a referral to a surgeon may still be made and an individualised discussion of risk and likely outcome included in the pre-operative counselling and consent process. Patients who are overweight A patient being significantly overweight increases their risk of peri-operative complication and may compromise the outcome of their surgery. Consensus opinion amongst surgeons is that patients with a BMI of 30 or more should lose weight before having genital surgery; and patients with a BMI of 40 or more should lose weight before having masculinising chest surgery. Referral to a surgeon may still be made and an individualised discussion of risk and likely outcome included in the preoperative counselling and consent process.
22 Appendix E - indicators Number Indicator Descriptor Notes Evidence documents Clinical Outcomes - quantitative data where possible using national data need to minimise the burden 101 For masculinising chest surgery the % of revisions undertaken over a 12 month period. 102 % of planned multi-stage procedures undertaken for patients receiving masculinising chest surgery. For masculinising chest surgery the % of revisions/complications undertaken over a 12 month period. For masculinising chest surgery the % of planned multi-stage procedures undertaken. Revision procedures and treatments for complications or poor outcomes that are recognised within 12 months Annual Report Annual Report Data source Domain CQC question HES 2, 3, 4 Effective, HES 2, 3, 4 Effective,
23 103 For masculinising genital surgery the % of revisions undertaken over a 12 month period. For the masculinising of genital surgery the % of revisions/complication rate undertaken over a 12 month period. Revision procedures and treatments for complications or poor outcomes that are recognised within 12 months Annual Report HES 2, 3, 4 Effective, 104 % of planned multi-stage procedures undertaken for patients receiving masculinising genital surgery. % of planned multistage procedures undertaken for patients receiving masculinising genital surgery. Annual Report HES 2, 3, 4 Effective,
24 105 For feminising genital surgery the % of revisions undertaken over a 12 month period. For feminising genital surgery the % of revisions undertaken over a 12 month period. Revision procedures and treatments for complications or poor outcomes that are recognised within 12 months Annual Report HES 2, 3, 4 Effective, 106 % of patients referred for second opinion 201 Patient feedback Annual Report Patient Experience - PROMS PREMS can be difficult to gather if no national survey can put in process indicator if required The provider has undertaken an exercise to obtain feedback from patients. Operational Policy HES 4, 5 Safe, effective, caring, % of patients, where not satisfied with procedure, referred to a second opinion postsurgery Selfdeclaration 4 Effective, caring,
25 202 Patient information Patient information is provided to all patients and includes details as listed in the service specification. different surgical techniques available (with referral to colleagues who provide alternative options) advantages and disadvantages of each technique limitations of a procedure to achieve ideal results; inherent risks and possible complications of the various techniques appropriate aftercare Operational Policy Structure and Process - infrastructure requirements, staffing, facilities etc Selfdeclaration 4 Effective,
26 301 A patient is cared for in a multidisciplinary environment, and there is a multidisciplinary support available. A patient is cared for in a multi-disciplinary environment, and there is a multi-disciplinary support available including: A nominated lead Clinician Surgeon Anaesthetist Operational Policy Selfdeclaration 1, 2, 3, 4, 5 Safe, effective, caring,, well-led Specialist Nurse Psychologist 302 Continued professional development Surgeons should demonstrate evidence of continuing training and mentoring in the relevant techniques and engage at least annually with national or international peers working in another organisation or surgical team. Operational Policy Selfdeclaration 1, 2, 3, 4 Safe, effective 303 Access to a named nurse There should be a named specialist nurse to support patients throughout the surgical pathway, from referral to discharge. Operational Policy Selfdeclaration 1, 2, 3, 4 Safe, effective, caring,
27 304 Patient pathway There should be a patient pathway in place as per the service specification. Operational Policy Selfdeclaration 1, 2, 3, 4, 5 Safe, effective, caring, 305 Clinical audit The team participates in clinical audit activity on an annual basis Operational Policy Selfdeclaration 1, 2, 3, 4 Safe, effective, caring.
A. Psychotherapy may be considered medically necessary as a treatment of gender dysphoria.
 UNIFORM MEDICAL PLAN TRANSGENDER SERVICES CLINICAL CRITERIA AND POLICY Uniform Medical Plan enrollees must refer to Regence Medical Policy No. 153 for all aspects of coverage of Transgender Services with
UNIFORM MEDICAL PLAN TRANSGENDER SERVICES CLINICAL CRITERIA AND POLICY Uniform Medical Plan enrollees must refer to Regence Medical Policy No. 153 for all aspects of coverage of Transgender Services with
Interim NHS England Gender Dysphoria Protocol and Service Guideline 2013/14 CPAG Approved
 Interim NHS England Gender Dysphoria Protocol and Service Guideline 2013/14 CPAG Approved 12-7-13 1 Contents No Item Page 1. Introduction 3 2. Protocol 3 2.1 Protocol Flow Chart 4 2.2 Protocol Notes 5
Interim NHS England Gender Dysphoria Protocol and Service Guideline 2013/14 CPAG Approved 12-7-13 1 Contents No Item Page 1. Introduction 3 2. Protocol 3 2.1 Protocol Flow Chart 4 2.2 Protocol Notes 5
Enter CRG document code
 Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review Enter CRG document code Gender Identity Services Steve Hamer The name of the individual leading on the service for
Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review Enter CRG document code Gender Identity Services Steve Hamer The name of the individual leading on the service for
Kaiser Foundation Health Plan of Washington Options, Inc. Federal Employees and Retirees Omni PPO Plan. Prior Authorizations
 Kaiser Foundation Health Plan of Washington Options, Inc. Federal Employees and Retirees Omni PPO Plan Prior Authorizations The Kaiser Foundation Health Plan of Washington Options, Inc. FEHB Omni PPO provides
Kaiser Foundation Health Plan of Washington Options, Inc. Federal Employees and Retirees Omni PPO Plan Prior Authorizations The Kaiser Foundation Health Plan of Washington Options, Inc. FEHB Omni PPO provides
Dr Gale Bearman Brisbane Gender Clinic
 Dr Gale Bearman Brisbane Gender Clinic Models of Clinical Care How to people with diverse gender identities obtain clinical care? How can professionals get started in providing clinical care? Wpath Standards
Dr Gale Bearman Brisbane Gender Clinic Models of Clinical Care How to people with diverse gender identities obtain clinical care? How can professionals get started in providing clinical care? Wpath Standards
BARIATRIC SURGERY SERVICES POLICY
 BARIATRIC SURGERY SERVICES POLICY Please note that all Central Lancashire Clinical Commissioning Policies are currently under review and elements within the individual policies may have been replaced by
BARIATRIC SURGERY SERVICES POLICY Please note that all Central Lancashire Clinical Commissioning Policies are currently under review and elements within the individual policies may have been replaced by
Breast Reduction. Individual Funding Request (IFR) Policy
 Policy") Breast Reduction Individual Funding Request (IFR) Policy Date of Adoption: 13 July 2016 Version: 1617 v2 Document Control Title of document Breast Reduction Individual Funding Request (IFR) Policy Authors
Breast Reduction Individual Funding Request (IFR) Policy Date of Adoption: 13 July 2016 Version: 1617 v2 Document Control Title of document Breast Reduction Individual Funding Request (IFR) Policy Authors
GENDER- AFFIRMING SURGERY AT METROPOLITAN. A Complete Guide
 GENDER- AFFIRMING SURGERY AT METROPOLITAN A Complete Guide The LGBTQ Health Center at Metropolitan offers a dedicated space where LGBTQ and especially TGNC patients can access affirming health care services.
GENDER- AFFIRMING SURGERY AT METROPOLITAN A Complete Guide The LGBTQ Health Center at Metropolitan offers a dedicated space where LGBTQ and especially TGNC patients can access affirming health care services.
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
MEDICAL COUNCIL OF NEW ZEALAND
 MEDICAL COUNCIL OF NEW ZEALAND NOVEMBER 2017 www.mcnz.org.nz Statement on cosmetic procedures Purpose of this statement 1. This statement outlines the standards expected of doctors who perform cosmetic
MEDICAL COUNCIL OF NEW ZEALAND NOVEMBER 2017 www.mcnz.org.nz Statement on cosmetic procedures Purpose of this statement 1. This statement outlines the standards expected of doctors who perform cosmetic
National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England. Core Values and Principles
 National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England Core Values and Principles Contents Page No Paragraph No Introduction 2 1 National Policy on Assessment 2 4 The Assessment
National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England Core Values and Principles Contents Page No Paragraph No Introduction 2 1 National Policy on Assessment 2 4 The Assessment
Wig and Hair Replacement Policy
 Leeds CCGs Wigs and Hair Replacement Policy 2016-19 Wig and Hair Replacement Policy Version: 2016-19 Ratified by: NHS Leeds West CCG Assurance Committee on; 16 vember 2016 NHS Leeds rth CCG Governance
Leeds CCGs Wigs and Hair Replacement Policy 2016-19 Wig and Hair Replacement Policy Version: 2016-19 Ratified by: NHS Leeds West CCG Assurance Committee on; 16 vember 2016 NHS Leeds rth CCG Governance
Health Sciences Centre, Team C, Dr. M. Wells (Breast and Hernia) Medical Expert
 Medical Expert") Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Policy for Cosmetic Surgery Removal Benign (non-cancerous) or Congenital Skin Lesions
 or Congenital Skin Lesions") NHS Birmingham CrossCity Clinical Commissioning Group NHS Birmingham South Central Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Solihull Clinical Commissioning
NHS Birmingham CrossCity Clinical Commissioning Group NHS Birmingham South Central Clinical Commissioning Group NHS Sandwell and West Birmingham Clinical Commissioning Group NHS Solihull Clinical Commissioning
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service
 Service") DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
Guidelines for the appointment of. General Practitioners with Special Interests in the Delivery of Clinical Services. Respiratory Medicine
 Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Specialised Services Service Specification: Inherited Bleeding Disorders
 Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Policy for Procedures of Limited Clinical Benefit (including low priority treatments)
") APPENDIX 1 Policy for Procedures of Limited Clinical Benefit (including low priority treatments) Please read in conjunction with the Policy for Individual Funding for Treatments outside Commissioned Services
APPENDIX 1 Policy for Procedures of Limited Clinical Benefit (including low priority treatments) Please read in conjunction with the Policy for Individual Funding for Treatments outside Commissioned Services
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
Research from the Health Protection Agency
 Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
Creating a person-centered transgender care program Kaiser Permanente
 Creating a person-centered transgender care program Kaiser Permanente IHI National Forum December 13, 2017 Session E2/D2 These presenters have nothing to disclose. 1 Presenters Erica Metz, MD She/her/hers
Creating a person-centered transgender care program Kaiser Permanente IHI National Forum December 13, 2017 Session E2/D2 These presenters have nothing to disclose. 1 Presenters Erica Metz, MD She/her/hers
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Anti-Coagulation Monitoring (warfarin, acenocoumarol, phenindione) Primary Care Service (PCS:01) NHS Standard Contract Service Profile Pack ( )
 Primary Care Service (PCS:01) NHS Standard Contract Service Profile Pack ( )") Anti-Coagulation Monitoring (warfarin, acenocoumarol, phenindione) Primary Care Service (PCS:01) This pack contains: Standard Contract Service Profile Pack () 1. Service Specification: (to be inserted
Anti-Coagulation Monitoring (warfarin, acenocoumarol, phenindione) Primary Care Service (PCS:01) This pack contains: Standard Contract Service Profile Pack () 1. Service Specification: (to be inserted
#NeuroDis
 Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
DRAFT - NHS CHC and Complex Care Commissioning Policy.
 DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
Final. Andrew McMylor / Dr Nicola Jones
 NHS Standard Contract - Service Specification Service Specification Service Final 24hour Ambulatory Blood Pressure Monitoring (24hrABPM) Commissioner Lead Lead Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
NHS Standard Contract - Service Specification Service Specification Service Final 24hour Ambulatory Blood Pressure Monitoring (24hrABPM) Commissioner Lead Lead Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
How NICE clinical guidelines are developed
 Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
Clinical Nurse Specialist Breast Cancer & Breast Reconstruction
 Date : January 2018 Position Title : Clinical Nurse Specialist - Department : Surgical Services. Location : Waitemata District Health Board Reporting To : Head of Division Nursing Surgical and Ambulatory
Date : January 2018 Position Title : Clinical Nurse Specialist - Department : Surgical Services. Location : Waitemata District Health Board Reporting To : Head of Division Nursing Surgical and Ambulatory
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Breast Asymmetry Surgery (Female)
") Breast Asymmetry Surgery (Female) Individual Funding Request (IFR) Policy Date of Adoption: 13 July 2016 Version: 1617 v2 Document Control Title of document Breast Asymmetry (female) Individual Funding
Breast Asymmetry Surgery (Female) Individual Funding Request (IFR) Policy Date of Adoption: 13 July 2016 Version: 1617 v2 Document Control Title of document Breast Asymmetry (female) Individual Funding
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE
 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE") NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
Jennifer Riley, Senior Commissioning Manager. Barry Silvert, Clinical Director Commissioning
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 7 Date of Meeting: 24 th June TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives) Pain
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 7 Date of Meeting: 24 th June TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives) Pain
Wandsworth CCG. Continuing Healthcare Commissioning Policy
 Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
53. MASTER OF SCIENCE PROGRAM IN GENERAL MEDICINE, UNDIVIDED TRAINING PROGRAM. 1. Name of the Master of Science program: general medicine
 53. MASTER OF SCIENCE PROGRAM IN GENERAL MEDICINE, UNDIVIDED TRAINING PROGRAM 1. Name of the Master of Science program: general medicine 2. Providing the name of level and qualification in the diploma
53. MASTER OF SCIENCE PROGRAM IN GENERAL MEDICINE, UNDIVIDED TRAINING PROGRAM 1. Name of the Master of Science program: general medicine 2. Providing the name of level and qualification in the diploma
Endometrial Cancer. Information for patients. Gynaecology Department. Feedback
 Feedback We appreciate and encourage feedback. If you need advice or are concerned about any aspect of care or treatment please speak to a member of staff or contact the Patient Advice and Liaison Service
Feedback We appreciate and encourage feedback. If you need advice or are concerned about any aspect of care or treatment please speak to a member of staff or contact the Patient Advice and Liaison Service
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Referral to Treatment (RTT) Access Policy
 Access Policy") General Referral to Treatment (RTT) Access Policy This is a controlled document and whilst this document may be printed, the electronic version posted on the intranet/shared drive is the controlled copy.
General Referral to Treatment (RTT) Access Policy This is a controlled document and whilst this document may be printed, the electronic version posted on the intranet/shared drive is the controlled copy.
PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Senior Manager, Performance and Compliance.
 UHB 033 Version No: 1 Previous Trust / LHB Ref No: Senior Manager, Performance and Compliance.") Reference No: PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Trust 364 Documents to read alongside this Policy. Ministerial Letter EH/ML/004/09 WAG Rules for Managing
Reference No: PATIENT ACCESS POLICY (ELECTIVE CARE) UHB 033 Version No: 1 Previous Trust / LHB Ref No: Trust 364 Documents to read alongside this Policy. Ministerial Letter EH/ML/004/09 WAG Rules for Managing
Adult Therapy Services. Community Services. Roundshaw Health Centre. Team Lead / Service Manager. Service Manager / Clinical Director
 THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
SERVICE SPECIFICATION
 SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 overview bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view
overview bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view
Hair Depilation. Individual Funding Request Policy. Date Adopted: March Version: 1516.v1. (Including laser therapy and electrolysis)
") Hair Depilation (Including laser therapy and electrolysis) Individual Funding Request Policy Date Adopted: March 2016 Version: 1516.v1 Document Control Title of document Hair Depilation Policy Authors
Hair Depilation (Including laser therapy and electrolysis) Individual Funding Request Policy Date Adopted: March 2016 Version: 1516.v1 Document Control Title of document Hair Depilation Policy Authors
Stage 2 GP longitudinal placement learning outcomes
 Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Section 6: Referral record headings
 Section 6: Referral record headings Referral record standards: the referral headings are primarily intended for recording the clinical information in referral communication between general practitioners
Section 6: Referral record headings Referral record standards: the referral headings are primarily intended for recording the clinical information in referral communication between general practitioners
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa
 Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary
 Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Refocusing CPA: a summary of the key changes. Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust
 Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
Final. Andrew McMylor / Dr Nicola Jones. Jeremy Fenwick, Battersea Healthcare CIC
 NHS Standard Contract - Service Specification Service Specification Service Commissioner Lead Lead Final Primary Care Based 12-Lead Electrocardiogram Service Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
NHS Standard Contract - Service Specification Service Specification Service Commissioner Lead Lead Final Primary Care Based 12-Lead Electrocardiogram Service Andrew McMylor / Dr Nicola Jones Jeremy Fenwick,
The Good Pain Medicine Specialist
 The Good Pain Medicine Specialist for Revalidation of Specialists in Pain Medicine FACULTY OF PAIN MEDICINE of the Royal College of Anaesthetists Revised April 2014 Table of Contents Introduction 3 Domain
The Good Pain Medicine Specialist for Revalidation of Specialists in Pain Medicine FACULTY OF PAIN MEDICINE of the Royal College of Anaesthetists Revised April 2014 Table of Contents Introduction 3 Domain
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
THE SERVICES. A. Service Specifications (B1) Ian Diley (Suffolk County Council)
 Ian Diley (Suffolk County Council)") THE SERVICES A. Service Specifications (B1) Service Specification No. Service Early Supported Discharge for Stroke Patients v5.0 Commissioner Lead Dr Mark Lim, T Woor (Suffolk Stroke Review Project Board)
THE SERVICES A. Service Specifications (B1) Service Specification No. Service Early Supported Discharge for Stroke Patients v5.0 Commissioner Lead Dr Mark Lim, T Woor (Suffolk Stroke Review Project Board)
Perioperative Nurse Coordinator Lead [Surgical]
![Perioperative Nurse Coordinator Lead [Surgical]](/thumbs/80/80543803.jpg "Perioperative Nurse Coordinator Lead [Surgical]") Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
COSMETIC BREAST SURGERY POLICY
 COSMETIC BREAST SURGERY POLICY Please note that all Central Lancashire Clinical Commissioning policies are currently under review and elements within the individual policies may have been replaced by the
COSMETIC BREAST SURGERY POLICY Please note that all Central Lancashire Clinical Commissioning policies are currently under review and elements within the individual policies may have been replaced by the
NHS. The guideline development process: an overview for stakeholders, the public and the NHS. National Institute for Health and Clinical Excellence
 NHS National Institute for Health and Clinical Excellence Issue date: April 2007 The guideline development process: an overview for stakeholders, the public and the NHS Third edition The guideline development
NHS National Institute for Health and Clinical Excellence Issue date: April 2007 The guideline development process: an overview for stakeholders, the public and the NHS Third edition The guideline development
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
Manchester University NHS Foundation Trust, Training Interface Group fellowship post in Oncoplastic Breast Surgery
 Introduction The fellowship programme is run through the Joint Committee on Surgical Training (JCST). Fellowship posts are open to all higher surgical and where appropriate, non-surgical trainees, that
Introduction The fellowship programme is run through the Joint Committee on Surgical Training (JCST). Fellowship posts are open to all higher surgical and where appropriate, non-surgical trainees, that
NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY
 PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Lozells Medical Practice Finch Road Primary Care Centre, Lozells,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Lozells Medical Practice Finch Road Primary Care Centre, Lozells,
The Scope of Practice of Assistant Practitioners in Ultrasound
 The Scope of Practice of Assistant Practitioners in Ultrasound Responsible person: Susan Johnson Published: Wednesday, April 30, 2008 ISBN: 9781-871101-52-2 Summary This document has been produced to provide
The Scope of Practice of Assistant Practitioners in Ultrasound Responsible person: Susan Johnson Published: Wednesday, April 30, 2008 ISBN: 9781-871101-52-2 Summary This document has been produced to provide
Our community nursing roles
 Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
St Monica s Specialist Breast Care Centre. Ethna Hickey- CNM2 Emma Holland- Specialist Breast Care Nurse Claire O Donnell-CNM1
 St Monica s Specialist Breast Care Centre Ethna Hickey- CNM2 Emma Holland- Specialist Breast Care Nurse Claire O Donnell-CNM1 Aims and objectives To provide an overview of the services of the Specialist
St Monica s Specialist Breast Care Centre Ethna Hickey- CNM2 Emma Holland- Specialist Breast Care Nurse Claire O Donnell-CNM1 Aims and objectives To provide an overview of the services of the Specialist
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP)
") Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP) Summary Helping you to get better sooner after surgery June 2012 Foreword These guidelines have been produced
Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP) Summary Helping you to get better sooner after surgery June 2012 Foreword These guidelines have been produced
Section 7: Core clinical headings
 Section 7: Core clinical headings Core clinical heading standards: the core clinical headings are those that are the priority for inclusion in EHRs, as they are generally items that are the priority for
Section 7: Core clinical headings Core clinical heading standards: the core clinical headings are those that are the priority for inclusion in EHRs, as they are generally items that are the priority for
Managing deliberate self-harm in young people
 Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
Job Description. Clinical Nurse Specialist in Breast care. An overview of Breast Cancer Services at the UPMC Beacon Hospital.
 Job Description Title: Clinical Nurse Specialist in Breast care Area of Assignment: Breast care Services Reports to: Oncology Unit Manager An overview of Breast Cancer Services at the UPMC Beacon Hospital.
Job Description Title: Clinical Nurse Specialist in Breast care Area of Assignment: Breast care Services Reports to: Oncology Unit Manager An overview of Breast Cancer Services at the UPMC Beacon Hospital.
Consultant to Consultant Referral Policy
 Consultant to Consultant Referral Policy Version Author Date Comments Approved by No V1.0 Mel Sims 19 January 2017 To be APPROVED Governing Body Reader information Reference Document purpose COM002 This
Consultant to Consultant Referral Policy Version Author Date Comments Approved by No V1.0 Mel Sims 19 January 2017 To be APPROVED Governing Body Reader information Reference Document purpose COM002 This
Job Description. Job title: Gynae-Oncology Clinical Nurse Specialist Band: 7. Department: Cancer Services Hours: 30
 Job Description Job title: Gynae-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 30 Reports to: Lead Nurse for Cancer We are a pioneering research active organisation and
Job Description Job title: Gynae-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 30 Reports to: Lead Nurse for Cancer We are a pioneering research active organisation and
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7. Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7. Optional to use, detail for local determination
TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT)
") TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT) Introduction The National Institute for Clinical Excellence has developed Guidance on Supportive and Palliative Care for patients with cancer. The standards
TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT) Introduction The National Institute for Clinical Excellence has developed Guidance on Supportive and Palliative Care for patients with cancer. The standards
Forensic Mental Health Service. Referrals to and Discharges from the Leicestershire Partnerships NHS Trust
 Referrals to and Discharges from the Leicestershire Partnerships NHS Trust Contents 1. Introduction... 3 2. Aims and Objectives of the Policy... 3 3. Referral Criteria... 3 4. Referral Procedure... 3 5.
Referrals to and Discharges from the Leicestershire Partnerships NHS Trust Contents 1. Introduction... 3 2. Aims and Objectives of the Policy... 3 3. Referral Criteria... 3 4. Referral Procedure... 3 5.
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST. PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control
 Documentation Control") NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
SERVICE SPECIFICATION 2 Vascular Access
 SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
JOB DESCRIPTION. Lead Diabetes Specialist Nurse. None. Calderdale and Huddersfield NHS Foundation Trust
 JOB DESCRIPTION POST TITLE: POST REFERENCE: Diabetes Specialist Nurse 372-MED500 BAND: Band 7 ACCOUNTABLE TO: RESPONSIBLE TO: LINE MANAGEMENT RESPONSIBILITY FOR: BASE: Matron/General Manager Lead Diabetes
JOB DESCRIPTION POST TITLE: POST REFERENCE: Diabetes Specialist Nurse 372-MED500 BAND: Band 7 ACCOUNTABLE TO: RESPONSIBLE TO: LINE MANAGEMENT RESPONSIBILITY FOR: BASE: Matron/General Manager Lead Diabetes
Physiotherapist Registration Board
 Physiotherapist Registration Board Standards of Proficiency and Practice Placement Criteria Bord Clárchúcháin na bhfisiteiripeoirí Physiotherapist Registration Board Contents Page Background 2 Standards
Physiotherapist Registration Board Standards of Proficiency and Practice Placement Criteria Bord Clárchúcháin na bhfisiteiripeoirí Physiotherapist Registration Board Contents Page Background 2 Standards
NURSE PRACTITIONER STANDARDS FOR PRACTICE
 NURSE PRACTITIONER STANDARDS FOR PRACTICE February 2012 Acknowledgement The College of Registered Nurses of Prince Edward Island gratefully acknowledges permission granted by the Nurses Association of
NURSE PRACTITIONER STANDARDS FOR PRACTICE February 2012 Acknowledgement The College of Registered Nurses of Prince Edward Island gratefully acknowledges permission granted by the Nurses Association of
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059
 Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059 Email: legalmail@doh.health.nsw.gov.au RE: Discussion Paper - Cosmetic Surgery and The Private
Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059 Email: legalmail@doh.health.nsw.gov.au RE: Discussion Paper - Cosmetic Surgery and The Private
For more information about having an anaesthetic please see our leaflet, Having an anaesthetic - please ask a member of staff for a copy.
 Forehead flap reconstruction If you have a wound on your nose after the removal of skin cancer, we may use the forehead flap reconstruction to repair your wound. This leaflet explains more about the procedure
Forehead flap reconstruction If you have a wound on your nose after the removal of skin cancer, we may use the forehead flap reconstruction to repair your wound. This leaflet explains more about the procedure
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Named Key Worker for Cancer Patients Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Named Key Worker for Cancer Patients Policy Version No.: 4 Effective 07 December 2017 From: Expiry Date: 07 December 2020 Date Ratified: 17 October
The Newcastle upon Tyne Hospitals NHS Foundation Trust Named Key Worker for Cancer Patients Policy Version No.: 4 Effective 07 December 2017 From: Expiry Date: 07 December 2020 Date Ratified: 17 October