Private Sector Cost Containment Strategies
|
|
|
- Ashley Egbert Blake
- 6 years ago
- Views:
Transcription
1 Private Sector Cost Containment Strategies Blue Cross Blue Shield of Michigan Value Partnerships Program Presentation to: National Coalition on Health Care Forum May 15, 2012 Thomas Leyden, MBA Director, Value Partnerships Blue Cross Blue Shield of Michigan
 4 Organized Systems of Care/Accountable Care Organizations 5 6 Aligning Hospital and Physician Incentives Overview of the Move from Fee for Service to Fee for Value /Reimbursement")
2 Presentation Objectives 1 BCBSM and the Value Partnerships Program 2 Hospital Initiatives (Collaborative Quality Initiatives) 3 Ambulatory Initiatives (PGIP, PCMH Designation and Tiered Payments) 4 Organized Systems of Care/Accountable Care Organizations 5 6 Aligning Hospital and Physician Incentives Overview of the Move from Fee for Service to Fee for Value /Reimbursement Transformation
3 About the Blue System Blue Cross Blue Shield Association (BCBSA) is a national federation of BCBS Plans in all 50 states and U.S. territories 38 independent, locally based and community operated Blue Plans Collectively covering nearly 100 million one in three Americans Networks with 90% of hospitals and 80% of physicians in every zip code 83 years experience providing health benefits in local communities 3
 and over 1 million out of state members 7,000 employees state-wide Michigan Blues have largest network in the state More than 150 hospitals")
4 Overview of BCBSM BCBSM is the largest single state non-profit Blues plan Serving 4.7 million Michigan members (45% in-state market share) and over 1 million out of state members 7,000 employees state-wide Michigan Blues have largest network in the state More than 150 hospitals (100% of all MI hospitals) Over 30,000 physicians (95% of all MI physicians) In 2010, BCBSM processed over 80 million claims and paid out over $17 billion in benefits Fulfilling a unique, nonprofit mission for more than 70 years and insurer of last resort for Michigan members Maintaining collaborative partnerships with providers committed to improving health of all Michigan residents and advancing quality of care they receive 4
5 Root Causes of High Cost Health Care System Poorly aligned incentives: Fee-for-service drives increased delivery of services and members lack benefit incentives to promote better health. Lack of population focus: Provider delivers services that are demanded and paid for, instead of focusing on the health of the overall population. Fragmented healthcare delivery: Physicians and hospitals lack information infrastructure and integration of care processes across the care continuum. Lack of focus on process excellence: Creates variation and re-work, not clinical process improvement. Weak primary care foundation: Missed opportunities for care coordination and lower cost approaches.
6 Our Approach to Payer/Provider Roles Payer Provider Align payment and performance Convene providers to forge future vision and plan means to achieve it Create a payment model that supports the business case for healthcare transformation Reward achievements measured on the population level Possess care relationship with patients Responsible for the process of care and system transformation Improve patient care
7 Overarching Principles Health care is local: natural communities of caregivers taking responsibility for creating systems serving community need Build community first; don t rush to payment solutions Harness intrinsic motivation of providers by ceding control: Purpose, autonomy and mastery must drive system development and performance, not short term gain Incentives, or payment reform, separate from community, and explicit purpose, will not succeed
8 BCBSM s All Payer Approach Value Partnerships encourages providers to have an all payer focus; catalyzing all payer system development, rather than payer-specific system development Developing systems of care which are used for all patients helps ensure that providers don't have to alter care processes based on whether patients have insurance, or which insurance they have An important factor in ensuring that best practices and care processes are reliably provided to all patients, all of the time Patients throughout Michigan, regardless of payer, benefit from improved care processes developed through an all-payer approach to practice transformation Helps further BCBSM's social mission of cultivating a healthier future for all Michigan residents


9 BCBSM s Value Partnerships Program Physicians Physician Group Incentive Program 34 Initiatives aimed at Capability Building, Improving Quality of Care Delivery, and Appropriate Utilization of Services Types of Initiatives Include: Improvement Capacity Condition-Focused Service-Focused Core-Clinical Process- Focused Clinical Information Technology-Focused Hospital Collaborative Quality Initiatives BCBSM Cardiovascular Consortium Percutaneous Coronary Intervention and Peripheral Vascular Intervention CQIs Michigan Society of Thoracic & Cardiovascular Surgeons Quality Collaborative Michigan Bariatric Surgery Collaborative Michigan Breast Oncology Quality Initiative Advanced Cardiac Imaging Consortium Michigan Surgical Quality Collaborative Peri-Operative Outcomes Initiative Hospital Medicine Safety Collaborative Michigan Trauma Quality Improvement Program Michigan Arthroplasty Registry Collaborative for Quality Improvement (1Q12) Michigan Radiation Oncology Quality Collaborative (1Q12) Hospitals Hospital P4P Incentive Program P4P program consists of Quality Measures CQIs Quality Indicators Efficiency Measures Cost-per-Case Hospital per member per month trends Michigan Health & Hospital Association: Keystone Center for Patient Safety & Quality BCBSA Best of Blue & BlueWorks Awards PGIP and CQIs PCMH (also received BlueWorks the premiere BCBSA award) MSQC, MBSC and MOQC (also received BlueWorks Awards for MSQC and MBSC) Other Awards and Recognition NBCH evalue8 Health Plan Innovation Award, CQI Program URAC Bronze Award, PCMH
10 BCBSM Value Partnerships Philosophy Design and execute programs in a customized and collaborative manner rather than using a one-size-fits-all approach. Recognize and reward performance of hospitals and physician organizations, not only individual physicians. Reward improvement, not just highest performance, to create meaningful incentives for all physician organizations. Focus on investments in long-term changes in care processes, rather than just top of mind behavior. 5 6 Encourages all-payer approach, rather than payer-specific system development. Focus on population-based cost measures, rather than per-episode cost, to avoid stimulating overuse.
11 Hospital Collaborative Quality Initiatives (CQIs)
12 Collaborative Quality Initiatives (CQIs) CQIs rely on comprehensive clinical data registries and/or databases that enable physicians at each CQI to examine the links between care processes and outcomes in complex, highly technical areas of care to contribute to an understanding of which care processes lead to optimal outcomes Goal of CQIs is to empower providers to self-assess and optimize their care by identifying opportunities to bring care into closer alignment with best practices developed in the CQI which lead to improved quality and lower costs for selected, high cost, high frequency and highly complex procedures and conditions Objectives of each CQI are to: address many of the key drivers of health care costs in surgical and medical care improve healthcare outcomes curb the increasing healthcare cost trend
13 Three Pillars of the Hospital CQI Program CQI Program Success The BCBSM/BCN CQI model has proven remarkably effective in raising the bar on clinical quality across a broad range of clinical conditions throughout Michigan Data Collection Collaborative Learning Improvement Implementation Timely feedback of robust, trusted, consortium-owned performance data to hospitals and providers Collaborative, data-driven learning fostered in a noncompetitive environment (meetings are typically held in person on a quarterly basis) Systematic development, implementation, and testing of hospital-specific and Michigan-wide quality improvement interventions CQI Foundation Coordinating Center BCBSM Participants Provides Clinical Leader Provides analytic and QI support to participants Convenes competitive hospitals and offers neutral ground for collaboration Provides participation payments for data gathering and analysis Contribute to comprehensive, validated all-payer data registry Share and learn from best practices 13
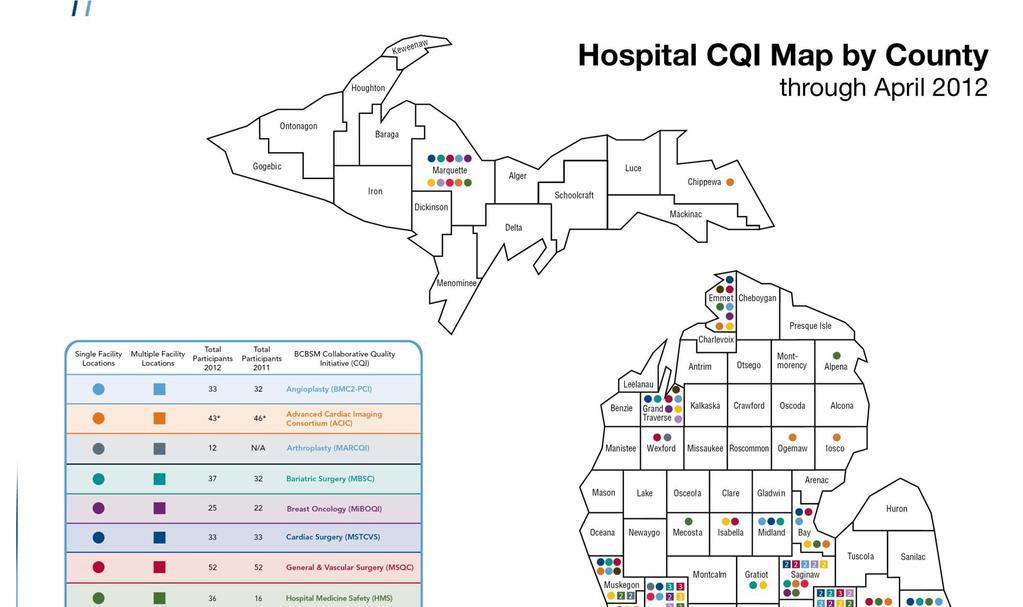
14 Collaborative Quality Initiatives (CQIs) BCBSM/BCN Collaborative Quality Initiatives Inception Date: Hospital Based: Michigan Cardiovascular Consortium Percutaneous Coronary Intervention (BMC2 PCI) July 1997 Michigan Society of Thoracic and Cardiovascular Surgeons (MSTCVS) Quality Sept 2005 Michigan Bariatric Surgery Consortium (MBSC) Oct 2005 Michigan Surgical Quality Collaborative (MSQC) Nov 2005 Michigan Breast Oncology Quality Initiative (MiBOQI) Apr 2006 Michigan Cardiovascular Consortium Peripheral Vascular Intervention (BMC2 PVI) Oct 2006 Hospital Medicine Safety (HMS) Consortium Oct 2010 Michigan Trauma Quality Improvement Project (MTQIP) Jan 2011 Peri Operative Outcomes Initiative (POI) Jan 2011 Michigan Arthroplasty Registry Collaborative for Quality Improvement (MARCQI) Feb 2012 Michigan Radiation Oncology Quality Collaborative (MROQC) Feb 2012 Hospital/Provider Based: Advanced Cardiac Imaging Consortium (ACIC) July 2007 Also, BCBSM is expanding CQIs via Professional CQIs: Lean for Clinical Redesign (LEAN) Apr 2008 Michigan Anticoagulation Quality Improvement Initiative (MAQI2) Sept 2009 Michigan Oncology Quality Consortium (MOQC) Jan 2010 Oncology Clinical Treatment Pathways (Pathways) Jan 2010 Michigan Transitions of Care Collaborative (MTC2) Jan 2010 Michigan Urological Surgery Improvement Collaborative (MUSIC) Jan 2012

15 15
16 The CQI Foundation BCBSM/BCN sponsored collaboratives Health plans provide active leadership support of program Consortium identifies and disseminates best practices CQI program coordinated by Coordinating Centers Coordinating Center assures rigor, guides crossinstitutional study of practice patterns and their relation to outcomes, and orchestrates QI interventions Multiple facilities collect and share data to improve the delivery and quality of care Locus of control remains with the providers complete, accurate, risk adjusted, confidential, provider-owned data
17 Collaborative Quality Initiatives: Underlying Assumptions Cross-group/institution collaboration yields more than competition on quality Improvement catalyzed by sharing best practices More can be learned from variation in care processes and outcomes across groups than within groups Permits more robust analyses of link between processes and outcomes of care than can be achieved by examining one group or institution Valid, evidence-based, nationally accepted performance measures cover a narrow slice of health care generally, and hospital care in particular Simple performance measures don t address areas of care which are highly technical, rapidly-evolving and associated with scientific uncertainty These areas best addressed through collaborative, interinstitutional, clinical data registries, with coordinated QI programs
18 Role of Coordinating Center Coordinating center primary functions: Serve as data warehouse Conduct data audits Performs data analyses to identify best practices and opportunities for improvement Convene quarterly meetings to share data Guide quality improvement efforts Evaluate participant s active participation
19 BMC2-PCI: Accomplishments to Date 32% reduction in hospital deaths 60% reduction in contrast-induced nephropathy (kidney injury from contrast dye used during angioplasty) 30% reduction in blood transfusions after angioplasty 32% reduction in vascular complications (resulting from injury to the arteries in the groin) 31% reduction in emergency revascularization (where angioplasty needs to be redone at the same site) 19% reduction in unplanned coronary artery bypass surgery 29% reduction in strokes or TIAs 19% reduction in gastrointestinal bleeding
20 General & Vascular Surgery (MSQC) Advances Michigan is outperforming national improvements in surgical outcomes, including complications & surgical site infections Overall MSQC changes in outcomes between 2006 Q2 and 2007 Q2 Time Period Total Cases Mean RVU % Mortality % Comp % SSI 2006q q % change from 2006q YTD Overall NSQIP changes in outcomes between 2006 Q2 and 2007 Q2 Time Period Total Cases Mean RVU % Mortality % Comp % SSI NSQIP 2006q2 25, NSQIP 207q2 46, % change from 2006q /16/2012
21 Michigan Bariatric Surgery Collaborative (MBSC) Quality Improvement Success Reduced rate of pre-operative IVC filter placement Quality Improvement Initiative Description: Inferior vena cava (IVC) filter is a device that is inserted into inferior vena cava to prevent pulmonary emboli (PE), which are potentially fatal to patients. IVC filters are used prophylactically in patients with high risk of PE. Bariatric patients are at a higherthan-average risk of PE due to reduced mobility, compromised cardiopulmonary status, decreased venous return, and obesity-related metabolic factors. Because PE accounts for almost 40% of perioperative deaths occurring in bariatric surgery patients, it is recommended that some form of VTE prophylaxis be used. However, effectiveness of IVC filters has never been proven. Through analysis of data in the clinical registry, MBSC Coordinating Center leadership identified significant variations in IVC filter usage pre-operatively in an effort to prevent post-operative PE (a practice that has increased over last two decades). The MBSC Coordinating Center also discovered that IVC filter use was not always preventing blood clots, but at times was contributing to increased complications such as filter migration, IVC thrombosis, and IVC injury.
22 MBSC Quality Improvement Success Initial Rate (Pre-improvement status): During , IVC filter use in Gastric Bypass patients varied from 0-35% for 20 hospitals in the MBSC 4 hospitals did not use any IVC filter 6 hospitals used IVC filter in more than 10% of patients During , 591 (8.5%) Michigan Gastric Bypass patients underwent IVC filter placement Complications linked to IVC filter placement: Postop VTE 13 (2.2%) Deaths 5 (0.9%) Grade I 63 (10.7%) Grade II 36 (6.1%) Grade III 9 (1.5%) Any complication 207 (35.0%) Average Cost of Complication in Gastric Bypass Patients: Based on 2006 claims data, payments are more than $13,500 for IVC filter patients (it is estimated that excess costs may total $270 million dollars in the US annually).
23 MBSC Quality Improvement Success: Reduced rate of pre-operative Inferior Vena Cava (IVC) filter placement Use of IVC filter in 20 Michigan Hospitals participating in MBSC 10% 9% 8% 7% 6% 5% 4% 3% 2% 1% 0% 1st Qtr 07 2nd Qtr 07 p< rd Qtr 07 4th Qtr 07 1st Qtr 08 2nd Qtr 08 Data about adverse complications first presented at quarterly meeting 3rd Qtr 08 4th Qtr 08 1st Qtr 09 2nd Qtr 09 Consider: It typically takes approximately 15 years to implement evidence-based medicine
24 CQI Savings BCBSM conducted a high level analysis of savings associated with improvements in quality resulting in reductions in adverse events (and cost avoidance associated with these improvements) for the past few years. To date, four CQIs have undergone this internal evaluation conducted by BCBSM Provider Performance, Innovation & Experience. Results are as follows: MSQC: o From , saved an estimated $49.2 for BCBSM o Estimated to have said $85.9M statewide in same time period BMC2 - PCI: From , saved an estimated $13.8M for BCBSM Savings of $102.0M statewide MBSC: From , saved an estimated $4.7 for BCBSM Savings of $14.6M statewide. MSTCVS: o From , saved an estimated $2.5 for BCBSM o Savings of $30.3M statewide.
25 Results of CQIs Receive National Exposure Through Peer Reviewed Publications * denotes a professional CQI MSQC Journal of the American College of Surgeons (Jan 2009) MSQC Anesthesiology (Mar 2009) MSTCVS Seminars in Thoracic and Cardiovascular Surgery (Spring 2009) ACIC Journal of the American Medical Association (June 2009) BMC2 PCI Journal of the American College of Cardiology (July 2009) MSQC Journal of the American College of Surgeons (July 2009) MSQC Journal of the American Medical Association (Oct 2009) MOQC Journal of Oncology Practice (Nov 2009) MSQC American Journal of Surgery (Nov 2009) MSQC Medical Care (Mar 2010) BMC2 PCI American Heart Journal (Jan 2011) BMC2 PCI Journal of the American College of Cardiology (Jan 2012) BMC2 PCI American Heart Journal (Apr BMC2 PCI American Heart Journal (Jan ACIC Journal of the American College of 2010) 2011) Cardiology (Feb 2012) BMC2 PCI Clinical Cardiology (May 2010) BMC2 VIC Archives of Surgery (Apr 2011) ACIC American Heart Journal (March 2012) MBSC Journal of the American Medical MBSC Obesity Surgery (2011) MSTCVS, MSQC, HMS, MBSC, MTQIP, Association (July 2010) MAQI* Journal of Thrombosis and Thrombolysis (Apr 2012) MBSC Annals of Surgery (Aug 2010) MSTCVS, MBSC, BMC2 PCI, and MSQC MOQC* Health Affairs (Apr 2012) Health Affairs (Apr 2011) MSQC Annals of Surgery (Sept 2010) MTQIP Journal of Trauma (March 2011) MSTCVS Annals of Thoracic Surgery (Oct BMC2 VIC Journal of the American College 2010) of Cardiology (June 2011) MSQC Archives of Surgery (Oct 2010) BMC2 PCI Journal of the American College of Cardiology (Sept 2011) BMC2 PCI Journal of the American College MiBOQI Surgery (Oct 2011) of Cardiology (Oct 2010) BMC2 PCI Journal of Invasive Cardiology (Oct 2010) 25

26 Improving Quality of Care in Michigan Through CQIs The CQI Projects effectively put the workings of Comparative Effectiveness Research in the hands of the Provider Community in real world situations empowering them to us sophisticated scientific methods to rigorously assess and improve care affecting the entire population making hospitals self optimizing institutions David Share, Assistant CMO, BCBSM Regional collaborations between hospitals and physicians may be more effective than either selective referral or pay for performance in improving the quality of health care at the population level The improvement programs target clinical conditions and procedures that are relatively common and that are associated with high costs per episode Health Affairs, April 2011 Vol 30(4). p.1 11 By David A. Share, Darrell A. Campbell, Nancy Birkmeyer, Richard L. Prager, Hitinder S. Gurm, Mauro Moscucci, Marianne Udow Phillips, and John D. Birkmeyer The large sample sizes and statistical power associated with regional collaborative improvement program registries allow for more robust, rapid assessment of relationships between process and outcomes and of the effects of quality improvement interventions than can be achieved by hospitals examining their own practice in isolation 26
27 Physician Group Incentive Program (PGIP)
28 One of PGIP s Initial Goals: Restoring Primary Care Support performance transformation initiatives PGIP rewards based on performance and building PCMH capabilities Higher E & M fees for PCMH designated primary care practices Selective privileging of qualifying PCMH practices to deliver services not payable for other physicians, i.e., case and disease management, selected diagnostic tests, etc Benefit designs that encourage patients to see PCMH designated physicians
29 PGIP At 5,000 Feet PGIP incentivizes providers to alter the delivery of care by encouraging responsible and proactive physician behavior, ultimately driving better health outcomes and financial impact. BCBSM provides the financing, tools and support so physicians can engage in specific initiatives that change the way healthcare is delivered... and drive meaningful impacts for our customers and our members. Efficient Utilization of Resources BCBSM/Provider Partnership PGIP Initiatives Delivery of Care Improved Quality of Care Enhanced Member Experience 29
30 PGIP: Health Plan Role Convene and catalyze; not engineer and control Provide resources and structure reimbursement to reward infrastructure development and process transformation Reward quality and cost results (improvement and optimal performance) at the population level Share data at organization, practice unit/office and physician level Leave management of individual patient care to practices and of physician practices to PO
31 PGIP: PO Role Collaborate on crafting future vision Collaborate on implementation PGIP quarterly meetings Common interest groups Regional learning collaboratives Animate physician members Develop and deploy new systems of care Work with organization members to examine and optimize performance
32 PGIP: Shared Vision POs take responsibility for developing systems of care Shared information systems Shared processes of care Shared accountability for population level performance Organizing concepts Lack of a system is the root cause: structure incentives to catalyze system development and system performance Patient Centered Medical Home Model Systems designed to respond to patients and community s needs
33 PGIP Key Program Results The Generic Prescribing Rate has risen from 38 percent in 2004 to 74 percent in 2011 PCMH practices demonstrate lower rates of hospitalization, radiology utilization and lower ED visits Direct Radiology savings were $24M in 2010 BCBSM cost trend fell to 3.1% in 1Q2011 with negative professional cost trend 33
34 Patient Centered Medical Homes (PCMH)
35 Patient Centered Medical Home With the PCMH model, the primary care physician leads a professional health care team that tracks and monitors the patient s overall health, working collaboratively to ensure a patient s health care needs are being met, from lifestyle and nutrition counseling to testing and monitoring health outcomes. In 2011, of the nearly 1,000 practices that were nominated for PCMH designation, 776 practices throughout the state were designated, representing more than 2,500 primary care physicians
36 BCBSM Approach to PCMH Model developed in Collaboration with PGIP Providers PGIP PCMH Initiatives Opportunity for PGIP POs to participate in 12 PCMH-focused PGIP Initiatives that support implementation of 129 specific PCMH capabilities Targeted assistance offered through collaboratively developed Interpretive Guidelines All s and Specialists in PGIP may participate More than 5,500 s are currently working on implementing PCMH capabilities Incentives for the obtainment of PCMH capabilities POs work on Initiatives to achieve practice transformation. PGIP PCMH Designation Program Opportunity for PGIP Practice Units to be PCMH- designated by BCBSM and rewarded for additional time and resources required (started in July 2009) Only s are eligible to participate Additional reward monies available via increased E&M fees: Office visits Preventive Increase office visit fees to PCMHdesignated practices (+10%) New codes for care management and selfmanagement support (in person and telephonic) payable to PGIP physicians: supports multi-disciplinary, team based care/care management Increase office visit fees for offices in PCMH-designated practices in POs with optimal population level cost performance (+10%)
37 Eligibility Requirements for PCMH Designation Program 1. Physician offices nominated by their PGIP PO 2. Commendable performance on quality/use/efficiency measures (adult and pediatric) Quality: Evidence Based Care and Preventive measures Use: ED use for primary care treatable conditions and high-tech and low-tech radiology rates Efficiency: Generic Dispensing Rate and trend 3. Critical mass of PCMH capabilities in place Self-reported data validated through site visits Practice Units that achieve PCMH Designation continue to participate in PCMH Initiatives and are expected to demonstrate ongoing progress towards fully implementing PCMH domains of function
38 BCBSM PCMH Designation PGIP Phys Org B PGIP Phys Org A PC-MH PC-MH PC-MH Nominee PC-MH PC-MH Nominee PC-MH Nominee PGIP Phys Org C Non PGIP Physicians




39 PCMH: Key Statistics Patient Centered Medical Home program includes: Approximately 5,600 primary care physicians working towards implementing PCMH capabilities Almost 2,000 specialists working towards implementing PCMH capabilities Number of participating providers increases each year 2011 BCBSM PCMH Designation includes: Over 2,500 primary care physicians and specialists in more than 770 practice units Over $25M in annual E&M uplifts for PCMH designated providers
40 PCMH Capabilities in Place Among those practices that were designated as patient-centered medical homes in 2011: Over 95% of PCMH-designated primary care physicians have: 24 hour phone access to a clinical decision-maker Patients who are fully informed about after-hours care options Medication review & management for all chronic patients A system in place for tracking abnormal test results Over 90% of PCMH-designated primary care physicians have: Primary prevention program to reduce patient risk of disease and injury Patient registry with evidence-based care guidelines Written procedure and staff training in place for referring patients to specialists
41 Performance of PCMH Designated Practices Continues to Improve as Program Expands Metric PCMH Designees Compared to non-pcmh Practices Year 2 Designation* Year 3 Designation Jan.- Dec Designated Physicians 2010 Attributed BCBSM Members Jan.-Dec Designated Physicians 2011 Attributed BCBSM Members Adults (18-64) 1,836 physicians 650,000 2,614 physicians 820, practices 502 practices Emergency department visits (per 1,000) -6.6% -9.9% Primary care sensitive emergency department visits (per 1,000) -7.0% -11.4% Ambulatory care sensitive inpatient discharges (per 1,000) -11.1% -22% High tech radiology services (per 1,000) -6.3% -7.5% High tech radiology standard cost PMPM -3.0% -4.9% Low tech radiology services (per 1,000) -5.9% -4.8% Low tech radiology standard cost PMPM -5.9% -5.0% Generic dispensing rate 3.3% 3.8% Despite adding 42% more physicians in 2011, there were significant increases in differentiation between PCMH and non designated physicians *Year 2 Designation: July June 2011 Year 3 Designation: July June 2012
42 Overview of the Move from Fee for Service to Fee for Value Reimbursement Transformation
43 BCBSM will direct an increasing proportion of professional payment to PCMH designated practices through higher fees based on populationbased practice and system performance. PGIP and its Continued Evolution Phase I PGIP Reward/Investment Pool Enhanced Fees for Designated Practices MD MD MD MD MD MD Reward Practice Performance Phase II Fees based on System Performance MD MD MD MD MD MD Reward System Performance MD MD MD MD MD MD
44 Transforming Physician Reimbursement at the Physician Office Level Incentive payments to physicians in office practice Increase office visit fees to PCMH-designated practices (+10%) New codes for care management and self-management support (in person and telephonic) payable to PGIP physicians: supports multi-disciplinary, team based care/care management Increase office visit fees for offices in PCMH-designated practices in POs with optimal population level cost performance (+10%)
45 Specialist Performance Measurement and Payment Payment Strategy: Increase E & M fees to specialists to recognize better performance measured at the overall population level BCBSM will employ CAVE analytics as well as other performance measures (e.g. PMPM) as foundation for this payment strategy Specialists are nominated based on following criteria: Is actively engaged with the PO Is involved in managing the use of services Is involved in optimizing quality of care Works collaboratively with s to develop and improve shared processes of care Coordinates care across settings and over time
46 Strategy: Modernize Hospital Reimbursement Move away from traditional FFS reimbursement by linking payments to: Performance measured on a population level Decreases in per-member-per-month payment trends Align hospital and physician payment incentives Create attributed populations for hospitals and physician organizations Establish common measurement system and performance goals Foster collaboration Link payment to creating population management infrastructure, improving processes of care and improving performance. 46


47 Moving towards Fee For Value Infrastructure 100 % - Payment 0 % - Pay for PCMH/OSC Infrastructure Development Pay for Performance (tied to savings from decreased use and improved quality) Capacity to Manage Population Level Quality, Efficiency and Outcomes Current State David Share and Bharath Mamathambika, Blue Cross Blue Shield of Michigan Future State
48 Conclusion
49 Value Partnerships: How Strategic Initiatives are Addressing the Root Causes of our High Cost Health Care System Poorly aligned incentives: Tiered fees based on performance measured at the population level Lack of population focus: All-patient registries (patient lists) and Physician Group Incentive Program rewards for performance Fragmented healthcare delivery: Organized Systems of Care aligned incentives for primary care physicians, hospitals, and specialists Lack of focus on process excellence: Collaborative Quality Initiatives Weak primary care foundation: Patient-Centered Medical Home Strengthening Providers Ability to Improve Care
50 Lessons Learned All payment methods have inherent risks: e.g., fee for service-over use; global payment-under use; episode payment- episode volume An incentive system must be driven by explicit purpose: BCBSM s is Improved population wellbeing at lower cost Moving from volume to value from procedure-based care to relationship-based care for both s and specialists Fee for Value: retains granular detail on diagnosis and service provision; no expensive system overhaul; enhanced population level performance
51 Lessons Learned Making a substantial portion of FFV reimbursement dependent on system development and performance can move the needle on cost and quality Collaboration among providers is essential: align incentives for s, specialists and facilities so they create clinically integrated systems which best serve the community, rather than compete for declining resources through technology wars Savings will come from moderating procedure, ED and inpatient use; right-sizing facility capacity is necessary and requires a glide path for facilities
52 Contact Information Tom Leyden, MBA Director Value Partnerships Program Blue Cross Blue Shield of Michigan 600 E. Lafayette Blvd Detroit, MI
Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance
 Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance Physician Group Incentive Program, Patient Centered Medical Homes, and Moving From Fee for Service
Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance Physician Group Incentive Program, Patient Centered Medical Homes, and Moving From Fee for Service
Presentation to: IHA NATIONAL PAY FOR PERFORMANCE SUMMIT March 25, 2014
 Blue Cross Blue Shield Michigan s Hospital Collaborative Quality Initiatives: Achieving Transformative Performance and Improved Relations through Collaboration Presentation to: IHA NATIONAL PAY FOR PERFORMANCE
Blue Cross Blue Shield Michigan s Hospital Collaborative Quality Initiatives: Achieving Transformative Performance and Improved Relations through Collaboration Presentation to: IHA NATIONAL PAY FOR PERFORMANCE
Moving from Fee-for-Service to Fee-for-Value: Blue Cross Blue Shield of Michigan s Value Partnership Programs
 Moving from Fee-for-Service to Fee-for-Value: Blue Cross Blue Shield of Michigan s Value Partnership Programs The Tenth National Pay for Performance Summit March 2015 Session Description This presentation
Moving from Fee-for-Service to Fee-for-Value: Blue Cross Blue Shield of Michigan s Value Partnership Programs The Tenth National Pay for Performance Summit March 2015 Session Description This presentation
2016 Blue Cross Blue Shield of Michigan Commercial PPO/Marketplace Quality Improvement Program Description
 2016 Blue Cross Blue Shield of Michigan Commercial PPO/Marketplace Quality Improvement Program Description March 31, 2016 Conflict of Interest Blue Cross Blue Shield of Michigan (Blue Cross) is committed
2016 Blue Cross Blue Shield of Michigan Commercial PPO/Marketplace Quality Improvement Program Description March 31, 2016 Conflict of Interest Blue Cross Blue Shield of Michigan (Blue Cross) is committed
Launch PCMH Program. Organized Systems of Care (OSCs) Launch of PGIP based on Chronic Care Model. Risk-based Reimbursement
 Launch of PGIP based on Chronic Care Model. Risk-based Reimbursement") Updated 1/19/2017 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Launch of PGIP based on Chronic Care Model Physician Organizations have the structure and technical expertise to create
Updated 1/19/2017 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 Launch of PGIP based on Chronic Care Model Physician Organizations have the structure and technical expertise to create
2018 Collaborative Quality Initiative Fact Sheet
 2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
W. Douglas Weaver, MD, MACC. American College of Cardiology SENATE FINANCE COMMITTEE
 Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Blue Cross Blue Shield of Michigan. Organized Systems of Care
 Blue Cross Blue Shield of Michigan Organized Systems of Care 1 PGIP: Catalyzing Health System Transformation in Partnership with Providers 2005 2006 2007 2008 2009 2010 2011 2012 PGIP Chronic Care Model
Blue Cross Blue Shield of Michigan Organized Systems of Care 1 PGIP: Catalyzing Health System Transformation in Partnership with Providers 2005 2006 2007 2008 2009 2010 2011 2012 PGIP Chronic Care Model
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018
 Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018 Nilesh Chandra Partner, PA Consulting Group Paul Pomerantz CEO, American Society of Anesthesiologists 1 Conflict of Interest Nilesh
Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018 Nilesh Chandra Partner, PA Consulting Group Paul Pomerantz CEO, American Society of Anesthesiologists 1 Conflict of Interest Nilesh
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
CIGNA Collaborative Accountable Care
 CIGNA Collaborative Accountable Care Connecting in ways that help make achieving health easier, more effective and more affordable October 14, 2016 Michael L. Howell, MD, MBA, FACP Market Medical Executive/Sr.
CIGNA Collaborative Accountable Care Connecting in ways that help make achieving health easier, more effective and more affordable October 14, 2016 Michael L. Howell, MD, MBA, FACP Market Medical Executive/Sr.
The Society of Thoracic Surgeons
 VIA EMAIL Practice Improvement and s Management Support (PIMMS) s Support The STS Headquarters 633 N Saint Clair St, Floor 23 Chicago, IL 60611-3658 (312) 202-5800 sts@sts.org STS Washington Office 20
VIA EMAIL Practice Improvement and s Management Support (PIMMS) s Support The STS Headquarters 633 N Saint Clair St, Floor 23 Chicago, IL 60611-3658 (312) 202-5800 sts@sts.org STS Washington Office 20
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
TRANSFORMING HEALTHCARE DELIVERY A Pathway to Affordable, High-Quality Care in America
 TRANSFORMING HEALTHCARE DELIVERY A Pathway to Affordable, High-Quality Care in America TABLE OF CONTENTS Executive Summary... 3 A Pathway to Affordable, High-Quality Care in America... 7 Appendix... 18
TRANSFORMING HEALTHCARE DELIVERY A Pathway to Affordable, High-Quality Care in America TABLE OF CONTENTS Executive Summary... 3 A Pathway to Affordable, High-Quality Care in America... 7 Appendix... 18
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013
 State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
Establishing a Culture of Quality and Safety and the Journey to High Reliability
 Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Physician Group Incentive Program Program Updates
 Physician Group Incentive Program Program Updates September 14, 2012 Tom Leyden, MBA Director, Value Partnerships PGIP Program Growth THANK YOU! PO efforts to continuously grow physician engagement in
Physician Group Incentive Program Program Updates September 14, 2012 Tom Leyden, MBA Director, Value Partnerships PGIP Program Growth THANK YOU! PO efforts to continuously grow physician engagement in
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Statement of the American College of Surgeons. Presented by David Hoyt, MD, FACS
 Statement of the American College of Surgeons Presented by David Hoyt, MD, FACS before the Subcommittee on Health Committee on Energy and Commerce United States House of Representatives RE: Using Innovation
Statement of the American College of Surgeons Presented by David Hoyt, MD, FACS before the Subcommittee on Health Committee on Energy and Commerce United States House of Representatives RE: Using Innovation
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Program Selection Criteria: Bariatric Surgery
 Program Selection Criteria: Bariatric Surgery Released June 2017 Blue Cross Blue Shield Association is an association of independent Blue Cross and Blue Shield companies. 2013 Benefit Design Capabilities
Program Selection Criteria: Bariatric Surgery Released June 2017 Blue Cross Blue Shield Association is an association of independent Blue Cross and Blue Shield companies. 2013 Benefit Design Capabilities
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model. Rome H. Walker MD February 28, 2008
 Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
A comprehensive reference guide for Aetna members, doctors and health care professionals Aetna Institutes of Quality facilities fact book
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions A comprehensive reference guide for Aetna members, doctors and health care professionals Aetna Institutes of
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions A comprehensive reference guide for Aetna members, doctors and health care professionals Aetna Institutes of
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
SAMPLE Bariatric Surgery Program Survey for Facilities and Surgeons
 I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Implementing Patient-Centered Medical Home Pilot Projects:
 Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Executive Summary 1. Better Health. Better Care. Lower Cost
 Executive Summary 1 To build a stronger Michigan, we must build a healthier Michigan. My vision is for Michiganders to be healthy, productive individuals, living in communities that support health and
Executive Summary 1 To build a stronger Michigan, we must build a healthier Michigan. My vision is for Michiganders to be healthy, productive individuals, living in communities that support health and
The Impact of Primary Care Practice Transformation on Cost, Quality, and Utilization
 EXECUTIVE SUMMARY The Impact of Primary Care Practice Transformation on Cost, Quality, and Utilization A SYSTEMATIC REVIEW OF RESEARCH PUBLISHED IN 2016 July 2017 PREPARED BY Made possible with support
EXECUTIVE SUMMARY The Impact of Primary Care Practice Transformation on Cost, Quality, and Utilization A SYSTEMATIC REVIEW OF RESEARCH PUBLISHED IN 2016 July 2017 PREPARED BY Made possible with support
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012
 Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
Workhorse or Unicorn: Incentive Realignment and Health Improvement After One Year of ACOs. Objectives
 Session L23 These presenters have nothing to disclose Workhorse or Unicorn: Incentive Realignment and Health Improvement After One Year of ACOs By James E. Orlikoff and Len Nichols Sunday, December 9,
Session L23 These presenters have nothing to disclose Workhorse or Unicorn: Incentive Realignment and Health Improvement After One Year of ACOs By James E. Orlikoff and Len Nichols Sunday, December 9,
BUILDING THE PATIENT-CENTERED HOSPITAL HOME
 WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
Hospital Acquired Conditions: using ACS-NSQIP to drive performance. J Michael Henderson Jackie Matthews Nirav Vakharia
 Hospital Acquired Conditions: using ACS-NSQIP to drive performance J Michael Henderson Jackie Matthews Nirav Vakharia Your Team: Quality & Patient Safety Institute Cleveland Clinic Mike Henderson: Chief
Hospital Acquired Conditions: using ACS-NSQIP to drive performance J Michael Henderson Jackie Matthews Nirav Vakharia Your Team: Quality & Patient Safety Institute Cleveland Clinic Mike Henderson: Chief
National ACO Summit. Third Annual. June 6 8, Follow us on Twitter and use #ACOsummit.
 Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. Opening Plenary Session Welcome and Overview Mark McClellan, MD, PhD Director, Engelberg Center for Health
Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. Opening Plenary Session Welcome and Overview Mark McClellan, MD, PhD Director, Engelberg Center for Health
Transforming Delivery Systems for Population Health
 Transforming Delivery Systems for Population Health George Isham, M.D., M.S. Senior Advisor, HealthPartners Senior Fellow, HealthPartners Institute for Education and Research October 9, 2015 Presenter
Transforming Delivery Systems for Population Health George Isham, M.D., M.S. Senior Advisor, HealthPartners Senior Fellow, HealthPartners Institute for Education and Research October 9, 2015 Presenter
ACS TQIP Collaborative Toolkit A guide for getting started and maintaining momentum
 ACS TQIP Collaborative Toolkit A guide for getting started and maintaining momentum Table of Contents Introduction... 2 Getting Started... 2 Maintaining Momentum... 3 Quality Improvement... 4 Collaborative
ACS TQIP Collaborative Toolkit A guide for getting started and maintaining momentum Table of Contents Introduction... 2 Getting Started... 2 Maintaining Momentum... 3 Quality Improvement... 4 Collaborative
National Academy of Medicine Value Incentives and Systems Innovation Collaborative September 16, 2016 Sam Nussbaum, MD
 National Academy of Medicine Value Incentives and Systems Innovation Collaborative September 16, 2016 Sam Nussbaum, MD Purpose 2 The Health Care Payment Learning & Action Network (LAN) was launched because
National Academy of Medicine Value Incentives and Systems Innovation Collaborative September 16, 2016 Sam Nussbaum, MD Purpose 2 The Health Care Payment Learning & Action Network (LAN) was launched because
Strategic Alignment in Health Care
 Strategic Alignment in Health Care Presented to CAJPA Fall Conference 9/15/16 1 Transforming Care Delivery Value-Based Pay for Performance Oncology Practice of the Future Maternity Care Focus - C-Sections
Strategic Alignment in Health Care Presented to CAJPA Fall Conference 9/15/16 1 Transforming Care Delivery Value-Based Pay for Performance Oncology Practice of the Future Maternity Care Focus - C-Sections
Primary Care Transformation in the Era of Value
 Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Comparison of ACP Policy and IOM Report Graduate Medical Education That Meets the Nation's Health Needs
 IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
A New Approach to Patient-Centered Procedural Care
 A New Approach to Patient-Centered Procedural Care Health Forum/ AHA Leadership Summit San Francisco, CA Creagh Milford, DO, MPH Associate Medical Director, Population Health Management, Partners HealthCare
A New Approach to Patient-Centered Procedural Care Health Forum/ AHA Leadership Summit San Francisco, CA Creagh Milford, DO, MPH Associate Medical Director, Population Health Management, Partners HealthCare
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
Improving quality of care during inpatient hospital stays
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Communications FACT SHEET FOR IMMEDIATE RELEASE Contact:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Communications FACT SHEET FOR IMMEDIATE RELEASE Contact:
Auditing and Monitoring Hospitals High-Risk Practice Areas Through External Peer Review
 Auditing and Monitoring Hospitals High-Risk Practice Areas Through External Peer Review Andrew G. Rowe, CEO AllMed Healthcare Management, Inc. Presentation Overview How Centers for Medicare & Medicaid
Auditing and Monitoring Hospitals High-Risk Practice Areas Through External Peer Review Andrew G. Rowe, CEO AllMed Healthcare Management, Inc. Presentation Overview How Centers for Medicare & Medicaid
Payment Strategies: A Comparison of Episodic and Population-based Payment Reform
 Payment Strategies: A Comparison of Episodic and Population-based Payment Reform November 2013 Policymakers across the country are currently engaged in discussions on how to improve the way that health
Payment Strategies: A Comparison of Episodic and Population-based Payment Reform November 2013 Policymakers across the country are currently engaged in discussions on how to improve the way that health
Ohio SIM: Episode-based payment updates. Webinar June 29, 2017
 Ohio SIM: Episode-based payment updates Webinar June 29, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ UT
Ohio SIM: Episode-based payment updates Webinar June 29, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ UT
OptumRx: Measuring the financial advantage
 OptumRx: Measuring the financial advantage New study shows $11-16 PMPM medical savings when Optum care management and Optum pharmacy are provided together with medical benefits. Page 1 Synopsis Optum recently
OptumRx: Measuring the financial advantage New study shows $11-16 PMPM medical savings when Optum care management and Optum pharmacy are provided together with medical benefits. Page 1 Synopsis Optum recently
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Product and Network Innovation: Strategies to Achieve Triple Aim Success. Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013
 Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
Accountable Care: Clinical Integration is the Foundation
 Solutions for Value-Based Care Accountable Care: Clinical Integration is the Foundation CLINICAL INTEGRATION CARE COORDINATION ACO INFORMATION TECHNOLOGY FINANCIAL MANAGEMENT The Accountable Care Organization
Solutions for Value-Based Care Accountable Care: Clinical Integration is the Foundation CLINICAL INTEGRATION CARE COORDINATION ACO INFORMATION TECHNOLOGY FINANCIAL MANAGEMENT The Accountable Care Organization
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Care Redesign: An Essential Feature of Bundled Payment
 Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
A strategy for building a value-based care program
 3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement
 Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Minnesota health care price transparency laws and rules
 Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
About the Report. Cardiac Surgery in Pennsylvania
 Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Basic Standards for Residency Training in Anesthesiology
 Basic Standards for Residency Training in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists Adopted BOT 7/2011, Effective 7/2012 Revised, BOT 6/2012,
Basic Standards for Residency Training in Anesthesiology American Osteopathic Association and American Osteopathic College of Anesthesiologists Adopted BOT 7/2011, Effective 7/2012 Revised, BOT 6/2012,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Healthcare 2015: Win-win or lose-lose?
 IBM Institute for Business Value Healthcare 2015: Win-win or lose-lose? A portrait and a path to successful transformation Presented at Disease Management Colloquium May 19, 2008 Jim Adams, IBM Center
IBM Institute for Business Value Healthcare 2015: Win-win or lose-lose? A portrait and a path to successful transformation Presented at Disease Management Colloquium May 19, 2008 Jim Adams, IBM Center
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH