Crisis on the Continuum: Roles and Responsibilities. Nena Lekwauwa, MD DMH/DD/SAS Susan Saik, MD DSOHF Art Eccleston, Psy.
|
|
|
- Samantha Owen
- 6 years ago
- Views:
Transcription
1 Crisis on the Continuum: Roles and Responsibilities Nena Lekwauwa, MD DMH/DD/SAS Susan Saik, MD DSOHF Art Eccleston, Psy.D DMH/DD/SAS
2 Overview of Practice Response System Learn about the crisis response system from the state s perspective The funding sources available for crisis treatment How do crisis services fit with the rest of the service continuum
3 Crisis System Philosophy: Services should be delivered in least restrictive setting possible, connected to consumers home communities whenever possible, and no more intense than needed to meet consumers needs. Reserve use of state hospitals for those most in need with most challenging conditions in need of longer lengths of stay. Increase use of alternatives to hospitalization whenever possible: Mobile Crisis, Facility Based Crisis, Social Setting Detox, Walk-In Clinics, etc. Maximize use of community inpatient beds.
4 Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments Legislatively mandated report (Session Law , Section 10.7B.) Purpose of the report was to evaluate emergency department length of stay in community-based hospitals in NC 1915 (b)/(c) waiver entities vs. non-waiver entities Medicaid recipients vs. non-medicaid recipients North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
5 Data Collection Process Community-based EDs provided data on admissions with behavioral health crises during the month of November Data collected on 8,757 behavioral health admissions 78 of 114 hospitals provided data - 68 % response rate Data was collected from hospitals but reported by LME catchment area North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
6 Behavioral Health ED Admissions by Disability Group Individuals Presenting to EDs with Behavioral Health Crises by Disability Group Total: 8,757 SA 2, % DD % Unknown % MH 6, % North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
7 Behavioral Health ED Admissions by Insurance Coverage Insurance Status of Individuals Presenting to EDs with Behavioral Health Crises Total: 8,757 Uninsured 2, % Unknown % Medicaid 2, % Other Third Party Payor 3, % North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
8 Behavioral Health ED Admissions by Disposition Disposition of Individuals Presenting to EDs with Behavioral Health Crises Transferred to other facility % Admitted % State psychiatric hospital % Community hospital psychiatric bed 1, % Total = 8,757 Left against medical advice % Left w ithout receiving medical advice % Other/Unknow n % Home w ith existing supports 4, % Home w ith referral to LME % Home w ith referral to private MH % North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
9 ED LOS for a Behavioral Health Crisis by Disposition Overall N=8,592 9:38 Other/Unknown N=566 10:07 Left without receiving medical advice N=50 3:30 Left against medical advice N=118 5:58 Transferred to other facility N=172 8:29 Admitted N=122 22:29 State psychiatric hospital N=239 26:38:00 Community hospital psychiatric bed N=1,904 14:11 Home with referral to LME N=365 10:59 Home with referral to private MH N=659 9:25 Home with existing supports N=4,45 6:38 Average LOS in hours and minutes 0:00 4:48 9:36 14:24 19:12 0:00 4:48 North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
10 Diagnostic Categories with 3 or More ED Readmissions in the Past 30 Days Top Five Diagnostic Categories With 3 or More ED Readmissions in the Past 30 Days N= % 20.00% 15.00% 10.00% 5.00% 0.00% Alcohol Abuse Anxiety Disorders Paranoia/Delusional Disorders Schizophrenia Depressive Disorders Series % 18.64% 12.43% 11.30% 9.04% North Carolina Department of Health and Human Services, 2011, Report on the Provision of Behavioral Health Crisis Services by Hospital Emergency Departments, NC Division of Mental Health, Developmental Disabilities and Substance Abuse Services Available at:
11 Reducing Recidivism Detox in ED and discharge without linkage to treatment services perpetuates cycle of returning to ED. Can we link patients to treatment earlier (from ED or from medical detox)? Outreach by ADATCs to EDs and Medical Detox to engage consumers earlier is a promising new approach.
12 Considering Alternative Settings of Care Almost 2/3 of individuals seen were discharged home with relatively short stays Is it possible that many of these individuals could have their needs met or better met in an alternative setting? If so, what would that setting look like? Would at least some of the individuals that were admitted also be able to be served in an alternative environment and possibly avoid hospitalization?
13 ED Workgroup The North Carolina Department of Health and Human Services instructed the North Carolina Division of Mental Health, Developmental Disabilities and Substance Abuse Services in partnership with various stakeholder groups to consider and advise on actions that would address the following issues:
14 ED Workgroup continued 1. Reducing the number of people entering the Emergency Department with mental illness by promoting early intervention systems and strategies. 2. Reducing the length of stay for individuals with mental illness admitted to hospital emergency departments. 3. Linking consumers to housing, services, and supports to prevent future Emergency Department admissions.
15 ED Workgroup continued To effectively address these issues, the Division of MH/DD/SAS in collaboration with its stakeholders, is working on developing an Action Plan. The plan will describe goals and action steps that will continue to strengthen and improve North Carolina s crisis service system. The Action Plan is intended to serve three major functions:
16 ED Workgroup continued 1. To serve as a roadmap to guide our immediate priorities, as well as priorities over the next several years, with flexibility to respond to unanticipated opportunities and challenges.
17 ED Workgroup continued 2. To act as a communication tool to share our plans with consumers, partners and the public, and engage wider support in achieving these goals.
18 ED Workgroup continued 3. To provide a list of priority solutions showing how additional funding could improve the system of care to individuals with mental illness.
19 Goals There are four primary goals and associated action steps that comprise the framework of this plan: Pre-Crisis Pre-Emergency Department Emergency Department Post-Emergency
20 Pre-Crisis GOAL: To promote early intervention systems and to prevent crisis events through a collaborative effort. Recommendations: 1. Develop and provide crisis/prevention/de-escalation training. 2. Require an enhanced crisis reduction plan for high risk, high volume consumers. 3. Increase provider accountability for consumer outcomes. 4. Convene internal critical care conferences for individuals who have high utilization of crisis services. 5. Develop funding and planning to provide transportation.
21 Pre-Emergency Department GOAL: To reduce the number of people entering the Emergency Department with Behavioral Health issues. Recommendations: 1. Enhance the effectiveness and efficiency of Mobile Crisis Management Services. 2. Augment the role of Facility Based Crisis Centers (FBC) and 24 hour Walk-In Clinics. 3. Work with Law Enforcement. 4. Enhance accountability in First Responders. 5. Develop consistent Screening, Triage, and Referral (STR) procedures. 6. Use non-emergency department resources for medical clearance evals. 7. Work with Magistrates. 8. Provide care coordination. 9. Diversify and strengthen workforce.
22 Emergency Department GOAL: To reduce emergency department length of stay for individuals who present with behavioral health crises. Recommendations: 1. Implement a computerized psychiatry bed registry. 2. Develop protocols and practice guidelines to standardize/utilize best practices for mobile crisis management teams in the emergency department. 3. Clarify and support the role of LMEs with regard to emergency department behavioral health crisis admissions. 4. Reduce legal obstacles. 5. Enhance disposition options for individuals with behavioral health crises in the emergency department. 6. Engage individuals with substance use disorders earlier and link to treatment services
23 Post-Emergency Department GOAL: To link consumers to housing, services, and supports to prevent future Emergency Department admissions. Recommendations: 1. Ensure available housing and essential benefits are available in order to help the person remain successfully in the community and out of emergency departments. 2. Development of a Uniform System of Care Coordination. 3. Implementing Assertive Engagement statewide. 4. Prior to discharge, appointments scheduled with-in 48 hours. 5. Establish local relationships among all stakeholders to facilitate seamless coordination of care.
24 Crisis Services Resources Individual/family/supp orts LME-STR/crisis lines First responders Mobile Crisis Management Walk-In Crisis Telepsychiatry NC START Crisis respite Facility Based Crisis Detox 3-way contract beds Other private inpatient beds State Psychiatric hospitals State ADATCs
25 Crisis Services: SFY11 Funding MCM: $5.7 million state allocation Medicaid = $4.22 M IPRS = $5.03 M Total claims paid = $9.25 M Total persons served = 18,564 Walk-In Crisis: $4.46 million state allocation
26 Crisis Services: SFY11 Funding NC START: $3.2 million state funding Facility Based Crisis Medicaid = $2.15 M IPRS = $7.33 M Total claims paid = $9.48 M Total persons served = 6,892
27 Services in Less Restrictive Settings Services must be robust, accessible, and predictably meet the needs of the consumer.
28 Comprehensive Crisis Center recognizable location - simplified decision tree sharing of unique resources facility and personnel Immediate/convenient access to stepped up or stepped down services Efficiencies gained allow for strengthening of collective crisis services.


29
30 DURHAM CENTER ACCESS: GOALS Reduce state hospital utilization Support community-based treatment Coordinate with outpatient providers to maximize consumer benefit and continuity of care during crisis events Stabilize the consumer and reintegrate into the community Assist individuals who are not engaged with accessing care
31 DCA CRISIS FACILITY: SERVICES 24-hour crisis facility for individuals in crisis 16 facility-based crisis and detox beds for short-term stabilization for adults as alternative to inpatient hospitalization hour crisis evaluation observation rooms (one for juveniles) for short-term intensive intervention to stabilize acute or crisis situations Telephone and face-to-face screening, triage and referral to community providers
32 DCA CRISIS FACILITY: SERVICES Crisis risk assessment Mental health and substance abuse assessment Psychiatric and petition evaluations Non-hospital medical detoxification service
33 TARGET POPULATION: Durham County citizens PROVIDER: DCA CRISIS FACILITY Freedom House Recovery Center TIMELINE: July 2004: Facility opens July 2006: Freedom House contracted August 2008: DCA moves to new facility on Crutchfield Street near Durham Regional Hospital
34 DCA MOBILE CRISIS Community-wide team response for individuals in crisis Teams have capacity to intervene quickly, day or night, when the crisis is occurring LME Alliance: The Durham Center, OPC and Alamance-Caswell TARGET POPULATION: Durham County citizens PROVIDER: Freedom House Recovery Center START DATE: November 2008
35 DCA MOBILE CRISIS: GOALS Stabilize individuals in crisis as quickly as possible and assist their return to pre-crisis level of functioning Avoid unnecessary hospitalizations Make referrals and link to needed services and supports Enable individuals in crisis or distress to access a range of crisis services in a timely and effective manner in their environment or other appropriate setting
36 DCA MOBILE CRISIS: GOALS Provide a consistent, integrated response to crises in the community 24/7/365 Make every effort to restore the individual to the previous level of functioning
37 DCA MOBILE CRISIS: LIMITATIONS Life-threatening emergencies or violent situations, such as a person with a weapon or one attempting to hurt self or others Domestic violence disturbances Requests for transportation in non-crisis situations Requests for step-down services from in-patient hospitalization Requests to serve individuals from other counties and states
38 DCA PSYCHIATRIC WALK-IN CLINICS Office-based outpatient services for adults, children and adolescents Immediate screening/assessment and brief, intensive interventions to resolve crisis and prevent admission to more restrictive level of care Service provided face-to-face at DCA and via telepsychiatry at 4 satellite locations Start date: February 2009 LME Alliance: The Durham Center, OPC and Alamance-Caswell
39 DCA PSYCHIATRIC WALK-IN CLINICS TARGET POPULATIONS AND ELIGIBILITY CRITERIA Children and adults from the identified catchment areas in need of psychiatric services AND: Discharged from State hospitals, private psychiatric hospitals, and community hospitals and are unable to secure a timely appointment in the community; OR Currently NOT served by the Provider Network and need immediate psychiatric assessment and care, medication evaluation and aftercare planning; OR Actively served by a provider, and presenting with needs exceeding provider capacity
40 DCA PSYCHIATRIC WALK-IN CLINICS OUTCOMES/GOALS Improved accessibility of urgent care services for individuals experiencing psychiatric and substance abuse difficulties Reduced need for consumers to go to EDs Reduced need for admissions to hospitals for consumers who can be served in the community Better structure for coordination of care Alternative to EDs for law enforcement interacting with consumers in distress or on petition
41 DCA ASSESSMENT TEAM A group of experienced MH and SA professionals housed at DCA to provide the Durham community with an independent assessment service Available to adults without insurance to determine clinical needs and connect them with appropriate treatment and assistance in the community 1 Supervisor, 3 Assessors, 2 QPs, 1 Admin Assistant, 1 part-time Peer Specialist Operates Monday-Friday, 8:30am-5:00pm
42 DCA ASSESSMENT TEAM: SERVICES Coordinated and planned approach to assessing and connecting individuals in need to the right services and supports available in the community A plan for continued treatment supported by the consumer, family and referring party Support and education Contact with consumer until connection is made with services, including for waitlisted consumers Renewed hope and confidence
43 DCA ASSESSMENT TEAM: RATIONALE Centralization of assessments provides standardization of the assessment process Assessments ensure a consistently intensive, comprehensive evaluation and better integration of services for co-occurring disorders Access to medication or on-site crisis services, SA services or other immediate placement
44 DCA ASSESSMENT TEAM: RATIONALE Providers are unable to accommodate waitlists resulting from reductions in service capacity necessitated by recent budget cuts Care Coordination/Behavioral Health Support Services when clinically appropriate
45 DCA PRIMARY CARE CLINIC OUTCOMES/GOALS Routine and/or non-emergent primary care, physical health screening and/or assessment Connection and/or re-connection to Lincoln Primary Care services Reduce the need for individuals served to go to emergency departments TARGET POPULATION: Durham County citizens participating in any other program at DCA PROVIDER: Lincoln Community Health Center
46 DCA PRIMARY CARE CLINIC LINCOLN COMMUNITY HEALTH CENTER: A leader in providing accessible, affordable, high-quality outpatient health care services to the medically-underserved in Durham County Collaborates with other community partners with a goal of 100% Access and 0 Health Disparities A JCAHO-accredited facility
47 DCA PRIMARY CARE CLINIC: SERVICES All individuals admitted to crisis services provided the opportunity for services Individuals in need of emergent medical care go to Emergency Department Individuals well-connected to primary care provider don t use Lincoln Laboratory services for medical (not BH) issues Operates Monday-Friday, 8:00am-Noon Six patients per day on average

48 The Durham Center and Durham Center Access are key partners in Durham System of Care Network of Care is a comprehensive online source of information about services available to individuals and families and agencies working with them Visit Network of Care at durhamnetworkofcare.org or System of Care at durhamsystemofcare.org

49 KEY COMMUNITY PARTNERS CJRC, The Durham Center, Lincoln Community Health Center, Freedom House Recovery Center Magistrates Office, Durham Police Department, Durham County Sheriffs Office, CIT Program Durham Provider Network First Responders Emergency Departments at Duke, Durham Regional Hospital, VA Medical Center





50

51 Forsyth Behavioral Health Emergency Department Crisis Care Model Todd M. Clark, PhD, LPC, LCAS NCCCP Annual Conference December 6, 2012

52 AGENDA Data Operations Clinical Partnerships Future
53 Data
54 6000 Annual BH Patient Volume FM C ED JUH closed adult Community units. Support Services Charter FMC opened BH 3-bay area in ED CPHS became LME. Target populations implemented HopeRidge - CRH opened w/ decreased Behavioral Health capacity. - IPRS defunded closed for Res SA Tx w/ Mcare/caid 4404 defunded Hospital, WS closed Average Daily Census 26 Patients: reduced 50% Average Length of Stay 38 Hours: reduced 33%
55 Operations
56 Remarkable Environment for the BH Patient Safety (Patients and Staff) 10-bed secured area in ED / 25-bed ED Holding area Private rooms Video assisted monitoring Staff rounding Staffing (In the E.D.) Nursing Team RNs and Psyc Techs (CNA) Dedicated BH Mid-levels (NP & PA) Access Team LPC, LCSW, LCAS Rec Therapy TelePsyc Services
57 Clinical
58 Decompensation Increases Length of Stay Evaluations Pharmacy Tech Reconcile meds Access Team Quick glance Assess & disposition Recreation Therapy Spending time Support system Community resources Coping strategies Relaxation strategies BH Mid-level Evaluation Re-assessments Medical acuity
59 Decompensation Increases Length of Stay Programming Recreation Therapy Reversing decompensation Safer and productive E.D. mileau Re-assessment opportunities Staffing cost reduction Alternative to sitters Telepsyc Services Immediate Psyc consult for ED provider Validate OP discharge plans Assist with fence sitter dispositions
60 Partnerships
61 Building Relationships LME Care Coordinators = gateway to resources Homeless Liaison Regular operational-focused meetings Administrators: remove systemic or oganizational barriers / provide resources Provider Agencies: CABHA, ACT Teams, Support Services Community Resources Homeless Shelters Long Term Care Facilities Medical/Medication Clinics Mobile Crisis Response Team BH Referral Development Rep 1. Invite them in. 2. Visit their shop. 3. Create the easy button.
62 Future Current Model: Temporary solution to mitigate the current tsunami of volume occurring in past 2 years. Failure: Behavioral consumer come to medical E.D. seeking care. Ideal: A robust continuum of community services that proactively meets the needs of consumers, where they are.

63 Questions?

64 Director Todd M. Clark PhD LPC O F P My # 1 job responsibility is to deliver the most remarkable patient experience, in every dimension, every time. tclark@novanthealth.org
65 First Responder
66 First Responder Requirements What is it? Applies to CABHAs Defines how we respond to clients in crisis Outlines responsibilities Implementation Update # 86 April 6, 2011
67 Critical Decision Points ED Crisis Plan Support Magistrate FBC EMS LEO Self Family Clinical Home WIC LME/STR MCM

68 First Responder: When and to whom does it apply? Applies to consumers receiving any services through a CABHA Applies to Crisis situations High level of mental or emotional distress, or an episode, which without immediate intervention will foreseeably result in the person s condition worsening, environmental instability or could result in harm to self or others. Is 24/7/365
69 First Responder: What are the requirements? Be able to respond directly and also collaborate/guide treatment when others involved Written policies and procedures for consumers needing assistance in a crisis Information for the consumer to call the CABHA first before other responders (such as EDs and MCM) Phone number that reaches a live person 24/7/365
70 First Responder: What are the requirements? Response may be telephonic but there must be an attempt to provide face to face services before referring consumer to alternative crisis responders. If a referral occurs to another crisis responder, the CABHA must communicate and facilitate coordination of care.
71 Reasonable Attempt Policy and procedure outlining how you respond to crises Patient ed. about the policy/procedure Assessment - may be telephonic but must follow accepted standards of care. (CC, History incl. how past crises were handled, symptoms, risk/dangerousness, support systems, etc) Conclusions and determination of needed level of care should be supported by facts contained in the assessment and a rationale. First Responder that is built into service definition must be responded to by the appropriate team.
72 MCM in the Continuum MCT embedded within CABHA Provider with array of services (also housing FBC, WIC, etc) Ability to assess needs and link to appropriate services/level of care Use of licensed staff for initial assessments Inclusion of psychiatrists in workflow QA Care Coordination utilizing applications that track the consumer from crisis through resolution
73 The Role Of The LME Christina Carter, MSW Chief Operating Officer Smoky Mountain Center 73
74 LME Responsibilities Care Coordination: LME clinicians & QPs monitor inpatient admission rates Rapid readmits of consumers who are not engaged in services Provider & Stakeholder meetings: LME staff call meetings with providers, hospitals and law enforcement to review long ED wait times and high risk cases Concurrent reviews: Inpatient facilities Facility based crisis and detox admissions Discharge planning for high risk and complex cases 74
75 LME Responsibilities Post discharge tracking to ensure engagement Gap analysis and trouble shooting for high risk consumers with unmet needs System management Stable funding with realistic billing and Medicaid expectations Monitor outcomes including average length of stay, wait times, rapid readmission rates, consumer satisfaction and engagement in services 75
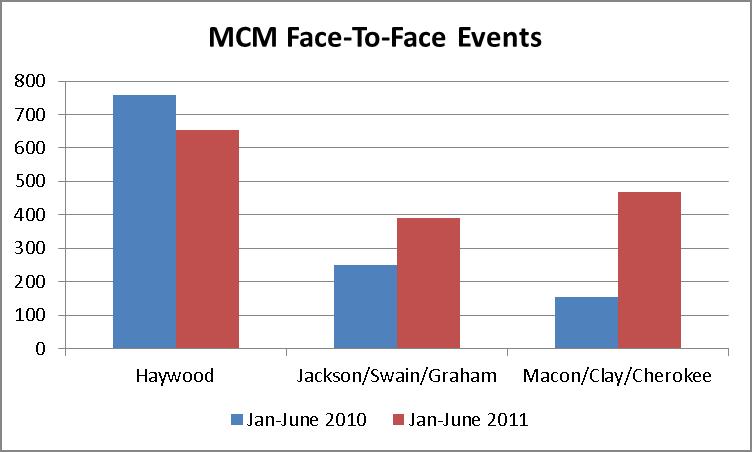
76 Integrating Mobile Crisis With The Service System Doug Trantham

77 The Smoky Mountain Center and Appalachian Community Services Crisis System
78 History Emergency services developed by SMC The Balsam Center crisis unit opened in 2004 First exam pilot initiated in March 2004 Opened Behavioral Health Unit at HRMC 2009 Converted to a full mobile crisis management model in 2010 Operation assumed by ACS July 1, 2010

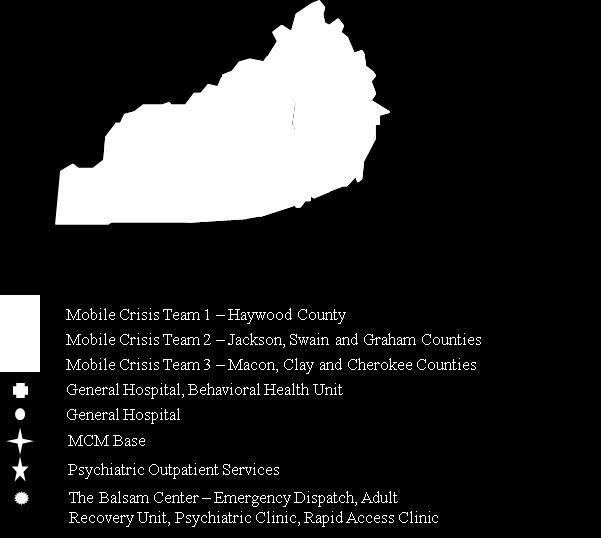
79 Service Area


80 Key Features Of The SMC/ACS Model
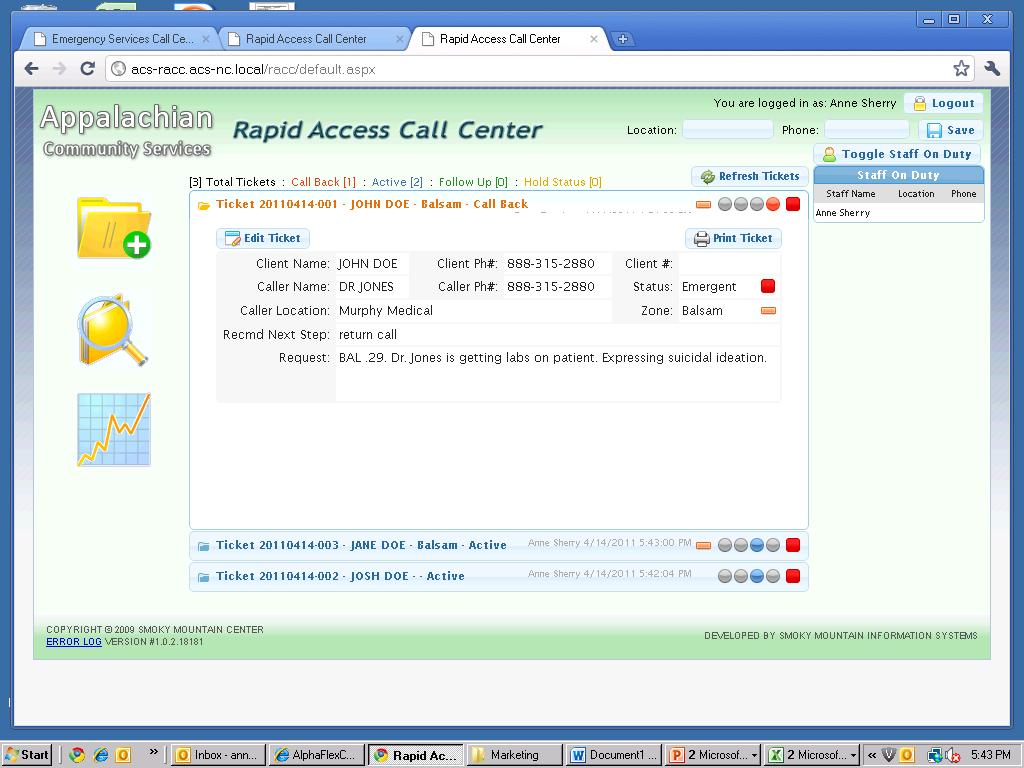
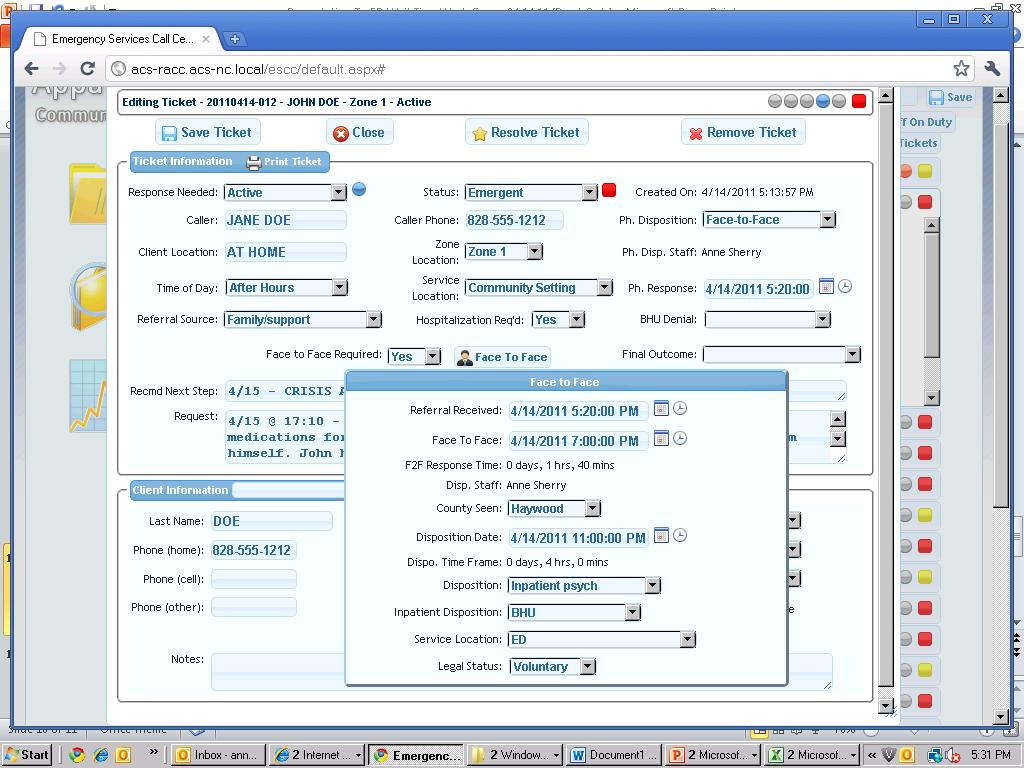
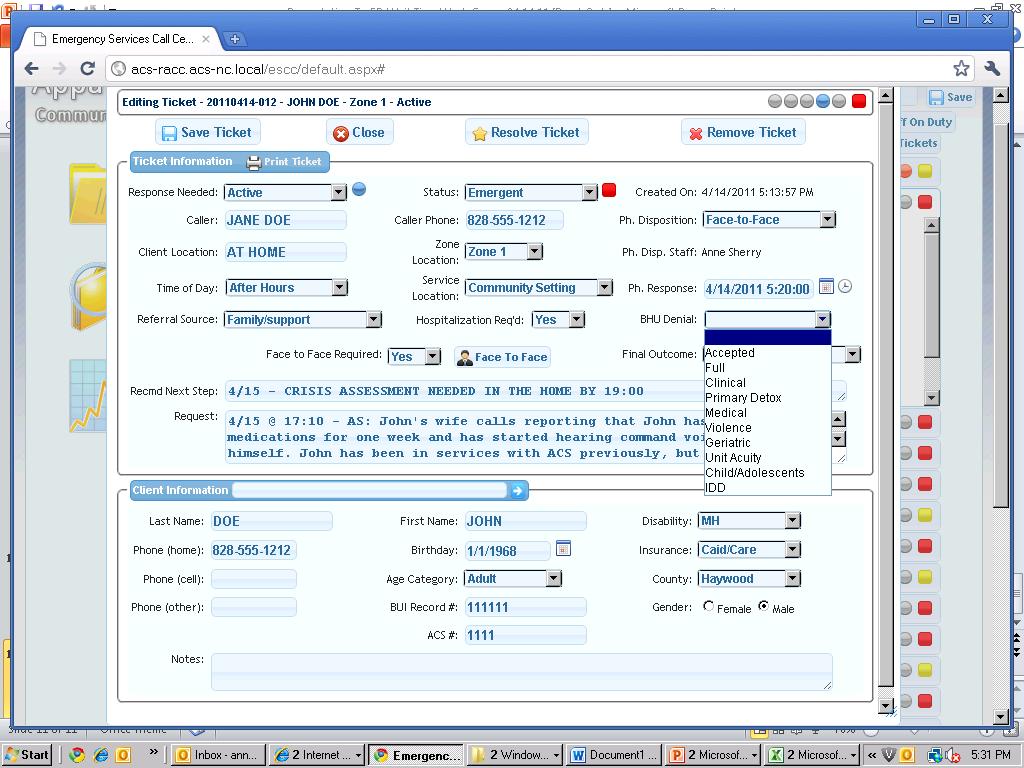
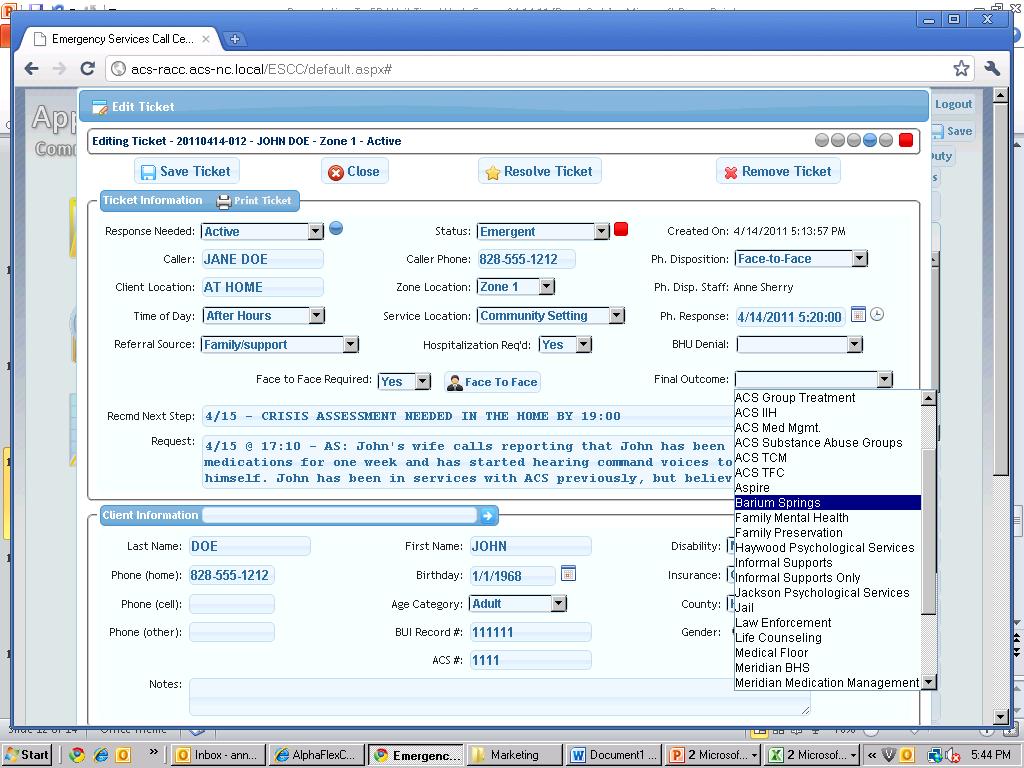
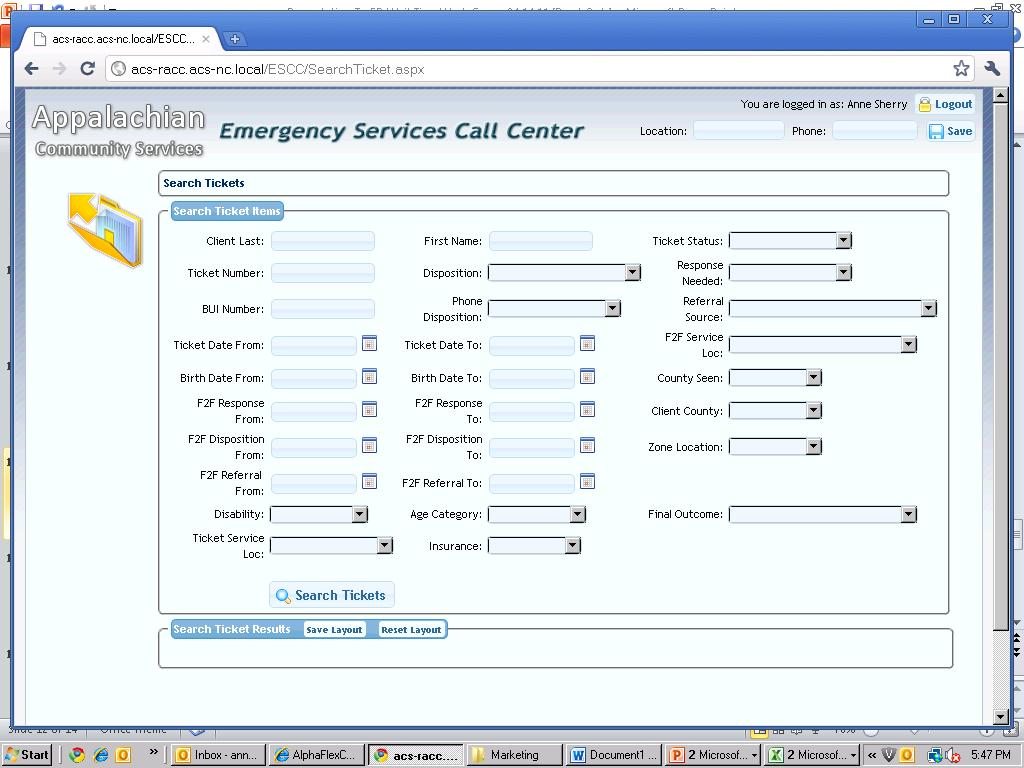
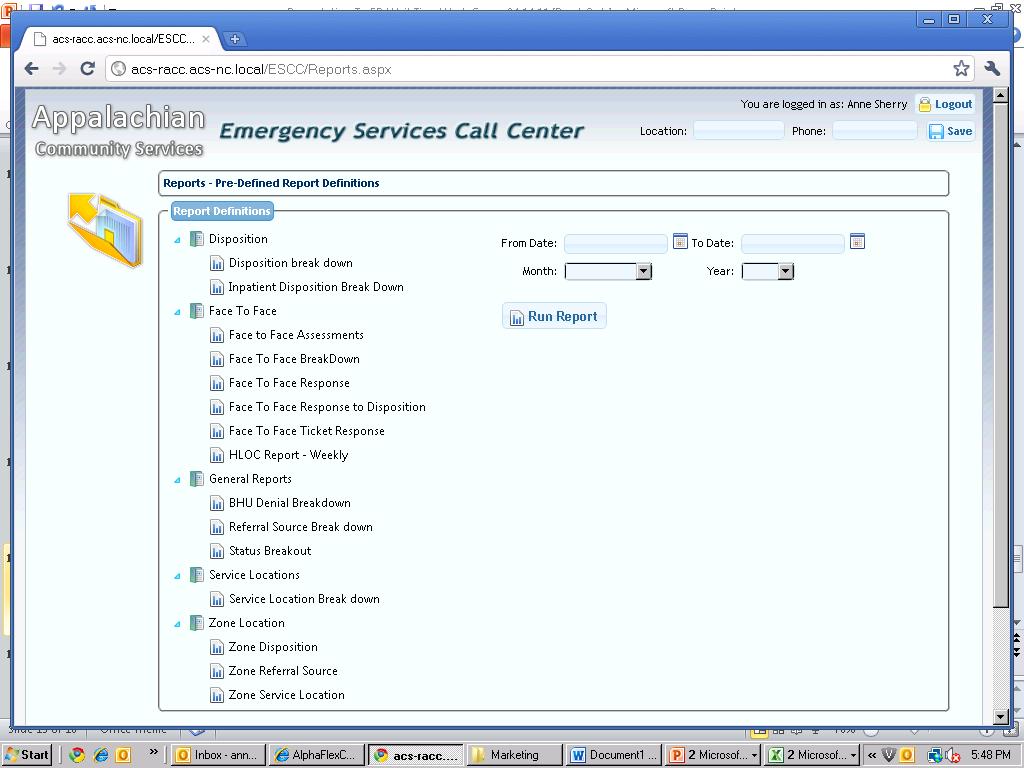
81 Emergency Dispatch Call center staffed 24/7/365 Receives all requests for service and information directly Tracks urgent/emergent referrals across region using custom web based tracking software Triages calls and assigns to available clinicians Reporting, quality assurance, faxing, support
82 Reliance on awake rather than on call staff Reliance on licensed clinicians for initial response Regular use of psychiatric backup MCM clinicians complete many IVC first exams - approximately per year (loss of LCAS in program restricts IVC capability) Provide emergency services under contract as well as billable MCM services Credentialed staff respond to local emergency departments Integrated with comprehensive CABHA including facility based crisis, walk-in centers, outpatient, psychiatric and enhanced services
83 MCM staff are specialists, but crisis response is a priority for all ACS staff Daily ED report sent To LME Official notification to LME of any client in ED beyond 72 hours, or any client expected to wait longer than 72 hours Team meetings scheduled with LME/providers/stakeholders for clients waiting in ED longer than 72 hours or cases of concern Very extensive marketing with community stakeholders.
84 Use of QPs for follow up and engagement Expansion of service upstream to avert crisis prior to involuntary petition or ED, and downstream to ensure engagement and stabilization following the crisis. Shifting from ED to community response Diversion from ED and IVC Promotion of CIT with law enforcement
85 Benefits One number to access services Avoid multiple levels of triage Calls are tracked until disposition, often for days or weeks, while maintaining continuity Many consumers are diverted to outpatient, crisis unit or local inpatient services Much greater penetration rate in rural communities
86
87 Community Response Community 30% 38% ED 70% 62%
88 Daily ED Report To LME Date/Time: 4/14/11 6:00 4/14/2011 6:00 Totals: SR N/C R SMC Number in EDs: Number in ED Awaiting Transfer: Facility: Murphy MC Haywood RMC Cherokee IH Harris RH Angel MC Highlands H Swain MC Response?: Yes Yes Number in ED: 2 2 Number Awaiting Txfr: Southern Region Patient # Primary Disability Facility Location Funding County Referral Source Age xxxx Adult MH Murphy MC ED Medicaid Cherokee Self-Referred (W xxxx Adult MH Haywood RMC ED Other Insuranc Haywood IVC xxxx Adult MH Murphy MC ED Indigent Cherokee Self-Referred (W xxxx Geriatric MH Haywood RMC ED 'Care/'Caid Haywood Self-Referred (W Elapsed time in hours Currently Violent? Gender Detox Admit Date Admit Time Disposition 04/13/11 23: Undetermined No Female No 04/13/11 23: Undetermined No Male No 04/13/11 23: Undetermined No Male No 04/13/11 17: Undetermined No Male No 3 Way Bed? SMC use Only
89
90
91
92
93
94
95
NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS
 MENTAL HEALTH DEVELOPMENTAL DISABILITIES & SUBSTANCE ABUSE NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS Status of Council Action: Developed by Clinical Services & Support Wrkgroup 1/11/08: Endorsed by
MENTAL HEALTH DEVELOPMENTAL DISABILITIES & SUBSTANCE ABUSE NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS Status of Council Action: Developed by Clinical Services & Support Wrkgroup 1/11/08: Endorsed by
CRISIS SERVICES. N. C. Department of Health and Human Services Division of Mental Health, Developmental Disabilities and Substance Abuse Services
 APRIL 2012 CRISIS SERVICES State Authorization: G. S. 122C-147.1; S.L. 2006-66 (Senate Bill 1741), Part X, Section 10.26 (a) - (f); S.L. 2007-323 (House Bill 1473), Part X, Section 10.49; S.L.2008-107
APRIL 2012 CRISIS SERVICES State Authorization: G. S. 122C-147.1; S.L. 2006-66 (Senate Bill 1741), Part X, Section 10.26 (a) - (f); S.L. 2007-323 (House Bill 1473), Part X, Section 10.49; S.L.2008-107
Division of Mental Health, Developmental Disabilities & Substance Abuse Services NC Mental Health and Substance Use Service Array Survey
 Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Behavioral Health Services. San Francisco Department of Public Health
 Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management
 Jan M. Kasofsky, PH.D. Executive Director, Capital Area Human Services Clinical Design Committee Chair A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management BATON ROUGE
Jan M. Kasofsky, PH.D. Executive Director, Capital Area Human Services Clinical Design Committee Chair A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management BATON ROUGE
ANNUAL REPORT Overview of services provided to Carteret County August 1, 2016 July 31, 2017
 ANNUAL REPORT Overview of services provided to Carteret County August 1, 2016 July 31, 2017 CONNECTING THE PIECES; CREATING STRONGER FAMILIES Serving Bertie, Beaufort, Brunswick, Camden, Carteret, Chowan,
ANNUAL REPORT Overview of services provided to Carteret County August 1, 2016 July 31, 2017 CONNECTING THE PIECES; CREATING STRONGER FAMILIES Serving Bertie, Beaufort, Brunswick, Camden, Carteret, Chowan,
OUTPATIENT SERVICES. Components of Service
 OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
EMERGENCY SERVICES PROGRAM (ESP)
") EMERGENCY SERVICES PROGRAM (ESP) Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally,
EMERGENCY SERVICES PROGRAM (ESP) Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally,
Quality Management & Program Development (QMPD)
") Quality Management & Program Development (QMPD) QMPD Areas of Responsibility Report/Trends Outcomes/Evaluation Data Analysis NC TOPPS/NC SNAP Strategic Planning Results Based Accountability Best Practices
Quality Management & Program Development (QMPD) QMPD Areas of Responsibility Report/Trends Outcomes/Evaluation Data Analysis NC TOPPS/NC SNAP Strategic Planning Results Based Accountability Best Practices
Outcome and Process Evaluation Report County-wide Triage Teams
 Mental Health Services Oversight and Accountability Commission (MHSOAC) Personnel Grant (SB 82) Triage Personnel Grant Report Outcome and Process Evaluation Report County-wide Triage Teams Grant Years
Mental Health Services Oversight and Accountability Commission (MHSOAC) Personnel Grant (SB 82) Triage Personnel Grant Report Outcome and Process Evaluation Report County-wide Triage Teams Grant Years
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare
 Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
What is the Judge Guy Herman Center for Mental Health Crisis Care?
 FAQs: Judge Guy Herman Center for Mental Health Crisis Care What is the Judge Guy Herman Center for Mental Health Crisis Care? The Judge Herman Center for Mental Health Crisis Care provides short term
FAQs: Judge Guy Herman Center for Mental Health Crisis Care What is the Judge Guy Herman Center for Mental Health Crisis Care? The Judge Herman Center for Mental Health Crisis Care provides short term
AOPMHC STRATEGIC PLANNING 2018
 SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
North Carolina s Transformation to Managed Care
 North Carolina s Transformation to Managed Care Jay Ludlam, Assistant Secretary Department of Health and Human Services December 2017 My background Only 10+ years of experience in Medicaid Assistant Attorney
North Carolina s Transformation to Managed Care Jay Ludlam, Assistant Secretary Department of Health and Human Services December 2017 My background Only 10+ years of experience in Medicaid Assistant Attorney
State-Funded Enhanced Mental Health and Substance Abuse Services
 and and Contents 1.0 Description of the Service... 3 2.0 Individuals Eligible for State-Funded Services... 3 3.0 When State-Funded Services Are Covered... 3 3.1 General Criteria... 3 3.2 Specific Criteria...
and and Contents 1.0 Description of the Service... 3 2.0 Individuals Eligible for State-Funded Services... 3 3.0 When State-Funded Services Are Covered... 3 3.1 General Criteria... 3 3.2 Specific Criteria...
AOPMHC STRATEGIC PLANNING 2016
 SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
Connecting Inpatient and Residential Treatment to Systems of Care
 0th Annual RTC Conference Presented in Tampa, March 007 Connecting Inpatient and Residential Treatment to Systems of Care Mary Armstrong, Ph.D., Norín Dollard, Ph.D., Stephanie Romney, Ph.D., Keren S.
0th Annual RTC Conference Presented in Tampa, March 007 Connecting Inpatient and Residential Treatment to Systems of Care Mary Armstrong, Ph.D., Norín Dollard, Ph.D., Stephanie Romney, Ph.D., Keren S.
The North Carolina Behavioral Health Crisis Referral System
 The North Carolina Behavioral Health Crisis Referral System Krista Ragan, MA BH-CRSys Program Manager, NC Division of Mental Health, Developmental Disabilities & Substance Abuse Services November 6 th,
The North Carolina Behavioral Health Crisis Referral System Krista Ragan, MA BH-CRSys Program Manager, NC Division of Mental Health, Developmental Disabilities & Substance Abuse Services November 6 th,
IV. Clinical Policies and Procedures
 A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
empowering people to build better lives their efforts to meet economic, social and emotional challenges and enhance their well-being
 Community Care Alliance empowering people to build better lives Adult Mental Health Services Basic Needs Assistance Child & Family Services Education Employment & Training Housing Stabilization & Residential
Community Care Alliance empowering people to build better lives Adult Mental Health Services Basic Needs Assistance Child & Family Services Education Employment & Training Housing Stabilization & Residential
Grady Health System, Atlanta GA. Upstream Crisis Intervention
 2014 Changes EMS Leadership Conference Augusta, Ga Grady Health System, Atlanta GA. Upstream Crisis Intervention Michael Colman, MPA, NRP, Director of EMS Operations at Grady Health Systems Arthur H. Yancey,
2014 Changes EMS Leadership Conference Augusta, Ga Grady Health System, Atlanta GA. Upstream Crisis Intervention Michael Colman, MPA, NRP, Director of EMS Operations at Grady Health Systems Arthur H. Yancey,
Department of Vermont Health Access Department of Mental Health. dvha.vermont.gov/ vtmedicaid.com/#/home
 Department of Vermont Health Access Department of Mental Health dvha.vermont.gov/ vtmedicaid.com/#/home ... 2 INTRODUCTION... 3 CHILDREN AND ADOLESCENT PSYCHIATRIC ADMISSIONS... 7 VOLUNTARY ADULTS (NON-CRT)
Department of Vermont Health Access Department of Mental Health dvha.vermont.gov/ vtmedicaid.com/#/home ... 2 INTRODUCTION... 3 CHILDREN AND ADOLESCENT PSYCHIATRIC ADMISSIONS... 7 VOLUNTARY ADULTS (NON-CRT)
Family & Children s Services. Center
 Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services Comprehensive Case Management for AMH/ASU.
 NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services Comprehensive Case Management for AMH/ASU Table of Contents 1.0 Description of the Procedure, Product, or Service...
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services Comprehensive Case Management for AMH/ASU Table of Contents 1.0 Description of the Procedure, Product, or Service...
CHILDREN'S MENTAL HEALTH ACT
 40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
What are MCOs? (b)/(c) refers to the type of waiver approved by CMS to allow this type of managed care program. The
/(c) refers to the type of waiver approved by CMS to allow this type of managed care program. The") Advocating in Medicaid Managed Care-Behavioral Health Services What is Medicaid managed care? How does receiving services through managed care affect me or my family member? How do I complain if I disagree
Advocating in Medicaid Managed Care-Behavioral Health Services What is Medicaid managed care? How does receiving services through managed care affect me or my family member? How do I complain if I disagree
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Cardinal Innovations Child Continuum of Care Philosophy. March 2014
 Cardinal Innovations Child Continuum of Care Philosophy March 2014 Disclaimer Information provided in this presentation pertains only to the counties in the Cardinal Innovations Healthcare Solutions Region.
Cardinal Innovations Child Continuum of Care Philosophy March 2014 Disclaimer Information provided in this presentation pertains only to the counties in the Cardinal Innovations Healthcare Solutions Region.
Smoky Mountain Center Report to the North Carolina General Assembly Joint Appropriations Subcommittee on Health and Human Services
 Smoky Mountain Center Report to the North Carolina General Assembly Joint Appropriations Subcommittee on Health and Human Services Presented by Brian Ingraham, CEO February 27, 2013 Access to Services:
Smoky Mountain Center Report to the North Carolina General Assembly Joint Appropriations Subcommittee on Health and Human Services Presented by Brian Ingraham, CEO February 27, 2013 Access to Services:
SUBSTANCE ABUSE & HEALTH CARE SERVICES HEALTH SERVICES. Fiscal Year rd Quarter
 HEALTH SERVICES To administer and manage contracted services to eligible persons in need of health care or related support services, and to promote health maintenance through education and intervention.
HEALTH SERVICES To administer and manage contracted services to eligible persons in need of health care or related support services, and to promote health maintenance through education and intervention.
Community Crisis Stabilization Treatment Response Protocols
 Community Crisis Stabilization Treatment Response Protocols Crisis Response-Treatment Protocols [February, 2017] 1461 Kensington Ave Buffalo, New York 14215 716.898.4950 millenniumcc.org Table of Contents
Community Crisis Stabilization Treatment Response Protocols Crisis Response-Treatment Protocols [February, 2017] 1461 Kensington Ave Buffalo, New York 14215 716.898.4950 millenniumcc.org Table of Contents
BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017
 OUTPATIENT PROGRAM PLAN 2017") BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017 REVIEWED AND UPDATED NOVEMBER 2017 OUR MISSION PHILOSOPHY The staff of the Berkeley Community Mental Health Center, in partnership
BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017 REVIEWED AND UPDATED NOVEMBER 2017 OUR MISSION PHILOSOPHY The staff of the Berkeley Community Mental Health Center, in partnership
MENTAL HEALTH CARE SERVICES AND EXPENDITURES. East Texas Council of Governments. June 30, Morningside.
 MENTAL HEALTH CARE SERVICES AND EXPENDITURES East Texas Council of Governments June 30, 2014 Morningside R e s e a r c h A N D C o n s u l t i n G, I n c www.morningsideresearch.com MENTAL HEALTH CARE
MENTAL HEALTH CARE SERVICES AND EXPENDITURES East Texas Council of Governments June 30, 2014 Morningside R e s e a r c h A N D C o n s u l t i n G, I n c www.morningsideresearch.com MENTAL HEALTH CARE
From Triage to Intervention: A Crisis Care Model for Persons with IDD. Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S
 From Triage to Intervention: A Crisis Care Model for Persons with IDD Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S Examples of Barriers Lack of information Access to professionals
From Triage to Intervention: A Crisis Care Model for Persons with IDD Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S Examples of Barriers Lack of information Access to professionals
Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions
: Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions") Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough understanding of Intensive
Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough understanding of Intensive
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Macomb County Community Mental Health Level of Care Training Manual
 1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
Major Dimensions of Managed Behavioral Health Care Arrangements Level 3: MCO/BHO and Provider Contract
 Introduction To understand how managed care operates in a state or locality it may be necessary to collect organizational, financial and clinical management information at multiple levels. For instance,
Introduction To understand how managed care operates in a state or locality it may be necessary to collect organizational, financial and clinical management information at multiple levels. For instance,
Urgent Matters Learning Webinar December 16, 2010
 Urgent Matters Learning Webinar December 16, 2010 Providing Health Care for the Acute Mentally Ill: A Community Response San Antonio, Texas David A. Hnatow, MD, FAAEM, FACEP Emergency Medicine Physician,
Urgent Matters Learning Webinar December 16, 2010 Providing Health Care for the Acute Mentally Ill: A Community Response San Antonio, Texas David A. Hnatow, MD, FAAEM, FACEP Emergency Medicine Physician,
MENTAL HEALTH, SUBSTANCE ABUSE, AND DEVELOPMENTAL SERVICES
 MENTAL HEALTH, SUBSTANCE ABUSE, AND DEVELOPMENTAL SERVICES The Department of Mental Health, Substance Abuse, and Developmental Services (MHSADS) is responsible for the public mental health, substance abuse,
MENTAL HEALTH, SUBSTANCE ABUSE, AND DEVELOPMENTAL SERVICES The Department of Mental Health, Substance Abuse, and Developmental Services (MHSADS) is responsible for the public mental health, substance abuse,
Crisis Triage, Walk-ins and Mobile Crisis Services
 Section 10.15 Crisis Triage, Walk-ins and Mobile Crisis Services 10.15.1 Introduction 10.15.2 References 10.15.3 Scope 10.15.4 Did you know? 10.15.5 Definitions 10.15.6 Procedures 10.15.6-A Triage 10.15.6-B
Section 10.15 Crisis Triage, Walk-ins and Mobile Crisis Services 10.15.1 Introduction 10.15.2 References 10.15.3 Scope 10.15.4 Did you know? 10.15.5 Definitions 10.15.6 Procedures 10.15.6-A Triage 10.15.6-B
San Francisco Department of Public Health Barbara A. Garcia, MPA Director of Health
 Overview San Francisco Department of Public Health Medical Respite Fact Sheet December 18, 2017 The Medical Respite program has provided essential post-hospital care to homeless clients in San Francisco
Overview San Francisco Department of Public Health Medical Respite Fact Sheet December 18, 2017 The Medical Respite program has provided essential post-hospital care to homeless clients in San Francisco
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
Cardinal Innovations Healthcare 2017 Needs and Gaps Analysis
 2017 Community Mental Health, Substance Use and Developmental Disabilities Services Needs and Gaps Analysis for the Triad Region (Formerly known as CenterPoint Human Services) This study assesses the community
2017 Community Mental Health, Substance Use and Developmental Disabilities Services Needs and Gaps Analysis for the Triad Region (Formerly known as CenterPoint Human Services) This study assesses the community
An Update on Our Work
 An Update on Our Work Improving the psychiatric crisis and emergency services system in Central Ohio Franklin County Psychiatric Crisis and Emergency System Task Force (PCES) May 2017 The need for emergency
An Update on Our Work Improving the psychiatric crisis and emergency services system in Central Ohio Franklin County Psychiatric Crisis and Emergency System Task Force (PCES) May 2017 The need for emergency
TENNESSEE S CRISIS RESPITE SERVICES
 TENNESSEE S CRISIS RESPITE SERVICES Tennessee Department of Mental Health and Substance Abuse Services Office of Crisis Services and Suicide Prevention Description A facility-based, voluntary service that
TENNESSEE S CRISIS RESPITE SERVICES Tennessee Department of Mental Health and Substance Abuse Services Office of Crisis Services and Suicide Prevention Description A facility-based, voluntary service that
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS)
") NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
Mental Health Board Member Orientation & Training
 1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
TARRANT COUNTY DIVERSION INITIATIVES
 TARRANT COUNTY DIVERSION INITIATIVES Texas Council June 2015 Ramey C. Heddins, CCHP Director Mental Health Support Services Kathleen Carr Rae, Public Policy Specialist WHAT IS THE PROBLEM? Prison 3-year
TARRANT COUNTY DIVERSION INITIATIVES Texas Council June 2015 Ramey C. Heddins, CCHP Director Mental Health Support Services Kathleen Carr Rae, Public Policy Specialist WHAT IS THE PROBLEM? Prison 3-year
Ohio Department of Mental Health (ODMH) Accomplishments
 Accomplishments") Ohio Department of Mental Health (ODMH) Accomplishments Since 2007, ODMH has achieved more than $30 million in operational cost savings in its state psychiatric hospitals and central office, while maintaining
Ohio Department of Mental Health (ODMH) Accomplishments Since 2007, ODMH has achieved more than $30 million in operational cost savings in its state psychiatric hospitals and central office, while maintaining
A Model for Psychiatric Emergency Services
 A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
Psychiatric Patient Boarding Problems in the Emergency Department
 Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Residential Level Transitions: Levels III and IV
 Residential Level Transitions: Levels III and IV Joint Legislative Oversight Committee on MH/DD/SAS September 8, 2010 Mark J. O Donnell, O M.P.H. DMH/DD/SAS 1 Why Changes Were Made? FY 2009-10 budget greatly
Residential Level Transitions: Levels III and IV Joint Legislative Oversight Committee on MH/DD/SAS September 8, 2010 Mark J. O Donnell, O M.P.H. DMH/DD/SAS 1 Why Changes Were Made? FY 2009-10 budget greatly
Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY
 ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
FAQs: Judge Guy Herman Center for Mental Health Crisis Care
 FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care offers a new type of mental health crisis care for adults living in
FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care offers a new type of mental health crisis care for adults living in
Understanding the Referral Criteria and Process to MH/SUD Care Coordination
 Understanding the Referral Criteria and Process to MH/SUD Care Coordination Overview of Alliance MH/SUD Care Coordination What is MH/SUD Care Coordination? What is the Eligibility Criteria for Care Coordination?
Understanding the Referral Criteria and Process to MH/SUD Care Coordination Overview of Alliance MH/SUD Care Coordination What is MH/SUD Care Coordination? What is the Eligibility Criteria for Care Coordination?
STATE OF CONNECTICUT. Department of Mental Health and Addiction Services. Concerning. DMHAS General Assistance Behavioral Health Program
 Page 1 of 81 pages Concerning Subject Matter of Regulation DMHAS General Assistance Behavioral Health Program a The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to
Page 1 of 81 pages Concerning Subject Matter of Regulation DMHAS General Assistance Behavioral Health Program a The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to
FAQs: Judge Guy Herman Center for Mental Health Crisis Care
 FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care is launching a new type of mental health crisis service for people living
FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care is launching a new type of mental health crisis service for people living
Report from Mental Health Taskforce On Mental Health Services in Macon County
 Report from Mental Health Taskforce On Mental Health Services in Macon County Compiled by: Macon County Mental Health Taskforce June 4, 2008 Introduction The Macon County Board of County Commissioners,
Report from Mental Health Taskforce On Mental Health Services in Macon County Compiled by: Macon County Mental Health Taskforce June 4, 2008 Introduction The Macon County Board of County Commissioners,
Clinical Services. clean NYS Driver s License, fingerprinting, criminal record check, and approval from NYS Office of Mental Health.
 Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Effective 11/13/2017 1
 Commonwealth of Massachusetts Executive Office of Health and Human Services www.mass.gov/masshealth In-Home Therapy Services Performance Specifications Providers contracted for this level of care or service
Commonwealth of Massachusetts Executive Office of Health and Human Services www.mass.gov/masshealth In-Home Therapy Services Performance Specifications Providers contracted for this level of care or service
Drug Medi-Cal Organized Delivery System
 Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Southwest Texas Regional Advisory Council
 Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Attachment A INYO COUNTY BEHAVIORAL HEALTH. Annual Quality Improvement Work Plan
 Attachment A INYO COUNTY BEHAVIORAL HEALTH Annual Quality Improvement Work Plan 1 Table of Contents Inyo County I. Introduction and Program Characteristics...3 A. Quality Improvement Committees (QIC)...4
Attachment A INYO COUNTY BEHAVIORAL HEALTH Annual Quality Improvement Work Plan 1 Table of Contents Inyo County I. Introduction and Program Characteristics...3 A. Quality Improvement Committees (QIC)...4
The Behavioral Health System. Presentation to the House Select Committee on Mental Health
 The Behavioral Health System Presentation to the House Select Committee on Mental Health John Hellerstedt, M.D. Commissioner Lauren Lacefield Lewis Assistant Commissioner Division for Mental Health and
The Behavioral Health System Presentation to the House Select Committee on Mental Health John Hellerstedt, M.D. Commissioner Lauren Lacefield Lewis Assistant Commissioner Division for Mental Health and
PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients.
 0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
Rating Tool for Community Level Implementation of the System of Care Approach. for Children, Adolescents, and Young Adults with Mental Health
 Introduction Rating Tool for Community Level Implementation of the System of Care Approach for Children, Adolescents, and Young Adults with Mental Health Purpose Challenges and their Families The purpose
Introduction Rating Tool for Community Level Implementation of the System of Care Approach for Children, Adolescents, and Young Adults with Mental Health Purpose Challenges and their Families The purpose
Children's Crisis Residential Services Study
 NAMI MINNESOTA and ASPIRE MN Children's Crisis Residential Services Study Report to the Minnesota Department of Human Services June 2017 Table of Contents Executive Summary... 3 Introduction...6 Background...11
NAMI MINNESOTA and ASPIRE MN Children's Crisis Residential Services Study Report to the Minnesota Department of Human Services June 2017 Table of Contents Executive Summary... 3 Introduction...6 Background...11
Beaver County Sequential Intercept Model and System of Care. Forensic Rights Conference December 1, 2011
 Beaver County Sequential Intercept Model and System of Care Forensic Rights Conference December 1, 2011 1 Agenda Overview of Beaver County Progression of Forensic / Behavioral Health Initiatives The Sequential
Beaver County Sequential Intercept Model and System of Care Forensic Rights Conference December 1, 2011 1 Agenda Overview of Beaver County Progression of Forensic / Behavioral Health Initiatives The Sequential
LOUISIANA MEDICAID PROGRAM ISSUED: 08/24/17 REPLACED: 07/06/17 CHAPTER 2: BEHAVIORAL HEALTH SERVICES APPENDIX B GLOSSARY/ACRONYMS PAGE(S) 5 GLOSSARY
 5 GLOSSARY") GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services
 Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
Brief Overview: Mental Health Urgent Care
 Brief Overview: Mental Health Urgent Care John Boyd, Psy.D, MHA, FACHE Sutter s System Chief Mental Health Officer Email: boydj@sutterhealth.org Phone: (916) 208-0267 johnboydpsyd Historical Context Insufficient
Brief Overview: Mental Health Urgent Care John Boyd, Psy.D, MHA, FACHE Sutter s System Chief Mental Health Officer Email: boydj@sutterhealth.org Phone: (916) 208-0267 johnboydpsyd Historical Context Insufficient
ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB)
") ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB) NOTICE OF INTENT TO CONTRACT (NIC) FOR ADMINISTRATIVE SERVICES ONLY (ASO) FOR HEALTH MAINTENANCE ORGANIZATION PLAN
ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB) NOTICE OF INTENT TO CONTRACT (NIC) FOR ADMINISTRATIVE SERVICES ONLY (ASO) FOR HEALTH MAINTENANCE ORGANIZATION PLAN
Medicaid and the. Bus Pass Problem
 Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
NC START. Lisa Wolfe NC START East Director. August Reinventing Quality Conference Baltimore MD
 NC START Lisa Wolfe NC START East Director August 9 2010 Reinventing Quality Conference Baltimore MD Who is eligible for NC START? At least 18 years of age Confirmed developmental disability diagnosis
NC START Lisa Wolfe NC START East Director August 9 2010 Reinventing Quality Conference Baltimore MD Who is eligible for NC START? At least 18 years of age Confirmed developmental disability diagnosis
Medicaid Funded Services Plan
 Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
Intensive In-Home Services Training
 Intensive In-Home Services Training Intensive In Home Services Definition Intensive In Home Services is an intensive, time-limited mental health service for youth and their families, provided in the home,
Intensive In-Home Services Training Intensive In Home Services Definition Intensive In Home Services is an intensive, time-limited mental health service for youth and their families, provided in the home,
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION
 -OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
Mobile Crisis Intervention
 Mobile Crisis Intervention Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications. Additionally, providers
Mobile Crisis Intervention Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications. Additionally, providers
Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness
 Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness Matthew Doherty, Director of National Initiatives August 14, 2014 Roles of USICH Coordinates the Federal response to
Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness Matthew Doherty, Director of National Initiatives August 14, 2014 Roles of USICH Coordinates the Federal response to
Alliance Behavioral Healthcare Level of Care Guidelines for State Funded Adult Mental Health and Substance Abuse Services
 Alliance Behavioral Healthcare of Care Guidelines for State Funded Adult Mental Health and Substance Abuse s Mental Health (Effective 10/1/2012) The levels of care criteria provide a framework for the
Alliance Behavioral Healthcare of Care Guidelines for State Funded Adult Mental Health and Substance Abuse s Mental Health (Effective 10/1/2012) The levels of care criteria provide a framework for the
Clinical Services. clean NYS Driver s License, fingerprinting, criminal record check, and approval from NYS Office of Mental Health.
 Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
FY 2016 PERFORMANCE PLAN
 Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
Clinical Criteria Inpatient Medical Withdrawal Management Substance Use Inpatient Withdrawal Management (Adults and Adolescents)
") 4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo.
 This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
COMPETITIVE BIDDING OF MANAGED CARE FOR MEDICAID BEHAVIORAL HEALTH
 COMPETITIVE BIDDING OF MANAGED CARE FOR MEDICAID BEHAVIORAL HEALTH Will Woodell Vice President North Carolina Public Sector February 24, 2011 1 Authorize DHHS to competitively bid the behavioral health
COMPETITIVE BIDDING OF MANAGED CARE FOR MEDICAID BEHAVIORAL HEALTH Will Woodell Vice President North Carolina Public Sector February 24, 2011 1 Authorize DHHS to competitively bid the behavioral health
BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care
 BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care Acute Inpatient Hospitalization I. DEFINITION OF SERVICE: Acute Inpatient Psychiatric Hospitalization is a 24-hour secure and protected, medically
BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care Acute Inpatient Hospitalization I. DEFINITION OF SERVICE: Acute Inpatient Psychiatric Hospitalization is a 24-hour secure and protected, medically
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria. Effective August 1, 2014
 Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
Outpatient Behavioral Health Basics 1
 7/5/2018 1 Outpatient Behavioral Health Basics July 2018 Webinar 1 Description: This class will review the SoonerCare Outpatient Behavioral Health Program. It will include an overview of commonly asked
7/5/2018 1 Outpatient Behavioral Health Basics July 2018 Webinar 1 Description: This class will review the SoonerCare Outpatient Behavioral Health Program. It will include an overview of commonly asked