The New HIS Measures. Holly Swiger PhD, MPH, RN. CAHSAH Annual Conference & Home Care Expo April 25 27, 2017 Rancho Mirage, CA
|
|
|
- Blaze Anthony
- 6 years ago
- Views:
Transcription




1 The New HIS Measures Holly Swiger PhD, MPH, RN 1
 of the Affordable Care Act of 2010 Pay for reporting Public")
2 Objectives Review the current HIS reporting requirements Understand he two new quality measure details Explain the four new HIS discharge data items 3 HQRP Hospice Quality Reporting Program is mandated by Section 3004(c) of the Affordable Care Act of 2010 Pay for reporting Public reporting 4 2

3 HQRP Since Fiscal Year (FY) 2014, the Secretary shall reduce the Annual Payment Update (APU) by 2% for a hospice that does not comply with the quality data submission 5 HIS Data Submission Requirements 6 3
4 HQRP Reporting Requirements To comply with FY 2019 requirements, hospice providers must: Submit at least 80% of all Hospice Item Set (HIS) records within 30 days of the event (patient s admission or discharge) for admissions & discharges occurring 1/1/17 to 12/31/17 Have an ongoing monthly participation in the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospice Survey by an approved third-party vendor, whom submits data quarterly 7 Reporting Requirements All Medicare hospice providers with active CNN number (provider number) must report Hospices awaiting certification will be expected to have HIS processes in place at the time of their initial survey for deemed status Must report both admission and discharge HIS reports for all admissions 8 4
5 Reporting Requirements Providers are required to begin reporting data on the date noted on their CCN notification letter. However, if the CCN notification letter was dated on or after November 1st, they would not be subject to any financial penalty for failure to comply with HQRP requirements for the relevant reporting year. CMS HIS Q & A October Reporting Requirements HIS data is collected and submitted on all patient admissions, regardless of the patient s: Payer Age Location of receipt of hospice services (home, NF, ALF, GIP) Length of stay Transfers from another hospice 10 5

6 Flowchart for Patient Admission 11 Data Collection HIS data can be collected: By the assessing clinician in conjunction with patient assessment activities By abstraction from the patient s clinical record Data can be collected/abstracted by one or more members of the hospice team: Nurse Social Worker Aide Volunteer 12 6
7 HIS Review A review must be completed to ensure completeness of the entire HIS Individuals who completed any part of the HIS must sign in Z0400 Attesting to accuracy Individuals who review for completeness must sign Z0500 Only attesting to completeness Not attesting to accuracy of other hospice team members responses 13 Data Collection Hospices submit HIS data to CMS through the Quality Improvement and Evaluation System (QIES) Assessment Submission and Processing (ASAP) system. 14 7
8 HIS Data Submission To submit records into the QIES ASAP system, Hospice providers need: CMSNet User ID and password. Juniper software installed. QIES User ID and password. HIS record in the proper electronic file format. 15 HIS Recommended Completion & Submission Deadlines Admission HIS HIS Admission Recommended Completion Deadline = Admission Date + 14 calendar days (Admission day = day 0) Discharge HIS (Due to Death, Discharge or Revocation) HIS Discharge Recommended Completion Deadline = Discharge Date + 7 calendar days (Completion of abstraction of HIS within 7 days of discharge) HIS Admission Record Submission Deadline = Admission Date + 30 calendar days HIS Discharge Record Submission Deadline = Discharge Date + 30 calendar days 16 8
9 Data Submission Timelines HIS Records SUBMITTED does not mean that the HIS Records are ACCEPTED!! All HIS Records must be successfully accepted by the QIES ASAP system within 30 calendar days of the event date 17 HIS Final Validation Reports The FVR is available in the Validation Report folder in the CASPER Reporting application. A link to the CASPER Reporting application is available on the Welcome to the CMS QIES Systems for Providers Web page. 18 9
 Pain Screening Pain Assessment Dyspnea Assessment Dyspnea Treatment Patients Treated with an Opiod who are Given a Bowel Regimen NA Hospice & Palliative Care Composite Process")
10 HIS Submission Threshold Calculation 19 HIS Quality Measures NQF NQF #1641 NQF #1647 NQF #1634 NQF #1637 NQF #1639 NQF #1638 NQF #1617 Measure Name Treatment Preferences Beliefs/Values Addressed (if desired by patient) Pain Screening Pain Assessment Dyspnea Assessment Dyspnea Treatment Patients Treated with an Opiod who are Given a Bowel Regimen NA Hospice & Palliative Care Composite Process Measure Comprehensive Assessment at Admission NA Hospice Visits When Death is Imminent Measure Pair20 10
11 Admission HIS 21 New Items for the Admission HIS Required for Admissions on or after 4/1/ A0550: Zip code 2. A1400: Payor Information 3. J0905: Pain Active Problem 4. Hospice and Palliative Care Quality Composite Measure 22 11

12 Current Issues on Identification of Administrative Information 23 Current Issues on Identification of Administrative Information Use the name as it appears on the Medicare Card 24 12


13 New Item on Identification of Administrative Information 25 Current Issues on Identification of Administrative Information Check all that apply, according to the patient/family! 26 13

14 Current Issues on Identification of Administrative Information 27 Payor Information Response J Self Pay: Should be selected if the patient has any amount of personal funds available to contribute to healthcare expense Response K No Payor Source: Should be selected if the patient does not have any of the payor sources in response to options A-I available, nor do they have any personal funds available to contribute to healthcare expenses. 14
15 Payor Information Response X Unknown: Should be selected if the patient is not confirmed to have any of the above payor sources in response options A-K Response Y Other: Should be selected if the patient has available one or more payor sources that is not listed in response options A-K. NQF #1641 Treatment Preferences Numerator Patient stays from the denominator where the patient/responsible party was asked about preference regarding use of cardiopulmonary resuscitation, or hospitalization, or other life-sustaining treatments no more than 7 days prior to admission or within 5 days of the admission date. Denominator - All patient stays, except those with exclusions. Patients under 18 are excluded
16 Current Issues in Section F: Preferences Scenario 1 Date of Admission 7/1/16 7/1/16 Clinical record for the patient includes a DNR order, signed by patient 6/15/16. Scenario 2 - Date of Admission 7/1/16 7/3/16 Nurse assessment checked box, Patient wants comfort care. 31 Current Issues in Section F: Preferences Scenario 3 Date of Admission 7/1/16 7/1/16 Nurse Assessment Note states, Talked with patient and caregiver about preferences for readmission to hospital. Patient was hesitant and said they weren t sure. Told patient that we could discuss this further on a future visit

17 NQF #1641 Beliefs/Values Addressed Numerator Number of patient stays from the denominator where the patient and/or caregiver was asked about spiritual/existential concerns no more than 7 days prior to admission or within 5 days of the admission date. Denominator - All patient stays, except those with exclusions. Patients under 18 are excluded. 33 Current Issues in Section F: Beliefs/Values Addressed Scenario 1 Date of Admission 8/1/16 SW Assessment Note dated 8/2/16 Patient s spouse in a great deal of spiritual distress and wants to speak with chaplain. Referral made. Scenario 2 - Date of Admission 8/1/16 Nurse Assessment Note dated 8/1/16 Patient identified as Baptist

18 Current Issues in Section I: Active Diagnoses Do not use external sources for your response This is your hospice primary diagnosis Even if your primary diagnosis changes during their stay on hospice, you do not update this 35 NQF #1634 Pain Screening Numerator - Patient stays from the denominator who are screened for the presence or absence of pain and, if present, rating of its severity using a standardized tool within 2 days of admission to hospice. Denominator - All patient stays except for those with exclusions. Patients under 18 are excluded
19 Current Issues in Section J: Health Conditions 37 Types of Standardized Pain Tool Utilized Numeric Examples of standardized numeric scales include but are not limited to, 10- point scale, the Symptom Distress Scale (McCorkle), the Memorial Symptom Assessment Scale (MSAS), and the Edmonton Symptom Assessment System (ESAS). Verbal Descriptor Examples of standardized verbal descriptor scales include, but are not limited to, the Brief Pain Inventory, the McGill pain questionnaire, and the 6- Point Verbal Pain Scale
20 Types of Standardized Pain Tool Utilized Patient Visual - Examples of standardized patient visual scales include, but are not limited to, the Wong- Baker FACES Pain Scale, a visual analog scale, and a distress thermometer. Staff Observation - Examples of standardized staff observation scales include, but are not limited to, the Critical Care Pain Observation Tool (CPOT), the Checklist of Nonverbal Pain Indicators (CNPI), the Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC), and Pain Assessment in Advanced Dementia (PAIN-AD). 39 Current Issues in Section J: Health Conditions 40 20
21 Pain Active Problem (J0905) All patients should be screened for pain. Should be in the initial assessment and be based on patient specific findings. If pain is identified at the time of admission or as an active problem there should be a comprehensive assessment. What Qualifies as an Active Pain Problem? Consider factors beyond pain severity at the time of the encounter: Historical report of pain or reports of recent symptoms Current treatment for pain with scheduled or prn medications It is possible that the clinician may determine pain is an active problem for the patient, even if pain is not present during the clinical encounter. 21

22 E-Kit What Qualifies as an Active Pain Problem? Comfort Kits and pre-printed admission orders alone are insufficient evidence to determine pain is an active problem. Treatment is not considered initiated until there is an order and there is documentation that the patient/caregiver was instructed to begin using the medication. Pro-active education on medications in a comfort kit in anticipation of symptoms alone is insufficient evidence to determine pain is an active problem. Old Version of Pain Screening 44 22

23 New J0900 Pain Screening Revised Sequence NQF #1637 Pain Assessment Numerator - Patient stays from the denominator who received a comprehensive pain assessment within 1 day of the pain screening and the pain assessment included at least 5 of the following characteristics: location, severity, character, duration, frequency, what relieves or worsens that pain, and the effect on function or quality of life. Denominator - Patients stays, except for those with exclusions, where the patient s pain severity at the pain screening was rated mild, moderate, or severe. Patients under 18 are excluded

24 Comprehensive Pain Assessment For inclusion in the new composite measure: 1. If applicable, a comprehensive pain assessment must occur within 1 day of the positive pain screen, and 1. Include at least five of the seven pain characteristics. Comprehensive Pain Assessment for Non-Verbal Patients A caregiver report about any of the above characteristics is acceptable. Clinical notes about assessment of nonverbal indicators of pain for any of the above characteristics are also acceptable
25 Comprehensive Pain Assessment for Non-Verbal Patients Nonverbal indicators of pain include nonverbal sounds such as crying, whining, and groaning; facial expressions, such as grimacing and clenching jaws; and protective body movements or postures such as bracing, guarding, rubbing, or clutching a body part. For example: An assessment that included pain location for a nonverbal patient may include documentation, such as patient grimaced and shouted when clinician touched their right leg or other documentation denoting patient exhibiting nonverbal cues of pain for a specific location on the body. 49 Comprehensive Pain Assessment for Non-Verbal Patients - An assessment that included pain severity for a nonverbal patient may include documentation about intensity of nonverbal expressions of pain (grimaces, winces, and clenched teeth/jaw) or protective body movements (bracing, guarding, rubbing, clutching, or holding of a certain body part/area). It could also include documentation of severity using a nonverbal standardized rating scale. - Character will not be able to be assessed on a patient as it is a descriptor by the patient
26 Comprehensive Pain Assessment for Non-Verbal Patients - An assessment that included pain duration for a nonverbal patient may include documentation about how long a patient exhibits any nonverbal cues of pain, such as patient cradled right arm throughout entire visit. - An assessment that included pain frequency for a nonverbal patient may include documentation about how often a patient exhibits any nonverbal cues of pain, such as most of the time, only at night, intermittently. 51 Comprehensive Pain Assessment for Non-Verbal Patients An assessment that included what relieves/worsens pain for a nonverbal patient may include documentation about actions, activities, or positions that relieve/worsen pain, such as patient exhibits fewer nonverbal signs of pain when sitting up versus lying down. An assessment that included pain s effect on function or quality of life for a nonverbal patient may include documentation about change in patient activity, such as family caregiver reports that patient is no longer able to sit up in bed without moaning
27 Comprehensive Pain Assessment for Non-Verbal Patients For any of the seven characteristics included in the pain assessment, select response options based on whether the clinician made an attempt to gather the information from the patient/caregiver. For example, if, for a nonverbal patient, the clinician asked the family/caregiver about pain location and the family/caregiver responded I m not sure or I don t know, 1, Location should be checked for J0910C because the clinician attempted to gather the information. 53 NQF #1639 Dyspnea Screening Numerator Percentage of patient stays during which the patient was screened for dyspnea during the initial nursing assessment. Denominator - All patient stays except for those with exclusions. Patients under 18 are excluded

28 Current Issues in Section J: Health Conditions Respiratory Status Always have a reason to answer YES! Always assess!!! 55 Current Issues in Section J: Health Conditions Respiratory Status Scenario 1 3/5/17 Clinical Note Patient very drowsy; appears to be comfortable during visit. Scenario 2 3/5/17 Clinical Note Patient reports no discomfort and is breathing shallowly but without signs of distress; no concerns about breathing from patient or family

29 NQF #1638 Dyspnea Treatment Numerator Patient stays from the denominator who received treatment within 1 day of screening positive for dyspnea. Denominator - Patient stays, except those with exclusions, where the patient screened positive for dyspnea at the initial screening encounter. Patients under 18 are excluded. 57 Current Issues in Section J: Health Conditions Dyspnea Treatment 58 29

30 NQF #1617 Bowel Regime for Opioids Numerator Patients from the denominator that are given a bowel regimen or there is documentation as to why this was not needed. Denominator - Patient stays, except for those with an exclusion, where a scheduled opioid that is initiated or continued. Patients under 18 are excluded. 59 Current Issues in Section N: Medications 60 30


31 Current Issues in Section N: Medications 61 Current Issues in Section N: Medications This is only if the patient has a scheduled or prn opioid ordered. Don t forget treatments such as non pharmaceutical measures such as increasing fluids, prune juice, etc

32 Current Issues in Section N: Medications Scenario 3/24/17 Orders Oxycodone 10 mg PO every 4 hours, PRN for pain. 3/24/17 Clinical Note Patient has diarrhea. 63 Composite Process Measure Comprehensive Assessment at Admission Active for Discharges on or after 4/1/2017 Numerator All patient stays from the denominator who meet the numerator criteria for the individual component QMs applicable to the patient. Denominator - All patient stays, except for those with exclusions. Patients under 18 are excluded
33 Hospice and Palliative Care Composite Process Measure This measure will provide consumers and providers with: A single measure regarding the overall quality and completeness of assessment of patient needs at hospice admission. A measure that can be used to meaningfully and easily compare quality across hospice providers. A measure that sets a higher standard of care for hospices. Hospice and Palliative Care Composite Process Measure This Quality Measure reports the percentage of hospice patients who received all seven HIS care processes for which they are eligible at admission to a hospice. The measure is calculated using data from existing HIS-Admission items. No new data collection will be required for this measure. Patient admissions occurring on or after April 1, 2017, will be included in the measure calculation. 33

34 Hospice and Palliative Care Composite Process Measure Hospice and Palliative Care Composite Process Measure Exclusions: Discharge data with no admission data Patients Under 18. Data will still be collected, but will not be calculated in the composite score. A major change to the measure specifications as part of the NQF endorsement was removal of the length of stay (LOS) criterion; all seven measures now have no LOS exclusion. 34
 CMS goal of increasing care in the last week of life and eventually reporting it publically.")
35 Discharge HIS 69 Discharge HIS Active for Discharges on or after 4/1/2017 Section O: Service Utilization (Hospice Visits When Death is imminent) CMS goal of increasing care in the last week of life and eventually reporting it publically
36 Section O: Service Utilization Paired Measure #1 Numerator Number of patients from the denominator receiving at least one visit from registered nurses, physicians, nurse practitioners or physician assistants in the last 3 days of life. Denominator - All patients, except for those with exclusions. Patients are excluded from the denominator if the patient did not expire in hospice care or the patient received any continuous home care, respite care, or general inpatient care in the last 3 days of life. 71 Discharge Quality Measures Applies to patients discharged due to death. Patients who had GIP, CC or Respite during the period of review are excluded. Phone calls are not counted. Post-Mortem visits are not counted. Visits provided to the patient s family may be counted. Patients under 18 are not excluded. 36


37 Visits in the Last 3 Days of Life Assesses the percentage of patients receiving at least one visit from the following disciplines: Registered Nurses Physicians Nurse Practitioners or Physician Assistants Visits in the Last 3 Days of Life 37
38 Section O: Service Utilization Paired Measure #2 Numerator Number of patients from the denominator receiving at least two visits from medical social workers, chaplains or spiritual counselors, licensed practical nurses or hospice aides in the last 7 days of life. Denominator - All patients, except for those with exclusions. Patients are excluded from the denominator if the patient did not expire in hospice care or the patient received any continuous home care, respite care, or general inpatient care in the last 7 days of life, or had a length of stay of one day. 75 Visits in the Last 7 Days of Life Assesses the percentage of patients receiving at least two visits from the following disciplines: Medical Social Workers Chaplains or Spiritual Counselors LVNs Hospice Aides 38

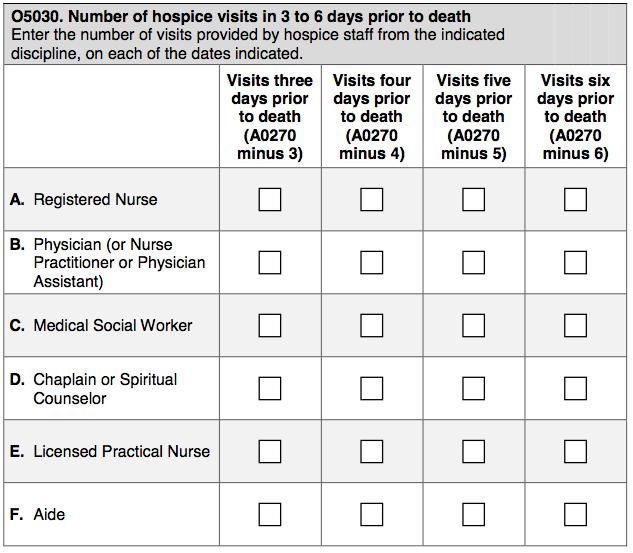
39 Section O: Service Utilization Paired Measure #2 77 Section O: Service Utilization Paired Measure #

40 Section O: Service Utilization Paired Measure #2 Three days prior to death is calculated as A0270 (Discharge Date) minus 3. Four days prior to death is calculated as A0270 minus 4. Five days prior to death is calculated as A0270 minus 5. Six days prior to death is calculated as A0270 minus


41 Section Z: Record Administration 81 Section Z: Record Administration 82 41

42 CASPER Hospice Level Quality Measure Report 83 HIS Collection & Submission Who will be doing the abstraction? Will it be individual staff, QAPI staff, managers? Who will be responsible to review for completeness and sign the Z0500? Who will submit the data? Who will review the Final Validation Report and follow up on Fatal Errors or Rejected Records? 84 42
43 HIS Summary Know & meet the timelines for completion & submission Ensure that staff complete all 7 assessments Reinforce confusing areas and teach new HIS data to be collected Be sure your EMR calculations are correct Report in XML format Track you re HIS data in Casper Follow the CMS Quarterly HIS Q & As 85 References FY 2017 Hospice Final Rule: The Hospice Item Set Manual: Assessment-Instruments/Hospice-Quality-Reporting/Hospice- Item-Set-HIS.html. Hospice Quality Reporting: Assessment-Instruments/Hospice-Quality- Reporting/index.html. 43
44 Resources Hospice User Guides and Training: CMS HQRP Website: PatientAssessment-Instruments/Hospice- QualityReporting/index.html Quality Help Desk: Technical Help Desk or (877) (Monday-Friday 7:00 a.m. - 7:00 p.m. Central Time) 87 Listservs: Resources MLN Connects enews ubscriber/new?pop=t&top ic_id=uscms_7819 ODF listserv HHHDME.html Federal Register: Review proposed and final rules 88 44


45 Thank You! Questions? 89 Session Sponsor Visit Sponsor at Booth # 112! 90 45



46 Speaker Information Holly Swiger PhD, MPH, RN Owner/Lead Consultant Stellar Concepts, Inc Sky High Drive
Overview HOSPICE QUALITY REPORTING PROGRAM (HQRP) 10/10/2016
 10/10/2016") Hospice Quality Reporting Requirements and Using Reports in Your QAPI Program Octobe Overview Identify the current and 2017 CMS Hospice Quality Reporting Requirements. Identify the financial risk of failure
Hospice Quality Reporting Requirements and Using Reports in Your QAPI Program Octobe Overview Identify the current and 2017 CMS Hospice Quality Reporting Requirements. Identify the financial risk of failure
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices. Presenter. Objectives 08/31/16
 Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
October Hospice Quality Reporting and Customer Service: Yes There IS a Connection! Simione Healthcare Consultants, LLC 1
 Midwest Palliative and End of Life Care Conference October 22-24, 2017 Hospice Quality Reporting and Kara Justis, MBA Director Kimberly Skehan, RN, MSN Senior Manager Simione Healthcare Consultants, LLC
Midwest Palliative and End of Life Care Conference October 22-24, 2017 Hospice Quality Reporting and Kara Justis, MBA Director Kimberly Skehan, RN, MSN Senior Manager Simione Healthcare Consultants, LLC
 Hospice Quality Reporting Where Are We Now? Subscriber Webinar Today s Agenda Review progress with HIS and lessons learned Discuss the upcoming CAHPS Hospice Survey Develop a plan to be ready for CAHPS
Hospice Quality Reporting Where Are We Now? Subscriber Webinar Today s Agenda Review progress with HIS and lessons learned Discuss the upcoming CAHPS Hospice Survey Develop a plan to be ready for CAHPS
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
FY 2017 Hospice Proposed Rule. Hospice Regulatory Review May Webinar Agenda. Hospice Regulatory Review
 Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule
![Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule](/thumbs/73/68786685.jpg "Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule") Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
HOSPICE QUALITY REPORTING PROGRAM
 4 HOSPICE QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 HOSPICE PATIENT STAY-LEVEL QUALITY MEASURE REPORT... 5 HOSPICE-LEVEL QUALITY MEASURE REPORT... 9 12/2016 v1.00 Certification And Survey Provider
4 HOSPICE QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 HOSPICE PATIENT STAY-LEVEL QUALITY MEASURE REPORT... 5 HOSPICE-LEVEL QUALITY MEASURE REPORT... 9 12/2016 v1.00 Certification And Survey Provider
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY
 MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
5/3/2017. QAPI Quality and Compliance HOSPICE. Hospice Quality Reporting Program QAPI & HQRP: DIFFERENCES AND SIMILARITIES
 QAPI Quality and Compliance HOSPICE Katie Wehri, CHPC Director of Operations Consulting Healthcare Provider Solutions Kwehri@healthcareprovidersolutions.com QAPI & HQRP: DIFFERENCES AND SIMILARITIES Hospice
QAPI Quality and Compliance HOSPICE Katie Wehri, CHPC Director of Operations Consulting Healthcare Provider Solutions Kwehri@healthcareprovidersolutions.com QAPI & HQRP: DIFFERENCES AND SIMILARITIES Hospice
CY 2016 Hospice Proposed Rule. HEALTHCAREfirst 5/13/2015. Hospice Regulatory Update FY Hospice Regulatory Review May 2015.
 Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice
 QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice CMS Quality Initiatives CMS has encouraged Healthcare to monitor itself and gather data Standard measures of quality care are
QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice CMS Quality Initiatives CMS has encouraged Healthcare to monitor itself and gather data Standard measures of quality care are
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
National Hospice and Palliative Care OrganizatioN. Facts AND Figures. Hospice Care in America. NHPCO Facts & Figures edition
 National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
Release Notes - Version (DRAFT) Release Date: 09/03/2011
 Release Date: 09/03/2011") Release Notes - Version 3.0.8 (DRAFT) Release Date: 09/03/2011 Please Sync all Off-Line Charting Prior to the Release Human Resources Tracking - Enhanced Human Resources Related Links have been added to
Release Notes - Version 3.0.8 (DRAFT) Release Date: 09/03/2011 Please Sync all Off-Line Charting Prior to the Release Human Resources Tracking - Enhanced Human Resources Related Links have been added to
HOSPICE FINAL RULE by SHARON HARDER, President - C3 Advisors, LLC
 FAQ: THE 2018 HOSPICE FINAL RULE 1 FAQ FREQUENTLY ASKED QUESTIONS ABOUT The 2018 HOSPICE FINAL RULE by SHARON HARDER, President - C3 Advisors, LLC and BETH NOYCE, RN, BSJMC, HCS-H, HCS-D, COS-C, Consultant
FAQ: THE 2018 HOSPICE FINAL RULE 1 FAQ FREQUENTLY ASKED QUESTIONS ABOUT The 2018 HOSPICE FINAL RULE by SHARON HARDER, President - C3 Advisors, LLC and BETH NOYCE, RN, BSJMC, HCS-H, HCS-D, COS-C, Consultant
FY 2015 IPF PPS Final Rule: USING THE WEBEX Q+A FEATURE
 FY 2015 IPF PPS Final Rule: USING THE WEBEX Q+A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions
FY 2015 IPF PPS Final Rule: USING THE WEBEX Q+A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions
LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012
 August 21, 2012") LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012 Purpose: What s New? In Brief LTCH Quality Reporting Program New developments Updated CMS LTCH QRP Manual Final FY13 rule:
LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012 Purpose: What s New? In Brief LTCH Quality Reporting Program New developments Updated CMS LTCH QRP Manual Final FY13 rule:
What do we promise people who are dying and those around them when we tell them about hospice care?
 Care Planning The Road to Meeting Patients and Families Where They Are Charlene Ross, MBA, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 602-740-0783 charlene@rchealthcaresolutions.com
Care Planning The Road to Meeting Patients and Families Where They Are Charlene Ross, MBA, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 602-740-0783 charlene@rchealthcaresolutions.com
Reference Guide for Hospice Medicaid Services
 Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Hospice Regulatory & Quality Reporting Update. Summary of FY2019 Hospice Wage Index Final Rule 9/12/2018 TRENDS IN HOSPICE UTILIZATION
 Hospice Regulatory & Quality Reporting Update Jennifer Kennedy, EdD, MA, BSN, RN, CHC National Hospice and Palliative Care Organization October 2018 Summary of FY2019 Hospice Wage Index Final Rule August
Hospice Regulatory & Quality Reporting Update Jennifer Kennedy, EdD, MA, BSN, RN, CHC National Hospice and Palliative Care Organization October 2018 Summary of FY2019 Hospice Wage Index Final Rule August
CAHPS Hospice Survey Podcast for Hospices Transcript Data Hospices Must Provide to their Survey Vendor
 CAHPS Hospice Survey Data Hospices Must Provide to their Survey Vendor Presentation available at: Slide 1 Welcome to the CAHPS Hospice Survey: Podcast for Hospices series. These podcasts were created for
CAHPS Hospice Survey Data Hospices Must Provide to their Survey Vendor Presentation available at: Slide 1 Welcome to the CAHPS Hospice Survey: Podcast for Hospices series. These podcasts were created for
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Hospice Clinical Record Review
 Purpose: Surveyors may use this worksheet when conducting clinical record reviews during a hospice survey. Directions: Fill in appropriate data. Table 1. Patient Information Patient Information Residence
Purpose: Surveyors may use this worksheet when conducting clinical record reviews during a hospice survey. Directions: Fill in appropriate data. Table 1. Patient Information Patient Information Residence
Automating documentation helps hospice agencies withstand greater scrutiny
 White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Form CMS (5/2017) Page 1
 Page 1") Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
 A Summer Potpourri Subscriber Audioconference Today s Topics Medicare Part D CR 8358 Additional Data Elements on Claims Wage Index Proposed Rule otimeframe for Submitting Notice of Election oattending
A Summer Potpourri Subscriber Audioconference Today s Topics Medicare Part D CR 8358 Additional Data Elements on Claims Wage Index Proposed Rule otimeframe for Submitting Notice of Election oattending
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
LTCH Lay of the Land: Reporting the LTCH CARE Data Set. July 30, 2012
 LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
Interim Final Interpretive Guidelines Version 1.1
 Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now!
 Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
IPFQR Program Manual and Paper Tools Review
 and Paper Tools Review Evette Robinson, MPH Project Lead, Inpatient Psychiatric Facility Quality Reporting (IPFQR) Program Value, Incentives, and Quality Reporting (VIQR) Outreach and Education Support
and Paper Tools Review Evette Robinson, MPH Project Lead, Inpatient Psychiatric Facility Quality Reporting (IPFQR) Program Value, Incentives, and Quality Reporting (VIQR) Outreach and Education Support
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications
 Program Description & Measurement Specifications") 2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule
 Calendar Year (CY) 2013 Final Rule") Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
FY2018 Hospice Wage Index Final Rule
 FY2018 Hospice Wage Index Final Rule To: NHPCO Provider Members From: NHPCO Health Policy Team Date: August 2, 2017 Summary at a Glance On August 1, 2017, the Federal Register posted the FY2018 Hospice
FY2018 Hospice Wage Index Final Rule To: NHPCO Provider Members From: NHPCO Health Policy Team Date: August 2, 2017 Summary at a Glance On August 1, 2017, the Federal Register posted the FY2018 Hospice
Sneak Peak: MDS 3.0 Changes & New QRP s. Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma
 Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC
 The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY. July 17, 2012
 PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
2014 HOSPICE REGULATORY UPDATE
 2014 HOSPICE REGULATORY UPDATE Holly Swiger, PhD, MPH, PHN, RN Stellar Concepts, Inc. WHISTLEBLOWERS MARCH 13, 2014 Hospice company to pay $3.92 million to settle false claims allegations; two whistleblowers
2014 HOSPICE REGULATORY UPDATE Holly Swiger, PhD, MPH, PHN, RN Stellar Concepts, Inc. WHISTLEBLOWERS MARCH 13, 2014 Hospice company to pay $3.92 million to settle false claims allegations; two whistleblowers
CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Medicare Part A provides a special program for persons needing hospice care.
 MEDICARE HOSPICE BENEFIT Medicare Part A provides a special program for persons needing hospice care. These services are delivered to hospice patients wherever the patient resides by a Medicarecertified
MEDICARE HOSPICE BENEFIT Medicare Part A provides a special program for persons needing hospice care. These services are delivered to hospice patients wherever the patient resides by a Medicarecertified
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Connecting the Dots for a Successful Quality Assessment/Performance Improvement (QAPI) Program
 Program") Connecting the Dots for a Successful Quality Assessment/Performance Improvement (QAPI) Program Kimberly Skehan, RN, MSN Senior Manager Simione Healthcare Consultants, LLC Jennifer Hale, RN, MSN, CHPN,
Connecting the Dots for a Successful Quality Assessment/Performance Improvement (QAPI) Program Kimberly Skehan, RN, MSN Senior Manager Simione Healthcare Consultants, LLC Jennifer Hale, RN, MSN, CHPN,
Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one
 Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one in a series of videos explaining the 13 quality measures
Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one in a series of videos explaining the 13 quality measures
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Overview of the Hospice Proposed Rule
 HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report
 Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
February Hospice Fundamentals All Rights Reserved 2. The Applicable Regulations. 42 CFR 418 Subparts
 The Role of the Subscriber Webinar 1 Today s Session The Medicare Regulations Patient Care Payment Understanding and Differentiating the Roles The Medical Director s The Functions Administrative Payment
The Role of the Subscriber Webinar 1 Today s Session The Medicare Regulations Patient Care Payment Understanding and Differentiating the Roles The Medical Director s The Functions Administrative Payment
Hospice Continuous Home Care LEGACY HOSPICE
 Hospice Continuous Home Care LEGACY HOSPICE The Basics CONTINUOUS HOME CARE OF THE HOSPICE PATIENT What is Continuous Home Care? A day on which an individual who has elected to receive hospice care is
Hospice Continuous Home Care LEGACY HOSPICE The Basics CONTINUOUS HOME CARE OF THE HOSPICE PATIENT What is Continuous Home Care? A day on which an individual who has elected to receive hospice care is
Contents [1] This document has been edited for spelling and punctuation errors.
![Contents [1] This document has been edited for spelling and punctuation errors.](/thumbs/72/67584533.jpg "Contents [1] This document has been edited for spelling and punctuation errors.") Centers for Medicare & Medicaid Services SNF Quality Reporting Program Call MLN Connects National Provider Call Moderator: Leah Nguyen July 12, 2016 1:30 pm ET Contents Announcements and Introduction...
Centers for Medicare & Medicaid Services SNF Quality Reporting Program Call MLN Connects National Provider Call Moderator: Leah Nguyen July 12, 2016 1:30 pm ET Contents Announcements and Introduction...
Conceptualization Panel rating: 2 Purpose. Completed 04/04 1
 Tool: Nursing Assistant-Administered Instrument to Assess Pain in Demented Individuals (NOPPAIN) Tool developer: Snow, A.L., Weber, J.B., O Malley, Cody, M., Beck, C., Bruera, E., Ashton, C., Kunik, M.E.
Tool: Nursing Assistant-Administered Instrument to Assess Pain in Demented Individuals (NOPPAIN) Tool developer: Snow, A.L., Weber, J.B., O Malley, Cody, M., Beck, C., Bruera, E., Ashton, C., Kunik, M.E.
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Inpatient Psychiatric Facilities Quality Reporting Program
 FY 2015 IPF PPS Final Rule Questions and Answers Moderator: Deb Price, PhD, MEd, MSPH Educational Coordinator, Inpatient Psychiatric Facilities Quality Reporting (IPFQR) (SC) Speaker: Renee Parks, BSN,
FY 2015 IPF PPS Final Rule Questions and Answers Moderator: Deb Price, PhD, MEd, MSPH Educational Coordinator, Inpatient Psychiatric Facilities Quality Reporting (IPFQR) (SC) Speaker: Renee Parks, BSN,
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016
 Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
SNF QUALITY REPORTING PROGRAM
 13 SNF QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 SNF REVIEW AND CORRECT REPORT... 5 05/2017 v1.00 Certification And Survey Provider Enhanced Reports SNF QRP 13-1 NOTE: Unless otherwise noted,
13 SNF QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 SNF REVIEW AND CORRECT REPORT... 5 05/2017 v1.00 Certification And Survey Provider Enhanced Reports SNF QRP 13-1 NOTE: Unless otherwise noted,
OASIS ITEM ITEM INTENT TIME POINTS ITEM(S) COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES
 COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES") (M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
PO Box 350 Willimantic, Connecticut (860) Connecticut Ave, NW Suite 709 Washington, DC (202)
 Connecticut Ave, NW Suite 709 Washington, DC (202)") PO Box 350 Willimantic, Connecticut 06226 (860)456-7790 1025 Connecticut Ave, NW Suite 709 Washington, DC 20036 (202)293-5760 Se habla español Produced under a grant from the Connecticut State Department
PO Box 350 Willimantic, Connecticut 06226 (860)456-7790 1025 Connecticut Ave, NW Suite 709 Washington, DC 20036 (202)293-5760 Se habla español Produced under a grant from the Connecticut State Department
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Barbara Resnick, PHD,CRNP University of Maryland School of Nursing
 Pain Careplans and Monitoring: Role of the Interprofessional Team Barbara Resnick, PHD,CRNP University of Maryland School of Nursing Disclosures I have no relevant disclosures LTC: Review Current Careplanning
Pain Careplans and Monitoring: Role of the Interprofessional Team Barbara Resnick, PHD,CRNP University of Maryland School of Nursing Disclosures I have no relevant disclosures LTC: Review Current Careplanning
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Introducing the Discharge to Community Quality Measure
 Introducing the Discharge to Community Quality Measure Rachel Delavan, Director of Research Dawn Murr-Davidson, RN BSN, Director of Quality Initiatives October 20, 2015 1 Objectives Define the discharge
Introducing the Discharge to Community Quality Measure Rachel Delavan, Director of Research Dawn Murr-Davidson, RN BSN, Director of Quality Initiatives October 20, 2015 1 Objectives Define the discharge
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals
 An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals Jon Langmead 10/31/2011 Centers for Medicare & Medicaid Services 1 Eligible
An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals Jon Langmead 10/31/2011 Centers for Medicare & Medicaid Services 1 Eligible
HOMECARE AND HOSPICE REIMBURSEMENT
 Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
Hospital Inpatient Quality Reporting (IQR) Program
 Program") FY 2018 Inpatient Prospective Payment System (IPPS) Proposed Rule Acute Care Hospital Quality Reporting Programs Overview Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient
FY 2018 Inpatient Prospective Payment System (IPPS) Proposed Rule Acute Care Hospital Quality Reporting Programs Overview Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Quality Improvement: Utilization Measures
 Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
FY2018 Proposed Rule: Payment and Quality Reporting
 FY2018 Proposed Rule: Payment and Quality Reporting Mary Dalrymple Managing Director, LTRAX Objectives Describe effects of reimbursement updates Look at new short stay payment system Touch on miscellaneous
FY2018 Proposed Rule: Payment and Quality Reporting Mary Dalrymple Managing Director, LTRAX Objectives Describe effects of reimbursement updates Look at new short stay payment system Touch on miscellaneous
Ambulatory Surgical Center Quality Reporting Program
 ASCQR 2016 Specifications Manual Update Questions & Answers Moderator: Mary Ellen Wiegand, RN, LHRM, CASC, CNOR Speakers: Mathematica Policy Research Telligen Yale Center for Outcomes Research and Evaluation
ASCQR 2016 Specifications Manual Update Questions & Answers Moderator: Mary Ellen Wiegand, RN, LHRM, CASC, CNOR Speakers: Mathematica Policy Research Telligen Yale Center for Outcomes Research and Evaluation
How to Account for Hospice Reimbursement Changes. Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016
 How to Account for Hospice Changes Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016 marcumllp.com Disclaimer This Presentation has been prepared for informational purposes
How to Account for Hospice Changes Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016 marcumllp.com Disclaimer This Presentation has been prepared for informational purposes
Medicare Hospice General Inpatient Level of Care
 Medicare General Inpatient Level of Care 2016 1811_0616 Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant 2 Disclaimer National Government Services, Inc. has
Medicare General Inpatient Level of Care 2016 1811_0616 Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant 2 Disclaimer National Government Services, Inc. has
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
QIES Help Desk. Objectives. Nursing Home Quality Initiatives and Five-Star Quality Rating System
 Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Home Care Accreditation
 Home Care Accreditation Q&A Guide Concise answers to frequently asked questions about how to begin the accreditation process, whom to call with questions and much more! Home Health Hospice Personal Care
Home Care Accreditation Q&A Guide Concise answers to frequently asked questions about how to begin the accreditation process, whom to call with questions and much more! Home Health Hospice Personal Care
Connecticut interchange MMIS
 Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
Hospital Inpatient Quality Reporting (IQR) Program
 Program") FY 2018 IPPS Proposed Rule Overview of the Hospital IQR Program and Medicare and Medicaid EHR Incentive Programs Proposals Specific to ecqms and MU Requirements Questions & Answers Moderator Artrina Sturges,
FY 2018 IPPS Proposed Rule Overview of the Hospital IQR Program and Medicare and Medicaid EHR Incentive Programs Proposals Specific to ecqms and MU Requirements Questions & Answers Moderator Artrina Sturges,
Climb Every Mountain: Improve Every OASIS Outcome
 KHCA Annual Meeting C3 Climb Every Mountain: Improve Every OASIS Outcome Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus September 21, 2017 Climb Every Mountain: Improve
KHCA Annual Meeting C3 Climb Every Mountain: Improve Every OASIS Outcome Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus September 21, 2017 Climb Every Mountain: Improve
Electronic Staffing Data Submission Payroll-Based Journal
 Centers for Medicare & Medicaid Services Electronic Staffing Data Submission Payroll-Based Journal Long-Term Care Facility Policy Manual Version 1.0 April 2015 TABLE OF CONTENTS Chapter 1: Overview 1.1
Centers for Medicare & Medicaid Services Electronic Staffing Data Submission Payroll-Based Journal Long-Term Care Facility Policy Manual Version 1.0 April 2015 TABLE OF CONTENTS Chapter 1: Overview 1.1
Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar
 Report Webinar") Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar Division of Aging Services (DoAS) and Division of Medical Assistance and Health Services (DMAHS) 1 Agenda
Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar Division of Aging Services (DoAS) and Division of Medical Assistance and Health Services (DMAHS) 1 Agenda