1 st Annual Neurosciences Critical Care Symposium June 5, 2010 Karen Ellmers, RN, MS, CCNS
|
|
|
- Lynn Page
- 6 years ago
- Views:
Transcription




1 What does it mean to be a Primary Stroke Center? 1 st Annual Neurosciences Critical Care Symposium June 5, 2010 Karen Ellmers, RN, MS, CCNS ellmersk@ohsu.edu 1
2 What are the goals of a Primary Stroke Center? Increased use of appropriate p diagnostic and therapeutic acute stroke treatments. Reduced peristroke complications. Improved patient outcomes. Same level of care 24/7/365. Joint Commission Certification Joint Commission Primary Stroke Center Certification requirements are in alignment with the Brain Attack Coalition (BAC) recommendations. To become certified you must demonstrate all 11 major elements of performance recommended by the BAC. 2


3 Major Elements of Performance Hospital and Administrative Support. Acute Stroke Team Made up of at a minimum, a physician and nurse trained in the diagnosis and treatment of the acute stroke patient and available 24/7. A way of activating the team and having them respond to patient s bedside within 15 minutes. A patient log must be kept. Major Elements of Performance Written Care Protocols: 3

4 4


5 Major Elements of Performance Emergency Medical Systems EMS/ED are integrated in care and transport of stroke patients. Emergency Department ED staff demonstrate familiarity with protocols and demonstrate use. Major Elements of Performance Stroke Units Does not require specific enclosed unit, but must be a unit where majority of patients are admitted. (ED, ICU, Acute Care). 5
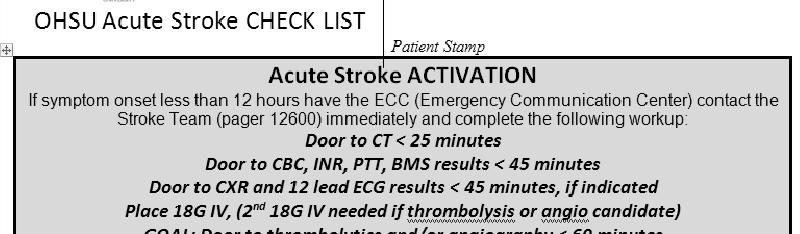
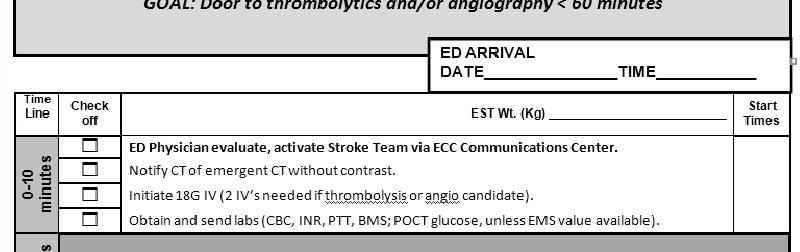
6 Major Elements of Performance Neurosurgical Services available within 2 hours, by transfer, if necessary. Neuroimaging 24/7 i basis Able to obtain brain image within 25 minutes and interpretation within 20 minutes of completion. Major Elements of Performance Laboratory Services Stroke lb labs within 45 minutes from order on 24/7 basis. ECG and chest x ray within 45 minutes from order, when clinically indicated. Outcome and quality improvement activities. Educational programs. 6
7 Comprehensive Stroke Center Health care personnel with specific expertise in a number of disciplines, including neurosurgery and vascular neurology. Advanced neuroimaging capabilities, such as MRI and various types of cerebral angiography. Surgical and endovascular techniques, including clipping and coiling of intracranial aneuryms, carotid endarectomy and stenting, and intra arterial thrombolytic therapy. Infrastructure and programmatic elements such as an intensive care unit and stroke registry. The Power of Data Over 1600 patients in our database allows for analysis of trends and identification of performance improvement projects. Data can be extracted and shared with direct care providers. A way to show them how their efforts impact care in a positive manner. Motivation to improve in areas needing attention. The Neurosciences Best Practices group selects & monitors the annual performance improvement (PI) projects. PI efforts are coordinated by the CNS, but all members of the team are involved in developing & implementing systems solutions. 7
8 Stroke Measures DVT prophylaxis 100% 100% 99% 100% Discharged on antithrombotics 98% 99% 100% 99% Anticoagulation for Afib 57% 100% 100% 100% % who arrive in ED within 120 min. of onset who receive tpa Antithrombotics started within 48 hours of admit LDL>100 discharged on cholesterol reducing agent 44% 86% 100% 100% 94% 96% 99% 99% 7% 90% 99% 99% Bedside swallow screen prior to any PO 80% 69% 74% 81% Patient/family stroke education provided 94% 95% Tobacco cessation provided during hospital stay 19% 96% 98% 99% Assessed for rehab needs 99% 99% 100 % Compliance with documented bedside swallow screen prior to oral intake th Qtr 08 1st Qtr 09 2nd Qtr 09 3rd Qtr 09 4th Qtr 09 1st Qtr 10 8
9 Critical Success Factors Examples of hardwiring changes include: Preprinted order sets. Readily available evidence based guidelines & quick reference lists. Consistent message from staff physicians to residents about expectations. Finding ways to make electronic medical record work in your favor, incorporating ideas from direct care nurses and physicians. Involving the Rapid Response Team to provide immediate and consistent nursing evaluation and expertise paired with rapid initiation of the Stroke Team response, when indicated. Critical Success Factors Interdisciplinary team collaboration essential to success. Early involvement of the leadership of key stakeholders. Go to all the members of the direct care team (nurses, physicians, speech therapists, etc.) for ideas, they know the barriers as well as the solutions. One on one coaching of nurses and physicians. 9
10 Critical Success Factors The Service Line structure, which includes EMS through to discharge placement, enhances the ability to analyze and optimize i how patients t move through the system. It allows for more team thinking of how we all work together to provide an efficient & optimal patient experience, rather than just thinking in silos about what occurs in and would work best for my own department. Regular communication among stakeholders through an organized committee/advisory ygroup structure helps to reinforce the team concept, p, helps to identify common goals, sets clear priorities, and builds positive working relationships. Oregon Stroke Center (OSC) at OHSU The OSC offers regional access to acute stroke treatment 24/7. The team physically evaluates patients at 4 Portland area hospitals. In addition, the OSC stroke physicians provide phone consultation on stroke management and patient transfer for physicians who call from Oregon, Washington, and Idaho. Calls go through the OHSU Transfer Center and are sent to a single Stroke Code pager activating the Stroke Team. 10


11 Oregon Stroke Center (OSC) at OHSU The physician responds to the initial page within 5 minutes. After discussion with the caller, the stroke physician determines whether the patient is a potential candidate for acute stroke treatment and activates the appropriate code through the Stroke Team pager. The Stroke Team physician and coordinator travel to the site where the patient is located. Depending on the case, the neurointerventionalist team on call may be alerted at this time. Simultaneously, the patient may be undergoing further diagnostic workup per the advice of the stroke physician. Oregon Stroke Center (OSC) at OHSU The stroke physician i and clinical i l coordinator reach the patient t site as soon as possible, but within 30 minutes (for the 4 area hospitals). They work together and guide the existing staff through appropriate care for the patients. For patients outside these facilities, the stroke physician may arrange for transfer of the patient to a facility that has the resources necessary for tertiary acute stroke care. 11


12 Critical Success Factors This level of consistent response 24/7 is possible through the assembling of a large team of players willing to take call: 6 area stroke neurologists, and 6 coordinators. OHSU also has 5 cerebral fellowship trained neurointerventionalists. OSC members meet regularly to share protocols and review cases. Local EMS systems collaborate and share the same stroke response protocols. This process takes the team concept out beyond the confines of an individual facility and expands it to the continuum from EMS to the ED to the ICU, across an entire region. And reduces the variation of what is provided for acute stroke management. Future Directions: Telemedicine/Telestroke What is telestroke? Use of telecommunications technologies to provide medical information and services. Interactive full motion audio and video for acute stroke care was first used in the early 1990 s. 12



13 Future Directions: Telemedicine/Telestroke Technology continues to be refined and now includes dedicated, high quality, interactive, ti bi directional audiovisual i systems combined with teleradiology for rapid viewing of brain images, and software that prompts you through the various aspects of an acute stroke workup. Future Directions: Telemedicine/Telestroke Th lti id i t t ith th ti t d/ th i The consulting provider can interact with the patient and/or their family and view aspects of the physical exam. 13

14 Future Directions: Telemedicine/Telestroke Why move in this direction? Outside the urban areas in Oregon there is limited access to neurologists. Regional partnerships can ensure more consistent availability of acute stroke treatment across communities and improve access to consults with stroke neurologists. More patients can stay in their home community, and patients that need to be transferred can do so. Future Directions: Telemedicine/Telestroke Regional stroke networks can be made of comprehensive stroke centers linked in with primary stroke centers, and stroke ready hospitals. This model has been shown to increase the numbers of patients receiving acute stroke treatments, in quicker timeframes, and with improved outcomes. 14
15 Stroke Advisory Group Nurse Educators: Erin Reback Ellie Roberts/Jackson Wild Mercedes Wilson ED Leadership: Drs. Daya, Sahni, and Schmidt Denise Foster Radiology James Anderson, MD, and Erwin Schwarz Laboratory MD Leader, Juanita Peterson Interventional Suite Stanley Barnwell, MD William Greenebaum Neurosurgery Aclan Dogan Neurology Wayne Clark, MD Helmi Lutsep, MD Inpatient Nurse Managers: Judy Van Dyke Randy Ward Hospital Therapy Services Connie Amos Michael Rennick Quality Improvement Christine Slusarenko Margie Harvey Pat Ivie Pharmacy Mike Brownlee Care Management Shannon Coady Karen Prescott/Claire Llewellyn Stroke Program Coordinator Karen Ellmers Administration Mark Lovgren Judi Workman Chuck Kilo Bibliography Alberts, M.J., et al. (2000). Recommendations for the Establishment of Primary Stroke Centers. JAMA, 283(23), pp Alberts, M.J., et al. (2005). Recommendations for Comprehensive Stroke Centers: A Consensus Statement from the Brain Attack Coalition. Stroke, 36(7), pp Ellmers, K.E., Lutsep, H.L., & Clark, W.M. (2009). Stroke Team Creation and Primary Stroke Center Certification. emedicine Clinical Knowledge Base, overview. A peer reviewed online journal. Accessed March 26, Pervez, M.A., et al. (2010). Remote Supervision of IV t PA fro Acute Ischemic Stroke by Telemedicine or Telephone Before Transfer to a Regional Stroke Center is Feasible and Safe. Stroke, 41(1), pp. e Schwamm, L.H., et al. (2009). A Review of the Evidence for the Use of Telemedicine Within Stroke Systems of Care: A Scientific Statement from the American Heart Association/American Stroke Association. Stroke, 40(7), pp Schwamm, L.H., et al. (2009). Recommendations for the Implementation of Telemedicine Within Stroke Systems of Care: A Policy Statement from the American Heart Association. Stroke, 40(7), pp
Element(s) of Performance for DSPR.1
 of Performance for DSPR.1") Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
PSC Certification: What really happens
 PSC Certification: What really happens Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN, SCRN Christy Franklin, MS, RN, CNRN Julie Fussner, BSN, RN, CPHQ, SCRN Disclosures Wendy J. Smith- I have no actual
PSC Certification: What really happens Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN, SCRN Christy Franklin, MS, RN, CNRN Julie Fussner, BSN, RN, CPHQ, SCRN Disclosures Wendy J. Smith- I have no actual
HFAP Stroke Survey. Overview of the Survey Process 8/17/2011
 HFAP Stroke Survey Surveyors Viewpoint Bernard C. McDonnell, D.O. Stroke Center Accreditation from the Surveyors Viewpoint 01.00.01 Primary stroke Center Facility Commitment. The leadership of the facility
HFAP Stroke Survey Surveyors Viewpoint Bernard C. McDonnell, D.O. Stroke Center Accreditation from the Surveyors Viewpoint 01.00.01 Primary stroke Center Facility Commitment. The leadership of the facility
East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R)
") East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R) RAC-R proudly supports and serves Jasper, Newton, Hardin, Orange, Liberty, Jefferson, Chambers, Galveston and
East Texas Gulf Coast Regional Trauma Advisory Council Regional Advisory Council - R (RAC-R) RAC-R proudly supports and serves Jasper, Newton, Hardin, Orange, Liberty, Jefferson, Chambers, Galveston and
Proposed Requirements for Comprehensive Stroke Center
 Proposed Requirements for Comprehensive Stroke Center Please Note: The current requirements for Disease-Specific Care Advanced Certification Program for Primary Stroke are included in this document. Proposed
Proposed Requirements for Comprehensive Stroke Center Please Note: The current requirements for Disease-Specific Care Advanced Certification Program for Primary Stroke are included in this document. Proposed
Acute Stroke Ready Hospital Certification Program
 Ready-or-Not? Acute Stroke Ready Here We Come! Acute Stroke Ready Hospital Certification Program Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer-The Joint Commission April 28, 2017 Presenter
Ready-or-Not? Acute Stroke Ready Here We Come! Acute Stroke Ready Hospital Certification Program Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer-The Joint Commission April 28, 2017 Presenter
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix
 Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix David Eickemeyer, MBA Associate Director, Certification April 20, 2017 Today s Agenda Three Levels of Stroke Certification
Update: Joint Commission Stroke Certification Standards and SAFER Scoring Matrix David Eickemeyer, MBA Associate Director, Certification April 20, 2017 Today s Agenda Three Levels of Stroke Certification
Using Telemedicine to Enhance Meaningful Use Qualification
 Beth DeStasio Director, Regulatory Affairs & Strategy, REACH Health September 2014 Copyright 2014 REACH Health, Inc. All rights Reserved Key Takeaways 1. As of September 4, 2014, the Center for Medicare
Beth DeStasio Director, Regulatory Affairs & Strategy, REACH Health September 2014 Copyright 2014 REACH Health, Inc. All rights Reserved Key Takeaways 1. As of September 4, 2014, the Center for Medicare
Stroke System-of- Care Plan. Mississippi State Department of Health
 Stroke System-of- Care Plan Mississippi State Department of Health Bureau of Acute Care Systems MSDH Board of Health Approved: October 14, 2015 Revised July 6, 2015 Stroke System-of-Care Plan Table of
Stroke System-of- Care Plan Mississippi State Department of Health Bureau of Acute Care Systems MSDH Board of Health Approved: October 14, 2015 Revised July 6, 2015 Stroke System-of-Care Plan Table of
NYS Department of Health Coverdell Stroke Quality Improvement and Registry Program
 NYS Department of Health Coverdell Stroke Quality Improvement and Registry Program An Overview with Considerations in Care Transitions for the Acute Stroke Patient Anna Colello, Esq. Director for Regulatory
NYS Department of Health Coverdell Stroke Quality Improvement and Registry Program An Overview with Considerations in Care Transitions for the Acute Stroke Patient Anna Colello, Esq. Director for Regulatory
DNV GL - Healthcare Advisory Notice Notice No:
 DNV GL - Healthcare Advisory Notice Notice No: 2015-06 DATE: September 3, 2015 SUBJECT: New Version Comprehensive Stroke Center Standards 2.0 DISTRIBUTION: All DNV GL - Healthcare Customers, Employees
DNV GL - Healthcare Advisory Notice Notice No: 2015-06 DATE: September 3, 2015 SUBJECT: New Version Comprehensive Stroke Center Standards 2.0 DISTRIBUTION: All DNV GL - Healthcare Customers, Employees
Stroke Distinction Report. Lakeridge Health Oshawa. Oshawa, ON. On-site Survey Dates: October 26, October 29, 2015
 Stroke Distinction Report Lakeridge Health Oshawa Oshawa, ON On-site Survey Dates: October 26, 2015 - October 29, 2015 Report Issued: November 12, 2015 About the Distinction Report Lakeridge Health Oshawa
Stroke Distinction Report Lakeridge Health Oshawa Oshawa, ON On-site Survey Dates: October 26, 2015 - October 29, 2015 Report Issued: November 12, 2015 About the Distinction Report Lakeridge Health Oshawa
SARASOTA MEMORIAL HOSPITAL POLICY
 smh0076850ps1070 SARASOTA MEMORIAL HOSPITAL POLICY TITLE EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner: Director, Patient Care 12/09/13 08/19/16 Clinical Non-Clinical
smh0076850ps1070 SARASOTA MEMORIAL HOSPITAL POLICY TITLE EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of Responsible Owner: Director, Patient Care 12/09/13 08/19/16 Clinical Non-Clinical
 SUNY DOWNSTATE MEDICAL CENTER UNIVERSITY HOSPITAL OF BROOKLYN POLICY AND PROCEDURE Subject: ADMISSION/TRANSFER OF STROKE PATIENTS Page 1 of 2 No: STK-1 Prepared by: Stroke Management Committee Original
SUNY DOWNSTATE MEDICAL CENTER UNIVERSITY HOSPITAL OF BROOKLYN POLICY AND PROCEDURE Subject: ADMISSION/TRANSFER OF STROKE PATIENTS Page 1 of 2 No: STK-1 Prepared by: Stroke Management Committee Original
Neurocritical Care. Does it make a difference?
 Neurocritical Care Does it make a difference? Dr Hilary Madder Neurosciences Intensive Care Unit John Radcliffe Hospital, Oxford ANZCA Neuroanaesthesia SIG July 2013 Neurocritical Care Capacity 32 neurosurgical
Neurocritical Care Does it make a difference? Dr Hilary Madder Neurosciences Intensive Care Unit John Radcliffe Hospital, Oxford ANZCA Neuroanaesthesia SIG July 2013 Neurocritical Care Capacity 32 neurosurgical
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program
 INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
Evaluation of Telestroke Services
 Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
GET WITH THE GUIDELINES-STROKE UPDATE. Abby Fairbank, MPH Senior Director, Quality & Systems Improvement American Heart Association
 GET WITH THE GUIDELINES-STROKE UPDATE Abby Fairbank, MPH Senior Director, Quality & Systems Improvement American Heart Association 1 OVERVIEW STROKE SYSTEM OF CARE PLAN HIGHLIGHT GWTG-STROKE MEASURES HIGHLIGHT
GET WITH THE GUIDELINES-STROKE UPDATE Abby Fairbank, MPH Senior Director, Quality & Systems Improvement American Heart Association 1 OVERVIEW STROKE SYSTEM OF CARE PLAN HIGHLIGHT GWTG-STROKE MEASURES HIGHLIGHT
Program goals and competencies for each year of training;
 Program goals and competencies for each year of training; NS-1 Perform a neurological exam Triage of neurosurgical emergencies Neurosurgical critical care management Interpret laboratory studies Identify
Program goals and competencies for each year of training; NS-1 Perform a neurological exam Triage of neurosurgical emergencies Neurosurgical critical care management Interpret laboratory studies Identify
Neurocritical Care Rotation - EUH
 Preceptor: Bill Asbury, B.S., Pharm.D. Office: EUH- EG35 Hours: ~ 8:00am-4:30pm Desk: 404-712-7491 Pager: 404-686-5500 pic 14028 ICU cell phone: 404-326-8256 PGY-2 Residency Training Program Neurocritical
Preceptor: Bill Asbury, B.S., Pharm.D. Office: EUH- EG35 Hours: ~ 8:00am-4:30pm Desk: 404-712-7491 Pager: 404-686-5500 pic 14028 ICU cell phone: 404-326-8256 PGY-2 Residency Training Program Neurocritical
The Need for Support of Stroke-Ready Certification in Rural United States: An Overview
 WHITE PAPER The Need for Support of Stroke-Ready Certification in Rural United States: An Overview Stacey Lang (RN, BSN), Therese Poland (RN, BSN, MSN), & Laura Owens (RN, MSN, MA, MBA, CCRN, CRRN). tpoland@hfap.org
WHITE PAPER The Need for Support of Stroke-Ready Certification in Rural United States: An Overview Stacey Lang (RN, BSN), Therese Poland (RN, BSN, MSN), & Laura Owens (RN, MSN, MA, MBA, CCRN, CRRN). tpoland@hfap.org
Core Elements of Delivery of Stroke Prevention Services
 Core Elements of Delivery of A critical component of secondary stroke prevention is access to specialized stroke prevention services (SPS), ideally provided by dedicated stroke prevention clinics. Stroke
Core Elements of Delivery of A critical component of secondary stroke prevention is access to specialized stroke prevention services (SPS), ideally provided by dedicated stroke prevention clinics. Stroke
Duke Life Flight. Systems of Care for Time Dependent Emergencies. Disclosures. Disclosures 9/19/2017
 Duke Life Flight Systems of Care for Time Dependent Emergencies Claire M Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center Wilmington, NC Disclosures Clinical
Duke Life Flight Systems of Care for Time Dependent Emergencies Claire M Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center Wilmington, NC Disclosures Clinical
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
AMGA 2013 ANNUAL CONFERENCE
 AMGA 2013 ANNUAL CONFERENCE Mercy Medical Group, Inc. Interdependent Multi-specialty group in Sacramento, CA. Hospital Aligned since 1993 (group practice began 1940 s) > 320 Physicians/APC s 6 Departments
AMGA 2013 ANNUAL CONFERENCE Mercy Medical Group, Inc. Interdependent Multi-specialty group in Sacramento, CA. Hospital Aligned since 1993 (group practice began 1940 s) > 320 Physicians/APC s 6 Departments
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Georgia Regents University: Evolution of One of the Country s Longest-Running Telestroke Programs
 Telemedicine Case Study Georgia Regents University: Evolution of One of the Country s Longest-Running Telestroke Programs Successes and Future Plans Each year, close to 800,000 people in the U.S. suffer
Telemedicine Case Study Georgia Regents University: Evolution of One of the Country s Longest-Running Telestroke Programs Successes and Future Plans Each year, close to 800,000 people in the U.S. suffer
I: Neurological/ Neurosurgical
 I: Neurological/ Neurosurgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 81 Competency: I-1 Neurological Nursing I-1-1 I-1-2 I-1-3 I-1-4 Demonstrate knowledge
I: Neurological/ Neurosurgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 81 Competency: I-1 Neurological Nursing I-1-1 I-1-2 I-1-3 I-1-4 Demonstrate knowledge
Kenny Barajas DNP, RN, CEN
 Advanced Disease-Specific Care Certification Requirements for Comprehensive Stroke Center Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer The Joint Commission Presenter Disclosure Statement ASRH,
Advanced Disease-Specific Care Certification Requirements for Comprehensive Stroke Center Kenny Barajas DNP, RN, CEN Disease Specific Care Reviewer The Joint Commission Presenter Disclosure Statement ASRH,
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Educational Goals & Objectives
 Educational Goals & Objectives The Neurology rotation will provide residents with an opportunity to evaluate and treat patients with neurological disorders. The goal is for residents to feel comfortable
Educational Goals & Objectives The Neurology rotation will provide residents with an opportunity to evaluate and treat patients with neurological disorders. The goal is for residents to feel comfortable
Neuro Labs and Best Practices in Stroke Programs. Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing
 Neuro Labs and Best Practices in Stroke Programs Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing Objectives Discuss the evolving best practices for neuro lab practice
Neuro Labs and Best Practices in Stroke Programs Sarah L. Livesay, DNP, RN, ACNP-BC Associate Professor Rush University College of Nursing Objectives Discuss the evolving best practices for neuro lab practice
Stroke Coordinator Boot Camp
 Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Arkansas Stroke Registry (ASR) Update Dave Vrudny, Arkansas Stroke Registry Program Manager. May 16, 2012
 Update Dave Vrudny, Arkansas Stroke Registry Program Manager. May 16, 2012") Arkansas Stroke Registry (ASR) Update Dave Vrudny, Arkansas Stroke Registry Program Manager May 16, 2012 TV News Story October 2011 Click for Video 2 Meeting Objectives Progress Since April 2011 Sample
Arkansas Stroke Registry (ASR) Update Dave Vrudny, Arkansas Stroke Registry Program Manager May 16, 2012 TV News Story October 2011 Click for Video 2 Meeting Objectives Progress Since April 2011 Sample
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Support (Level III) Stroke Facility Criteria Guidance
 Stroke Facility Criteria Guidance") Support (Level III) Stroke Facilities ( SSFs ) - provides resuscitation, stabilization and assessment of the stroke victim and either provides the treatment or arranges for immediate transfer to a higher
Support (Level III) Stroke Facilities ( SSFs ) - provides resuscitation, stabilization and assessment of the stroke victim and either provides the treatment or arranges for immediate transfer to a higher
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
STROKE INITIATIVE. Sanford Tracy Medical Center. Danette Ronnfeldt, PA-C Jeri Schons, CNO Jean Metcalf, R.PH
 STROKE INITIATIVE Sanford Tracy Medical Center Danette Ronnfeldt, PA-C Jeri Schons, CNO Jean Metcalf, R.PH SANFORD TRACY Duluth Twin Cities Tracy Sioux Falls, SD SANFORD TRACY 25 bed Critical Access Hospital
STROKE INITIATIVE Sanford Tracy Medical Center Danette Ronnfeldt, PA-C Jeri Schons, CNO Jean Metcalf, R.PH SANFORD TRACY Duluth Twin Cities Tracy Sioux Falls, SD SANFORD TRACY 25 bed Critical Access Hospital
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
KGH Endovascular Thrombectomy Acute Ischemic Stroke Pilot Study Evaluation Report 2017
 KGH Endovascular Thrombectomy Acute Ischemic Stroke Pilot Study Evaluation Report 2017 WHY? - Context for EVT Most significant advance in stroke care in 20 years 5 Landmark Trials in 2015: strong evidence
KGH Endovascular Thrombectomy Acute Ischemic Stroke Pilot Study Evaluation Report 2017 WHY? - Context for EVT Most significant advance in stroke care in 20 years 5 Landmark Trials in 2015: strong evidence
Readiness Assessment Document for Acute Telestroke Collaboration (Sample. Checklist from OTN)
") Readiness Assessment Document for Acute Telestroke Collaboration (Sample Checklist from OTN) Telestroke Referring Site Application This application should be completed in conjunction with your Regional/District
Readiness Assessment Document for Acute Telestroke Collaboration (Sample Checklist from OTN) Telestroke Referring Site Application This application should be completed in conjunction with your Regional/District
Acute/Subacute Area Overview/Statement of Problem
 Acute/Subacute Area Overview/Statement of Problem Stroke is a medical emergency, and medical attention and specialized evaluation must be provided rapidly in order to minimize disability. Optimal stroke
Acute/Subacute Area Overview/Statement of Problem Stroke is a medical emergency, and medical attention and specialized evaluation must be provided rapidly in order to minimize disability. Optimal stroke
TIME CRITICAL DIAGNOSIS SYSTEM
 TIME CRITICAL DIAGNOSIS SYSTEM Recommendations to Advance Emergency Medical Care for Stroke and STEMI in Missouri Time Critical Diagnosis System Task Force for Stroke and STEMI August 2008 online version
TIME CRITICAL DIAGNOSIS SYSTEM Recommendations to Advance Emergency Medical Care for Stroke and STEMI in Missouri Time Critical Diagnosis System Task Force for Stroke and STEMI August 2008 online version
KY Medicaid Co-pays Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following:
 This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
KY Medicaid Co-pays. Acute admissions medical Per admission diagnoses $0 Acute health care related to. Per admission substance abuse and/or for
 This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
ONTARIO STROKE NETWORK STROKE DISTINCTION REPORT
 ONTARIO STROKE NETWORK STROKE DISTINCTION REPORT Organization: Kingston General Hospital (KGH) Address: 76 Stuart Street, Kingston, ON, K7L 2V7 Contact Name: Colleen Murphy & Cally Martin Contact Information:
ONTARIO STROKE NETWORK STROKE DISTINCTION REPORT Organization: Kingston General Hospital (KGH) Address: 76 Stuart Street, Kingston, ON, K7L 2V7 Contact Name: Colleen Murphy & Cally Martin Contact Information:
INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE
 INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE Bacharach Institute for Rehabilitation offers a number of in and outpatient rehabilitation programs and services designed
INPATIENT ACUTE REHABILITATION HOSPITAL LIMITATIONS, SCOPE AND INTENSITY OF CARE Bacharach Institute for Rehabilitation offers a number of in and outpatient rehabilitation programs and services designed
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Neurocritical Care Fellowship Program Requirements
 Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
American College of Rheumatology Fellowship Curriculum
 American College of Rheumatology Fellowship Curriculum Mission: The mission of all rheumatology fellowship training programs is to produce physicians that 1) are clinically competent in the field of rheumatology,
American College of Rheumatology Fellowship Curriculum Mission: The mission of all rheumatology fellowship training programs is to produce physicians that 1) are clinically competent in the field of rheumatology,
1/9/2017. Systems of Care in EMS: An Integrated System of Cardiac Care. Describe systems-based response to time-sensitive clinical conditions
 Systems of Care in EMS: An Integrated System of Cardiac Care NAEMSP Medical Director s Course January 23, 2017 Jefferson Williams, MD, MPH, FACEP Deputy Medical Director Wake County EMS System Clinical
Systems of Care in EMS: An Integrated System of Cardiac Care NAEMSP Medical Director s Course January 23, 2017 Jefferson Williams, MD, MPH, FACEP Deputy Medical Director Wake County EMS System Clinical
Stroke and TIA Service and Quality Core Standards 2016
 Stroke and TIA Service and Quality Core Standards 2016 Authors: Jackie Hudleston and Dr David Hargroves with Stroke Clinical Advisory Group Email: england.secn@nhs.net www.secn.nhs.uk Table of Contents
Stroke and TIA Service and Quality Core Standards 2016 Authors: Jackie Hudleston and Dr David Hargroves with Stroke Clinical Advisory Group Email: england.secn@nhs.net www.secn.nhs.uk Table of Contents
Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program
 Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program Hector E. James M.D., FAANS,FAAP,FCCM. Division of Pediatric Neurosurgery and Lucy Gooding Pediatric
Initiating, Developing, Structuring and Quality Improvement Aspects of a Pediatric Neurosurgery Program Hector E. James M.D., FAANS,FAAP,FCCM. Division of Pediatric Neurosurgery and Lucy Gooding Pediatric
RIKS-STROKE - ACUTE PHASE FOR REGISTRATION OF STROKE
 Version 14.a To be used for all acute stroke registrations from 1 January 2014 onwards. To register a TIA diagnosis without thrombolytic therapy please use separate TIA form. RIKS-STROKE - ACUTE PHASE
Version 14.a To be used for all acute stroke registrations from 1 January 2014 onwards. To register a TIA diagnosis without thrombolytic therapy please use separate TIA form. RIKS-STROKE - ACUTE PHASE
Sentinel Stroke National Audit Programme (SSNAP)
") Sentinel Stroke National Audit Programme (SSNAP) Acute organisational audit proforma 2016 Clinical Standards, Royal College of Physicians, London. On behalf of the Intercollegiate Stroke Working Party.
Sentinel Stroke National Audit Programme (SSNAP) Acute organisational audit proforma 2016 Clinical Standards, Royal College of Physicians, London. On behalf of the Intercollegiate Stroke Working Party.
Tele-urgent Services
 Ronald S. Weinstein, M.D. Director, Arizona Telemedicine Program Success factors Barriers Success factors Barriers to success 1 5. eicu (e Intensive Care Unit) 5. eicu (e Intensive Care Unit) 2 Teleradiology
Ronald S. Weinstein, M.D. Director, Arizona Telemedicine Program Success factors Barriers Success factors Barriers to success 1 5. eicu (e Intensive Care Unit) 5. eicu (e Intensive Care Unit) 2 Teleradiology
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 PROTOCOL 17A: Adult General Medical s Adult General Medical s Four (4) Levels of General Medical s Priority I and II Priority III No Will time and distance to the hospital of choice be detrimental to the
PROTOCOL 17A: Adult General Medical s Adult General Medical s Four (4) Levels of General Medical s Priority I and II Priority III No Will time and distance to the hospital of choice be detrimental to the
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
EMERGENCY DEPARTMENT ALGORITHM for ACUTE STROKE PATIENT
 EMERGENCY DEPARTMENT ALGORITHM for ACUTE STROKE PATIENT Patient presents to triage with signs and symptoms of stroke patient triaged CTAS Level 2 Emergency nurse completes assessment medical directive
EMERGENCY DEPARTMENT ALGORITHM for ACUTE STROKE PATIENT Patient presents to triage with signs and symptoms of stroke patient triaged CTAS Level 2 Emergency nurse completes assessment medical directive
Interprofessional Education Seminar Series: A Certificate Program for Health Care Providers. Basic Education of Selected Healthcare Professionals
 Interprofessional Education Seminar Series: A Certificate Program for Health Care Providers Basic Education of Selected Healthcare Professionals Audiology Dentist Dietician Evaluate and treat hearing and
Interprofessional Education Seminar Series: A Certificate Program for Health Care Providers Basic Education of Selected Healthcare Professionals Audiology Dentist Dietician Evaluate and treat hearing and
NSW Child Health Network Allied Health Education & Clinical Support Program Clinical Handover Report
 NSW Child Health Network Allied Health Education & Clinical Support Program Clinical Handover Report Carmel Blayden (M Health Science), Allied Health Educator Western Child Health Network, Ward 11, Bloomfield
NSW Child Health Network Allied Health Education & Clinical Support Program Clinical Handover Report Carmel Blayden (M Health Science), Allied Health Educator Western Child Health Network, Ward 11, Bloomfield
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Physicians Who Care for People with MS
 Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
Trauma Service Area - B (BRAC) Regional Stroke Plan
 Regional Stroke Plan") Trauma Service Area - B (BRAC) Regional Stroke Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, TX 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran, Cottle,
Trauma Service Area - B (BRAC) Regional Stroke Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, TX 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran, Cottle,
BENCHMARKING REPORT. Survey on carotid artery stenting privileging. Help us to help you. The mission. The design
 BENCHMARKING REPORT Survey on carotid artery stenting privileging Earlier this year, the Credentialing Resource Center (CRC) surveyed medical staff professionals (MSP) regarding which specialties should
BENCHMARKING REPORT Survey on carotid artery stenting privileging Earlier this year, the Credentialing Resource Center (CRC) surveyed medical staff professionals (MSP) regarding which specialties should
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care
 Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
Telestroke Alaska Evidence Based Care Across the Great Frontier
 Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
Bethesda Hospital PGY1 Residency Program Learning Experiences
 Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Running head: LEADERSHIP ANALYSIS: ROUNDING 1
 Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Neurology quality indicators
 Neurology A new approach for London Neurology quality indicators For adult neurological services December 2016 Acknowledgements The London Neuroscience Clinical Network is grateful to all who have contributed
Neurology A new approach for London Neurology quality indicators For adult neurological services December 2016 Acknowledgements The London Neuroscience Clinical Network is grateful to all who have contributed
Meaningful Use: A Brief Overview for Society of Health Systems
 Meaningful Use: A Brief Overview for Society of Health Systems Kevin Martin May 20, 2011 2011 Maestro Strategies LLC all rights reserved The Evolving Health Care Environment Multiple regulatory changes
Meaningful Use: A Brief Overview for Society of Health Systems Kevin Martin May 20, 2011 2011 Maestro Strategies LLC all rights reserved The Evolving Health Care Environment Multiple regulatory changes
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Interprofessional Rounding Presentations
 Interprofessional Rounding Presentations Sue Kelly & Diana Williamson, Grey Bruce Health Services Sandi Pincombe, St. Thomas Elgin General Hospital Sheila Hunt, London Health Sciences Centre INTER-PROFESSIONAL
Interprofessional Rounding Presentations Sue Kelly & Diana Williamson, Grey Bruce Health Services Sandi Pincombe, St. Thomas Elgin General Hospital Sheila Hunt, London Health Sciences Centre INTER-PROFESSIONAL
Review of Stroke (Acute Phase) and TIA Services
 and TIA Services") Review of Stroke (Acute Phase) and TIA Services Mid Staffordshire Health Economy Visit Date: 6 th December, 2011 Report Date: February 2012 WMQRS Mid Staffs Stroke Final Report V1 20120214.Doc 1 IDEX Introduction...
Review of Stroke (Acute Phase) and TIA Services Mid Staffordshire Health Economy Visit Date: 6 th December, 2011 Report Date: February 2012 WMQRS Mid Staffs Stroke Final Report V1 20120214.Doc 1 IDEX Introduction...
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
Nursing Care for Acute Ischemic Stroke Patients
 Nursing Care for Acute Ischemic Stroke Patients Highlights of lessons learned 2016 Annie Sanford MSN, RN Stroke Program Manager Swedish Medical Center, Seattle, WA 1 Learning Objectives: By attending this
Nursing Care for Acute Ischemic Stroke Patients Highlights of lessons learned 2016 Annie Sanford MSN, RN Stroke Program Manager Swedish Medical Center, Seattle, WA 1 Learning Objectives: By attending this
Consultation Paper. Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network
 Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
2009 Final Medicare Physician Fee Schedule (CMS-1403-FC) Rule Summary
 Rule Summary") 2009 Final Medicare Physician Fee Schedule (CMS-1403-FC) Rule Summary The 2009 Final Medicare Physician Fee Schedule will be published in the Federal Register on November 19, 2008. A display copy of this
2009 Final Medicare Physician Fee Schedule (CMS-1403-FC) Rule Summary The 2009 Final Medicare Physician Fee Schedule will be published in the Federal Register on November 19, 2008. A display copy of this
503 Psychiatric and Mental Health Nursing Clinical Performance Appraisal
 503 Psychiatric and Mental Health Nursing Clinical Performance Appraisal Clinical Objective 1: Develop communication skills that facilitate accurate problem identification and development of a therapeutic
503 Psychiatric and Mental Health Nursing Clinical Performance Appraisal Clinical Objective 1: Develop communication skills that facilitate accurate problem identification and development of a therapeutic
An Acute Care Nurse Practitioner Model of Care for Stroke Patients
 An Acute Care Nurse Practitioner Model of Care for Stroke Patients Holly A. Schenzel, BSN, RN DNP Student, Creighton University, School of Nursing, Omaha, NE Email: hollyannmarie@hotmail.com Telephone:
An Acute Care Nurse Practitioner Model of Care for Stroke Patients Holly A. Schenzel, BSN, RN DNP Student, Creighton University, School of Nursing, Omaha, NE Email: hollyannmarie@hotmail.com Telephone:
Surgical Critical Care Sub I
 Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
ONC Direct, CCD. National Consortium of Telehealth Resource Centers and PatientLink. MyLinks, vcarecommand
 Use Case Title: Telehealth & Stroke Continuum of Care Overview: Time is brain for Emily, a rural stroke patient. Telehealth expedites time to care with rapid pre-hospital video assessment in the ambulance
Use Case Title: Telehealth & Stroke Continuum of Care Overview: Time is brain for Emily, a rural stroke patient. Telehealth expedites time to care with rapid pre-hospital video assessment in the ambulance
REVISED ED STROKE ALERT PROCESS
 October 2016; Q3 Update REVISED ED STROKE ALERT PROCESS The SNGH Emergency Department Stroke Alert process is about to see some great changes! In response to the decrease in the target time to tpa (Alteplase)
October 2016; Q3 Update REVISED ED STROKE ALERT PROCESS The SNGH Emergency Department Stroke Alert process is about to see some great changes! In response to the decrease in the target time to tpa (Alteplase)
Hospital Compare Quality Measure Results for Oregon CAHs: 2015
 KEY FINDINGS: Flex Monitoring Team STATE DATA REPORT February 2017 Hospital Compare Quality Measure Results for Oregon : 2015 Michelle Casey, MS; Tami Swenson, PhD; Alex Evenson, MA University of Minnesota
KEY FINDINGS: Flex Monitoring Team STATE DATA REPORT February 2017 Hospital Compare Quality Measure Results for Oregon : 2015 Michelle Casey, MS; Tami Swenson, PhD; Alex Evenson, MA University of Minnesota
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Progress Notes Extra
 Medical Staff Office Cathy Crabtree : (937) 734-1212 Deb Charles: (937) 734-1229 Josie Hall: (937-734-1216 Tanya Webber: (937) 734-1213 September 2013 Progress Notes Extra Fall General Medical Staff Meeting
Medical Staff Office Cathy Crabtree : (937) 734-1212 Deb Charles: (937) 734-1229 Josie Hall: (937-734-1216 Tanya Webber: (937) 734-1213 September 2013 Progress Notes Extra Fall General Medical Staff Meeting
Clinical Applications
 Clinical Applications Ronald S. Weinstein, M.D. Director, Arizona Telemedicine Program Success factors Barriers Success factors Barriers to success 1 Tele-urgent Services 1. Teleradiology 2. Telecardiology
Clinical Applications Ronald S. Weinstein, M.D. Director, Arizona Telemedicine Program Success factors Barriers Success factors Barriers to success 1 Tele-urgent Services 1. Teleradiology 2. Telecardiology
ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010
 ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010 Objective Action Desired Output / Monitor and manage all those at risk of stroke and, refer as appropriate to smoking cessation services,
ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010 Objective Action Desired Output / Monitor and manage all those at risk of stroke and, refer as appropriate to smoking cessation services,
UNMH Neurology Clinical Privileges. Name: Effective Dates: From To
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective May 20, 2016: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective May 20, 2016: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial