2009 Final Medicare Physician Fee Schedule (CMS-1403-FC) Rule Summary
|
|
|
- Brook Glenn
- 6 years ago
- Views:
Transcription
1 2009 Final Medicare Physician Fee Schedule (CMS-1403-FC) Rule Summary The 2009 Final Medicare Physician Fee Schedule will be published in the Federal Register on November 19, A display copy of this final rule with a comment period can be found in its entirety on the Centers for Medicare and Medicaid (CMS) website at the following hyperlink: FC.pdf?agree=yes&next=Accept Comments will be accepted until December 29, Unless otherwise indicated, the provisions of this final rule with comment period are effective January 1, On July 15, 2008, after the release of the 2009 proposed Medicare fee schedule, Congress enacted the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA). Many of the provisions in MIPPA addressed similar issues that were raised in the proposed rule. The 2009 final rule is a combination of finalized proposals from the proposed rule, requests for further comments on proposals from the proposed rule, and discussion of implementation of provisions from MIPPA. The following are provisions of the final rule of interest to neurologists: 2009 Payment Update for Physician Services 1.1% Update Announced Telehealth Services Multiple Procedure Payment Reduction for Diagnostic Imaging Reduction in Technical Component Payment for Imaging Services Portable X-Ray Issues Part B Drug Payment Competitive Acquisition Program (CAP) Clinical Lab Fee Schedule Update Expansion of Independent Diagnostic Testing Facility (IDTF) Quality Standards to Physicians and NPPs Providing Diagnostic Services Physician Self-Referral and Anti-Markup Issues Exception for Incentive Payment and Shared Savings Programs Quality Initiatives (PQRI, E-Prescribing, Physician Resource Use Feedback Program) Other Miscellaneous Provisions 2009 Payment Update for Physician Services 1.1% Update Announced CMS implemented a 1.1% positive adjustment for physician services for A scheduled 15.1% cut was averted through a provision in MIPPA. Despite this positive adjustment, due to technical changes in the calculation of the physician payment rates the conversion factor (CF) will decrease in Conversion Factor: The 2009 CF will decrease from $ (2008) to $ (2009). This decrease is a result of another provision in MIPPA that requires CMS to change the way it calculates budget neutrality. CMS is required to apply a budget neutrality adjustment because changes caused by the Third Five Year Review of Work RVUs (implemented in 2007 and 2008) and changes in work RVUs in the 2009 MPFS exceeded $20 million. When the $20 million threshold is exceeded, CMS is required by law to offset these costs through a budget neutrality adjustment. While in the previous two years this adjustment had been applied to reductions in 1
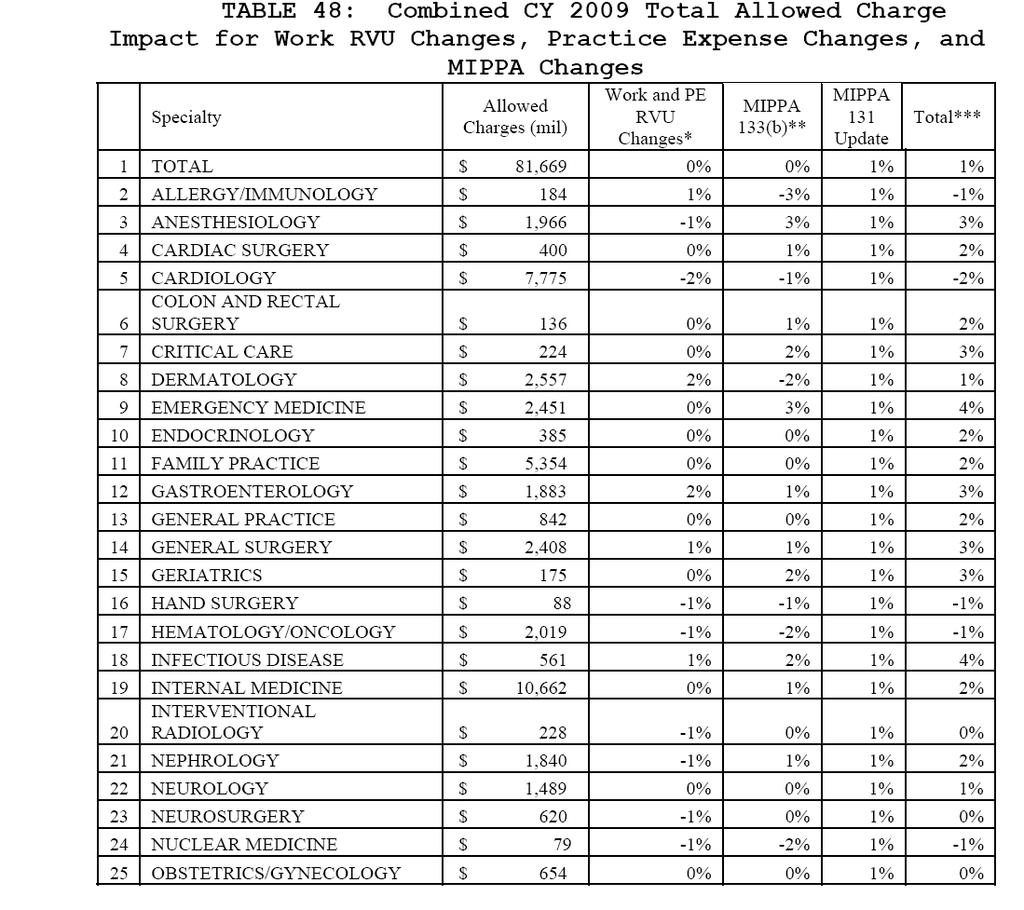
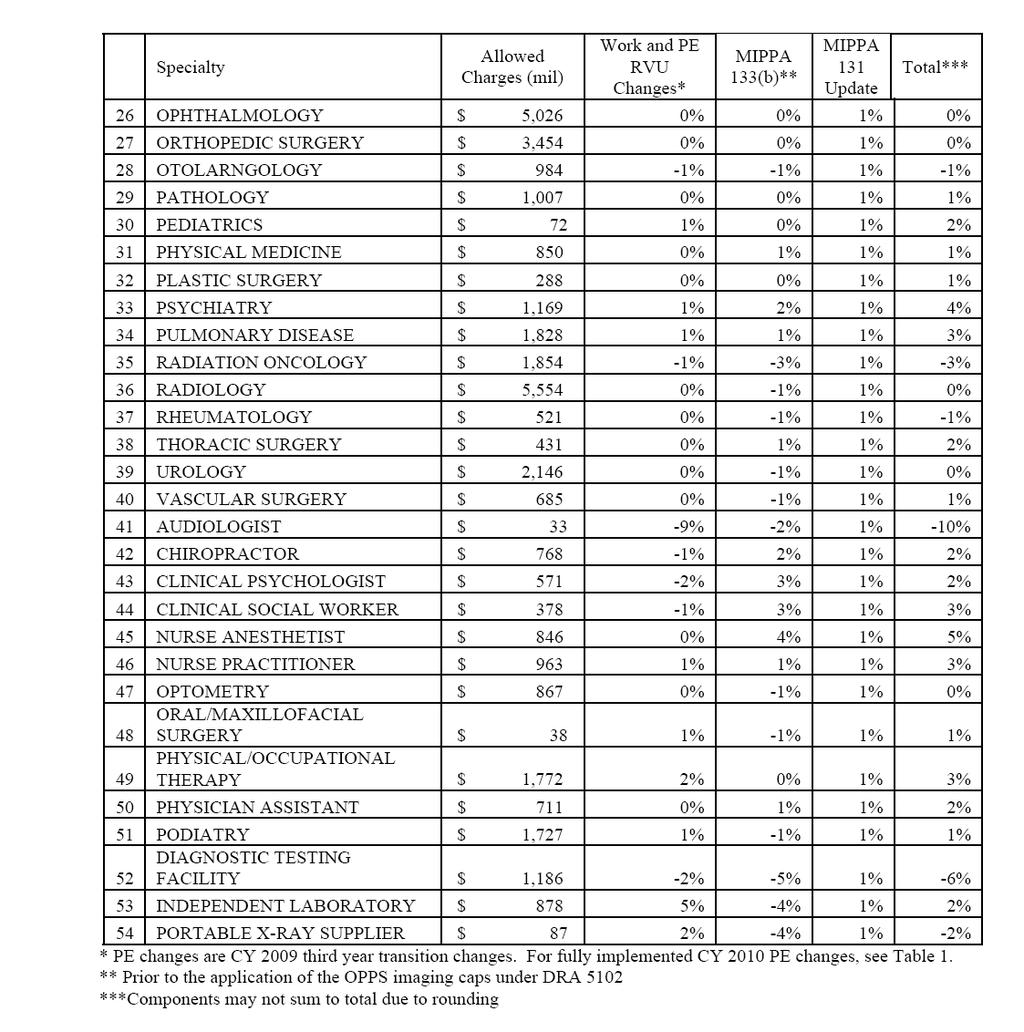
2 work RVUs, MIPPA requires CMS to apply the adjustment to the conversion factor (CF). This technical change resulted in an approximate 6% reduction in the conversion factor. Impact of New Budget Neutrality Adjustment Methodology: The application of budget neutrality on the CF being implemented in 2009 will have a greater impact on procedures with high PE values because the previous methodology only reduced work RVUs, this new methodology which adjusts the CF reduces all components of physician payment (work, practice expense (PE), and malpractice RVUs). In other words, procedures done in the office with high cost supplies, and/or expensive equipment will face greater reductions under the 2009 method of budget neutrality (CF adjusted) versus the method implemented in previous years (work RVUs adjusted). Year 3 of 4 Year Transition to New PE Methodology: The final factor impacting physician payment in 2009 are changes to PE RVUs. PE RVUs represent the resources used in furnishing supplies, office rent/lease, equipment and personnel wages (excluding malpractice expense) when providing physician services. In CY 2007 CMS implemented a new methodology for calculating PE RVUs. CMS is implementing this new methodology over a four year period. CY 2009 will be the third year of this transition. The new methodology will be fully implemented by Practice expense for any new codes created during this period will be based on the new methodology. The impact of this transition to a new PE methodology varies by individual code. CMS also finalized minor PE changes to a number of individual codes and continued its discussion on reconfiguring payment localities. Payment localities are used to estimate differences in local costs. The Agency is not making any changes to payment localities at this time. Impact on Specialties: Table 48 from the final rule shows the impact of the work RVU changes, practice expense changes and MIPPA changes by specialty. Based on this analysis, Neurology is estimated to experience an impact of 1% from all of these changes in the 2009 final rule. An excerpt from the table is below and the full table is attached. Table 48: Combined CY 2009 Total Allowed Charge Impact for Work RVU Changes, Practice Expense Changes, and MIPPA Changes Specialty Allowed Work and MIPPA MIPPA 131 Total Charges PE Changes* 133(b)** Update Total $81,669 0% 0% 1% 1% Neurology $1,489 0% 0% 1% 1% * PE changes are CY 2009 changes 3 rd year transitional changes. Prior to the application of the OPPS imaging caps under DRA * MIPPA 133(b) requires CMS to apply budget neutrality adjustment to CF. * MIPPA 131 provides for a 1.1% update for CY Table 49 shows the 2009 Medicare payment rates for high volume selected procedures. An excerpt of the chart highlighting several evaluation and management procedures follows. 2
3 Table 49: Impact of Final Rule with Comment Period and Estimated Physician Update on Payment for Selected Procedures CPT Descriptor Facility (Hospital Non-Facility (Office) % Change % Change Office/outpatient $41.90 $ % $59.80 $ % visit, est Office/outpatient $65.61 $ % $89.89 $ % visit, est Office $92.93 $ % $ $ % consultation Office $ $ % $ $ % consultation Initial inpatient $ $ % N/A N/A N/A consult Initial inpatient consult $ $ % N/A N/A N/A Telehealth Services Medicare policy allows for coverage and payment for Medicare telehealth includes consultation, office visits, individual psychotherapy, and pharmacologic management any additional services specified by the Secretary delivered via a telecommunications system. CMS maintains a list of eligible services. For 2009 CMS proposed creating a new series of HCPCS codes for follow-up inpatient telehealth consultations. Follow-up inpatient telehealth consultations are consultative visits furnished via telehealth to complete an initial consultation or subsequent consultative visits requested by the attending physician. In this final rule, CMS finalized this proposal to add follow-up inpatient telehealth consultation, as represented by HCPCS codes G0406 through G0408, to the list of Medicare telehealth services. G0406, Follow-up inpatient telehealth consultation, limited, typically 15 minutes communicating with the patient via telehealth G0407, Follow-up inpatient telehealth consultation, intermediate, typically 25 minutes communicating with the patient via telehealth G0408, Follow-up inpatient telehealth consultation complex, typically 33 minutes or more communicating with the patient via telehealth Changes to Multiple Procedure Payment Reduction for Diagnostic Imaging Effective January 1, 2006 CMS implemented a multiple procedure payment reduction (MPR) on certain diagnostic imaging procedures. When two or more procedures within one of 11 imaging code families are furnished on the same patient in a single session, the TC of the highest priced procedure is paid at 100 percent and the TC of the subsequent procedure is paid at 75 percent (a 25 percent reduction). The reduction does not apply to the PC. For CY 2009 CMS will make several changes to the MPR list: ten new procedures have been added and one code will be removed from the list since it was deleted for
4 CPT Descriptor Action Magnetic image, jaw joint Added Fmri brain by tech Added Cardiac mri for morph Added Cardiac mri w/stress img Added Cardiac mri for morph w/dye Added Card mri w/stress img & dye Added US exam k transpl w/doppler Added US exam K transpl w/ or w/out Deleted Doppler Us exam, scrotum Added Mri, one breast Added Mri, both breasts Added Reduction in Technical Component Payment for Imaging Services Section 5102 of DRA cap requires CMS to cap the technical component of the MPFS payment amount for certain imaging services by the hospital outpatient prospective payment system (HOPPS) amount for imaging services furnished on or after January 1, For the 2009 the list of codes subject to HOPPS cap has been revised to reflect new and deleted CPT codes for Codes (Nuclear medicine data proc) and (Nuclear med data proc) have been deleted. Code (Tte w/doppler, complete) has been added to the list. Portable X-Ray Issues The current requirements in regulations for the qualifications for technical personnel for portable x-ray services require a training of 24 months. A number of changes in the training and accreditation organizations and the curriculum have occurred since these regulations were established. CMS believes the current regulations are outdated and do not reflect current standards. CMS has finalized proposal to revise references to accrediting organizations to reflect the current entities involved and delete the requirement for formal training of not less than 24 months. Part B Drug Payment Competitive Acquisition Program The Competitive Acquisition Program (CAP) is an alternative to the ASP method of obtaining certain Part B drugs administered in physicians offices. Physicians who choose to participate in the CAP obtain approximately 190 drugs on the CAP drug list from an approved CAP vendor that was selected through a competitive bidding process and approved by CMS. A physician bills Medicare for administering a CAP drug. An approved CAP vendor bills Medicare for the CAP drug and collects applicable cost-sharing amounts from a beneficiary. In the 2009 proposed MPFS several refinements to the CAP program were proposed. However since the publication of the proposed rule CMS has announced the postponement of the 2009 CAP program due to contractual issues with CAP bidders. Currently the Agency is soliciting public feedback on the CAP from participating physicians, potential vendors, and other interested parties. 4
5 Clinical Lab Fee Schedule Update The freeze on the annual update to the lab fee schedule expires on January 1, For the period beginning January 1, 2009 the update will be 5.0 %. MIPPA reduces this increase by 0.5 percent for each of the years 2009 through For CY 2009 payment will be updated by 4.5 percent. Expansion of Independent Diagnostic Testing Facility (IDTF) Quality Standards to Physicians and NPPs Providing Diagnostic Services In the proposed rule CMS solicited comments on a proposal to require that physicians and NPPs who furnish diagnostic testing services, except mammography services, meet most of the quality and performance standards required for Independent Diagnostic Testing Facilities (IDTF). For 2009, CMS is not adopting its proposal to require physicians and NPPs to meet certain quality and performance standards when providing diagnostic testing services, except mammography services, within their medical practice setting. CMS has stated that they have deferred finalizing this proposal based on Section 135 of MIPPA which requires advanced diagnostic imaging service suppliers to be accredited by an accreditation organization by January 1, By deferring this decision, CMS maintains the option of finalizing this proposal in the future rulemaking efforts if it deems necessary. CMS is also finalizing several billing requirement proposals related for mobile entities providing diagnostic services: Entities furnishing diagnostic services must enroll in Medicare program as an IDTF regardless of where the services are furnished Mobile diagnostic services bill for the services they furnish unless it is part of a hospital service CMS is also finalizing several proposals related to enrollment and billing privileges of IDTFs in the Medicare program whose billing privileges have been revoked. Anti-Markup Issues The 2009 MPFS finalized new policies on the application of the anti-markup provisions as they relate to technical and professional components of diagnostic services, other than clinical laboratory services, provided by both for-profit and not-for-profit organizations. These policies will become effective on January 1, What is the Anti-Markup Provision? - Anti-markups become an issue when the individual performing the services is different than the individual billing Medicare for the service. If the anti-markup provision applies the billing physician must charge CMS the lower of: 1) the performing supplier s net charge to the billing physician; 2) the billing physician s actual charge or 3) the fee schedule charge for the test if the performing supplier billed Medicare directly. Scenarios in Which the Anti-Markup Provision Does NOT Apply to the TC and/or PC At least one of the two scenarios must be met in order for the anti-markup to not apply. 5
6 The performing physician performs substantially all of their professional services for the billing physician. In this rule CMS has defined substantially all as at least 75% of his or her professional services. This rule will disallow many part-time arrangements. The performing physician provides the service in the office where the billing physician conducts substantially the full range of patient care services that he or she generally furnishes. Potential Challenges of the Anti-Markup Provisions for Physician Organizations The substantially all scenario rule potentially can be more challenging for smaller practices that may not have enough volume to utilize 75 percent of a provider s time. This rule would probably be less difficult for larger practices with higher volume. Meeting the same building requirement will be difficult for group practices who do not have sufficient volume to meet the substantially all scenario. Exception for Incentive Payment and Shared Savings Programs The Medicare program and other private industry stakeholders are increasingly exploring various types of gainsharing, pay for performance and other similar programs. There is concern that existing exceptions to the physician self-referral statute may not be sufficiently flexible enough to encourage such programs. To address this potential challenge, in the 2009 proposed rule CMS proposed a targeted exception to the physician self-referral statute. CMS proposed a new, targeted exception to the physician self-referral statute for various types of gainsharing, pay-for-performance, value-based purchasing, and similar styled programs that use economic incentives to foster high quality, cost-effective care. These types of programs seek to align physician economic incentives with those of hospitals by offering physicians a share of the hospitals variable cost savings attributable to the physicians efforts in controlling the costs of providing patient care. This exception would permit incentive payments between physicians and entities furnishing designated health services (DHS), provided that certain conditions are satisfied. The purpose of this proposal was not to create any new programs but to propose an exception that would allow payment to a physician under such a program. CMS believes that such an exception would remove barriers to participation in existing programs. In this final 2009 CMS is not finalizing any proposals and is reopening the public comment period, seeking additional information. The Agency felt they received insufficient information and there was not consensus among commenters regarding possible modifications to the proposal. Commenters are requested to respond with greater specificity and provide practical examples when possible. Quality Initiatives (PQRI, E-Prescribing, Physician Resource Use Feedback Program) Physician Quality Reporting Initiative (PQRI) The Physician Quality Reporting Initiative (PQRI) was authorized by the Medicare, Medicaid, and SCHIP Extension Act (MMSEA) of In 2007 and 2008 participating professionals 6
7 were eligible for a bonus of 1.5 percent of the estimated total allowed charges for all covered professional services furnished during the reporting period PQRI Program Description - The final 2009 rule addresses several elements of the PQRI program. Bonus payment MIPPA made PQRI a permanent program and established a 2 percent bonus for the 2009 program Measures CMS approved measures for the 2009 program. These include measures from the 2008 PQRI program, additional National Quality Forum (NQF) endorsed measures, additional AQA-adopted measures and additional measures that had not received AQA adoption or NQF endorsement at the time the proposed rule was published but their inclusion was dependent on it. Paired measures The 2009 PQRI will include 4 measure sets that will be considered paired measures. Closely related individual measures that are recommended but not required to be submitted together. These paired measures do not constitute a measure group but may be subject to the measure validation strategy posted on the PQRI section of the CMS website. E-prescribing E-prescribing has been removed from the PQRI program and will be handled separately. Specifications - Detailed specifications providing guidance on the reporting of measures for the 2009 PQRI program will be posted on the CMS website no later than December 31. Audiologists Audiologists are now eligible to participate in PQRI. Participation Options - For the 2009 PQRI program providers can submit measures either individually or in measure groups. Measure groups are established by CMS. The 2009 program does not have any neurology-related measure groups. Additionally measures can be reported either through claims or patient registries. While in most cases the reporting period is from January 1 to December 31, 2009, there are opportunities for a shorter alternative reporting period (July 1-December 31, 2009) when reporting measure groups in certain circumstances Neurology-Related Measures- The 2009 PQRI program will include the same neurologyrelated measures used in the 2008 PQRI program: Stroke and Stroke Rehabilitation: Carotid Imaging Reports Stroke and Stroke Rehabilitation: Deep Vein Thrombosis Prophylaxis (DVT) for Ischemic Stroke or Intracranial Hemorrhage Stroke and Stroke Rehabilitation: Discharged on Antiplatelet Therapy Stroke and Stroke Rehabilitation: Anticoagulant Therapy Prescribed for Atrial Fibrillation at Discharge Stroke and Stroke Rehabilitation: Tissue Plasminogen Activator (t-pa) Considered Stroke and Stroke Rehabilitation: Screening for Dysphagia Stroke and Stroke Rehabilitation: Consideration of Rehabilitation Services Electronic Health Record (EHR) based submission for Reporting Individual Measures - In the 2009 proposed rule CMS proposed to begin EHR data submission for PQRI CMS will not finalize this proposal for 2009 and instead will complete the 2008 testing and continue additional 7
8 testing in In addition, upon completion of satisfactory testing, CMS will qualify EHR vendors and their specific products. By December 31, 2008 CMS will post on the PQRI section of the website a list of requirements that EHR vendors must be able to meet in order to selfnominate their product. To participate in the 2009 testing process, vendors must self nominate by Feb 13, Public Reporting of PQRI Data - It was indicated in the proposed rule that the data on PQRI quality measures that are submitted at the individual level could be the basis for public reporting of quality measurement performance results at individual or group level in the future. The Agency s broader goal is to make quality of care data publicly available. In this final rule CMS is soliciting comments on the appropriate use of PQRI data. Physician and Other Health Care Professional Compare Website MIPPA requires the Secretary to post on the CMS website, in an easily understandable format, a list of names of eligible professionals (or group practices) who satisfactorily submitted data on quality measures for the PQRI and the names of the eligible professional (or group practices) who are successful electronic subscribers. This cannot be applied retrospectively. CMS plans to launch a Physician and Other Health Care Professional Compare website that will enhance the information found on the current Physician and Other Health Care Professional Directory. The Agency s intent is to identify the eligible professionals who satisfactorily submit data on quality measures for the 2009 PQRI program on the CMS website in CMS will only post successful participants who receive a bonus payment. E-Prescribing MIPPA has authorized a new incentive program for eligible professionals who are successful electronic prescribers. In order to be eligible to participate in the E-prescribing program the electronic quality measure must apply to at least 10 percent of the professional s total Part B allowed charges. E-prescribers must report one of three G-codes described below at least 50% of the time to be considered successful and receive a bonus: All prescriptions related to the visit were electronically prescribed No prescriptions were generated during the visit Some or all prescriptions written or phoned in due to patient request, state or federal law, the pharmacy s system being unable to receive data electronically or because the prescription was for a narcotic or controlled substance The program uses a mix of carrots and sticks to encourage participation. Successful participants will be eligible for the following bonus payments: 2% in 2009; 2% in 2010; 1% in 2011; 1% in 2012; and, 0.5% in Eligible participants who are not successful or do not participate will face the following reductions to their Medicare payments: 1% in 2012; 1.5% in 2013; and - 2.0% in 2014 and each subsequent year. CMS will report publicly the names of eligible professionals who are successful electronic prescribers. Physician Resource Use Feedback Program MIPPA requires the Secretary to establish a Physician Feedback Program using Medicare claims data and other data to provide confidential feedback reports to physicians that measure the resources involved in furnishing care to Medicare beneficiaries. CMS is currently implementing Phase I of the program, reviewing claims data from in two cities to develop feedback 8
9 reports. Resource use will be measured on the episode basis and per capita basis. The Agency is soliciting comments on this program to begin finalizing the program for the future. Other Miscellaneous Provisions High Cost Supplies In the proposed rule CMS identified the top 65 high cost supply items over $150 and requested specialty societies to submit documentation on specific pricing information. There was one neurology-related supply on the list: electrode, grid (SD058). CMS was not satisfied with the data received and will continue working with physician groups and other parties to collect additional data. Potentially Misvalued Services The proposed rule discussed several methods of identifying potentially misvalued services. CMS stated in the final rule that it will continue to work with the American Medical Association (AMA) and may propose additional changes in future rulemaking. Services Often Billed Together and Expansion of the Multiple Procedure Reduction (MPPR) CMS has a long-standing policy of reducing payment for multiple surgical procedures performed on the same patient, by the same physician, on the same day. In recent years this policy has been extended to diagnostic and diagnostic imaging procedures. Concern has been raised that there may be inequities between specialties in the current coding and payment system regarding the extent to which there are opportunities for additional coding and payment for services performed on the same day. In the proposed rule CMS proposed to perform a data analysis of non-surgical CPT codes that are often billed together to explore this issue further. In the final rule CMS said they will continue to work with the AMA, the Medicare Advisory Payment Commission (MedPAC) and medical specialty societies to determine whether there are additional services that should be either bundled or subjected to a MPPR. Provider Enrollment and Billing Rules CMS finalized a number of proposals related to provider enrollment and billing rules including: establishing an effective billing date for physicians and non-physician practitioners, submitting claims after a final adverse action or CMS revocation, revised reporting responsibilities related to change of ownership, final adverse action, or change of location for physicians and nonphysician practitioners, and beneficiary signatures for non-emergency ambulance services. The rule also includes a number of other provisions including: expansion of the Initial Preventive Physical Examination (IPPE) benefit, authority to the Secretary to cover additional preventive services, and an extension of the 1.00 floor on the geographic adjustment to the physician work component of the fee schedule. 9
10 10
11 11
2010 Medicare Physician Fee Schedule Final Rule Summary
 2010 Medicare Physician Fee Schedule Final Rule Summary On October 30, 2009 the Centers for Medicare and Medicaid Services (CMS) posted a display copy of the final Medicare physician fee schedule (MPFS)
2010 Medicare Physician Fee Schedule Final Rule Summary On October 30, 2009 the Centers for Medicare and Medicaid Services (CMS) posted a display copy of the final Medicare physician fee schedule (MPFS)
2009 Medicare Physician Fee Schedule
 2009 Medicare Physician Fee Schedule July 16, 2008 Boston Brussels Chicago Düsseldorf Houston London Los Angeles Miami Munich New York Orange County Rome San Diego Silicon Valley Washington, D.C. Strategic
2009 Medicare Physician Fee Schedule July 16, 2008 Boston Brussels Chicago Düsseldorf Houston London Los Angeles Miami Munich New York Orange County Rome San Diego Silicon Valley Washington, D.C. Strategic
CY2015 Final Rule Summary Medical Oncology
 CY2015 Final Rule Summary Medical Oncology Medicare Physician Fee Schedule (MPFS) Prepared By: Revenue Cycle Inc. Prepared On: October 31, 2014 http://www.revenuecycleinc.com/disclaimer. 1817 West By using
CY2015 Final Rule Summary Medical Oncology Medicare Physician Fee Schedule (MPFS) Prepared By: Revenue Cycle Inc. Prepared On: October 31, 2014 http://www.revenuecycleinc.com/disclaimer. 1817 West By using
Corporate Reimbursement Policy Telehealth
 Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary
 CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary On July 13, 2017, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2018.
CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary On July 13, 2017, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2018.
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
I. Disclosure Requirements for Financial Relationships Between Hospitals and Physicians
 2400:1018 BNA s HEALTH LAW & BUSINESS SERIES provided certain additional elements (based largely on the physician recruitment exception) are satisfied. 133 10. Professional courtesy, 42 C.F.R. 411.357(s)
2400:1018 BNA s HEALTH LAW & BUSINESS SERIES provided certain additional elements (based largely on the physician recruitment exception) are satisfied. 133 10. Professional courtesy, 42 C.F.R. 411.357(s)
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues. History of the Physician Fee Schedule
 American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Institute on Medicare and Medicaid Payment Issues. Baltimore Marriott Waterfront Hotel
 Institute on Medicare and Medicaid Payment Issues Baltimore Marriott Waterfront Hotel March 28-30, 2012 1 Diagnostic Imaging Accreditation and Regulatory Requirements Today s Talk Attack on Payment MPPR
Institute on Medicare and Medicaid Payment Issues Baltimore Marriott Waterfront Hotel March 28-30, 2012 1 Diagnostic Imaging Accreditation and Regulatory Requirements Today s Talk Attack on Payment MPPR
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A
 Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Medical Practice Executive Insights
 Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
CY 2012 Medicare Outpatient Prospective Payment System (OPPS) Final Rule
 Final Rule") CY 2012 Medicare Outpatient Prospective Payment System (OPPS) Final Rule Lori Mihalich-Levin, J.D. (lmlevin@aamc.org; 202-828-0599) Jennifer Faerberg (jfaerberg@aamc.org; 202-862-6221) Jane Eilbacher (jeilbacher@aamc.org;
CY 2012 Medicare Outpatient Prospective Payment System (OPPS) Final Rule Lori Mihalich-Levin, J.D. (lmlevin@aamc.org; 202-828-0599) Jennifer Faerberg (jfaerberg@aamc.org; 202-862-6221) Jane Eilbacher (jeilbacher@aamc.org;
Medicare s Proposed CY 2016 Physician Fee Schedule
 Issue Brief Medicare s Proposed CY 2016 Physician Fee Schedule Background On July 15, 2015, the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed CY 2016 Medicare
Issue Brief Medicare s Proposed CY 2016 Physician Fee Schedule Background On July 15, 2015, the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed CY 2016 Medicare
Excerpts of the Code of Federal Regulations Referenced in Proposed Rule CMS 1403 P
 Excerpts of the Code of Federal Regulations Referenced in Proposed Rule CMS 1403 P The document below reflects the sections of the regulations currently in effect for Independent Diagnostic Testing Facilities
Excerpts of the Code of Federal Regulations Referenced in Proposed Rule CMS 1403 P The document below reflects the sections of the regulations currently in effect for Independent Diagnostic Testing Facilities
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule
 Final Rule") Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule
 and Quality Payment Program (QPP) Proposed Rule") Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule On July 12, 2018, the Centers for Medicare and Medicaid Services (CMS) released the Revisions
Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule On July 12, 2018, the Centers for Medicare and Medicaid Services (CMS) released the Revisions
2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS
 2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS OVERVIEW: The Centers for Medicare and Medicaid Services (CMS) released the proposed 2014 Medicare Physician Fee Schedule in July. Final code
2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS OVERVIEW: The Centers for Medicare and Medicaid Services (CMS) released the proposed 2014 Medicare Physician Fee Schedule in July. Final code
2018 Biliary Reimbursement Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Medicare Physician Fee Schedule Final Rule for Calendar Year 2018 Detailed Summary of the Payment Provisions
 Medicare Physician Fee Schedule Final Rule for Calendar Year 2018 Detailed Summary of the Payment Provisions The American College of Radiology (ACR) has prepared this detailed analysis of changes to the
Medicare Physician Fee Schedule Final Rule for Calendar Year 2018 Detailed Summary of the Payment Provisions The American College of Radiology (ACR) has prepared this detailed analysis of changes to the
Highmark Reimbursement Policy Bulletin
 Highmark Reimbursement Policy Bulletin CLICK HERE FOR HISTORY VERSIONS Bulletin Number: RP-007 Subject: Multiple Procedure Payment Reduction (MPPR) for Certain Diagnostic Imaging Procedures Effective Date:
Highmark Reimbursement Policy Bulletin CLICK HERE FOR HISTORY VERSIONS Bulletin Number: RP-007 Subject: Multiple Procedure Payment Reduction (MPPR) for Certain Diagnostic Imaging Procedures Effective Date:
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals. August 11, 2010
 Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix
: The Doc Fix") April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Physician Quality Reporting System (PQRS) Changes
 Changes") Physician Quality Reporting System (PQRS) Changes Summary: Extends through 2014 payments under the Physician Quality Reporting System (PQRS, formerly the Physician Quality Reporting Initiative or PQRI)
Physician Quality Reporting System (PQRS) Changes Summary: Extends through 2014 payments under the Physician Quality Reporting System (PQRS, formerly the Physician Quality Reporting Initiative or PQRI)
Emergency Department Update 2010 Outpatient Payment System
 Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Medicare Home Health Prospective Payment System
 Medicare Home Health Prospective Payment System Payment Rule Brief Final Rule Program Year: CY 2013 Overview On November 8, 2012, the Centers for Medicare and Medicaid Services (CMS) officially released
Medicare Home Health Prospective Payment System Payment Rule Brief Final Rule Program Year: CY 2013 Overview On November 8, 2012, the Centers for Medicare and Medicaid Services (CMS) officially released
Our comments focus on the following components of the proposed rule: - Site Neutral Payments,
 Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health & Human Services Hubert H. Humphrey Building 200 Independence Ave., S.W. Room 445-G Washington, DC 20201
Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health & Human Services Hubert H. Humphrey Building 200 Independence Ave., S.W. Room 445-G Washington, DC 20201
FY 2014 Inpatient Prospective Payment System Proposed Rule
 FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
Executive Summary, November 2015
 Medicare Physician Fee Schedule Final Rule for Calendar Year 2016 Makes Changes in Stark Law Regulatory Provisions and Contains Important Updates of Medicare Payment Policies Executive Summary, November
Medicare Physician Fee Schedule Final Rule for Calendar Year 2016 Makes Changes in Stark Law Regulatory Provisions and Contains Important Updates of Medicare Payment Policies Executive Summary, November
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
Jurisdiction Nebraska. Retirement Date N/A
 If you wish to save the PDF, please ensure that you change the file extension to.pdf (from.ashx). Local Coverage Determination (LCD): Independent Diagnostic Testing Facilities (IDTFs) (L31626) Contractor
If you wish to save the PDF, please ensure that you change the file extension to.pdf (from.ashx). Local Coverage Determination (LCD): Independent Diagnostic Testing Facilities (IDTFs) (L31626) Contractor
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
201 & 202 of the Balanced Budget Refinement Act of 1999 (BBRA), provides authority
, provides authority") Background Section 4523 of the Balanced Budget Act of 1997 (BBA), as amended by sections 201 & 202 of the Balanced Budget Refinement Act of 1999 (BBRA), provides authority for CMS to implement an outpatient
Background Section 4523 of the Balanced Budget Act of 1997 (BBA), as amended by sections 201 & 202 of the Balanced Budget Refinement Act of 1999 (BBRA), provides authority for CMS to implement an outpatient
Legal Issues in Medicare/Medicaid Incentive Programss
 Meaningful Use Legal Issues in Medicare/Medicaid Incentive Programss Jane Eckels, Esq. Partner, Health Information Technology Group Deputy Chair, Technology, ebusiness and Digital Media Group Overview
Meaningful Use Legal Issues in Medicare/Medicaid Incentive Programss Jane Eckels, Esq. Partner, Health Information Technology Group Deputy Chair, Technology, ebusiness and Digital Media Group Overview
The Affordable Care Act
 The Affordable Care Act Medical City, Dallas, TX October 26, 2012 Presented by Cheryl West, MPH Director, Government Affairs, AARC Affordable Care Act (ACA) 2 What I m Not Going to Talk About 3 What I
The Affordable Care Act Medical City, Dallas, TX October 26, 2012 Presented by Cheryl West, MPH Director, Government Affairs, AARC Affordable Care Act (ACA) 2 What I m Not Going to Talk About 3 What I
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Re: Payment Policies under the Physician Fee Schedule Proposed Rule for CY 2014; 78 Fed. Reg. 43,281 (July 19, 2013); CMS-1600; RIN 0938-AR56
; CMS-1600; RIN 0938-AR56") September 6, 2013 Marilyn B. Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW
September 6, 2013 Marilyn B. Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
CY 2019 Physician Fee Schedule Proposed Rule Summary
 CY 2019 Physician Fee Schedule Proposed Rule Summary On July 11, 2018, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2019, which for
CY 2019 Physician Fee Schedule Proposed Rule Summary On July 11, 2018, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2019, which for
Hospital Outpatient Quality Reporting (OQR) Program Requirements: CY 2015 OPPS/ASC Final Rule
 Program Requirements: CY 2015 OPPS/ASC Final Rule") Hospital Outpatient Quality Reporting (OQR) Program Requirements: CY 2015 OPPS/ASC Final Rule Elizabeth Bainger, MS, BSN, CPHQ Centers for Medicare & Medicaid Services (CMS) Program Lead Hospital Outpatient
Hospital Outpatient Quality Reporting (OQR) Program Requirements: CY 2015 OPPS/ASC Final Rule Elizabeth Bainger, MS, BSN, CPHQ Centers for Medicare & Medicaid Services (CMS) Program Lead Hospital Outpatient
CY2017 Medicare Outpatient Prospective Payment System (OPPS) Final Rule with Interim Final Comment (IFC)
 Final Rule with Interim Final Comment (IFC)") Housekeeping You will not hear any audio until the webinar begins. To join the audio, select call me and enter your phone number or select I will call in. If you select I will call in, follow the prompts
Housekeeping You will not hear any audio until the webinar begins. To join the audio, select call me and enter your phone number or select I will call in. If you select I will call in, follow the prompts
Emergency Department Update 2009 Outpatient Payment System
 Emergency Department Update 2009 Outpatient Payment System ED Facility Level Guidelines Critical Care Composite APCs and No Diagnosis Limitations OPPS Facility Conversion Factor Update Hospital Outpatient
Emergency Department Update 2009 Outpatient Payment System ED Facility Level Guidelines Critical Care Composite APCs and No Diagnosis Limitations OPPS Facility Conversion Factor Update Hospital Outpatient
RECOVERY AUDIT CONTRACTORS
 RECOVERY AUDIT CONTRACTORS RAC SUBSCRIPTION SERVICE Being Proactive Telemedicine Rule and CMS Updates May 10, 2011 2011 Aegis Compliance & Ethics Center, LLP 1 Faculty Brian Annulis, JD Partner, Meade
RECOVERY AUDIT CONTRACTORS RAC SUBSCRIPTION SERVICE Being Proactive Telemedicine Rule and CMS Updates May 10, 2011 2011 Aegis Compliance & Ethics Center, LLP 1 Faculty Brian Annulis, JD Partner, Meade
EHR Incentives. Profit by using LOGO a certified EHR. EHR vs. EMR. PQRI Incentives. Incentives available
 EHR vs. EMR EHR Incentives Company Profit by using LOGO a certified EHR EMR - Electronic records of health-related information on an individual that can be created, gathered, managed, and consulted by
EHR vs. EMR EHR Incentives Company Profit by using LOGO a certified EHR EMR - Electronic records of health-related information on an individual that can be created, gathered, managed, and consulted by
September 6, Submitted electronically at
 9312 Old Georgetown Road Bethesda, MD 20814-1621 Tel: 301-571-9200 Fax: 301-530-2752 www.apma.org September 6, 2013 Marilyn B. Tavenner Administrator Centers for Medicare & Medicaid Services Department
9312 Old Georgetown Road Bethesda, MD 20814-1621 Tel: 301-571-9200 Fax: 301-530-2752 www.apma.org September 6, 2013 Marilyn B. Tavenner Administrator Centers for Medicare & Medicaid Services Department
Reimbursement for Anticoagulation Services
 Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Protecting Access to Medicare Act of 2014
 Protecting Access to Medicare Act of 2014 Protects Current Medicare Beneficiaries Doc Fix : Prevents the 24% cut in reimbursement to doctors who treat Medicare patients on April 1, 2014 and replaces it
Protecting Access to Medicare Act of 2014 Protects Current Medicare Beneficiaries Doc Fix : Prevents the 24% cut in reimbursement to doctors who treat Medicare patients on April 1, 2014 and replaces it
CMS Meaningful Use Incentives NPRM
 CMS Meaningful Use Incentives NPRM Margret Amatayakul MBA, RHIA, CHPS, CPHIT, CPEHR, CPHIE, FHIMSS President, Margret\A Consulting, LLC Faculty and Board of Examiners, Health IT Certification, LLC Notice
CMS Meaningful Use Incentives NPRM Margret Amatayakul MBA, RHIA, CHPS, CPHIT, CPEHR, CPHIE, FHIMSS President, Margret\A Consulting, LLC Faculty and Board of Examiners, Health IT Certification, LLC Notice
December 30, Dear Administrator Tavenner:
 Ms. Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1612-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
Ms. Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1612-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
Assignment of Medicare Fee-for-Service Beneficiaries
 February 6, 2015 Ms. Marilyn B. Tavenner, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1461-P Room 445-G, Hubert H. Humphrey Building 200
February 6, 2015 Ms. Marilyn B. Tavenner, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1461-P Room 445-G, Hubert H. Humphrey Building 200
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
2017 Proposed Rule Physician Fee Schedule in the Federal Register
 2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
Provider-Based Hospital Departments Are We Compliant?
 Critical Access Hospital and Provider-Based Hospital Departments Are We Compliant? September 14, 2017 1 Reasons for Hospital/Clinic Integration History of Provider-Based Regulations Provider-Based Requirements
Critical Access Hospital and Provider-Based Hospital Departments Are We Compliant? September 14, 2017 1 Reasons for Hospital/Clinic Integration History of Provider-Based Regulations Provider-Based Requirements
Submission #1. Short Description: Medicare Payment to HOPDs, Section 603 of BiBA 2015
 Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Overview of Meaningful Use Medicare and Medicaid EHR Incentive Programs
 Contents Page # I. Background 1 FR 1846 Regulation Language Summary: This proposed rule would implement the provisions of the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub. L. 111-5) that
Contents Page # I. Background 1 FR 1846 Regulation Language Summary: This proposed rule would implement the provisions of the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub. L. 111-5) that
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
Prior to implementation of the episode groups for use in resource measurement under MACRA, CMS should:
 Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
ASCs and Meaningful Use. Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy
 ASCs and Meaningful Use Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy Today s Discussion Review of Meaningful Use and implications
ASCs and Meaningful Use Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy Today s Discussion Review of Meaningful Use and implications
September 2, Dear Administrator Tavenner:
 September 2, 2014 Marilyn B. Tavenner, MHA, BSN, RN Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services P. O. Box 8013 Baltimore, MD 21244-8013 RE: Medicare
September 2, 2014 Marilyn B. Tavenner, MHA, BSN, RN Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services P. O. Box 8013 Baltimore, MD 21244-8013 RE: Medicare
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Advancing Care Coordination Proposed Rule
 Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
AHLA. O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths. Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA
 AHLA O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA Fraud and Compliance Forum October 6-7, 2014 Alice G. Gosfield American
AHLA O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA Fraud and Compliance Forum October 6-7, 2014 Alice G. Gosfield American
HOME DIALYSIS REIMBURSEMENT AND POLICY. Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation
 HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
H.R MEDICARE TELEHEALTH PARITY ACT OF 2017
 FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
2011 Melanoma Physician Quality Reporting (PQRS): FREQUENTLY ASKED QUESTIONS
: FREQUENTLY ASKED QUESTIONS") Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
September 6, Dear Ms. Tavenner:
 September 6, 2013 Marilyn Tavenner Acting Administrator and Chief Operating Officer Centers for Medicare and Medicaid Services Department of Health and Human Services P. O. Box 8013 Baltimore, MD 21244-8013
September 6, 2013 Marilyn Tavenner Acting Administrator and Chief Operating Officer Centers for Medicare and Medicaid Services Department of Health and Human Services P. O. Box 8013 Baltimore, MD 21244-8013
Medicare Diagnostic Testing, Anti-Markup Restrictions and IDTF Standards THOMAS W. GREESON, DANIEL H. MELVIN TABLE OF CONTENTS
 Medicare Diagnostic Testing, Anti-Markup Restrictions and IDTF Standards THOMAS W. GREESON, DANIEL H. MELVIN TABLE OF CONTENTS I. Medicare Coverage... 1 A. Basis for Medicare Coverage of Diagnostic Testing
Medicare Diagnostic Testing, Anti-Markup Restrictions and IDTF Standards THOMAS W. GREESON, DANIEL H. MELVIN TABLE OF CONTENTS I. Medicare Coverage... 1 A. Basis for Medicare Coverage of Diagnostic Testing
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010
 The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1
 Services 1") GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
Eligibility. Program Structure and Process for Receiving Incentives
 Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Oklahoma Health Care Authority. Telemedicine
 Oklahoma Health Care Authority Telemedicine Telemedicine Policy: OAC 317:30-3-27 Billing Technology 2 Telemedicine Applicability & Scope The purpose of the SoonerCare telemedicine is to improve access
Oklahoma Health Care Authority Telemedicine Telemedicine Policy: OAC 317:30-3-27 Billing Technology 2 Telemedicine Applicability & Scope The purpose of the SoonerCare telemedicine is to improve access
STARK AND REIMBURSEMENT: A DEEPER DIVE TO DEBUNK THE MYTHS. Alice G. Gosfield, Esquire Alice G. Gosfield and Associates, P.C.
 STARK AND REIMBURSEMENT: A DEEPER DIVE TO DEBUNK THE MYTHS I. Scope of Stark Alice G. Gosfield, Esquire Alice G. Gosfield and Associates, P.C. Philadelphia, PA A. DHS only by virtue of definition of a
STARK AND REIMBURSEMENT: A DEEPER DIVE TO DEBUNK THE MYTHS I. Scope of Stark Alice G. Gosfield, Esquire Alice G. Gosfield and Associates, P.C. Philadelphia, PA A. DHS only by virtue of definition of a
Overview of Select Health Provisions FY 2015 Administration Budget Proposal
 Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
2015 MEDICARE UPDATES
 Disclaimer 2015 MEDICARE UPDATES The information contained in these slides are current at the time of writing. However, CMS can change the information at any time. Please monitor the ISMA website and all
Disclaimer 2015 MEDICARE UPDATES The information contained in these slides are current at the time of writing. However, CMS can change the information at any time. Please monitor the ISMA website and all
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Chapter 13 Section 2. Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups
 Groups") Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Agenda Based on Medicare / CMS Guidelines
 January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
Coding Guidelines for Certain Respiratory Care Services January 2018 (updates in red)
") Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
September 2, Dear Administrator Tavenner:
 September 2, 2014 Marilynn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS -1612-P Mail Stop 7500 Security Boulevard Baltimore,
September 2, 2014 Marilynn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS -1612-P Mail Stop 7500 Security Boulevard Baltimore,
December 3, 2010 BY COURIER AND ELECTRONIC MAIL
 Charles N. Kahn III President & CEO December 3, 2010 BY COURIER AND ELECTRONIC MAIL Donald Berwick, M.D. Administrator Centers for Medicare & Medicaid Services Attention: CMS-6028-P Hubert H. Humphrey
Charles N. Kahn III President & CEO December 3, 2010 BY COURIER AND ELECTRONIC MAIL Donald Berwick, M.D. Administrator Centers for Medicare & Medicaid Services Attention: CMS-6028-P Hubert H. Humphrey
TCS FAQ s. How will the implementation of national standard code sets reduce burden on the health care industry?
 TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered
 CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
Eligible Professional Core Measure Frequently Asked Questions
 Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
CHANGE M OCTOBER 23, CHAPTER 5 Section 4, pages 1 and 2 Section 4, pages 1 and 2
 CHANGE 149 6010.58-M OCTOBER 23, 2017 REMOVE PAGE(S) INSERT PAGE(S) CHAPTER 5 Section 4, pages 1 and 2 Section 4, pages 1 and 2 CHAPTER 7 Section 2, pages 3 and 4 Section 2, pages 3 and 4 CHAPTER 13 Section
CHANGE 149 6010.58-M OCTOBER 23, 2017 REMOVE PAGE(S) INSERT PAGE(S) CHAPTER 5 Section 4, pages 1 and 2 Section 4, pages 1 and 2 CHAPTER 7 Section 2, pages 3 and 4 Section 2, pages 3 and 4 CHAPTER 13 Section
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is