BMC Health Services Research 2011, 11:285
|
|
|
- Evangeline Wells
- 6 years ago
- Views:
Transcription

1 BMC Health Services Research This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. A longitudinal, multi-level comparative study of quality and safety in European hospitals: the QUASER study protocol BMC Health Services Research 2011, 11:285 doi: / Glenn B Robert (glenn.robert@kcl.ac.uk) Janet E Anderson (janet.anderson@kcl.ac.uk) Susan J Burnett (s.burnett@imperial.ac.uk) Karina Aase (karina.aase@uis.no) Boel Andersson-Gare (boel.andersson-gare@lj.se) Roland Bal (r.bal@bmg.eur.nl) Johan Calltorp (johan.caltorp@comhem.se) Francisco Nunes (francisco.nunes@iscte.pt) Anne-Marie Weggelaar (annemarie@weggelaar.com) Charles A Vincent (c.vincent@imperial.ac.uk) Naomi J Fulop (naomi.fulop@kcl.ac.uk) The QUASER Team (not@valid.com) ISSN Article type Study protocol Submission date 17 May 2011 Acceptance date 26 October 2011 Publication date 26 October 2011 Article URL Like all articles in BMC journals, this peer-reviewed article was published immediately upon acceptance. It can be downloaded, printed and distributed freely for any purposes (see copyright notice below). Articles in BMC journals are listed in PubMed and archived at PubMed Central. For information about publishing your research in BMC journals or any BioMed Central journal, go to Robert et al. ; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
2 A longitudinal, multi-level comparative study of quality and safety in European hospitals: the QUASER study protocol. Glenn B Robert*, National Nursing Research Unit, King s College London, 57 Waterloo Road, London, SE1 8WA, England glenn.robert@kcl.ac.uk Janet E Anderson, King s Patient Safety and Service Quality Research Centre, King s College London, 150 Stamford Street, London, SE1 9NH, England, janet.anderson@kcl.ac.uk Susan J Burnett, Centre for Patient Safety & Service Quality, Imperial College, St Mary's Campus, Norfolk Place, London, W2 1PG, UK, England s.burnett@imperial.ac.uk Karina Aase, Department for Media, Cultural and Social Studies, University of Stavanger, 4036 Stavanger, Norway, karina.aase@uis.no Boel Andersson-Gare, The Jönköping Academy for Improvement of Health and Welfare, Box 1026, Jönköping, Sweden, boel.andersson-gare@lj.se Roland Bal, Institute of Health Policy & Management, Erasmus University Rotterdam, Postbus 1738, 3000 DR Rotterdam, the Netherlands, r.bal@bmg.eur.nl Johan Calltorp, The Jönköping Academy for Improvement of Health and Welfare, Box 1026, Jönköping, Sweden, johan.calltorp@comhem.se Francisco Nunes, Instituto Superior de Ciências do Trabalho e da Empresa (ISCTE), Av.ª das Forças Armadas, Lisboa, Portugal, francisco.nunes@iscte.pt 1
3 Anne-Marie Weggelaar, Institute of Health Policy & Management, Erasmus University Rotterdam, Postbus 1738, 3000 DR Rotterdam, the Netherlands, Charles A Vincent, Centre for Patient Safety & Service Quality, Imperial College, St Mary's Campus, Norfolk Place, London W2 1PG, UK, England, c.vincent@imperial.ac.uk Naomi J Fulop, King s Patient Safety and Service Quality Research Centre, King s College London, 42 Weston Street, London, SE1 3QD, England, naomi.fulop@kcl.ac.uk The QUASER team (see acknowledgements). *corresponding author 2
4 ABSTRACT Background: although there is a wealth of information available about quality improvement tools and techniques in healthcare there is little understanding about overcoming the challenges of day-to-day implementation in complex organisations like hospitals. The Quality and Safety in Europe by Research (QUASER) study will investigate how hospitals implement, spread and sustain quality improvement, including the difficulties they face and how they overcome them. The overall aim of the study is to explore relationships between the organisational and cultural characteristics of hospitals and how these impact on the quality of health care; the findings will be designed to help policy makers, payers and hospital managers understand the factors and processes that enable hospitals in Europe to achieve - and sustain - high quality services for their patients. Methods/design: in-depth multi-level (macro, meso and micro-system) analysis of healthcare quality policies and practices in 5 European countries, including longitudinal case studies in a purposive sample of 10 hospitals. The project design has three major features: a working definition of quality comprising three components: clinical effectiveness, patient safety and patient experience a conceptualisation of quality as a human, social, technical and organisational accomplishment 3
5 an emphasis on translational research that is evidence-based and seeks to provide strategic and practical guidance for hospital practitioners and health care policy makers in the European Union. Throughout the study we will adopt a mixed methods approach, including qualitative (indepth, narrative-based, ethnographic case studies using interviews, and direct nonparticipant observation of organisational processes) and quantitative research (secondary analysis of safety and quality data, for example: adverse incident reporting; patient complaints and claims). Discussion: the protocol is based on the premise that future research, policy and practice need to address the sociology of improvement in equal measure to the science and technique of improvement, or at least expand the discipline of improvement to include these critical organisational and cultural processes. We define the organisational and cultural characteristics associated with better quality of care in a broad sense that encompasses all the features of a hospital that might be hypothesised to impact upon clinical effectiveness, patient safety and/or patient experience. 4
6 BACKGROUND There is now a good understanding and knowledge of the types of quality improvement (QI) interventions that are undertaken in healthcare (1) but less understanding of how to increase their effectiveness (2). Studies on healthcare quality increasingly point to understanding organisational issues in health service delivery as central to explaining variations in care and making progress towards sustained quality improvement. The Institute of Medicine s watershed To Err is Human (3) and Crossing the Quality Chasm (4) reports specifically identified organisational failings as one of the root causes of poor quality, with the latter devoting an entire chapter to analysing healthcare organisations as complex, adaptive systems and the implications of this perspective for implementing change. As elaborated by others (5-7) this perspective includes recognising the multiple levels of the healthcare system. High-level influences such as policy, payment rules, regulation and accreditation are strongly mediated by dynamics and responses not only at the levels of hospitals, but also the smaller care delivery units within hospitals that deliver services directly to patients. A rigorous, if relatively small, body of research does exist in the health services literature which specifically attempts to unravel this black box of organisation at the hospital level and its impact on the quality of care (8-9). This work has focused on identifying hospital predictors of successful implementation of quality improvement, typically using multivariate statistical methods and quasi-experimental data, and has highlighted a number of factors that appear to be associated with successfully implementing change in hospitals (10). The factors that predict successful quality improvement implementation include leadership 5
7 support (11), particular dimensions of organisational culture and climate (12-13), and teambased structures and composition (14), as well as investing in the measurement of quality and making quality projects do-able (15-16). As noted previously (17), there is also an increasing evidence-base relating to the factors that influence how improving quality can be successfully implemented and assimilated into the routine practice of frontline clinical teams. Such work has been heavily influenced by the micro-systems focus in the work of researchers from Dartmouth-Hitchcock in the United States (18-19). There has been a traditional preference for broad, survey-based research to explore factors associated with successful quality improvement (for example the recent EU-funded MARQuIS project (20) and the work of the European Observatory on Health Systems and Policies). However, as Øvretveit and Staines (21) have pointed out: Apart from a few projects, the details of which interventions were actually made are often not presented, and there are few adequate or independent research descriptions of actual implementations of organisational and system wide programs over time. Given the paucity of in-depth studies to date, it is hardly surprising that the minutiae of quality improvement programs and processes remain largely shrouded in mystery. This is not to argue that large-scale surveys of national policies across large numbers of countries are not important; it is simply to say that without further detailed investigation of the findings of such surveys, health care leaders - whilst being aware of broad trends and directions - will remain uninformed as to the detailed how to - or implementation - of successful quality improvement at the hospital level. The predominant focus in the majority of studies in healthcare quality has been solely on technical factors that are thought to influence the quality of care (despite the socio- 6
8 technical systems perspective in which information technology and deeper, cultural processes are studied symmetrically). As a consequence it has been all too easy to forget (or simply fail to acknowledge) the fact that every aspect of care is accomplished through people in their everyday actions and interactions with and for each other - a social process. If quality is viewed in this way issues such as identity, politics, leadership, value systems, organisational slack, and learning, can begin to receive the same attention as the technical factors that have dominated the research field to date. Furthermore, most studies have rarely taken the time to construct theories or explanations for what they observe or find in their analyses (22). This is particularly true of the organisational and cultural dimensions of quality improvement. Unfortunately the existing evidence-base has also been less adept at shedding light on how factors at different levels of a healthcare system relate to one another, and how in practice hospitals should go about influencing and setting key success factors in motion. The European Union-funded QUASER study will seek to extend recent research that has addressed these theoretical and methodological issues. Bate, Mendel and Robert (17) undertook a three-year international study that was explicitly designed to help practitioners and researchers understand the factors and processes that enable hospitals in the US and Europe (England and the Netherlands) to achieve - and sustain - high quality services for their patients. This original study took as its starting point that whilst technical factors, such as information systems, do play a major role in accounting for the quality gap, organisational and cultural factors are crucial in understanding how quality and safety improvement occurs. 7
9 Based on in-depth, multi-level case studies of seven leading hospital, this research found that high-performing hospitals were able to achieve, and then sustain, high levels of quality because they recognised and had been extremely successful in addressing - on an ongoing basis - six common challenges. The six common challenges that were identified from the case studies were: 1. structural - organising, planning and co-ordinating quality efforts 2. political - addressing and dealing with the politics of change surrounding any QI effort 3. cultural - giving quality a shared, collective meaning, value and significance within the organisation 4. educational - creating a learning process that supports improvement 5. emotional - engaging and mobilizing people by linking QI efforts to inner sentiments and deeper commitments and beliefs 6. physical and technological - the designing of physical systems and technological infrastructure that supports and sustains quality efforts The researchers represented these common challenges by means of a codebook which took the form of a checklist that practitioners can use to identify where the organisational gaps in their local improvement efforts may lie and what they may need to do to address them. Based on the systematic review and coding of the organisational case studies, multiple illustrations of the different types of challenges and solutions were extracted from the individual case study narratives and assigned to the different challenges. In total, the 8
10 codebook includes 56 such solutions spread across the six challenges, all derived inductively from the organisational cases themselves. The QUASER study will extend and apply this original research in several important ways: by studying a range of hospitals at different stages on their quality journeys (as opposed to just high performing hospitals) by explicitly including clinical effectiveness, patient safety and patient experience as key components of what we mean by quality (as opposed to focusing just on service improvement) by incorporating available qualitative and quantitative measures of quality into a crosscase, comparative analysis (as opposed to a purely qualitative analysis) by including a much broader range of countries (England, the Netherlands, Norway, Portugal and Sweden) by providing context-specific guidance to (a) hospitals depending on where they are on their quality journey, and (b) payers and those assessing the quality of hospital care Finally, given that each of the macro (national healthcare system), meso (hospital) and micro (frontline clinical team) levels, separately and in interaction with each other, affects clinical effectiveness, patient safety and patient experience the QUASER study will retain a particular focus on the dynamics and interactions between these different levels (23-25) as possible key determinants of sustained quality in healthcare. A favourable ethical opinion for this research study was granted by NRES Committee South East Coast - Surrey in April 2011, REC reference: 11/LO/
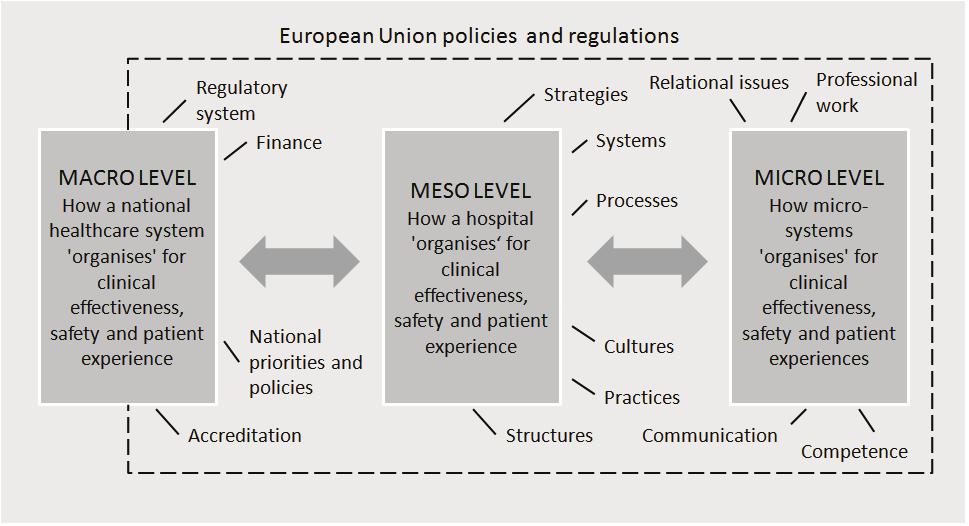
11 METHODS/DESIGN Organisational case studies are a preferred research method within complex and dynamic contexts where it is difficult to isolate variables or where there are strong interactions between variables (26). The case study can generate hypotheses from exploratory data which can then be tested in wider samples using different methods, and - particularly relevant to the aims of the QUASER project - they address questions of process as opposed to the input/output model of much quantitative research. Process research is characterised by the dynamic study of behaviour within organisations, focusing on organisational context, activity and actions which unfold over time (27-28). The comparative design we will adopt will allow pattern recognition across the 10 hospitals in order to generate generic as well as issue-specific learning. Fieldwork will be undertaken in two hospitals in each of the five EU partner countries (England, the Netherlands, Norway, Portugal and Sweden) making a total of ten hospitals, over a period of 12 months. The countries were chosen as they represent variation in the important aspects of healthcare that we want to capture; for example, differences in the way that healthcare services are funded, and in the way that progress had been made in each country on their quality journey. Data collection and analysis will be standardised across all case study sites using an agreed framework. A central feature of the project is to study quality from a multi-level perspective (23-25) incorporating three levels: macro (national healthcare system), meso (hospital) and micro (frontline clinical team) (see figure 1). 10
12 [INSERT FIGURE 1 A MULTI-LEVEL PERSPECTIVE TO STUDY QUALITY] At the meso level all ten hospitals will be studied. At the micro level we will select one hospital in each country and study processes in two clinical micro systems. There will therefore be a total of ten micro system case studies within five hospitals. The rationale for studying two micro systems in a single hospital is to compare the relative influence of macro, meso and micro level processes on quality and to understand how macro and meso level processes are mediated at the micro system level. Selection of case study hospitals A simple and easily communicable selection process has been developed that can be applied in each of the five participating countries to select two hospitals that appear from available indicators to be at different stages of the quality journey, with the final selection also informed by using national accreditation, regulation or similar measures in each country. For our research purposes: the hospitals included must be general hospitals, that is, they must include a mix of general medicine and general surgical services, admitting both emergency and planned cases the hospitals may be teaching hospitals but in our final selection we will aim to ensure that there are both teaching and non-teaching hospitals 11
13 the hospitals must provide maternity services (as this micro-system will be part of the research in one of the hospitals in each country). The intention is to select hospitals similar in size; in particular we wish to exclude outliers, for example very large or very small hospitals - in order to be able to recognise the variation that exists between partner countries. The following information about the shortlisted hospitals in each country will therefore also be considered as part of the selection process: number of beds number of staff types of services provided type of population served (city, town or rural) Throughout the selection process we will document the reasons for selecting the process and outcome measures in each country, the sources of data used and the evidence or criteria used to determine the robustness of the data. Fieldwork The following fieldwork (see figure 2) will be undertaken over a 12-month period in each of the five European countries. [INSERT FIGURE 2 PROTOCOL FOR FIELDWORK] Macro-system 12
14 At the macro level the aim is to understand how broader socio-political influences impact on healthcare quality at the meso and micro level and, in turn, how these are influenced by developments in meso and micro practices. We will draw on existing data in each country. Seven categories of macro level influences on healthcare quality have been identified as shown in figure 2. Prior to the fieldwork discussed in detail below each partner country will prepare a structured analysis of the macro-system level, based on these categories, in which the hospital case study sites in their countries are operating. Meso- system Ten acute hospitals in five EU countries (two from each of the five participating countries) will be invited to participate. In all of the participating hospitals the meso-systems will be studied. At an early stage of engagement with each of the hospitals the national research teams will identify a site captain or contact (usually a member of the senior management team) who will be able and prepared to assist with introducing the research to relevant staff and advising the research team throughout the study. At the meso-level the aim is to understand organisation-wide structures and processes for managing quality and the complexities of implementing quality improvement programmes. In each of the ten participating hospitals the fieldwork is expected to comprise: at least ten semi-structured, audio-recorded interviews with senior/middle managers at the beginning of the fieldwork; staff interviewees will be identified initially through discussions with the site captain in each hospital and then a snowballing approach will be used, as necessary 13
15 observation of key meetings/events throughout the duration of the fieldwork the longitudinal study of a tracer quality improvement project or programme (through staff interviews and/or focus groups, non-participant observation of relevant project events/meetings, shadowing of staff and documentary analysis); in one of the two hospitals in each country this tracer project will relate to healthcare acquired infections to enable cross-case analysis between the five countries at least ten semi-structured interviews with senior/middle managers at end of fieldwork; these interviews will focus on reflecting back the emerging findings from the fieldwork and seeking the views of the interviewees as to the validity of these. using available routinely collected quantitative data indicating hospital quality to assess where the hospital is on its quality journey and help us to understand the relationship between organisational factors and quality. The semi-structured interview schedule will cover topics such as: historical context: the story so far in this hospital with regard to quality current quality improvement initiatives how quality is organised the quality strategy supporting frontline staff supported in terms of quality improvement measuring quality sharing good practice across professional and clinical boundaries 14
16 education, training and development programmes external environment and wider networks (regulators, payers). One practical objective of the meso-system interviews will be to identify the formal organisational structure and systems for managing quality in the hospital. As well as the interviews themselves researchers will also seek to collate any relevant documentation (organisational charts, annual reports, quality strategies, routinely available data on quality etc). From this information the research teams will identify key committees, meetings and events at which to conduct non-participant observation throughout the remaining period of the fieldwork. Fieldnotes will be taken at all meetings that are observed and the research teams will be focusing on providing rich, longitudinal insights into the overall research questions. Through the meso-system interviews each national research team will also identify a tracer quality improvement project or programme in each of the two hospitals they are studying. In one of the hospitals in each country this tracer project will relate to healthcare acquired infections. The other project may relate to any (or all) of the three components of the QUASER study definition of quality: clinical effectiveness, patient safety and patient experience. The project executive will ensure that - across the ten hospitals - there are exemplars of projects relating to all three components of our definition of quality. The tracer project or programme will ideally be: about to start or be in the early stages of implementation being implemented in more than one clinical micro-system or service have an identified project manager/lead who is able to facilitate research access 15
17 a formal part of the hospitals ongoing quality improvement strategy planned to be completed at or after the end of the fieldwork. The tracer projects will then be studied longitudinally during the remainder of the fieldwork through a combination of semi-structured interview schedules, documentary analysis, focus groups with staff, shadowing of staff and/or non-participant observation of key events/project meetings, with the latter again focusing on providing longitudinal insights into the overall research question. Fieldwork relating to the tracer projects may be undertaken at all levels of the hospitals as appropriate (and may overlap with the fieldwork in the selected microsystems in one of the hospitals in each country). This aspect of the fieldwork (and during the study of the selected micro-systems in one of the hospitals) may include shadowing key staff for agreed periods of time (e.g. a shift). It is not the purpose of the QUASER study to formally evaluate the success or otherwise of the tracer projects but rather to study them - in real time - as exemplars of how quality/quality improvement is implemented to enable lessons to be drawn from across the ten case studies. The meso-system interviews will also inform the selection of the second clinical microsystem - in addition to maternity services - in one of the hospitals in each partner country. All interviews will be conducted and transcribed in the native language of each partner country. English written summaries will be shared in the group of researchers, to enable the exchange of findings. Micro-system At the micro-system level the aim is to understand the influence of local factors on quality in two clinical micro systems in one hospital in each of the five participating EU countries. It is 16
18 proposed that maternity care is one of the micro systems selected as it is high on the agenda of quality and safety improvement efforts in all participating countries and therefore data rich. The other clinical micro system will be selected when the maternity case study is underway or completed. The aim is to select a micro system that will contrast with maternity on its quality journey and allow us to study the differing effects of meso level influences at the micro level. We are particularly interested in how meso level initiatives are implemented at the local level, practitioner s acceptance and perceptions of those initiatives and how such initiatives are shaped and adapted by frontline staff. We are also interested in initiatives that originate at the micro level without prompting from the meso or macro levels and how this occurs. Local leaders and champions of quality and their perceptions of the receptiveness of the meso level of the organisation to quality improvement will be a particular focus of our investigation. The focus will be on the interaction between the macro, meso and micro levels and how processes at either level can either facilitate or hinder quality improvement efforts. We will be introduced to the leaders (clinical and managerial) of each of the chosen microsystems by the Phase I site captains (typically a member of the senior management team) we will have worked with in each of the hospitals; the site captain will be asked to assist the research team in arranging initial meetings with micro-system leaders. We will explain the aims and methods of the proposed research to the micro-system leaders, seek to answer any questions they may have about the proposed methods and value of the research, and explain how the findings will be fed back to them and their organisation. As with the meso- 17
19 system fieldwork we would anticipate each research team conducting exit interviews with leaders of the two micro-systems towards the end of the 12-month period of fieldwork. Overall, we will spend a minimum of six months working in each of the two microsystems using a multi-method approach; data collection will include a minimum of 15 face-to-face interviews, observations of organisational processes and documentary analysis. Routinely collected quantitative data will be obtained to indicate quality. The semi-structured interview schedule at the micro-system level will cover the following broad topics: what it is like to work in this unit/micro-system? team and multi-disciplinary working culture, mindsets and outlooks relationships/collaboration outside unit and hospital leaders and leadership styles interactions with meso- and macro-systems role of information/ information technology definitions of quality the use of guides and guidance In some of the case studies it may be more appropriate to undertake focus groups with frontline staff; these would largely be structured around the same set of questions as in the face-to-face interviews. Identification and recruitment of research participants 18
20 Interviewees will be identified through discussions with the site captain but will include at the meso-system level the Chief Executive, Director of Clinical Governance, Director of Nursing, and Director of Operations. Staff members who fulfil key roles in managing quality improvement programmes as well as staff in the selected microsystems will also be included. An with a covering letter, staff information sheet, and outline of the semi structured interview schedule to be used will be sent to each potential interviewee at least 2 weeks prior to the date of the proposed interview. Potential interviewees will be asked to confirm their willingness to participate by return . The staff information sheet and covering letter both make clear that participation is entirely voluntary. As described above, if appropriate, focus groups with small numbers of frontline staff (up to 8) will be held to supplement or replace the staff interviews at the microsystem level. As with the interviews an with a covering letter, staff information sheet, and outline of the themes to be discussed at the focus group (as based on the semi structured interview schedule) will be sent to each potential participant at least 2 weeks prior to the date of the proposed focus group. Potential participants will be asked to confirm their willingness to participate by return . The staff information sheet and covering letter both make clear that participation is entirely voluntary. Staff interviewees at the meso and microsystem levels may also be identified through their attendance and participation in events and meetings relating to quality improvement where non-participant ethnographic observation will be undertaken. Additionally, shadowing of staff in appropriate settings depending on the specific microsystem will take place as agreed with the staff member; the presence of the researcher will be renegotiated on a daily basis with both staff and patients. Staff who are invited to agree to be shadowed for an fixed 19
21 period of time will be identified through nonparticipant observation at meetings/key events using a purposive sampling approach. An with a covering letter and staff information sheet will be sent to each potential staff member to be shadowed at least 2 weeks prior to the date of the proposed shadowing. Potential staff to be shadowed will be asked to confirm their willingness to participate by return . The participant information sheet and covering letter both make clear that participation is entirely voluntary. DISCUSSION Building on earlier findings from Bate et al (17), the meso and micro-system fieldwork - as well as the analysis of the macro-system - will seek to answer the following questions: how is QI structured, planned and co-ordinated? how is quality built into hospitals? how are the politics of change negotiated? how are shared understandings & commitment to quality built? how do staff learn about quality and quality improvement? how are individual and collective enthusiasm for quality and quality improvement engendered and supported? how is the physical, informational, social and technological infrastructure used to support quality and quality improvement? what are the respective roles of the macro-, meso- and micro-system levels in terms of (a) the successful implementation and spread of quality improvement, and (b) sustained quality? 20
22 Data analysis Our approach to data collection and analysis will be to use a preliminary theoretical framework (29) rather than a purely grounded theory (30), so that data analysis is a combination of induction (data-driven generalisation) and deduction (theory-driven exploration of hypotheses) (27). This approach has been used previously by the team in organisational research (31). We want to try to understand at a deep level the kind of processes that enable hospitals in Europe to achieve quality improvement; what is it that enables them to achieve excellence (as perceived by their patients and peers and supported by clinical and performance data), and what enables them to continually improve their services over considerable periods of time. Validity and reliability Regular meetings of the research teams from each of the partner countries will provide opportunities to discuss and refine the protocol during the course of the fieldwork but it is also anticipated that research teams will be in regular contact in the periods between these meetings to share lessons and discuss any problems that may arise. This will ensure that the fieldwork conducted in the different countries is consistent and reliable. Ongoing discussions amongst researchers and a wider advisory board will provide opportunities for reflexivity and the development of insights into the effect of context on quality improvement. Generalisability In addition to the fieldwork described above the development of the outputs arising from the study (a Quality & Safety Guide for Hospitals and a Framework for Assessing Hospital 21
23 Quality) will be informed by a parallel process of translational workshops involving both hospitals and payers in a wider stakeholder group from a broader range of European countries. These stakeholders will attend three translational workshops during the course of the project ensuring that issues facing hospitals across the EU will be considered and that the eventual outputs of the project have been designed for the needs of users across the EU. The stakeholders will review progress and ensure that the lessons and findings from the research are going to be relevant and of use to them; they will also provide input on how the materials/tools that are ultimately designed may need to be customised for their particular national contexts. 22
24 LIST OF ABBREVIATIONS EU: European Union; QUASER: Quality and Safety in Europe by Research; QI: Quality Improvement. COMPETING INTERESTS The authors declare that they have no competing interests. AUTHORS CONTRIBUTIONS GR jointly drafted the original proposal, prepared the meso and micro-system fieldwork protocol, and drafted this paper; JA, NF & SB jointly drafted the original proposal and commented on the meso and micro-system fieldwork protocol (JA also prepared the macrosystem framework and parallel stakeholder process that will inform the development of outputs from the project; NF is principal investigator for the study; SB led the hospital selection process); KA, B A-G, RB, JC, FN, A-M W, & CV all commented on the fieldwork protocol and macro-system framework, and contributed to the design of the hospital selection process to be applied in their respective countries. All authors read and approved the final manuscript. ACKNOWLEDGEMENTS AND FUNDING The study Quality and Safety in European Union Hospitals: A Research-based Guide for Implementing Best Practice and a Framework for Assessing Performance (QUASER) has received funding from the European Community's Seventh Framework Programme (FP7/ ) under grant agreement n
25 We wish to acknowledge the following members of the QUASER project: Lisbeth Hoeg- Jensen, Heidi Poestges and Anna Renz, England; Julia Quartz and Hester van de Bovenkam, the Netherlands; Siri Wiig and Christian von Plessen, Norway; Sara Gomes and Alexandra Fernandes, Portugal; Pär Höglund, Tony Andersson, Anette Karltun and Johan Sanne, Sweden. REFERENCES 1. Boaden, R., Harvey, G., Moxham, C. & Proudlove, N. (2008). Quality improvement: Theory and practice in healthcare. Warwick; NHS Institute for Innovation and Improvement. 2. Walshe, K. (2009) Pseudo innovation: the development and spread of healthcare quality improvement methodologies. International Journal for Quality in Healthcare, 21(3): IOM (Institute of Medicine). To Err is Human: building a safer healthcare system. Kohn LT, Corrigan, Donaldson MS, editors. Washington, DC: The National Academies Press; IOM (Institute of Medicine). Crossing the Quality Chasm: a new health system for the twenty-first century. Washington, DC: The National Academies Press; West, E. (2000). Organisational sources of safety and danger: Sociological contributions to the study of adverse events. Quality in Health Care, 9: Firth-Cozens, J. (2001). Cultures for improving patient safety through learning: The role of teamwork. Quality and Safety in Health Care, 13 (Suppl 2): ii3-ii9. 7. Catino, M., Albolini, S., & Vannucci, A. (2005). An organizational multi-level model for the analysis of failures in medicine The case of fortuitous connection. In: R Tartaglia, S Bagnara, T Bellandi and S Albolino (eds.) Healthcare Systems Ergonomics and Patient Safety: Proceedings on the International Conference on Healthcare Systems Ergonomics and Patient Safety (HEPS 2005), Florence, Italy, 30 March-2 April London; Taylor & Francis 8. Lukas, CvD., Holmes, SK., Cohen AB., et al. (2007) Transformational change in healthcare systems: an organisational model. Health Care Management Review, 32(4):
26 9. Curry LA, Spatz E, Cherlin E et al. (2011) What Distinguishes Top-Performing Hospitals in Acute Myocardial Infarction Mortality Rates?: A Qualitative Study. Ann Intern Med, 154: Bevan, H., Ham, C. & Plsek, P. (2008). The next leg of the journey: how do we make High Quality Care for All a reality? NHS Institute for Innovation & Improvement; Warwick 11.Shipton, H., Armstrong, C., West, M. & Dawson, J. (2008). The impact of leadership and quality climate on hospital performance. International journal for quality in health care, 20, Singer, S., Meterko M, Baker, L et al. (2007) Workforce perceptions of hospital safety culture: development and validation of the patient safety climate in health care organisations survey. Health Services Research, 42(5): Hartmann CW, Rosen AK, Meterko M et al. (2008) An overview of patient safety climate in the VA. Health Services Research, 43(4): Shortell SM, Marsteller JA, Lin M et al. (2004) The role of perceived team effectiveness in improving chornic illness care. Medical Care, 42(11): Broer, Tineke, Anna Nieboer, and Roland Bal Opening the black box of quality improvement collaboratives: an actor-network theory approach. BMC Health Services Research 10 (265). 16 Strating, Mathilde, Anna Nieboer, Teun Zuiderent-Jerak, and Roland Bal Creating effective quality improvement collaboratives: a multiple case study. BMJ Quality and Safety:early view: Bate, S.P., Mendel, P., & Robert, G. (2008) Organising for Quality, The improvement journeys of leading hospitals in Europe and the United States. Oxford: Radcliffe Publishing 18.Batalden PB, Godfrey MM, Nelson EC. (2007) Quality by design: a clinical micro-system approach. New York: Wiley. 19.Batalden PB, Nelson EC, Mohr JJ et al. (2003) Micro-systems in healthcare: part 5. How leaders are leading. Joint Commission Journal on Quality & Safety, 29(6): Spencer, E & Walshe, K. (2006) Deliverable 6. Healthcare quality strategies in Europe. A survey of quality improvement policies and strategies in healthcare systems of member states of the European Union. Centre for Public Policy & Management, University of Manchester; Manchester 25
27 21.Øvretveit J, & Staines A. (2007). Sustained improvement? Findings from an independent case study of the Jönköping quality programme. Quality Management in Healthcare, 16(1): Grol, RPTM., Bosch, MC, Hulscher, MEJL, Eccles, MP., & Wensing, M. (2007) Planning and studying improvement in patient care: the use of theoretical perspectives. Milbank Quarterly, 85(1): House R, Rousseau DM, Thomas-Hunt M. (1995) The meso-paradigm: a framework for the integration of micro and macro organizational behaviour. Research in organizational Behaviour, 17: Rousseau, DM. (2011) Reinforcing the micro/macro bridge: organisational thinking and pluralistic vehicles. Journal of Management, 37(2): Hitt, MA, Beamish PW, Jackson SE and Mathieu, JE. (2007) Building theoretical and empirical bridges across levels: multilevel research in management. Academy of Management Journal, 50(5): Yin, R. (1994). Case study research. Design and methods. UK: Sage 27.Pettigrew, A. (1990). Longitudinal field research on change: Theory and practice. Organization Science, 1, Langley, A. (1999) Strategies for theorising from process data. Academy of Management Review, 24(4): Miles, M.D. (1979). Qualitative data as an attractive nuisance The problem of analysis. Administrative Science Quarterly, 24, Glaser, B. & Strauss, A. (1967). The discovery of grounded theory. Chicago: Aldine. 31.Fulop N, Protopsaltis G, King A, Allen P, Hutchings A. & Normand C (2005). Changing organisations: a study of the context and processes of mergers of health care providers in England. Social Science and Medicine (6)
28 LIST OF FIGURES FIGURE 1 FIGURE 2 A MULTI-LEVEL PERSPECTIVE TO STUDY QUALITY PROTOCOL FOR FIELDWORK 27
29 Figure 1
30 0 ΦΥΡ ς ςωηπ ΟΗΨΗΟ )Υ ΠΗΖΡΥΝ ΙΡΥ ΓΗςΦΥΛΕΛΘϑ Π ΦΥΡ ΟΗΨΗΟ ΦΡΘΩΗ[Ω ΘΓ ΚΡΖ ΩΚΛς ΛΘΙΟΞΗΘΦΗς ΩΚΗ ΡΥϑ ΘΛς ΩΛΡΘ Ο Π Θ ϑηπηθω ΡΙ ΤΞ ΟΛΩ ΛΘ ΚΡςΣΛΩ Ος ΛΘ Η ΦΚ ΦΡΞΘΩΥ ΚΗ ΟΩΚΦ ΥΗ ΦΡΘΩΗ[Ω ΙΞΘΓΛΘϑ ΘΓ ΦΦΗςς ΥΗϑΞΟ ΩΡΥ ΙΥ ΠΗΖΡΥΝ ΦΦΥΗΓΛΩ ΩΛΡΘ ΘΓ ΠΡΘΛΩΡΥΛΘϑ ΛΘΙΡΥΠ ΩΛΡΘ Ψ ΛΟ ΕΛΟΛΩ ΥΗςΡΞΥΦΗς Ψ ΛΟ ΕΟΗ Σ ΩΛΗΘΩ ΥΛϑΚΩς 0ΗςΡ ΘΓ ΠΛΦΥΡ ς ςωηπς 0ΗςΡ ΘΓ ΠΛΦΥΡ ς ςωηπ ΟΗΨΗΟς +ΡςΣΛΩ Ος ΘΓ 0ΗςΡ ς ςωηπ /ΡΘϑΛΩΞΓΛΘ Ο ςωξγ ΡΙ ΩΥ ΦΗΥ 4, ΣΥΡΜΗΦΩ ΣΥΡΦΗςςΗς Ε ΖΚΛΦΚ ΦΟΛΘΛΦ Ο ΗΙΙΗΦΩΛΨΗΘΗςς Σ ΩΛΗΘΩ ς ΙΗΩ ΘΓ ΡΥ Σ ΩΛΗΘΩ Η[ΣΗΥΛΗΘΦΗ ΥΗ Π Θ ϑηγ ΘΓ ΡΥϑ ΘΛςΗΓ ΘΓ ΣΟ ΡΞΩ ΡΨΗΥ ΩΛΠΗ ςηθλρυ ςω ΙΙ ΛΘΩΗΥΨΛΗΖς 1ΡΘ Σ ΥΩΛΦΛΣ ΘΩ ΡΕςΗΥΨ ΩΛΡΘ ΡΙ ΝΗ ΠΗΗΩΛΘϑς ΘΓ ΗΨΗΘΩς Π Σ ΝΗ ΦΡΠΠΛΩΩΗΗς 4, ςωυξφωξυης ΗΩΦ 6ΗΠΛ ςωυξφωξυηγ ΛΘΩΗΥΨΛΗΖς ςκ ΓΡΖΛΘϑ ΡΙ ςω ΙΙ ΙΡΦΞς ϑυρξσς ± Ω ΟΟ ΟΗΨΗΟς ΡΙ ΚΡςΣΛΩ Ο 4Ξ ΟΛΩ ΘΓ ΣΗΥΙΡΥΠ ΘΦΗ Γ Ω ± ΦΡΟΟ ΩΗ ςηφρθγ Υ Θ Ο ςλς ςηθλρυ ςω ΙΙ ΛΘΩΗΥΨΛΗΖς ΡΦΞΠΗΘΩ Υ Θ Ο ςλς,γηθωλι ΚΡΖ ΠΗςΡ ΟΗΨΗΟ ΛΘΩΗΥ ΦΩς ΖΛΩΚ ΠΛΦΥΡ ς ςωηπ ΟΗΨΗΟ ΩΡ ΛΘΙΟΞΗΘΦΗ ΦΟΛΘΛΦ Ο ΗΙΙΗΦΩΛΨΗΘΗςς Σ ΩΛΗΘΩ ς ΙΗΩ ΘΓ Σ ΩΛΗΘΩ Η[ΣΗΥΛΗΘΦΗ Ω ΙΥΡΘΩΟΛΘΗ +ΡςΣΛΩ Ο 6ΩΞΓ ΡΙ ΩΖΡ ςσηφλιλφ ΠΛΦΥΡ ς ςωηπς 0 ΩΗΥΘΛΩ 1ΡΘ Σ ΥΩΛΦΛΣ ΘΩ ΡΕςΗΥΨ ΩΛΡΘ ΡΙ ΝΗ ΠΗΗΩΛΘϑς ΘΓ ΗΨΗΘΩς ςηπλ ςωυξφωξυηγ ΛΘΩΗΥΨΛΗΖς ± ςω ΙΙ 0ΛΦΥΡ ς ςωηπ 6Κ ΓΡΖΛΘϑ ΡΙ ςω ΙΙ ΘΓ ΡΥ ΙΡΦΞς ϑυρξσς 5ΡΞΩΛΘΗ Γ Ω ΡΦΞΠΗΘΩ Υ Θ Ο ςλς Θ Ο ςλς :ΥΛΩΩΗΘ ΥΗΣΡΥΩ ΡΘ ΠΞΟΩΛ ΟΗΨΗΟ Φ ςη ςωξγλης ΞςΛΘϑ ϑυηηγ ΩΗΠΣΟ ΩΗ ΘΓ ΙΥ ΠΗΖΡΥΝ ΦΥΡςς Φ ςη Θ Ο ςλς Figure 2
Approaches to quality improvement in. study
 Approaches to quality improvement in five European countries: the QUASER study Professor Naomi Fulop University College London Presentation to the Microsystem Festival, 28 th February 2014, Jönköping,
Approaches to quality improvement in five European countries: the QUASER study Professor Naomi Fulop University College London Presentation to the Microsystem Festival, 28 th February 2014, Jönköping,
QUASER The Hospital Guide. A research-based tool to reflect on and develop your quality improvement strategies Version 2 (October 2014)
") QUASER The Hospital Guide A research-based tool to reflect on and develop your quality improvement strategies Version 2 (October 2014) Funding The research leading to these results has received funding
QUASER The Hospital Guide A research-based tool to reflect on and develop your quality improvement strategies Version 2 (October 2014) Funding The research leading to these results has received funding
Quality Improvement in Health and Social Care
 Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
From Metrics to Meaning: Culture Change and Quality of Acute Hospital Care for Older People
 From Metrics to Meaning: Culture Change and Quality of Acute Hospital Care for Older People Executive summary for the National Institute for Health Research Service Delivery and Organisation programme
From Metrics to Meaning: Culture Change and Quality of Acute Hospital Care for Older People Executive summary for the National Institute for Health Research Service Delivery and Organisation programme
CHSD. Encouraging Best Practice in Residential Aged Care Program: Evaluation Framework Summary. Centre for Health Service Development
 CHSD Centre for Health Service Development Encouraging Best Practice in Residential Aged Care Program: Evaluation Framework Summary Centre for Health Service Development UNIVERSITY OF WOLLONGONG April,
CHSD Centre for Health Service Development Encouraging Best Practice in Residential Aged Care Program: Evaluation Framework Summary Centre for Health Service Development UNIVERSITY OF WOLLONGONG April,
Final Report ALL IRELAND. Palliative Care Senior Nurses Network
 Final Report ALL IRELAND Palliative Care Senior Nurses Network May 2016 FINAL REPORT Phase II All Ireland Palliative Care Senior Nurse Network Nursing Leadership Impacting Policy and Practice 1 Rationale
Final Report ALL IRELAND Palliative Care Senior Nurses Network May 2016 FINAL REPORT Phase II All Ireland Palliative Care Senior Nurse Network Nursing Leadership Impacting Policy and Practice 1 Rationale
Short Report How to do a Scoping Exercise: Continuity of Care Kathryn Ehrich, Senior Researcher/Consultant, Tavistock Institute of Human Relations.
 Short Report How to do a Scoping Exercise: Continuity of Care Kathryn Ehrich, Senior Researcher/Consultant, Tavistock Institute of Human Relations. short report George K Freeman, Professor of General Practice,
Short Report How to do a Scoping Exercise: Continuity of Care Kathryn Ehrich, Senior Researcher/Consultant, Tavistock Institute of Human Relations. short report George K Freeman, Professor of General Practice,
NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME
 NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME PROGRAMME OF RESEARCH ON ACCESS TO HEALTH CARE A Empirical studies to evaluate innovations to improve access repeat call B Empirical study of priority
NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME PROGRAMME OF RESEARCH ON ACCESS TO HEALTH CARE A Empirical studies to evaluate innovations to improve access repeat call B Empirical study of priority
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Effectively implementing multidisciplinary. population segments. A rapid review of existing evidence
 Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Volume 15 - Issue 2, Management Matrix
 Volume 15 - Issue 2, 2015 - Management Matrix Leadership in Healthcare: A Review of the Evidence Prof. Michael West ******@***lancaster.ac.uk Professor - Lancaster University Thomas West ******@***aston.ac.uk
Volume 15 - Issue 2, 2015 - Management Matrix Leadership in Healthcare: A Review of the Evidence Prof. Michael West ******@***lancaster.ac.uk Professor - Lancaster University Thomas West ******@***aston.ac.uk
Organisational factors that influence waiting times in emergency departments
 ACCESS TO HEALTH CARE NOVEMBER 2007 ResearchSummary Organisational factors that influence waiting times in emergency departments Waiting times in emergency departments are important to patients and also
ACCESS TO HEALTH CARE NOVEMBER 2007 ResearchSummary Organisational factors that influence waiting times in emergency departments Waiting times in emergency departments are important to patients and also
UWE has obtained warranties from all depositors as to their title in the material deposited and as to their right to deposit such material.
 Moule, P., Armoogum, J., Dodd, E., Donskoy, A.-L., Douglass, E., Taylor, J. and Turton, P. (2016) Practical guidance on undertaking a service evaluation. Nursing Standard, 30 (45). pp. 46-51. ISSN 0029-6570
Moule, P., Armoogum, J., Dodd, E., Donskoy, A.-L., Douglass, E., Taylor, J. and Turton, P. (2016) Practical guidance on undertaking a service evaluation. Nursing Standard, 30 (45). pp. 46-51. ISSN 0029-6570
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
School of Nursing and Midwifery. MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102)
") School of Nursing and Midwifery MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102) Programme Outline 2017 1 Programme lead Dr Ian Brown. Lecturer Primary Care Nursing 0114
School of Nursing and Midwifery MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102) Programme Outline 2017 1 Programme lead Dr Ian Brown. Lecturer Primary Care Nursing 0114
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme
 The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
Quality of Care Approach Quality assurance to drive improvement
 Quality of Care Approach Quality assurance to drive improvement December 2017 We are committed to equality and diversity. We have assessed this framework for likely impact on the nine equality protected
Quality of Care Approach Quality assurance to drive improvement December 2017 We are committed to equality and diversity. We have assessed this framework for likely impact on the nine equality protected
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Royal College of Nursing Clinical Leadership Programme. Advancing Excellence in Clinical Leadership. Clinical Leader
 Royal College of Nursing Clinical Leadership Programme Advancing Excellence in Clinical Leadership Clinical Leader Pre-programme Information Booklet January 2004 Contents Introduction Beliefs and Values
Royal College of Nursing Clinical Leadership Programme Advancing Excellence in Clinical Leadership Clinical Leader Pre-programme Information Booklet January 2004 Contents Introduction Beliefs and Values
TAMESIDE & GLOSSOP SYSTEM WIDE SELF CARE PROGRAMME
 Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
How to measure patient empowerment
 How to measure patient empowerment Jaime Correia de Sousa Horizonte Family Health Unit Matosinhos Health Centre - Portugal Health Sciences School (ECS) University of Minho, Braga Portugal Aims At the
How to measure patient empowerment Jaime Correia de Sousa Horizonte Family Health Unit Matosinhos Health Centre - Portugal Health Sciences School (ECS) University of Minho, Braga Portugal Aims At the
Clinical audit: a guide
 Clinical audit: a guide All nurses are expected to take part in clinical audits. Stephen Ashmore and Tracy Ruthven explain how it should be done HEALTHCARE PROFESSIONALS across the NHS are being encouraged
Clinical audit: a guide All nurses are expected to take part in clinical audits. Stephen Ashmore and Tracy Ruthven explain how it should be done HEALTHCARE PROFESSIONALS across the NHS are being encouraged
Innovating for Improvement
 Innovating for Improvement Call for applications Round 3 July 2015 The Health Foundation Tel 020 7257 8000 www.health.org.uk CONTENTS 1. About the Health Foundation 3 2. Introduction to Innovating for
Innovating for Improvement Call for applications Round 3 July 2015 The Health Foundation Tel 020 7257 8000 www.health.org.uk CONTENTS 1. About the Health Foundation 3 2. Introduction to Innovating for
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS
 INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
6 TH CALL FOR PROPOSALS: FREQUENTLY ASKED QUESTIONS
 6 TH CALL FOR PROPOSALS: FREQUENTLY ASKED QUESTIONS MARCH 2018 Below are some of the most common questions asked concerning the R2HC Calls for Proposals. Please check this list of questions before contacting
6 TH CALL FOR PROPOSALS: FREQUENTLY ASKED QUESTIONS MARCH 2018 Below are some of the most common questions asked concerning the R2HC Calls for Proposals. Please check this list of questions before contacting
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ)
") Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ) Author: Secondary Care Analysis (PROMs), NHS Digital Responsible Statistician: Jane Winter 1 Copyright 2016 Health and Social Care
Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ) Author: Secondary Care Analysis (PROMs), NHS Digital Responsible Statistician: Jane Winter 1 Copyright 2016 Health and Social Care
Knowledge and Skills for. Government response to the Consultation on the Knowledge and Skills Statement for. Social Workers in Adult Services
 Knowledge and Skills for Social Workers in Adult Services Government response to the Consultation on the Knowledge and Skills Statement for Social Workers in Adult Services March 2015 Title: Government
Knowledge and Skills for Social Workers in Adult Services Government response to the Consultation on the Knowledge and Skills Statement for Social Workers in Adult Services March 2015 Title: Government
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY
 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1
 EVALUATION Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1 Research Summary No. 9 March 2012 Introduction The current model of primary care in the United States is
EVALUATION Assessing and Increasing Readiness for Patient-Centered Medical Home Implementation 1 Research Summary No. 9 March 2012 Introduction The current model of primary care in the United States is
Rutgers School of Nursing-Camden
 Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
Nursing skill mix and staffing levels for safe patient care
 EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
CALL FOR PROPOSALS FOR THE CREATION OF UP TO 25 TRANSFER NETWORKS
 Terms of reference CALL FOR PROPOSALS FOR THE CREATION OF UP TO 25 TRANSFER NETWORKS Open 15 September 2017 10 January 2018 September 2017 1 TABLE OF CONTENT SECTION 1 - ABOUT URBACT III & TRANSNATIONAL
Terms of reference CALL FOR PROPOSALS FOR THE CREATION OF UP TO 25 TRANSFER NETWORKS Open 15 September 2017 10 January 2018 September 2017 1 TABLE OF CONTENT SECTION 1 - ABOUT URBACT III & TRANSNATIONAL
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
Federica Favalli, Antonello Zangrandi. University of Parma, Parma, Italy. Andrea Francesconi. University of Trento, Trento, Italy.
 Economics World, Mar.-Apr. 2017, Vol. 5, No. 2, 154-163 doi: 10.17265/2328-7144/2017.02.008 D DAVID PUBLISHING Physicians and Managers Approach to Quality Experience in Italian Hospitals Federica Favalli,
Economics World, Mar.-Apr. 2017, Vol. 5, No. 2, 154-163 doi: 10.17265/2328-7144/2017.02.008 D DAVID PUBLISHING Physicians and Managers Approach to Quality Experience in Italian Hospitals Federica Favalli,
The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus
 University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Leadership and Better Patient Care: Managing in the NHS
 Leadership and Better Patient Care: Managing in the NHS Executive Summary Professor Paula Nicolson 1, Ms. Emma Rowland 2, Dr. Paula Lokman 1, Dr. Rebekah Fox 3, Professor Yiannis Gabriel 4, Dr. Kristin
Leadership and Better Patient Care: Managing in the NHS Executive Summary Professor Paula Nicolson 1, Ms. Emma Rowland 2, Dr. Paula Lokman 1, Dr. Rebekah Fox 3, Professor Yiannis Gabriel 4, Dr. Kristin
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Understanding Patient Safety
 Understanding Patient Safety Understanding Patient Safety edited by Lynne Currie iii Quay Books Division, MA Healthcare Ltd, St Jude s Church, Dulwich Road, London SE24 0PB British Library Cataloguing-in-Publication
Understanding Patient Safety Understanding Patient Safety edited by Lynne Currie iii Quay Books Division, MA Healthcare Ltd, St Jude s Church, Dulwich Road, London SE24 0PB British Library Cataloguing-in-Publication
The allied health professions and health promotion: a systematic literature review and narrative synthesis
 The allied health professions and health promotion: a systematic literature review and narrative synthesis Justin Needle 1, Roland Petchey 1, Julie Benson 1, Angela Scriven 2, John Lawrenson 1 and Katerina
The allied health professions and health promotion: a systematic literature review and narrative synthesis Justin Needle 1, Roland Petchey 1, Julie Benson 1, Angela Scriven 2, John Lawrenson 1 and Katerina
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Innovating for Improvement
 Call for applications June 2018 Call for applications Innovating for Improvement Round 7: Supporting the workforce Contents The Health Foundation 3 1 The programme an introduction to Innovating for Improvement
Call for applications June 2018 Call for applications Innovating for Improvement Round 7: Supporting the workforce Contents The Health Foundation 3 1 The programme an introduction to Innovating for Improvement
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Integrating quality improvement into pre-registration education
 Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
PROGRAMME SPECIFICATION KEY FACTS. Health Sciences. Part-time. Total UK credits 180 Total ECTS 90 PROGRAMME SUMMARY
 PROGRAMME SPECIFICATION KEY FACTS Programme name Award School Department or equivalent Programme code Type of study Total UK credits 180 Total ECTS 90 Health Services Research MSc Health Sciences Health
PROGRAMME SPECIFICATION KEY FACTS Programme name Award School Department or equivalent Programme code Type of study Total UK credits 180 Total ECTS 90 Health Services Research MSc Health Sciences Health
A theoretical conceptualisation of nursing practice as a complex system
 A theoretical conceptualisation of nursing practice as a complex system Lauralie Richard, Ph.D. Research Fellow General Practice and Rural Health Dunedin School of Medicine University of Otago 27 th International
A theoretical conceptualisation of nursing practice as a complex system Lauralie Richard, Ph.D. Research Fellow General Practice and Rural Health Dunedin School of Medicine University of Otago 27 th International
Consultant Radiographers Education and CPD 2013
 Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Ethical approval for national studies in Ireland: an illustration of current challenges.
 Royal College of Surgeons in Ireland e-publications@rcsi Psychology Articles Department of Psychology 1-4-2004 Ethical approval for national studies in Ireland: an illustration of current challenges. Mary
Royal College of Surgeons in Ireland e-publications@rcsi Psychology Articles Department of Psychology 1-4-2004 Ethical approval for national studies in Ireland: an illustration of current challenges. Mary
Patient Experience Strategy
 Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
Evaluation of the Threshold Assessment Grid as a means of improving access from primary care to mental health services
 Evaluation of the Threshold Assessment Grid as a means of improving access from primary care to mental health services Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation
Evaluation of the Threshold Assessment Grid as a means of improving access from primary care to mental health services Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation
EDUCATION PROGRAMME. UEFA Research Grant Programme 2018/19 edition. Regulations
 EDUCATION PROGRAMME UEFA Research Grant Programme 2018/19 edition Regulations UEFA Research Grant Programme Regulations 1. Eligibility Applicants for a grant must either: have obtained a doctorate and
EDUCATION PROGRAMME UEFA Research Grant Programme 2018/19 edition Regulations UEFA Research Grant Programme Regulations 1. Eligibility Applicants for a grant must either: have obtained a doctorate and
Physician-leaders and hospital performance: Is there an association?
 Physician-leaders and hospital performance: Is there an association? Journal of the European Association of Hospital Managers November 2011 The question of whether hospitals are better run by doctors or
Physician-leaders and hospital performance: Is there an association? Journal of the European Association of Hospital Managers November 2011 The question of whether hospitals are better run by doctors or
Standards of Proficiency for Higher Specialist Scientists
 Standards of Proficiency for Higher Specialist Scientists July 2015 Version 1.0 Review date: 31 July 2016 Contents Introduction... 3 About the Academy Register - Practitioner part... 3 Routes to registration...
Standards of Proficiency for Higher Specialist Scientists July 2015 Version 1.0 Review date: 31 July 2016 Contents Introduction... 3 About the Academy Register - Practitioner part... 3 Routes to registration...
ESRC Postdoctoral Fellowships Call specification
 Summary ESRC Postdoctoral Fellowships Call specification The Economic and Social Research Council (ESRC) is pleased to announce the introduction of a Postdoctoral Fellowship (PDF) scheme aimed at providing
Summary ESRC Postdoctoral Fellowships Call specification The Economic and Social Research Council (ESRC) is pleased to announce the introduction of a Postdoctoral Fellowship (PDF) scheme aimed at providing
Study on Organisational Changes, Skills and the Role of Leadership required by egovernment (Working title)
") Study on Organisational Changes, Skills and the Role of Leadership required by egovernment (Working title) Version 4 21/02/2005 Christine Leitner OUTLINE Background The present working plan of the EPAN
Study on Organisational Changes, Skills and the Role of Leadership required by egovernment (Working title) Version 4 21/02/2005 Christine Leitner OUTLINE Background The present working plan of the EPAN
The national Clinical Research Nurse workforce how is it structured?
 The national Clinical Research Nurse workforce how is it structured? Dr Helen Jones Head of Research Nursing Helenc.jones@nhs.net Background 1 Background Where did it all start? Development of the Clinical
The national Clinical Research Nurse workforce how is it structured? Dr Helen Jones Head of Research Nursing Helenc.jones@nhs.net Background 1 Background Where did it all start? Development of the Clinical
4 Year Patient and Public Involvement Strategy
 4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
caredata CD Full Text - copyright NISW/Social Services Research Group Mixing it in the Mixed Economy Paul Waddington
 caredata CD Full Text - copyright NISW/Social Services Research Group Mixing it in the Mixed Economy Paul Waddington Professor/Senior Research Fellow, University of Central England Abstract: The article
caredata CD Full Text - copyright NISW/Social Services Research Group Mixing it in the Mixed Economy Paul Waddington Professor/Senior Research Fellow, University of Central England Abstract: The article
BBRSC, MRC and Wellcome Trust response to the Bateson Review Recommendations. July 2011
 BBRSC, MRC and Wellcome Trust response to the Bateson Review Recommendations July 2011 Recommendation 1: The Panel noted that the processes needed to maximise scientific quality and impact are already
BBRSC, MRC and Wellcome Trust response to the Bateson Review Recommendations July 2011 Recommendation 1: The Panel noted that the processes needed to maximise scientific quality and impact are already
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
Copyright 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
 32 May 2011 Nursing Management Future of Nursing special Leadership at all levels By Tim Porter-O Grady, DM, EdD, ScD(h), FAAN This five-part editorial series examines the Institute of Medicine s (IOM)
32 May 2011 Nursing Management Future of Nursing special Leadership at all levels By Tim Porter-O Grady, DM, EdD, ScD(h), FAAN This five-part editorial series examines the Institute of Medicine s (IOM)
LEARNING FROM THE VANGUARDS:
 LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
Report on the Delphi Study to Identify Key Questions for Inclusion in the National Patient Experience Questionnaire
 Report on the Delphi Study to Identify Key Questions for Inclusion in the National Patient Experience Questionnaire Sinead Hanafin PhD December 2016 1 Acknowledgements We are grateful to all the people
Report on the Delphi Study to Identify Key Questions for Inclusion in the National Patient Experience Questionnaire Sinead Hanafin PhD December 2016 1 Acknowledgements We are grateful to all the people
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
A Maternity Network for Wales
 A Maternity Network for Wales Scoping Paper July 2013 Introduction This scoping exercise arises from a recommendation made in the Health and Social Care Committee s report One-day Inquiry into Stillbirth
A Maternity Network for Wales Scoping Paper July 2013 Introduction This scoping exercise arises from a recommendation made in the Health and Social Care Committee s report One-day Inquiry into Stillbirth
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS
 NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS Publication Gateway Reference Number: 07850 Detailed findings 3 NHS Workforce Race Equality Standard
NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS Publication Gateway Reference Number: 07850 Detailed findings 3 NHS Workforce Race Equality Standard
Report of a Scoping Exercise for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO)
") Continuity of Care Report of a Scoping Exercise for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO) Summer 2000 prepared by George Freeman and Sasha Shepperd
Continuity of Care Report of a Scoping Exercise for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO) Summer 2000 prepared by George Freeman and Sasha Shepperd
Health and Social Care White Paper (Our health, our care, our say: a new direction for community services): Implications for Local Government
: Implications for Local Government") Published 02/06 Health and Social Care White Paper (Our health, our care, our say: a new direction for community services): Implications for Local Government The Health and Social Care White Paper signals
Published 02/06 Health and Social Care White Paper (Our health, our care, our say: a new direction for community services): Implications for Local Government The Health and Social Care White Paper signals
Fulfilling lives: Supporting people with multiple and complex needs
 Fulfilling lives: Supporting people with multiple and complex needs Questions and Answers 23 July 2012 Definition of multiple and complex needs 1 What do you mean by multiple and complex needs? For this
Fulfilling lives: Supporting people with multiple and complex needs Questions and Answers 23 July 2012 Definition of multiple and complex needs 1 What do you mean by multiple and complex needs? For this
After Francis Policy Commentary
 After Francis Policy Commentary Over the last two decades, the collection and use of patient experience information has become commonplace in England s NHS and many other international health systems.
After Francis Policy Commentary Over the last two decades, the collection and use of patient experience information has become commonplace in England s NHS and many other international health systems.
PgCert/PgDip/MSc/ Continuing Professional Development
 PgCert/PgDip/MSc/ Continuing Professional Development in COMMUNITY CARE in the Glasgow School of Social Work at the Universities of Strathclyde and Glasgow Prospectus 2010 The University of Glasgow, charity
PgCert/PgDip/MSc/ Continuing Professional Development in COMMUNITY CARE in the Glasgow School of Social Work at the Universities of Strathclyde and Glasgow Prospectus 2010 The University of Glasgow, charity
Schwartz Rounds information pack for smaller organisations
 Schwartz Rounds information pack for smaller organisations Contents What is a Schwartz Round?... 2 Origins of Schwartz Rounds... 2 Format of Rounds... 3 Benefits of Rounds... 4 Staff benefits... 4 Patient
Schwartz Rounds information pack for smaller organisations Contents What is a Schwartz Round?... 2 Origins of Schwartz Rounds... 2 Format of Rounds... 3 Benefits of Rounds... 4 Staff benefits... 4 Patient
Economic Impact of the University of Edinburgh s Commercialisation Activity
 BiGGAR Economics Economic Impact of the University of Edinburgh s Commercialisation Activity A report to Edinburgh Research and Innovation 29 th May 2012 BiGGAR Economics Midlothian Innovation Centre Pentlandfield
BiGGAR Economics Economic Impact of the University of Edinburgh s Commercialisation Activity A report to Edinburgh Research and Innovation 29 th May 2012 BiGGAR Economics Midlothian Innovation Centre Pentlandfield
MSc Surgical Care Practice
 MSc Surgical Care Practice Professional Accreditation UCAS Code: Course Length: 2 Years Full-Time Start Dates: September 2015, September 2016 Department: Faculty of Health and Social Care Location: Armstrong
MSc Surgical Care Practice Professional Accreditation UCAS Code: Course Length: 2 Years Full-Time Start Dates: September 2015, September 2016 Department: Faculty of Health and Social Care Location: Armstrong
Steven Visser 1*, Henk F van der Molen 1,2, Judith K Sluiter 1 and Monique HW Frings-Dresen 1
 Visser et al. BMC Musculoskeletal Disorders 2014, 15:132 STUDY PROTOCOL Open Access Guidance strategies for a participatory ergonomic intervention to increase the use of ergonomic measures of workers in
Visser et al. BMC Musculoskeletal Disorders 2014, 15:132 STUDY PROTOCOL Open Access Guidance strategies for a participatory ergonomic intervention to increase the use of ergonomic measures of workers in
The views of public health teams working in local authorities Year 1. February 2014
 The views of public health teams working in local authorities Year 1 February 2014 Foreword One of the Royal Society for Public Health s key priorities is to support the public health workforce in its
The views of public health teams working in local authorities Year 1 February 2014 Foreword One of the Royal Society for Public Health s key priorities is to support the public health workforce in its
Study definition of CPD
 1. ABSTRACT There is widespread recognition of the importance of continuous professional development (CPD) and life-long learning (LLL) of health professionals. CPD and LLL help to ensure that professional
1. ABSTRACT There is widespread recognition of the importance of continuous professional development (CPD) and life-long learning (LLL) of health professionals. CPD and LLL help to ensure that professional
The Basic Principles of Developing Standards for Accreditation. Triona Fortune Deputy Chief Executive Officer 25 November 2014
 The Basic Principles of Developing Standards for Accreditation Triona Fortune Deputy Chief Executive Officer 25 November 2014 Overview- Standards Why? Where? Basic principles of how to write 2 3 What is
The Basic Principles of Developing Standards for Accreditation Triona Fortune Deputy Chief Executive Officer 25 November 2014 Overview- Standards Why? Where? Basic principles of how to write 2 3 What is
Quality assessment / improvement in primary care
 Quality assessment / improvement in primary care Drivers of quality Patients should receive the care they need, which is known to be effective, and in a way that does not harm them. Patients should not
Quality assessment / improvement in primary care Drivers of quality Patients should receive the care they need, which is known to be effective, and in a way that does not harm them. Patients should not
Evidence based practice and clinical leadership. Professor Bridie Kent University of Plymouth November 2017
 Evidence based practice and clinical leadership Professor Bridie Kent University of Plymouth November 2017 1 Leadership - what it means to me "The greatest leader is not necessarily the one who does the
Evidence based practice and clinical leadership Professor Bridie Kent University of Plymouth November 2017 1 Leadership - what it means to me "The greatest leader is not necessarily the one who does the
Priorities and work programme
 Priorities and work programme Purpose of report For discussion and direction. Summary This report invites members to agree the priorities for 2017/18, to note progress to date in delivering the improvement
Priorities and work programme Purpose of report For discussion and direction. Summary This report invites members to agree the priorities for 2017/18, to note progress to date in delivering the improvement
Briefing: Quality governance for housing associations
 25 March 2014 Briefing: Quality governance for housing associations Quality and clinical governance in housing, care and support services Summary of key points: This paper is designed to support housing
25 March 2014 Briefing: Quality governance for housing associations Quality and clinical governance in housing, care and support services Summary of key points: This paper is designed to support housing
ALIGN Flexible Research Fund Terms of Reference
 ALIGN Flexible Research Fund Terms of Reference The ALIGN project is inviting proposals for its inaugural Flexible Research Fund. The Fund aims to support knowledge generation and translation and learning
ALIGN Flexible Research Fund Terms of Reference The ALIGN project is inviting proposals for its inaugural Flexible Research Fund. The Fund aims to support knowledge generation and translation and learning
Transformation of Services and Care Pathway Redesign in the NHS: Further Reforms in Health Policy
 Transformation of Services and Care Pathway Redesign in the NHS: Further Reforms in Health Policy Mike Mallinson Access Partnership ISPOR May 2013 London Philadelphia Singapore Agenda Objective Approach
Transformation of Services and Care Pathway Redesign in the NHS: Further Reforms in Health Policy Mike Mallinson Access Partnership ISPOR May 2013 London Philadelphia Singapore Agenda Objective Approach
Quality Management in Medical Foundation Training: Lessons for Pharmacy
 Pharmacy Education, 2013; 13 (1): 75-81 Quality Management in Medical Foundation Training: Lessons for Pharmacy ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
Pharmacy Education, 2013; 13 (1): 75-81 Quality Management in Medical Foundation Training: Lessons for Pharmacy ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose
 Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
EVALUATION OF THE SMALL AND MEDIUM-SIZED ENTERPRISES (SMEs) ACCIDENT PREVENTION FUNDING SCHEME
 ACCIDENT PREVENTION FUNDING SCHEME") EVALUATION OF THE SMALL AND MEDIUM-SIZED ENTERPRISES (SMEs) ACCIDENT PREVENTION FUNDING SCHEME 2001-2002 EUROPEAN AGENCY FOR SAFETY AND HEALTH AT WORK EXECUTIVE SUMMARY IDOM Ingeniería y Consultoría S.A.
EVALUATION OF THE SMALL AND MEDIUM-SIZED ENTERPRISES (SMEs) ACCIDENT PREVENTION FUNDING SCHEME 2001-2002 EUROPEAN AGENCY FOR SAFETY AND HEALTH AT WORK EXECUTIVE SUMMARY IDOM Ingeniería y Consultoría S.A.
H2020 Programme. Guidelines on Open Access to Scientific Publications and Research Data in Horizon 2020
 EUROPEAN COMMISSION Directorate-General for Research & Innovation H2020 Programme Guidelines on Open Access to Scientific Publications and Research Data in Horizon 2020 Version 3.1 25 August 2016 History
EUROPEAN COMMISSION Directorate-General for Research & Innovation H2020 Programme Guidelines on Open Access to Scientific Publications and Research Data in Horizon 2020 Version 3.1 25 August 2016 History
Europe and Global Challenges 4 th Call
 Information for Applicants 78h Call for Applications Europe and Global Challenges 4 th Call Deadline 1 September 2016 Information Riksbankens Jubileumsfond www.rj.se Dr. Fredrik Lundmark Phone: +46 8 50626421
Information for Applicants 78h Call for Applications Europe and Global Challenges 4 th Call Deadline 1 September 2016 Information Riksbankens Jubileumsfond www.rj.se Dr. Fredrik Lundmark Phone: +46 8 50626421