San Francisco HICAP- Part D Intake 407 Sansome Street, 4 th Floor San Francisco, CA (Phone) (Fax) HICAP Disclosure sta
|
|
|
- Edmund Sherman
- 5 years ago
- Views:
Transcription
1
2
3
4
5
6
7
8
9
10

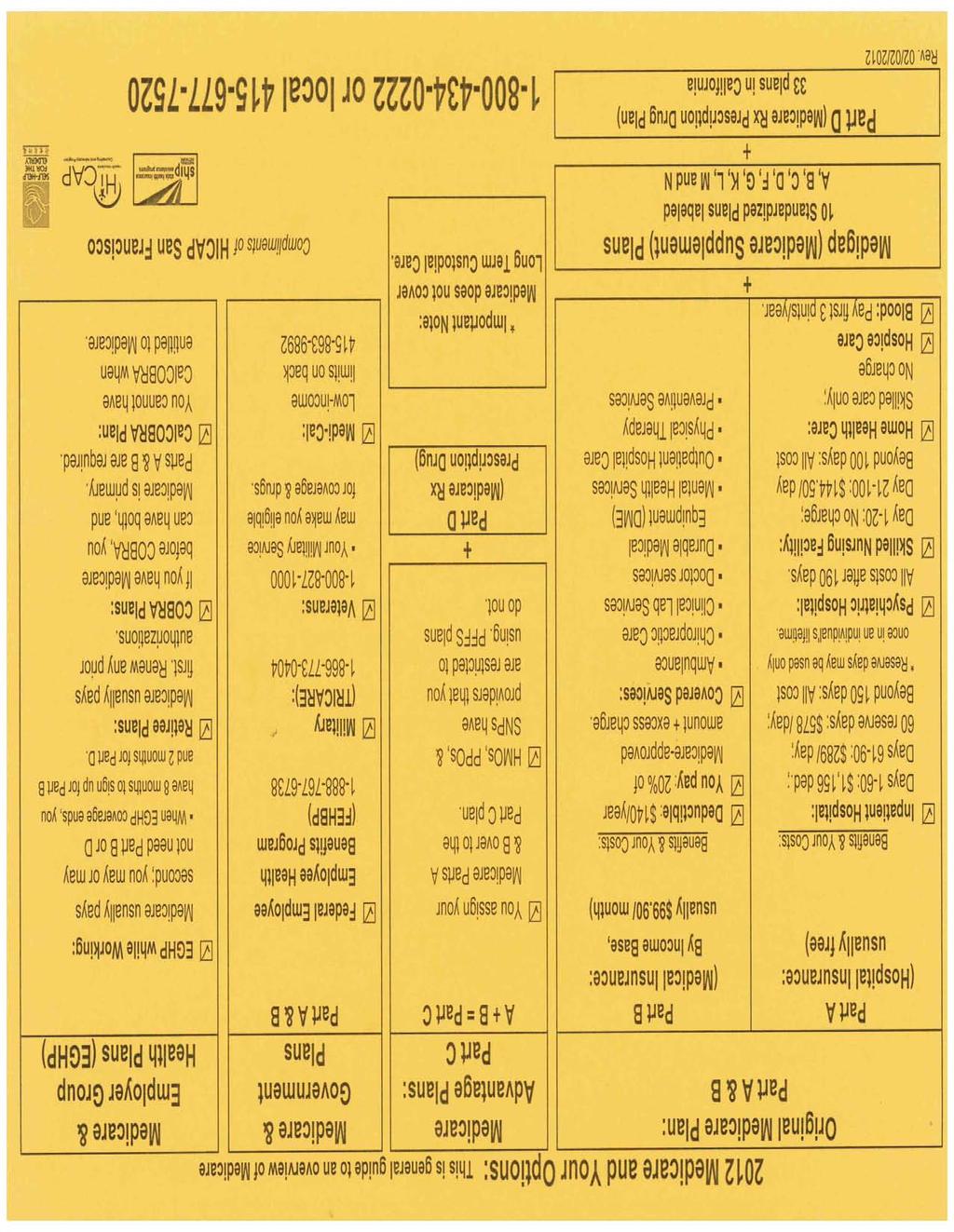
11 San Francisco HICAP- Part D Intake 407 Sansome Street, 4 th Floor San Francisco, CA (Phone) (Fax) HICAP Disclosure statement Please check box after reading HICAP counseling services are provided by Counselors registered by the California Department of Aging who are acting in good faith to provide information about health insurance policies and benefits to you, the client. Any information shall not be construed to be legal advice, and the volunteer HICAP Counselor is generally not liable for acts and omissions in providing counseling to recipients of this service. (W&I Code, Section 9541(f).) If you choose a plan and have difficulty in completing the necessary forms or process for enrollment, the HICAP Counselor will assist you. However, you will be responsible for the actual plan contract. The HICAP Counselor will NOT choose your plan for you. Name Address Phone Number Language Male Female Marital status Single Married Divorced Separated Widowed Medicare Claim # Date of Birth Part A Effective Date OR Part B Effective Date I do not have Part A.
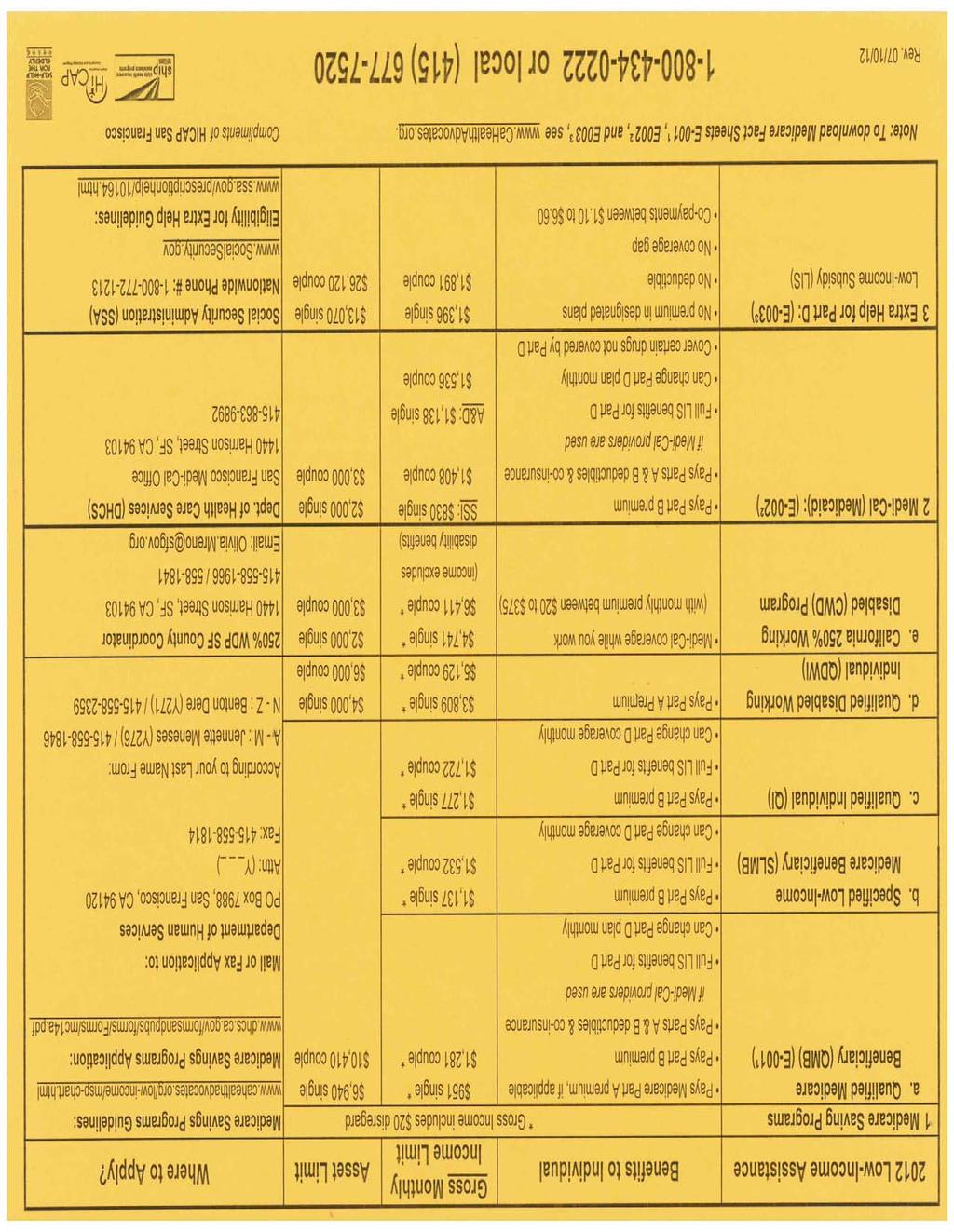
12 Current Medicare Coverage (Check all that apply) Medi-Cal Medi-Cal with Share of Cost Veterans Benefits Original Medicare Medigap Part D Medicare Advantage Plan (HMO/ PPO) You may qualify for Extra Help for Part D. Please ask HICAP if your monthly income is Less than $1,369/month and have assets less than $13,070 (single) Less than $1,891/month and have assets less than $26,120 (married) Enter your Prescription Drugs. You may attach a drug list print-out from your pharmacy. Generic alternatives may save money. Drug Name Dosage (e.g. ml, mg) Frequency (e.g. twice daily) Monthly supply (e.g. 30, 60, 90) Is there a pharmacy you prefer to use? No Yes (if yes, please provide the name and address of your preferred pharmacy)
13 2013 Medicare Part D Stand-Alone Prescription Drug Plans HICAP (800) or Medicare Beneficiary must have Medicare Part A and/or B to enroll in a Prescription Drug Plan. medicare.gov Monthly Low Drug Plan Organization Name Plan Name Plan Annual Co-Payments after deductible has been met Gap Mail Income Quality Enrollment Telephone Number Premium Deductible and prior to reaching $2,970 in full drug cost Coverage Order Subsidy Rating Website Information and Enrollment Tier 1 Tier 2 Tier 3 Tier 4 Tier 5/6 Plan Aetna Medicare Rx Plans CVS Pharmacy Plan $28.60 $325 $2 $5 $45 47% 25% No Yes Yes aetnamedicare.co Premier Plan $ $0 $5 $33 $45 49% 33% Many Generics Some Brands Yes 3.5 Anthem Blue Cross Standard $41.30 $325 $2 $6 $39 $85 25% No Yes Plus $76.80 $0 $2 $7 $45 $90 $95 / 33% Few Generics Yes 3.0 anthem.com/ca/medicare Gold $ $0 $2 $7 $45 $90 $95 / 33% Many Generic Some Brands Yes 3.0 Blue Shield Basic $53.40 $325 $4 $37 $76 25% 25% No Yes blueshieldca.co Enhanced $72.50 $0 $5 $45 $90 25% 33% No Yes 4.0 Cigna cignamedicarerx.c Plan One $325 $0 $8 $28 $70 25% No Yes 3.0 Envision Silver Plan $29.10 $325 25% 25% 23% 28% 25% No No Yes envisionrxplus.co Gold Plan $54.00 $150 $2 or 1% $5 or 1% $25 or 1% 30% 29% Some Generics Yes 3.0 Express Scripts Value $61.00 $325 $4 $6 25% 27%-50% 25% No Yes express-scriptsmedicare.c Choice $91.60 $200 $8 $45 $95 28% 28% Many Generics Yes 4.0 First Health Value Plus $24.20 $0 $0 $35 $70 33% 33% No Yes Premier $47.90 $325 $1 $25 43% N/A N/A No Yes 3.0 myfirsthealthpland.com Premier Plus $ $0 $0 $20 25% 43% 33% Some Generics Some Brands Yes 3.5 HealthMarkets Medicare Reader's Digest Value Plan hmic-medicare.c $32.30 $325 $1 $2.50 $37 27% N/A No Yes new Health Spring myhealthspring.c Humana Health Spring Drug Plan Wal Mart Plan $18.50 $325 $325 25% $1 25% $3 25% 20% 25% 35% 25% 25% No No Yes Yes Yes Enhancd $47.50 $0 $2 $5 $44 $90 33% No Yes 3.5 humana-medicare.com Complete $ $0 $5 $37 $69 $33 33% Some Generics Some Brands Yes 3.5 Rev.10/15/2012 Information subject to change.contact plans to verify information. Tier 1 = Preferred GenericsTier 2 = Non Preferred GenericsTier 3 = Preferred BrandsTiers 4 = Non Preferred Brands Tier 5 = Specialty Drugs
14 Logo Here :-) 2013 Medicare Part D Stand-Alone Prescription Drug Plans HICAP (800) or Medicare Beneficiary must have Medicare Part A and/or B to enroll in a Prescription Drug Plan. medicare.gov Monthly Low Drug Plan Organization Name Plan Annual Co-Payments after deductible has been met Gap Mail Income Quality Enrollment Telephone Number Plan Name Premium Deductible and prior to reaching $2,970 in full drug cost Coverage Order Subsidy Rating Website Information and Enrollment Tier 1 Tier 2 Tier 3 Tier 4 Tier 5/6 Plan Silver Script Basic $30.60 $325 $2 21% 43% 25% N/A No Yes Yes Choice $29.10 $0 $0 $34 35% 33% N/A No Yes 3.0 silverscript.com Plus $ $0 $0 $34 35% 33% N/A Many Generics Some Brands Yes 3.0 Smart Rx Saver $31.40 $325 $0 $20 $32 $85 25% No Yes Yes new smartdrx.com Plus $73.00 $0 $0 $20 $32 $85 25% Some Generics Yes new United American Select $36.50 $325 $1 $4 $37 $95 25% No Yes uamedicarepartd.c Enhanced $60.80 $80 $1 $7 $40 $95 29% No Yes 3.5 United Health Care - AARP MedicareRx Saver Plus $15.00 $325 $1 $2 $25 $45 25% No Yes Yes MedicareRx Preferred $47.90 $0 $3 $5 $40 $85 33% No Yes 3.0 aarpmedicarerx.com MedicareRx Enhanced $98.00 $0 $2 $5 $40 $76 33% Some Generics Some Brands Yes 3.0 Well Care Classic $33.00 $0 $6 $45 $95 33% 33% No Yes wellcarepdp.c Extra $ $0 25% 25% 50% 33% Many Generics Yes 3.0 Used by permission from Council of Aging Orange County
15 San Francisco 2013 Medicare Advantage Plans Page 1 of 2 Care1st Chinese Com. Health Plan Health Net of California Humana Humana Kaiser Permanente Plan Name Care1st AdvantageOptimum Plan (H ) HMO Senior Program (H ) HMO Health Net Healthy Heart (H ) HMO Humana Gold Plus (H ) HMO Humana Gold Plus (H ) HMO Senior Advantage (H ) HMO Monthly Premium $28, MOOP $3400 $40, MOOP $3400 $89, MOOP $6700 $32, MOOP $5000 $62, MOOP $3400 $76, MOOP $3400 Phone Number Prospective Members ext Prospective Members Prospective Members Prospective Members Prospective Members Prospective Members Current Members Current Members Current Members Current Members Current Members Current Members Web Site Address Network Provider Brown and Toland Chinese Community Health Plan Physicians Brown and Toland; Hill Physicians Kaiser Network Network Hospital CPMC CPMC, Chinese Hospital, St. Francis, St. Mary's CPMC, UCSF, St. Francis, St. Mary's CPMC CMPC Kaiser Permanente Physician Visit $0 primary care. $10 specialist. $15 primary care, specialist, urgent care. $10 primary care, specialist or in-network urgent care. $0 primary care. $10 specialist. $0 primary care. $5 specialist. $25 primary care. $25 specialist. Inpatient Hospital Outpatient Surgery $100/day for days 1-5; $0 for days 6-90 and beyond. Unlimited days each benefit period. Except in an emergency, your doctor must notify plan of admission. $20-$75 for each visit to outpatient surgical center. $20-50 for each visit to outpatient hospital facility. $ /day for days 1-7;$0 for days 7-90 and beyond. Unlimited days each benefit period. Except in an emergency, your doctor must notify plan of admission. $ for each visit to the surgical center or outpatient hospital facility. Authorization rules may apply. $320/day for days 1-5; $0 for days 6-90 and beyond. Unlimited days each benefit period. Except in an emergency, your doctor must notify plan of admission. $125 for each visit to outpatient surgical center. $250 for each visit to outpatient hospital facility. $125/day for days 1-8; $0 for days 9-90 and beyond. Unlimited days each benefit period. Except in an emergency, your doctor must notify plan of admission. $150 for each visit to outpatient surgical center. $10-$200 (or 20% of cost) for each visit to outpatient hospital facility. $100/day for days 1-8; $0 for days 9-90 and beyond. Unlimited days each benefit period. Except in an emergency, your doctor must notify plan of admission. $50 for each visit to outpatient surgical center. $5-$125 (or 20% of cost) for each visit to outpatient hospital facility. $255/day for days 1-7; $0/day for days 8-90; $0 copay for additional days. Except in emergency. Doctor must tell the plan you are being admitted into a hospital. $250 for each outpatient surgical center visit. $0-$250 for each visit to hospital facility. Mental Health Inpatient : Days 1-8 $100/day; Days 9-90 $0/day, Inpatient : Days 1-7 $250/day; Days 8-90 $0/day. except in an emergency, doctors must inform the plan. Additional days are $0 except, in emergency, doctor Outpatient : Individual therapy w/ psychiatrist and must inform plan. without & group therapy w/ psychiatrist and without Outpatient : Individual therapy w/ psychiatrist and $10; Partial hospitalized program $0. without & group therapy w/ psychiatrist and without $25; Partial hospitalized program services $0. Inpatient : Part of 190 lifetime days inpatient hospital care; $900/day. In an emergency, doctor must inform plan. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $25; Partial hospitalized program $0. Inpatient : Days 1-8 $125/day; Days 9-90 $0/day, except in an emergency, doctors must inform the plan. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $10; Partial hospitalized program $25. Inpatient : Days 1-8 $100/day; Days 9-90 $0/day, except in an emergency, doctors must inform the plan. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $5; Partial hospitalized program $25. Inpatient : Days 1-7 $255/day; Days 8-90 $0/day. Additional days are $0, except in an emergency, doctors must inform the plan. Outpatient : Individual therapy w/ psychiatrist and without $25. Group therapy w/ psychiatrist and without $12; Partial hospitalized program services $0. Ambulance Service $100; if admitted into the hospital you pay $0. $175 for Medicare-covered ambulance services. Authorization rules may apply. $275 for Medicare-covered ambulance services. Authorization rules may apply. $150 for Medicare-covered ambulance services. Authorization rules may apply. $150 for Medicare-covered ambulance services. Authorization rules may apply. $200 for Medicare-covered ambulance visit. Emergency Care $50; $25,000 plan coverage limit for supplemental emergency services outside the U.S. every year; if immediately admitted into the hospital you pay $0. $65; waived if admitted within 24 hours for the same condition. Worldwide coverage. $65; waived if admitted immediately. Worldwide coverage. Annual $50,000 limit for emergency services outside the U.S. $65; if immediately admitted into the hospital you pay $0. Worldwide coverage. $65; if immediately admitted into the hospital you pay $0. Worldwide coverage. $65; if immediately admitted into the hospital you pay $0. Worldwide coverage. Diagnostic Test, X- Ray & Lab Service $0 for Medicare-covered x-rays, clinical/ diagnostic lab tests and diagnostic radiology services. 10% for Medicare-covered therapeutic radiology services. $0 for x-rays, clinical/ diagnostic lab tests and therapeutic radiology service. $0-100 for diagnostic radiology services. $0 for x-rays, lab services & diagnostic procedures & tests. $60 for diagnostic & therapeutic radiology services, not including x-ray. $0-$10 for lab services & diagnostic procedures & tests. $0-$125 (or 20% cost) for diagnostic, not including x-ray services. $0-$10 (or 10% cost) for x- rays. $10 (or 20% cost) copay for therapeutic radiology services. $0-$5 for lab services. $0-$10 for x-rays, diagnostic procedures & tests. $0-$125 for diagnostic services, not including x-rays. $5 (or 20% cost) copay for therapeutic radiology services. $0-$30 for lab services, diagnostic procedures and tests. $30 for x-rays. $145 copay diagnostic radiology services, not including x-ray. Prescription Drugs Copay Tier 1: Preferred generic $0/ 30 day supply Tier 2: Non-preferred generic $5/ 30 day supply Tier 3: Preferred generic $30 /30 day supply Tier 4: Non-preferred generic $50 /30 day supply Tier 5: Specialty 30% coinsurance /30 day supply Tier 1: Generic $10 /30 day supply Tier 2: Brand name $40 /30 day supply Tier 3: Specialty 20% coinsurance /30 day supply Tier 1: Preferred generic $3 /30 day supply Tier 2: Non-preferred generic $12 /30 day supply Tier 3: Preferred Brand $45 /30 day supply Tier 4: Non-preferred brand $95 /30 day supply Tier 5: 33% coinsurance /30 day supply Tier 1: Preferred generic $5 /30 day supply Tier 2: Non-Preferred generic $10 /30 day supply Tier 3: Preferred brand $45 /30 day supply Tier 4: Non-Preferred brand $45 /30 day supply Tier 5: Specialty Tier 33% coinsurance /30 day supply Tier 1: Preferred Generic $0/ 30 day supply Tier 2: Non-Preferred generic $10 /30 day supply Tier 3: Preferred brand $45 /30 day supply Tier 4: Non-preferred brand $95 /30 day supply Tier 5: Specialty Tier 33% coinsurance /30 day supply Tier 1: Preferred generic $5 /30 day supply Tier 2: Generic $10 /30 day-supply Tier 3: Preferred brand name $45 /30 day supply Tier 4: Non-Preferred brand name $65 /30 day supply Tier 5: 25% coinsurance /30 day supply Tier 6: Injectable Part D vaccines /no charge Dental Vision $0 copay for 1 cleaning every six months and 1 dental x-ray every 2 years. $0-$570 copay for Medicarecovered dental benefits. $5 copay for 1 fluoride treatment a year. $0 copay for 1 pair of Medicare-covered eyeglasses or contact lenses after cataract surgery. $0 copay for Medicare-covered eye exams to look at eye condition. $5 copay for up to 1 supplemental routine eye exams every year. Optional Supplemental Package: $14.60 monthly premium includes preventive and comprehensive dental. No additional rider. Two Optional Supplemental Packages: $19 or $29 monthly premium includes preventive and comprehensive dental, chiropractic, acupuncture, eye wear, and education and wellness programs. 3 Optional Supplemental Packages: $10-$28 monthly premium includes eye exam, eye wear, preventative dental, comprehensive dental. 3 Optional Supplemental Packages: $10-$28 monthly premium includes eye exam, eye wear, preventative dental, comprehensive dental. 3 Optional Supplemental Packages: $10-$28 monthly premium includes eye exam, eye wear, preventative dental, comprehensive dental. 3 Optional Supplemental Packages: $10-$28 monthly premium includes eye exam, eye wear, preventative dental, comprehensive dental. Optional Supplemental Package: Advantage Plus - $20 monthly premium includes preventive and comprehensive dental, eye wear, and hearing aids. For more information, call San Francisco HICAP , or Medicare or or contact plan directly. DRAFT Updated 10/17/2012
16 San Francisco 2013 Medicare Advantage Plans Page 2 of 2 SCAN Health Plan SCAN Health Plan United Healthcare Health Net of California Anthem Blue Cross Plan Name Plus (H ) HMO Classic (H ) HMO AARP Medicare Complete (H ) HMO Health Net Seniority Plus Green (H ) HMO Anthem Medicare Preferred Standard (H ) PPO Monthly Premium $27.50, MOOP $3000 $49, MOOP $3400 $0, MOOP $6700 **NO Part D. $99, MOOP $3400 $85, MOOP $3800 Phone Number Prospective Members Prospective Members Prospective Members Prospective Members Prospective Members Current Members Current Members Current Members Current Members Current Members Web Site Address Network Provider Brown and Toland; Hill Physicians Brown and Toland; Hill Physicians Brown and Toland; Hill Physicians Brown and Toland; Hill Physicians Lower copayments for in-network providers than for out-of-network providers. You may go to any doctor, specialist or hospital out-of-network. Network Hospital CPMC, St. Francis, St. Mary's CPMC, St. Francis, St. Mary's CPMC, St. Mary's, UCSF, UCSF Cancer Center CPMC, UCSF, St. Francis, St. Mary's Physician Visit Inpatient Hospital Outpatient Surgery Mental Health Ambulance Service 20% of the cost for each Medicare-covered primary care visit, specialist visit, urgent care days covered each benefit period. Will not be charged additional sharing for professional services. In an emergency, doctor must tell plan you will be admitted into the hospital. 20% for each visit to outpatient surgical center or outpatient hospital facility. Inpatient : Inpatient psychiatric services count toward 190-day lifetime inpatient psychiatric hospital care in a lifetime. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without 35% of cost. Partial hospitalized program services 20% of cost. $5 primary care. $10 specialist. $5 primary care. $10 specialist. $10 primary care or specialist. In-Network : $15 primary care. $45 for specialist. Out-of-Network : $35 primary care. $55 for specialist. $125 for days 1-8; $0 for days $0 copay for $395/day for days 1-4. $0 for days Unlimited $275/day for days 1-7; $0 for days 8-90 and beyond. additional days, except in emergency. Doctor must tell days each benefit period. Except in an emergency, Unlimited days each benefit period. Except in an the plan you are being admitted into a hospital. your doctor must notify plan of admission. emergency, your doctor must notify plan of admission. $175 for each visit to outpatient surgical center. $200 for each visit to outpatient hospital facility. Inpatient : Days 1-8 $125/day; Days 9-90 $0/day. Additional days are $0 except in an emergency, doctors must inform plan. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $25. Partial hospitalized program services $25. 20% for each visit to outpatient surgical center or outpatient hospital facility. Inpatient : Days 1-7 $255/day; Days 8-90 $0/day; Additional days are $0; except in emergency, doctor must inform plan. Outpatient : Individual therapy w/ psychiatrist & without $25. Group Therapy w/ psychiatrist and without $12; Partial hospitalized Medicare program services $60. $125 for each visit to outpatient surgical center. $275 for each visit to outpatient hospital facility. Inpatient : Part of 190 lifetime days inpatient hospital care; $900/day; in an emergency, doctor must inform plan. Outpatient : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $25; Partial hospitalized program $0. 20% of Medicare-approved cost. $150 for Medicare-covered ambulance benefits. $200 for Medicare-covered ambulance service. $125 for Medicare-covered ambulance services. Authorization rules may apply. Emergency Care 20% of the cost (up to $65). $65; if immediately admitted into the hospital you pay $0. $65; waive if admitted within 24 hours for same condition. Worldwide coverage. $50; waived if admitted immediately. Worldwide coverage. Yearly $50,000 limit for emergency services outside the U.S. In-Network : $695 copay for each Medicare-covered stay. Out-of-Network : 15% of the cost of each stay. Unlimited days each benefit period. Except in an emergency, your doctor must authorize. In-Network : 15% of cost for each Medicare-covered ambulatory surgical center visit; $0- $45 copay (or 15% of the cost) for each Medicare-covered outpatient hospital facility visit. Authorization rules may apply. Out-of Network : 25% of cost for each ambulatory surgical center or outpatient hospital facility visit. Inpatient: In-Network: Up to 190 days of inpatient psychiatric hospital care in a lifetime. Inpatient psychiatric hospital services count toward the 190-day lifetime limitation only if certain conditions are met. This limitation does not apply to inpatient psychiatric services furnished in a general hospital. $695 copay for each hospital stay. Except in an emergency, your doctor must tell the plan that you are going to be admitted to the hospital. Out-of-Network : 15% of the cost for each hospital stay. Outpatient: In-Network : Individual therapy w/ psychiatrist and without & group therapy w/ psychiatrist and without $40. Out-of-Network : 30% of the cost for Mental Health visits w/ psychiatrist and without. 30% of the cost for partial hospitalization program services. In- or Out-of-Network : $200 for Medicare-covered ambulance service. Authorization rules may apply. $65 for Medicare-covered ER visits; waived if admitted within 72 hours for same condition. Worldwide coverage. Diagnostic Test, X- Ray & Lab Service Prescription Drugs Copay 20% of cost for diagnostic tests, x-rays and lab services. Tier 1: Preferred Generic $0 /31 day supply Tier 2: Non- Preferred Generic $0 /31 day supply Tier 3: Preferred brand 25% of cost /31 day supply Tier 4: Non- Preferred brand 25% of cost /31 day supply Tier 5: Specialty 25% coinsurance /31 day supply Tier 6: Select Care $10 /31 day supply $0 for lab services, diagnostic procedures and tests. 20% of costs for x-rays. Tier 1: Preferred generic drugs $5 /31 day supply Tier 2: Non-Preferred generic drugs $10 /31 day supply Tier 3: Preferred brand drugs $45 /31 day supply Tier 4: Non-Preferred brand drugs $75 /31 day supply Tier 5: Specialty drugs 33% of cost /31 day supply Tier 6: Select care drugs $10 /31 day supply $13 for lab tests. $15 for x-rays. 20% for diagnostic procedures & tests, including therapeutic radiology services. Tier 1: Preferred Generic $5 /31 day supply Tier 2: Non-Preferred Generic $8 /31 day supply Tier 3: Preferred brand $45 /31 day supply Tier 4: Non-Preferred brand $95 /31 day supply Tier 5: Specialty Tier 33% coinsurance /31 day supply $0 for x-rays, lab services & diagnostic procedures & tests. $60 for diagnostic, not including x-ray & therapeutic radiology services. This plan does not offer prescription drug coverage. Note: You cannot enroll in a Part D, in addition to this plan. 20% of cost for Part B-covered drugs. In-network : $0 copay for Medicare-covered lab services. $65- $200 copay for Medicare-covered diagnostic radiology services (not including x-rays). 20% of the cost for Medicare-covered therapeutic radiology services. $0- $200 copay for Medicare-covere diagnostic procedures and tests. $65 copay for Medicare-covered x-rays. Out-of-Network : 30% of the cost for Medicare-covered therapeutic radiology services, Medicare-covered outpatient x-rays, Medicare-covered diagnostic radiology services, Medicare-covered diagnostic procedures, tests, and lab services. In-Network: $90 deductible on all drugs, except Tiers 1, 5, and 6. Tier 1: Preferred Generic $4 /30 day supply Tier 2: Non-preferred Generic $8 /30 day supply Tier 3: Preferred Brand: $40 /30 day supply Tier 4: Non-preferred Brand: $90 /30 day supply Tier 5: Injectable Drugs: 33% coinsurance /30 day supply Tier 6: Specialty: 33% coinsurance /30 day supply Dental Optional Supplemental Package: $15 monthly premium in addition to the monthly plan premium. Includes preventative dental. Optional Supplemental Benefits: #1: Basic Options- $8 monthly premium includes preventive dental. #2: High Option- $15 monthly premium includes preventative dental. Two Optional Supplemental Packages: #1: Deluxe Rider- $37 monthly premium includes preventive and comprehensive, dental, vision & 2 Optional Supplemental Packages: $19 or $29 monthly premium includes preventive and comprehensive dental, chiropractic, acupuncture, eye wear, and education and wellness programs. hearing aids. Vision No additional rider. 2 Optional Supplemental Packages: $19 or $29 #2: Dental 467 Rider- $15 monthly premium includes monthly premium includes preventive and preventive dental. comprehensive dental, chiropractic, acupuncture, eye wear, and education and wellness programs. 20% of cost for Part B-covered drugs for in-network and out-of-network. 3 Optional Supplemental Packages: #1: Preventive Dental - $12 monthly premium includes preventive dental. #2: Comprehensive Dental & Vision - $31 monthly premium includes preventive and comprehensive dental, eye exams, eye wear. #3: Combination Package - $36 monthly premium includes preventive and comprehensive dental, eye exams, eye wear, chiropractic, and acupuncture. For more information, call San Francisco HICAP , or Medicare or or contact plan directly. DRAFT Updated 10/17/2012
HEALTH PLANS FOR PARTICIPANTS
 Kern County 2018 Retiree HEALTH PLANS FOR PARTICIPANTS OVER AGE 65 (Must have BOTH Medicare Parts A & B) For current participating physician information, please contact each plan directly. This summary
Kern County 2018 Retiree HEALTH PLANS FOR PARTICIPANTS OVER AGE 65 (Must have BOTH Medicare Parts A & B) For current participating physician information, please contact each plan directly. This summary
2009 BENEFIT HIGHLIGHTS HEALTH NET PEARL HAWAII OPTION 1
 2009 BENEFIT HIGHLIGHTS HEALTH NET PEARL HAWAII OPTION 1 Hawaii, Honolulu, Kalawao, Kauai and Maui counties MEDICAL COVERAGE Monthly Plan Premium $0 Calendar Year Out-Of-Pocket Maximum1 $1,200 Inpatient
2009 BENEFIT HIGHLIGHTS HEALTH NET PEARL HAWAII OPTION 1 Hawaii, Honolulu, Kalawao, Kauai and Maui counties MEDICAL COVERAGE Monthly Plan Premium $0 Calendar Year Out-Of-Pocket Maximum1 $1,200 Inpatient
FREEDOM BLUE PPO R CO 307 9/06. Freedom Blue PPO SM Summary of Benefits and Other Value Added Services
 FREEDOM BLUE PPO R9943 2007 CO 307 9/06 Freedom Blue PPO SM Summary of Benefits and Other Value Added Services Introduction to Summary of Benefits for Freedom Blue January 1, 2007 - December 31, 2007 California
FREEDOM BLUE PPO R9943 2007 CO 307 9/06 Freedom Blue PPO SM Summary of Benefits and Other Value Added Services Introduction to Summary of Benefits for Freedom Blue January 1, 2007 - December 31, 2007 California
2019 Health Net Seniority Plus Amber I (HMO SNP) H0562: 055 Fresno, Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Francisco
 H0562: 055 Fresno, Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Francisco") 2019 Health Net Seniority Plus Amber I (HMO SNP) H0562: 055 Fresno, Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Francisco and Tulare Counties, CA H0562_19_7837SB_055_M_Accepted
2019 Health Net Seniority Plus Amber I (HMO SNP) H0562: 055 Fresno, Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Francisco and Tulare Counties, CA H0562_19_7837SB_055_M_Accepted
Freedom Blue PPO SM Summary of Benefits
 Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
2012 Summary of Benefits
 2012 Summary of Benefits San Francisco County, CA Benefits effective January 1, 2012 H0562 Health Net of California, Inc. Material ID # H0562_2012_0055 CMS Approved 08122011 SECTION I Introduction to
2012 Summary of Benefits San Francisco County, CA Benefits effective January 1, 2012 H0562 Health Net of California, Inc. Material ID # H0562_2012_0055 CMS Approved 08122011 SECTION I Introduction to
Summary of Benefits. New York: Bronx, Kings, New York, Queens and Richmond Counties
 Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
Summary of benefits Health Net. seniority plus green. Benefits effective January 1, 2009 H0562 Medicare Advantage HMO
 2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2016 Summary of Benefits
 2016 Summary of Benefits Health Net Jade (HMO SNP) Kern, Los Angeles and Orange counties, CA Benefits effective January 1, 2016 H0562 Health Net of California, Inc. H0562_2016_0175 CMS Accepted 09082015
2016 Summary of Benefits Health Net Jade (HMO SNP) Kern, Los Angeles and Orange counties, CA Benefits effective January 1, 2016 H0562 Health Net of California, Inc. H0562_2016_0175 CMS Accepted 09082015
For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com or call us for more information.
 This Summary of Benefits contains 2018 plan information for: Geisinger Gold Secure Rx (HMO SNP) For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com
This Summary of Benefits contains 2018 plan information for: Geisinger Gold Secure Rx (HMO SNP) For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com
MEDICARE CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS.
 ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
Summary of Benefits. for Anthem Medicare Preferred Premier (PPO)
") Summary of Benefits for Available in Androscoggin, Cumberland, Franklin, Hancock, Kennebec, Lincoln, Oxford, Penobscot, Piscataquis, Sagadahoc, Somerset, Waldo, and Washington Counties, ME Anthem Blue
Summary of Benefits for Available in Androscoggin, Cumberland, Franklin, Hancock, Kennebec, Lincoln, Oxford, Penobscot, Piscataquis, Sagadahoc, Somerset, Waldo, and Washington Counties, ME Anthem Blue
Summary of Benefits. for Blue Medicare Access Value SM (Regional PPO) Available in Ohio
 Available in Ohio") Summary of Benefits for SM Available in Ohio Anthem Blue Cross and Blue Shield is a Health plan with a Medicare contract.anthem Insurance Companies, Inc. (AICI) is the legal entity that has contracted
Summary of Benefits for SM Available in Ohio Anthem Blue Cross and Blue Shield is a Health plan with a Medicare contract.anthem Insurance Companies, Inc. (AICI) is the legal entity that has contracted
Information for Dual-Eligible Members with Secondary Coverage through California Regular Medi-Cal (Fee-for-Service)
") Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2015 December 31, 2015 Los Angeles County This publication is a supplement to the 2015 Evidence of Coverage and
Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2015 December 31, 2015 Los Angeles County This publication is a supplement to the 2015 Evidence of Coverage and
2018 Benefit Highlights
 Orange County 2018 Benefit Highlights SCAN Plus (HMO) Medicare Advantage Plan What Are Additional Benefits and Services? Additional Benefits are benefits and services not offered by Original Medicare.
Orange County 2018 Benefit Highlights SCAN Plus (HMO) Medicare Advantage Plan What Are Additional Benefits and Services? Additional Benefits are benefits and services not offered by Original Medicare.
Correction Notice. Health Partners Medicare Special Plan
 Correction Notice Special Plan Following are corrections that apply to both the English and Spanish versions of the 2015 for Special (HMO SNP): Original Information Page 1, under the heading SECTIONS IN
Correction Notice Special Plan Following are corrections that apply to both the English and Spanish versions of the 2015 for Special (HMO SNP): Original Information Page 1, under the heading SECTIONS IN
Medical Plan Options - Retirees Age 65 or Over/ Disabled Participants with Medicare Coverage
 Program Name U of M Retiree Plan with Group MedicareBlue SM Rx Group Platinum Blue SM Plan C with Group MedicareBlue SM Rx Freedom Plan & Freedom Plan & Type of Policy Coordinates with Medicare and includes
Program Name U of M Retiree Plan with Group MedicareBlue SM Rx Group Platinum Blue SM Plan C with Group MedicareBlue SM Rx Freedom Plan & Freedom Plan & Type of Policy Coordinates with Medicare and includes
Information for Dual-Eligible Members with Secondary Coverage through California Regular Medi-Cal (Fee-for-Service)
") Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
Summary of Benefits for SmartValue Classic (PFFS)
") Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
Y0021_H4754_MRK1427_CMS File and Use PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract
 Y0021_H4754_MRK1427_CMS File and Use 08262012 PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract Section I - Introduction to Summary of s Thank you for your interest in.
Y0021_H4754_MRK1427_CMS File and Use 08262012 PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract Section I - Introduction to Summary of s Thank you for your interest in.
PROFESSIONAL SERVICES. 1199SEIU VIP Premier (HMO) Medicare INPATIENT HOSPITAL SERVICES. 1199SEIU VIP Premier (HMO) Medicare
 Medicare INPATIENT HOSPITAL SERVICES. 1199SEIU VIP Premier (HMO) Medicare") PROFESSIONAL SERVICES PCP office visits Specialist office visits Annual physical exam/preventive care Physical, speech & occupational therapy Flu and pneumonia vaccinations Diagnostic services including
PROFESSIONAL SERVICES PCP office visits Specialist office visits Annual physical exam/preventive care Physical, speech & occupational therapy Flu and pneumonia vaccinations Diagnostic services including
Summary of Benefits. Regence MedAdvantage + Rx Classic (PPO) GROUP RETIREE PLAN
 GROUP RETIREE PLAN") 2013 Summary of Benefits GROUP RETIREE PLAN Regence MedAdvantage + Rx Classic (PPO) Regence BlueCross BlueShield of Oregon is an Independent Licensee of the Blue Cross and Blue Shield Association ORMARXG-05761
2013 Summary of Benefits GROUP RETIREE PLAN Regence MedAdvantage + Rx Classic (PPO) Regence BlueCross BlueShield of Oregon is an Independent Licensee of the Blue Cross and Blue Shield Association ORMARXG-05761
Section I Introduction to Summary of Benefits
 Section I Introduction to Summary of Benefits Thank you for your interest in + Rx Classic (PPO) and. Our plans are offered by Regence BlueShield, a Medicare Advantage Preferred Provider Organization (PPO)
Section I Introduction to Summary of Benefits Thank you for your interest in + Rx Classic (PPO) and. Our plans are offered by Regence BlueShield, a Medicare Advantage Preferred Provider Organization (PPO)
2018 Benefit Highlights
 Los Angeles, Riverside and San Bernardino Counties 2018 Benefit Highlights SCAN Connections (HMO SNP) Medicare Advantage Plan The SCAN Story SCAN, a not-for-profit health plan, was founded in 1977 by seniors,
Los Angeles, Riverside and San Bernardino Counties 2018 Benefit Highlights SCAN Connections (HMO SNP) Medicare Advantage Plan The SCAN Story SCAN, a not-for-profit health plan, was founded in 1977 by seniors,
for brand drugs) $15 $20
 $15 $20") Reading AARP MedicareComplete HMO Premiums/month $14 Max Out of Pocket, In- $6,700 Primary Care Dr. Visits $15 Specialist Office Visit $45 Urgent Care $30-40 Mental Health, Subst Abuse $345 per day Out-patient
Reading AARP MedicareComplete HMO Premiums/month $14 Max Out of Pocket, In- $6,700 Primary Care Dr. Visits $15 Specialist Office Visit $45 Urgent Care $30-40 Mental Health, Subst Abuse $345 per day Out-patient
Summary of Benefits. AARP MedicareComplete Choice (PPO) January 1, 2012 December 31, 2012 H
 January 1, 2012 December 31, 2012 H") Summary of Benefits January 1, 2012 December 31, 2012 AARP MedicareComplete Choice H5516-001 North Carolina: Alamance, Chatham, Davidson, Davie, Forsyth, Guilford, Mecklenburg, Orange, Randolph, Rockingham,
Summary of Benefits January 1, 2012 December 31, 2012 AARP MedicareComplete Choice H5516-001 North Carolina: Alamance, Chatham, Davidson, Davie, Forsyth, Guilford, Mecklenburg, Orange, Randolph, Rockingham,
Summary Of Benefits. WASHINGTON Pierce and Snohomish
 Summary Of Benefits WASHINGTON Pierce and Snohomish 2018 Molina Medicare Choice (HMO SNP) (800) 665-1029, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local time H5823_18_1099_0007_WAChoSB Accepted 9/26/2017
Summary Of Benefits WASHINGTON Pierce and Snohomish 2018 Molina Medicare Choice (HMO SNP) (800) 665-1029, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local time H5823_18_1099_0007_WAChoSB Accepted 9/26/2017
OF BENEFITS. Cigna-HealthSpring TotalCare (HMO SNP) H Cigna H3949_15_19921 Accepted
 H Cigna H3949_15_19921 Accepted") agesummary OF BENEFITS Cover erage Cigna-HealthSpring TotalCare (HMO SNP) H3949-009 2014 Cigna H3949_15_19921 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get
agesummary OF BENEFITS Cover erage Cigna-HealthSpring TotalCare (HMO SNP) H3949-009 2014 Cigna H3949_15_19921 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get
H1463-HMO 20 (HMO) HMO 20 (HMO) / HMO 20Rx (HMO) Summary of Benefits
 HMO 20 (HMO) / HMO 20Rx (HMO) Summary of Benefits") H1463- / Summary of Benefits January 1, 2014 December 31, 2014 Call us 8 a.m. to 8 p.m. daily Toll-free 1-800-965-4022 TTY/TDD 1-800-526-0844 www.healthalliancemedicare.org med-hmo20sob-0713 H1463_14_8837
H1463- / Summary of Benefits January 1, 2014 December 31, 2014 Call us 8 a.m. to 8 p.m. daily Toll-free 1-800-965-4022 TTY/TDD 1-800-526-0844 www.healthalliancemedicare.org med-hmo20sob-0713 H1463_14_8837
January 1, 2015 December 31, Maintenance Organization (HMO) offered by HEALTHNOW NEW YORK INC. with a Medicare contract)
 offered by HEALTHNOW NEW YORK INC. with a Medicare contract)") BLUECROSS BLUESHIELD SENIOR BLUE 601 (HMO), BLUECROSS BLUESHIELD SENIOR BLUE HMO SELECT (HMO) AND BLUECROSS BLUESHIELD SENIOR BLUE HMO 651 PARTD (HMO) (a Medicare Advantage Health Maintenance Organization
BLUECROSS BLUESHIELD SENIOR BLUE 601 (HMO), BLUECROSS BLUESHIELD SENIOR BLUE HMO SELECT (HMO) AND BLUECROSS BLUESHIELD SENIOR BLUE HMO 651 PARTD (HMO) (a Medicare Advantage Health Maintenance Organization
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS
 INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Fresno, Merced, Stanislaus and San Joaquin Counties H5928_15_029_SB_CTCA_2
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Fresno, Merced, Stanislaus and San Joaquin Counties H5928_15_029_SB_CTCA_2
2019 Summary of Benefits
 2019 Summary of Benefits H6345 This is a summary of drug and health services covered by January 1, 2019 - December 31, 2019. is Medicare Advantage HMO Plan (HMO stands for Health Maintenance Organization)
2019 Summary of Benefits H6345 This is a summary of drug and health services covered by January 1, 2019 - December 31, 2019. is Medicare Advantage HMO Plan (HMO stands for Health Maintenance Organization)
$100 Hospital Ambulatory Surgical Center (ASC) Specialist: $30/visit Chiropractic (Medicare-covered) Podiatry (Medicare-covered)
 Specialist: $30/visit Chiropractic (Medicare-covered) Podiatry (Medicare-covered)") 2009 BENEFIT HIGHLIGHTS HEALTH NET PEARL NEW YORK OPTION 1 Albany, Broome, Cayuga, Chenango, Erie, Franklin, Genessee, Herkimer, Lewis, Livingston, Madison, Monroe, Montgomery, Oneida, Onondaga, Ontario,
2009 BENEFIT HIGHLIGHTS HEALTH NET PEARL NEW YORK OPTION 1 Albany, Broome, Cayuga, Chenango, Erie, Franklin, Genessee, Herkimer, Lewis, Livingston, Madison, Monroe, Montgomery, Oneida, Onondaga, Ontario,
Annual Notice of Changes for 2016
 Health Alliance Medicare PPO 10 (PPO) offered by Health Alliance Connect, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of Health Alliance Medicare PPO 10. Next year, there
Health Alliance Medicare PPO 10 (PPO) offered by Health Alliance Connect, Inc. Annual Notice of Changes for 2016 You are currently enrolled as a member of Health Alliance Medicare PPO 10. Next year, there
SUMMARY OF BENEFITS 2009
 HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
VIVA MEDICARE Select (HMO)
") INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE January 1, 2014 - December 31, 2014 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc., which
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE January 1, 2014 - December 31, 2014 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc., which
HealthPartners Freedom Plan (Cost) 2011 Medical Summary of Benefits Wisconsin
 2011 Medical Summary of Benefits Wisconsin") HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
Providence Medicare Advantage Plans
 This is an advertisement Providence Medicare Advantage Plans 2018 Plan Comparison Western Oregon, Tri-County and Clark County, Washington H9047 _ 2018PHA38 _ ACCEPTED Service area map Columbia Clark Washington
This is an advertisement Providence Medicare Advantage Plans 2018 Plan Comparison Western Oregon, Tri-County and Clark County, Washington H9047 _ 2018PHA38 _ ACCEPTED Service area map Columbia Clark Washington
2018 Summary of Benefits
 2018 Summary of MVP Health Plan, Inc. (HMO-POS) (HMO-POS) (HMO-POS) H3305: Plan 022, Plan 021 and Plan 020 This is a summary of drug and health services covered by MVP Health Plan January 1, 2018 - December
2018 Summary of MVP Health Plan, Inc. (HMO-POS) (HMO-POS) (HMO-POS) H3305: Plan 022, Plan 021 and Plan 020 This is a summary of drug and health services covered by MVP Health Plan January 1, 2018 - December
2018 Benefit Highlights
 Orange County 2018 Benefit Highlights SCAN Classic (HMO), SCAN Balance (HMO SNP), and Heart First (HMO SNP) Medicare Advantage Plans What Are Additional Benefits and Services? Additional Benefits are benefits
Orange County 2018 Benefit Highlights SCAN Classic (HMO), SCAN Balance (HMO SNP), and Heart First (HMO SNP) Medicare Advantage Plans What Are Additional Benefits and Services? Additional Benefits are benefits
Summary of Benefits For Advantage Health NY - SNP (HMO SNP)
") Summary of Benefits For Advantage Health NY - SNP January 1, 2014 December 31, 2014 Summary of Benefits, H2773-003 Advantage Health NY - SNP H2773_QHPNY0658 Accepted Advantage Health NY - SNP 1 SECTION
Summary of Benefits For Advantage Health NY - SNP January 1, 2014 December 31, 2014 Summary of Benefits, H2773-003 Advantage Health NY - SNP H2773_QHPNY0658 Accepted Advantage Health NY - SNP 1 SECTION
Providence Medicare Advantage Plans
 This is an advertisement Providence Medicare Advantage Plans 2018 Plan Comparison King and Snohomish County Service area map Snohomish King 2018 Providence Medicare Service Area Summit + RX (HMO-POS) Harbor
This is an advertisement Providence Medicare Advantage Plans 2018 Plan Comparison King and Snohomish County Service area map Snohomish King 2018 Providence Medicare Service Area Summit + RX (HMO-POS) Harbor
Summary of Benefits. Medicare Advantage Plan (PPO) January 1, 2013 December 31, Medicare Solution. A UnitedHealthcare
 January 1, 2013 December 31, Medicare Solution. A UnitedHealthcare") 2013 Summary of Benefits January 1, 2013 December 31, 2013 Medicare Advantage Plan (PPO) A UnitedHealthcare Medicare Solution The service area for this plan includes select counties in South Carolina.
2013 Summary of Benefits January 1, 2013 December 31, 2013 Medicare Advantage Plan (PPO) A UnitedHealthcare Medicare Solution The service area for this plan includes select counties in South Carolina.
Summary of Benefits. Available in the Bronx, Kings, New York, Queens, and Richmond Counties in New York
 Summary of Benefits for Empire MediBlue Plus SM (HMO) Available in the Bronx, Kings, New York, Queens, and Richmond Counties in New York This plan is an HMO plan with a Medicare contract. Services provided
Summary of Benefits for Empire MediBlue Plus SM (HMO) Available in the Bronx, Kings, New York, Queens, and Richmond Counties in New York This plan is an HMO plan with a Medicare contract. Services provided
Summary of Benefits PFFS. FreedomBlue SM. Pennsylvania January 1, 2010 through December 31, 2010
 2010 FreedomBlue SM PFFS Summary of Benefits Pennsylvania January 1, 2010 through December 31, 2010 A detailed side-by-side comparison of FreedomBlue PFFS plans and Original Medicare. H9793_09_0350 CMS
2010 FreedomBlue SM PFFS Summary of Benefits Pennsylvania January 1, 2010 through December 31, 2010 A detailed side-by-side comparison of FreedomBlue PFFS plans and Original Medicare. H9793_09_0350 CMS
First Look: Plan Benefit Filings
 July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
Summary of Benefits for Anthem MediBlue Dual Advantage (HMO SNP)
") Summary of Benefits for Available in: Select Counties* in Maine *See Page 2 for a list of counties. Plan year: January 1, 2018 December 31, 2018 In this section, you ll learn about some of the benefits
Summary of Benefits for Available in: Select Counties* in Maine *See Page 2 for a list of counties. Plan year: January 1, 2018 December 31, 2018 In this section, you ll learn about some of the benefits
CALIFORNIA Small Group HMO Aetna Health of California, Inc. Plan Effective Date: 04/01/2007. Aetna Value Network* HMO $30/$40
 PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
Schedule of Benefits
 Schedule of Benefits ANTHEM Small Business Health Options Program (SHOP) This is a brief schedule of benefits. Refer to your Anthem Certificate of Coverage (Booklet) for complete details on benefits, conditions,
Schedule of Benefits ANTHEM Small Business Health Options Program (SHOP) This is a brief schedule of benefits. Refer to your Anthem Certificate of Coverage (Booklet) for complete details on benefits, conditions,
MSG0117 Group Health Options, Inc. Medicare Supplement Plans 2017
 MSG0117 Group Health Options, Inc. Medicare Supplement Plans 2017 The Group Health difference Why choose Group Health? Here are just a few of the reasons why many Medicare enrollees choose and re-enroll
MSG0117 Group Health Options, Inc. Medicare Supplement Plans 2017 The Group Health difference Why choose Group Health? Here are just a few of the reasons why many Medicare enrollees choose and re-enroll
Summary of Benefits. Available in Delaware, Nassau, and Rockland Counties, NY
 Summary of Benefits for SM Available in Delaware, Nassau, and Rockland Counties, NY Empire BlueCross BlueShield is a Health plan with a Medicare contract. Services provided by Empire HealthChoice Assurance,
Summary of Benefits for SM Available in Delaware, Nassau, and Rockland Counties, NY Empire BlueCross BlueShield is a Health plan with a Medicare contract. Services provided by Empire HealthChoice Assurance,
Summary Of Benefits. CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego
, San Bernardino (partial), and San Diego") Summary Of Benefits CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego 2018 Molina Medicare Options Plus (HMO SNP) (800) 665-0898, TTY/TDD 711 7 days a week,
Summary Of Benefits CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego 2018 Molina Medicare Options Plus (HMO SNP) (800) 665-0898, TTY/TDD 711 7 days a week,
Select Summ ary. VIVA MEDICARE Plus Select (HMO) INTRODUCTION TO THE SUMMARY OF BENEFITS FOR. You have choices in your health care.
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR. You have choices in your health care.") INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE Plus January 1, 2013 - December 31, 2013 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc./,
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE Plus January 1, 2013 - December 31, 2013 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc./,
Annual Notice of Changes for 2017
 Network PlatinumPlus (PPO) offered by Network Health Insurance Corporation Annual Notice of Changes for 2017 You are currently enrolled as a member of Network PlatinumPlus. Next year, there will be some
Network PlatinumPlus (PPO) offered by Network Health Insurance Corporation Annual Notice of Changes for 2017 You are currently enrolled as a member of Network PlatinumPlus. Next year, there will be some
SmartSaver. A Medicare Advantage Medical Savings Account Plan. Summary of Benefits and Other-Value Added Services. From Blue Cross of California
 SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
2013 SUMMARY OF BENEFITS Brand New Day HMO D Special Needs Plan (SNP) (For Members with Medicare & Medi-Cal)
 (For Members with Medicare & Medi-Cal)") 2013 SUMMARY OF BENEFITS Brand New Day HMO D Special Needs Plan (SNP) (For Members with Medicare & Medi-Cal) H0838_2013SB_024_File & Use: Contract#H0838 SECTION I - INTRODUCTION TO SUMMARY
2013 SUMMARY OF BENEFITS Brand New Day HMO D Special Needs Plan (SNP) (For Members with Medicare & Medi-Cal) H0838_2013SB_024_File & Use: Contract#H0838 SECTION I - INTRODUCTION TO SUMMARY
2014 Summary of Benefits. Health Net Seniority Plus (Employer HMO) Benefits effective January 1, 2014 and later (Medical plan 9XN)
 Benefits effective January 1, 2014 and later (Medical plan 9XN)") 2014 Summary of Benefits Health Net Benefits effective January 1, 2014 and later (Medical plan 9XN) Material ID# H0562_EG_2014_0008_ Compliance Approved 08132013 Introduction to the Summary of Benefits
2014 Summary of Benefits Health Net Benefits effective January 1, 2014 and later (Medical plan 9XN) Material ID# H0562_EG_2014_0008_ Compliance Approved 08132013 Introduction to the Summary of Benefits
SUMMARY OF BENEFITS. H5649_090412_1065_SB CMS Accepted
 2013 SUMMARY OF BENEFITS H5649_090412_1065_SB CMS Accepted Introduction Section I Introduction to the for MEDICARE PLAN (HMO), MEDI-MEDI PLAN (HMO SNP), and PREMIER PLAN (HMO) January 1 - December 31
2013 SUMMARY OF BENEFITS H5649_090412_1065_SB CMS Accepted Introduction Section I Introduction to the for MEDICARE PLAN (HMO), MEDI-MEDI PLAN (HMO SNP), and PREMIER PLAN (HMO) January 1 - December 31
Extra Value Summary YOU HAVE CHOICES ABOUT HOW TO GET YOUR MEDICARE BENEFITS TIPS FOR COMPARING YOUR MEDICARE CHOICES
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2016 - December 31, 2016 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2016 - December 31, 2016 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
PROFESSIONAL SERVICES INPATIENT HOSPITAL SERVICES OUTPATIENT FACILITY SERVICES
 PROFESSIONAL SERVICES PCP office visits Specialist office visits Annual physical exam/preventive care Physical, Speech & Occupational Therapy Cardiac/Pulmonary Rehab Flu & Pneumonia Vaccinations Diagnostic
PROFESSIONAL SERVICES PCP office visits Specialist office visits Annual physical exam/preventive care Physical, Speech & Occupational Therapy Cardiac/Pulmonary Rehab Flu & Pneumonia Vaccinations Diagnostic
HEALTH CARE BENEFITS YOU CAN COUNT ON. Retired Employees Health Program (REHP)
") HEALTH CARE BENEFITS YOU CAN COUNT ON 2014 Retired Employees Health Program () PEBTF_2014 Thank you for your interest in Geisinger Gold Classic. Our plan is offered by Geisinger Health Plan/Geisinger Gold
HEALTH CARE BENEFITS YOU CAN COUNT ON 2014 Retired Employees Health Program () PEBTF_2014 Thank you for your interest in Geisinger Gold Classic. Our plan is offered by Geisinger Health Plan/Geisinger Gold
Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary
Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary
Select Summary YOU HAVE CHOICES ABOUT HOW TO GET YOUR MEDICARE BENEFITS TIPS FOR COMPARING YOUR MEDICARE CHOICES
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2015 - December 31, 2015 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2015 - December 31, 2015 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
Anthem Blue Cross Your Plan: Modified Classic HMO 15/30/250 Admit/125 OP Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Modified Classic HMO 15/30/250 Admit/125 OP Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Anthem Blue Cross Your Plan: Modified Classic HMO 15/30/250 Admit/125 OP Your : California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Summary Of Benefits January 1, December 31, 2014 Optima Medicare Optima Medicare Basic HMO Optima Medicare Enhanced HMO
 Summary Of Benefits January 1, 2014 - December 31, 2014 Optima Medicare Optima Medicare Basic HMO Optima Medicare Enhanced HMO www.optimahealth.com/medicare Table of Contents 3 Letter from Michael Dudley,
Summary Of Benefits January 1, 2014 - December 31, 2014 Optima Medicare Optima Medicare Basic HMO Optima Medicare Enhanced HMO www.optimahealth.com/medicare Table of Contents 3 Letter from Michael Dudley,
2019 Summary of Benefits
 2019 Summary of Benefits H6351 This is a summary of drug and health services covered by January 1, 2019 - December 31, 2019. is Medicare Advantage HMO Plan (HMO stands for Health Maintenance Organization)
2019 Summary of Benefits H6351 This is a summary of drug and health services covered by January 1, 2019 - December 31, 2019. is Medicare Advantage HMO Plan (HMO stands for Health Maintenance Organization)
Anthem Blue Cross Effective: January 1, 2018 Your Plan: University of California CORE Plan Your Network: Anthem Prudent Buyer PPO
 Anthem Blue Cross Effective: January 1, 2018 Your Plan: University of California CORE Plan Your Network: This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Effective: January 1, 2018 Your Plan: University of California CORE Plan Your Network: This summary of benefits is a brief outline of coverage, designed to help you with the selection
2012 Summary of Benefits
 North Carolina Network Private-Fee-For-Service 2012 N12SB42680102 Charlotte Rale SB Combo 001-002 001 - Patriot (PFFS) 002 - Patriot Plus (PFFS) Counties: Caswell, Cleveland, Durham, Granville, Guilford,
North Carolina Network Private-Fee-For-Service 2012 N12SB42680102 Charlotte Rale SB Combo 001-002 001 - Patriot (PFFS) 002 - Patriot Plus (PFFS) Counties: Caswell, Cleveland, Durham, Granville, Guilford,
SUMMARY OF BENEFITS. Hamilton County Department of Education Network Copay Plan. Connecticut General Life Insurance Co.
 SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Hamilton County Department of Education Annual deductibles and maximums Lifetime maximum Pre-Existing Condition Limitation (PCL) Coinsurance All
SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Hamilton County Department of Education Annual deductibles and maximums Lifetime maximum Pre-Existing Condition Limitation (PCL) Coinsurance All
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS
 INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Alameda,,,, San Francisco and Counties H5928_15_029_SB_TD_2 INTRODUCTION
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Alameda,,,, San Francisco and Counties H5928_15_029_SB_TD_2 INTRODUCTION
2015 Summary of Benefits
 2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
Anthem Blue Cross Your Plan: Modified Classic HMO 20/40/250 Admit /125 OP Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Modified Classic HMO 20/40/250 Admit /125 OP Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection
Anthem Blue Cross Your Plan: Modified Classic HMO 20/40/250 Admit /125 OP Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection
The MITRE Corporation Plan
 Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
We can never insure one-hundred percent of the population against one-hundred percent of the hazards and vicissitudes of life. Franklin D.
 Medicare Explained We can never insure one-hundred percent of the population against one-hundred percent of the hazards and vicissitudes of life. Franklin D. Roosevelt comments on signing The Social Security
Medicare Explained We can never insure one-hundred percent of the population against one-hundred percent of the hazards and vicissitudes of life. Franklin D. Roosevelt comments on signing The Social Security
Summary of Benefits. Tufts Medicare Preferred HMO PLANS Tufts Medicare Preferred HMO GIC
 Tufts Medicare Preferred HMO PLANS 2018 Summary of Benefits Tufts Medicare Preferred HMO GIC The benefit information provided is a summary of what we cover and what you pay. It does not list every service
Tufts Medicare Preferred HMO PLANS 2018 Summary of Benefits Tufts Medicare Preferred HMO GIC The benefit information provided is a summary of what we cover and what you pay. It does not list every service
Summary Of Benefits. Molina Medicare Options Plus (HMO SNP) (866) , TTY/TDD days a week, 8 a.m. 8 p.m. local time
 (866) , TTY/TDD days a week, 8 a.m. 8 p.m. local time") Summary Of Benefits OHIO Brown, Butler, Clark, Clermont, Clinton, Columbiana, Delaware, Fairfield, Fayette, Franklin, Greene, Hamilton, Highland, Hocking, Lake, Madison, Miami, Montgomery, Morrow, Perry,
Summary Of Benefits OHIO Brown, Butler, Clark, Clermont, Clinton, Columbiana, Delaware, Fairfield, Fayette, Franklin, Greene, Hamilton, Highland, Hocking, Lake, Madison, Miami, Montgomery, Morrow, Perry,
Summary Of Benefits. FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk
 Summary Of Benefits FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk 2018 Molina Medicare Options Plus (HMO SNP) (866) 553-9494, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local
Summary Of Benefits FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk 2018 Molina Medicare Options Plus (HMO SNP) (866) 553-9494, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local
This plan is pending regulatory approval.
 Bronze Full PPO 3000 OffEx Benefit Summary (For groups 1 to 50) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective October 1, 2015 THIS MATRIX IS INTENDED TO BE USED
Bronze Full PPO 3000 OffEx Benefit Summary (For groups 1 to 50) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective October 1, 2015 THIS MATRIX IS INTENDED TO BE USED
CA Group Business 2-50 Employees
 PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Member Coinsurance Copay Maximum (per calendar year) Lifetime Maximum Referral Requirement PHYSICIAN SERVICES Primary
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Member Coinsurance Copay Maximum (per calendar year) Lifetime Maximum Referral Requirement PHYSICIAN SERVICES Primary
Summary Of Benefits. NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia
 Summary Of Benefits NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia 2018 Molina Medicare Options Plus (HMO SNP) (866) 440-0127,
Summary Of Benefits NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia 2018 Molina Medicare Options Plus (HMO SNP) (866) 440-0127,
Blue Shield Gold 80 HMO 0/30 + Child Dental INF
 Blue Shield Gold 80 HMO 0/30 + Child Dental INF Benefit Summary (For groups 1 to 100) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective January 1, 2017 THIS MATRIX
Blue Shield Gold 80 HMO 0/30 + Child Dental INF Benefit Summary (For groups 1 to 100) (Uniform Health Plan Benefits and Coverage Matrix) Blue Shield of California Effective January 1, 2017 THIS MATRIX
SUMMARY OF BENEFITS. Advantage (HMO) H
 H") SUMMARY OF BENEFITS January 1, 2017 - December 31, 2017 Cigna-HealthSpring Advantage (HMO) H4513-009 Our service area includes the following counties in Texas: Angelina, Brazoria, Cameron, Chambers, Fort
SUMMARY OF BENEFITS January 1, 2017 - December 31, 2017 Cigna-HealthSpring Advantage (HMO) H4513-009 Our service area includes the following counties in Texas: Angelina, Brazoria, Cameron, Chambers, Fort
SUMMACARE BRONZE 4000Q-15 SCHEDULE OF BENEFITS
 SUMMACARE BRONZE 4000Q-15 SCHEDULE OF BENEFITS Enrollee Services Per Member/Per Family Calendar Year Deductible (In-network and out-of-network deductibles are separate. Deductible applies to all covered
SUMMACARE BRONZE 4000Q-15 SCHEDULE OF BENEFITS Enrollee Services Per Member/Per Family Calendar Year Deductible (In-network and out-of-network deductibles are separate. Deductible applies to all covered
SUMMARY OF BENEFITS. Cigna-HealthSpring. Advantage SMS (HMO) H January 1, December 31, Cigna H4407_16_32690 Accepted
 H January 1, December 31, Cigna H4407_16_32690 Accepted") SUMMARY OF BENEFITS January 1, 2016 - December 31, 2016 Cigna-HealthSpring Advantage SMS (HMO) H4407-011 2015 Cigna H4407_16_32690 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS This booklet
SUMMARY OF BENEFITS January 1, 2016 - December 31, 2016 Cigna-HealthSpring Advantage SMS (HMO) H4407-011 2015 Cigna H4407_16_32690 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS This booklet
2018 Summary of Benefits Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA
 GEORGIA / SOUTH CAROLINA") 2018 Summary of Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA For more information, call 1-844-895-8643 Y0122_0172 Accepted DSNP This page intentionally left blank 2018 Summary of Eon Deluxe (HMO SNP)
2018 Summary of Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA For more information, call 1-844-895-8643 Y0122_0172 Accepted DSNP This page intentionally left blank 2018 Summary of Eon Deluxe (HMO SNP)
Vivity offered by Anthem Blue Cross Your Plan: Custom Classic HMO 25/45/500 Admit /250 OP Your Network: Vivity
 Vivity offered by Anthem Blue Cross Your Plan: Custom Classic HMO 25/45/500 Admit /250 OP Your : Vivity This summary of benefits is a brief outline of coverage, designed to help you with the selection
Vivity offered by Anthem Blue Cross Your Plan: Custom Classic HMO 25/45/500 Admit /250 OP Your : Vivity This summary of benefits is a brief outline of coverage, designed to help you with the selection
Summary of Benefits Report SENIOR CARE PLUS: VALUE BASIC PLAN (HMO)-009 January 1, 2015 December 31, 2015 WASHOE COUNTY, NEVADA
-009 January 1, 2015 December 31, 2015 WASHOE COUNTY, NEVADA") SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get your Medicare benefits One choice is to get your Medicare benefits through Original Medicare (fee-for-service Medicare).
SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get your Medicare benefits One choice is to get your Medicare benefits through Original Medicare (fee-for-service Medicare).
PLAN DESIGN AND BENEFITS - PA POS 4.2 with $5/$15/$30 RX PARTICIPATING PROVIDERS
 PLAN FEATURES Deductible (per calendar year) PHYSICIAN SERVICES Primary Care Physician Visits Specialist Office Visits Maternity OB Visits Allergy Treatment Allergy Testing PREVENTIVE CARE Routine Adult
PLAN FEATURES Deductible (per calendar year) PHYSICIAN SERVICES Primary Care Physician Visits Specialist Office Visits Maternity OB Visits Allergy Treatment Allergy Testing PREVENTIVE CARE Routine Adult
Summary of Benefits Fidelis Dual Advantage (HMO SNP) and Dual Advantage Flex Plan (HMO SNP) January 1, 2018 December 31, 2018 CMS Contract #H3328
 and Dual Advantage Flex Plan (HMO SNP) January 1, 2018 December 31, 2018 CMS Contract #H3328") Summary of Benefits (HMO SNP) and Dual Advantage Flex Plan (HMO SNP) January 1, 2018 December 31, 2018 CMS Contract #H3328 Thank you for your interest in Plans. Our plans are offered by The New York State
Summary of Benefits (HMO SNP) and Dual Advantage Flex Plan (HMO SNP) January 1, 2018 December 31, 2018 CMS Contract #H3328 Thank you for your interest in Plans. Our plans are offered by The New York State
Overview monthly plan premium
 2018 Overview monthly plan premium Peoples Health Choices Gold (HMO) Welcome! Thank you for your interest in Peoples Health. We ve heard many times from our plan members that their health means everything
2018 Overview monthly plan premium Peoples Health Choices Gold (HMO) Welcome! Thank you for your interest in Peoples Health. We ve heard many times from our plan members that their health means everything
HEALTH PLAN BENEFITS AND COVERAGE MATRIX
 HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
2017 SEMI-MONTHLY PREMIUMS. Employee and Spouse $ Employee and Child(ren) $ Family $332.12
 $ Family $332.12") 2017 BB&T BENEFITS PROGRAM GUIDE SUPPLEMENTAL INFORMATION FOR CALIFORNIA ASSOCIATES PREPARING FOR BENEFITS ENROLLMENT This supplement to the 2017 BB&T Benefits Program Guide contains additional information
2017 BB&T BENEFITS PROGRAM GUIDE SUPPLEMENTAL INFORMATION FOR CALIFORNIA ASSOCIATES PREPARING FOR BENEFITS ENROLLMENT This supplement to the 2017 BB&T Benefits Program Guide contains additional information
Plan Overview. Health Net Platinum 90 HSP. Benefit description Member(s) responsibility 1,2
 responsibility 1,2") PureCare HSP is available through Covered CA in Kings, Madera, Sacramento, and Yolo counties, and parts of El Dorado, Fresno, Nevada, Placer, and Santa Clara counties. Plan Overview Health Net Platinum
PureCare HSP is available through Covered CA in Kings, Madera, Sacramento, and Yolo counties, and parts of El Dorado, Fresno, Nevada, Placer, and Santa Clara counties. Plan Overview Health Net Platinum
2017 Summary of Benefits
 H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
Vivity offered by Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your Network: Vivity
 Vivity offered by Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your : Vivity This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary
Vivity offered by Anthem Blue Cross Your Plan: Custom Premier HMO 10/100% Your : Vivity This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary
RSNA EMPLOYEE BENEFIT TRUST PLAN II S2502 NON GRANDFATHERED PLAN BENEFIT SHEET
 BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children birth to age 26 Filing Limit 1 year from date of service Mailing Address & PPO Company. Remit claims to:
BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children birth to age 26 Filing Limit 1 year from date of service Mailing Address & PPO Company. Remit claims to:
Blue Choice. Hospital/$50, Physician's Office/Lesser of $50 or 20%; physician $40, facility $50. $35/trip $100/trip $50/trip $100/trip $100/trip
 HOSPITAL SERVICES Hospital Inpatient : Paid in full No cost No cost No cost No cost Hospital Outpatient Hospital $40 or $60 per visit, : $20 per visit Hospital/$50, Physician's Office/Lesser of $50 or
HOSPITAL SERVICES Hospital Inpatient : Paid in full No cost No cost No cost No cost Hospital Outpatient Hospital $40 or $60 per visit, : $20 per visit Hospital/$50, Physician's Office/Lesser of $50 or
Welcome to Regence! Meet your employer health plan
 is an Independent Licensee of the Blue Cross and Blue Shield Association Regence BlueCross BlueShield of Utah Welcome to Regence! Meet your employer health plan 1 Health insurance is a big, wonderful benefit.
is an Independent Licensee of the Blue Cross and Blue Shield Association Regence BlueCross BlueShield of Utah Welcome to Regence! Meet your employer health plan 1 Health insurance is a big, wonderful benefit.
Kaiser Permanente (No. and So. California) 2018 Union
 2018 Union") Kaiser Permanente (No. and So. California) General Information Lifetime Maximum Benefit Annual Maximum Benefit Coinsurance Percentage Precertification Requirements Precertification Penalty Health Savings
Kaiser Permanente (No. and So. California) General Information Lifetime Maximum Benefit Annual Maximum Benefit Coinsurance Percentage Precertification Requirements Precertification Penalty Health Savings
Get More Than. Original Medicare. Summary of Benefits MA Special Needs Plan (HMO SNP) 014. H5826_MA_193_2016_v_01_SB014 Accepted.
 014. H5826_MA_193_2016_v_01_SB014 Accepted.") Get More Than Original Medicare Offered by 2016 Summary of Benefits MA Special Needs Plan (HMO SNP) 014 H5826_MA_193_2016_v_01_SB014 Accepted Section I Introduction to the Summary of Benefits for Community
Get More Than Original Medicare Offered by 2016 Summary of Benefits MA Special Needs Plan (HMO SNP) 014 H5826_MA_193_2016_v_01_SB014 Accepted Section I Introduction to the Summary of Benefits for Community