PUBLIC SESSION MINUTES. 1 Chair
|
|
|
- Nickolas Park
- 5 years ago
- Views:
Transcription
1 The Shrewsbury and Telford Hospital NHS Trust Paper 2 TRUST BOARD MEETING Held on Thursday 26 February 2015 at 2.00pm Seminar Rooms 1&2, Shropshire Education & Conference Centre Royal Shrewsbury Hospital PUBLIC SESSION MINUTES Present: In attendance Meeting Secretary Apologies: Mr P Latchford Mr H Darbhanga Dr R Hooper Mr D Jones Mrs D Leeding Mr B Newman Dr S Walford Mr P Herring Mrs S Bloomfield Dr E Borman Mrs D Kadum Mr N Nisbet Mrs J Clarke Miss V Maher Mr A Osborne Mrs D Vogler Mrs S Mattey None Received Chair Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Chief Executive (CEO) Director of Nursing and Quality (DNQ) Medical Director (MD) Chief Operating Officer (COO) Finance Director (FD) Director of Corporate Governance/Company Secretary (DCG) Workforce Director (WD) Communications Director (CD) Director of Business & Enterprise (DBE) Committee Secretary /019 WELCOME: The Chair welcomed everyone and reminded members that it is a meeting in public rather than a public meeting; questions could be asked at the end or during the meeting, at his discretion /020 CHAIR S AWARD The Director of Business & Enterprise presented the Chair s Award citation for Theatre Senior Operating Department Practitioner, Steve Bennett. The members were informed that Mr Bennett has played a pivotal role in shaping theatre services across the Trust, placing patient care and safety at the fore. Mr Bennett was nominated by colleagues in RSH Theatres to reflect their genuine appreciation for the work that he has undertaken in supporting the reconfiguration of Surgical and Head and Neck Services, and his further support working with the successful Women & Children s reconfiguration project. Mr Bennett has been responsible for the introduction of new instrumentation up to the value of 2 million over the past 18 months, ensuring smooth transition of services. This additional work was undertaken whilst maintaining his clinical commitments in theatre. The DBE acknowledged Mr Bennett s outstanding contribution and continued commitment to achieving all of the Trust values - Proud to Care, Make it Happen, Together we Achieve and We Value Respect. Mr Bennett said he was delighted to receive recognition for the work that goes on behind the scenes /021 PATIENT S STORY The Director of Nursing & Quality introduced Felicity Thomas to deliver this month s Patient Story on behalf of Mrs Mackay and her family and friends. 1 Chair
2 The story relates to Mr Barrie Mackay and the treatment that he received at RSH. Sadly, the family felt that Mr Mackay was the recipient of routine, unconcerned care. Treating the patient as a human being was notably absent; and many examples of this hinged around issues of communication, or non-communication, at all levels. Communication was poor and although the family understood that nurses had a job to do, they felt that generally the nurses appeared too busy to provide information and comfort to patients and their families. The poor communication was exacerbated by the fact that Mr Mackay was discharged and re-admitted as an emergency, three times, to three different teams and wards, so there was a lack of continuity of care. Other lapses of communication impinged on clinical issues. There seemed no evidence of any inter-disciplinary consultation with the colorectal team to inform Mr MacKay s treatment. Unfortunately, Mr Mackay's treatment did not inspire confidence. His concern about low back and abdominal pain had been reported to his GP in November He had a scan at RSH on 23 December 2013 but despite many enquiries, the result of this scan was not made available until late in February After this delay there was no time for further investigation before Mr Mackay was admitted to hospital on 11 March 2014 and diagnosed with "probable appendicitis". Mr Mackay had a haemicolectomy on 13th April and deteriorated further. An emergency procedure was performed on the morning of 30 April After significant efforts and phone calls from Mrs MacKay she spoke to the consultant anaesthetist who had been present during the procedure. This doctor told her that Mr Mackay was very poorly. Mrs Mackay asked whether she should come to the hospital immediately and was advised to phone ITU at 8.30 am. However, Mrs Mackay attended ITU within the hour where she was informed that Mr Mackay had already passed away. Mrs Mackay had been denied the opportunity of sharing her husbands last hours of life. The Board was told that the family felt that this account of Mr MacKay s care highlighted that this experience was completely at odds with all the Values that the hospital purports to hold, and that Mrs Mackay has embarked upon this journey as she does not want anyone else to suffer this level of lack of quality care. However as a positive in this, Mrs Mackay was aided, especially in the early stages, by Ms Rebecca Smith of the Patient Advice and Liaison Service (PALS). The family felt this service was not sufficiently promoted nor valued around the hospital at that time. The Board were informed that details of the PALS service are now included in bedside information packs for patients and made available for visitors. The PALS Team was also instrumental in setting up a positive meeting with the Medical Director and Head of Nursing of the Scheduled Care Group which allowed Mrs Mackay to make suggestions for improvement in some hospital systems. The Patient Story reinforced the CQC Inspection finding that 'End Of Life care was assessed as Inadequate. The family have been advised that the End of Life service is to receive funding and development, and a Steering Committee has been commissioned to direct this improvement. Mrs Mackay suggested the following are issues that require further attention: Better liaison between GP and hospital services, especially in the case of repeated re-admissions Use of anonymised patient stories, such as this, as part of in-house training A re-focusing of rigour in standards of care at all levels; inclusive of agency and temporary staff A clarification of lines of communication/designation and accessibility to clinical teams and consultants An open-book approach to what is going on in the hospital environment and in patient care so that the patient and their family feel informed and included in progress and care plans. The Chair offered sincere apologies to Mrs Mackay and her family and friends on behalf of the organisation. Mrs Mackay reported that it is her sole aim to raise awareness of standards and the importance of quality of care and treating patient s in a holistic way and regarding them as a human being. 2 Chair
3 The family and Board members were assured by the Director of Nursing & Quality that discussions have been held with the individuals involved in Mr Mackay s care. The four Trust Values Proud to Care, Make it Happen, We Value Respect and Together we Achieve will reinforce standards of care in the future and staff will be held to account when they fall short of expected standards. The DNQ asked Mrs Mackay if she would be happy for the Patient Story to be used in future nurse training sessions, and the MD asked if it could be used at future doctor s training sessions. Mrs Mackay agreed this positive way forward. Mrs Mackay s friends, who were also present, reported that RSH is their local hospital and they were alarmed by the quality of care that their friend had received. They reported that they may need to rely on the service in the future and have concerns that it may also let them down. The Chair reported that it is also his local hospital and he would like the public to maintain the pressure to ensure high quality of care is standard Following discussion, the Board members noted the following: The Trust is now a Values driven organisation which make clear the behaviours that are expected The introduction of Gemba Walks for Board members and senior managers, which focus on qualitative issues such as how an area feels and what staff and patients/carers think about it, rather than a checklist inspection The strengthening of the Patient Experience and Involvement Panel (PEIP) to review services and care at the Trust The introduction of the Hello, my name is. Campaign to ensure more openness and better communication Subsequent to the Patient Story the Chair confirmed that he would contact Mrs Mackay personally. Action: Chair /022 DECLARATIONS OF INTERESTS The Declaration of Interests register was presented for information. The DCG confirmed that Dr Hooper s (NED) following changes have been applied: Two removals (Director of Carlisle College and Director of Acton Mill Care Farm Limited) and; Two additions (Director of Hollyhead Estates Limited and Director of Oak Street Wimbligton Limited) /023 MINUTES OF THE MEETING HELD IN PUBLIC on 29 January For accuracy, the following amendments were agreed: Page 7 relating to 12-hour Trolley Breaches amend to a number of extended Trolley Waits Page 9 relating to Industrial Action amend to January 2015 The remainder of the Minutes were APPROVED /024 ACTIONS / MATTERS ARISING FROM THE FORMAL BOARD MEETING HELD ON 29 January /003 Patient s Story DNQ to identify if there is a theme on the Surgical Assessment Unit (SAU) in relation to Pain Management. The DNQ confirmed that she has held discussions with the senior nurse manager on the SAU and huge improvements have already been noticed. The members agreed that this is a good example of the Trust Value Make it Happen following the Patient s Story discussion at last month s meeting. Action Completed. 3 Chair
4 2015.2/007 3-Month Forward Plan DNQ to present the Patient Experience Strategy to the Board for approval. Action: DNQ Due: September 2015 Trust Board Added to Forward Plan. Action Completed /008 Chief Executive s Overview FutureFit Update CEO/DBE to provide update in relation to the shortlist proposal. Agenda Item. Action Completed /009 CQC Inspection Report (Oct 2014) DNQ to present the organisation s action plan to the Feb 2015 Trust Board. Agenda Item. Action Completed /011 Trust Performance Report COO to investigate analytical data in relation to FTT/delays and include in the performance report. Agenda Item. Action Completed /012 People Strategy Update Employee Engagement WD to present Employee Engagement presentation to the June 2015 Trust Board. Action: WD Due: June 2015 Trust Board Added to Forward Plan. Action Completed /012 People Strategy Update Recruitment WD to record improvement in growth against a graph and include in the Performance Report The WD reported that she had unfortunately omitted this information and confirmed that she would include for future Trust Board papers. Action: WD Due: March 2015 Trust Board Included in Trust Performance Report. Action Completed /014 Trust Committee Meetings Business Development & Engagement Committee (BDEC) CEO/DBE to identify if the BDEC is achieving what it set out to The DBE and CEO confirmed that they had held a conversation and do believe in the list of opportunities which will become more tangible. Action Completed /016 Questions from the Floor DNQ to provide an update in relation to End of Life Care to the April 2015 Trust Board Action: DNQ Due: April 2015 Trust Board Added to Forward Plan. Action Completed /016 Questions from the Floor COO to provide an update to the February 2015 Trust Board in relation to the Walk-in Centre Included in Trust Performance Report. Action Completed /025 3-MONTH FORWARD PLAN for the period 26 February April 2015 was presented for information. The DCG reported that the FCUS Post Project Review has been corrected to FCHS Post Project Review. The Review was discussed at the February Finance Committee meeting and will be presented to the July 2015 Trust Board. Action: CS to update Forward Plan. Action Completed. Action: DBE Item Due: July 2015 Trust Board. Added to Forward Plan. The remainder of the Forward Plan was agreed /026 CHIEF EXECUTIVE S OVERVIEW: Emergency Pressure - emergency pressures continue to be a concern. The Fit to Transfer (FTT) figure had peaked at 113 during week commencing 23 February 2015, which has a serious impact on the Trust s ability to provide emergency beds for new admissions. The members were informed that the CEO and Executive Directors are in liaison with Commissioners regarding operational planning and contract negotiations for 2015/16. Finance The CEO confirmed that SaTH is on plan for the projected out-turn (as detailed within the Trust Performance Report). 4 Chair
5 Freedom to Speak Up Sir Robert Francis Review The CEO informed the members of the Freedom to Speak Up review in which Sir Robert Francis sets out 20 Principles and Actions which aim to create the right conditions for NHS staff to speak up, share what works right across the NHS and get all organisations up to the standard of the best and provide redress when things go wrong in future. The report will be taken through the Workforce Committee and Trust Health, Safety & Security Committee routes and assurance provided to Trust Board /027 FUTUREFIT SHORTLIST The DBE presented a paper which highlighted that the Future Fit Programme Board received shortlisting scenarios from the Evaluation Panel during February The Programme Board had an extensive discussion of the Panel s recommendations in the light of evidence provided, and agreed the following acute services scenarios shortlist: Emergency Centre (EC) and Diagnostic & Treatment Centre (DTC) on a new site EC on a new site, DTC at Princess Royal Hospital (PRH) EC on a new site, DTC at Royal Shrewsbury Hospital (RSH) EC at PRH, DTC at RSH EC at RSH, DTC at PRH Do minimum (existing dual site acute services maintained, provider and commissioner efficiency strategies implemented but not major services change) The Programme Board agreed that there should be further debate on the best and safest configuration of obstetric services within these scenarios. This should include reviewing the clinical evidence and workforce models to understand whether obstetrics could operate on a site alongside a DTC, alongside an EC or alongside either. The Urgent Care Centres (UCCs) Programme Board agreed to proceed to work on prototyping two urban UCCs; one in Shrewsbury and the other in Telford; and exploring the most appropriate rural urgent care solutions in partnership with local communities. The Chair highlighted that the Future Fit model is dependent on the feasibility of the Urgent Care models. He supported the process but highlighted that costings had been omitted, as well as the relevance of the location to other services and providers, which are also important factors. The DBE confirmed that the next phase will analyse the modelling and financial factors; this will take place over the next few months. The MD reported that additional work has taken place, particularly regarding the lifespan of the various options. A large amount of discussion has also taken place relating to the geography aspect. The challenge is to change current working practices and ensure they are implemented. The DBE confirmed that Future Fit project will continue and that GPs and the Community Trust will continue to be fully included. Key steps will be taken over the next few months and assurance will be provided to the Trust Board of the processes and governance arrangements. The Chair opened the meeting to questions from the floor at this point. Mr Rook (member of the Patient Experience and Involvement Panel) highlighted that the proposal relates to a new way of delivering healthcare, and suggested a review of the whole healthcare system beforehand. However the CEO reminded members that the Trust is not in a position to delay required changes for any longer-term analysis/evaluation. The situation for Emergency services at SaTH required that an agreed way forward in the medium term needs to be found within the scope of the current agreed terms of reference for the project 5 Chair
6 Following discussion, the members endorsed the process that has been taken to date and the recommended shortlisted scenarios but welcomed the submission of additional information to ensure the appropriateness of the proposals as further modelling by the Programme Workstreams takes place /028 Q3 PROGRESS REPORT ON DELIVERING OUR STRATEGIC PRIORITIES AND OPERATIONAL OBJECTIVES The DBE presented a Q3 2014/15 progress report on delivering SaTH s operational objectives. The paper highlighted that a key feature of the planning process is a review of progress against the delivery of SaTH s strategic and operational plans. The Trust has made good progress in improving clinical outcomes and patient experience and future plans will continue to build on this. Improving outcomes for patients and reducing harm remains a priority in the plan. Developing plans to ensure the sustainability of our services is an immediate requirement for the Trust. Significant work has taken place to mitigate risks within challenged specialties; this includes revised models of care, capacity reviews and service reconfiguration. Embedding revised pathways and developing robust short to medium term strategies for our clinical services is a priority for next year. Alongside this the Trust will continue to work with the wider health economy in developing a long term strategy for services in Shropshire. The planned developments in the Trust s People Strategy are progressing well. The Trust will continue to build upon this success and to increase and enhance staff engagement to support this. Developing transformational plans to support challenged specialties and progress 7 day working remains a priority for next year. Much work has taken place with regard to customer relationships including engagement with patients, local health partners and our GPs. The Trust will continue to strengthen these relationships and to build business plans that reflect the environment in which we operate and the impact that we have on our key stakeholders. Understanding our business through detailed service line reviews will inform future operational and business decisions. Delivering a sustainable financial plan remains a challenge. The Trust has worked extremely hard to secure support for and has made progress in the delivery of recurring cost improvement programmes. Proposed reductions in income and the need to invest in equipment and infrastructure will further increase the financial challenge for the Trust. Priorities for the Trust in will include delivering transformational change, identifying technological solutions and securing ongoing short term financial support. Mr Jones (NED) highlighted the Strategic Priorities RAG rating status and enquired if it s a little too positive. The CEO reported that it is an accurate reflection based on assessment of the achievement of agreed milestones against trajectory in the 14/15 Business Plan. The Chair highlighted that Strategic Priority 7 Develop our leaders and promote staff engagement to make our organisation a great place to work through our People Strategy is RAG rated Green; however he stressed the Board s determination to convey an assertive message regarding the achievement of 100% for Staff Appraisals, which was a fundamental requirement to ensure the alignment of individual and organisational objectives. Mrs Leeding (NED) commented that the document relates more to delivery rather than outcomes. The DBE confirmed that the priorities have been reviewed and evaluated several times before the Plan was agreed by the Board in March For future iterations of the reviews it was suggested that it might be sensible to have a RAG rating for what was required by way of milestones, plus a RAG rating to determine to what extent these actually achieved the objective. Action: DBE The Chair asked the members if they were content with the level of progress achieved. The members agreed that a good level of progress has been achieved against the ten objectives, particularly given the high levels of operational pressures the Trust had faced. 6 Chair
7 2015.2/029 CARE QUALITY COMMISSION INSPECTION ACTION PLAN The DNQ presented an action plan which has been produced to address areas of improvement and compliance in response to the CQC Inspection during October 2014 and subsequent publication of the CQC report on 20 January Each of the Care Groups have produced detailed action plans to respond to the recommendations. The DNQ confirmed that she met with the CQC to discuss the action plan against the five domains (safety, effective, caring, responsive and well led). A number of actions have already been completed and the target is to complete the majority of work within this calendar year. The CQC and Trust will agree a date of reinspection towards the end of the calendar year. Quarterly meetings have also been scheduled with the CQC and the action plan will be presented to the Patient Experience and Involvement Panel during March The DNQ also reported that she would share the action plan with Commissioners, TDA, stakeholders, etc. Dr Walford (NED) confirmed that the action plan had been presented at the Quality & Safety Committee and he enquired if Q&S are primarily responsible for receiving an update or whether the Trust Board would receive an update on a regular basis. The Chair suggested the Q&S Committee receive the detail on a quarterly basis and the Board receive detail at high level every six months. Action: DNQ Due: September 2015 Trust Board. Added to Forward Plan. The members discussed the Gemba Walks process and the DNQ agreed that additional work is required to assist in closing the loop on issues raised. The Chair highlighted that Gemba Walks have not yet been inserted into his diary schedule; the Chair and DNQ agreed to discuss further. Action: DNQ / Chair The Chair also highlighted that he would like an update in relation to the progress of the Employee Engagement Strategy. The WD agreed to provide an update in relation to the Well Led domain at the March 2015 Trust Board. Action: WD Due: March 2015 Trust Board Update included in Workforce Committee Update. Action Completed /030 TRUST PERFORMANCE REPORT AND GOVERNANCE AND MONITOR LICENCE BOARD CERTIFICATES The Board RECEIVED the Trust Performance Report in respect of the month of January SaTH is currently at Escalation Level 4 (of 5) in the NHS Trust Development Authority s Accountability Framework. This is classified as a Material issue requiring interaction led by the TDA s Director of Delivery Development. Regular meetings are held with the TDA to update on SaTH s improvement trajectories. QUALITY & SAFETY (Patient Safety, Effectiveness and Patient Experience) The Director of Nursing & Quality (DNQ) provided an overview of the activity in January 2015: Infection Prevention & Control showed six cases of C difficile in January; 0 MRSA bacteraemia cases (pre-48 hours); two cases of MSSA Bacteraemia and three cases of E-coli Bacteraemia. Vancomycin Resistant Enterococci (VRE) There has been a cluster of cases reported of VRE within the Trust which is an infrequent occurrence. VRE are a type of bacteria called enterococci that have developed resistance to many antibiotics. The IPC Team has targeted the wards where VRE has occurred and provided further training, support in cleanliness and prevention, assessed practice as well as viewing decontamination processes. Each case will be reviewed through the RCA process. Serious Incidents There were 23 SIs reported in January; these related to 12-hour trolley breaches (12; 5 which occurred in December but were reported in January), RIDDOR/SI reportable falls (5), Grade 3 7 Chair
8 Pressure Ulcer (2), IPC issues (2), Surgical error (1) and Delayed diagnosis (1). Pressure Ulcers There were two Grade 3 Pressure Ulcers reported in January Root cause analysis of each is in progress and as yet the avoidability criteria remains undetermined. Safe Staffing January saw a sustained heightened level of patient activity. Both sites (RSH and PRH) were at level 3 or 4 escalation status for most of the month; requiring the opening of additional beds across both main sites as part of the Trust s escalation procedure. This warranted, on occasion, support from non-substantive ward and non-clinical staff, along with shared staffing resources between wards to mitigate risk and ensure the maintenance of quality and patient safety; however, the amount of time provided and resources shared is difficult to quantify due to the short notice and immediacy of requests however the priority is to provide support and this time and resource is therefore not reflected in the staffing data reported. The Heads of Nursing and Midwifery, Matrons and Ward Managers continue to monitor the actual versus planned staffing levels across the Trust on a daily basis. Safeguarding Adults & Children During January there were three adult safeguarding alerts made towards the Trust; this is the same number as December Two alerts remain in progress and one has been found to be substantiated relating to poor discharge information provided about the patient. The Trust raised 13 safeguarding alerts against other care providers and carers during January 2015; and there was one child safeguarding referral made to social services by the Trust during January Following investigation into this referral, no action was instigated. Risk Adjusted Mortality Index (RAMI) Update The RAMI has been updated with the latest available national data and shows that the Trust is performing well against national peers up to November December s figure increased to 94, however the year to date figure remains below the national position. 12-hour Trolley Breaches The number of patients kept waiting for more than 12 hours on a trolley within the Trust s Emergency Department have been reviewed and have had completed RCAs. Findings show that none of the patients received sub-optimal care or were harmed as a result of waiting. A comprehensive report from the review will be completed and considered by the Quality & Safety Committee going forward. The Board received and noted the nurse staffing levels monthly report OPERATIONAL PERFORMANCE The Chief Operating Officer (COO) presented the following update in relation to Operational Performance during the month of January 2015: A&E 4 Hour Access Standard - In January 2015, 82.71% of patients were admitted or discharged within the 4 hour quality target. This was below the trajectory for January and shows a continued deterioration of performance across the Trust. Demand versus plan Emergency Department attendances For the period to the end of December was 3.14% greater than the same period last year and 3.2% in month. During the month of January 2015 the Trust remained in high levels of escalation with patients bedded down in the Emergency Department (ED) waiting for beds. This resulted in a further six 12-hour breaches. RCAs were completed for this group of patients and as part of the RCA process, a full deep dive was carried out with colleagues from both CCGs and the Shropshire Community Trust. No harm was found to have occurred for any of these as a result of the wait. Demand versus plan Non Elective activity Emergency admissions were 7% lower in January compared to the 3.89% increase in December. The acuity of patients increased with the main reason for admission being respiratory infections, cardiac conditions and falls; specifically within the elderly and frail population. Year to date April 2014 to January 2015 in comparison to the same period in 2013 nonelective admissions are 2.99% higher (1,777 admissions).. Referral to Treatment (RTT) : Patients Admitted to Hospital The Trust achieved the RTT standard of 90% for Admitted Patients during January with 90.23%; however Trauma & Orthopaedics, Max Fax and Gynaecology failed to deliver the standard due to the number of elective cancellations. The standard is becoming difficult to achieve as the over 18 week waits are re-dated and treated. The admitted backlog has increased from 163 (October 2014) to 495 (January 2015). A recovery plan is currently being produced. The Scheduled Care Group is also undertaking a review of patient flow to ensure all systems and processes are in place and that all capacity is maximised. Dr Walford (NED) suggested ring-fencing elective activity. It was felt that currently this would be unrealistic due to emergency pressures. 8 Chair
9 Referral to Treatment (RTT) : Non-Admitted to Hospital The Trust delivered the RTT standard of 95% for Non-Admitted Patients during January with 96.58% however four specialties failed to deliver the target. Further analysis is being undertaken to establish the reasons for the failure; this will form part of the Centre s rectification plan. Fit to Transfer (FTT) During January, the Fit to Transfer (FTT) list consistently rose above 50. In January the Secretary of State requested that the Clinical Commissioning Groups (CCGs) reduce the number of patients on the FTT list by 50% in two weeks, with a further 50% reduction in the following two weeks. This meant that there should be no more than 38 patients on the FTT list over two days by 15 February Whilst on occasion this target has been met, it has not been sustained. Due to the slow progress in the reduction in the numbers of patients on the FTT list, alternative solutions are being explored with the independent sector to increase care home capacity in the Shrewsbury area and intermediate care capacity, working with the Shropshire Community Trust. A number of meetings are held on a weekly basis with Commissioners and a series of actions are in place. Urgent Care Centre (UCC) The Prototype UCC opened at RSH on 15 December It is open 8am 8pm, 7 days per week, and provides a Primary Care walk-in service adjacent to the RSH Emergency Department (ED). The UCC has recently seen an increase in patients; the greatest increase during weekends, specifically on a Saturday. Competencies and skills need to be built within the workforce in the UCC to enable them to take more minor injury patients in the future. The model of care will continue to develop in line with the development of Ambulatory Emergency Care (AEC). A project management group has been established and meets monthly to progress these developments. Cancer All of the 9 cancer standards were achieved in December. The January predicted figures do not indicate any exceptions; however 31 day second or subsequent treatment surgery is not stable. A single further breach could see the Trust s position change to a state of non-compliance. The Cancer Services will monitor this position closely. In order to stabilise the complaint level of the Cancer Waiting Time targets, there is currently a review of the escalation process, a multi-disciplinary team review and a referral form review (Breast, Gynaecology and Colorectal). Dr Hooper (NED) suggested highlighting in the Operational Performance the Health Economy s responsibilities for 12 hour breaches, ED, FTT and Non-Elective activity. The COO reported that a number of care packages, domiciliary packages, care home placements etc are required from Commissioners every week and that there was daily focus on these operational issues. The Chair opened the meeting to questions from the floor. Mr Shepherd informed the members the he is a member of a Patient Group which was established in November He reported that he felt the cooperation of all healthcare providers is 100% and therefore does not feel the process can be undertaken in a more timely fashion. Mr Jones (NED) highlighted that the Executive team should be fully supported by the NEDs in next year s contract negotiations. FINANCIAL PERFORMANCE The Trust s budget forecast assumed the delivery of a deficit at month 10 amounting to 6.276m; the actual deficit recorded amounted to 9,507m. To reconcile to the original plan submitted to the NTDA, a phased spend adjustment of 393,000 has been made to both plan and actual spend, bringing a reported position to the NTDA of a deficit at month 10 of 9.9m. The Trust is continuing to forecast an end of year deficit amounting to m. Income At this stage in the financial year focus shifts to the outturn position and in particular the assumptions being made in respect of activity levels that need to be delivered in the remaining months of the financial year to achieve the targeted level of income, and the level of risk associated with the income levels assumed within the forecast outturn. In the remaining two months of the year, activity levels are assumed to be marginally 9 Chair
10 lower than the levels delivered on average per month in the year to date Pay Position - In the month of January, Pay spending was 18,389m as compared with the expected level of Pay spending of 18,137m as contained within the Recovery Plan. During the month, the number of WTE employed within the Trust increased to 5, WTE. This level of staffing is substantially greater than staffing levels recorded during the 2014/15 year. The increase is principally associated with spending in respect of nursing staff. Agency Spending This remained high in the month of January, amounting to 1.274m ( WTE). This is an increase in the levels seen in the month of December. Bank Usage The level of Bank usage in the month of January ( WTE) has increased from December ( WTE). Non-Pay - Non Pay spending in the month of January further reduced when compared with the levels recorded in the month December, and has returned to expenditure levels seen earlier in the financial year. Cost Improvement Programme - Savings realised in the month amounted to 11,168m as compared with a target of 14,497m. It is anticipated that the Trust will deliver savings in year of 13.5m as compared with the original CIP ( 15.2m). The shortfall has occurred because the trust has been unable to secure savings from nursing, medical staffing and has also been required to retain escalations beds. The Trust is also now forecasting that 90% of CQUIN funds will be achieve in the year, which includes the savings forecasted. Rectification savings have been identified amounting to 6.338m. The Trust has discounted Income from CCGs amounting to 1.5m and reduced the level of Agency nurse savings in the remaining months of the year. Cash Flow At the end of January, the cash position on the balance sheet amounted to 2.124m. The FD circulated a copy of a letter (copy attached to the Minutes) that has been received from the Department of Health relating to formal confirmation that the financing application for revenue support PDC of 19,200,000 relating to financial year 2014/15 has been approved. The members formally RECEIVED the letter of approval and ACCEPTED the terms and conditions specified. WORKFORCE The Workforce Director (WD) introduced this section of the paper: Sickness - During January sickness absence for the Trust is 4.66%, a decrease from December 2014, which the highest level seen in Estates at 6.8%. Appraisals The Appraisal completion rate is at 84% against a target of 100% completion by all relevant staff for This is an increase of 1% but a significant step change will need to take place to secure coverage at 100%. Discussions are being held with Care Groups about how to achieve this through Confirm and Challenge meetings, and through management meetings. Statutory & Mandatory Training A review of training capacity is underway to support increased demand; this includes working with teams and departments to bring training to them. Performance remains static at 63%. The WD reported that when the Trust has been at Escalation Level 4, some members of frontline staff have been required to cancel training to remain as staffing on the wards. Temporary Staffing Demand remains high, particularly in nursing. Demands for agency nurses is high across the country, therefore fill rates are spread across a number of tiers, leading to a higher cost. This is a similar picture from neighbouring Trusts. Work is underway to address this, including working with other NHS organisations. Recruitment A review of staff recruitment has been completed to ensure effectiveness; a number of changes have been implemented, such as testing and being able to re-sit on the day, offers being made on the day and the interview process. SaTH is holding two information days to recruit 70 Health Care Assistants (HCAs) to a range of roles across wards, outpatient areas and temporary staffing. Interest in the days has been pleasing with both days fully booked. 10 Chair
11 SELF CERTIFICATIONS The members discussed the Governance and Monitor Licence Board Certifications which were APPROVED subject to the continued financial support from the TDA /031 Q3 COMPLAINTS & PALS REPORT (OCT DEC 2014) The DNQ reported that during Quarter 3, the Trust received a total of 97 formal complaints compared with 90 in the previous quarter. The total year to date is 288 compared with 332 formal complaints received between April December The Trust continues to maintain a high performance in response rates against the target with 93% of complaints being closed within the agreed timescales during this quarter. Where the Trust is unable to respond within the response time initially agreed with the complainant, the complainant is kept fully informed of any delays and a new response date agreed. The number of formal complaints received during the quarter equated to 1.5% per 1,000 bed days compared with 1.6% in the previous quarter. Until end February 2015, three complaints continue to be under investigation. Of the remaining complaints completed, 19% were upheld, 42% were partly upheld and the remaining 39% not upheld by the Trust. The top specialties receiving complaints during the quarter were: Acute Medicine 24 Emergency Medicine 11 Surgery 10 Orthopaedics 7 Obstetrics 4 Urology 4 As in previous quarters, the main issues relate to clinical care. Complaints specifically about communication and nursing care are continuing to see a downward trend. Nursing issues have shown a steady fall over the last few quarters. Issues that continue to be highlighted in complaints are pain relief, hygiene, record keeping, failure to act on abnormal results, failure to record fluid balance, falls, noise at night and discharge planning. Parliamentary & Health Service Ombudsman (PHSO) Where a patient or relative remains dissatisfied following the Trust s response to their complaint, they may forward their complaint to the Parliamentary & Heath Service Ombudsman for review. On receipt the Ombudsman will undertake an assessment and may ask the Trust to take further steps to resolve the complaint, close the case without investigation or decide to investigate the case further. During the quarter, the Trust was notified of four cases referred to the Ombudsman; one of these relates to a complaint received in The other 3 complaints, initially received in previous financial years, are currently being investigated. During Quarter 3, the Ombudsman concluded 2 investigations; one cases was upheld and the other not upheld. PALS During Quarter 3 the PALS team handled 491 compared with 465 concerns in the previous quarter. Main themes relate to appointments, concerns about the patient s medical treatment and pathways, and general attitude of staff. The DNQ reported that the issue of staff attitude will continue to be addressed. The DNQ confirmed that the Annual Complaints Report will be presented to the Trust Board early next year. 11 Chair
12 The members were informed that the Clinical Governance Executive are focusing on medical complaints. The Chair requested an update be presented to the March 2015 Trust Board. Action: MD Due: March 2015 Trust Board Agenda Item. Action Completed /032 GP ENGAGEMENT STRATEGY The DBE presented the paper which highlighted that the NHS Five Year Forward view stresses that healthcare services need to be delivered in a different way in the future and describes the need to break down the barriers between primary and secondary care. Maintaining good relationships with GPs is critical to the successful delivery of the proposed new ways of working and will provide a strong foundation upon which to drive and deliver transformation. GP satisfaction and perception of our organisation can impact on referral patterns and market share. Going forward, this means SaTH needs to adopt a more focused account management style approach to GP engagement and a focus on embedding the use of market intelligence information to inform decision making is required. The GP Engagement Strategy has been developed to provide a structured framework and process to support the Trust in delivering its strategy and to develop and embed robust engagement principles and activities across the organisation. The GP Engagement Strategy identifies 5 key priorities that will provide a focus for our engagement programme which will enable us to build relationships and develop services that provide the best care for our patients with a detailed Work Plan underpinning the Strategy. Mr Newman (NED) noted that the Strategy and Work Plan does not contain delivery dates and suggested these be added. There was discussion about the most appropriate form of engagement and the FD advised that in his previous organisation clinical engagement was the key to improved relations with GPs. The COO confirmed that many providers use a clinical senate approach to improve engagement between primary and secondary care by focusing on specific pathways. Following discussion, the Chair agreed that additional work is required on the Strategy before it could be approved by the Board. The DBE confirmed that multiple level engagement is required to quantify the strategic, business and operational aspects of GP engagement which would be worked up through Executive Directors and re-presented to the Board in due course / NATIONAL NHS STAFF SURVEY SaTH RESULTS The WD informed the members that the NHS National Staff Survey took place between September December She reminded the Board that during this period, Unions were in dispute with the Government over pay. The survey consists of 120 questions and is based on the following four pledges: Staff Pledge 1: To provide all staff with clear roles and responsibilities and rewarding jobs for teams and individuals that make a difference to patients, their families and carers and communities Staff Pledge 2: To provide all staff with personal development, access to appropriate education and training for their jobs, and line management support to enable them to fulfil their potential Staff Pledge 3: To provide support and opportunities for staff to maintain their health, well-being and safety Staff Pledge 4: To engage staff in decisions that affect them and the services they provide, individually, through representative organisations and through local partnership working arrangements. All staff will be empowered to put forward ways to deliver better and safer services for patients and their families. 12 Chair
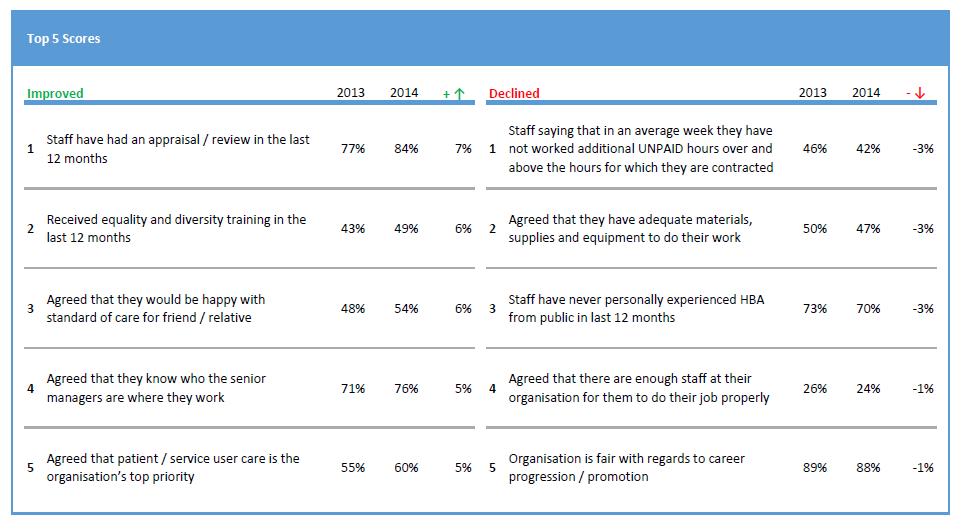
13 The WD presented the results which had been released by CQC (Presentation in Information Pack). The full report is available at The Trust has seen a 9% decrease in terms of response rate since the 2013 survey; with a total of just over 2,364 responses received. This is a response rate of 46% which is above average for Acute Trust s in England. An additional three themes were introduced this year; these relate to: Staff satisfaction Equality and diversity Patient experience measures The Trust s score for the overall indicator of staff engagement for SaTH equated to 3.62 (1 indicating that staff are poorly engaged [with their work, their team and their Trust], and 5 indicating that staff are highly engaged. The Trust s score was in the lowest (worst) 20% when compared with Trust s of a similar type. The Trust asked two additional questions one related to Workforce indicators and the other to Sustainability. The key areas that have seen the most improvement relate to: KF28. Percentage of staff experiencing discrimination at work in the last 12 months (Trust score 10%) KF19. Percentage of staff experiencing harassment, bullying or abuse from staff in the last 12 months (22%) KF17. Percentage of staff experiencing physical violence from staff in the last 12 months (2%) KR27. Percentage of staff believing the Trust provides equal opportunities for career progression or promotion (88%) KR20. Percentage of staff feeling pressure in last 3 months to attend work when feeling unwell (26%) The bottom five ranking scores relate to: KF29. Percentage of staff agreeing that feedback from patients/service users is used to make informed decisions in their directorate/department (44%) KF14. Fairness and effectiveness of incident reporting procedures (3.43) KF3. Work pressure felt by staff (3.20) KF15. Percentage of staff agreeing that they would feel secure raising concerns about unsafe clinical practice (62%) KF21. Percentage of staff reporting good communication between senior management and staff (24%) The CEO reported that he felt assured of the Trust s improved direction of travel; however it was suggested that further analysis be undertaken as there are wide variations in certain areas/groups. Mr Newman enquired if there is correlation of those departments against the CQC s outcomes. The WD confirmed that she would undertake this analysis before releasing results to Centres /034 HR POLICY PAPERS The WD presented the following Trust Policies for approval: HR11 Pay Protection o This policy has been updated to reflect changes to the length of pay protection and the section on excess travel entitlements has also be changed HR64 Sponsorship of Secondment of Healthcare Workers for Professional Registration Training o This policy has been updated to clarify the application and selection process, the eligibility criteria, the requirements for maintaining contact during training and the conditions for withdrawal, should this be required. The policy had been consulted with the Local Counter Fraud Team and comments received had been incorporated into the policy relating to restrictions around temporary employment during study periods, following acceptance of the point by Staff Side Representatives. Following discussion, the members APPROVED the two HR policies. 13 Chair
14 2015.2/035 BOARD ASSURANCE FRAMEWORK (BAF) The CEO introduced this item. He reminded the Board that the BAF enables the Board to provide evidence that it has systematically identified the Trust s objectives and managed the principal risks to achieving them. The proposed Board Assurance Framework had been discussed and outcomes agreed at the February 2015 Risk Committee meeting and is supported by the Trust s risk management processes. Changes since the previous presentation are highlighted and include additional assurance received. The BAF also includes the controls in place and sources of assurance, with the lead Director for each risk. It was confirmed that the arrows shown on the BAF relate to improvement and deterioration The CEO advised that after discussion the Risk Committee had agreed that CRR561 relating to Performance Standards should continue to be split into three categories given the improved position in relation to two of the areas; giving A&E targets (currently rated Red=); Cancer waiting times (currently Green ); and RTT targets (currently Green ), and that the residual risk ratings of each should be Amber/Green as the delivery remained fragile given the emergency operational pressures the trust was facing. The Risk Committee also discussed the strategic financial risk and agreed with the recommendation from Operational Risk Group that the Liquidity and Income & Expenditure categories of risk CRR670 relating to Financial and Investment Strategy should also be separated, given the non-repayable support PDC of 19.2m received from the Department of Health. Following discussion, the Board members agreed that the Liquidity risk rating should remain at Amber/Green but the I&E risk rating should be amended from Red= to Red. Action: DCG Amendment made to Board Assurance Framework. Action Completed /036 STANDING ORDERS, STANDING FINANCIAL INSTRUCTIONS AND RESERVATION OF POWERS TO THE BOARD The FD presented the Standing Orders, Standing Financial Instructions and Reservation of Powers and Delegation of Powers to the Board documents which have been reviewed and key changes outlined within the documents. Following discussion, the members APPROVED the documents /037 TRUST COMMITTEE MEETINGS UPDATE The Chair presented the following Trust Committee updates, for information: Audit Committee 12 February 2015; The members were informed that Internal Audit have made recommendation that Non-Executive Directors (NED) should confirm they were content with their oversight of discussions about the Trust s long term funding options. Following discussion, the Board members agreed that this is generally discussed during Board Development sessions and at Finance Committee rather than during formal Board meetings. The members confirmed that there is a high level of engagement and did not believe this needed further strengthening It was also noted that the WD had an outstanding action on the Board Governance Assurance Framework in relation to succession planning, which would be addressed through the Workforce Committee Workforce Committee 13 February 2015; The Committee had discussed their Terms of Reference and agreed the importance to ensure a strong focus on the organisations people agenda, focusing on strategy, current challenges and opportunities and performance. Risk Committee 19 February 2015; The Committee agreed proposed risk appetite statements which will be discussed at the April 2015 Trust Board. Action: CEO Due: April 2015 Trust Board Development session. Added to Board Development Programme. Action Completed. Quality & Safety Committee 18 February The members were informed that performance against the Ophthalmology 18-week standards is now being met and the processes that required improvement to reduce safety concerns have been substantially resolved. Finance Committee 24 February In relation to the Financial Strategy 2015/16; the report summarised that contract discussions are ongoing however the capacity effects of additional emergency demand remain across the cost base and income levels. The Committee remain 14 Chair
15 concerned that the key risks, especially those relating to the impact of excess demand, delayed transfer and structural inefficiencies continue to lie with the Trust than more evenly shared. Prospects of effective reduction of these demand levels are seen as limited. Emphasis was placed on these risks to be appropriately addressed across the health economy as the contract negotiations develop. The Board RECEIVED and REVIEWED the Committee updates /038 ANY OTHER BUSINESS No further business raised /039 QUESTIONS/COMMENTS FROM THE FLOOR The Chair asked for questions from the floor. Mr Sandbach reported that he had 8 questions and asked he if could forward 6 of these to the Chair separately. The Chair agreed this approach. Subsequent to the meeting the Trust sent Mr Sandbach a written response to all 8 Questions. Mr Sandbach asked the following two questions Relating to Agenda Item 17 - Annual Review of Standing Orders, Standing Financial Instructions (SFIs) and Scheme of Delegation: Q1 - Can wherever possible be inserted to (c) of the Standing Financial Instructions, i.e: (c) shall ensure that (where ever possible) the capital investment is not undertaken without confirmation of purchaser(s) support and the availability of resources to finance all revenue consequences, including capital charges. A1 - The written response confirmed that this would be considered the next time the SFIs were reviewed Q2 - Would the Board be willing to change the workflow systems and service locations? If by doing so risk, both clinical and financial, is significantly reduced and / or eliminated. A2 - The written response confirmed that the Trust uses the assessment of risk to review and revise our strategic and operational priorities on an ongoing basis. This is undertaken in a variety of ways, for example: Our plans and priorities for the coming year will be set out in the Operating Plan which we expect to present to the Trust Board for final approval later this year in the context of discussions with commissioners on the contract arrangements for 2015/16. Progress against our Operating Plan is reviewed through our Integrated Performance Report as well as through period updates on our operational objectives, including the Q3 report to the Trust Board. These reviews inform our assessment or risk and any in-year changes to our plans and priorities. The Trust s assessment of the principal risks is set out in the Board Assurance Framework, which was approved at the meeting of the Trust Board on 26 February The Trust s approach to risk management is set out in our risk management strategy, which was reviewed and approved by the Trust Board on 31 July A narrative summary of our approach to governance and risk management and how this has guided our decisions during the year is set out in the Annual Governance Framework which is published within the Annual Report. 15 Chair
16 Mr Rook of the Patient Experience and Involvement Panel (PEIP) raised the following issues: Q3 - CQC Inspection Action Plan The colours that feature within the Trust CQC Inspection Action Plan (blue and green) which appear to be misleading as the majority of Trust documentation is Red Amber Green (RAG) rated. A3 The CQC were content with the Trust s colour coding. This will be further discussed at at the Patient Experience and Involvement Panel (PEIP). Q4 - Lack of physiotherapy support on Ward 17 (Endocrinology and Care of the Older Person) at PRH - Identified following a recent Gemba Walk. It appears the Ward has one physiotherapist, and Mr Rook reported that the Physio had 22 patients to see and mobilise in one day. He therefore urged the Board to consider increasing the number of therapy support staff as this may have a bearing on the level of discharges. A4 - The issue of responding to Gemba Walk feedback is being addressed by the DNQ; and the COO is reviewing the level of therapy support staff. Q5 - Paediatric nurse staffing levels Mr Rook highlighted the 66% average fill rate of nursing and midwifery staffing levels on Ward 19 (Childrens Ward) at PRH and queried the safety of this level. A5 - The DNQ reported that this fill-rate level is due to the Childrens Ward and Childrens Assessment Unit being co-located. The staffing levels are risk assessed and the workload is managed appropriately. The DNQ confirmed that care is provided at the correct standard. Also, staff recruitment is currently taking place. Mr G Shepherd, Shropshire Patient Group Representative, raised the following questions: Q6 - Urgent Care Centre Mr Shepherd reported that the Walk-in Centre relocation to an Urgent Care Centre service at RSH received some negative publicity following the last Board meeting, which he does not feel is justified as the Centre has purely relocated from Monkmoor to the Urgent Care Centre at the RSH site. The members were informed that the processes at the front-door of the Urgent Care Centre are completely different; however we have noted that on average 27% of patients are utilising the Urgent Care Centre which is an improvement for the A&E Department. A6 - The CEO and COO supported Mr Shepherd s concerns and confirmed that the press article was not reflective of the service available. Following discussion, the COO agreed to hold a conversation with Mr Shepherd regarding the patient activity. Q7 - CQC Inspection Plan It was queried why some of the actions had only been implemented following the CQC Inspection and asked that there was a robust review to ensure all actions had been fully embedded. A7 - There is a quarterly review of progress with the CQC; the CQC will also re-inspect to ensure all actions are implemented. The action plan with also be monitored through the PEIP. The Chair thanked the members of the public for their comments during the Public session and highlighted that the Board are very appreciative of their time and work undertaken /040 DATE OF NEXT MEETING Formal Board Meeting Thursday at 2.00pm in the Lecture Theatre, Education Centre, Princess Royal Hospital The meeting closed at 5.20pm 16 Chair
17 MATTERS ARISING FROM THE PUBLIC TRUST BOARD MEETING ON 26 FEBRUARY 2015 Item Issue /007 3-Month Forward Plan To present the Patient Experience Strategy to the Board for approval /012 People Strategy Update Employee Engagement Employee engagement presentation to be provided to the June 2015 Trust Board /016 Questions from the Floor To provide an update in relation to End of Life Care to the April 2015 Trust Board ACTION DUE DATE OWNER DNQ September 2015 Added to Forward Plan Action Completed WD June 2015 Added to Forward Plan Action Completed DNQ April 2015 Added to Forward Plan Action Completed /021 Patient s Story To contact family personally Chair March /024 Actions/Matters Arising /012 People Strategy Update Recruitment To include information in IPR WD March 2015 In IPR. Action Completed /025 3-Month Forward Plan To present FCHS Post Project Review to July Trust Board DBE July 2015 Added to Forward Plan Action Completed /028 Q3 Progress Review To include RAG rating in future iterations of the reviews DBE September /029 CQC Inspection Action Plan To present to Quality & Safety Committee on a quarterly basis and to Board every six months To liaise with Chair to add Gemba Walks to his diary schedule To provide update to March Trust Board in relation to progress of Employee Engagement Strategy Well Led domain DNQ DNQ/Chair WD September 2015 Added to Forward Plan March 2015 March 2015 In Workforce Cttee Update Action Completed /032 GP Engagement Strategy To provide update to March Trust Board in relation to medical complaints /035 Board Assurance Framework To make the agreed amendments to the Board Assurance Framework (I&E risk should be amended from Red= to Red ) /037 Trust Committee Meetings Update To present Risk Appetite statements to April Trust Board Development Session MD March 2015 Agenda Item. Action Completed DCG March 2015 BAF Updated. Action Completed. CEO April 2015 Added to Board Development Programme. Completed. 17 Chair
18
19



20 Our Staff Survey Results 2014 Trust Board 26 February
21 Staff Survey The NHS National Staff Survey took place between October and December The survey reports 29 key findings. The survey asks questions based on the four pledges to staff from the NHS constitution. Pledge 1 To provide staff with clear roles, responsibilities and rewarding jobs For teams and individuals that make a difference Pledge 2 To provide all staff with personal development, access to appropriate training and line manager support Pledge 3 To provide support and opportunities for staff to maintain their health, wellbeing and safety Pledge 4 To engage staff in decisions that affect them and the services that they provide There were also 3 additional themes: Staff satisfaction, Patient experience and Equality & Diversity There are 2 types of key finding % score or scale summary score which is calculated by converting staff responses to particular questions into particular score therefore the minimum is 1 and the maximum 5. 2
22 Staff Survey Response Rate 2014 Trust Response 46% (down 9%) Average Acute Response 43% (down 7%) National Average Response 41% (down 8%) 3
23 Benchmarked results Above average 2 Average 6 Below average 10 Lowest 11 Distribution has changed 4
24 The Organisation 5

25 Recommend the trust as place to work and receive care 6
26 Friends and Family Test Q Question I would recommend this organisation as a place to work Friends and Family Test 57% Staff Survey 50% If a friend or relative needed treatment I would be happy with the standard of care provided by this organisation 67% 54% 7
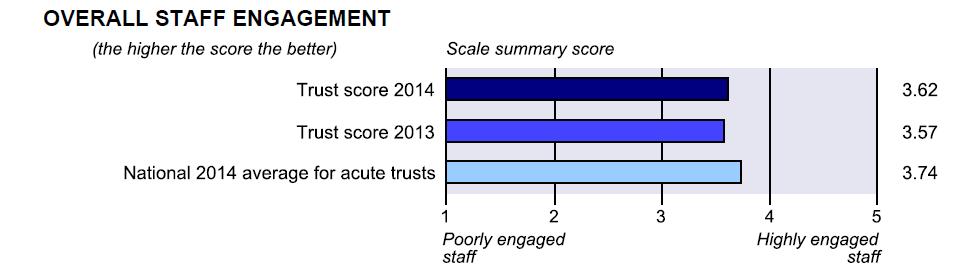
27 Staff Engagement 8
28 Our Values 79% of staff knew our Values 52% agreed the values were lived by staff 9





29 Our response Our commitments Focus on improvement Driven by staff 10
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Debbie Vogler, Director of Business & Enterprise. Kate Shaw, Associate Director of Service Transformation
 Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
PUBLIC SESSION MINUTES. Chair
 1 The Shrewsbury and Telford Hospital NHS Trust TRUST BOARD MEETING Held on Thursday 3 December 2015 Seminar Rooms 1&2, Shropshire Education & Conference Centre, RSH Paper 2 Present: In attendance Meeting
1 The Shrewsbury and Telford Hospital NHS Trust TRUST BOARD MEETING Held on Thursday 3 December 2015 Seminar Rooms 1&2, Shropshire Education & Conference Centre, RSH Paper 2 Present: In attendance Meeting
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
is asked to NOTE the update provided on fragile services.
 Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Charlotte Banks Staff Involvement Lead. Stage 1 only (no negative impacts identified) Stage 2 recommended (negative impacts identified)
 Stage 2 recommended (negative impacts identified)") Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Sarah Bloomfield, Director of Nursing and Quality
 Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Patient Experience Strategy. Director of Nursing & Quality
 Reporting to: Trust Board 2 February 2017 Paper 8 Title Sponsoring Director Author(s) Patient Experience Strategy Director of Nursing & Quality Graeme Mitchell Previously considered by Executive Summary
Reporting to: Trust Board 2 February 2017 Paper 8 Title Sponsoring Director Author(s) Patient Experience Strategy Director of Nursing & Quality Graeme Mitchell Previously considered by Executive Summary
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
Stewart Mason, Emergency Planning and Resilience Officer Tom Jones, Clinical Programme Manager
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Reporting to: Trust Board Meeting - 26 th June Title Integrated Performance Report - May 2014/15. Previously considered by Not Applicable
 Reporting to: Trust Board Meeting - 26 th June 2014 Paper 6 Title Integrated Performance Report - May 2014/15 Sponsoring Director Author(s) Peter Herring - Chief Executive Directors Previously considered
Reporting to: Trust Board Meeting - 26 th June 2014 Paper 6 Title Integrated Performance Report - May 2014/15 Sponsoring Director Author(s) Peter Herring - Chief Executive Directors Previously considered
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS 22 FEBRUARY 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
PUBLIC SESSION MINUTES. Chair. Director of Corporate Governance / Company Secretary
 1 Present: Mr P Latchford Mr H Darbhanga Mr C Deadman Dr D Lee Mrs T Mingay Mr B Newman Dr C Weiner Mr S Wright Dr E Borman Mrs D Kadum Mr N Nisbet Mrs D Fowler Mrs J Clarke The Shrewsbury and Telford
1 Present: Mr P Latchford Mr H Darbhanga Mr C Deadman Dr D Lee Mrs T Mingay Mr B Newman Dr C Weiner Mr S Wright Dr E Borman Mrs D Kadum Mr N Nisbet Mrs D Fowler Mrs J Clarke The Shrewsbury and Telford
Trust Key Performance Indicators
 Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
SUMMARY REPORT TRUST BOARD IN PUBLIC 3 May 2018 Agenda Number: 9
 SUMMARY REPORT TRUST BOARD IN PUBLIC 3 May 2018 Agenda Number: 9 Title of Report Accountable Officer Author(s) Purpose of Report Recommendation Consultation Undertaken to Date Signed off by Executive Owner
SUMMARY REPORT TRUST BOARD IN PUBLIC 3 May 2018 Agenda Number: 9 Title of Report Accountable Officer Author(s) Purpose of Report Recommendation Consultation Undertaken to Date Signed off by Executive Owner
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Report to: Trust Board 25 th April Enclosure 4. Title Integrated Performance Report March Sponsoring Executive Director
 Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Service Transformation Report. Resource and Performance
 SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
How CQC monitors, inspects and regulates independent doctors and clinics providing primary care
 How CQC monitors, inspects and regulates independent doctors and clinics providing primary care October 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor independent doctors and clinics
How CQC monitors, inspects and regulates independent doctors and clinics providing primary care October 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor independent doctors and clinics
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
An improvement resource for the district nursing service: Appendices
 National Quality Board Edition 1, January 2018 Safe, sustainable and productive staffing An improvement resource for the district nursing service: Appendices This document was developed by NHS Improvement
National Quality Board Edition 1, January 2018 Safe, sustainable and productive staffing An improvement resource for the district nursing service: Appendices This document was developed by NHS Improvement
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
APPENDIX 7C BENEFITS REALISATION PLAN
 APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Quality Assurance Committee Annual Report April 2017 March 2018
 Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Agenda Item number: 8.1 Enclosure: 3. Discussion. Date reviewed. 22 nd September
 Board meeting date: 27 th October 2011 Agenda Item number: 8.1 Enclosure: 3 Title Quality Report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Dr Alastair
Board meeting date: 27 th October 2011 Agenda Item number: 8.1 Enclosure: 3 Title Quality Report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Dr Alastair
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
Title of report Freedom to Speak Up Guardian (FSUG) Trust Board in public
 Trust Board in public") Title of report Freedom to Speak Up Guardian (FSUG) Trust Board in public Date: Thursday 26 th July 2018 Agenda item: 6.2 Executive sponsor Report author(s) Report discussed previously: (name of subcommittee/group
Title of report Freedom to Speak Up Guardian (FSUG) Trust Board in public Date: Thursday 26 th July 2018 Agenda item: 6.2 Executive sponsor Report author(s) Report discussed previously: (name of subcommittee/group
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
The Shrewsbury and Telford Hospital NHS Trust. Trust Board 24 th February The Future Configuration of Hospital Services Programme
 Enclosure 2 The Shrewsbury and Telford Hospital NHS Trust Trust Board 24 th February 2011 The Future Configuration of Hospital Services Programme Executive Lead Adam Cairns, Chief Executive Authors Kate
Enclosure 2 The Shrewsbury and Telford Hospital NHS Trust Trust Board 24 th February 2011 The Future Configuration of Hospital Services Programme Executive Lead Adam Cairns, Chief Executive Authors Kate
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
2011 National NHS staff survey. Results from London Ambulance Service NHS Trust
 2011 National NHS staff survey Results from London Ambulance Service NHS Trust Table of Contents 1: Introduction to this report 3 2: Overall indicator of staff engagement for London Ambulance Service NHS
2011 National NHS staff survey Results from London Ambulance Service NHS Trust Table of Contents 1: Introduction to this report 3 2: Overall indicator of staff engagement for London Ambulance Service NHS