Reducing Clinician Burnout in Implementing Chronic Care Management
|
|
|
- Damian Cummings
- 5 years ago
- Views:
Transcription

1


2 Reducing Clinician Burnout in Implementing Chronic Care Management
3 Learning Objectives Describe the benefits of Chronic Care Management (CCM) for patients and practices; Create a high-level workflow for CCM; Understand the barriers to CCM and strategies to overcome them; and Identify at least one process change to reduce clinician burden
4 Agenda Chronic Care Management (CCM) Overview Patient Benefits of CCM Services Practice Benefits of CCM Services Three Different CCM Approaches Utilizing Existing Practice Resources Outsourcing via Technology Pharmacy Partnering
5 CCM Overview and Benefits
6 Why CCM? CMS data shows two-thirds of Medicare beneficiaries have chronic conditions Chronic conditions are costly CCM contributes to better outcomes and higher patient satisfaction CCM helps patients better manage their care and focus on health and quality of life goals
7 CCM Description Chronic Care Management (CCM) services By: a physician or non-physician practitioners and their clinical staff For: patients with multiple (two or more) chronic conditions How often: 20 minutes or more per calendar month Separate billing codes established to provide payment for additional time and resources spent to provide between-appointment help patients need to stay on track with their care plans
8 Who Qualifies for CCM? Patients must have: Two or more chronic conditions expected to last at least 12 months, or until the death of the patient Examples include Alzheimer s Disease and related dementia, arthritis, asthma, cancer, cardiovascular disease, depression, diabetes, hypertension, obesity Chronic conditions place patients at significant risk Risk includes death, acute exacerbation or decompensation, or functional decline Establishment or revision of comprehensive care plan
9 Who Qualifies for CCM? Medicare Beneficiaries: All Part B recipients are covered Part B deductible and coinsurance apply Patients may also pay a monthly fee Inform patient before they agree to CCM services that a copay is required Informed consent can be verbal or written Collect copay at the time the CCM service is being performed to increase copay collection rate
10 CCM Service Line Target patients Use postcards or letters to inform them of service Have care team call and explain, obtaining consent Create, revise, or monitor care plan Work with patients on their plan Educate, motivate, check-in Repeat
11 CCM Service Line Target patients Educate, motivate, check-in Use postcards or letters to inform them of service Work with patients on their plan Have care team call and explain, obtaining consent
12 CCM Service Line Summary of CCM services: At least 20 minutes per month of CCM services Personalized care plan based on individual needs Coordinated care between doctor, pharmacy, specialists, testing centers, hospitals, and others Phone check-ins between visits 24/7 emergency access to a health care professional
13 Comprehensive Care Plans Care plan should include: A systematic assessment of the patient s medical, functional, and psychosocial needs System-based approaches to ensure timely receipt of all recommended preventive care services Medication reconciliation with review of adherence and potential interactions Oversight of beneficiary self-management of medications Care plan should be patient-centered and should be based on an environmental assessment of the patient s needs and available resources and support
14 Comprehensive Care Plan Elements Typically includes, but is not limited to: Problem list Expected outcome and prognosis Measurable treatment goals Symptom management Planned interventions and identification of the individuals responsible for each intervention Medication management Community/social services ordered A description of how services of agencies and specialists outside the practice will be directed/coordinated Schedule for periodic review and, when applicable, revision of the care plan
15 Asking for CCM Copay Use effective communication and language Ex: It is our payment policy to collect the appropriate payment due from the patient at the time services are rendered. Offer a script to front desk, clinical staff and patient schedulers Inform patient when on the phone or during a visit that there is a copay, patient will receive a bill, and there are different payment options Use appropriate language when collecting payment Ex: According to your insurance benefits, it shows that your financial responsibility includes a $ copay, % coinsurance, and a $ deductible
16 Billing for CCM CCM services may be billed by: Physicians Non-Physician Practitioners (NPPS): Physician Assistants, Clinical Nurse Specialists, Nurse Practitioners, Certified Nurse Midwives Rural Health Clinics (RHCs) Federally Qualified Health Centers (FQHCs) Hospitals, including Critical Access Hospitals (CAHs) *Note: only one physician, NPP, RHC, or FQHC and one hospital can bill for a patient during a calendar month
17 CCM Coding Summary Billing Code Payment Clinical Staff Time Care Planning Billing Practitioner Work Non-Complex CCM CPT Complex CCM CPT Complex CCM Add-On CPT 99489, use with CCM Initiating Visit (AWV, IPPE, TCM, or Other faceto-face E/M) Add-On to CCM Initiating Visit G0506 $43 20 minutes or more of clinical staff time in qualifying services Established, implemented, revised or monitored $94 60 minutes Established or substantially revised $47 Each additional 30 minutes of clinical staff time Established or substantially revised Ongoing oversight, direction and management Ongoing oversight, direction and management + Medical decision-making of moderate-high complexity Ongoing oversight, direction and management + Medical decision-making of moderate-high complexity $ Usual face-to-face work required by the billed initiating visit code $64 N/A Established Personally performs extensive assessment and CCM care planning beyond the usual effort described by the separately billable CCM initiating visit
18 The Value of CCM Patients benefit from CCM: Team of professionals to help plan for better health Ex: monthly check-ins, ready access to care team improved care coordination Patients receive a comprehensive care plan May receive list of suggested resources and community services Patients using CCM will receive needed support between visits Ex: Regular touch point may help patients be more engaged in their treatment plan, opportunity to articulate the importance of self-care such as diabetes testing and medication adherence
19 The Value of CCM Practice benefits from CCM: Improved care coordination: practice will receive payment specifically for managing chronic care patients Support patient compliance and help patients feel more connected Ex: some professionals credit CCM with improving patient satisfaction and compliance, decreased hospital and ED visits Sustainability and growth Ex: may help sustain ongoing care management work, help find new patient resources
20 The Value of CCM Business case for billing for CCM services: Payment rate for CPT 99490: $42.84 Revenue per physician: o Average patient panel for PCP: 1,450 (American Board of Family Medicine) o 17% of total population Medicare-eligible (Kaiser Family Foundation) o 2/3 of Medicare beneficiaries have chronic conditions (CMS) o 1,450 patients * 17% of patients * 2/3 with chronic conditions * $42.84 per CCM patient ~$7,069/physician annually ($589/physician monthly) 20
21 CCM Reimbursement Scenario One LPN in the practice is responsible for CCM: Spends 20 minutes on the phone with 165 patients per month for CCM services Total time spent: 55 hours Average monthly hours for 1 FTE: available monthly hours for other tasks (27 per week) Total revenue per month: 165 patients * $42.84 per patient = $7,069/month 21
22 CCM Reimbursement Scenario Monthly Revenue Potential % of CCM eligible patients: # of CCM Beneficiaries 100% 50% 25% LPN Hours LPN Gross Revenue LPN Net Revenue $7,069 $3,556 $1,756 $1,982 $(1,531) $(3,331) 22
23 CCM Methods in Practice
24 CCM Methods Prime Care Family Practice Utilizing Existing Practice Resources Bowie Internal Medicine Outsourcing via Technology Emporia Medical Associates Pharmacy Partnering
25 Utilizing Existing Resources: Prime Care Family Practice
26 Background: Prime Care Family Practice 7 clinician primary care practice in central Virginia Committed to starting CCM to: Provide a higher level of service to patients Create additional revenue stream Started with focus on Diabetes and Hypertension Began program by leveraging existing infrastructure and personnel Used nurse that was working on AWV and TCM to take over CCM
27 Barriers: Prime Care Family Practice Didn t think they had the time or resources to implement CCM Historically only had fragmented care management Engaging clinicians who already had a high degree of burden Difficulty efficiently scheduling patients Did not empanel patients patients going from physician to physician
28 Implementation: Prime Care Family Practice Clinicians continually review and modify protocols LPN manages patientcentered program Utilize EHR module to ID eligible patients LPN regularly communicates with patient to manage care Enrollment via shared decision making between patient and clinician Warm handoff to LPN who initiates care management activities
29 Results: Prime Care Family Practice Program Results Practice went from 1 billed CCM encounter in 2015 to 905 in 2016 Using existing infrastructure to build service Satisfier for patients and clinicians alike Success is reflected in quality scores compared to MIPS EHR benchmarks: NQF 0018 (Hypertension Control) 8th decile NQF 0059 (A1c Control) 9th decile 904 Additional CCM Encounters Billed from CY-2015 to CY-2016


30 Results: Prime Care Family Practice Better Care & Experience of Care Greater access to medical team Decreased risk of requiring ED or inpatient admission Lower long-term health care costs More Time at Top of License Reduced burnout thanks to team-based approach More productive visits for complex patients


31 Results: Prime Care Family Practice A Smooth-Running Practice Increased revenue stream from CCM billing Greater operational efficiencies Well-managed patients = happier patients Evidence of Transformation Developed patient and family-centered care design Optimized EHR Used data to drive change, improve operational efficiency, and use as a model for sustainable business operations
32 Outsourcing via Technology: Bowie Internal Medicine Associates
33 Background: Bowie Internal Medicine Associates 6 clinicians Serving community for 40 years Offers extended hours, patient portal Internally bills all of their own insurance statements and bills Incorporated the ideas and strategy of their whole team to make changes to CCM process
34 Barriers: Bowie Internal Medicine Associates Barriers to creating a CCM process: Developing a risk analysis system to determine whether patients could qualify for CCM Creation of a care plan documentation process through their EHR IMS/Meditab Documenting to support the coding of CCM codes 99487, 99489, and Calculating the time spent working with chronic care patients outside of their office visit appointments Distinguishing the level of decision making by clinicians regarding their patients
35 Implementation: Bowie Internal Medicine Associates Levering Technology: Chronic Care IQ CCM patients call CCM phone line Directed to provider s care team Length of call tracked and time stamped in patient chart Clinical staff makes any additional CCM documentation in chart via Chronic Care IQ CPT codes automatically generated and report able to be exported
36 # of CCM Services Billed Results: Bowie Internal Medicine Associates Chronic Care Management Services Billed 2000 Number of CCM Services Billed To Date Projection for CY % Relative Improvement from CY-2015 to CY CY-2015 CY-2016 CY-2017 Q Reporting Period





37 Results: Bowie Internal Medicine Associates CCM services resulted in: $ Increased revenue Improved continuity of care Better documentation Improved teamwork New leadership roles and responsibility Greater individual pride in work
38 Partnering with Independent Pharmacy: Emporia Medical Associates
39 Background: Emporia Medical Associates 4 clinicians High chronic care population Ranked 133 (last) in health outcomes in Virginia in 2017 Initiated CCM program partnering with an independent pharmacy first of its kind
40 Barriers: Emporia Medical Associates 1 clinician transitioning from paper charts to EHR 1 clinician out on medical leave Very busy, unsure how to incorporate needed service Pharmacy needed access to EHR

41 Implementation: Emporia Medical Associates 1. Recruit eligible patients 2. Create a care plan with a local pharmacy 3. Bill for CCM service 4. Reimburse pharmacy for CCM services and follow-up with pharmacy as needed 1. Monthly meetings with patient 2. Implements care plan 3. Reconciles medications and coaches patients 4. Coordinates data collection with practice 1. Monthly meetings with pharmacist 2. Medications are reconciled 3. Provided guidance for a healthy lifestyle 4. Provided tools for self-monitoring 1. CCM billing codes 2. Care plan 3. Patient education 4. Data collection

42 Resources: Emporia Medical Associates




43 Results: Emporia Medical Associates CCM services resulted in: Partnership with independent pharmacy 85% of patients kept CCM appointments 100% of patients reported improvement in quality of life after dieting and exercising Improved medication adherence and patient monitoring skills
44 # of CCM Services Billed Results: Emporia Medical Associates Chronic Care Management Services Billed Implemented service as a pilot with emphasis on diabetes + 2 more conditions 0 Clinician on medical leave, but able to continue, but not spread 20 Baseline Q Q Q Reporting Period 48 Continued commitment to service, expanding past diabetes % Relative Improvement from Q to Q Emporia Medical Associates has established an internal goal of billing 10 CCM services per clinician per month. This equates to a goal of 480 CCM services billed by the end of 2018.
45 Success: Emporia Medical Associates Patient Success: Patient A: did not know it was necessary to refrigerate insulin Patient now has better A1C levels Patient B: used same lancets for over a year, did not follow meal plans, did not maintain medication list Patient now has overall better health and less risk for infection

46 CCM Resources

47 Sample CCM Workflow

48 CMS Patient Postcard
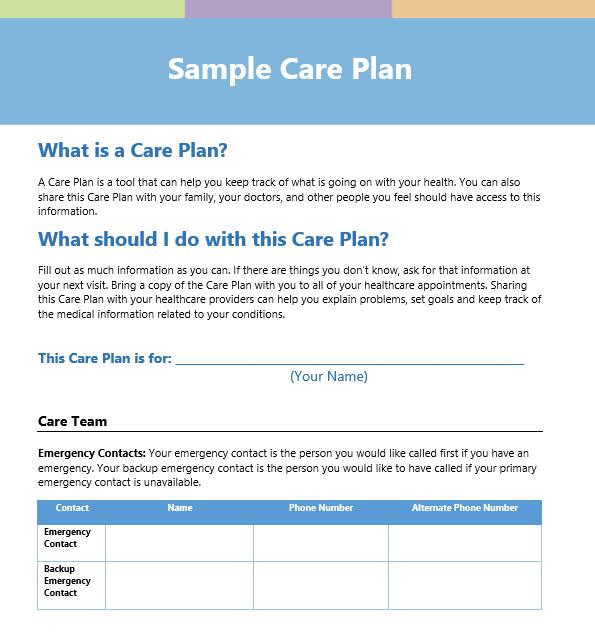
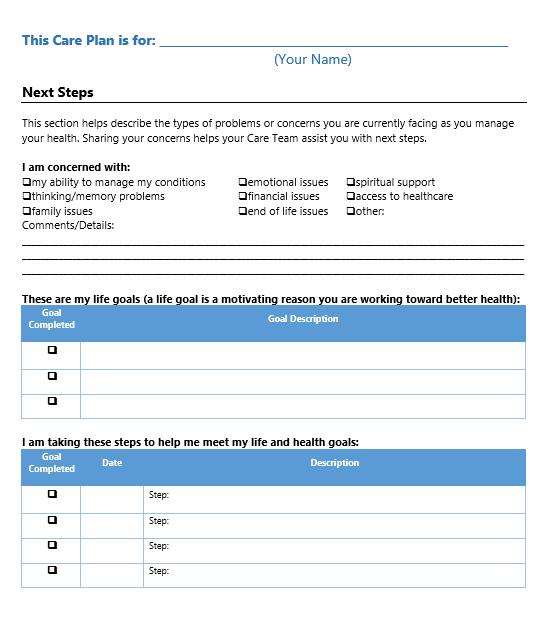
49 Sample Comprehensive Care Plan
50 Key Takeaways CCM can help: Patients Better manage and understand their care, engagement Practices Improved teamwork, documentation, and empowerment Providers Reduced burnout and reimbursement opportunities
51 Testimonials of Success: Any service that is patient centered, but also adds revenue to our business is welcome. -Pharmacist Partner This is an extra resource on top of whatever we are able to do, so the patient has another person helping them control their disease. Lead Clinician
52 Resources CMS Resources CMS CCM Tip Sheet CMS CCM Resource Center CMS Patient Postcard Other Resources HQI Video: A Partnership in Chronic Care Management HQI CCM Toolkit ACP CCM Toolkit AAFP CCM Resources AMA Steps Forward

53 Contact Information Virginia Brooks, MHA, CPHQ Vice President, Physician Services
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Transitional Care Management We provide these services a-la-carte...
 Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Chronic Care Management (CCM): An Overview for Pharmacists. March Developed Through a Collaboration Among:
: An Overview for Pharmacists. March Developed Through a Collaboration Among:") Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Chronic Care Management INFORMATION RESOURCE
 Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
WHY SHOULD A CHC/FQHC CARE?
 Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Providing and Billing Medicare for Chronic Care Management
 Providing and Billing Medicare for Chronic Care Management 2015 Medicare Physician Fee Schedule Final Rule November 2014 (PYA). No portion of this white paper may be used or duplicated by any person or
Providing and Billing Medicare for Chronic Care Management 2015 Medicare Physician Fee Schedule Final Rule November 2014 (PYA). No portion of this white paper may be used or duplicated by any person or
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
The Business Case for Chronic Care Management in the Ambulatory Care Practice
 The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
 2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Behavioral and Mental Health: High-Weighted. Behavioral and Mental Health: Medium-Weighted. Implementation of co-location PCP and MH services
 Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
New Options in Chronic Care Management
 New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
Cognitive Emotional Social Behavioral functioning
 TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual
 Program Training Manual") MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual September 2017 Table of Contents CCM PROGRAM OVERVIEW... 4 3 STEPS TO BEGIN CCM:... 5 Identify the Patient...
MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual September 2017 Table of Contents CCM PROGRAM OVERVIEW... 4 3 STEPS TO BEGIN CCM:... 5 Identify the Patient...
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Disclosure Statement
 2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE
 INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
3/28/2016. Evaluation and Management. Evaluation and Management Emerging Trends. Disclosures. Evaluation and Management The History
 Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Table of Contents for CCC Toolkit
 Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Using Updox to Succeed with MIPS
 Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Annual Wellness Visit (AWV) Delivery Business Case
 Delivery Business Case") Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
INTRODUCTION TO POPULATION HEALTH. Kathy Whitmire, Vice President
 INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Medicare Chronic Care Management. November 8, 2017
 Medicare Chronic Care Management November 8, 2017 2 Overview 1) Overview of the Medicare CCM program 2) Chronic Care Management 2018 Service Update 3) Implementing at your Organization 1) Key Questions
Medicare Chronic Care Management November 8, 2017 2 Overview 1) Overview of the Medicare CCM program 2) Chronic Care Management 2018 Service Update 3) Implementing at your Organization 1) Key Questions
Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future
 Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future No portion of this white paper may be used or duplicated by any person or entity for any purpose without
Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future No portion of this white paper may be used or duplicated by any person or entity for any purpose without
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM
 and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM") Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Choosing Improvement Activities
 Choosing Improvement Activities If you answer Yes to any of the questions, you may be eligible for the Improvement Activity listed. Do you remind pts of missed or overdue services? IA_PM_13 Do you have
Choosing Improvement Activities If you answer Yes to any of the questions, you may be eligible for the Improvement Activity listed. Do you remind pts of missed or overdue services? IA_PM_13 Do you have
NARHC Spring Institute
 NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities
 Annual training for delegated entities and facilities") 2018 MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities Quality Department CAN_2790318S CMS Requirements The Centers of Medicare & Medicaid Services (CMS)
2018 MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities Quality Department CAN_2790318S CMS Requirements The Centers of Medicare & Medicaid Services (CMS)
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
PROVIDER. Newsletter BETTER QUALITY IS OUR GOAL IN THIS ISSUE MEDICARE 2015 ISSUE II
 MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
MIPS Scoring: Explanation and Estimation 2/7/2017 and 2/10/2017
 CMS Transforming Clinical Practices Initiative and The Southern New England Practice Transformation Network (SNE PTN) MIPS 2017- Scoring: Explanation and Estimation 2/7/2017 and 2/10/2017 2 Review Determine
CMS Transforming Clinical Practices Initiative and The Southern New England Practice Transformation Network (SNE PTN) MIPS 2017- Scoring: Explanation and Estimation 2/7/2017 and 2/10/2017 2 Review Determine
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center
 Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles. November 12, Wisconsin Council on Medical Education & Workforce
 A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
Take Action Now to Avoid Medicare Penalties
 Take Action Now to Avoid Medicare Penalties The Centers for Medicare and Medicaid Services (CMS) says over 33,600 psychiatrists provide services reimbursed under Medicare Part B. The Merit-based Incentive
Take Action Now to Avoid Medicare Penalties The Centers for Medicare and Medicaid Services (CMS) says over 33,600 psychiatrists provide services reimbursed under Medicare Part B. The Merit-based Incentive
Documentation for CCC Reimbursement
 Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21.
 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Joy At Work - BellinHealth and HealthPartners
 Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
RE: CMS-1631-PM Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016
 September 8, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-2333-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Main Office
September 8, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-2333-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Main Office
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Improvement Activities Data Validation Criteria
 Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
Rural Health Clinic Billing
 Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?