John L. Bender, MD Julie DeSaire. IT Utilization: EHR and integrated Registry Functionality
|
|
|
- Shon Russell Adams
- 5 years ago
- Views:
Transcription

1 John L. Bender, MD Julie DeSaire National Priorities Partnership goal: Improving the health of the population IT Utilization: EHR and integrated Registry Functionality
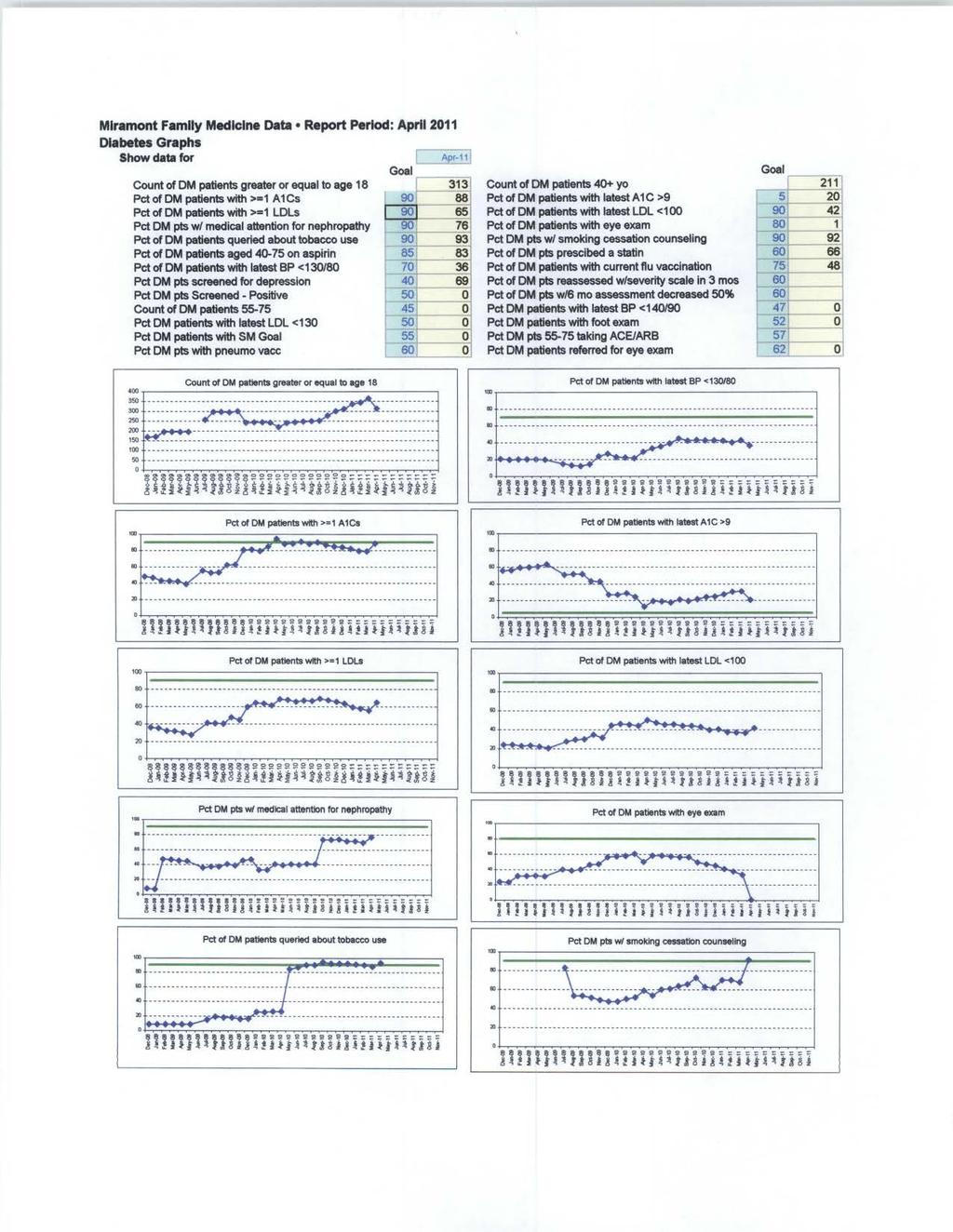
2 Stories of Success Miramont Family Medicine 2010 Davies Ambulatory Award Contact: John L Bender, MD and Julie DeSaire Title: Improving the Health of the Patient Population Utilizing our EHR, patient registry, and clinical based guidelines to engage our patients and improve outcomes. Background knowledge Miramont Family Medicine (MFM) has four locations in Northern Colorado, two in Fort Collins, one each in Wellington and Red Feather Lakes. MFM is a multi-specialty clinic of 13 providers and 50 employees. Our providers round at three hospitals and 11 nursing homes. We currently serve over 20,000 patients annually. We implemented our second EHR, e-md s in 2007, which can be accessed through a secure Virtual Private Network (VPN) connection from any location with internet capabilities. MFM has been named by the Northern Colorado Business Report as the 4 th fastest growing company, in our region, for Miramont Family Medicine s model for success is exemplary in a community where 34 Primary Care Physicians have either bankrupted or prematurely closed their doors in the last eight years. Local Problem Before implementing our EHR, we knew we had a diabetic population, but we would not have been able to run a simple report and tell you how many diabetic s we had in our practice, much less what their A1-C rates were. After the implementation, we found that the reporting capabilities of our EHR were not robust enough for our Patient Centered Medical Home. We engaged the use of Clinical Integration Networks of America (CINA) to mine our data. We felt like we were doing a good job of taking care of our diabetics, but once we had the data, we knew we needed to implement critical interventions to improve our outcomes. Our data showed us that we were only documenting 42% of our diabetics A1-C s and that 60% of those had an A1-C over 9.0. Through our patient centered medical home weekly meeting we developed systems of improvement. Intended Improvement Our initial aim was to decrease the A1-C scores of our diabetic population; however, we knew that we would need to design additional interventions to really impact our patient s overall health. We began with 3 objectives for our diabetic population, 1) document a current A1-C, 2) document a current LDL, and 3) evaluate the patient s feet. By utilizing our EHR s flowsheet, CINA was able to pull data into the registry that we could use to implement individual patient interventions. Patient care has definitely improved since we started using the EHR. As reported to our state registry, our diabetic patients are more compliant, more educated, and more engaged in their own healthcare. Our percentage of diabetic patients with documented A1-C s has gone from 42% to 88% and our A1-C s over 9.0 has dropped to 20%. (appendix A)
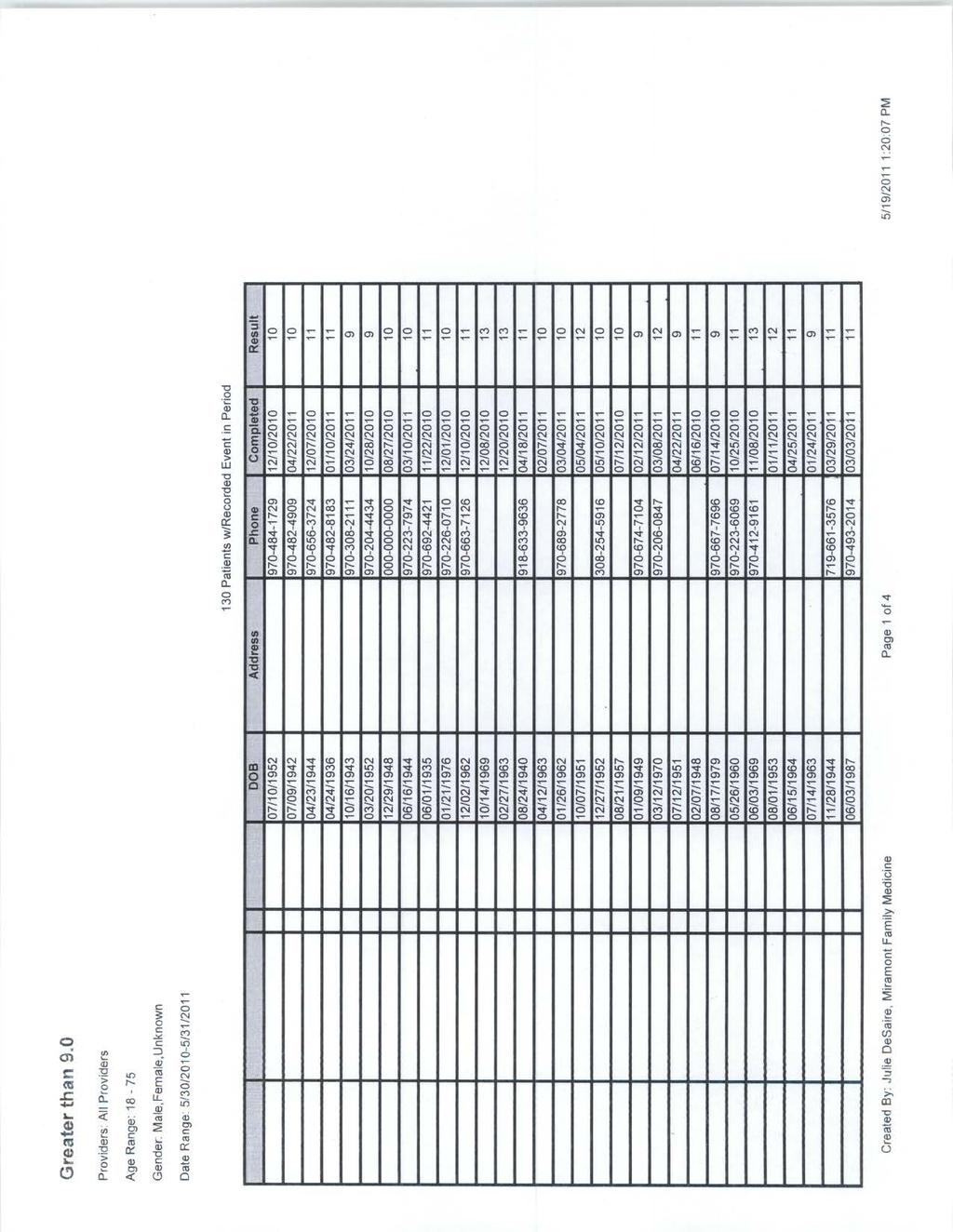
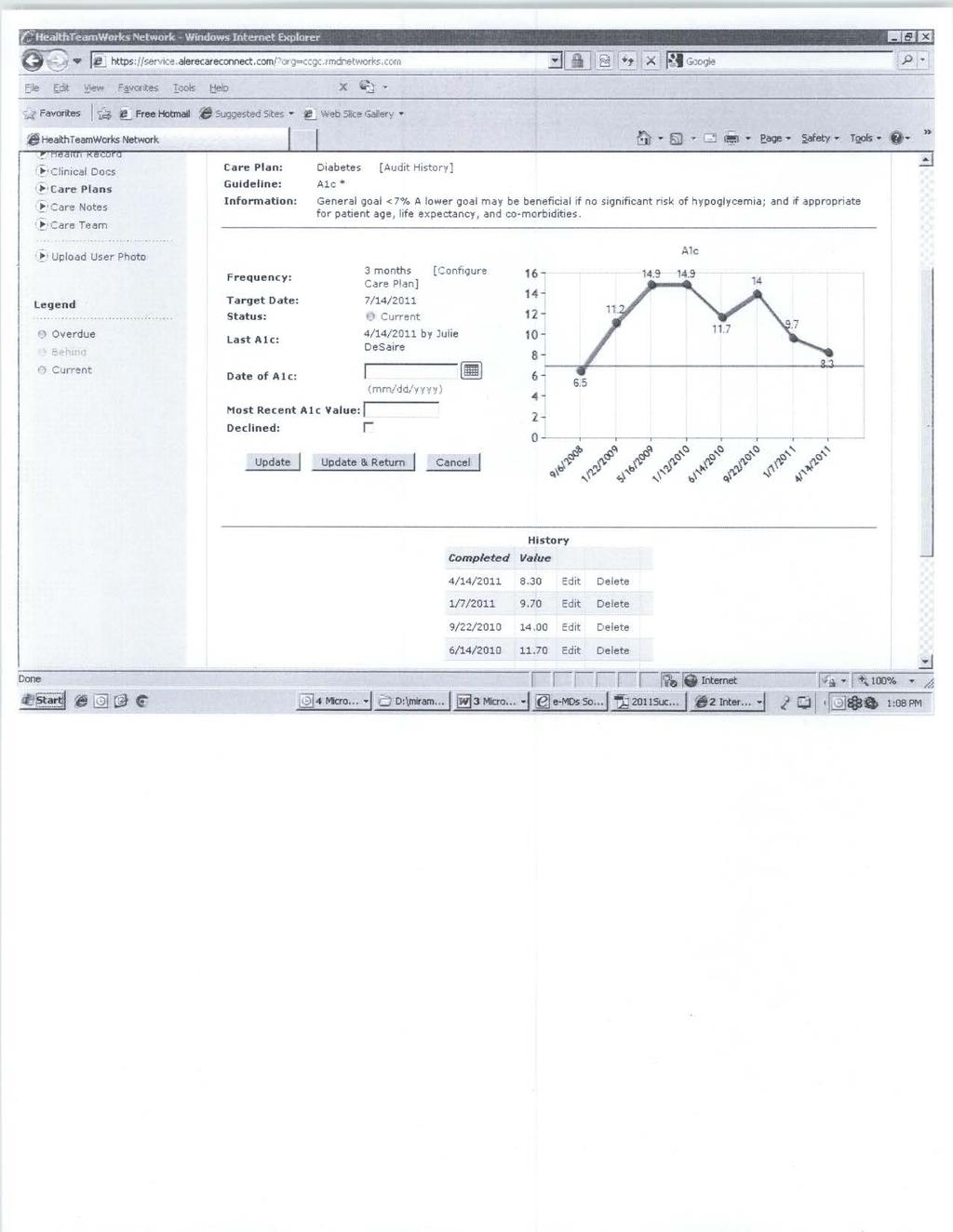
3 Planning the Intervention Miramont Family Medicine is a Level III, Patient Centered Medical Home, recognized by NCQA. We meet weekly to go over quality, safety, and efficiency issues within our practice. We utilize Lean Training and PDSA cycle testing to maximize improvement within our clinic. As part of our weekly Patient Centered Medical Home meetings we review specific patient reports regarding disease states that provide the most impact to the healthcare system. The chronic disease states that we are following include; diabetes, heart/stroke, prevention, and depression. We found through the reporting that in some areas of care we were doing a great job, where as in other areas we needed to step up our interventions to improve our outcomes. We used several different reports available to us through our EHR, our statewide registry and reports from CINA. (appendix B) to identify those patients that required intervention. We started by looking at patients that had an A1-C value over 9.0. We utilized our registry to report on the individual metrics. We then developed an intervention for these patients. We needed to get these patients back into the clinic and find out what their individual barriers to care were. We found that patients had socio-economic issues, apathy issues about their illness or were overwhelmed with what to do regarding their disease process. We developed a team approach to care involving not only the physician, but also the medical assistant, diabetic educator, and psychologist. For those patients that had apathy regarding their illness, our diabetic educator had them come in for one on one education about their conditions, creating awareness within the patients. She then added group classes for the patient to include the family or care givers. For patients that seemed to be overwhelmed, we included referrals to our in-house psychologist to help the patients that felt that they had no control over the process. Combining those visits with our diabetic educator eased those patients into education and group classes. For those patients that had socio-economic reasons for not coming in on a regular basis or not taking prescribed medications, we reached out to our medical community for assistance. We applied for grants to help patients cover the cost of care. We engaged our drug company representatives to help us with low cost or no cost pharmaceuticals for those patients that needed them. We these interventions we began to see the A1-C values fall. Before we began our interventions we showed that 56% of our diabetic population had an A1-C over 9.0 and after the intervention we showed that 20% of our population had and A1-C value over 9.0. (appendix C) We had a patient on our initial listing of patients with A1-C levels over 9.0, with an A1-C of While reviewing the patients chart, it was noted that the patient seemed to have some apathy in regards to his condition. He was a young man of only 19, and was covered under his parents insurance. We contacted the patient to have him come in and learned that he had dropped out of college and lost his health insurance coverage and had no funds to come in. We worked with the patient to get him into see our psychologist and diabetic educator and even saw the patient at no charge in order to improve his health. Our diabetic educator and psychologist were able to work with him to get re-enrolled in school and back on his parent s health plan. They worked on his nutrition and exercise habits and over time were able to lower his A1-C to 8.3, the lowest it has been since he started coming to our clinic. We continue to work with this patient and hope to see his A1-C drop below a 7.0. (appendix D) HIT Dimensions Utilized Miramont Family Medicine has committed to becoming the best patient medical centered medical home. As part of that commitment, we have implemented several different IT solutions. We utilize our EHR to not only chart our patient s care, but to also, e-prescribe, clinical decision support, physician order entry, flow-sheets, and document management. We have interfaced our
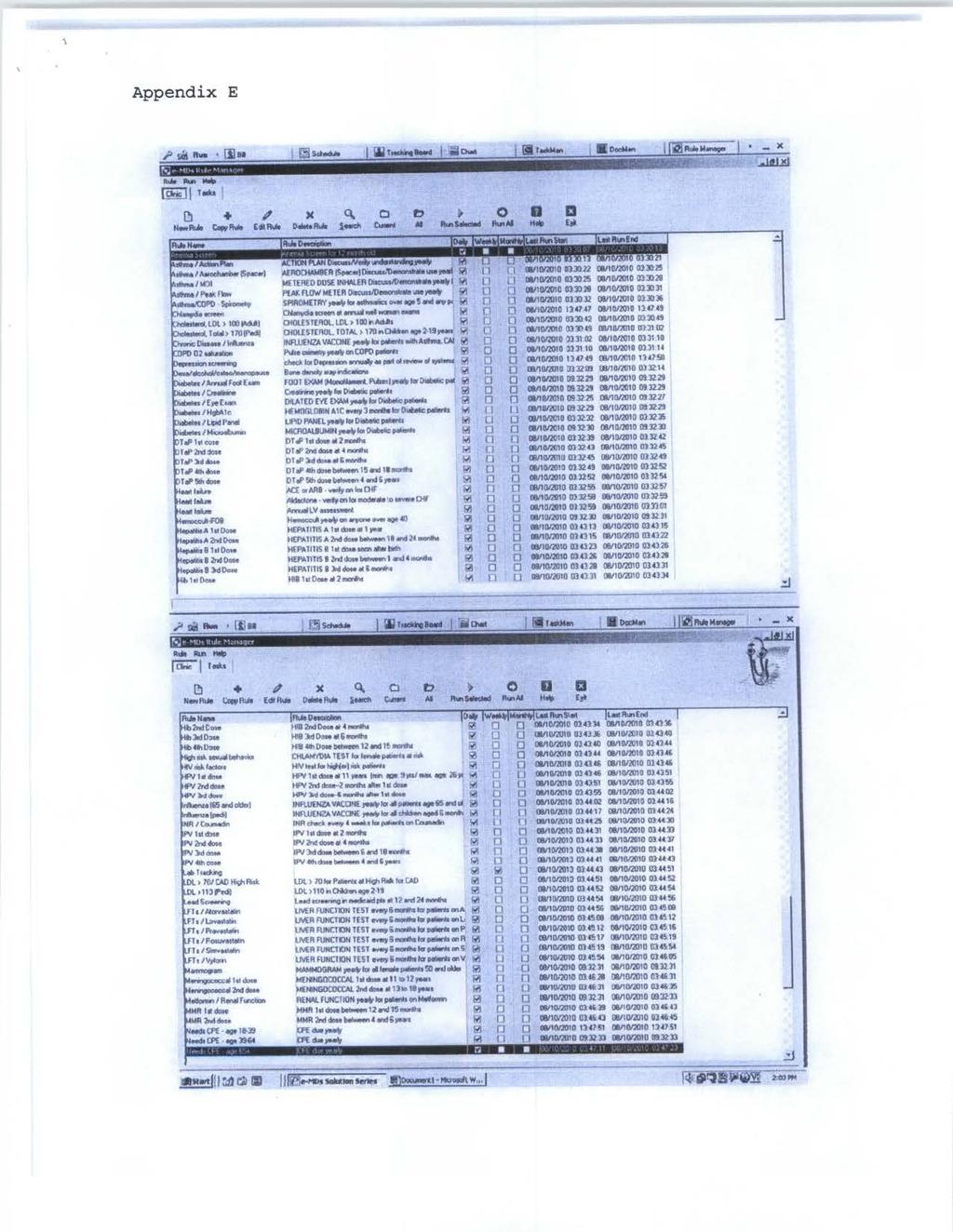
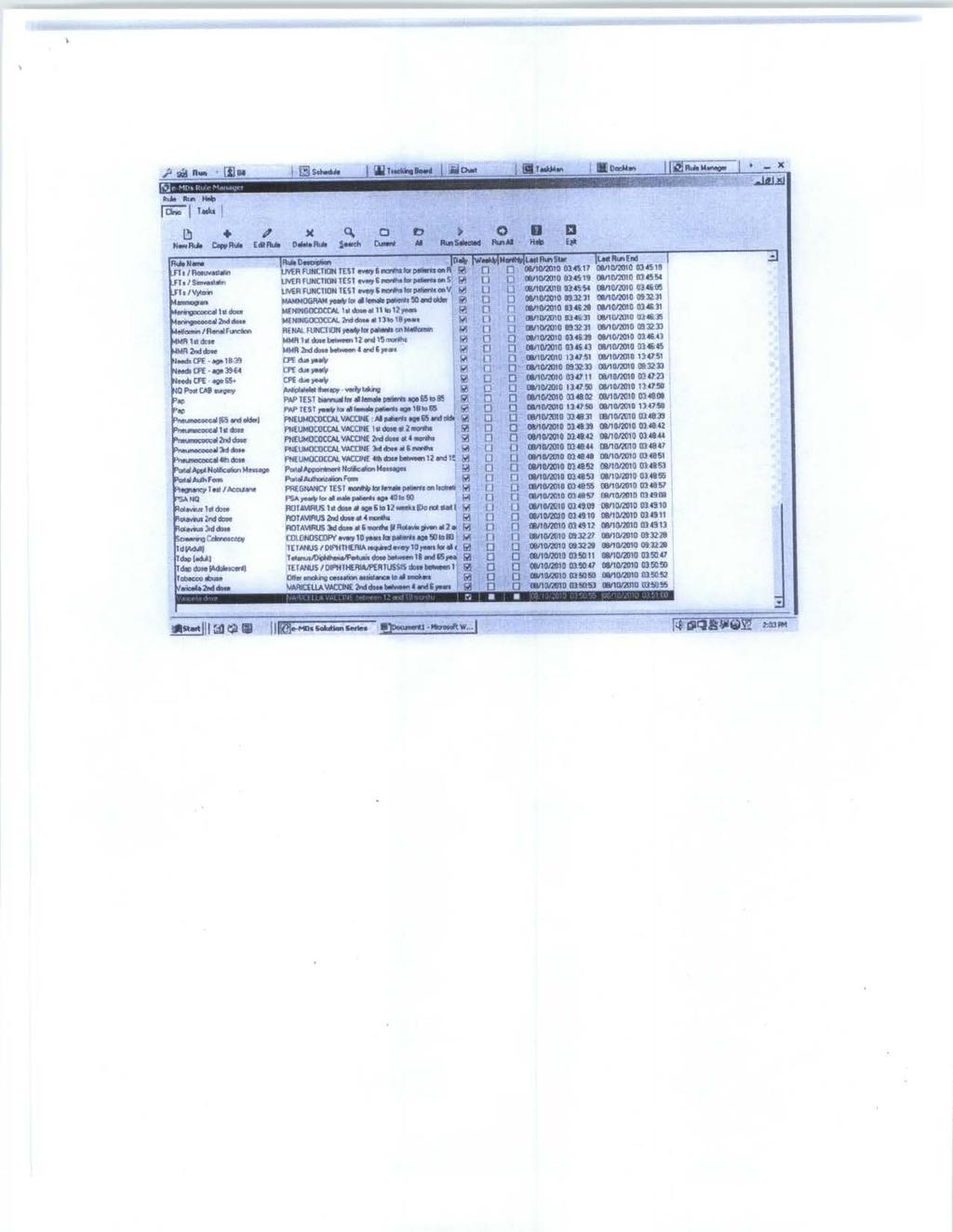
4 EHR with our hospital, clinical laboratories and state immunization information system. We added CINA to be able to provide immediate data on a patient level so that appropriate interventions could be done. Another functionality we use within our EHR for immediate data on the patient level is our Rules and Reminders. The use of the Rules and Reminders module has increased our patient compliance and revenues. The module runs a series of 187 rules chosen by the providers. The rules specify parameters for preventive services and certain tests such as a starting age for mammograms, or intervals for colonoscopy, or creatinine testing for a diagnosis of diabetes (appendix E). The rules algorithms are then run for all rules across the database of 20,000 patients, every night after the database backup is complete. In other words, the module checks the patient chart for CPT codes that match a specific test or procedure that the patient needs to have done on a regular basis, such as an A1-C in a diabetic, or a yearly mammogram. It then creates a work list that needs to be addressed as reminders attached to each individual patient chart and is present next time the chart is opened. The list can also be sorted as a function of recall, e.g. which patients are due for mammography at this time. Outcomes (a) Miramont Family Medicine has been involved with the Patient Centered Medical Home concept since 2007, when we first implemented our current EHR. Through the process we have learned what works, what doesn t, and where our best opportunities for bending the cost curve are. We know that managing our chronic care patients and keeping them out of the hospitals and ER s saves the system money. We manage change within our clinic by using PDSA cycle testing. We have found through small tests of change that we have a larger impact on our patients. If we find something that doesn t work, we can immediately switch gears to find something that will for that patient. One size does not fit all, but it fits most and with our willingness to make changes on the fly we are able to provide care in manner that is beneficial to all of our patients. When we plan for an intervention, we map the process, look for waste and efficiencies. Through this process, we find where we can have the most impact on patient care. Also through this process, we may find other steps that are labor intensive or duplicated and eliminate them. Outcomes (b) Improved outcomes has been our mantra for sometime. We get excited even if we are only able to move the bar by one patient. We have improved our metrics for diabetic care, heart/stroke, prevention, depression and obesity. Although, we are not at the levels we would like to be at, we continue to strive for perfection. Barriers Encountered We expected staff adoption to be our largest barrier. We also expected to have data collections barriers. We were able to eliminate the majority of data collection barriers with the implementation of CINA s data mining server. The staff adoption was a more difficult barrier. We broke through the barrier by using positive feedback to our providers and staff members. We used specific success stories by early adopters to reinforce why we were doing what we were doing. We created a positive, safe environment for discussion in PCMH meeting for staff to voice concerns. Finally, we used data collection and reports to show our progress, making it easier to accept our new models. Challenges Faced During our implementation process, we learned that our demographic data transfer had not been completed, causing a lot of duplicate work after we started using the system. Since we did not have live data to work with, we had to create simulated patients. Creating test patients and
5 simulated visits and billing took longer and overall delayed the implementation of the EHR. Any changes that we had made to improve templates for our work flow during this time were being reverted to the original settings when the data transfer took place. We then had to go back and modify them again. The data-transfer problem was corrected by the vendor before our go-live date. Looking back, we would have made sure that our data transfer was completed before our scheduled training. Challenges we expected included staff adoption at all of our locations, concerns from clinicians about being overwhelmed with to many steps they weren t prepared to address, in the allotted patient appointment time. We started this project at the main clinic, we utilized the clinical decision support system in all locations, and those other locations adopted the new approach in time as well. Moving new processes to the other clinics was a slower process and we needed to guard against any delay in adoption at the other clinics having a negative impact on the primary site. We believed with appropriate tracking and feedback of the effectiveness of screening and treatment we would be able to overcome any negative impact from the other clinics. Summary We are still working within the confines of our multi-stakeholder, multi-payor Patient Centered Medical Home pilot project are hoping that the results of our pilot will have an impact on healthcare delivery systems. We know that we are bending the cost of care curve in our practice and continue to work to ensure that our patient s conditions are well monitored and that appropriate interventions are utilized. The strength of our pilot project has been that we share our data with other practices in our pilot and by nature our doctors are competitive and in seeing that someone else is doing something different with a better result, we can share that information and test the process within our own practice and look for improvement. In the beginning, we didn t want to share our data as it was not very good; however, if it moved, we measured it, and it improved. Our lesson in improvement was even bad data can be improved upon. Interpretation Our outcomes have improved, but not as quickly as we had expected. We expected that the majority of patients would readily accept our new processes and would feel more engaged in their own healthcare; however, some patients felt that they were being pushed through the system. We had a medical house, but not yet a home. We continually work to improve our processes and systems and we are committed to delivering excellent, compassionate, modern, timely healthcare in an environment that promotes patient and staff growth, health and happiness. Conclusions The interventions we have done on behalf of our patients have improved the health of the patient populations. Our outcomes have improved with each patient visit and continue to put Miramont Family Medicine in front of the other pilots. We continually strive for excellence. We continue to add new projects and new metrics to our patient care model, knowing that what we have learned along the way can be used to integrate new services or new metrics. Financial Considerations Miramont Family Medicine subscribes to the doctrine that as Family Medicine providers we need to invest in ourselves. We have made friends with the lawyers, bankers and community leaders in order to increase our investment. We have invested over $200,000 into our EHR and IT closet and are willing to invest more if efficiencies and safety can be improved upon (appendix F). We have reaped the benefits of our investment by becoming part of the PCMH pilot project and other research project in which we are paid for our de-identified data. Cost savings have come from having a fully integrated EHR and practice management system.
6
7
8
9
10
11
12
13
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Core Item: Clinical Outcomes/Value
 Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Hillside Medical Office
 EHR Case Study Hillside Medical Office Hillside Medical Partners with Pulse to Quickly Achieve Meaningful Use pulseinc.com Pulse Complete EHR 8 board-certified physicians. 40 employees. Over 65 years of
EHR Case Study Hillside Medical Office Hillside Medical Partners with Pulse to Quickly Achieve Meaningful Use pulseinc.com Pulse Complete EHR 8 board-certified physicians. 40 employees. Over 65 years of
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Menu Item: Population Management
 Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
How to Register and Setup Your Practice with HowsYourHealth. Go to the main start page of HowsYourHealth:
 How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
The results will also be used for public reporting for MN Community Measurement on mnhealthscores.org.
 Introduction Welcome to the Health Information Technology (HIT) Ambulatory Clinic Survey. The Minnesota Department of Health (MDH) established the Minnesota Statewide Quality Reporting and Measurement
Introduction Welcome to the Health Information Technology (HIT) Ambulatory Clinic Survey. The Minnesota Department of Health (MDH) established the Minnesota Statewide Quality Reporting and Measurement
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Pursuing the Triple Aim: CareOregon
 Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Patient Centered Medical Home Clinician Assessment
 Patient Centered Medical Home Clinician Assessment Please answer the following questions based on the procedures and approaches used by you and your immediate care team (e.g. those nurses and office staff
Patient Centered Medical Home Clinician Assessment Please answer the following questions based on the procedures and approaches used by you and your immediate care team (e.g. those nurses and office staff
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Saint Francis Cancer Center Combines MOSAIQ, Epic and Palabra for a Perfect Documentation Workflow ONCOLOGISTS PALABRA: THE SOFTWARE ACTUALLY LOVE
 PALABRA: THE SOFTWARE ONCOLOGISTS ACTUALLY LOVE CASE STUDY CONTRIBUTORS Dr. Stephen Z. Sack, MD, Radiation Oncologist Tyleen A. Smith, BSN, RN, Clinical Manager Dr. Charles Stewart, MD, PhD, Radiation
PALABRA: THE SOFTWARE ONCOLOGISTS ACTUALLY LOVE CASE STUDY CONTRIBUTORS Dr. Stephen Z. Sack, MD, Radiation Oncologist Tyleen A. Smith, BSN, RN, Clinical Manager Dr. Charles Stewart, MD, PhD, Radiation
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
OPNS Suite of Products Opportunities Contact OPNS Informatics Department
 EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Requirements Document for the Blue Quality Physician Program sm Criteria Effective 08/03/2015
 All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings
 Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings INTRODUCTION Beginning in April 2012, providers that registered for the Michigan Department of Health and Human Services (MDHHS)
Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings INTRODUCTION Beginning in April 2012, providers that registered for the Michigan Department of Health and Human Services (MDHHS)
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
YOUR HEALTH INFORMATION EXCHANGE
 YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
Primary Care Specialist Physician Compact
 I. Purpose To provide optimal health care for our patients. To provide a framework for better communication and safe transition of care between primary care and specialty care providers. II. Principles
I. Purpose To provide optimal health care for our patients. To provide a framework for better communication and safe transition of care between primary care and specialty care providers. II. Principles
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Tribal Health. Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes
 Tribal Health Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes Join the Tribal Health leader Tap into the single, shared database of our EHR and practice management
Tribal Health Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes Join the Tribal Health leader Tap into the single, shared database of our EHR and practice management
FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017
 FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017 Do we have to do the quality measures that we have previously done from the
FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017 Do we have to do the quality measures that we have previously done from the
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA
 REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
Grove Medical Associates, P.C. A Case Study in Continuous Quality Improvement
 CASE STUDY The Organization Privately owned internal medicine practice 5 physicians, 1 location 9,000+ active patients The Challenge Find an Electronic Medical Record solution that would track continuous
CASE STUDY The Organization Privately owned internal medicine practice 5 physicians, 1 location 9,000+ active patients The Challenge Find an Electronic Medical Record solution that would track continuous
Tools for Better Health. Referral Toolkit. Health Care Providers
 Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Managing Population Health in Northeast Georgia: One Medical Group's Experience
 September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
UPDATE ON MEANINGFUL USE. HITECH Stimulus Act of 2009: CSC Point of View
 HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
2014, Healthcare Intelligence Network
 Note: This is an authorized excerpt from 2014 Healthcare Benchmarks: The Patient-Centered Medical Home. To download the entire report, go to http://store.hin.com/product.asp?itemid=4832 or call 888-446-3530.
Note: This is an authorized excerpt from 2014 Healthcare Benchmarks: The Patient-Centered Medical Home. To download the entire report, go to http://store.hin.com/product.asp?itemid=4832 or call 888-446-3530.
Component Description Unit Topics 1. Introduction to Healthcare and Public Health in the U.S. 2. The Culture of Healthcare
 Component Description (Each certification track is tailored for the exam and will only include certain components and units and you can find these on your suggested schedules) 1. Introduction to Healthcare
Component Description (Each certification track is tailored for the exam and will only include certain components and units and you can find these on your suggested schedules) 1. Introduction to Healthcare
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Residency PCMH Longitudinal Curriculum Competency Based Goals and Objectives
 PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare
: Billing, Codes and Need at Adelante Healthcare") Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Start Small, Think Big! Fusing Clinical & Business Metrics to Improve Quality & Effect Change. 44 accc-cancer.org July August 2016 OI
 Start Small, Think Big! Fusing Clinical & Business Metrics to Improve Quality & Effect Change 44 accc-cancer.org July August 2016 OI BY MELISSA CRONN AND LORRI SMITH, RN, BSN Words such as tranquility,
Start Small, Think Big! Fusing Clinical & Business Metrics to Improve Quality & Effect Change 44 accc-cancer.org July August 2016 OI BY MELISSA CRONN AND LORRI SMITH, RN, BSN Words such as tranquility,
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE
 9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
Example 1: Self-Management: Development of a Self-Management form, Part 1
 PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Using your EHR to Facilitate Effective Patient Population Management Real World Strategies. Jen Brull, MD Family Physician Plainville, KS
 Using your EHR to Facilitate Effective Patient Population Management Real World Strategies Jen Brull, MD Family Physician Plainville, KS Objectives Utilize both population health and patient-specific tools
Using your EHR to Facilitate Effective Patient Population Management Real World Strategies Jen Brull, MD Family Physician Plainville, KS Objectives Utilize both population health and patient-specific tools
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Recognition, Publications, & Activities
 Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE
 Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE CONTEXT Increasing number of critical access hospitals and other rural providers
Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE CONTEXT Increasing number of critical access hospitals and other rural providers
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs
 HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
Use of Information Technology in Physician Practices
 Use of Information Technology in Physician Practices 1. Do you have access to a computer at your current office practice? YES NO -- PLEASE SKIP TO QUESTION #2 If YES, please answer the following. a. Do
Use of Information Technology in Physician Practices 1. Do you have access to a computer at your current office practice? YES NO -- PLEASE SKIP TO QUESTION #2 If YES, please answer the following. a. Do
A Multi-Phased Approach to Using Clinical Data to Drive Evidence-Based EMR Redesign. Kulik, Carole Marie; Foad, Wendy; Brown, Gretchen
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Administrators. Medical Directors. 61% The negative impact on our hospital-based program s. 44% We will need to consider the most appropriate or most
 2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
Texas ACO invests in the Quanum portfolio to improve patient care
 Case study: Premier Management Company North Texas Texas ACO invests in the Quanum portfolio to improve patient care Premier Management Company (PMC) manages 3 accountable care organizations (ACOs) in
Case study: Premier Management Company North Texas Texas ACO invests in the Quanum portfolio to improve patient care Premier Management Company (PMC) manages 3 accountable care organizations (ACOs) in
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Naples Internal Medicine Associates
 CASE STUDY Implementing Chronic Care Management to Improve Patient Outcomes The Challenge How to effectively implement a Medicare rule that pays medical providers up to $42 per patient, per month, for
CASE STUDY Implementing Chronic Care Management to Improve Patient Outcomes The Challenge How to effectively implement a Medicare rule that pays medical providers up to $42 per patient, per month, for
Xtreme Makeover PCMH edition. The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference
 Xtreme Makeover PCMH edition The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference Conflict of Interest Disclosure John L. Bender, M.D. Has no
Xtreme Makeover PCMH edition The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference Conflict of Interest Disclosure John L. Bender, M.D. Has no
Tools, Resources and Modules
 SECTION 4 Tools, Resources and Modules Tools/Worksheets Tab A Resources/Glossary Tab B Modules Tab C TAB A Tools and Worksheets - 2 - Tools and Worksheets Table of Contents Action Plan Tool for Patient
SECTION 4 Tools, Resources and Modules Tools/Worksheets Tab A Resources/Glossary Tab B Modules Tab C TAB A Tools and Worksheets - 2 - Tools and Worksheets Table of Contents Action Plan Tool for Patient
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
Physician / Investigator. Over 40% of clinical trial data are entered into health record and EDC 1
 EHR4CR AN INNOVATIVE PLATFORM AND BUSINESS MODEL ACDM Annual Conference, 9 Richard Perkins, eclinical Forum Electronic Health Records for Clinical Research 1 Industry-centric growth in ICT 57% of R&D investment
EHR4CR AN INNOVATIVE PLATFORM AND BUSINESS MODEL ACDM Annual Conference, 9 Richard Perkins, eclinical Forum Electronic Health Records for Clinical Research 1 Industry-centric growth in ICT 57% of R&D investment
Bridging the Digital Divide: Patient-Focused Technology for Better Care Outcomes
 Bridging the Digital Divide: Patient-Focused Technology for Better Care Outcomes Jim Higgins Chief Executive Officer, Solutionreach Lehi, Utah Donna Scowden, Practice administrator. Peachtree Park Pediatrics
Bridging the Digital Divide: Patient-Focused Technology for Better Care Outcomes Jim Higgins Chief Executive Officer, Solutionreach Lehi, Utah Donna Scowden, Practice administrator. Peachtree Park Pediatrics
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Partners HealthCare Primary Care Quality and Patient Experience Reports 2017
 Partners HealthCare Primary Care Quality and Patient Experience Reports 2017 North Shore Health System QUALITYANDSAFETY.PARTNERS.ORG 1 INTRODUCTION Dear Patients, Colleagues and members of the Commonwealth
Partners HealthCare Primary Care Quality and Patient Experience Reports 2017 North Shore Health System QUALITYANDSAFETY.PARTNERS.ORG 1 INTRODUCTION Dear Patients, Colleagues and members of the Commonwealth
PATIENT CENTERED. Medical Home. Attestation. Facility Compliance
 2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs