Quality Care Collaborative Handbook
|
|
|
- Kathleen Lloyd
- 5 years ago
- Views:
Transcription
, an agency of the U.S. Department of Health and Human Services.")
1 Telligen Quality Care Collaborative Handbook This material provided by Telligen, the Medicare Quality Innovation Network Quality Improvement Organization for Illinois, handbook was prepared by CCME and resources were provided by the South Dakota Foundation for Medical Care, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-IL-C2-03/
2 TABLE OF CONTENTS Introduction 3 Section 1: Overview 5 Principles of Process Improvement 5 Section 2: Leadership and QAPI Steering Committee 7 Leadership Support 7 QAPI Steering Committee Goals and Responsibilities 7 Section 3: Performance Measurement 9 Section 4: Performance Improvement Project (PIP) 10 Plan-Do-Study-Act Cycle (PDSA) 10 Section 5: Evaluation 11 Section 6: Let s Get started with a plan for a PIP 12 Section 7: Appendices and Quality Improvement Tools 13 (Process Mapping, Brainstorming, Run charts, Benchmarking, Root Cause Analysis, PDSA, Dashboards) Section 8: Quality Improvement Tools and Examples 19 (5 Whys, Fishbone Diagram, PDSA Work Sheet, Goal Setting Work Sheet, Dashboard) Section 9: Recommended Tools and Resources 33 (QAPI at a Glance, Advancing Excellence, INTERACT, TeamSTEPPS) Reports from Telligen 42 Calculation of the Composite Measure 42 Nursing Home Composite Score Trending Graphs 43 Reports to Telligen 45 QAPI Self-Assessment (annually) 45 NHQCC Change Package 50 Contact Information 51 2
3 INTRODUCTION Data Driven Collaboration Data Tells a Story Data are facts used to analyze or plan something. These facts can be numbers, words, measurements, observations, or descriptions. Often the data collected needs to be translated into a form that is more convenient to use or easier to understand. For example, each resident has a health information record which contains numerous pieces of data about that individual. Similarly, each nursing home has a composite score comprised of numerous long-stay quality measures which are representative of systems-level data about that facility. All of the data pieces put together tell a more complete story than any one piece of datum by itself. A key, but often overlooked, step when working with data is to share the story the results with residents and family members; those individuals, regardless of their roles, providing care and services to residents; and the governing body of the long term care facility. Data are essential in helping us see a story as we navigate the change journey. Most good stories have a familiar plot: an explanation of the current state of affairs, setting off on a journey or transformation of some sort, followed by the introduction of new information, whereby a situation arises indicating a course correction may be in order decisions need to be made then descriptive anecdotes of cause and effect precede a conclusion. Thus, the plot line for performance improvement may be as follows: baseline data, working the Plan-Do-Study-Act method, attending to data trends and new information including best practices/guidelines and regulations using QAPI (Quality Assurance and Performance Improvement) tools, determining next steps and trying out small tests of change, then hard-wiring improvements at a systems level. Data-Driven Decision-Making Data s purpose is to allow a way for us to objectively measure performance over time. This is achieved by tracking data elements over time to identify trends, with the intent that what we do, our processes, influences results, or outcomes. Standardized performance measures (often spoken of as measures ) and data sets are tools which help us understand, manage, and improve care and services. Quality and safety are the most common categories of performance measures talked about in health care. The goal is to use data in a timely manner to address not only the immediate needs of residents but also to look at patterns for underlying causes in order to prevent the same problems from recurring; this requires a culture shift achieved by everyone committing to a Just Culture. For example, rather than spending time and energy putting out fires, the nursing home focuses efforts and resources on fire prevention. Working together in the collaborative makes this possible. Types of Data In order to determine the effective performance of nursing homes, data will be collected and reported: at the beginning of the collaborative, baseline data; throughout the collaborative, monthly or quarterly; and at the end of the collaborative. Data elements will include (but are not limited to): QAPI Self-Assessment Tool CMS 5-Star Quality Rating System NNHQCC (National Nursing Home Quality Care Collaborative) Composite Score Composition of QAPI Team and Champions for PIPs Resource utilization, such as Advancing Excellence and active participation in Learning Action Network (LAN) Areas of focus for Performance Improvement Projects (PIP) Communication plans for implementing successful strategies Tactics for integrating PIPs into QAPI program Procedures for accountability Evaluation of resources 3
4 In order to determine the effectiveness of the QIN/QIO (Quality Innovation Network/Quality Improvement Organization), data will be collected prior to and throughout the collaborative and reported as aggregates to nursing homes and the broader health care community. The data elements are as follows: Collaborative structure involving three states Recruitment of nursing homes Enrollment process and obtaining Participation Agreements Nursing home engagement, including participation of residents LAN effectiveness, pertaining to content and format Rapid cycle tests of change Peer Coaching Targets for specific quality measures (for example, decrease in antipsychotic prescription use and increase mobility) Engagement of stakeholders in the long term care community Resource utilization and comparison with other QIN/QIO nationally The collaborative efforts of all participants create a way to share expertise on a larger scale. For instance, nursing homes will individually report its QAPI Self-Assessment Tool to the QIN/QIO and the QIN/QIO will report aggregate findings to nursing homes, as well as comparing baseline data to data 18 months later at the end of the collaborative. 4
5 SECTION 1 Overview A Process Improvement plan (example QAPI Plan) serves as the foundation of the nursing home s commitment to continuously improve the quality of the care it provides. Quality services are safe, effective, resident centered and timely. Ongoing improvement of care is a commitment to: Evidence-based, effective practices. Providing care in a timely and efficient manner, with appropriate coordination and continuity across all phases of care and departments. Honor resident s needs and wishes. Individual needs and expectations of residents and families are respected. Residents or those whom they designate have the opportunity to participate in decisions regarding their treatment. Services are provided with sensitivity and caring All adverse events are tracked and analyzed. Risk to residents, providers, and others is minimized, and errors in the delivery of care are prevented Principles of Process Improvement Quality improvement (QI) is a systematic approach to assessing and improving care on a priority basis. The approach to QI is based on the following principles: Resident Focus: Services are based on meaningful resident and family dialogue to promote and preserve wellness and to expand personal choice. This approach promotes maximum flexibility and choice to meet individually defined goals and to permit person-centered services. Staff Empowerment: Effective programs are based on meaningful and respectful relationships among members of the staff and between staff and residents. QI depends upon staff who are trained and empowered to work as a team in real time to problem solve and use critical thinking skills to improve resident outcomes. Leadership Involvement: Strong leadership that provides direction and support of QI activities is key to performance improvement. Involvement of organizational leadership ensures that QI initiatives are consistent with the mission, values, and goals of the facility. Data Driven Practice: Successful QI processes create feedback loops, using data to inform the practice and measure results. Fact-based decisions are likely to be correct decisions. The most common mistake is not closing the feedback loop. QI Tools: For continuous improvement of care, tools and methods are needed to foster knowledge and understanding. Tools such as run charts, cause and effect diagrams, process maps, and dashboards are used by staff to turn data into useful information for improving care. Root cause analysis (RCA) and Plan-Do-Study- Act (PDSA) are methods to drive critical thinking and problem-solving. Prevention Over Correction: Quality Assurance Performance Improvement (QAPI) is proactive and drives good processes to achieve excellent outcomes rather than fix processes after the fact. Continuous Improvement: Processes must be continually reviewed and improved. Small incremental changes do make an impact providers can always find an opportunity to make things better. No matter what barriers exist in a nursing home environment, incremental change is possible. Team Based: Interdisciplinary teams which include frontline staff drive the work of improvement. A QAPI Steering Committee provides overall management of process improvement, and determines the focus of activities. Performance Improvement Projects (PIPs): Individual QI projects called PIPs, are used by teams to address identified outcomes and processes that need improvement. 5
6 Just Culture: Organizations respond to errors by examining their systems and processes, not by blaming individuals. Unintentional errors are differentiated from intentional errors or reckless behavior. Leadership maintains a balance between justice and accountability by focusing on systems and identifying opportunities for learning rather than on one individual who can be blamed for the error or unexpected outcome. Focus of activities Note: When necessary Administration, Medical Directors and Nursing leaders are responsible for maintaining accountability of individual s performance to adhere to consensus-based expectations which support resident safety. Everyone in the organization helps promote quality by coaching each other when behavior breeches are observed. 6
7 SECTION 2 Leadership and the QAPI Steering Committee Leadership Support The Quality Assurance Performance Improvement (QAPI) Steering Committee provides ongoing operational leadership of performance improvement activities at the nursing home. Core membership should include the director of nursing (DON), administrator, and medical director and department heads. This committee identifies the goals and specific objectives to be accomplished each year and oversees the progress of QAPI. The goals include training of clinical and administrative staff on performance improvement principles and specific QI initiatives. Progress in meeting these goals and objectives is an important part of the annual evaluation of QI activities. Leaders support QI activities through the planned coordination and communication of measurement results related to QI initiatives. The goal is every employee of the nursing home who provides care or service is able to speak to his/her role in QAPI. Leaders ensure that staff, residents and family members are aware and have input into QI Initiatives. They charter performance improvement project teams and provide resources, guidance that support to the teams. This planned communication can take place through a variety of methods for example: Storyboards and/or posters of teamwork, PIPs, and data trends displayed in common areas. Resident and family participation in QI through satisfaction surveys and family councils. Committee reports to staff, residents, and families. Distribution of newsletters and/or handouts about QI projects. Discussion during department and team meetings. QAPI Steering Committee Goals and Responsibilities Short-term goals: Indicate a plan for facility-wide QAPI training. Describe the plan to provide staff time and equipment for training as needed. Long-term goals: Implement quantitative measurement to assess key processes and outcomes. Identify sources of data that you will monitor. Describe the process for collecting and analyzing data. Develop a data tracking system (i.e., dashboard) to display and track monthly data of selected outcome measures and process measures (Process Measure Framework Tool). Bring together managers, clinicians, and frontline staff to review quantitative data and major clinical adverse events to identify and describe problems. Focus on process and not individual performance. 7
8 Plan education and training on best practices to managers, clinicians, and frontline staff. Develop or adopt necessary tools, such as practice guidelines and satisfaction surveys. Monitor new processes and evaluate if the outcomes achieve the goal. Meet performance improvement goals and internal and external reporting requirements. Steering Committee s Responsibilities: 1. Develop and approve a facility wide QAPI plan and review annually. 2. Establish a meeting format that includes: schedule, agendas, minutes and method for communicating with all members. 3. Develop a method to document meeting agendas/minutes, PIPs, PDSAs etc. 4. Complete the QAPI Self-Assessment and review at least annually. 5. Develop indicators of performance on a priority basis and evaluate routinely. 6. Establish measurable objectives based upon priorities identified through the use of established criteria. 7. Formally adopt a systematic approach to QI, using PDSA. 8. Charter and support specific QI initiatives or Performance Improvement Projects. 8
9 SECTION 3 Performance Measurement Performance Measurement is the process of regularly assessing the results produced by systems of care. It involves identifying processes, systems, and outcomes that are integral to the performance of the care delivery system; selecting indicators of these processes, systems, and outcomes; and analyzing information related to these indicators on a regular basis. CQI (Continuous Quality Improvement) involves taking action as needed based on the results of the data analysis and the opportunities for improvement they identify. The purpose of performance measurement is to: Identify problems and opportunities to improve the selected processes and enhance outcomes. Assess the stability of processes or outcomes to determine whether there is an undesirable degree of variation or a failure to perform at an expected level. Assess the outcome of the care provided. Assess whether a new or improved process meets performance expectations. Measurement and assessment involves: Selection of a process or outcome to be measured on a priority basis. Identification and/or development of performance indicators for the selected process or outcome to be measured. Aggregating data so that it is summarized and quantified to measure a process or outcome. Assessment of performance with regard to these indicators at planned and regular intervals. Taking action to address performance discrepancies when indicators show that a process is not stable, is not performing at an expected level, or represents an opportunity for QI. Reporting within the organization on findings, conclusions, and actions taken as a result of performance assessment. 9
10 SECTION 4 Performance Improvement Project (PIP) The QAPI Steering Team continuously reviews the nursing home s performance data. This is an agenda item for every meeting. Once the performance of a selected process has been measured, assessed, and analyzed, the information gathered from the performance indicator(s) is used to identify a Performance Improvement Project or PIP to be undertaken. Based on priorities established by the QAPI Steering Team, the decision to undertake the initiative is made and a PIP charter is completed. The basic model staff can use to conduct a PIP is called Plan-Do-Study-Act (PDSA). The PDSA cycle is a systematic method with a track record for achieving effective, reliable and consistent results. Data drives improvement efforts. The QAPI Steering Team analyzes data to determine which process or system needs improvement. Data sources can be CASPER (Certification And Survey Provider Enhanced Reports) data, audits, incidents, inspection results, complaints, surveys and other internal tracked items. The purpose of an initiative is to improve the performance of existing services or to design new ones. Plan-Do Study-Act (PDSA) Plan. The first step involves identifying opportunities for improvement. At this point, the focus is to analyze data, identify concerns and determine new potential outcomes. Ideas for improving processes are identified. Staff and residents that are involved or affected are identified, data is compiled, and solutions are proposed. This step requires the most time and effort. Do. This step involves implementing the proposed solution usually on a trial basis on one unit. Conducting a smallscale pilot of the proposed change is always recommended. Study. At this stage, data are again collected to compare the results of the new process with those of the previous one. Did the changes make a difference in the area you were trying to improve? Did the changes result in the outcomes you wanted? If not, why. What did the team learn? Act. Does the change need to be adapted and re-studied? Can the change be adopted and extended to other areas? At this stage, the PIP team involves others who will be affected by the changes, those whose cooperation is needed to implement the changes on a larger scale, and those who may benefit from what has been learned. Finally, it means documenting and reporting findings and following up. PAN A CT D O S TUDY 10
11 SECTION 5 Evaluation A first step is the completion of the QAPI Self-Assessment. This is an annual evaluation conducted by the QAPI Steering Committee and kept on file, along with the (QI Plan) written QAPI plan. The QAPI Self-Assessment is an evaluation tool created for nursing homes to use. It is completed at least annually to evaluate QAPI overall. This tool is composed of 24 statements that prompt a nursing home s QAPI team to discuss and exam their systems and processes throughout the facility and determine the performance indicators the nursing home will use to measure if the objectives are being achieved. The following summarizes the points that are captured in the 24 statements on the QAPI Self-Assessment. The QAPI Framework tool is an all-inclusive list of tools. Tools for annual activities and useful to assess improvement, sustainment and progress are available on the QAPI website, Provider-Enrollment-and-Certification/QAPI/NHQAPI.html. The evaluation summarizes: The goals and objectives of the facility-wide QI Plan. The QI activities conducted during the past year, including the targeted process, systems, and outcomes. The performance indicators utilized. The findings of the measurement, data summaries, assessment, and analysis processes. The QI initiatives taken in response to the findings. Annual activities and useful tools to assess improvement sustainment and progress include: 1. Monitoring the progress towards meeting the annual QAPI goals and objectives. Tools the team can use are QAPI Self-Assessment and Measure/Indicator Development Worksheet. 2. On the QAPI Self-Assessment, include a brief summary of progress and include notes in the appropriate section of each of the 24 statements on The QAPI Self-Assessment. 3. Provide a brief summary of the findings for each of the other performance tools and the indicators you used during the year. These summaries should include both the outcomes of the measurement process and the conclusions and actions taken in response to these outcomes. For each PIP, provide a brief description of the activities that took place, including the results. What are the next steps? How will you hold the gains? Team can use the following tools: Performance Improvement Project (PIP) Inventory, Measure/Indicator Collection and Monitoring Plan and Sustainability Decision Guide. 4. Based upon the evaluation, state the actions your team determined to be necessary to improve the effectiveness of the QI Plan in the coming year. 11
12 SECTION 6 Let's get started with a plan for a performance improvement project STEP 1: STEP 2: STEP 3: STEP 4: STEP 5: STEP 6: STEP 7: STEP 8: STEP 9: Use available data to identify and prioritize systems and processes to improve. Select the process to be improved and establish a well-defined process improvement goal. The goal may be established by the team. What do we want to improve? Use the SMART formula to help describe your goal: Specific, Measurable, Attainable, Realistic, Timeframe. (e.g. useful tool: Worksheet to Create PIP Charter & Goal Setting Worksheet). Organize a PIP team to improve the process. This involves selecting the right people to serve on the team and identifying the resources available for the improvement effort, such as people, time, money, and materials (e.g. useful tool: Performance Improvement Project (PIP) Launch Checklist). Defines the current process using a flowchart or process map. This tool is used to generate a step-by-step map of the activities, actions, and decisions which occur between the starting and stopping points of the process (e.g. useful tool: Flowchart Guide). Examines the process and simplifies it by identifying and removing redundant or unnecessary activities. People may have seen the process on paper in its entirety for the first time in Step 3. This can be a real eyeopener which prepares them to take these first steps in improving the process. Identifies the baseline by developing a plan for collecting data. This data will be used as a yardstick for comparison later (e.g. useful tool: Measure Indicator Collection and Monitoring Plan). Assess data trends. The team creates a run chart or other graph from data collected in Step 5 to gain a better understanding of what is happening in the process. The follow-up actions of the team are dictated by whether cause variation is found in the process. Identify the root causes that prevent the process from meeting the objective. The PDSA cycle starts here, using the flowchart or process map from step 4, brainstorming and root cause analysis to generate possible reasons why the process fails to meet the desired objective (e.g. useful tool: Guide for Performing Root Cause Analysis (RCA) with Performance Improvement Project (PIP) & PDSA Cycle Template). Begins running PDSA cycles to test the change based on the possible reasons for the process s inability to meet the objective set for it. These root causes were identified in Step 7. The planned improvement involves revising the steps in the simplified process map created in Step 4. Collect data and add to a run chart. Assess where the change improved the process. Run PDSA cycles until the PIP team agrees the change idea should be implemented facility wide, modified or abandoned. Modify the data collection plan developed in Step 5, if necessary. STEP 10: Establish ongoing monitoring of improvement for sustainment (e.g. useful tool: Sustainability Decision Guide). Congratulations! You have just completed your first PDSA cycle. 12
13 SECTION 7 Appendices Quality Improvement Tools Appendix 1: Process Mapping Recognizing A Change in Condition Map out the steps to a process in a linear path and note any components to the right that are essential to that specific step in the process. Process Mapping as a QI exercise compares the policy and procedure to the actual way a process is occurring. It allows for identification of deviations. The use of process mapping with a team allows staff to pinpoint exact opportunities for improvement. EXAMPLE OF A PROCESS DESIGNED TO REDUCE AVOIDABLE HOSPITAL READMISSIONS Resident has a change in condition Observe the change, complete the Stop and Watch tool CNA notifies nurse immediately Nurse assesses resident and gathers relevant information Vital signs Cognitive level review S/S of reported concern Nurse reports change of condition to physician Complete SBAR prior to call Gather chart Notify supervisor Nurse records orders in chart Repeats to confirm Nurse initiates orders Notify family Explain plan of care to resident 13
14 Appendix 2: Brainstorming & Root Cause Analysis Brainstorming is a tool used by teams to bring out the ideas of each individual and present them in an orderly fashion to the rest of the team. Brainstorming provides an environment free of criticism. Team members generate issues and agree to defer judgment on the relative value of each idea. Brainstorming is used when one wants to develop a large number of ideas about issues to tackle, possible causes, approaches to use, or actions to take. Brainstorming is a good time to think outside the box. It fosters new ideas which can lead to creative solutions. The advantages of brainstorming are that it: 1. Rapidly produces a large number of ideas. 2. Equalizes involvement by all team members. 3. Fosters a sense of ownership in the final decision as all members actively participate. 4. Provides input to other tools, such as a Fishbone Diagram or other RCA tool. 5. Encourages creativity and critical thinking. Root cause analysis (RCA) is a systematic process for identifying the most basic factors/causes that underlie variation in performance. It helps teams determine what happened, why it happened, and how to reduce the likelihood of it happening again. First, the team must identify the underlying cause of a problem before members can identify effective interventions that can be implemented in order to make improvements. Focus on systems and processes, not individual performances. Individual blame never serves the QI process well. One RCA technique is the 5 Whys Tool that helps to promote deep thinking about a specific problem that doesn t appear to be too complex. First, accurately state the complete problem. Second, ask why this problem is taking place. Record all answers. For each of the broad answers given, ask a series of whys until there is no further new information provided or the information provided by the team becomes redundant. Encourage complete honesty, and be determined to get to the bottom of the problem and to resolve the issue. Another method to guide and document the RCA process is the Fishbone Diagram. It helps the team identify, sort, display, and analyze multiple possible causes of a more complex problem for which hidden causes are suspected or for which interventions have not corrected or sustained. The Fishbone is also a RCA process the can address problems with a history or are known to be more challenging to manage. The problem or adverse event is written in the box on the right. Boxes at the end of the larger bones are general categories used to guide the discussion. For most issues in nursing homes, the categories are staff factors, care methods, environmental factors, and equipment factors. These categories, however, can be adapted as needed. List causes for each category, filling in the smaller bones of the fish. Begin with the most obvious causes. Then keep adding causes to produce the detail needed for future critical thinking about solutions. 14
15 Appendix 3: Run Charts A run chart is the most basic tool to show how a process performs over time. Data points are plotted in order on a line graph. Run charts are most effectively used to assess process stability through a visual display of variation. A run chart can help to determine whether or not a process is stable, consistent, and predictable. Simple statistics such as median and range may also be displayed. The run chart is most helpful in: 1. Understanding variation in an outcome or process performance. 2. Monitoring performance of a process or outcome over time to detect signals of change. RUN CHART Facility-Acquired Pressure Ulcers Note: The diagram can include a trend line to identify possible changes in performance. 15
16 Appendix 4: Benchmarking A benchmark is a point of reference by which something can be measured, compared, or judged. It can be an industry standard against which a performance indicator is monitored and found to be above, below, or comparable to the benchmark. National and state benchmarks are provided for all quality measures (QM). For example, the current national average for all reporting nursing homes in the United States for the percent of longstay residents who received an antipsychotic medication is 23.4 percent. The current average in North Carolina is 20.8 percent. A new national benchmark is a 15 percent reduction. If your facility s average is 25 percent, how do you compare to the state and national averages? What would be your new benchmark with a 15 percent reduction? Currently your facility is 1.6 percent above the national average and 4.2 percent above the state average. With a 15 percent reduction, the new benchmark for your facility would be 21 percent. For some measures, internal benchmarking is more appropriate. In this case, for example the number of falls per month, a facility might trend their monthly rate for the previous year using a run chart. Based on the variation, the team would then set an internal benchmark for a new target number of monthly falls. The new benchmark for number of falls per month might be a reduction of 20 percent or it might be a specific number, e.g., less than 12 falls per month. 16
17 Appendix 6: PDSA Cycle Each performance improvement project, or PIP, requires careful and organized planning by the assigned team. Using Plan-Do-Study-Act (PDSA) as a formal problem-solving model helps the team manage and complete the process in a systematic and logical manner. Suggested activities for each component of the PDSA cycle are: 1. Plan a. Develop or design a new process or improve an existing process you have identified. b. Decide how you will test the new process. c. Investigate and integrate evidence-based practices into your design. d. Identify measures that can be used to determine if new strategies are successful in improving the outcome. e. Determine what data are needed and how to collect the data for measurement. f. Get the right people involved in development and testing. 2. Do a. Using a small scale pilot project, run the test of the new or redesigned process. b. Collect data. c. Document observations, both expected and unexpected. 3. Study a. Analyze data and test results. b. Determine whether the change was successful. c. Identify challenges, barriers, and lessons learned. d. Summarize what you learned from the test. e. Share results with everyone impacted and get feedback. 4. Act a. If needed, modify and re-test the change. b. If successful, spread the change to other units. c. If unsuccessful, abandon it and develop a new approach to test. 17
18 Appendix 7: Dashboard A dashboard provides an easy at-a-glance view of key performance indicators identified by the QAPI Steering Committee as critical to successful provision of quality care. While some data measures will be common throughout all nursing homes, each facility s dashboard is unique based on its mission, values, and goals. Dashboards are visual summaries of key trends, comparisons, and exceptions. In order to be effective, dashboards must be simple with minimal distractions and be organized within the visual presentation of information. Dashboards come in many forms and may use a variety of numbers and graphs. Examples of visual tools used to illustrate data on a dashboard include a pie chart, bar chart, funnel, line graph, or run chart. To be useful, the data in dashboards must include real time data. Teams need current information. Dashboards also show historical trends of the organization s key performance indicators. This allows teams to make sound, informed decisions in a timely manner. 18
19 SECTION 8 Tools and Examples Five Whys Worksheet Accurately state the problem. (5 Whys is used in trouble shooting, quality improvement and problem solving. It is best suited for simple or moderately complex problems.) PROBLEM: Why is this happening? Enter all the reasons why. You may need more boxes. For each reason, begin asking WHY. REASON #1 REASON #2 REASON #3 WHY? WHY? WHY? WHY? WHY? WHY? WHY? WHY? WHY? WHY? WHY? WHY? 19
20 Five Whys Worksheet Example Accurately state the problem. PROBLEM: Rise in number of facility-acquired Stage III pressure ulcers from 0 to 3 on Unit One during September Why is this happening? Enter all the reasons why. You may need more boxes. For each reason, begin asking WHY. REASON #1 Poor positioning REASON #2 Lack of consistent skin inspection by frontline staff REASON #3 Low protein and caloric intake of high-risk residents WHY? Lack of accessible positioning equipment WHY? Charge nurse does not hold CNA accountable. WHY? Not enough attention during mealtimes to individual residents WHY? Supplies not on unit and difficult to obtain WHY? Skin condition not part of routine shift reports WHY? Insufficient staffing for so many residents that need mealtime assistance WHY? Few extra pillows and many old cushions WHY? No longer using pink skin inspection sheet WHY? Lack of support from other staff during busy times and staff schedules WHY? Low priority for administration WHY? Not a priority; too many other things going on WHY? Always been this way 20
21 Root Cause Analysis Using the Fishbone Diagram Ideas for Brainstorming: 1. Staff Factors Lack of knowledge and training, staffing levels, scheduling, lack of communication, low accountability, poor teamwork 2. Care Methods Processes not followed, lack of documentation, shift-to-shift breakdown, insufficient rounding, low anticipation of resident needs 3. Environmental Factors Lack of safety inspection and correction of hazards 4. Equipment Factors Broken or lost equipment, incorrect devices in use, insufficient supply, low budget priority 21

22 Root Cause Analysis Using the Fishbone Diagram Ideas for Brainstorming: 1. Staff Factors Lack of knowledge and training, staffing levels, scheduling, lack of communication, low accountability, poor teamwork 2. Care Methods Processes not followed, lack of documentation, shift-to-shift breakdown, insufficient rounding, low anticipation of resident needs 3. Environmental Factors Lack of safety inspection and correction of hazards 4. Equipment Factors Broken or lost equipment, incorrect devices in use, insufficient supply, low budget priority 22
23 23
24 24
25 e ove Mr. Bro c air alar or 7 ay ri g e ay i i o i crea e i all. o alar ill e e ro 7 a a e ill o ex erie ce a all. a. o i g 4 P every o r.. E gage er i gro ac ivi ie o i e er roo. c. o ac era y a, a i i ia e re ora ive rogra or a la io, re g e i g, a ala ce. e ove alar. Mr. Bro i c c e le i a la o rly ro i g. o i y ac ivi ie irec or o a e a e gage re i e. o i y re ora ive a o e roll re i e a egi rogra. O lar ill o e e. o all ill occ r. er o all e o alar ro 7 a
26 lar a re ove or o e ee, a e ree ra egie ere i le e e. Mr. Bro a o all. a i c l or a o ro every o r. Mr. Bro i o ay i gro ac ivi ie. a i e i e ore eci c oile i g a er, ai, a er o al ee ro g 4 P ro i g roce. e l a c e o erva io, a e re i e ee ere i e i e. o a o i y. e ove alar er a e ly. c ivi ie a o ex lore ore o Mr. Bro er o al i ory a e gage i ore ea i g l ac ivi ie. a o a ici a e oile i g a o i io i g ee i e i e ri g ro i g. o i e ai e ica io or ai i e i e ri g ro i g. e ora ive rogra o co i e. 26
27 Goal-Setting Worksheet Goal setting is important for any measurement related to performance improvement. This worksheet is intended to help teams establish appropriate goals for individual measures and also for performance improvement projects. Goals should be clearly stated and describe what the organization or team intends to accomplish. Use this worksheet to establish a goal by following the SMART formula outlined below. Note that setting a goal does not involve describing what steps will be taken to achieve the goal. It is helpful to post the written goal somewhere visible and regularly communicate the goal during meetings in order to stay focused and remind caregivers that everyone is working toward the same goal. Describe the problem to be solved: Use the SMART formula to develop a goal: SPECIFIC: Describe the goal in terms of three W questions. What do we want to accomplish? Who will be involved and who will be affected? Where will it take place? MEASURABLE: Describe how you will know if the goal is reached. What is the measure you will use? What is the current data figure (i.e., count, percent, rate) for that measure? What do you want to increase/decrease that number to? 27
28 ATTAINABLE: Defend the rationale for setting the goal measure above. Did you base the measure figure you want to attain on a particular best practice or average score or benchmark? Is the goal measure set at the right mark to be challenging without being unreasonable? RELEVANT: Describe how the goal fits into your QI Plan. Briefly describe how the goal being set will address the problem stated above. TIME-BOUND: Define the timeline for achieving the goal. What is the target date for achieving this goal? GOAL STATEMENT: 28
29 Goal-Setting Worksheet Goal setting is important for any measurement related to performance improvement. This worksheet is intended to help teams establish appropriate goals for individual measures and also for performance improvement projects. Goals should be clearly stated and describe what the organization or team intends to accomplish. Use this worksheet to establish a goal by following the SMART formula outlined below. Note that setting a goal does not involve describing what steps will be taken to achieve the goal. It is helpful to post the written goal somewhere visible and regularly communicate the goal during meetings in order to stay focused and remind caregivers that everyone is working toward the same goal. Describe the problem to be solved: Our retention of newly hired CNAs is low. This causes interruptions in resident care and negatively affects staff performance. Use the SMART formula to develop a goal: SPECIFIC: Describe the goal in terms of three W questions. What do we want to accomplish? Reduce turnover rate of new CNAs Who will be involved and who will be affected? Nursing staff and those responsible for the hiring process Where will it take place? During the interview and hiring process MEASURABLE: Describe how you will know if the goal is reached. What is the measure you will use? Number of CNA terminations within 6 months of hire What is the current data figure (i.e., count, percent, rate) for that measure? 50 percent turnover What do you want to increase/decrease that number to? Decrease to 25 percent 29
30 ATTAINABLE: Defend the rationale for setting the goal measure above Did you base the measure figure you want to attain on a particular best practice or average score or benchmark? Internal trends and corporate benchmark Is the goal measure set at the right mark to be challenging without being unreasonable? Yes RELEVANT: Describe how the goal fits into your QI Plan. Briefly describe how the goal being set will address the problem stated above. Will improve consistency of care, help improve communication and build teamwork, and improve quality of resident care TIME-BOUND: Define the timeline for achieving the goal. What is the target date for achieving this goal? Within the next six months GOAL STATEMENT: We will reduce the percentage of CNA terminations within the first 6 months of their hire date by 25 percent over the next 6 months as documented by the DON in employee records. Goal statement examples: 1. Increase the number of long-term residents with a vaccination against both influenza and pneumococcal disease documented in their medical record from 61 percent to 90 percent by December 31, For the next 30 days, hold a 5 10 minute team huddle using the Post-Fall Investigation form within one hour after 100 percent of resident falls on Unit B. This huddle will be directed by the charge nurse and attended by unit CNAs, therapy, ADON, and nurse supervisor. The ADON will track all huddles and falls during this period. 3. Reduce the number of facility acquired Stage III pressure ulcers in long-stay residents from 6 to 0 by December 31, 2013, as documented in the medical record and internal monitoring sheet. 30

31 Dashboard Examples 31
32 References: Bowers B, Nolet K, Roberts T, Esmond S. Implementing Change in Long-Term Care: A Practical Guide to Transformation. University Wisconsin Madison School of Nursing; Implementation_Manual_Part_1_FINAL.pdf. Accessed March 8, Centers for Medicare and Medicaid Services. Nursing Home Quality Assurance and Performance Improvement. cation/ surveycertificationgeninfo/qapi. htmlassurance. Accessed March 7, Institute for Health Care Improvement (IHI). How to Improve. HowtoImprove/default.aspx. Accessed March 7, Isabella Corporation Project. Getting Better All the Time: Working Together for Continuous Improvement. New York: Cobble Hill Health Center and Isabella Geriatric Center; gettingbetterall-the-time.pdf. Accessed March 8, Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance (2nd edition). San Francisco: Jossey-Bass Publishers; New York State Office of Mental Health, Office of Quality Management website. Quality Improvement Plan Template. Accessed January 3, Planetree and Picker Institute. Long-Term Care Improvement Guide. Planetree Project Team pickerinstitute.org/publications-and-resources/. Accessed March 8,

33 SECTION 9 Recommended Tools and Resources Nursing Home QAPI CMS Resources QAPI will take many nursing homes into a new realm in quality - a systematic, comprehensive, data-driven, proactive approach to performance management and improvement. This guide provides detailed information about the nuts and bolts Telligen recommends you download and save a copy of the QAPI at a Glance as well as save the QAPI website as a favorite for future reference. Additional tools and resources for implementing QAPI can be found at the CMS Website: 33

34 Data Collection Tools Recommended by Telligen Telligen recommends the use of the free tracking tools developed by the Advancing Excellence Campaign in America s Nursing Homes. The Advancing Excellence in America s Nursing Homes Campaign is a major initiative of the Advancing Excellence in Long Term Care Collaborative. The Collaborative assists all stakeholders of long term care. The Campaign helps nursing homes improve the quality of care and quality of life for the more than 1.5 million residents of America s nursing homes by providing resources and tools aimed to reduce avoidable hospitalizations, improve clinical outcomes, strengthen the workforce and person centered care principles. This free website: aligns with Quality Assurance Performance Improvement QAPI and developed a step by step framework that will guide you through a quality improvement project. Collaborative participants will find downloadable excel spreadsheets (including recorded trainings) they can use if there quality improvement activities. It is recommended that each facility using these tools, register as a participant and share their data on the website. Doing so will, provide participants with graphs and provide Telligen with the opportunity to aggregate collaborative participant s data to track progress. Data agreements are available; contact your quality improvement facilitator to learn more. 34

35 Example: Staff Turnover Data Collection Tools 35

36 INTERACT QUALITY IMPROVEMENT TOOLS Tracking Hospitalization Rates - Acute Care Transfer Log - Calculating Hospitalization Rates Quality Improvement Reviews Root Cause Analysis - QI Tool for Review of Acute Care Transfers - QI Summary worksheet COMMUNICATION TOOLS For Communication within the Nursing Home (NH) - Stop and Watch Early Intervention Tool - SBAR Communication Form - Medication Reconciliation Worksheet for Post- Hospital Care For Communication Between Nursing Home and Hospital - Tip Sheet Engaging Your Hospitals - NH Capabilities List - NH- Hospital Transfer Form - NH Hospital Data List - Acute Care Transfer - Hospital Post-Acute Transfer Form - Hospital Post-Acute Data List ADVANCE CARE PLANNING TOOLS - Communication Guide - Tracking Tool - Comfort Care Order Set - Decision about going to hospital - Education on CPR and Tube Feeding - Identifying those appropriate for Hospice/Palliative Care Orders DECISION SUPPORT TOOLS Acute change in Condition - Acute Change in Condition File Cards Care Paths - Acute Mental Status - Change in Behavior - Dehydration - Fever - GI Symptoms; nausea, vomiting, diarrhea - Shortness of Breath - Symptoms of CHF - Symptoms of Lower Respiratory Illness - Symptoms of UTI - Fall 36


37 Example INTERACT Version Stop and Watch Tool Example INTERACT Version Nursing Home Capabilities List 37

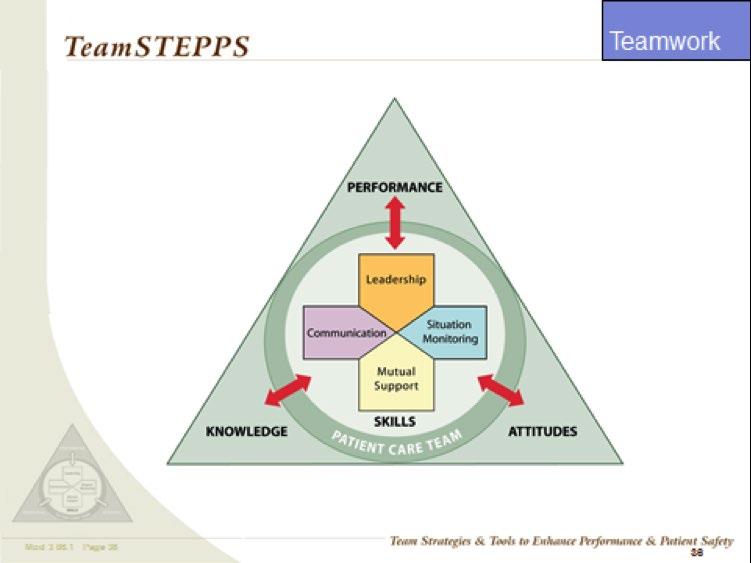
38 TeamSTEPPS 38
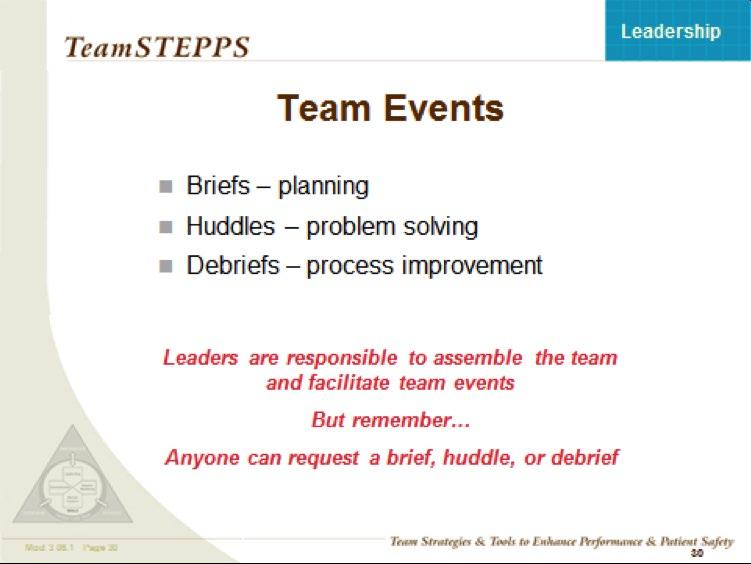
39 TeamSTEPPS Strategies 39
40 40
41 41
42 REPORTS FROM TELLIGEN National Nursing Home Quality Care Collaborative (NNHQCC) The NNHQCC is a fast paced, all teach all learn initiative, modeled after the Institute for Healthcare Improvement breakthrough collaborative model. This improvement initiative is led by the Centers for Medicare & Medicaid Services (CMS) and Quality Innovation Network-Quality Improvement Organizations (QIN-QIOs). The NNHQCC Collaborative 1 runs from April 2015 through September The NNHQCC seeks to rapidly spread the practices of high performing nursing homes with the aim of ensuring that every nursing home resident receives the highest quality of care. Specifically, the NNHQCC will strive to instill quality and performance improvement practices, eliminate healthcare acquired conditions, and dramatically improve resident satisfaction through the achievement of a rate of 6 or less using the NNHQCC quality composite measure by September 30, Measuring Collaborative Success Participating nursing homes will focus on processes that improve their systems and measure individual tests of change. Each nursing home team will have direct access to what they need to become more proficient with using Plan-Do-Study-Act (PDSA) improvement cycle results, clinical outcome measures, and their composite score. Calculating the NNHQCC Quality Composite Measure Score The composite is comprised of thirteen NQF-endorsed, long-stay quality measures that represent larger systems within the long term care setting: 1. Percent of residents with one or more falls with major injury 2. Percent of residents with a UTI 3. Percent of residents who self-report moderate to severe pain 4. Percent of high-risk residents with pressure ulcer 5. Percent of low-risk residents with loss of bowels or bladder 6. Percent of residents with catheter inserted or left in bladder 7. Percent of residents physically restrained 8. Percent of residents whose need for help with ADL has increased 9. Percent of residents who lose too much weight 10. Percent of residents who have depressive symptoms 11. Percent of residents who received antipsychotic medications 12. Percent of residents assessed and appropriately given flu vaccine* 13. Percent of residents assessed and appropriately given Pneumococcal vaccine* *The direction of the two vaccination measures should be reversed because they are directionally opposite of the other measures. This is done by subtracting the numerator from the denominator to obtain a new numerator. By keeping all measure directions consistent, the composite score can be interpreted as: the lower, the better. The composite score is calculated by summing the 13 measure numerators to obtain the composite numerator, summing the 13 measure denominators to obtain the composite denominator, then dividing the composite numerator by the composite denominator and multiplying by 100. This method of calculation is based on the opportunity model concept.** **This measure is intended for the sole purpose of measuring progress in the NNHQCC. It is not intended to replace any existing CMS measures or scores such as the Five Star Rating System. These measures were chosen for the composite because timely data are available for measuring progress in this fast paced Collaborative. QIN-QIOs have access to the quality measure data necessary to calculate composite scores for their state. 42
43 Nursing Home Composite Score and Long-Stay Quality Measures Trend Report Data displayed in this report are based on data extracted from the QIES workbench by the NCC QIN-QIO. All time periods displayed represent a 6-month time period with months displayed on the horizontal axes representing the last month of the 6-month time period. For example the label "July- 14" represents data from the 6-month time period starting in February 2014 and going through July State medians and percentiles are provided for comparison purposes. Please keep in mind that higher rates are better for influenza and pneumococcal vaccination measures, while lower rates are better in all other measures presented in this report. NOTE: To provide more statistical validity, the state medians and percentiles were calculated using only homes that had 10 residents in the denominator of the corresponding measure. Nursing Home Composite Score 43
44 Falls with Major Injury (L) 44

45 REPORTS TO TELLIGEN TOOL QAPI Self-Assessment Tool Directions: Use this tool as you begin work on QAPI and then for annual or semiannual evaluation of your organization s progress with QAPI. This tool should be completed with input from the entire QAPI team and organizational leadership. This is meant to be an honest reflection of your progress with QAPI. The results of this assessment will direct you to areas you need to work on in order to establish QAPI in your organization. You may find it helpful to add notes under each item as to why you rated yourself a certain way. Date of Review: Next review scheduled for: Doing great Almost there On our way Just starting Not started Rate how closely each statement fits your organization Our organization has developed principles guiding how QAPI will be incorporated into our culture and built into how we do our work. For example, we can say that QAPI is a method for approaching decision making and problem solving rather than considered as a separate program. Notes: Our organization has identified how all service lines and departments will utilize and be engaged in QAPI to plan and do their work. For example, we can say that all service lines and departments use data to make decisions and drive improvements, and use measurement to determine if improvement efforts were successful. Notes: Our organization has developed a written QAPI plan that contains the steps that the organization takes to identify, implement and sustain continuous improvements in all departments; and is revised on an ongoing basis. For example, a written plan that is done purely for compliance and not referenced would not meet the intent of a QAPI plan. Notes: Our board of directors and trustees (if applicable) are engaged in and supportive of the performance improvement work being done in our organization. For example, it would be evident from meeting minutes of the board or other leadership meetings that they are informed of what is being learned from the data, and they provide input on what initiatives should be considered. Other examples would be having leadership (board or executive leadership) representation on performance improvement projects or teams, and providing resources to support QAPI. Notes: 45
QAPI: Driving Quality or Just Driving You Crazy
 QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
Nursing Home Walk of Fame Visiting What Really Works. Call in Number
 Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
2014 QAPI Plan for [Facility Name]
![2014 QAPI Plan for [Facility Name]](/thumbs/74/70066237.jpg "2014 QAPI Plan for [Facility Name]") presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
10/22/2015. QIO Program Restructures. QIO Program Restructures ANHA Activities/Social Services Convention Person-Centered Care
 2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications
 Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles. Objectives QAPI. Regulatory Phases
 QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
HSAG the QIN-QIO NHQCC II and CDI Initiative Kick-off
 (HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
(HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
Advancing Excellence Phase 2 Goals
 Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement. Patty Austin, RN, CPHQ Project Coordinator
 QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
3/24/2016. Value of Quality Management. Quality Management in Senior Housing: Back to the Basics. Objectives. Defining Quality
 Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
LSSCC Action Period 1: Composite Score Reports June 25, 2015
 LSSCC Action Period 1: Composite Score Reports June 25, 2015 The National Nursing Home Quality Care Collaborative (NNHQCC) Composite Measure! Composite Measure tool used to help monitor NNHQCC progress
LSSCC Action Period 1: Composite Score Reports June 25, 2015 The National Nursing Home Quality Care Collaborative (NNHQCC) Composite Measure! Composite Measure tool used to help monitor NNHQCC progress
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
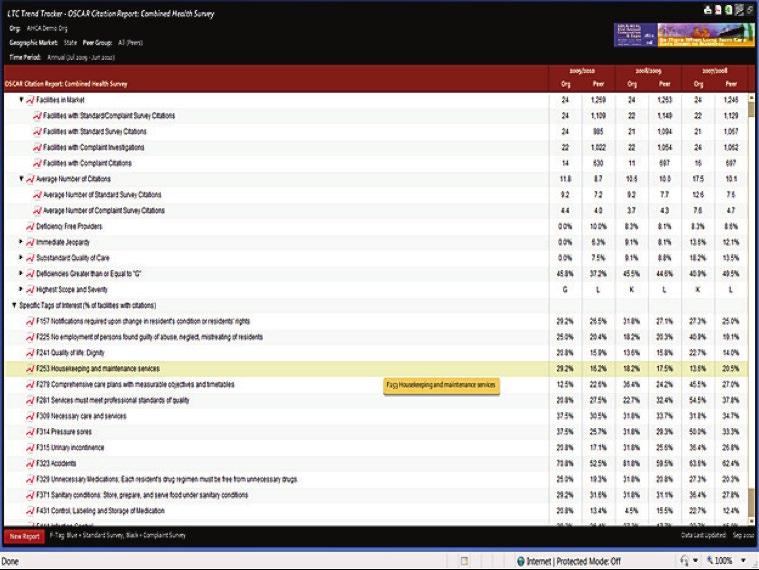
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study
 Case Study") Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Leading and Sustaining Systemic Change Collaborative: Overview
 Leading and Sustaining Systemic Change Collaborative: Overview Beth Hercher, CPHQ Quality Improvement Advisor Julie Clark, LPTA Quality Improvement Advisor John Wright, MSN, RN-BC, WCC Quality Improvement
Leading and Sustaining Systemic Change Collaborative: Overview Beth Hercher, CPHQ Quality Improvement Advisor Julie Clark, LPTA Quality Improvement Advisor John Wright, MSN, RN-BC, WCC Quality Improvement
Presentation Objectives
 Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI)
") United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
What Story Is Your SNF Data Telling?
 What Story Is Your SNF Data Telling? Holly Harmon, RN, MBA, LNHA Senior Director of Clinical Services Thank you to our Launch Sponsor: Objectives Recognize the value of data informed practice Identify
What Story Is Your SNF Data Telling? Holly Harmon, RN, MBA, LNHA Senior Director of Clinical Services Thank you to our Launch Sponsor: Objectives Recognize the value of data informed practice Identify
Implementing QAPI: Translating Data into Action. Objectives
 Implementing QAPI: Translating Data into Action Jane C Pederson, MD, MS April 16, 2013 Objectives Prioritize improvement opportunities based on data Identify a baseline measure for an improvement project
Implementing QAPI: Translating Data into Action Jane C Pederson, MD, MS April 16, 2013 Objectives Prioritize improvement opportunities based on data Identify a baseline measure for an improvement project
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
9/27/2017. Getting on the Path to Excellence. The path we are taking today! CMS Five Elements
 Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
National Nursing Home Quality Care Collaborative Participation Agreement
 National Nursing Home Quality Care Collaborative Participation Agreement Nursing Home Participant Information Nursing Home Name: Telephone # Administrator: Email: Director of Nursing: Email: Owner: Telephone
National Nursing Home Quality Care Collaborative Participation Agreement Nursing Home Participant Information Nursing Home Name: Telephone # Administrator: Email: Director of Nursing: Email: Owner: Telephone
Kentucky Nursing Home Collaborative Action Period 1. Scott Gibson, Quality Improvement Advisor
 Kentucky Nursing Home Collaborative Action Period 1 Scott Gibson, Quality Improvement Advisor June 9, 2015 QIO Program Restructures New multistate, five-year contract began Aug 1, 2014 Quality Innovation
Kentucky Nursing Home Collaborative Action Period 1 Scott Gibson, Quality Improvement Advisor June 9, 2015 QIO Program Restructures New multistate, five-year contract began Aug 1, 2014 Quality Innovation
LeadingAge New York Technology Solutions
 LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
QAPI Plan QAPI Plan. snits: Sanitas, Denver, CO. Effective Date: 01-Jan-2018
 QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications
 Program Description & Measurement Specifications") 2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Maryland Patient Safety Center s Call for Solutions Submission. Organization: Atlantic General Hospital
 Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now!
 Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
Collaborative Progress Where are We Now?
 Collaborative Progress Where are We Now? Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant May 30 th, 2013 Learning Session 2, Part 1 Qualis Health is one of the nation s leading healthcare
Collaborative Progress Where are We Now? Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant May 30 th, 2013 Learning Session 2, Part 1 Qualis Health is one of the nation s leading healthcare
Pressure Ulcers to Zero Collaborative Guide
 Pressure Ulcers to Zero Collaborative Guide Table of Contents Page Number Purpose of the guide 2 Why get involved? 3 Pressure Ulcer Definition 5 What is the Pressure Ulcers to Zero Collaborative 6 Getting
Pressure Ulcers to Zero Collaborative Guide Table of Contents Page Number Purpose of the guide 2 Why get involved? 3 Pressure Ulcer Definition 5 What is the Pressure Ulcers to Zero Collaborative 6 Getting
Understanding the Five Star Quality Rating System Design For Nursing Home Compare
 Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
Root Cause and Data Analysis
 Root Cause and Data Analysis Michelle Synakowski LeadingAge NY Policy Analyst/Consultant 2 1 3 Systemic Analysis and Action Systematic approach to problem analysis Thorough Highly organized Structured
Root Cause and Data Analysis Michelle Synakowski LeadingAge NY Policy Analyst/Consultant 2 1 3 Systemic Analysis and Action Systematic approach to problem analysis Thorough Highly organized Structured
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care
 Partnership to Improve Dementia Care") The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
TOP 10 IDEAS TO INVOLVE ALL STAFF IN ADVANCING EXCELLENCE
 TOP 10 IDEAS TO INVOLVE ALL STAFF IN ADVANCING EXCELLENCE Advancing Excellence Long-Term Care Collaborative (AELTCC) is a not-for-profit organization made up of over 30 national stakeholders involved with
TOP 10 IDEAS TO INVOLVE ALL STAFF IN ADVANCING EXCELLENCE Advancing Excellence Long-Term Care Collaborative (AELTCC) is a not-for-profit organization made up of over 30 national stakeholders involved with
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Learning Objectives. QAPI at a Glance: 8/22/16. Achieving Success with QAPI. Participants will be able to describe:
 Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors. Summer 2012
 Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors Summer 2012 Developed by the U.S. Department of Education Office of Migrant Education through a contract with
Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors Summer 2012 Developed by the U.S. Department of Education Office of Migrant Education through a contract with
Improving Nursing Home Compare for Consumers. Five-Star Quality Rating System
 Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Telligen. Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016
 Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator
 Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
A Measurement Guide for Long Term Care
 Step 6.10 Change and Measure A Measurement Guide for Long Term Care Introduction Stratis Health, in partnership with the Minnesota Department of Health, is pleased to present A Measurement Guide for Long
Step 6.10 Change and Measure A Measurement Guide for Long Term Care Introduction Stratis Health, in partnership with the Minnesota Department of Health, is pleased to present A Measurement Guide for Long
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report
 Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
INSERT ORGANIZATION NAME
 INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Effective Date: January 9, 2017
 Effective Date: January 9, 2017 Overview: The safety and quality of care, treatment, and services depend on many factors, including the following: - A culture that fosters safety as a priority for everyone
Effective Date: January 9, 2017 Overview: The safety and quality of care, treatment, and services depend on many factors, including the following: - A culture that fosters safety as a priority for everyone
Home Health Value-Based Purchasing Series: HHVBP Model 101. Wednesday, February 3, 2016
 Home Health Value-Based Purchasing Series: HHVBP Model 101 Wednesday, February 3, 2016 About the Alliance 501(c)(3) non-profit research foundation Mission: To support research and education on the value
Home Health Value-Based Purchasing Series: HHVBP Model 101 Wednesday, February 3, 2016 About the Alliance 501(c)(3) non-profit research foundation Mission: To support research and education on the value
HIMSS Submission Leveraging HIT, Improving Quality & Safety
 HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
University of Michigan Health System Part IV Maintenance of Certification Program [Form 12/1/14]
![University of Michigan Health System Part IV Maintenance of Certification Program [Form 12/1/14]](/thumbs/83/88988679.jpg "University of Michigan Health System Part IV Maintenance of Certification Program [Form 12/1/14]") Report on a QI Project Eligible for Part IV MOC: Improving Medication Reconciliation in Primary Care Instructions Determine eligibility. Before starting to complete this report, go to the UMHS MOC website
Report on a QI Project Eligible for Part IV MOC: Improving Medication Reconciliation in Primary Care Instructions Determine eligibility. Before starting to complete this report, go to the UMHS MOC website
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Thank You for Joining!
 Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
LeadingAge New York Technology Solutions
 LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
Developing an Organizational QAPI Plan
 Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs)
 FREQUENTLY ASKED QUESTIONS (FAQs)") MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs) What is the MQii? The Malnutrition Quality Improvement Initiative (MQii) aims to advance evidence-based, high-quality
MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs) What is the MQii? The Malnutrition Quality Improvement Initiative (MQii) aims to advance evidence-based, high-quality
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
Disclaimer. Learning Objectives
 Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
MODULE 8 HOW TO COLLECT, ANALYZE, AND USE HEALTH INFORMATION (DATA) ACCOMPANIES THE MANAGING HEALTH AT THE WORKPLACE GUIDEBOOK
 ACCOMPANIES THE MANAGING HEALTH AT THE WORKPLACE GUIDEBOOK") MODULE 8 HOW TO COLLECT, ANALYZE, AND USE HEALTH INFORMATION (DATA) ACCOMPANIES THE MANAGING HEALTH AT THE WORKPLACE GUIDEBOOK MODULE 8: How to Collect, Analyze, and Use Health Information (Data) You have
MODULE 8 HOW TO COLLECT, ANALYZE, AND USE HEALTH INFORMATION (DATA) ACCOMPANIES THE MANAGING HEALTH AT THE WORKPLACE GUIDEBOOK MODULE 8: How to Collect, Analyze, and Use Health Information (Data) You have
A Comprehensive Framework for Patient Safety
 These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Indiana Pressure Ulcer Reduction Initiative
 Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Design for Nursing Home Compare 5-Star Rating System: Users Guide
 Design for Nursing Home Compare 5-Star Rating System: Users Guide December 2008 Contents Introduction...1 Methodology...3 Survey Domain...3 Scoring Rules...3 Rating Methodology...4 Staffing Domain...5
Design for Nursing Home Compare 5-Star Rating System: Users Guide December 2008 Contents Introduction...1 Methodology...3 Survey Domain...3 Scoring Rules...3 Rating Methodology...4 Staffing Domain...5
A GUIDE TO Understanding & Sharing Your Survey Results
 A GUIDE TO Understanding & Sharing Your Survey Results Learning & al Development Table of Contents The 2017 UVA Health System Survey provides insight and awareness gained through team member feedback,
A GUIDE TO Understanding & Sharing Your Survey Results Learning & al Development Table of Contents The 2017 UVA Health System Survey provides insight and awareness gained through team member feedback,
COPs 2018 Now is the Time. HCAC 2017 Conference PreConference 2017 The Crag Business Group, Inc.
 COPs 2018 Now is the Time HCAC 2017 Conference PreConference FOCUS & THEMES Revisions of the Home Health Agency provider requirements..focus on a patient-centered, data-driven, outcome-oriented process
COPs 2018 Now is the Time HCAC 2017 Conference PreConference FOCUS & THEMES Revisions of the Home Health Agency provider requirements..focus on a patient-centered, data-driven, outcome-oriented process
Quality Assessment and Performance Improvement in the Ophthalmic ASC
 Quality Assessment and Performance Improvement in the Ophthalmic ASC ELETHIA DEAN RN,BSN, MBA, PHD Regulatory Requirements QAPI Program required by: Medicare Most states ASC licensing regulations Accrediting
Quality Assessment and Performance Improvement in the Ophthalmic ASC ELETHIA DEAN RN,BSN, MBA, PHD Regulatory Requirements QAPI Program required by: Medicare Most states ASC licensing regulations Accrediting
AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY
 AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY PUBLIC HEARING JUNE 30, 2016 1:00 P.M. 4:00 P.M. 1 AGENDA Welcome Project Overview Stakeholder Engagement Payment Methodology Options Quality Incentive
AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY PUBLIC HEARING JUNE 30, 2016 1:00 P.M. 4:00 P.M. 1 AGENDA Welcome Project Overview Stakeholder Engagement Payment Methodology Options Quality Incentive
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
TECHNICAL ASSISTANCE GUIDE
 TECHNICAL ASSISTANCE GUIDE COE DEVELOPED CSBG ORGANIZATIONAL STANDARDS Category 3 Community Assessment Community Action Partnership 1140 Connecticut Avenue, NW, Suite 1210 Washington, DC 20036 202.265.7546
TECHNICAL ASSISTANCE GUIDE COE DEVELOPED CSBG ORGANIZATIONAL STANDARDS Category 3 Community Assessment Community Action Partnership 1140 Connecticut Avenue, NW, Suite 1210 Washington, DC 20036 202.265.7546
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar
 Intervention Kick-Off Webinar") Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
THE 3 STEP PROCESS FOR SUCCESSFUL EMPLOYEE GOAL MANAGEMENT IN ACUTE CARE
 THE 3 STEP PROCESS FOR SUCCESSFUL EMPLOYEE GOAL MANAGEMENT IN ACUTE CARE Patient Experience Continuous Improvement ALIGN 3 Steps: Align, Execute, Evaluate There is no longer any doubt about the impact
THE 3 STEP PROCESS FOR SUCCESSFUL EMPLOYEE GOAL MANAGEMENT IN ACUTE CARE Patient Experience Continuous Improvement ALIGN 3 Steps: Align, Execute, Evaluate There is no longer any doubt about the impact
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING
 January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the