Built to Last: Our Population Health Model University of Utah Health Julie Day / Annie Mervis
|
|
|
- Reynard Booth
- 5 years ago
- Views:
Transcription

1 Built to Last: Our Population Health Model University of Utah Health Julie Day / Annie Mervis March 9, 2018 Phoenix, Arizona 1
2 Key components of a population health strategy what do you think? Using your cell phone Text To: xyz123 In the message box write one or two words that you consider key to a population health strategy 2
3 Objectives 1. Articulate the elements of a working population health management infrastructure 2. Understand the elements of a successful integrated behavioral health model 3. Identify useful measures of success within a population health integrated model and how to work with the community to build reporting capability 4. Understand the approach to creating a value-based contract 3
4 4

5 Population Health A Little Background 5

6 Population Health Management PHM means the proactive application of strategies and interventions to defined groups of individuals across the continuum of care in an effort to improve the health of the individuals within the group at the lowest necessary cost. Healthcatalyst 6

7 Aims of Population Health Increased patient engagement Better patient self-efficacy More appropriate utilization of health care resources Decreased ED visits Decreased admissions/readmissions INCREASED QUALITY OF LIFE DECREASED COST OF CARE 7

8 Our Team s North Star To proactively enhance patient engagement by establishing therapeutic relationships that result in better quality of life and lower health care costs in a cost effective, sustainable manner. 8

9 Risk Stratifying the Population Is Foundational 9


10 Diagnoses, ED visits, Hospitalizations Limited mobility, Limited Socialization, Depression Limited number of diagnoses-fairly stable May need tests updated Health Maintenance Healthy Health Maintenance
11

12 The CPG Population Health Model 12
13 Diagnoses, ED visits, Hospitalizations Limited mobility, Limited Socialization, Depression 13
14 RISK ADJUSTING THE POPULATION EPIC Foundational Risk Score is currently used for adults Pediatric Risk score was developed internally ADULT RISK SCORE Age # of Hospital Admissions # of ED Visits Chronic Conditions COPD Diabetes CHF Liver Disease Mental Health: Depression No PCP Medicaid Coverage PEDIATRIC RISK SCORE # of Hospital Admissions # of ED Visits # of outpatient visits Breathing problems Mental Health: Anxiety Depression Outpatient medications Medicaid Coverage 14
15 What are the Building Blocks? A like-minded multidisciplinary team Care Managers Social Workers Clinical Pharmacists Carved out paid time for Care Conferences with the Provider and team 15
16 Population Health Strategies INTRADISCIPLINARY CARE CONFERENCES Attendees: Provider, MA/RN, Care Manager, Social Worker, Clinical Pharmacist. Frequency: Care Conferences are held monthly for each provider. Patient identification: Referral from provider Considered high risk on risk registry or based on external utilization data from payers. 16
17 Referring to the Population Health Team 1. Warm Hand-off Introduce the patient to the team member(s) while patient is in clinic. This results in a higher probability that the patient will engage with our services. Often, we can resolve an issue at that time. 2. Consult in EPIC to appropriate service(s) Our referral team will outreach to the patient and set up a future appointment with us. 3. Talk to team member to request Care Conference Discussion 17
18 Team Functions - PROVIDER Establish trusting relationship with patients Facilitate patient engagement with team members (Refer to appropriate team members) Attend team conferences and contribute to the development of patient care plan Analyze and collaborate on needs of high risk patients 18
19 Provider Measures Referrals to Care Management Social Work/GATE Clinical Pharmacy Quality outcomes Patient Experience Easy to understand explanations Listened to Answered Questions Understands what is important to you Respects what you have to say 19
. Longitudinal outreach and monitoring of patient s progress toward care plan goals. Coordination of community resources.")
20 Team Functions Care Manager Coordination of care and resources for patient s medical and overall health needs. Home Health/Skilled Nursing Facility/LTAC placements. Coordination of insurance benefits (i.e., Medicare, Medicaid, PCN, commercial). Longitudinal outreach and monitoring of patient s progress toward care plan goals. Coordination of community resources. Assessment of barrier impacting patients health and/or ability to access health resources effectively. Coordination of Care Team Conferences Management of High Risk Adult and Pediatric Registries. Living Well Program Home Visits 20
21 Care Management Measures Percent of high risk patients with a care plan Goals Treatment Goal Lifestyle Goal Contingency Plan (what to do if something goes wrong) Volume of Touches Calls In-person MyChart Volume per Panel Volume per provider Time Tracker 21

22 22

23 Team Functions Social Worker Short term, problem-based psychotherapy (3-5 sessions) Depression/Anxiety Screening Gate Consults Health Behavior Assessment Interventions Coordination of resources for behavioral health needs. Behavioral Health Crisis Intervention (suicidal ideation) APS/DCFS cases and referrals Housing 23

24 Social Work Report for Calendar Year

25 Team Functions Clinical Pharmacist Comprehensive Medication Management (Clinical Practice Agreement) Diabetes Hypertension Hyperlipidemia Asthma Polypharmacy/Medication reconciliation Medication Education to improve understanding of medication regime. Increase medication compliance Adverse Events Monitoring Tobacco Cessation 25
26 Clinical Pharmacy Measures Number of medication reconciliations done Trend AEs Percent of key chronic medications that are being refilled MTM programs established with number of enrollees: Diabetes, Hyperlipidemia, Hypertension, Asthma 26

27 Clinical Pharmacy Metrics 27

28 Team Functions-Nurse Prevention Education Chronic Disease Education Medical record requests from outside facilities DME Screenings Training and workflow development 28
29 Nurse Measures Volumes for: Individual Education Sessions Group Education Sessions Trainings accomplished Screenings accomplished 29






30 SHARED OUTCOMES 30

31 Epic Healthy Planet Primary Care Adult Risk Measures 31
32 Team effect to improve A1C < 9 on a cohort seen by clinical pharmacy July 2015 June

33 What happens at a Care Conference? What issues are facing Jabba the Hut? Poor Diet? Substance Abuse? Mobility? Depression? Social Support? Financial Issues? Identify the issues and together figure out a plan and goals to discuss with the patient. 33

34 The Longitudinal Plan of Care This is the Place for Sharing! 34

35 How do we manage transitions? 35
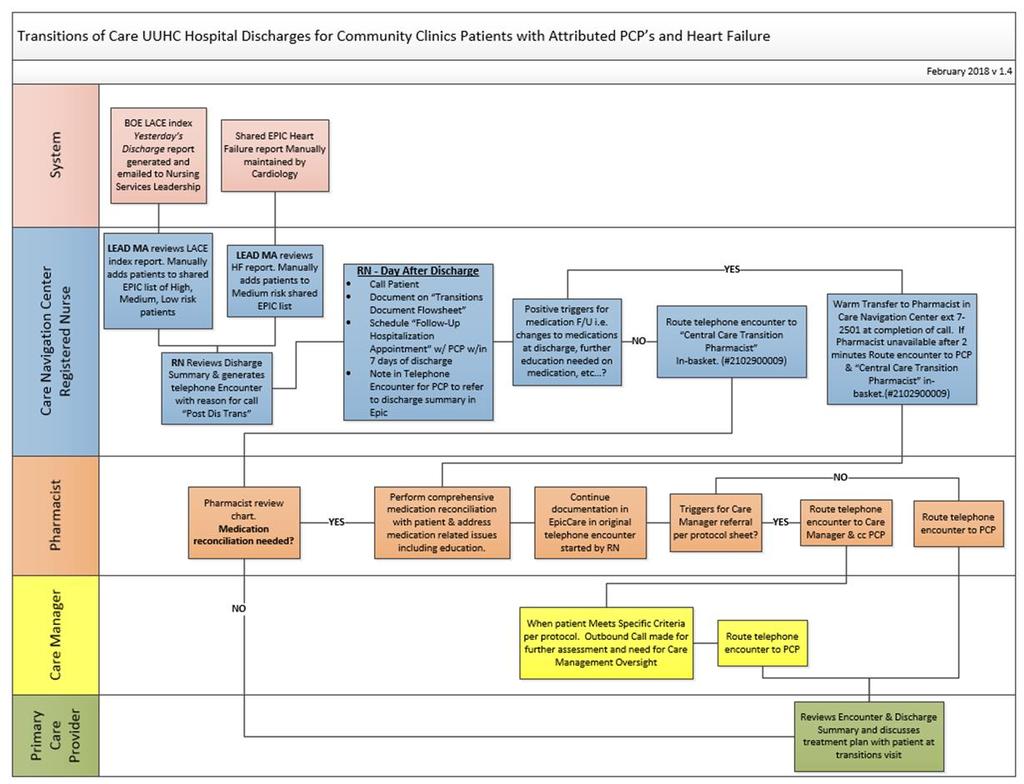
36 36
37 37
38 How do we support reliable care? Managing Gaps in Care Registry Outreach Care Navigation Center Bulk Outreach Birthday letters MyChart Center-based teams Point of Service Management Pre-visit Planning 38

39 How do we engage teams in quality improvement? Monthly Team Process Improvement Meetings Review current measure performance and workflow Identify and prioritize barriers Develop interventions Decide on process measures to collect on the floor to monitor implementation of intervention Review impact on quality measure Providers paid average RVU for team meeting time 39
40 40
41 FY18 Depression screening project 41

42 CMS Quality Payment Program Preliminary
43 43

44 One Riddle Being Solved 44

45 Missing Data Community Clinic patients utilization in facilities outside our system Collaboration with our Statewide Clinical Health Information Exchange 45
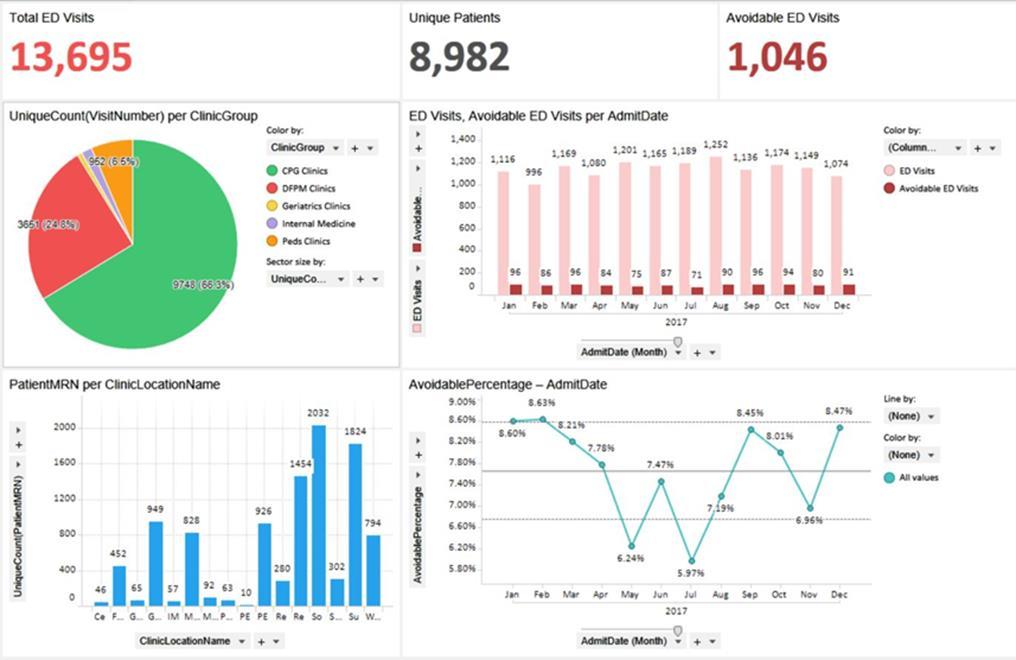
46 chie Data Uses Daily ADT reports pushed from chie to care managers Hospital admits Hospital discharges ED discharges Used for outreach and to schedule follow-up with PCP Next LACE score to risk stratify patients The big picture dashboard Hospital Admissions per 1000 ED visits per 1000 Patients with > 4 ED Visits Avoidable ED Visits Next 30 day Readmissions Rate Total Cost of Care 46

47 DRAFT 47

48 48
49 Lessons Learned Community-based Dashboard development is an iterative process Language barriers: Technical vs. Operational Face to Face matters 49

50 This program has been going from strength to strength and I would be loath to see it compromised in any way, as it is a foundational success upon which we should build. - Dr. David A. 50
51 Pause for Audience Participation Using your cell phone Text To: xyz123 In the message box write one or two words that depict components of the Population Health Management strategy just described. 51

52 Deeper Dive Into Behavioral Health Integration 52

53 The Problems That Need To Be Solved PCP varying confidence in addressing behavioral health concerns Encountering behavioral health concerns lead to: Provider burnout Interference of clinic workflow 1 in 4 adults suffer from a diagnosable mental disorder (Brian & Behavior Research Foundation, BBR, n.d.)


54 January 2014 February ,000 of 291,350 visits in the University Community Clinics had a co-morbid mental health condition 41% No Co morbidity 59% Co-morbid 54

55 55
56 Goals of Integration Increase availability of behavioral health services within the medical model PCP support in addressing their patients behavioral health needs Improve patient clinical outcomes and satisfaction through integrated care 56

57 57
58 Identified Challenges Limited resources for medication management Limited resources for mental health providers due to contractual carve outs and burdensome administrative processes Limited access to mental health providers Challenges navigating the mental health system Limited community resources Social systems breakdown 58
59 One Lesson Learned Co-location and a standard model practice led to Continued limited access Little communication at team level Fundamentally separate practices 59
60 Made the Move to Full Integration Partnership with Community Clinics, Community Physicians Group, UNI, Department of Psychiatry, and College of Social Work Chose to focus on comprehensive care of patients, remove any barriers for any patient Embedded Social Workers into hallways shared with primary care providers 60




61 No behavioral health needs Behavioral health needs discovered Social worker + patient Real-Time Care Team Coordination Triage Assessment Short-Term Therapy Sessions (3-5 sessions) Groups Community Resources/ Referral to specialized services Coordinate with Population Health Connection to internal psychiatric resources Patient Advocacy Crisis Intervention 61
62 One Way to Generate Revenue Health Behavior and Assessment Intervention Codes 62
63 Pause for Audience Participation Using your cell phone Text To: xyz123 In the message box write one or two words that depict components of the integrated behavioral health program just described. 63

64 Getting On Top of Contracting 64
65 One Contract Deal 65
66 The Details on Potential 66
67 STAR Visits: Addressing 90% of HCCs in 60% of Patients 67

68 80% Adherence to HEDIS/STAR Measures 68
69 Other Components of the Contract 69
70 Lessons Learned Quarterly reporting/evaluation is too frequent Double check language in contract to ensure a win/win Start with partners who will be flexible in working to create a win/win 70
71 ROE= COA/TPI Healthcatalyst 71




72 RETURN ON ENGAGEMENT 72
73 Text a one word idea you can use when you return to your organization. 73
74 Questions? ROE= COA/TPI 74
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012
 Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah
 University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah Primary Preceptors: Redwood Health Center Macheala Jacquez, PharmD, BCACP; Megan Lowe, PharmD, BCACP;
University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah Primary Preceptors: Redwood Health Center Macheala Jacquez, PharmD, BCACP; Megan Lowe, PharmD, BCACP;
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
Chapter 2 Provider Responsibilities Unit 6: Behavioral Health Care Specialists
 Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Variables that impact the cost of delivering SB 1004 palliative care services. Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017
 Variables that impact the cost of delivering SB 1004 palliative care services Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017 SB 1004 Palliative Care SB 1004 (Hernandez, Chapter 574, Statutes
Variables that impact the cost of delivering SB 1004 palliative care services Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017 SB 1004 Palliative Care SB 1004 (Hernandez, Chapter 574, Statutes
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Medicaid and the. Bus Pass Problem
 Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
SECTION 3. Behavioral Health Core Program Standards. Z. Health Home
 SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Synergy Through Integration:
 WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
ATTACHMENT A Delivery System Reform Incentive Payment (DSRIP) Program Renewal Request
 Program Renewal Request") Background ATTACHMENT A The New Jersey Department of Health (DOH) operates the Delivery System Reform Incentive Payment (DSRIP) program as required by Section 93(e) of the Special Terms and Conditions
Background ATTACHMENT A The New Jersey Department of Health (DOH) operates the Delivery System Reform Incentive Payment (DSRIP) program as required by Section 93(e) of the Special Terms and Conditions
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics
 Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics IMPLEMENTATION TOOLKIT Implementation Planning for Co-located Primary Care and Behavioral Health Services
Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics IMPLEMENTATION TOOLKIT Implementation Planning for Co-located Primary Care and Behavioral Health Services
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Center for Community Health Navigation at NewYork-Presbyterian Hospital
 Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014
 SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014 Jaron Asher, MD Medical Director at Places for People in St. Louis, MO Chief
SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014 Jaron Asher, MD Medical Director at Places for People in St. Louis, MO Chief
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
2017 QUALITY PLAN WORK PLAN. Kaiser Permanente of Washington 2017 Quality Work Plan
 Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Integrating Behavioral Health Across Integrated Delivery Systems
 Integrating Behavioral Health Across Integrated Delivery Systems Speaker Lori Raney, MD, Principal, Robin Henderson, PsyD, Chief Executive, Behavioral Health Providence Medical Group May 12, 2016 HealthManagement.com
Integrating Behavioral Health Across Integrated Delivery Systems Speaker Lori Raney, MD, Principal, Robin Henderson, PsyD, Chief Executive, Behavioral Health Providence Medical Group May 12, 2016 HealthManagement.com
October Program/Policy Updates
 October 2017 An An Update Update for for Highmark Highmark Health Health Options Options Providers Providers and and Clinicians Clinicians Program/Policy Updates Clinical Practice and Preventive Health
October 2017 An An Update Update for for Highmark Highmark Health Health Options Options Providers Providers and and Clinicians Clinicians Program/Policy Updates Clinical Practice and Preventive Health
Solution Title: Meeting the Challenge of Health Care Change
 Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
March 15, 2017 UCCCN Learning Session - Summary
 March 15, 2017 UCCCN Learning Session - Summary Healthy U Molina Health Choice Utah SelectHealth Pediatric Specialty Learning Session Panelists (Insurers) Liz Armour-Roth, Manager, Care Management Sheila
March 15, 2017 UCCCN Learning Session - Summary Healthy U Molina Health Choice Utah SelectHealth Pediatric Specialty Learning Session Panelists (Insurers) Liz Armour-Roth, Manager, Care Management Sheila
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Section IX Special Needs & Case Management
 Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
HHW-HIPP0314 (9/13) MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.
 MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.") HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Physical Health Integration Within Behavioral Healthcare: Promising Practices
 Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
What is a CHW? Today s Agenda 9/6/17. Community Health Workers and Pharmacy Technicians: Allies in Promoting Patient-centered Care
 Community Health Workers and Pharmacy Technicians: Allies in Promoting Patient-centered Care Michigan Society of Pharmacy Technician Presentation Priscilla Hohmann Program Manager, MiCHWA September 16,
Community Health Workers and Pharmacy Technicians: Allies in Promoting Patient-centered Care Michigan Society of Pharmacy Technician Presentation Priscilla Hohmann Program Manager, MiCHWA September 16,
2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE
 2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE PHN PROGRAM AWARDS (COMMUNITY SUICIDE PREVENTION PINE RIDGE SERVICE UNIT AND THE GREAT PLAINS AREA) PHN Rodney R. Sahr RN, BSN
2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE PHN PROGRAM AWARDS (COMMUNITY SUICIDE PREVENTION PINE RIDGE SERVICE UNIT AND THE GREAT PLAINS AREA) PHN Rodney R. Sahr RN, BSN
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.