|
|
|
- Jessica Harper
- 5 years ago
- Views:
Transcription
1
2
3
4
5
6
7 Kate JohnsTon, Program Specialist
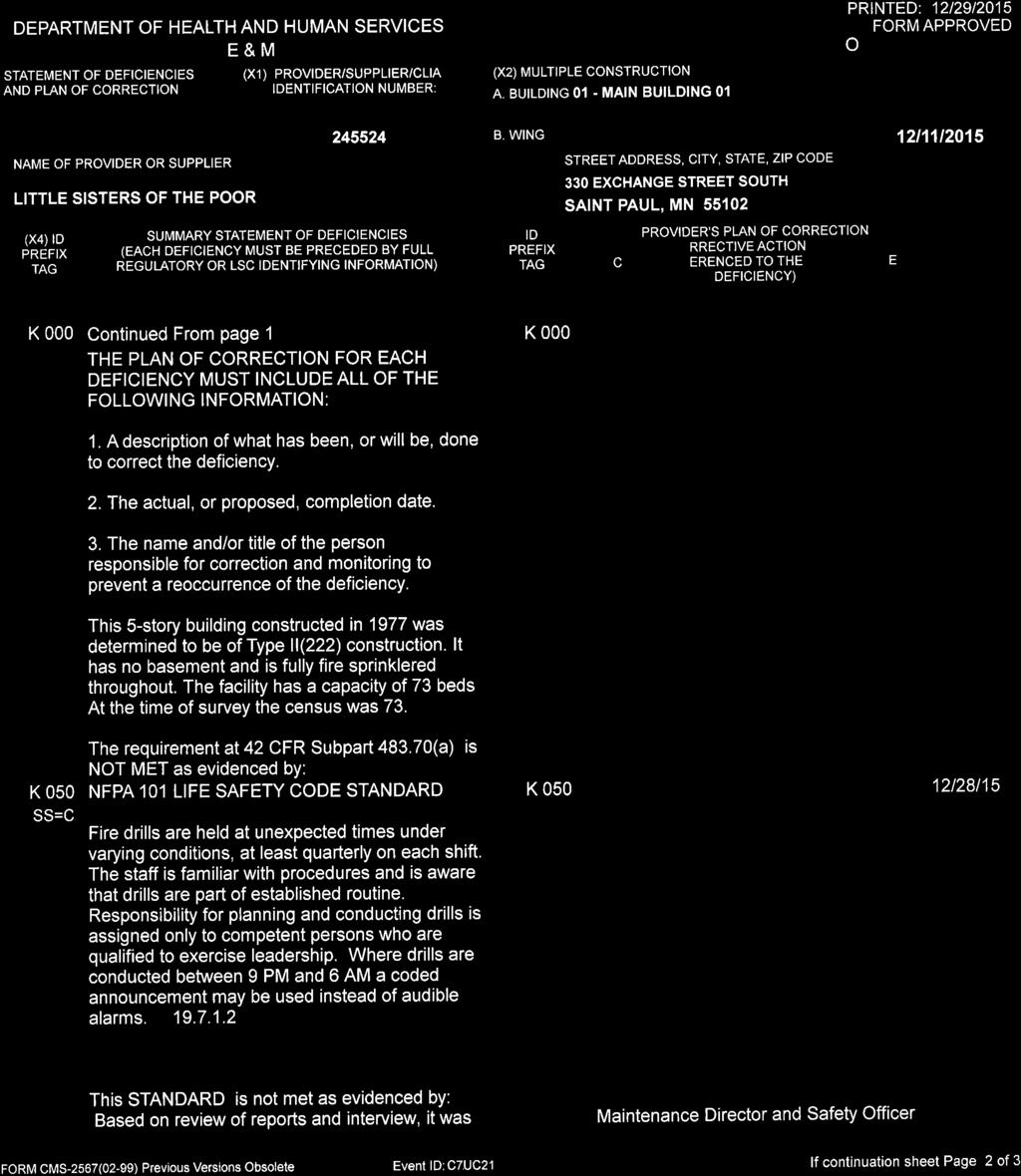
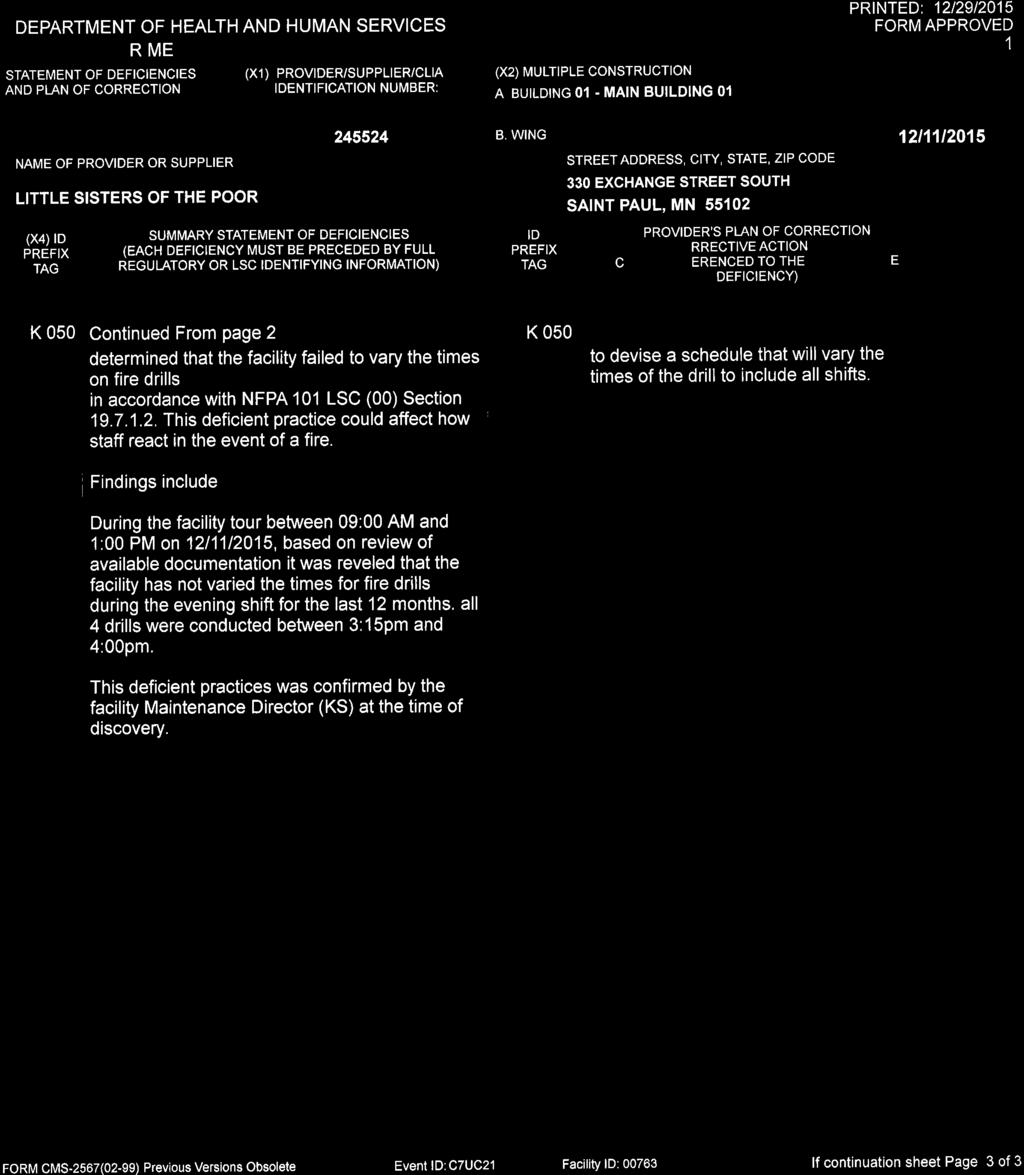
8 Electronically delivered December 24, 2015 Sr. Mary Elizabeth Anderson, Administrator Little Sisters Of The Poor 330 Exchange Street South Saint Paul, Minnesota RE: Project Number S Dear Sr.. Anderson: On December 10, 2015, a standard survey was completed at your facility by the Minnesota Departments of Health and Public Safety to determine if your facility was in compliance with Federal participation requirements for skilled nursing facilities and/or nursing facilities participating in the Medicare and/or Medicaid programs. This survey found the most serious deficiencies in your facility to be widespread deficiencies that constitute no actual harm with potential for no more than minimal harm (Level C), as evidenced by the attached CMS-2567 whereby corrections are required. Copies of the Statement of Deficiencies (CMS-2567) and Form A are enclosed. Please note that this notice does not constitute formal notice of imposition of alternative remedies or termination of your provider agreement. Should the Centers for Medicare & Medicaid Services determine that termination or any other remedy is warranted, it will provide you with a separate formal notification of that determination. This letter provides important information regarding your response to these deficiencies and addresses the following issues: Electronic Plan of Correction - when a plan of correction will be due and the information to be contained in that document; Informal Dispute Resolution - your right to request an informal reconsideration to dispute the attached deficiencies. Please note, it is your responsibility to share the information contained in this letter and the results of this visit with the President of your facility's Governing Body. Protecting, Maintaining and Improving the Health of Minnesotans
9 Little Sisters Of The Poor December 24, 2015 Page 2 DEPARTMENT CONTACT Questions regarding this letter and all documents submitted as a response to the resident care deficiencies (those preceded by a "F" tag), i.e., the plan of correction should be directed to: Susanne Reuss, Unit Supervisor Minnesota Department of Health Licensing and Certification Program Health Regulation Division P.O. Box East Seventh Place, Suite 220 St. Paul, Minnesota Telephone: (651) Fax: ELECTRONIC PLAN OF CORRECTION (epoc) An epoc for the deficiencies must be submitted within ten calendar days of your receipt of this letter. Your epoc must: - Address how corrective action will be accomplished for those residents found to have been affected by the deficient practice; - Address how the facility will identify other residents having the potential to be affected by the same deficient practice; - Address what measures will be put into place or systemic changes made to ensure that the deficient practice will not recur; - Indicate how the facility plans to monitor its performance to make sure that solutions are sustained. The facility must develop a plan for ensuring that correction is achieved and sustained. This plan must be implemented, and the corrective action evaluated for its effectiveness. The plan of correction is integrated into the quality assurance system; - Include dates when corrective action will be completed. The corrective action completion dates must be acceptable to the State. If the plan of correction is unacceptable for any reason, the State will notify the facility. If the plan of correction is acceptable, the State will notify the facility. Facilities should be cautioned that they are ultimately accountable for their own compliance, and that responsibility is not alleviated in cases where notification about the acceptability of their plan of correction is not made timely. The plan of correction will serve as the facility s allegation of compliance; and, - Include electronic acknowledgement signature of provider and date. The state agency may, in lieu of a revisit, determine correction and compliance by accepting the
10 Little Sisters Of The Poor December 24, 2015 Page 3 facility's epoc if the epoc is reasonable, addresses the problem and provides evidence that the corrective action has occurred. If an acceptable epoc is not received within 10 calendar days from the receipt of this letter, we will recommend to the CMS Region V Office that one or more of the following remedies be imposed: Optional denial of payment for new Medicare and Medicaid admissions (42 CFR (a)); Per day civil money penalty (42 CFR through ). Failure to submit an acceptable epoc could also result in the termination of your facility s Medicare and/or Medicaid agreement. PRESUMPTION OF COMPLIANCE - CREDIBLE ALLEGATION OF COMPLIANCE The facility's epoc will serve as your allegation of compliance upon the Department's acceptance. In order for your allegation of compliance to be acceptable to the Department, the epoc must meet the criteria listed in the plan of correction section above. You will be notified by the Minnesota Department of Health, Licensing and Certification Program staff and/or the Department of Public Safety, State Fire Marshal Division staff, if your epoc for their respective deficiencies (if any) is acceptable. VERIFICATION OF SUBSTANTIAL COMPLIANCE Upon receipt of an acceptable epoc, a revisit of a facility may be conducted to verify that compliance with the regulations has been attained. If a revisit is conducted, it will occur after the date you identified that compliance was achieved in your plan of correction. INFORMAL DISPUTE RESOLUTION In accordance with 42 CFR , you have one opportunity to question cited deficiencies through an informal dispute resolution process. You are required to send your written request, along with the specific deficiencies being disputed, and an explanation of why you are disputing those deficiencies, to: Nursing Home Informal Dispute Process Minnesota Department of Health Health Regulation Division P.O. Box St. Paul, Minnesota This request must be sent within the same ten days you have for submitting an epoc for the cited deficiencies. All requests for an IDR or IIDR of federal deficiencies must be submitted via the web at: You must notify MDH at this website of your request for an IDR or IIDR within the 10 calendar day
11 Little Sisters Of The Poor December 24, 2015 Page 4 period allotted for submitting an acceptable plan of correction. A copy of the Department s informal dispute resolution policies are posted on the MDH Information Bulletin website at: Please note that the failure to complete the informal dispute resolution process will not delay the dates specified for compliance or the imposition of remedies. Questions regarding all documents submitted as a response to the Life Safety Code deficiencies (those preceded by a "K" tag), i.e., the plan of correction, request for waivers, should be directed to: Mr. Tom Linhoff, Interim Supervisor Health Care Fire Inspections State Fire Marshal Division tom.linhoff@state.mn.us Telephone: (651) Fax: (651) Feel free to contact me if you have questions. Sincerely, Kate JohnsTon, Program Specialist Program Assurance Unit Licensing and Certification Program Health Regulation Division 85 East Seventh Place, Suite 220 P.O. Box St. Paul, Minnesota kate.johnston@state.mn.us Telephone: (651) Fax: (651)
12
13
14
15
16
17
18
Protecting, Maintaining and Improving the Health of Minnesotans
 CMS Certification Number (CCN): 245210 Delivered electronically September 25, 2014 Mr. Rob Lahammer, Administrator Lake Minnetonka Shores 4527 Shoreline Drive Spring Park, Minnesota 55384 Protecting, Maintaining
CMS Certification Number (CCN): 245210 Delivered electronically September 25, 2014 Mr. Rob Lahammer, Administrator Lake Minnetonka Shores 4527 Shoreline Drive Spring Park, Minnesota 55384 Protecting, Maintaining
Mary Heim, HPR-Social Work Specialist 09/03/2013
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: NKFZ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: NKFZ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8MXL Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8MXL Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00940
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: FU8X PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: FU8X PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Brenda Fischer, Unit Supervisor 09/13/2012 Colleen B. Leach, Program Specialist 09/18/2012
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: LNUX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: LNUX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: X60T Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: X60T Facility ID:
Patricia Halverson, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: VWX6 Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: VWX6 Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00712
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: H0RJ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: H0RJ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00695
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: D9GP PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: D9GP PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
James Anderson, State Fire Marshall
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2HL7 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2HL7 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Michelle McFarland, HFE NEII
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: PH3B Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: PH3B Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00351
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: M4JX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: M4JX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00858
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2LL3 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2LL3 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8L7Q Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8L7Q Facility ID:
Jessica Sellner, HFE, NEII 11/23/2011 Colleen B. Leach, Program Specialist 01/13/2012
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: DDG9 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: DDG9 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 2FT5 Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 2FT5 Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00719
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 93NN PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 93NN PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Gary Nederhoff, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 94CQ Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 94CQ Facility ID:
07/23/ /21/2013 (L20)
") DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 04CB PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 04CB PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00903
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: RHTV PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: RHTV PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 245507 596340100 12/06/2012
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 245507 596340100 12/06/2012
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00166
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 6PJU PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 6PJU PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Patricia Halverson, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES 1. MEDICARE/MEDICAID PROVIDER NO. (L1) 2.STATE VENDOR OR MEDICAID NO. (L2) 5. EFFECTIVE DATE CHANGE OF OWNERSHIP (L9) 6. DATE OF SURVEY (L34) 8. ACCREDITATION STATUS:
DEPARTMENT OF HEALTH AND HUMAN SERVICES 1. MEDICARE/MEDICAID PROVIDER NO. (L1) 2.STATE VENDOR OR MEDICAID NO. (L2) 5. EFFECTIVE DATE CHANGE OF OWNERSHIP (L9) 6. DATE OF SURVEY (L34) 8. ACCREDITATION STATUS:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00360
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: BFJG PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: BFJG PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00861
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 33K1 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 33K1 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00598
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: L7X6 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: L7X6 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Lou Anne Page, HFE NE II
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: Z6PT PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: Z6PT PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 0D7L Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 0D7L Facility ID:
Timothy Rhonemus, NFE NEII
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 6VZG Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 6VZG Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: JSZI Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: JSZI Facility ID:
Terri Ament, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: MKQC Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: MKQC Facility ID:
Gail Anderson, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 0H11 Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 0H11 Facility ID:
Jonathan Hill, HFE NE II. Kate JohnsTon, Program Specialist. Posted 11/16/2015 Co.
 7 11/04 Jonathan Hill, HFE NE II 11/04 Kate JohnsTon, Program Specialist 1 3 Posted 11/16/2015 Co. Protecting, Maintaining and Improving the Health of Minnesotans CMS Certification Number (CCN): 245411
7 11/04 Jonathan Hill, HFE NE II 11/04 Kate JohnsTon, Program Specialist 1 3 Posted 11/16/2015 Co. Protecting, Maintaining and Improving the Health of Minnesotans CMS Certification Number (CCN): 245411
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: GR6J Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: GR6J Facility ID:
Writing a Plan of Correction
 Writing a Plan of Correction for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252 www.polaris-group.com Writing
Writing a Plan of Correction for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252 www.polaris-group.com Writing
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 23242
 CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : KHKN PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 23242 1. MEDICARE/MEDICA PROVER NO. (L1) 2.STATE VENDOR
CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : KHKN PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 23242 1. MEDICARE/MEDICA PROVER NO. (L1) 2.STATE VENDOR
Jane Teipel, HFE NEII
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : S9GX Facility : 00847 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : S9GX Facility : 00847 1. MEDICARE/MEDICA
Lisa Carey, HFE NE II
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : VNT4 PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00797 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : VNT4 PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00797 1. MEDICARE/MEDICA
Center for Clinical Standards and Quality/Survey & Certification Group
 DRAFT DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2 21 16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DRAFT DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2 21 16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
Gayle Lantto, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : 6EX1 PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00756 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : 6EX1 PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00756 1. MEDICARE/MEDICA
Gayle Lantto, Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 5LL3 Facility : 00979 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 5LL3 Facility : 00979 1. MEDICARE/MEDICA
IMPORTANT NOTICE PLEASE READ CAREFULLY SENT VIA FEDEX AND INTERNET (Receipt of this notice is presumed to be May 7, 2018 date notice ed)
") Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 ` Refer to: 34-5529.NOTC.G.05.07.18.docx IMPORTANT NOTICE PLEASE
Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 ` Refer to: 34-5529.NOTC.G.05.07.18.docx IMPORTANT NOTICE PLEASE
#212 How to Submit a Successful Informal Dispute Resolution (IDR)
") #212 How to Submit a Successful Informal Dispute Resolution (IDR) Wisconsin Health Care Association April 12, 2018 3:30pm to 4:30pm By: Leah Killian Smith, BA, NHA, RHIA, HSE Director of Quality & Government
#212 How to Submit a Successful Informal Dispute Resolution (IDR) Wisconsin Health Care Association April 12, 2018 3:30pm to 4:30pm By: Leah Killian Smith, BA, NHA, RHIA, HSE Director of Quality & Government
Gloria Derfus, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: CU09 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: CU09 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
G-TAGS A RE T HEY THE N EW IJ S?
 G-TAGS A RE T HEY THE N EW IJ S? LIBBY YOUSE, LNHA LONG TERM CARE LEADERSHIP COACH QIPMO SINCLAIR SCHOOL OF NURSING UNIVERSITY OF MISSOURI WHY TAKE A LOOK AT G TAGS November of 2016 brought in Phase I
G-TAGS A RE T HEY THE N EW IJ S? LIBBY YOUSE, LNHA LONG TERM CARE LEADERSHIP COACH QIPMO SINCLAIR SCHOOL OF NURSING UNIVERSITY OF MISSOURI WHY TAKE A LOOK AT G TAGS November of 2016 brought in Phase I
Teresa Ament, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : JOZS PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00861 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL : JOZS PART I - TO BE BY THE STATE SURVEY AGENCY Facility : 00861 1. MEDICARE/MEDICA
Michele McFarland, HFE NE II
 CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 2S25 Facility : 00124 1. MEDICARE/MEDICA PROVER NO. (L1) 2.STATE VENDOR
CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 2S25 Facility : 00124 1. MEDICARE/MEDICA PROVER NO. (L1) 2.STATE VENDOR
Annual Quality Improvement Report on the Nursing Home Survey Process
 Commissioner s Office 625 Robert St. N., Suite 500 P.O. Box 64975 St. Paul, MN 55164-0975 (651) 201-5000 Annual Quality Improvement Report on the Nursing Home Survey Process Minnesota Department of Health
Commissioner s Office 625 Robert St. N., Suite 500 P.O. Box 64975 St. Paul, MN 55164-0975 (651) 201-5000 Annual Quality Improvement Report on the Nursing Home Survey Process Minnesota Department of Health
IMPORTANT NOTICE PLEASE READ CAREFULLY SENT VIA FEDEX AND INTERNET
 Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 Refer to: 5213.abIJ.06.27.18. docx ` June 27, 2018 IMPORTANT
Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 Refer to: 5213.abIJ.06.27.18. docx ` June 27, 2018 IMPORTANT
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 02HR Facility : 00538 1. MEDICARE/MEDICA PROVER NO. (L1) 245255 2.STATE
CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 02HR Facility : 00538 1. MEDICARE/MEDICA PROVER NO. (L1) 245255 2.STATE
Annual Quality Improvement Report on the Nursing Home Survey Process
 Annual Quality Improvement Report on the Nursing Home Survey Process Report to the Minnesota Legislature Minnesota Department of Health Federal Fiscal Year 2010 Released Commissioner s Office 625 Robert
Annual Quality Improvement Report on the Nursing Home Survey Process Report to the Minnesota Legislature Minnesota Department of Health Federal Fiscal Year 2010 Released Commissioner s Office 625 Robert
Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates
 Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates Charlene Kawchak-Belitsky, R.N., BSN, NHA Senior manager, IDR/IIDR, MPRO Presented to LeadingAge Michigan
Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates Charlene Kawchak-Belitsky, R.N., BSN, NHA Senior manager, IDR/IIDR, MPRO Presented to LeadingAge Michigan
PACAH 2018 SPRING CONFERENCE April 26, 2018
 PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES
 DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES Mary Spracklin RN, M.S.N Rosemary Kirlin RN, M.S.N September 30, 2014 ROLE OF THE STATE AGENCY (SA) The Centers for Medicare and Medicaid Services (CMS)
DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES Mary Spracklin RN, M.S.N Rosemary Kirlin RN, M.S.N September 30, 2014 ROLE OF THE STATE AGENCY (SA) The Centers for Medicare and Medicaid Services (CMS)
Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014
 Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014 HEALTH REGULATION DIVISION Annual Quality Improvement Report: The Nursing
Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014 HEALTH REGULATION DIVISION Annual Quality Improvement Report: The Nursing
HFEL Office of Program Compliance State Enforcement (12/20/2013)
") HFEL Office of Compliance State (12/20/2013) Secretary Survey Deficiency reported on a State Survey Send Action Alert e-mail or fax to Team and Secretary Send Packet by interoffice mail to OPC 1 Prepare
HFEL Office of Compliance State (12/20/2013) Secretary Survey Deficiency reported on a State Survey Send Action Alert e-mail or fax to Team and Secretary Send Packet by interoffice mail to OPC 1 Prepare
Annual Quality Improvement Report on the Nursing Home Survey Process and Progress Reports on Other Legislatively Directed Activities
 Annual Quality Improvement Report on the Nursing Home Survey Process and Progress Reports on Other Legislatively Directed Activities Report to the Minnesota Legislature 2004 Minnesota Department of Health
Annual Quality Improvement Report on the Nursing Home Survey Process and Progress Reports on Other Legislatively Directed Activities Report to the Minnesota Legislature 2004 Minnesota Department of Health
Pub State Operations Provider Certification Transmittal- ADVANCE COPY
 CMS Manual System Pub. 100-07 State Operations Provider Certification Transmittal- AVANCE COPY epartment of Health & Human Services (HHS) Centers for Medicare & Medicaid Services (CMS) ate: XXXX SUBJECT:
CMS Manual System Pub. 100-07 State Operations Provider Certification Transmittal- AVANCE COPY epartment of Health & Human Services (HHS) Centers for Medicare & Medicaid Services (CMS) ate: XXXX SUBJECT:
Lyla Burkman, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 9DHU Facility : 00078 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 9DHU Facility : 00078 1. MEDICARE/MEDICA
Complaint Investigations of Minnesota Health Care Facilities
 Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2004 to June 30, 2007 and
Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2004 to June 30, 2007 and
PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS
 PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS Email: DAN.ARNOLD@HOMEINSTEAD.COM March 14, 2017 Mr. Daniel Arnold, Administrator Home Instead Senior Care 1883 Station Parkway NW, Ste
PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS Email: DAN.ARNOLD@HOMEINSTEAD.COM March 14, 2017 Mr. Daniel Arnold, Administrator Home Instead Senior Care 1883 Station Parkway NW, Ste
Protecting, Maintaining and Improving the Health of Minnesotans. Re: Enclosed Follow-up Survey Results - Project Number SL
 Email: JENNIFERCAREFULLY@YAHOO.COM August 31, 2015 Ms. Jennifer Persaud, Administrator Care-Fully Senior Home Care 13361 Wyola Road Minnetonka, MN 55305 Re: Enclosed Follow-up Survey Results - Project
Email: JENNIFERCAREFULLY@YAHOO.COM August 31, 2015 Ms. Jennifer Persaud, Administrator Care-Fully Senior Home Care 13361 Wyola Road Minnetonka, MN 55305 Re: Enclosed Follow-up Survey Results - Project
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: GRIK Facility ID: 00936 1. MEDICARE/MEDICAID PROVIDER NO.
CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: GRIK Facility ID: 00936 1. MEDICARE/MEDICAID PROVIDER NO.
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : MLV4 Facility : 00226 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : MLV4 Facility : 00226 1. MEDICARE/MEDICA
PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS
 PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS Certified Mail # 7015 1520 0000 6771 3650 Email: MARKGLESENER@GLESENERS.COM August 1, 2016 Mr. Mark Glesener, Administrator Gleseners
PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANS Certified Mail # 7015 1520 0000 6771 3650 Email: MARKGLESENER@GLESENERS.COM August 1, 2016 Mr. Mark Glesener, Administrator Gleseners
Determination of Compliance: The Division of Health Improvement, Quality Management Bureau has determined your agency is in:
 Date: October 18, 2012 To: Pat Posey, President Provider: A New Vision Case Management, Inc. Address: P.O. Box 56685 State/Zip: Albuquerque, New Mexico 87187 E-mail Address: anewvisioncm@aol.com Region:
Date: October 18, 2012 To: Pat Posey, President Provider: A New Vision Case Management, Inc. Address: P.O. Box 56685 State/Zip: Albuquerque, New Mexico 87187 E-mail Address: anewvisioncm@aol.com Region:
Danette Bakken, HFE II
 CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 3O28 Facility : 00125 1. MEDICARE/MEDICA PROVER NO.(L1) 245528 2. STATE
CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 3O28 Facility : 00125 1. MEDICARE/MEDICA PROVER NO.(L1) 245528 2. STATE
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73
 DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73 NURSING FACILITIES/MEDICAID - REMEDIES 411-073-0000 Purpose The purpose of
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73 NURSING FACILITIES/MEDICAID - REMEDIES 411-073-0000 Purpose The purpose of
Informal Dispute Resolution Finding Your Seat at the Table
 Informal Dispute Resolution Finding Your Seat at the Table Jennifer L. Hardesty, PharmD, FASCP Chief Clinical Officer, Corporate Compliance Officer Remedi SeniorCare William M. Vaughan BSN, RN Vice President,
Informal Dispute Resolution Finding Your Seat at the Table Jennifer L. Hardesty, PharmD, FASCP Chief Clinical Officer, Corporate Compliance Officer Remedi SeniorCare William M. Vaughan BSN, RN Vice President,
Center for Medicaid, CHIP, and Survey & Certification/Survey & Certification Group. Memorandum Summary
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
Gloria Derfus, Unit Supervisor
 DEPARTMENT OF HEALTH AND HUMAN SERVIES ENTERS FOR MEDIARE & MEDIA SERVIES MEDIARE/MEDIA ERTIFIATION AND TRANSMITTAL PART I - TO BE OMPLETED BY THE STATE SURVEY AGENY : 0QGF Facility : 00522 1. MEDIARE/MEDIA
DEPARTMENT OF HEALTH AND HUMAN SERVIES ENTERS FOR MEDIARE & MEDIA SERVIES MEDIARE/MEDIA ERTIFIATION AND TRANSMITTAL PART I - TO BE OMPLETED BY THE STATE SURVEY AGENY : 0QGF Facility : 00522 1. MEDIARE/MEDIA
P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s
 P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s March 19, 2018 Ms. Beth Schroeder, Administrator Minnesota Masonic Home Care Center
P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s March 19, 2018 Ms. Beth Schroeder, Administrator Minnesota Masonic Home Care Center
Trends in Nursing Facility Standard Health Survey Citations
 Trends in Nursing Facility Standard Health Survey Citations Prepared by Research Department American Health Care Association March 2015 Trends in Nursing Facilities Standard Health Survey Citations TABLE
Trends in Nursing Facility Standard Health Survey Citations Prepared by Research Department American Health Care Association March 2015 Trends in Nursing Facilities Standard Health Survey Citations TABLE
June 22, Ms. Erin Hilligan, Administrator Ebenezer Home Care 2722 Park Ave South Saint Louis Park, MN 55416
 Email: EHILLIG1@FAIRVIEW.ORG June 22, 2016 Ms. Erin Hilligan, Administrator Ebenezer Home Care 2722 Park Ave South Saint Louis Park, MN 55416 Re: Enclosed State Licensing Orders Project Number SL28789004
Email: EHILLIG1@FAIRVIEW.ORG June 22, 2016 Ms. Erin Hilligan, Administrator Ebenezer Home Care 2722 Park Ave South Saint Louis Park, MN 55416 Re: Enclosed State Licensing Orders Project Number SL28789004
NEBRASKA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NEBRASKA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NEBRASKA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
Lisa Hakanson, HFE NEII
 CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : X8U4 Facility : 00979 1. MEDICARE/MEDICA PROVER NO. (L1) 245264 2.STATE
CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : X8U4 Facility : 00979 1. MEDICARE/MEDICA PROVER NO. (L1) 245264 2.STATE
Protecting, Maintaining and Improving the Health of Minnesotans
 Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7008 1830 0003 8091 7548 April 16, 2010 Mary Adams, Administrator Solbakken 7733 West 99 th Street Circle Bloomington, MN
Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7008 1830 0003 8091 7548 April 16, 2010 Mary Adams, Administrator Solbakken 7733 West 99 th Street Circle Bloomington, MN
WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY
 WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY Presented to: Massachusetts Senior Care Association October 27, 2017 Today s Presenters 2 Robert Griffin, Esq. Managing Partner Anthony
WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY Presented to: Massachusetts Senior Care Association October 27, 2017 Today s Presenters 2 Robert Griffin, Esq. Managing Partner Anthony
31 (L37) (L38) (L39) (L42) (L43)
 (L38) (L39) (L42) (L43)") DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 2NB3 Facility : 00365 MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : 2NB3 Facility : 00365 MEDICARE/MEDICA
Cheryl Johnson, HFE NEII
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : VN0N Facility : 00587 1. MEDICARE/MEDICA
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICA SERVICES MEDICARE/MEDICA CERTIFICATION AND TRANSMITTAL PART I - TO BE BY THE STATE SURVEY AGENCY : VN0N Facility : 00587 1. MEDICARE/MEDICA
The Division of Health Improvement, Quality Management Bureau has determined your agency is now in:
 Date: February 26, 2014 To: Barbara Anderson, Executive Director Provider: R-Way, LLC Address: 4001 Office Court, Suite 905 State/Zip: Santa Fe, New Mexico 87507 E-mail Address: Barbann1123@aol.com Region:
Date: February 26, 2014 To: Barbara Anderson, Executive Director Provider: R-Way, LLC Address: 4001 Office Court, Suite 905 State/Zip: Santa Fe, New Mexico 87507 E-mail Address: Barbann1123@aol.com Region:
Complaint Investigations of Minnesota Health Care Facilities
 Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2007 to June 30, 2010 and
Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2007 to June 30, 2010 and
Informal Dispute Resolution. Rules, Process, and Case Theory
 Informal Dispute Resolution Rules, Process, and Case Theory The Rules KSA 39-947a and KAR 26-39-438 through 440 provide the statutory and regulatory framework for the IDR process. The CMS SOM and supporting
Informal Dispute Resolution Rules, Process, and Case Theory The Rules KSA 39-947a and KAR 26-39-438 through 440 provide the statutory and regulatory framework for the IDR process. The CMS SOM and supporting
October 27, the Centers. established
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Western Division of Survey and Certification Seattle Regional Office 701 Fifth Avenue, Suite 1600 Seattle, WA 98104 IMPORTAN
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Western Division of Survey and Certification Seattle Regional Office 701 Fifth Avenue, Suite 1600 Seattle, WA 98104 IMPORTAN
Managing employees include: Organizational structures include: Note:
 Nursing Home Transparency Provisions in the Patient Protection and Affordable Care Act Compiled by NCCNHR: The National Consumer Voice for Quality Long-Term Care, April 2010 Part I Improving Transparency
Nursing Home Transparency Provisions in the Patient Protection and Affordable Care Act Compiled by NCCNHR: The National Consumer Voice for Quality Long-Term Care, April 2010 Part I Improving Transparency
DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE
 DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE I NUMBER DATE OF ISSUE December 27,2007 J EFFECTIVE DATE January 1,2008 00-08-01 ------- SUBJECT' BY: Process for
DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE I NUMBER DATE OF ISSUE December 27,2007 J EFFECTIVE DATE January 1,2008 00-08-01 ------- SUBJECT' BY: Process for
A final version of the correction order form is enclosed. This document will be posted on the MDH website.
 Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7009 1410 0000 2303 7434 April 14, 2010 Laura Lokken, Administrator Golden Oaks 4067 Reinke Road Hermantown, MN 55811 Re:
Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7009 1410 0000 2303 7434 April 14, 2010 Laura Lokken, Administrator Golden Oaks 4067 Reinke Road Hermantown, MN 55811 Re:
2012: Living Supports (Supported Living, Family Living); Inclusion Supports (Customized Community Supports, Community Integrated Employment Services)
; Inclusion Supports (Customized Community Supports, Community Integrated Employment Services)") Date: September 22, 2016 To: Diane Romero, Executive Director Provider: Ensuenos y Los Angelitos Development Center Address: 1030 Salazar Rd State/Zip: Taos, New Mexico 87571 E-mail Address: dromero@eladc.org
Date: September 22, 2016 To: Diane Romero, Executive Director Provider: Ensuenos y Los Angelitos Development Center Address: 1030 Salazar Rd State/Zip: Taos, New Mexico 87571 E-mail Address: dromero@eladc.org
CMS and DOH Enforcement Activities and Proactive Strategies
 PACAH 2017 Spring Conference April 27, 2017 CMS and DOH Enforcement Activities and Proactive Strategies Paula G. Sanders, Esquire CMS Requirements of Participation (RoPs) Published October 4, 2016 (81
PACAH 2017 Spring Conference April 27, 2017 CMS and DOH Enforcement Activities and Proactive Strategies Paula G. Sanders, Esquire CMS Requirements of Participation (RoPs) Published October 4, 2016 (81
2012: Living Supports (Supported Living); Inclusion Supports (Customized Community Supports) and Other (Customized In-Home Supports)
; Inclusion Supports (Customized Community Supports) and Other (Customized In-Home Supports)") Date: September 27, 2016 To: Melvin Parker, Co-Owner Provider: Onyx Supportive Living, LLC Address: 211 Montano NW Suite H State/Zip: Albuquerque, New Mexico 87107 E-mail Address: mparker@oslllc.com Region:
Date: September 27, 2016 To: Melvin Parker, Co-Owner Provider: Onyx Supportive Living, LLC Address: 211 Montano NW Suite H State/Zip: Albuquerque, New Mexico 87107 E-mail Address: mparker@oslllc.com Region:
AMENDED June 18, 2015 By Certified Mail and Facsimile
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Midwest Division of Survey and Certification Chicago Regional Office 233 North Michigan Avenue, Suite 600 Chicago, IL 60601-5519
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Midwest Division of Survey and Certification Chicago Regional Office 233 North Michigan Avenue, Suite 600 Chicago, IL 60601-5519
P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s
 P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s August 15, 2018 Ms. Katie Davis, Administrator Good Samaritan Society - Albert Lea 75507
P r o t e c t i n g, M a i n t a i n i n g a n d I m p r o v i n g t h e H e a l t h o f A l l M i n n e s o t a n s August 15, 2018 Ms. Katie Davis, Administrator Good Samaritan Society - Albert Lea 75507
FLORIDA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL FLORIDA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL FLORIDA DID NOT ALWAYS VERIFY CORRECTION OF DEFICIENCIES IDENTIFIED DURING SURVEYS OF NURSING HOMES PARTICIPATING IN MEDICARE AND MEDICAID
Protecting, Maintaining and Improving the Health of Minnesotans
 Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7008 2810 0001 2558 0590 October 28, 2009 Donna Taylor, Administrator Ridgeview LLC 2020 Ridgeview Drive International Falls,
Protecting, Maintaining and Improving the Health of Minnesotans Certified Mail # 7008 2810 0001 2558 0590 October 28, 2009 Donna Taylor, Administrator Ridgeview LLC 2020 Ridgeview Drive International Falls,
Protecting, Maintaining and Improving the Health of Minnesotans
 Certified Mail # 7005 0390 0006 1222 1422 April 4, 2006 Larry Lindberg, Administrator Midwest Medical Holdings LLC 8400 Coral Sea St Suite 100 Blaine, MN 55449 Re: Licensing Follow Up Revisit Dear Mr.
Certified Mail # 7005 0390 0006 1222 1422 April 4, 2006 Larry Lindberg, Administrator Midwest Medical Holdings LLC 8400 Coral Sea St Suite 100 Blaine, MN 55449 Re: Licensing Follow Up Revisit Dear Mr.
DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 069 LONG TERM CARE ASSESSMENT
 411-069-0000 Definitions DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 069 LONG TERM CARE ASSESSMENT Unless the context indicates otherwise,
411-069-0000 Definitions DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 069 LONG TERM CARE ASSESSMENT Unless the context indicates otherwise,
SUBJECT Supported Living Cost Containment Measures YEAR PROCEDURE NUMBER APD
 SUBJECT Supported Living Cost Containment Measures YEAR 1-8-08 PROCEDURE NUMBER APD 17-001 PROCEDURE MAINTENANCE ADMINISTRATOR: Home and Community-Based Services PURPOSE: This operating procedure describes
SUBJECT Supported Living Cost Containment Measures YEAR 1-8-08 PROCEDURE NUMBER APD 17-001 PROCEDURE MAINTENANCE ADMINISTRATOR: Home and Community-Based Services PURPOSE: This operating procedure describes
Sherri Proffer, RN, Program Manager. Dorothy Ukegbu, RN Coordinator, 02/20/2014 1
 Sherri Proffer, RN, Program Manager Dorothy Ukegbu, RN Coordinator, 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures
Sherri Proffer, RN, Program Manager Dorothy Ukegbu, RN Coordinator, 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures
A GUIDE TO HOSPICE SERVICES
 A GUIDE TO HOSPICE SERVICES PURPOSE: Minnesota Rules 4664.0140, subpart 1 states: "Every individual applicant for a license, and every person who provides direct care, supervision of direct care, or management
A GUIDE TO HOSPICE SERVICES PURPOSE: Minnesota Rules 4664.0140, subpart 1 states: "Every individual applicant for a license, and every person who provides direct care, supervision of direct care, or management
College of American Pathologists 325 Waukegan Road, Northfield, Illinois Advancing Excellence
 Attachment A College of American Pathologists 325 Waukegan Road, Northfield, Illinois 60093-2750 800-323-4040 http://www.cap.org Advancing Excellence August 31, 20XX Reference Number: 2365 CAP Number:
Attachment A College of American Pathologists 325 Waukegan Road, Northfield, Illinois 60093-2750 800-323-4040 http://www.cap.org Advancing Excellence August 31, 20XX Reference Number: 2365 CAP Number: