ED Overcrowding and CEDOCS: The Community Emergency Department Overcrowding Scale
|
|
|
- Carol Mitchell
- 5 years ago
- Views:
Transcription

1
2 ED Overcrowding and CEDOCS: The Community Emergency Department Overcrowding Scale Steven Weiss, MD Professor of Emergency Medicine University of New Mexico Health Sciences Center
3 Overcrowding Introduction Causes Consequences Solutions NEDOCS studies CEDOCS 3
4 Introduction EDs provide an important public service mission Overcrowding diminishes the capability of the ED to manage emergencies effectively 4
5 Introduction In the 1990s o US hospitals: due to downsizing, mergers and closures lost > 100,000 beds 7800 medical/surgical ICU beds o # ED visits grew 15% 5
6 Introduction How crowded is overcrowded? Although ED crowding has been a topic of frequent investigation, current definitions of the problem are often implicit or focus on factors outside of the ED itself A more consistent approach to defining ED crowding would help to clarify the distinctions between causes, characteristics, and outcomes. 6
7 Introduction No gold standard No standardized scale or definition We do not know what overcrowding is but we know it when we see it! 7
8 Academic ED overcrowding Survey of 84/120 Academic EDs 51% reported daily overcrowding 94% reported overcrowding 3+ days/wk Causes o Hospital Beds 88% o Consultant delays 82% o Radiology delays 80% o Nursing shortage 78% 8
9 Rochester NY Multiple strategies tried ED internal strategies less successful Best results were from rapid removal of inpatients from the ED. 9
10 Arizona Diversion 30-50% of the time Long ED waits Major cause is shortage of inpatient beds 10
11 Publications on ED crowding Year # Publications
12 International Publications on ED crowding Japan Honk Kong/China Australia Netherlands Italy Israel Taiwan Canada India Australia 12
13 Overcrowding Introduction Causes Consequences Solutions Previous studies CEDOCS 13
14 Causes of Overcrowding 1. Increases in ED patient volumes 2. Increased complexity of diseases and associated evaluations 3. Lack of inpatient hospital beds and resources 4. National shortage of nursing and other hospital staff 5. On-call physician issues 14
15 Causes of Overcrowding (cont.) 6. Reduced primary care services 7. Managed care barriers 8. Inadequate funding 9. Prudent layperson standard 10. Non-urgent use of the ED 11. The uninsured 15
16 Overcrowding Introduction Causes Consequences Solutions Previous studies CEDOCS 16
17 Consequences of Overcrowding 1. Patients who leave without being seen 2. Patient dissatisfaction 3. Ambulance Diversion 4. Increased ED length of Stay 5. Quality Indicators 17
18 Consequences of Overcrowding 6. Medical Errors 7. Death and disability 8. Resident Education 9. Loss of autonomy 10. Issues of justice 18
19 Overcrowding Introduction Causes Consequences Solutions Previous studies CEDOCS 19
20 Short term solutions A. EMS Practices B. ED Practices C. Hospital Practices 20
21 A. EMS Practices 1. Medical Direction 2. Diversion protocols 3. Regional information management systems 4. Regional diversion saturation override 21
22 B. ED Practices 1. Real time monitoring of ED crowding metrics 2. Expanded observation services 3. Best demonstrated practices 4. Advanced triage protocols 5. Flexible triage staffing 22
23 B. ED Practices (cont.) 6. Intra-ED communications 7. Flexible bed assignments 8. Flexible staffing 9. State-of-the-art fast-track 10. ED case management 23
24 B. ED Practices (cont.) 11. Foreign language translators 12. Point-of-care payment/testing 13. Staff support and moral boosters 14. Diversion criteria 15. Use of temporary facilities 24
25 C. Hospital Practices (cont.) 1. Changing hospital culture 2. Bed monitoring process 3. Focus on inpatient operational metrics 4. Practitioner control and oversight 5. Streamlining discharges 6. Rapid admission unit 25
26 C. Hospital practices (cont.) 7. Discharge hospitality suite 8. High patient census management e.g boarding 9. Diversion readiness 10.Expedite admissions 11. Code Help 12. Internal disaster plans 26
27 Overcrowding Introduction Causes Consequences Solutions Previous studies CEDOCS 27
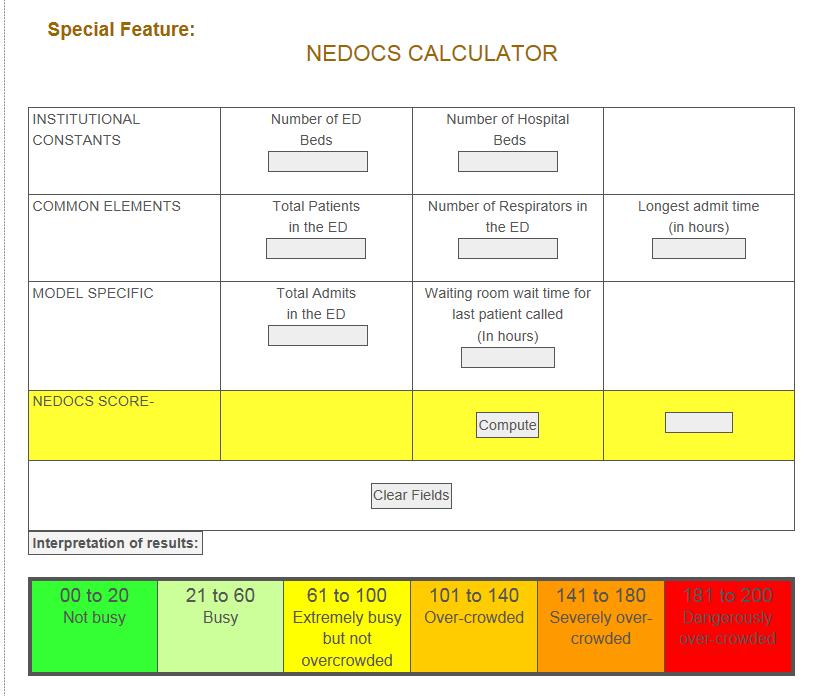
28 Part 2 Results NEDOCS score The reduced model of overcrowding o o o o o number of ED patients number of respirators in use in the ED Total admits in the ED Waiting room time for last patient called Longest admit time 28
29 29
30 Limitations Lack of a true gold standard definition Differences in definition of terms such as diversion and critical care patients Generalizable only to other academic EDs Pediatric EDs not specifically addressed Community hospitals not specifically addressed 30
31 Comparison with EDWIN EDWIN is defined as Σn i t i /Na(BT-BA), n i = number of patients in the ED in triage category t i t i = triage category based on ESI categories(1-5, 5 being most acute) Na = number of attending physicians on duty BT = number of treatment bays BA = number of admitted/obs patients in the ED 31
32 LWBS Overcrowding was found in 44% of our sampling times There was a significant correlation between LWBS and the NEDOCS score Correlation was best for LWBS and overcrowding scale 2 hours after patient registration 32
33 Overcrowding Introduction Causes Consequences Solutions Previous studies CEDOCS 33
34 Academic ED Overcrowding Scale Community ED Overcrowding scale Development of Full scale (Site Evaluation form) Stage 1A Development of Full scale (Site Evaluation form) Stage 1B Evaluation of Full scale and Reduced scale development Stage 2A Evaluation of Full scale and Reduced scale development Stage 2B Prospective Validation of scale Stage 3A Prospective Validation of scale Stage 3B Fusion of the scales for evaluation of entire community ED overcrowding issues. Stage 4 Application of scale to complex issues 1. Patients leaving prior to full medical care. 2. Medical Errors 3. Diversion 4. Patient ED Acuity levels. 5. Patient Satisfaction Stage 5
35 16 Total Hospital (Red=lowest, Bold=Highest) 35
36
37 The Psychiatric Patients 35% of sampling times had at least 1 psychiatric patient on hold Median of 2 patients (1, 2) Median time was 8 hrs (4, 14hrs) Maximum was 27 patients and 109 hours waiting in the ED

38 The Psychiatric Patients
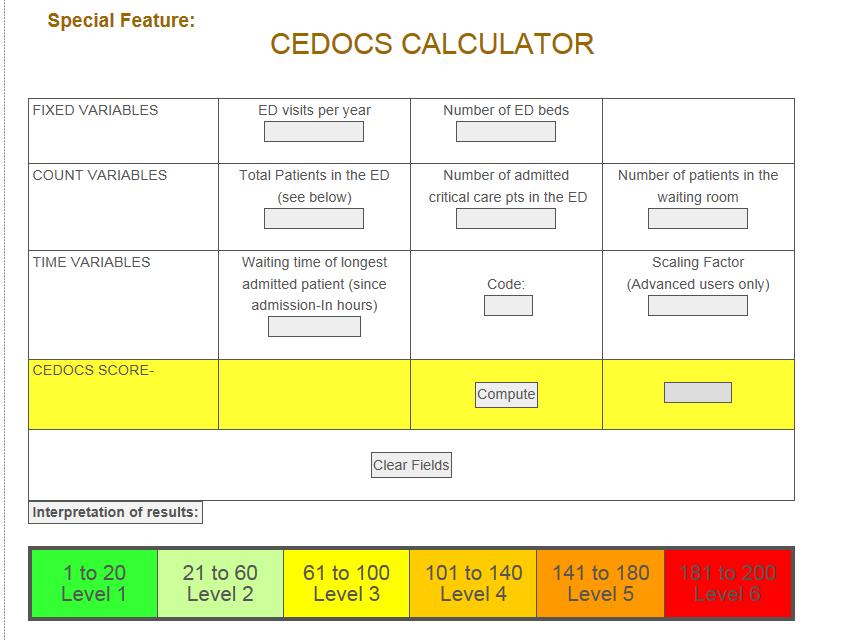
39 NEDOCS vs CEDOCS NEDOCS Number of ed beds Number of hosp beds ED patients Respirators Admits in the ED Admitted patient wait time Waiting room wait time CEDOCS Number of ed beds Number of ED visits/year ED patients Critical care patients Waiting room patients Admitted patient wait time
40 Correlation Values VAS OUTCOME CEDOCS NEDOCS R 2 comparison to Overcrowding NEDOCS 39% CEDOCS 47% 40
41 41
42 Website CEDOCS NEDOCS 42
43 QUESTIONS?
44 Thank you Steven Weiss, MD
The Future of Emergency Care in the United States Health System. Regional Dissemination Workshop New Orleans, LA November 2, 2006
 The Future of Emergency Care in the United States Health System Regional Dissemination Workshop New Orleans, LA November 2, 2006 Sponsors Josiah Macy, Jr. Foundation Agency for Healthcare Research and
The Future of Emergency Care in the United States Health System Regional Dissemination Workshop New Orleans, LA November 2, 2006 Sponsors Josiah Macy, Jr. Foundation Agency for Healthcare Research and
Emergency Department Patient Flow Strategies. University of Maryland Medical Center
 Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
ED crowding: Causes, Consequences, Solutions
 ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
The Impact of Emergency Department Use on the Health Care System in Maryland. Deborah E. Trautman, PhD, RN
 The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Frequently Asked Questions (FAQ) CALNOC 2013 Codebook
 CALNOC 2013 Codebook") Frequently Asked Questions (FAQ) CALNOC 2013 Codebook Maternal/Child and ED Service Lines QUESTION: Are the ED and Maternal/Child measures mandatory? What are the ramifications if we choose not to add
Frequently Asked Questions (FAQ) CALNOC 2013 Codebook Maternal/Child and ED Service Lines QUESTION: Are the ED and Maternal/Child measures mandatory? What are the ramifications if we choose not to add
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services,
 Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED
 Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital
 "Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
A Model for Psychiatric Emergency Services
 A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
Improving ED Flow through the UMLN II
 Improving ED Flow through the UMLN II Good Samaritan Hospital Medical Center West Islip, NY 437 beds, 50 ED beds http://www.goodsamaritan.chsli.org Good Samaritan Hospital Medical Center, a member of Catholic
Improving ED Flow through the UMLN II Good Samaritan Hospital Medical Center West Islip, NY 437 beds, 50 ED beds http://www.goodsamaritan.chsli.org Good Samaritan Hospital Medical Center, a member of Catholic
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Toronto s Mental Health and Addictions Emergency Department Alliance
 Toronto s Mental Health and Addictions Emergency Department Alliance Ian Dawe, MHSc, MD, FRCP(C) Physician-in-Chief Ontario Shores Centre for Mental Health Sciences Head, Division of General Psychiatry
Toronto s Mental Health and Addictions Emergency Department Alliance Ian Dawe, MHSc, MD, FRCP(C) Physician-in-Chief Ontario Shores Centre for Mental Health Sciences Head, Division of General Psychiatry
Publication Year: 2013
 THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
The Patient Experience: Challenges and Opportunities in the Safety Net
 The Patient Experience: Challenges and Opportunities in the Safety Net Leon L. Haley Jr., MD, MHSA, FACEP Executive Associate Dean, Clinical Services Grady Chief Medical Officer, EMCF Associate Professor
The Patient Experience: Challenges and Opportunities in the Safety Net Leon L. Haley Jr., MD, MHSA, FACEP Executive Associate Dean, Clinical Services Grady Chief Medical Officer, EMCF Associate Professor
Improving patient satisfaction by adding a physician in triage
 ORIGINAL ARTICLE Improving patient satisfaction by adding a physician in triage Jason Imperato 1, Darren S. Morris 2, Leon D. Sanchez 2, Gary Setnik 1 1. Department of Emergency Medicine, Mount Auburn
ORIGINAL ARTICLE Improving patient satisfaction by adding a physician in triage Jason Imperato 1, Darren S. Morris 2, Leon D. Sanchez 2, Gary Setnik 1 1. Department of Emergency Medicine, Mount Auburn
SENATE, No. 989 STATE OF NEW JERSEY. 218th LEGISLATURE INTRODUCED JANUARY 16, 2018
 SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED JANUARY, 0 Sponsored by: Senator JOSEPH F. VITALE District (Middlesex) Senator LORETTA WEINBERG District (Bergen) Co-Sponsored by: Senator Gordon
SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED JANUARY, 0 Sponsored by: Senator JOSEPH F. VITALE District (Middlesex) Senator LORETTA WEINBERG District (Bergen) Co-Sponsored by: Senator Gordon
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Thank you for joining us today!
 Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Low Acuity Emergency Department Visits. Joanna Cohen, MD June 2018
 Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC
 Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Emergency Departments An Essential Access Point to Care. ED Visits (millions) 22,000 20,000. Emergency Visits per ED 18,000 16,000 14,000 12,000
 22,000 20,000. Emergency Visits per ED 18,000 16,000 14,000 12,000") Emergency Departments An Essential Access Point to Care The Emergency Medical Treatment and Labor Act (EMTALA) recognizes the essential role of hospital emergency departments and requires that emergency
Emergency Departments An Essential Access Point to Care The Emergency Medical Treatment and Labor Act (EMTALA) recognizes the essential role of hospital emergency departments and requires that emergency
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds.
 Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
Emergency Departments The State of the Union Background and Benchmarks
 . Emergency Departments The State of the Union Background and Benchmarks! Prepared by: James Augustine, MD! Director of Clinical Operations, EMP! Associate Clinical Professor, Wright State University Department
. Emergency Departments The State of the Union Background and Benchmarks! Prepared by: James Augustine, MD! Director of Clinical Operations, EMP! Associate Clinical Professor, Wright State University Department
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
American College of Emergency Physicians Physician Poll on Psychiatric Emergencies October, 2016
 American College of Emergency Physicians Physician Poll on Psychiatric Emergencies October, 2016 The American College of Emergency Physicians (ACEP) conducted an online poll of 26,812 emergency physicians
American College of Emergency Physicians Physician Poll on Psychiatric Emergencies October, 2016 The American College of Emergency Physicians (ACEP) conducted an online poll of 26,812 emergency physicians
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Improving Patient Flow & Reducing Emergency Department (ED) Crowding
 Crowding") February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
Missed Nursing Care: Errors of Omission
 Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Creating a No Wait ED
 This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput : The Cambridge Health Alliance Experience
 Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
A System-Wide Approach to Creating High Performance Emergency Departments
 A System-Wide Approach to Creating High Performance Emergency Departments Copyright 2011 EmCare, Inc. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or
A System-Wide Approach to Creating High Performance Emergency Departments Copyright 2011 EmCare, Inc. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or
The annual number of ED visits in the United States
 RESEARCH DOES AN ED FLOW COORDINATOR IMPROVE PATIENT THROUGHPUT? Authors: Seamus O. Murphy, BSN, RN, CEN, CPEN, CTRN, CPHQ, NREMT-P, Bradley E. Barth, MD, FACEP, Elizabeth F. Carlton, MSN, RN, CCRN, CPHQ,
RESEARCH DOES AN ED FLOW COORDINATOR IMPROVE PATIENT THROUGHPUT? Authors: Seamus O. Murphy, BSN, RN, CEN, CPEN, CTRN, CPHQ, NREMT-P, Bradley E. Barth, MD, FACEP, Elizabeth F. Carlton, MSN, RN, CCRN, CPHQ,
Triage of children in the
 Triage of children in the emergency department Jocelyn Gravel MD, MSc Emergency department CHU Sainte-Justine June 7 th 2011 Disclosure No financial relationship to disclose or potential conflicts of interest
Triage of children in the emergency department Jocelyn Gravel MD, MSc Emergency department CHU Sainte-Justine June 7 th 2011 Disclosure No financial relationship to disclose or potential conflicts of interest
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE
 PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
wall time collaborative
 wall time collaborative a partnership to reduce ambulance patient off-load delays The 8 th Annual Behavioral Health Care Symposium December 9, 2013 wall time collaborative a partnership to reduce ambulance
wall time collaborative a partnership to reduce ambulance patient off-load delays The 8 th Annual Behavioral Health Care Symposium December 9, 2013 wall time collaborative a partnership to reduce ambulance
Clinical Study Patients Prefer Boarding in Inpatient Hallways: Correlation with the National Emergency Department Overcrowding Score
 Emergency Medicine International Volume 2011, Article ID 840459, 4 pages doi:10.1155/2011/840459 Clinical Study Patients Prefer Boarding in Inpatient Hallways: Correlation with the National Emergency Department
Emergency Medicine International Volume 2011, Article ID 840459, 4 pages doi:10.1155/2011/840459 Clinical Study Patients Prefer Boarding in Inpatient Hallways: Correlation with the National Emergency Department
NELHIN- Non-Urgent Inter-Facility Patient Transportation Pilot / Demonstration Projects
 NELHIN- Non-Urgent Inter-Facility Patient Transportation Pilot / Demonstration Projects Timiskaming District Non-Urgent Interfacility Patient Transportation Demonstration Project A Growing Problem Over
NELHIN- Non-Urgent Inter-Facility Patient Transportation Pilot / Demonstration Projects Timiskaming District Non-Urgent Interfacility Patient Transportation Demonstration Project A Growing Problem Over
How Integrated Clinical Services and Technologies are Making Healthcare Work Better. Local Practice Divisional Support National Resources
 How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
Hospital Surge Capacity for Mass Casualty Events The Israeli System
 Hospital Surge Capacity for Mass Casualty Events The Israeli System Kobi Peleg, PhD, MPH Head, National Center Trauma & Emergency Medicine Research Head, Disaster medicine Department, School of Public
Hospital Surge Capacity for Mass Casualty Events The Israeli System Kobi Peleg, PhD, MPH Head, National Center Trauma & Emergency Medicine Research Head, Disaster medicine Department, School of Public
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Are We Ready and How Do We Know? The Urgent Need for Performance Measures in Hospital Emergency Management
 Are We Ready and How Do We Know? The Urgent Need for Performance Measures in Hospital Emergency Management Nicholas V. Cagliuso, Sr., PhD (c), MPH Coordinator, Emergency Preparedness NewYork-Presbyterian
Are We Ready and How Do We Know? The Urgent Need for Performance Measures in Hospital Emergency Management Nicholas V. Cagliuso, Sr., PhD (c), MPH Coordinator, Emergency Preparedness NewYork-Presbyterian
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
FOCUS on Emergency Departments DATA DICTIONARY
 FOCUS on Emergency Departments DATA DICTIONARY Table of Contents Contents Patient time to see an emergency doctor... 1 Patient emergency department total length of stay (LOS)... 3 Length of time emergency
FOCUS on Emergency Departments DATA DICTIONARY Table of Contents Contents Patient time to see an emergency doctor... 1 Patient emergency department total length of stay (LOS)... 3 Length of time emergency
Behavioral Wellness. Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART
 Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010
 Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
San Diego County 4 th Annual Overcrowding Summit. Roneet Lev, MD, FACEP
 San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
Explain how the innovation works and why your organization chose this
 Innovation Summary: The New York Presbyterian-Weill Cornell Medicine ED Telehealth Express Care Service uses telemedicine to rapidly evaluate patients who seek care at our Emergency Departments. While
Innovation Summary: The New York Presbyterian-Weill Cornell Medicine ED Telehealth Express Care Service uses telemedicine to rapidly evaluate patients who seek care at our Emergency Departments. While
Australasian Health Facility Guidelines. Part B - Health Facility Briefing and Planning Medical Assessment Unit - Addendum to 0340 IPU
 Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
Fast Track Development at Aultman Hospital
 Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Using discrete event simulation to improve the patient care process in the emergency department of a rural Kentucky hospital.
 University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 6-2013 Using discrete event simulation to improve the patient care process
University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 6-2013 Using discrete event simulation to improve the patient care process
Stony Brook University Hospital: ED Overcrowding: Redefining the Problem with a Full Capacity Protocol
 Stony Brook University Hospital: ED Overcrowding: Redefining the Problem with a Full Capacity Protocol Problem to Be Resolved: Boarding patients in the emergency department Hospital: Location: Stony Brook
Stony Brook University Hospital: ED Overcrowding: Redefining the Problem with a Full Capacity Protocol Problem to Be Resolved: Boarding patients in the emergency department Hospital: Location: Stony Brook
Office of the Assistant Secretary for Preparedness and Response
 Office of the Assistant Secretary for Preparedness and Response Gregg Lord, MS, NREMT-P Director, Emergency Care Coordination Center HHS/ASPR Office of the Assistant Secretary for Preparedness and Response
Office of the Assistant Secretary for Preparedness and Response Gregg Lord, MS, NREMT-P Director, Emergency Care Coordination Center HHS/ASPR Office of the Assistant Secretary for Preparedness and Response
The Safe Staffing for Quality Care Act will have a profound impact on the Advanced
 Anne Marie Holler NUR 503 Group Project- Safe Staffing for Quality Care Act 11/21/11 Impact of Safe Staffing for Quality Care Act The Safe Staffing for Quality Care Act will have a profound impact on the
Anne Marie Holler NUR 503 Group Project- Safe Staffing for Quality Care Act 11/21/11 Impact of Safe Staffing for Quality Care Act The Safe Staffing for Quality Care Act will have a profound impact on the
The Effect of Emergency Department Crowding on Paramedic Ambulance Availability
 EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH The Effect of Emergency Department Crowding on Paramedic Ambulance Availability Marc Eckstein, MD Linda S. Chan, PhD From the Department of Emergency Medicine
EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH The Effect of Emergency Department Crowding on Paramedic Ambulance Availability Marc Eckstein, MD Linda S. Chan, PhD From the Department of Emergency Medicine
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY. B. To define procedures for communicating changes in diversion status.
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY Policy Reference No.: 5020 Supersedes: February 1, 2009 I. PURPOSE A. To establish guidelines under which Receiving Hospital Emergency Departments
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY Policy Reference No.: 5020 Supersedes: February 1, 2009 I. PURPOSE A. To establish guidelines under which Receiving Hospital Emergency Departments
Gender. Age DEMOGRAPHICS POINTS OF DISTINCTION COMISSION FOR ACCREDITATION OF REHABILITATION FACILITIES STATE OF FLORIDA BRAIN AND SPINAL CORD PROGRAM
 POINTS OF DISTINCTION 89-bed Acute Adult Inpatient Rehabilitation Unit, All private rooms 4 th largest Rehabilitation provider in the state of Florida Admitted 2157 patients from April 2017 through March
POINTS OF DISTINCTION 89-bed Acute Adult Inpatient Rehabilitation Unit, All private rooms 4 th largest Rehabilitation provider in the state of Florida Admitted 2157 patients from April 2017 through March
SAN MATEO MEDICAL CENTER
 ADMINISTRATIVE AND QUALITY MANAGEMENT - Accounting/Payroll - Finance and Decision Support - Patient Financial Services - Revenue and Reimbursement - Compliance/HIPAA - Materials Management - Community
ADMINISTRATIVE AND QUALITY MANAGEMENT - Accounting/Payroll - Finance and Decision Support - Patient Financial Services - Revenue and Reimbursement - Compliance/HIPAA - Materials Management - Community
ED Process Improvement Program HSAA (2012/13)
") Peterborough Regional Health Centre Update ED Process Improvement Program HSAA (2012/13) Central East Local Health Integration Network August 22, 2012 1 Overview of Presentation Focus on process improvement
Peterborough Regional Health Centre Update ED Process Improvement Program HSAA (2012/13) Central East Local Health Integration Network August 22, 2012 1 Overview of Presentation Focus on process improvement
LAC+USC Healthcare Network 1707 E Highland, Suite North State Street
 Proceedings of the 2008 Winter Simulation Conference S. J. Mason, R. R. Hill, L. Mönch, O. Rose, T. Jefferson, J. W. Fowler eds. DISCRETE EVENT SIMULATION: OPTIMIZING PATIENT FLOW AND REDESIGN IN A REPLACEMENT
Proceedings of the 2008 Winter Simulation Conference S. J. Mason, R. R. Hill, L. Mönch, O. Rose, T. Jefferson, J. W. Fowler eds. DISCRETE EVENT SIMULATION: OPTIMIZING PATIENT FLOW AND REDESIGN IN A REPLACEMENT
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS
 APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
A&E Clinical Quality Indicators June 2013
 A&E Clinical Quality Indicators June 2013 (RJE) Initial Assessment Treatment Total time in A&E Patient arrives in A&E 1.1 95% of patients waited under 17 minutes from arrival to initial assessment 1.2
A&E Clinical Quality Indicators June 2013 (RJE) Initial Assessment Treatment Total time in A&E Patient arrives in A&E 1.1 95% of patients waited under 17 minutes from arrival to initial assessment 1.2
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
EMS Subspecialty Certification Review Course. Learning Objectives
 EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION
 KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION Facility Name: Chief Administrative Officer: Chief Financial Officer: Chief Medical Officer: Corporate Tax Status: If Facility Medi-cal Certified?
KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION Facility Name: Chief Administrative Officer: Chief Financial Officer: Chief Medical Officer: Corporate Tax Status: If Facility Medi-cal Certified?
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed.
 Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT
 TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT PROJECT CHARTER Title: Toronto Western Hospital Emergency Department Acute & Sub-acute Beds Utilization Project Team: QI team: o Lucas Chartier MD, Director
TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT PROJECT CHARTER Title: Toronto Western Hospital Emergency Department Acute & Sub-acute Beds Utilization Project Team: QI team: o Lucas Chartier MD, Director
NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS
 MENTAL HEALTH DEVELOPMENTAL DISABILITIES & SUBSTANCE ABUSE NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS Status of Council Action: Developed by Clinical Services & Support Wrkgroup 1/11/08: Endorsed by
MENTAL HEALTH DEVELOPMENTAL DISABILITIES & SUBSTANCE ABUSE NORTH CAROLINA COUNCIL OF COMMUNITY PROGRAMS Status of Council Action: Developed by Clinical Services & Support Wrkgroup 1/11/08: Endorsed by
Emergency Medical Treatment and Active Labor Act. Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs
 Emergency Medical Treatment and Active Labor Act Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs What is EMTALA? The Emergency Medical Treatment and Active Labor Act is a 1986
Emergency Medical Treatment and Active Labor Act Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs What is EMTALA? The Emergency Medical Treatment and Active Labor Act is a 1986
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services
 Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
DASH Direct Admissions as Easy as 1-2-3
 DASH Direct Admissions as Easy as 1-2-3 SEAMLESS COORDINATION. EASE OF USE. POWERFUL TWO-WAY COMMUNICATION. As pioneers in the delivery of care, EmCare offers simple and practical yet powerful technologies
DASH Direct Admissions as Easy as 1-2-3 SEAMLESS COORDINATION. EASE OF USE. POWERFUL TWO-WAY COMMUNICATION. As pioneers in the delivery of care, EmCare offers simple and practical yet powerful technologies
The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay
 The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay Rose Colangelo Manager, ED Scripps Memorial Hospital Objectives
The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay Rose Colangelo Manager, ED Scripps Memorial Hospital Objectives
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo. Session ID: 325
 Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
2014 Newport Hospital Staffing Annual Report
 Patient Care Unit Name: Intensive Care Unit 2014 Newport Hospital Staffing Annual Report Critical Care 10 [x] Critical Care/ Intensive Care Unit [ ] Psychiatric Unit [ x ] Adult Number of patients upon
Patient Care Unit Name: Intensive Care Unit 2014 Newport Hospital Staffing Annual Report Critical Care 10 [x] Critical Care/ Intensive Care Unit [ ] Psychiatric Unit [ x ] Adult Number of patients upon
Join Us At The Table! NDNQI Site & Survey Coordinator Roles
 Join Us At The Table! NDNQI Site & Survey Coordinator Roles Jan Davidson Angela Christopher Donald Kelly Session ID 060 Transforming Nursing Data Into Quality Outcomes Las Vegas, Nevada January 30, 2007
Join Us At The Table! NDNQI Site & Survey Coordinator Roles Jan Davidson Angela Christopher Donald Kelly Session ID 060 Transforming Nursing Data Into Quality Outcomes Las Vegas, Nevada January 30, 2007
REDUCTION OF PSYCHIATRIC PATIENT BOARDING IN THE ED
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
Assessment of emergency room cycle time in a tertiary hospital in Egypt
 Al-Tehewy M, et al, of emergency room cycle time in a tertiary hospital 65 of emergency room cycle time in a tertiary hospital in Egypt *Mahi M. Al-Tehewy, *Ihab S. Habil, *Nayera. S. Mostafa and **Mohammed
Al-Tehewy M, et al, of emergency room cycle time in a tertiary hospital 65 of emergency room cycle time in a tertiary hospital in Egypt *Mahi M. Al-Tehewy, *Ihab S. Habil, *Nayera. S. Mostafa and **Mohammed
Division of ACF / Assisted Living Surveillance
 Division of ACF / Assisted Living Surveillance Valerie A. Deetz, Director May 2, 2017 May 2, 2017 2 Mission Statement The Division of Adult Care Facilities (ACF) and Assisted Living Surveillance will ensure
Division of ACF / Assisted Living Surveillance Valerie A. Deetz, Director May 2, 2017 May 2, 2017 2 Mission Statement The Division of Adult Care Facilities (ACF) and Assisted Living Surveillance will ensure
School of Nursing Applying Evidence to Improve Quality
 Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Healthcare Finance Management Association: Continuous Improvement Foundations
 Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
(formerly called Long-Term Acute Care Psychiatric Capacity Team ) As of October 15, 2010
 As of October 15, 2010") MPC REGIONAL PSYCHIATRIC CAPACITY ANALYSIS AND RECOMMENDATIONS Approved by RHC (October 20, 2010) and its Regional Psychiatric Capacity Team (October 8, 2010) (formerly called Long-Term Acute Care Psychiatric
MPC REGIONAL PSYCHIATRIC CAPACITY ANALYSIS AND RECOMMENDATIONS Approved by RHC (October 20, 2010) and its Regional Psychiatric Capacity Team (October 8, 2010) (formerly called Long-Term Acute Care Psychiatric
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY. Minor correction to III.E.2(a) added on 2/22/2017.
 added on 2/22/2017.") I. PURPOSE SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY Minor correction to III.E.2(a) added on 2/22/2017. To establish procedures for hospitals to divert 911 ambulance patients. Policy
I. PURPOSE SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DIVERSION POLICY Minor correction to III.E.2(a) added on 2/22/2017. To establish procedures for hospitals to divert 911 ambulance patients. Policy
Value Proposition: Tiered Network Plan Design for Navigator by Tufts Health Plan
 Value Proposition: Tiered Network Plan Design for Navigator by Tufts Health Plan John D. Freedman, MD, MBA National Health Policy Forum July 28, 2005 Outline Objectives Understand market dynamics and rationale
Value Proposition: Tiered Network Plan Design for Navigator by Tufts Health Plan John D. Freedman, MD, MBA National Health Policy Forum July 28, 2005 Outline Objectives Understand market dynamics and rationale
MINISTRY OF HEALTH AND LONG-TERM CARE. Summary of Transfer Payments for the Operation of Public Hospitals. Type of Funding
 MINISTRY OF HEALTH AND LONG-TERM CARE 3.09 Institutional Health Program Transfer Payments to Public Hospitals The Public Hospitals Act provides the legislative authority to regulate and fund the operations
MINISTRY OF HEALTH AND LONG-TERM CARE 3.09 Institutional Health Program Transfer Payments to Public Hospitals The Public Hospitals Act provides the legislative authority to regulate and fund the operations
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care
 Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care Clarke Woods, BS, RRT, FABC, Director, Cardiopulmonary Services, Pinnacle
Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care Clarke Woods, BS, RRT, FABC, Director, Cardiopulmonary Services, Pinnacle
Common Challenges of a Global Respiratory Protection Program
 Common Challenges of a Global Respiratory Protection Program Nicole Vars McCullough, PhD, CIH April 2017 British Occupational Hygiene Society Meeting Standardized Respiratory Protection Programs Top benefits
Common Challenges of a Global Respiratory Protection Program Nicole Vars McCullough, PhD, CIH April 2017 British Occupational Hygiene Society Meeting Standardized Respiratory Protection Programs Top benefits
Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department
 Original Article J Clin Med Res. 2017;9(11):911-916 Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department J. Laureano Phillips a, Bradford E. Jackson b, c,
Original Article J Clin Med Res. 2017;9(11):911-916 Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department J. Laureano Phillips a, Bradford E. Jackson b, c,