Evidenced-Based Sepsis Care at St Joseph s Medical Center, Stockton.
|
|
|
- Aileen McDonald
- 5 years ago
- Views:
Transcription

1 Evidenced-Based Sepsis Care at St Joseph s Medical Center, Stockton. Dr Kass MD MPH FACCP DAASM Dr Herrera DO Jacquie DeMellow RN MS CCRN Sarah Solberg RN MS CNS Michelle Romero RN BSN TNCC ENPC
2 Learning Objectives After this presentation participants will be able to Describe the processes that were put in place for early identification of a patient with Severe Sepsis. Describe the history and evolution of the Sepsis Team at St Josephs Hospital. Identify where we stand in improving early delivery of antibiotics and fluid resuscitation in Severe Sepsis. Discuss strategies in overcoming the challenges of the 6 Hour and 24 Hour Bundle 2
3 Sepsis Death: Necrotizing Fasciitis Woman with history of IV drug abuse causing multiple necrotic abscesses of the legs and arms walked into the Emergency Room with complaint of flu-like symptoms. Labs were drawn in triage. After a 3.5 hour wait in the lobby, she was brought to a room because of a critically high white blood cell count (66,000) and discovered to be hypotensive (BP 82/42) with a pulse of 147. IV fluids and IV antibiotics were initiated and she was admitted to telemetry. Seven hours later, she coded and was transferred to the ICU where she coded again and expired. Cause of death was likely sepsis from necrotizing fasciitis. 3
4 Sepsis Death: Necrotizing Fasciitis (6 hour window 22:25) 1557 Sign in (walked in) 1625 Triage: Flu like symptoms since last night: BP 95/55, pulse 102, resp 18, 97% RA, 4/5 abdominal pain 1721 Blood cultures drawn; Magnesium 2.9 H, Liver enzymes HH, troponin 0.65, creatinine 1.85 H, K+ 5.2 H, WBC 66.1, bands 16 H 1920 Lactic acid level drawn (6.3 HH) 1930 Roomed, BP 82/42 (MAP 55), pulse 147, 5/5 abdominal pain, alert and oriented x IV fluids started at wide open rate, morphine 4mg IVP, Rocephin IV 2020 Foley catheter inserted, BP 101/58 (MAP 72), pulse 93, 95% on 2LNP, alert and oriented x 4, 5/5 pain 2110 BP 91/69 (MAP 76), pulse 94, 96% on 2LNP, 5/5 pain 2120 Blood gas drawn: ph BP 118/67 (MAP 84), pulse 86, 97% 2LNP, 5/5 pain: Dilaudid 1mg IV administered 4
5 Sepsis Death: Necrotizing Fasciitis (6 hour window 22:25) 2250 Admit to Oncology: BP 96/74 (MAP 81), T 37, Resp 16, SpO2 94% RA 0055 Telephone admission orders included IV 90/hr CBC, chem. Panel in AM Morphine 2mg IV prn pain Wound care consult 0110 Telephone order sepsis protocol 0115 Hung IV NS at 90ml/hr 0145 Morphine 2mg IVP pain 10/10 and Ambien 10mg 0400 Morphine 2mg IVP pain 10/ Morphine 2mg IVP pain 10/10. Urine output 300ml in 8 hours, 1290ml IV input Critical WBC 79k called to Nurse 5
6 Sepsis Death: Necrotizing Fasciitis 0645 Patient demanding her methadone now: given 0655 Patient states relief from pain, drowsy, pale, diaphoretic. ALOC yet still verbally responsive to verbal and tactile stimuli RRT called, found patient unresponsive not breathing no pulses 0658 Code Blue called 0745 Patient transferred to ICU 0850 Admitting physician and intensivist at bedside, dobutamine and vasopressin ordered stat 0906 Central line inserted by intensivist, followed by left groin arterial line 0950 Daptomycin and Doripenem IV ordered 1036 CXR bilateral pulmonary edema (patient received 6 liters of IV NS between 0831 and 1050) 1125 Code blue called for PEA family decided to remove ventilator, patient pronounced 6

7 7

8 SJMC Sepsis Team 8
9 Definitions Systemic Inflammatory Response Syndrome: SIRS is widespread inflammatory response and is clinically recognized by the presence of two or more of following: Temperature >38ºC or <36ºC Heart rate >90 beats/min Respiratory rate >20 breaths/min or PaCO2 <32 mmhg WBC >12,000 cells/mm3, <4000 cells/mm3, or with >10 percent immature (band) forms 9
10 Definitions Sepsis- infection plus systemic manifestations of infection. Severe sepsis- sepsis plus sepsis induced organ dysfunction or tissue hypoperfusion Septic shock- sepsis induced hypotension persisting despite adequate fluid resuscitation. Levy MM, Fink MP, Marshall JC, et al: 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003; 31: Bone RC, Balk RA, Cerra FB, et al, and members of the ACCP/SCCM Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 1992; 101: and Crit Care Med 1992; 20:
11 EARLY GOAL-DIRECTED THERAPY IN THE TREATMENT OF SEVERE SEPSIS AND SEPTIC SHOCK Randomly assigned patients with severe sepsis or septic shock to receive either six hours of early goal-directed therapy or standard therapy (as a control) before admission to the intensive care unit. Rivers et al. NEJM
12 Mortality (%) The Importance of Early Goal-Directed Therapy for Sepsis Induced Hypoperfusion NNT to prevent 1 event (death) = Standard therapy 50 EGDT In-hospital mortality (all patients) 28-day mortality 60-day mortality Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345: Surviving Sepsis Campaign 12
13 EARLY GOAL-DIRECTED THERAPY IN THE TREATMENT OF SEVERE SEPSIS AND SEPTIC SHOCK During the interval from 7 to 72 hours, the patients assigned to early goal directed therapy had a significantly higher mean central venous oxygen saturation (70.4+/-10.7 percent vs /-11.4 percent), a lower lactate concentration (3.0 +/-4.4 vs. 3.9+/-4.4 mmol per liter), a lower base deficit (2.0+/-6.6 vs. 5.1_/-6.7 mmol per liter), and a higher ph (7.40 +/-0.12 vs /-0.12) than the patients assigned to control group. 13
14 Conclusions Early goal-directed therapy provides significant benefits with respect to outcome in patients with severe sepsis and septic shock. 14
15 Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock Kumar et al. Crit Care Med 2006 Vol. 34. No. 6 A retrospective cohort study Fourteen intensive care units Medical records of 2731 adult patients with septic shock 15
16 16

17 Clinical Innovations Severe Sepsis Goals By implementing nationally recognized evidence-based best practices, CHW will reduce severe sepsis-related in-hospital mortality by 5% and save $15 Million by June 30,


18 FY08 Goals for St. Joseph s Stockton: FY08 mortality goal: Lower mortality rate by 30% FY08 cost reduction goal: Lower inflation adjusted direct variable cost by 5%. 18
19 Strategies to Achieve Severe Sepsis Goals 1) Deploy hospital-based Clinical Innovations Sepsis Teams with clinical leaders to focus on sustained, improved sepsis outcomes using LEAN, Six Sigma and other process improvement methods 2) Identify severe sepsis and septic shock patients early and treat aggressively using the 2008 Surviving Sepsis Campaign Severe Sepsis Guidelines Educate physicians and nurses to recognize severe sepsis Leverage Rapid Response Teams Use technology (Cerner Sepsis Case Finders) to identify potential cases 3) Develop processes to support consistent implementation of the first four elements of the 6-hour Sepsis Bundle 4) Monitor compliance to the first four elements of the 6-hour sepsis bundle, provide physician-specific feedback and perform system wide benchmarking 5) Improve clinical documentation on severe sepsis patients 6) When needed, involve Palliative Care clinicians early to support the patient and family goals of care 19
20 3-Year CI Sepsis CHW System Results FY Mortality reduction = 58.2% (p <.05) Lives Saved = 1,153 Cost reduction = $36.2M 86% (N=32) Hospitals met both cost & mortality reduction goals 20
21 3-Year CI Sepsis St Joseph s Medical Center Results Mortality reduction = 44% Lives Saved = 27 Cost reduction = $1, 320,663 We met both cost & mortality reduction goals 21


22 Sepsis Health Grades Ratings ***Corresponds with project baseline*** 22
23 23

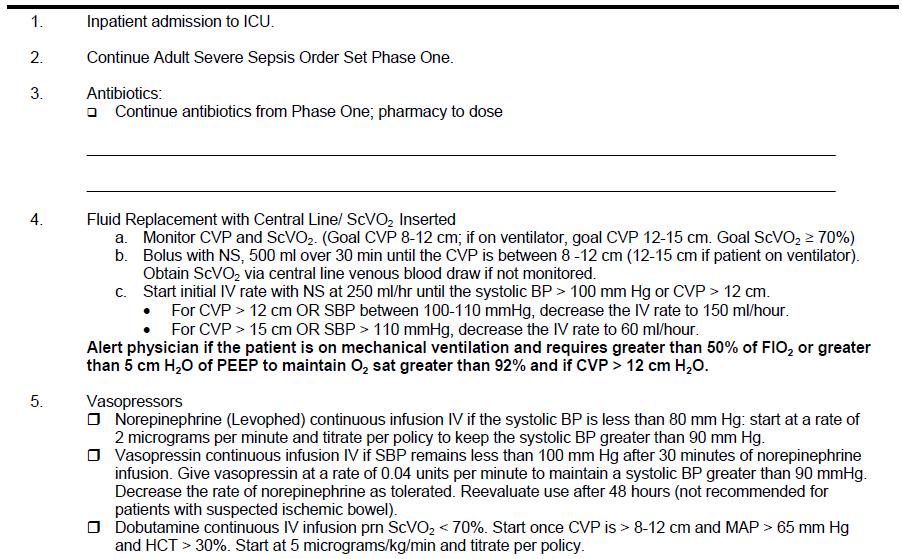
24 Phase One Order Set
25 25
26 26
27 Future Goals of the Sepsis Team FY 09 Increased use of protocols by ED physician. Combine Phase I with Phase II to ensure continuity. Combining Blood Cultures with Serum Lactates Screening patient s for Severe Sepsis whenever Blood Cultures are ordered. Identifying patients early before they get hypotensive. Use of the Oximetric Central Venous Catheter. Continue to review cases that fall out. 27
28 Future Goals of the Sepsis Team FY 09 Increased use of protocols by ED physician. Combine Phase I with Phase II to ensure continuity. Combining Blood Cultures with Serum Lactates Screening patient s for Severe Sepsis whenever Blood Cultures are ordered. Identifying patients early before they get hypotensive. Use of the Oximetric Central Venous Catheter. Continue to review cases that fall out. 28

29 Grand Rounds Meditech 29
30 SEMR78 SEMR03 SEMR22 SEMR08 SEMR75 SEMR80 SEMR06 SEMR79 SEMR07 SEMR52 SEMR46 SEMR71 SEMR69 Grand Total % cases with sepsis order set used Sepsis Order Set Used by ER MD 100% 90% 91% 80% 70% 75% 68% 60% 50% 56% 53% 50% 49% 40% 30% 27% 33% 33% 20% 10% 0% 0% 13% 0% 7% Cases Reviewed 2008 / Physician ID 30
31 Future Goals of the Sepsis Team FY 09 Increased use of protocols by ED physician. Combine Phase I with Phase II to ensure continuity. Combining Blood Cultures with Serum Lactates Screening patient s for Severe Sepsis whenever Blood Cultures are ordered. Identifying patients early before they get hypotensive. Use of the Oximetric Central Venous Catheter. Continue to review cases that fall out. 31
32 32
33 33
34 34
35 35
36 Future Goals of the Sepsis Team FY 09 Increased use of protocols by ED physician. Combine Phase I with Phase II to ensure continuity. Combining Blood Cultures with Serum Lactates Screening patient s for Severe Sepsis whenever Blood Cultures are ordered. Identifying patients early before they get hypotensive. Use of the Oximetric Central Venous Catheter. Continue to review cases that fall out. 36
37 MR# Discharg e /4/09 ED Committe e Reason for Review Date Assigned Results/Actions Taken Pt is DNR. Consider surgical consult in am 1/4/10 Care appropriate /9/09 ED No sepsis order set 1/4/10 Care appropriate /23/09 ED Blood culture timing 1/4/10 Care appropriate /3/09 ED Abx timing. Comfort Care 1/4/10 Care appropriate /5/09 ED Lactate w/in 6 hrs. Blood culture timing 1/4/ /27/09 ED 1/4/10 Care appropriate. Remind Committee to use Sepsis Order Set /7/09 ED ABX timing. 1/4/10 Mgmt controversial. No action needed /30/09 ED Inadequate bolus in ED 1/4/10 Care appropriate /27/09 ED Lactate w/in 6 hrs 1/4/ /23/09 ED Lactate w/in 6 hrs 1/4/10 Care appropriate. Remind Committee to use Sepsis Order Set /11/09 ED Transfer to ICU vs. floor 1/4/10 Does not need ED Review /14/09 Medicine /25/09 ED No fluid bolus. Abx timing. Comfort care 1/4/10 Lactate w/in 6 hrs. Abx timing 1/4/ /3/09 ED No sepsis order set 1/4/ /9/09 ED Fluid bolus inadequate 1/4/10 Care appropriate /18/09 Medicine 1/4/10 37
38 70 yr old lady brought into ED for chills and rigors. She had a temp of 39 C and history of dry cough Vital Signs T 39 HR 111 RR 32 BP 147/80 mmhg SpO2 100% on room air Labs WBC 8 Hgb HCT - 29 Plts Na K Cl CO2-22 BUN 39 Cr Lactate CXR -? RLL Pneumonia 38
39 11:44 Triage time (Sepsis screen +ve) 12:40 Lactate drawn 12:40 Blood Cultures drawn 12:49 IV Ceftriaxone given 12:00-1Liter Normal Saline 15:00-1 Liter Normal Saline Patient discharged home with follow up to primary physician and with renal physician for Creatinine
40 40
41 41
42 42
43 43
44 44
45 45
46 46
47 Milestones ICU and ED Physician champions. More aggressive fluid resuscitation. Steroids clarified. Lactate clearance. PICC Lines vs CVP lines. Eliminate Xigris. Sepsis Screening tool in Meditech. 47
48 Existing processes in place Sepsis screening tool in ED, on admission data base, daily flow sheet and RRT form. Order Sets with bulleted items except for antibiotics. RRT Order Set - start Sepsis Protocol while waiting for physician confirmation -in patients that screen positive for Sepsis. If Sepsis Patient, PICC line top priority. Chart audits 20 per month and all RRT s with Sepsis Presentation. 48

49 49
50 50
51 51
52 Sepsis Drug Xigris Pulled From Worldwide Market Robert Lowes Posted: 10/25/2011 October 25, 2011 Eli Lilly is withdrawing activated drotrecogin alfa (Xigris), a drug intended to treat severe sepsis in high-risk patients, from all markets including the United States in the wake of a new study showing that the agent did no better than a placebo in reducing mortality. The European Medicines Agency (EMA), the European equivalent of the US Food and Drug Administration (FDA), announced today that the manufacturer had informed it of the decision to pull activated drotrecogin alfa from the market worldwide, as well as discontinue all ongoing clinical trials involving the drug. The EMA stated that physicians should stop ongoing treatment of patients with activated drotrecogin alfa and should no longer start new patients on the agent a warning repeated by the FDA today. Activated drotrecogin alfa is a recombinant form of human activated protein C. The drug's efficacy has been questioned ever since the FDA authorized it for use here almost 10 years ago after a 20 to 20 vote by an agency advisory panel to recommend approval. 52
53 53
54 54
55 55
56 56
57 57
58 The ED Story 58
59 EMERGENCY DEPARTMENT Most of the hospital admissions for Sepsis begin here..in the Emergency Dept. 70% of all hospital admissions come through the ED Early identification of sepsis patients is key to timely treatment and implementation of the important sepsis bundle 59
60 60
61 61

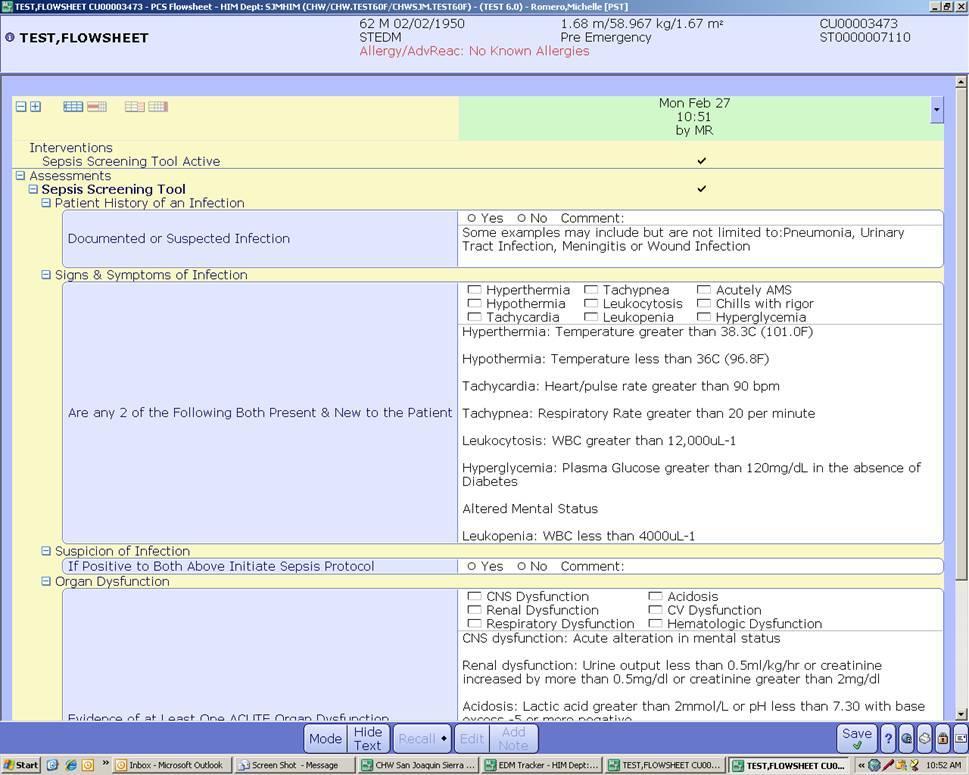
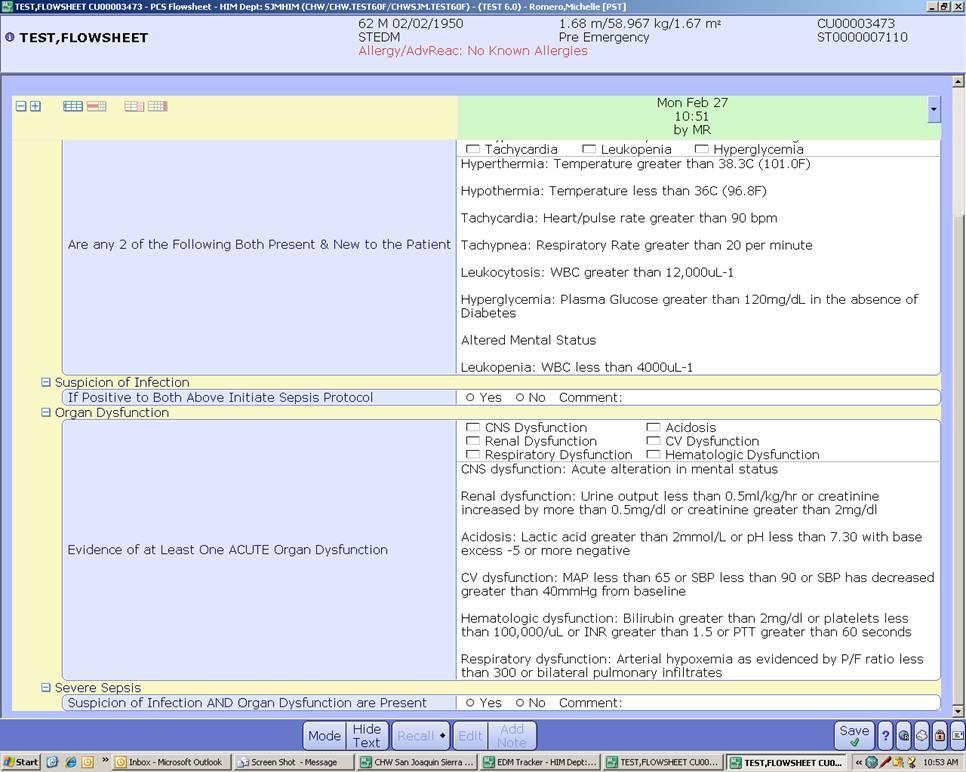
62 Meditech Electronic Health Record Moved Sepsis Screening Tool up into top five nurse assessment on triage screen 62
63 Nurse Education Importance of early Sepsis Screen on all patients who enter the ED Time goal: less than 30 minutes of arrival Often determined upon hearing pt. chief complaint & vital sign assessment Door to Vital Sign < 15 minutes 63
64 Communication Nurse communication with provider when suspect sepsis for a patient. Provider in triage (PA) does initial Medical Screening Exam (MSE). Encouraged to initiate Phase One Sepsis Orders. Use color coded alert to place on top of patient s chart while awaiting physician evaluation. Nurse request physician: This patient has screened (+) for Sepsis. Would you like to start the Sepsis Order Set?. 64

65 Sepsis Flag SUSPECT SEPSIS 65
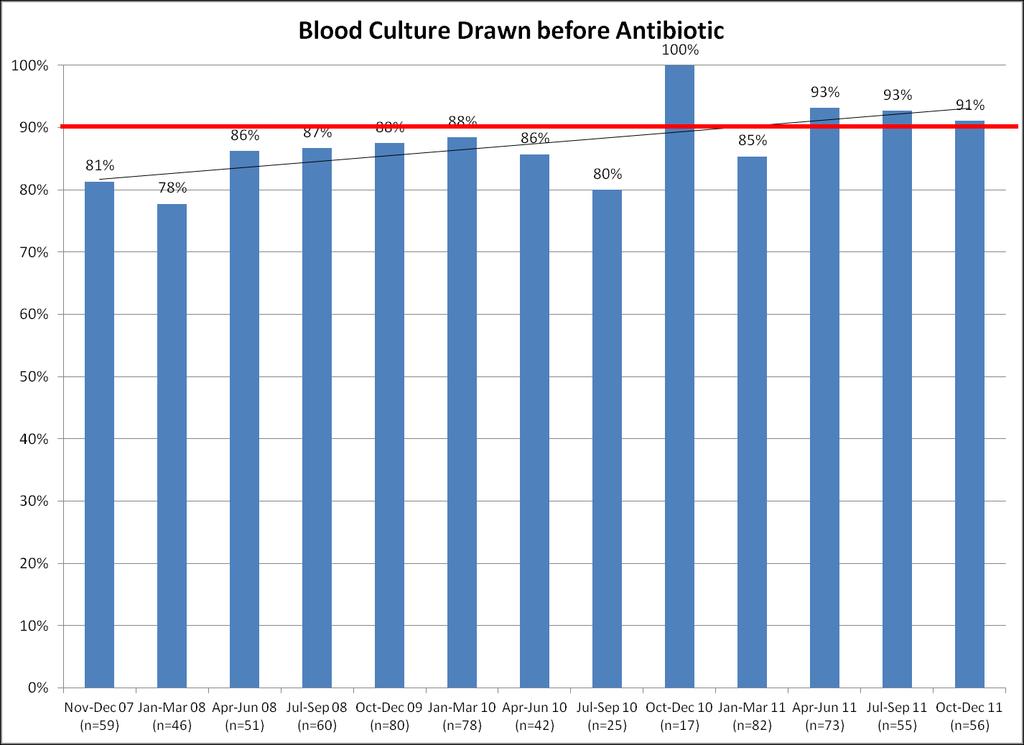
66 Blood Culture prior to Antibiotics Ongoing education about blood cultures prior to antibiotic administration Green dot placed on pt. armband by Lab after blood draw for blood culture Nurse confirms blood culture drawn Expedite antibiotics ASAP after blood cultures drawn 66
67 Antibiotic Challenge Physician enters order for antibiotic into Med orders in Meditech Pharmacist must do initial review or antibiotic order and release med Nurse waits for med to be released, then returns to remove med from Omnicell Working with Pharmacy now on trying to get key antibiotic on override to expedite administration 67
")
68 Proposed ED Triage Screen (in Test Mode) 68
69 Secondary Sepsis Screen If patient screens (-) on initial Sepsis Screen, a secondary screen is done after pertinent lab results return Sepsis Screen shows up on patient Worklist with a reminder every 30 min. to click Lab results to review Labs & conduct Secondary Sepsis Screen 69

70 Secondary Screen in ED 70

71 Worklist Secondary Sepsis Screen 71
72 Chart Audit Starting 11/11 an audit is being conducted on 20 ED patient charts/week to see if key assessments are being completed within prescribed time goals: 1. Door to Vital Signs < 15 minutes 2. Door to Sepsis Screen < 30 minutes 3. Door to Provider < 30 minutes 72
73 ED Sepsis Screening < 30 min N = 40 random audit Nov % Dec % Jan % Feb % 73
74 What has worked? Moving Sepsis Screening Tool up to Top 5 for Triage Nursing Assessment Change in Triage Flow process with additional nurse for patient reception and plan for surge to assess patients quickly Visual tools to alert provider for Sepsis Continued education with staff on need for early identification of potential sepsis patients and need to implement Sepsis Order set ASAP. 74
75 Continued Improvement Meditech: Secondary Sepsis Screen added to patient worklist with continued reminders to check for lab results & conduct secondary screen Continue to incorporate elements of Sepsis Bundle in the Sepsis Panel order screen for physicians Sepsis Order set to print out on patients who screen (+) for sepsis 75
76 The Work Goes On As with most process improvement in the hospital, key elements are: COMMUNICATION: Nurses, providers, physicians TALK SHARE.SUGGEST EDUCATION: Continue with nurse education regarding rapid assessment, early identification & sepsis bundle FEEDBACK: Let people know how we are doing, and what we can improve on! 76

77 Thank you!
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
The Power of the Pyramid:
 The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Emergency. Best Critical Care Practices
 Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6
 Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Establishing an Emergency Department Sepsis Screen
 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)
 Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)") ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016
 NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016 You are working in the emergency department (ED) of a community hospital when the ambulance arrives with A.N., a 28-year-old woman who was involved in a
NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016 You are working in the emergency department (ED) of a community hospital when the ambulance arrives with A.N., a 28-year-old woman who was involved in a
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Sepsis Mortality - A Four-Year Improvement Initiative
 Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
2014 Maryland Patient Safety Center s Call for Solutions
 Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Stampede Sepsis: A Statewide Collaborative
 Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Supplementary Appendix
 Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Greater New York Hospital Association United Hospital Fund. STOP Sepsis Collaborative Toolkit. of Severe Sepsis in the Emergency Department
 Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care. Dial in # 855/ Reference conference ID#
 MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
Number of sepsis admissions to critical care and associated mortality, 1 April March 2013
 Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Surviving Sepsis. Legacy Meridian Park Medical Center Legacy Mount Hood Medical Center
 Surviving Sepsis Legacy Meridian Park Medical Center Legacy Mount Hood Medical Center May 5, 2011 Maria Kulla RN, BSN, CCRN, ICU Nurse Sarah Barsotti RN, BSN, ICU Nurse Project Teams Legacy Mount Hood
Surviving Sepsis Legacy Meridian Park Medical Center Legacy Mount Hood Medical Center May 5, 2011 Maria Kulla RN, BSN, CCRN, ICU Nurse Sarah Barsotti RN, BSN, ICU Nurse Project Teams Legacy Mount Hood
Introduction of a comprehensive management protocol for severe sepsis is associated with sustained improvements in timeliness of care and survival
 1 Division of Critical Care Medicine, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada 2 Department of Emergency Medicine, University of British Columbia, Vancouver,
1 Division of Critical Care Medicine, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada 2 Department of Emergency Medicine, University of British Columbia, Vancouver,
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals
 A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
Our Sepsis Improvement Journey
 A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
Provider-Payer Relations: Sample Cases. Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017
 Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
ACTION PLANS. OHA Statewide Sepsis Initiative. January 13, 2016
 ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
Preventing Sepsis Mortality
 Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation
 Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2
 Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
 Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA. July 26 th, :00 a.m. 12:00 p.m. CDT
 AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
Knowledge about systemic inflammatory response syndrome and sepsis: a survey among Dutch emergency department nurses
 van den Hengel et al. International Journal of Emergency Medicine (2016) 9:19 DOI 10.1186/s12245-016-0119-2 International Journal of Emergency Medicine ORIGINAL RESEARCH Knowledge about systemic inflammatory
van den Hengel et al. International Journal of Emergency Medicine (2016) 9:19 DOI 10.1186/s12245-016-0119-2 International Journal of Emergency Medicine ORIGINAL RESEARCH Knowledge about systemic inflammatory
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
STARTER PACK: Webinar #1 SEPSIS
 STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
How Cookeville Regional Medical Center Set Up a Sepsis Program
 How Cookeville Regional Medical Center Set Up a Sepsis Program Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org SepsisSolutionsInternational
How Cookeville Regional Medical Center Set Up a Sepsis Program Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org SepsisSolutionsInternational
Code Sepsis Initiatives
 Code Sepsis Initiatives Code Sepsis Core Team St. Joseph Hospital Orange, California March 14 th, 2018 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Hospital (SJO) Overview of Presentation
Code Sepsis Initiatives Code Sepsis Core Team St. Joseph Hospital Orange, California March 14 th, 2018 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Hospital (SJO) Overview of Presentation
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
OPAT CELLULITIS PATHWAY
 OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Facilitation Interns Acquisition of
 Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
Patient Safety and Quality Measures for CRRT: The UAB Experience. Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012
 Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
RECOMMENDATION FOR CONSIDERATION
 Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Kansas Heart and Stroke Collaborative
 Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
SEPSIS Management in Scotland
 SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Seeking Sepsis in the Emergency Department- Identifying Barriers to Delivery of the Sepsis 6
 BMJ Quality Improvement Reports 2016; u206760.w3983 doi: 10.1136/bmjquality.u206760.w3983 Seeking Sepsis in the Emergency Department- Identifying Barriers to Delivery of the Sepsis 6 James Bentley, Susan
BMJ Quality Improvement Reports 2016; u206760.w3983 doi: 10.1136/bmjquality.u206760.w3983 Seeking Sepsis in the Emergency Department- Identifying Barriers to Delivery of the Sepsis 6 James Bentley, Susan
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
CMS and NHSN: What s New for Infection Preventionists in 2013 Part II
 CMS and NHSN: What s New for Infection Preventionists in 2013 Part II Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the two major
CMS and NHSN: What s New for Infection Preventionists in 2013 Part II Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the two major
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Administrative Without, TB control fails. TB Infection Control What s New? Early disease prevention Modern cough etiquette
 Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS
 #9: EARLY DETECTION & TREATMENT OF SEPSIS") Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
The impact of nighttime intensivists on medical intensive care unit infection-related indicators
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Disclosure of Proprietary Interest. HomeTown Health HCCS
 HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding