2019 COLLECTION TYPE: MEDICARE PART B CLAIMS. MEASURE TYPE: Process High Priority
|
|
|
- Jeffery Berry
- 5 years ago
- Views:
Transcription
1 Quality ID #182 (NQF 2624): Functional Outcome Assessment National Quality Strategy Domain: Communication and Care Coordination Meaningful Measure Area: Patient Reported Functional Outcomes 2019 COLLECTION TYPE: MEDICARE PART B CLAIMS MEASURE TYPE: Process High Priority DESCRIPTION: Percentage of visits for patients aged 18 years and older with documentation of a current functional outcome assessment using a standardized functional outcome assessment tool on the date of the encounter AND documentation of a care plan based on identified functional outcome deficiencies on the date of the identified deficiencies INSTRUCTIONS: This measure is to be submitted each denominator eligible visit for patients seen during the 12 month performance period. The functional outcome assessment is required to be current as defined in the definition section. This measure may be submitted by Merit-based Incentive Payment System (MIPS) eligible clinicians who perform the quality actions described in the measure based on the services provided and the measure-specific denominator coding. Measure Submission Type: Measure data may be submitted by individual MIPS eligible clinicians using Medicare Part B claims. The listed denominator criteria are used to identify the intended patient population. The numerator quality-data codes included in this specification are used to submit the quality actions allowed by the measure on the claim form(s). All measurespecific coding should be submitted on the claim(s) representing the denominator eligible encounter and selected numerator option. DENOMINAT: All visits for patients aged 18 years and older Denominator Criteria (Eligible Cases): Patients aged 18 years on date of encounter AND Patient encounter during the performance period (CPT): 97161, 97162, 97163, 97164, 97165, 97166, 97167, 97168, 98940, 98941, 98942, 98943, 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, NUMERAT: Patients with a documented current functional outcome assessment using a standardized tool AND a documented care plan based on the identified functional outcome deficiencies Definitions: Standardized Tool A tool that has been normed and validated. Examples of tools for functional outcome assessment include, but are not limited to: Oswestry Disability Index (ODI), Roland Morris Disability/Activity Questionnaire (RM), Neck Disability Index (NDI), Patient-Reported Outcomes Measurement Information System (PROMIS), Disabilities of the Arm, Shoulder and Hand (DASH), and Western Ontario and McMaster University Osteoarthritis Index Physical Function subscale (WOMAC-PF). Note: A functional outcome assessment is multi-dimensional and quantifies pain and musculoskeletal/neuromusculoskeletal capacity; therefore the use of a standardized tool assessing pain alone, such as the visual analog scale (VAS), does not meet the criteria of a functional outcome assessment standardized tool.

2 Chou R, Devo R, Friedly J, Skelly A, Hashimoto R, Weimer M...& Brodt ED. (2017). Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med, 166: Functional Outcome Assessment Patient completed questionnaires designed to measure a patient's limitations in performing the usual human tasks of living and to directly quantify functional and behavioral symptoms. Current (Functional Outcome Assessment) A patient having a documented functional outcome assessment utilizing a standardized tool and a care plan if indicated within the previous 30 days. Functional Outcome Deficiencies Impairment or loss of function related to musculoskeletal/neuromusculoskeletal capacity, may include but are not limited to: restricted flexion, extension and rotation, back pain, neck pain, pain in the joints of the arms or legs, and headaches. Care Plan A care plan is an ordered assembly of expected/planned activities or actionable elements based on identified deficiencies. These may include observations, goals, services, appointments and procedures, usually organized in phases or sessions, which have the objective of organizing and managing health care activity for the patient, often focused on one or more of the patient s health care problems. Care plans may also be known as a treatment plan. Not Eligible (Denominator Exception) A patient is not eligible if one or more of the following reasons(s) is documented at the time of the encounter: Patient refuses to participate Patient unable to complete questionnaire Patient is in an urgent or emergent medical situation where time is of the essence and to delay treatment would jeopardize the patient s health status Numerator Instructions: Documentation of a current functional outcome assessment must include identification of the standardized tool used. NUMERAT NOTE: The intent of this measure is for a functional outcome assessment tool to be utilized at a minimum of every 30 days but submission is required at each visit due to coding limitations. Therefore, for visits occurring within 30 days of a previously documented functional outcome assessment, the numerator quality-data code G8942 should be used for submission purposes. Numerator Quality-Data Coding Options: Functional Outcome Assessment Documented as Positive AND Care Plan Documented Performance Met: G8539: Functional outcome assessment documented as positive using a standardized tool AND a care plan based, on identified deficiencies on the date of the functional outcome assessment, is documented Functional Outcome Assessment Documented, No Functional Deficiencies Identified, Care Plan not Required
3 Performance Met: G8542: Functional outcome assessment using a standardized tool is documented; no functional deficiencies identified, care plan not required Functional Outcome Assessment Documented AND Care Plan Documented, if Indicated, Within the Previous 30 Days Performance Met: G8942: Functional outcome assessment using a standardized tool is documented within the previous 30 days and a care plan, based on identified deficiencies on the date of the functional outcome assessment, is documented Functional Outcome Assessment not Documented, Patient not Eligible Denominator Exception: G8540: Functional outcome assessment NOT documented as being performed, documentation the patient is not eligible for a functional outcome assessment using a standardized tool at the time of the encounter Functional Outcome Assessment Documented, Care Plan not Documented, Patient not Eligible Denominator Exception: G9227: Functional outcome assessment documented, care plan not documented, documentation the patient is not eligible for a care plan at the time of the encounter Functional Outcome Assessment not Documented, Reason not Given Performance Not Met: G8541: Functional outcome assessment using a standardized tool not documented, reason not given Functional Outcome Assessment Documented as Positive, Care Plan not Documented, Reason not Given Performance Not Met: G8543: Documentation of a positive functional outcome assessment using a standardized tool; care plan not documented, reason not given RATIONALE: Standardized outcome assessments, questionnaires or tools are a vital part of evidence-based practice. Despite the recognition of the importance of outcomes assessments, questionnaires and tools, recent evidence suggests their use in clinical practice is limited. Utilization of the appropriate outcomes assessment, questionnaires, and tools enhances clinical practice by (1) identifying and quantifying body function and structure limitations, (2) formulating evaluation, diagnosis, and prognosis, (3) forming the plan of care, (4) assisting in evaluating the patient progress towards the goals and validating the benefits of treatment, (5) improving communication between client, clinician, and third party payer, (6) assisting to improve the documentation of care provided (Lesher, et al., 2016; Potter, et al., 2011; Schenk, et al. 2016). The use of standardized tests and measures early in an episode of care establishes the baseline status of the patient/client, providing a means to quantify change in the patient's/client's functioning. Outcome measures, along with other standardized tests and measures used throughout the episode of care, as part of periodic reexamination, provide information about whether predicted outcomes are being realized (American Physical Therapy Association (APTA), 2016). Early in the intervention process, occupational therapists should select outcomes that are valid, reliable, sensitive to change; congruent with client goals and based on their actual or purported ability to predict future outcomes. Outcomes are applied to measure progress and adjust goals and interventions. Results are used to make decisions about future direction of intervention (American Occupational Therapy Association (AOTA), 2014).
4 Few outcome measures are routinely used to assess patients with neck pain other than a numeric pain rating scale. A comparison of practice patterns to current evidence suggests overutilization of some measures that have questionable reliability and underutilization of some with better supporting evidence. This practice analysis suggests that there is substantial need to implement more consistent outcome measurement (MacDermid et al., 2013). Barriers to use of classification systems and outcome measures were lack of knowledge, too limiting, and time. Classification systems are being used for decision-making in physical therapy practice for patients with lower back pain (LBP). Lack of knowledge and training seems to be the main barrier to the use of classification systems in practice (Davies et al., 2014). Lesher, et al. (2016) noted that Occupational Therapists who use assessment tools may not have understood the tools design or intent leading to overinterpretation, underinterpreation, or misuse of the tool. Treatment for musculoskeletal disorders and associated lost wages is on the increase in the U.S. One in every 2 Americans have a musculoskeletal disorder leading to an estimated cost of $213 billion for treatment, care, and lost wages (Bone and Joint Initiative, USA, 2016). Hoy, et al (2014) noted in the Global Burden of Disease Study, musculoskeletal disorders accounted for 6.8% of the total disability adjusted life years (DALYs). Of the musculoskeletal disorders, arthritis was noted to be the most common cause of disability with an estimated 51.8 million people experiencing some level of disability from arthritis (Bone and Joint Initiative, USA, 2016). Osteoarthritis of the upper limbs produces higher disability scores and earlier episodes of disability; while osteoarthritis of the knees, hips, and spine worsens with age and causes progressive disability (Montero, et al., 2016). The total cost of treating osteoarthritis is $580.9 billion, an increase of 13 percent since 2000, with an estimated 25 million people losing an average of 11.4 days of work for a total of million lost work days (Bone and Joint Initiative, USA, 2016). While arthritis is considered the most common cause of disability, there are several other musculoskeletal disorders that are prevalent. The U.S. Bureau of Labor Statistics (2015) reported that musculoskeletal disorders had the highest incidence of injury, 31% of cases, which accounted for more than four thousand lost work days, with sprains, strains, and tears being the most commonly reported. Of those injuries, the most commonly affected was the upper extremities, with hands and shoulder injuries accounting for the majority of missed days (U.S. Bureau of Labor Statistics, 2015). Also, Marik, et al. (2016) noted that half of the population will experience shoulder pain leading to decreased strength and restricted range of motion (ROM) impacting quality of life and limiting involvement in meaningful occupational activities. In addition, Blanchette, et al. (2016) reported that low back pain is one of the leading causes of disability worldwide, one of the most common reasons patients seek medical care, most common occupational disorder, and major cause of lost work days. CLINICAL RECOMMENDATION STATEMENTS: As a category, functional outcome assessments of everyday tasks are very suitable for evaluating treatment of dysfunctions of the neuromusculoskeletal system. Many questionnaires could be used; choice should depend upon the validity, reliability, responsiveness, and practicality demonstrated in the scientific literature. Functional questionnaires seek to directly quantify symptoms, function and behavior, rather than draw inferences from relevant physiological tests. Clinicians contemplating the use of functional instruments should be aware of differences between questionnaires and choose the most appropriate assessment tool for the specific purpose (Haldeman et al., 2005) (Evidence Class: I, II, III, Consensus Level: 1). Lesher, et al. (2017) and Wales, et al. (2017) found that functional assessments can be descriptive, evaluative, discriminative and/or predictive, and should be tested and validated in the population being tested. The tool should be selected based on purpose of the assessment and type of injury sustained (Lesher, et al, 2017; and Wales, et al., 2016). Utilization of validated pain and function scales help to differentiate treatment approaches in order to improve the patient's ability to function (ICSI, 2012). Clinicians should use validated functional outcome assessment tools, such as the Disabilities of the Arm, Shoulder and Hand (DASH), the American Shoulder and Elbow Surgeons shoulder scale (ASES), or the Shoulder Pain and Disability Index (SPPADI). These should be utilized before and after interventions intended to alleviate the impairments of body function and structure, activity limitations, and participation restrictions associated with adhesive capsulitis (Kelley et al., 2013) (Guideline). Clinicians should use validated self-report questionnaires, such as the Oswestry Disability Index and the Roland-Morris Disability Questionnaire. These tools are useful for identifying a patient s baseline status relative to
5 pain, function, and disability and for monitoring a change in a patient s status throughout the course of treatment (Delitto et al., 2012) (Guideline). Clinicians should use validated self-report questionnaires for patients with neck pain, to identify a patient s baseline status and to monitor changes relative to pain, function, disability, and psychosocial functioning (Blanpied et al, 2017) (Guideline). Tracking the outcomes of an implementation program is critical to evaluating its benefit to patients (Kramer et al., 2013). Understanding the clinical course of a condition can help assessment of individual patient outcomes by providing a meaningful point of reference with which to compare an individual patient s progress (Leaver et al., 2013). The Council on Chiropractic Education (2012) recommended keeping appropriate records of the patient's evaluation and case management needs to aptly respond to changes in patient status, or failure of the patient to respond to care. The Institute of Medicine s (2012) Living Well with Chronic Illness: A Call for Public Health Action stated the surveillance systems need to be improved to assess health-related quality of life and functional status of patients. The American Physical Therapy Association recommends that clinicians should utilize easily reproducible activity limitation and participation restriction measures associated with the patient s neck pain to assess the changes in the patient s level of function over the episode of care (Blanpied et al, 2017) (Guideline). The American College of Physicians 2017 guidelines for noninvasive treatment of acute, subacute, and chronic low back pain noted that the clinician should utilize non-pharmacologic interventions, such as exercise, spinal manipulation, heat, psychological therapies, etc., prior to pharmacologic interventions. Patients who received non-pharmacologic interventions demonstrated improvement in pain and overall function with fewer harms experience than those patients who received pharmacologic therapies (Chou, R., et al., 2017; & Qaseem, A., et al., 2017). Outcome assessment scales provide a concise, valid way to track function and improvement in function. Anchored numerical scales are recommended for tracking routine progress, particularly pain interference with important activities. Regional or condition functional outcome scales should be routinely used at baseline and periodic follow-ups. More frequent follow-up is recommended with higher frequency care (Washington State Department of Labor and Industries, 2014). COPYRIGHT: These measures were developed by Quality Insights, Inc. as a special project under the Quality Insights' Medicare Quality Improvement Organization (QIO) contract HHSM PA001C with the Centers for Medicare & Medicaid Services. These measures are in the public domain. Limited proprietary coding is contained in the measure specifications for convenience. Users of the proprietary code sets should obtain all necessary licenses from the owners of these code sets. Quality Insights, Inc. disclaims all liability for use or accuracy of any Current Procedural Terminology (CPT [R]) or other coding contained in the specifications. CPT contained in the Measures specifications is copyright American Medical Association. All Rights Reserved. These performance measures are not clinical guidelines, do not establish a standard of medical care, and have not been tested for all potential applications. THE MEASURES AND SPECIFICATIONS ARE PROVIDED AS IS WITHOUT WARRANTY OF ANY KIND.
6
7
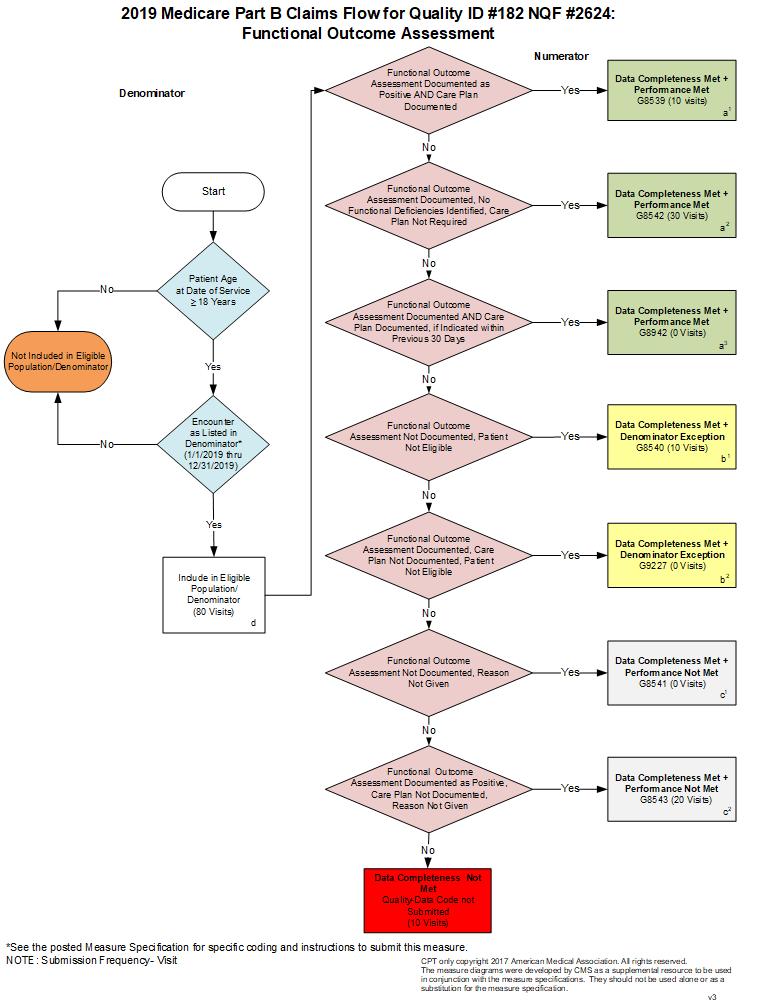
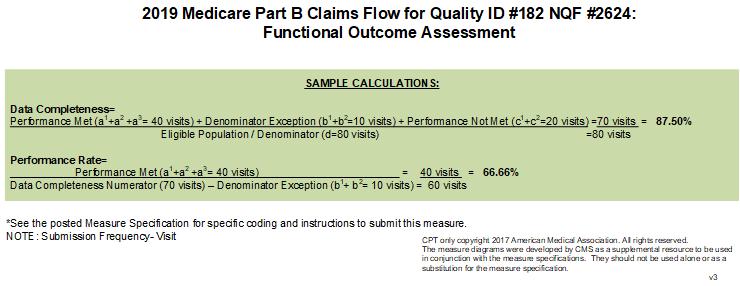
8 2019 Medicare Part B Claims Flow Narrative for Quality ID#182 NQF# 2624: Functional Outcome Assessment Please refer to the specific section of the Specification to identify the denominator and numerator information for use in submitting this Individual Specification. 1. Start with Denominator 2. Check Patient Age: a. If Patient Age is greater than or equal to 18 Years at Date of Service equals No during the performance period, do not include in Eligible Population. Stop Processing. b. If Patient Age is greater than or equal to 18 Years at Date of Service equals Yes during the performance period, proceed to check Encounter Performed. 3. Check Encounter Performed: a. If Encounter as Listed in the Denominator equals No, do not include in Eligible Population. Stop Processing. b. If Encounter as Listed in the Denominator equals Yes, include in Eligible Population. 4. Denominator Population: a. Denominator Population is all Eligible Visits in the Denominator. Denominator is represented as Denominator in the Sample Calculation listed at the end of this document. Letter d equals 80 visits in the Sample Calculation. 5. Start Numerator 6. Check Functional Outcome Assessment Documented as Positive AND Care Plan Documented: a. If Functional Outcome Assessment Documented as Positive AND Care Plan Documented equals Yes, include in Data Completeness Met and Performance Met. b. Data Completeness Met and Performance Met letter is represented as Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter a¹ equals 10 visits in the Sample Calculation. c. If Functional Outcome Assessment Documented as Positive AND Care Plan Documented equals No, proceed to check Functional Outcome Assessment Documented, No Functional Deficiencies Identified, Care Plan Not Required. 7. Check Functional Outcome Assessment Documented, No Functional Deficiencies Identified, Care Plan Not Required: a. If Functional Outcome Assessment Documented, No Functional Deficiencies Identified, Care Plan Not Required equals Yes, include in Data Completeness Met and Performance Met. b. Data Completeness Met and Performance Met letter is represented as Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter a² equals 30 visits in the Sample Calculation. c. If Functional Outcome Assessment Documented, No Functional Deficiencies Identified, Care Plan Not Required equals No, proceed to check Functional Outcome Assessment Documented AND Care Plan Documented, if Indicated within Previous 30 Days.
9 8. Check Functional Outcome Assessment Documented AND Care Plan Documented, if Indicated within Previous 30 Days: a. If Functional Outcome Assessment Documented AND Care Plan Documented, if Indicated within Previous 30 Days equals Yes, include in the Data Completeness Met and Performance Met. b. Data Completeness Met and Performance Met letter is represented as Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter a³ equals 0 visits in the Sample Calculation. c. If Functional Outcome Assessment Documented AND Care Plan Documented, if Indicated within Previous 30 Days equals No, proceed to check Functional Outcome Assessment Not Documented, Patient Not Eligible. 9. Check Functional Outcome Assessment Not Documented, Patient Not Eligible: a. If Functional Outcome Assessment Not Documented, Patient Not Eligible equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented as Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b¹ equals 10 visits in the Sample Calculation. c. If Functional Outcome Assessment Not Documented, Patient Not Eligible equals No, proceed to check Functional Outcome Assessment Documented, Care Plan Not Documented, Patient Not Eligible. 10. Check Functional Outcome Assessment Documented, Care Plan Not Documented, Patient Not Eligible: a. If Functional Outcome Assessment Documented, Care Plan Not Documented, Patient Not Eligible equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented as Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b² equals 0 visits in the Sample Calculation. c. If Functional Outcome Assessment Documented, Care Plan Not Documented, Patient Not Eligible equals No, proceed to check Functional Outcome Assessment Not Documented, Reason Not Given. 11. Check Functional Outcome Assessment Not Documented, Reason Not Given: a. If Functional Outcome Assessment Not Documented, Reason Not Given equals Yes, include in Data Completeness Met and Performance Not Met. b. Data Completeness Met and Performance Not Met letter is represented as Data Completeness in the Sample Calculation listed at the end of this document. Letter c¹ equals 0 visits in the Sample Calculation. c. If Functional Outcome Assessment Not Documented, Reason Not Given equals No, proceed to check Functional Outcome Assessment Documented as Positive, Care Plan Not Documented, Reason Not Given. 12. Check Functional Outcome Assessment Documented as Positive, Care Plan Not Documented, Reason Not Given: a. If Functional Outcome Assessment Documented as Positive, Care Plan Not Documented, Reason Not Given equals Yes, include in Data Completeness Met and Performance Not Met.

10 b. Data Completeness Met and Performance Not Met letter is represented as Data Completeness in the Sample Calculation listed at the end of this document. Letter c² equals 20 visits in the Sample Calculation. c. If Functional Outcome Assessment Documented as Positive, Care Plan Not Documented, Reason Not Given equals No, proceed to check Data Completeness Not Met. 13. Check Data Completeness Not Met: a. If Data Completeness Not Met, Quality Data Code not submitted. 10 visits have been subtracted from the Data Completeness Numerator in the Sample Calculation.
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC
 The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety
 Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Quality ID#141 (NQF 0563): Primary Open-Angle Glaucoma (POAG): Reduction of Intraocular Pressure (IOP) by 15% OR Documentation of a Plan of Care National Quality Strategy Domain: Communication and Care
Quality ID#141 (NQF 0563): Primary Open-Angle Glaucoma (POAG): Reduction of Intraocular Pressure (IOP) by 15% OR Documentation of a Plan of Care National Quality Strategy Domain: Communication and Care
A Guidebook to the 2015 Physician Quality Reporting System
 A Guidebook to the 2015 Physician Quality Reporting System Last Updated: December 22, 2014 What is PQRS? The Physician Quality Reporting System (PQRS), formally known as the Physician Quality Reporting
A Guidebook to the 2015 Physician Quality Reporting System Last Updated: December 22, 2014 What is PQRS? The Physician Quality Reporting System (PQRS), formally known as the Physician Quality Reporting
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination
: Care Plan National Quality Strategy Domain: Communication and Care Coordination") Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Quality Payment Program: The future of reimbursement
 Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Note: This is an outcome measure and will be calculated solely using registry data.
 Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
DENOMINATOR: All final reports for patients, regardless of age, undergoing a CT procedure
 Quality ID #361: Optimizing Patient Exposure to Ionizing Radiation: Reporting to a Radiation Dose Index Registry National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #361: Optimizing Patient Exposure to Ionizing Radiation: Reporting to a Radiation Dose Index Registry National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
This Material is Copyright Protected
 ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination
 Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Measure #138: Melanoma: Coordination of Care National Quality Strategy Domain: Communication and Care Coordination
 Measure #138: Melanoma: Coordination of Care National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #138: Melanoma: Coordination of Care National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care
 Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
DENOMINATOR: All final reports for patients, regardless of age, undergoing a CT procedure
 Quality ID #362: Optimizing Patient Exposure to Ionizing Radiation: Computed Tomography (CT) Images Available for Patient Follow-up and Comparison Purposes National Quality Strategy Domain: Communication
Quality ID #362: Optimizing Patient Exposure to Ionizing Radiation: Computed Tomography (CT) Images Available for Patient Follow-up and Comparison Purposes National Quality Strategy Domain: Communication
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 537 of 593
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Measure #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Measure #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Quality ID #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Note: This is an outcome measure and will be calculated solely using registry data.
 Measure #384: Adult Primary Rhegmatogenous Retinal Detachment Surgery: No Return to the Operating Room Within 90 Days of Surgery National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS
Measure #384: Adult Primary Rhegmatogenous Retinal Detachment Surgery: No Return to the Operating Room Within 90 Days of Surgery National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS
Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety
: Perioperative Temperature Management National Quality Strategy Domain: Patient Safety") Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care
 Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
CMS Issues 2018 Proposed Physician Fee Schedule: What Spine Surgeons Should Know
 CMS Issues 2018 Proposed Physician Fee Schedule: What Spine Surgeons Should Know Overview On July 13, 2017, the Centers for Medicare & Medicaid Services (CMS) issued a proposed rule that updates payment
CMS Issues 2018 Proposed Physician Fee Schedule: What Spine Surgeons Should Know Overview On July 13, 2017, the Centers for Medicare & Medicaid Services (CMS) issued a proposed rule that updates payment
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
to Orthopedic Patient-Reported Outcome Collection Tools
 to Orthopedic Patient-Reported Outcome Collection Tools A BUYER S GUIDE TO PATIENT-REPORTED Part of the OUTCOME Value-Driven COLLECTION Service TOOLS Line Series of E-Books 1 Introduction 2 The importance
to Orthopedic Patient-Reported Outcome Collection Tools A BUYER S GUIDE TO PATIENT-REPORTED Part of the OUTCOME Value-Driven COLLECTION Service TOOLS Line Series of E-Books 1 Introduction 2 The importance
Physidan Quality Reportin System
 PQR Physidan Quality Reportin System Presented to the AKA Getting started with PQRS Providers who participate between 2011-14 are eligible for incentive payments is they successfully transmit the information
PQR Physidan Quality Reportin System Presented to the AKA Getting started with PQRS Providers who participate between 2011-14 are eligible for incentive payments is they successfully transmit the information
Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety
 Complications Rate National Quality Strategy Domain: Patient Safety") Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Mary Stilphen, PT, DPT
 Mary Stilphen, PT, DPT Mary Stilphen PT, DPT is the Senior Director of Cleveland Clinic s Rehabilitation and Sports Therapy department in Cleveland, Ohio. Over the past 4 years, she led the integration
Mary Stilphen, PT, DPT Mary Stilphen PT, DPT is the Senior Director of Cleveland Clinic s Rehabilitation and Sports Therapy department in Cleveland, Ohio. Over the past 4 years, she led the integration
Clinical Appropriateness Guidelines
 Clinical Appropriateness Guidelines Guideline Description and Administrative Guidelines Effective Date: September 5, 2017 Proprietary Date of Origin: 03/30/2005 Last revised: 07/26/2016 Last reviewed:
Clinical Appropriateness Guidelines Guideline Description and Administrative Guidelines Effective Date: September 5, 2017 Proprietary Date of Origin: 03/30/2005 Last revised: 07/26/2016 Last reviewed:
AJRR Registry Platform. System Workflow Training January 2017
 AJRR Registry Platform System Workflow Training January 2017 Discussion Topics OVERVIEW: STARTING A PRO PROGRAM AT YOUR INSTITUTION Defining Your Program PROM Collection Workflow Options PART 1: REGISTRY
AJRR Registry Platform System Workflow Training January 2017 Discussion Topics OVERVIEW: STARTING A PRO PROGRAM AT YOUR INSTITUTION Defining Your Program PROM Collection Workflow Options PART 1: REGISTRY
Demonstrating the Chain of Medical Necessity. Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President
 Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Shoulder program of care. reference guide OCTOBER 2012
 Shoulder program PROGRAM OF CARE of care reference guide OCTOBER 2012 Reference guide Acknowledgements The WSIB acknowledges the significant contributions of the following regulatory colleges, regulated
Shoulder program PROGRAM OF CARE of care reference guide OCTOBER 2012 Reference guide Acknowledgements The WSIB acknowledges the significant contributions of the following regulatory colleges, regulated
Risk Adjustment Methods in Value-Based Reimbursement Strategies
 Paper 10621-2016 Risk Adjustment Methods in Value-Based Reimbursement Strategies ABSTRACT Daryl Wansink, PhD, Conifer Health Solutions, Inc. With the move to value-based benefit and reimbursement models,
Paper 10621-2016 Risk Adjustment Methods in Value-Based Reimbursement Strategies ABSTRACT Daryl Wansink, PhD, Conifer Health Solutions, Inc. With the move to value-based benefit and reimbursement models,
BACK, NECK, AND SHOULDER PAIN IN HOME HEALTH CARE WORKERS
 BACK, NECK, AND SHOULDER PAIN IN HOME HEALTH CARE WORKERS Eric M. Wood, University of Utah Kurt T. Hegmann, University of Utah Arun Garg, University of Wisconsin-Milwaukee Stephen C. Alder, University
BACK, NECK, AND SHOULDER PAIN IN HOME HEALTH CARE WORKERS Eric M. Wood, University of Utah Kurt T. Hegmann, University of Utah Arun Garg, University of Wisconsin-Milwaukee Stephen C. Alder, University
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Optum Physical Health Clinical Forms Instruction Manual
 Optum Physical Health Clinical Forms Instruction Manual OptumHealth Care Solutions Physical Health includes OptumHealth Care Solutions, LLC, ACN Group IPA of New York, Inc., Managed Physical Network, Inc.,
Optum Physical Health Clinical Forms Instruction Manual OptumHealth Care Solutions Physical Health includes OptumHealth Care Solutions, LLC, ACN Group IPA of New York, Inc., Managed Physical Network, Inc.,
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
National Quality Strategy (NQS) Domain: Communication and Care Coordination. Measure Type: Composite; Process
 Domain: Communication and Care Coordination. Measure Type: Composite; Process") Surgical Phase of Care Measure 6 ACS20 Optimal Postoperative Communication Plan and Patient Care Coordination Composite National Quality Strategy (NQS) Domain: Communication and Care Coordination Measure
Surgical Phase of Care Measure 6 ACS20 Optimal Postoperative Communication Plan and Patient Care Coordination Composite National Quality Strategy (NQS) Domain: Communication and Care Coordination Measure
Medicare: This subset aligns with the requirements defined by CMS and is for the review of Medicare and Medicare Advantage beneficiaries
 InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
PQRS Claims Based Data Collection Sheets 2014
 Measure #128 Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-up Is the patient 18+ years of age? Yes No (Not eligible) Did you bill an eligible CPT code? 97001 No (Not eligible)
Measure #128 Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-up Is the patient 18+ years of age? Yes No (Not eligible) Did you bill an eligible CPT code? 97001 No (Not eligible)
Using the patient s voice to measure quality of care
 Using the patient s voice to measure quality of care Improving quality of care is one of the primary goals in U.S. care reform. Examples of steps taken to reach this goal include using insurance exchanges
Using the patient s voice to measure quality of care Improving quality of care is one of the primary goals in U.S. care reform. Examples of steps taken to reach this goal include using insurance exchanges
Medications: Defining the Role and Responsibility of Physical Therapy Practice
 This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
Value model in the new healthcare paradigm: Producing value at a single specialty center.
 Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Performance Measures Methodology Document Performance Measures Committee March 2018
 Performance Measures Methodology Document Performance Measures Committee March 2018 Orthopaedic Practice in the US 2014 1 Survey work is conducted for the benefit of and is owned by the AAOS. Not to be
Performance Measures Methodology Document Performance Measures Committee March 2018 Orthopaedic Practice in the US 2014 1 Survey work is conducted for the benefit of and is owned by the AAOS. Not to be
Subject: DRAFT CMS Quality Measure Development Plan (MDP): Supporting the Transition to the Merit-based Incentive Payment System (MIPS) and
: Supporting the Transition to the Merit-based Incentive Payment System (MIPS) and") February 24, 2016 Attention: Eric Gilbertson Centers for Medicare & Medicaid Services MACRA Team Health Services Advisory Group, Inc. 3133 East Camelback Road Suite 240 Phoenix, AZ 85016-4545 Submitted
February 24, 2016 Attention: Eric Gilbertson Centers for Medicare & Medicaid Services MACRA Team Health Services Advisory Group, Inc. 3133 East Camelback Road Suite 240 Phoenix, AZ 85016-4545 Submitted
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Value-based Care Report. February How Value-based Care is improving quality and health.
 Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Patient-Reported Outcome Performance Measures
 Patient-Reported Outcome Performance Measures Current Environment And Next Steps Prepared for the Pharmaceutical Research and Manufacturers of America (PhRMA) by Discern Health December 2017 Executive
Patient-Reported Outcome Performance Measures Current Environment And Next Steps Prepared for the Pharmaceutical Research and Manufacturers of America (PhRMA) by Discern Health December 2017 Executive
CHAPTER 1. Documentation is a vital part of nursing practice.
 CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
2016 Physician Quality Reporting System (PQRS) Reporting Updates
 Reporting Updates") 2016 Physician Quality Reporting System (PQRS) Reporting Updates American Psychiatric Association (APA) Daniel Green, MD., F.A.C.O.G Medical Officer, CMS Division of Electronic and Clinician Quality (DECQ)
2016 Physician Quality Reporting System (PQRS) Reporting Updates American Psychiatric Association (APA) Daniel Green, MD., F.A.C.O.G Medical Officer, CMS Division of Electronic and Clinician Quality (DECQ)
Advances in Osteopathic Medicine
 Advances in Osteopathic Medicine Moving the value of osteopathic care from patients to populations Richard Snow DO, MPH Applied Health Services - Principal Choptank Community Health System Primary Care
Advances in Osteopathic Medicine Moving the value of osteopathic care from patients to populations Richard Snow DO, MPH Applied Health Services - Principal Choptank Community Health System Primary Care
Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population
 Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population Unified Quality Improvement Symposium March 31, 2017 Background Venous thromboembolism (VTE) is a
Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population Unified Quality Improvement Symposium March 31, 2017 Background Venous thromboembolism (VTE) is a
PROFESSIONAL PRACTICE 1. SAFETY Practices in a safe manner that minimizes the risk to patient, self, and others.
 PERFORMANCE CRITERIA PROFESSIONAL PRACTICE 1. SAFETY Practices in a safe manner that minimizes the risk to patient, self, and others. a. Establishes and maintains safe working environment. b. Recognizes
PERFORMANCE CRITERIA PROFESSIONAL PRACTICE 1. SAFETY Practices in a safe manner that minimizes the risk to patient, self, and others. a. Establishes and maintains safe working environment. b. Recognizes
eprescribing Information to Improve Medication Adherence
 eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
RE: Medicare Program; Request for Information Regarding the Physician Self-Referral Law
 1055 N. Fairfax Street, Suite 204, Alexandria, VA 22314, TEL (703) 299-2410, (800) 517-1167 FAX (703) 299-2411 WEBSITE www.ppsapta.org August 24, 2018 Seema Verma, MPH Administrator Centers for Medicare
1055 N. Fairfax Street, Suite 204, Alexandria, VA 22314, TEL (703) 299-2410, (800) 517-1167 FAX (703) 299-2411 WEBSITE www.ppsapta.org August 24, 2018 Seema Verma, MPH Administrator Centers for Medicare
RF ABLATION SYSTEM REIMBURSEMENT GUIDE EFFECTIVE JANUARY 2018
 REIMBURSEMENT GUIDE EFFECTIVE JANUARY 2018 Medtronic provides this information for your convenience only. It does not constitute legal advice or a recommendation regarding clinical practice. Information
REIMBURSEMENT GUIDE EFFECTIVE JANUARY 2018 Medtronic provides this information for your convenience only. It does not constitute legal advice or a recommendation regarding clinical practice. Information
Anthony Delitto, PT, Ph.D, FAPTA. Philadelphia, PA
 Implementing EBP: It s Time We Paid Attention to Measuring Clinical i l Performance Anthony Delitto, PT, Ph.D, FAPTA November 2, 2009 Philadelphia, PA Pontiac Assembly Line 1970 Grand Prix Performance
Implementing EBP: It s Time We Paid Attention to Measuring Clinical i l Performance Anthony Delitto, PT, Ph.D, FAPTA November 2, 2009 Philadelphia, PA Pontiac Assembly Line 1970 Grand Prix Performance
emja: Measuring patient-reported outcomes: moving from clinical trials into clinical p...
 Página 1 de 5 emja Australia The Medical Journal of Home Issues emja shop My account Classifieds Contact More... Topics Search From the Patient s Perspective Editorial Measuring patient-reported outcomes:
Página 1 de 5 emja Australia The Medical Journal of Home Issues emja shop My account Classifieds Contact More... Topics Search From the Patient s Perspective Editorial Measuring patient-reported outcomes:
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
NQF-Endorsed Measures for Person- and Family- Centered Care Phase 2
 NQF-Endorsed Measures for Person- and Family- Centered Care Phase 2 FINAL REPORT March 31, 2016 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I
NQF-Endorsed Measures for Person- and Family- Centered Care Phase 2 FINAL REPORT March 31, 2016 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I
Provider Orientation to Magellan s Outpatient Behavioral Health Model
 Provider Orientation to Magellan s Outpatient Behavioral Health Model July 2017 Big-picture objectives Magellan Healthcare s outpatient care management model: Reduces provider administrative tasks Expedites
Provider Orientation to Magellan s Outpatient Behavioral Health Model July 2017 Big-picture objectives Magellan Healthcare s outpatient care management model: Reduces provider administrative tasks Expedites
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY
 MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
PQRS Cheat Sheet. Physical Therapy Reporting- Individual Measures
 PQRS Cheat Sheet Physical Therapy Reporting- Individual Measures According to APTA, to participate in PQRS using individual measures, you must report on a minimum of 3 measures for 50% of all Medicare
PQRS Cheat Sheet Physical Therapy Reporting- Individual Measures According to APTA, to participate in PQRS using individual measures, you must report on a minimum of 3 measures for 50% of all Medicare
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
REPORT TO ARMED SERVICES COMMITTEES OF THE SENATE AND HOUSE OF REPRESENTATIVES
 REPORT TO ARMED SERVICES COMMITTEES OF THE SENATE AND HOUSE OF REPRESENTATIVES Section 729 of the National Defense Authorization Act for Fiscal Year 2016 (Public Law 114-92) Plan for Development of Procedures
REPORT TO ARMED SERVICES COMMITTEES OF THE SENATE AND HOUSE OF REPRESENTATIVES Section 729 of the National Defense Authorization Act for Fiscal Year 2016 (Public Law 114-92) Plan for Development of Procedures
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Population and Sampling Specifications
 Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
Providing and Documenting Medically Necessary Behavioral Health Services
 Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Medical Appropriateness and Risk Adjustment
 Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
ICD 10 Preparation for NSMM
 This document explains regulation changes coming in 2014 that will impact how we collect and document clinical appropriateness using diagnosis codes (ICD-9 conversion to ICD-10). Please familiarize yourself
This document explains regulation changes coming in 2014 that will impact how we collect and document clinical appropriateness using diagnosis codes (ICD-9 conversion to ICD-10). Please familiarize yourself
OP ED-THROUGHPUT GENERAL DATA ELEMENT LIST. All Records
 Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Coding for the Practitioner
 Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation
 Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Improving Pain Outcomes in Home Health Patients
 Improving Pain Outcomes in Home Health Patients Through Implementation of an Evidence-Based Guideline Bundle Pain is often undertreated and underreported in the elderly. Many of these individuals receive
Improving Pain Outcomes in Home Health Patients Through Implementation of an Evidence-Based Guideline Bundle Pain is often undertreated and underreported in the elderly. Many of these individuals receive
MEDICAL POLICY No R5 PSYCHOLOGICAL EVALUATION AND MANAGEMENT OF NON-MENTAL HEALTH DISORDERS
 PSYCHOLOGICAL EVALUATION AND MANAGEMENT OF NON-MENTAL HEALTH DISORDERS Effective Date: September 8, 2014 Review Dates: 10/07, 10/08, 10/09, 6/10, 6/11, 6/12, 6/13, 8/14, 8/15, 8/16, 8/17 Date Of Origin:
PSYCHOLOGICAL EVALUATION AND MANAGEMENT OF NON-MENTAL HEALTH DISORDERS Effective Date: September 8, 2014 Review Dates: 10/07, 10/08, 10/09, 6/10, 6/11, 6/12, 6/13, 8/14, 8/15, 8/16, 8/17 Date Of Origin:
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Visions of Excellence in Inpatient Settings 1/23/2013
 Success factors (review) Innovation at home (worksheet) Visions of Excellence (self assessment) Leadership Change in Role and Process Embrace Technology Collaborative Models Change the discussion Changing
Success factors (review) Innovation at home (worksheet) Visions of Excellence (self assessment) Leadership Change in Role and Process Embrace Technology Collaborative Models Change the discussion Changing
OP ED-Throughput General Data Element List. All Records All Records. All Records All Records All Records. All Records. All Records.
 Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
January 1, 20XX through December 31, 20XX. LOINC(R) is a registered trademark of the Regenstrief Institute.
 is a registered trademark of the Regenstrief Institute.") e Title Median Time from ED Arrival to ED Departure for Admitted ED Patients e Identifier ( Authoring Tool) 55 e Version number 5.1.000 NQF Number 0495 GUID 9a033274-3d9b- 11e1-8634- 00237d5bf174 ment
e Title Median Time from ED Arrival to ED Departure for Admitted ED Patients e Identifier ( Authoring Tool) 55 e Version number 5.1.000 NQF Number 0495 GUID 9a033274-3d9b- 11e1-8634- 00237d5bf174 ment
CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures
 July 15, 2013 Acumen, LLC 500 Airport Blvd., Suite 365 Burlingame, CA 94010 RE: CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures To Whom It May Concern:
July 15, 2013 Acumen, LLC 500 Airport Blvd., Suite 365 Burlingame, CA 94010 RE: CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures To Whom It May Concern:
Value-based Care Report. February How Value-based Care is improving quality and health.
 Value-based Care Report February 2018 How Value-based Care is improving quality and health. Value-based Care delivers: Value-based Care means better health, better care and lower costs. Placing greater
Value-based Care Report February 2018 How Value-based Care is improving quality and health. Value-based Care delivers: Value-based Care means better health, better care and lower costs. Placing greater
Flexible care packages for people with severe mental illness
 Submission Flexible care packages for people with severe mental illness February 2011 beyondblue: the national depression initiative PO Box 6100 HAWTHORN WEST VIC 3122 Tel: (03) 9810 6100 Fax: (03) 9810
Submission Flexible care packages for people with severe mental illness February 2011 beyondblue: the national depression initiative PO Box 6100 HAWTHORN WEST VIC 3122 Tel: (03) 9810 6100 Fax: (03) 9810
OP ED-THROUGHPUT GENERAL DATA ELEMENT LIST. All Records
 Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Inpatient Psychiatric Facility Quality Reporting (IPFQR) Program: Follow-Up After Hospitalization for Mental Illness (FUH) Measure
 Program: Follow-Up After Hospitalization for Mental Illness (FUH) Measure") Inpatient Psychiatric Facility Quality Reporting (IPFQR) Program: Follow-Up After Hospitalization for Mental Illness (FUH) Measure Sherry Yang, PharmD Director, IPF Measure Development and Maintenance
Inpatient Psychiatric Facility Quality Reporting (IPFQR) Program: Follow-Up After Hospitalization for Mental Illness (FUH) Measure Sherry Yang, PharmD Director, IPF Measure Development and Maintenance