A Tale of Two Projects: RED & BOOST
|
|
|
- Kathlyn Cunningham
- 5 years ago
- Views:
Transcription
1 A Tale of Two Projects: RED & BOOST Jeff Greenwald, MD Associate Professor of Medicine Boston University School of Medicine Director, Hospital Medicine Unit Boston Medical Center Care Transitions Seminar April 29, 2009 Westborough, MA
2 30 Day Rehospitalization Rates All discharges 19.6% Medical discharges 21.1% Surgical discharges 15.6% N Eng J Med 2009;360:
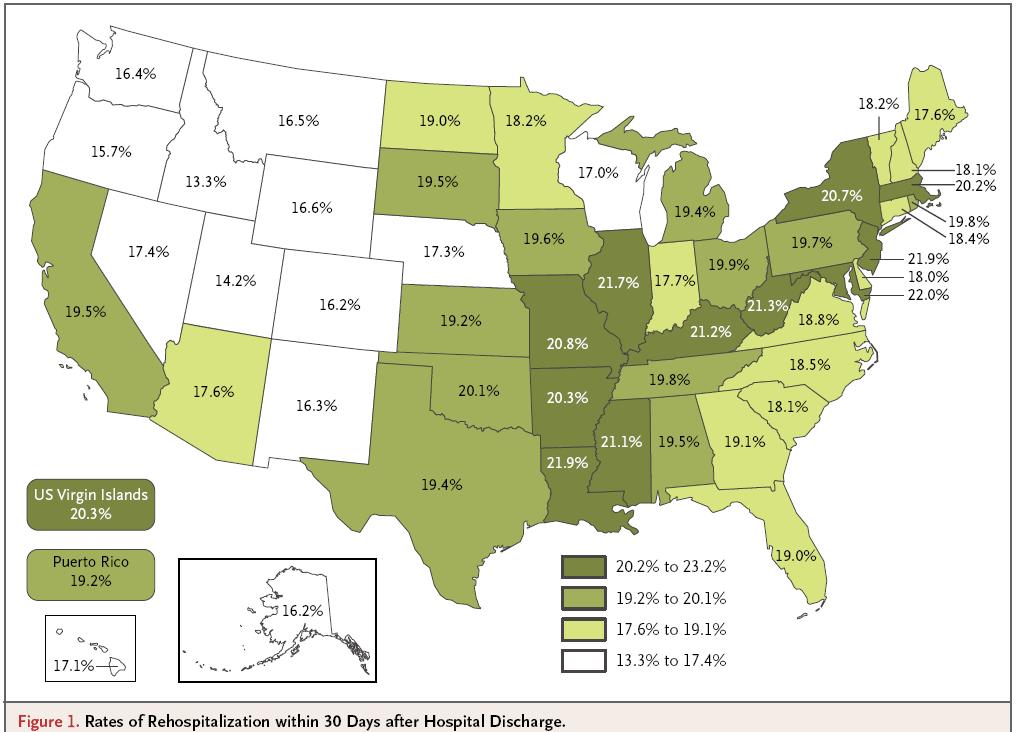
3 N Eng J Med 2009;360:
4 Is readmission a marker of poor quality care? Discharge Health Care System Lapse of communication Patient New Medical Problem Clinician Lab/Test error Deteriorization of known medical problem Discharge summary to PCP Inpatient team to PCP Not ordered Distant from discharge Not performed Early Post-discharge Community services with PCP Not seen Drug/Alcohol use Indadequate Patient Education Not acted upon Language/Cultural barrier Medication Error Inappropriate discharge Medication non-adherence Lack of timely follow-up Inappropriate medication Doesn't keep follow-up appointment Lapse in community services Inadequate use of community services Rehospitalization
5 Introducing Project RED AHRQ Funded Brian Jack, MD = Principle Investigator Boston University School of Medicine/ Boston Medical Center Principle results published in Annals of Internal Medicine, Feb 3, Slides courtesy of Brian Jack, MD
6 MethodsRandomized Controlled Trial RED Intervention N=375 Enrollment N=750 Randomization 30-day Outcome Data Telephone Call EMR Review Usual Care N=375 Enrollment Criteria: English speaking Have telephone Able to independently consent Not admitted from institutionalized setting Adult medical patients admitted to Boston Medical Center (urban academic safety-net hospital)
7 3 Components of RED Intervention In Hospital Nurse Discharge Advocate (DA) Interacts with care team: medication reconciliation and national guidelines Patient preparation for discharge Prepare After Hospital Care Plan (AHCP) After Discharge Clinical Pharmacist Call Follow-up 2-4 days Reinforce dc plan and review medications

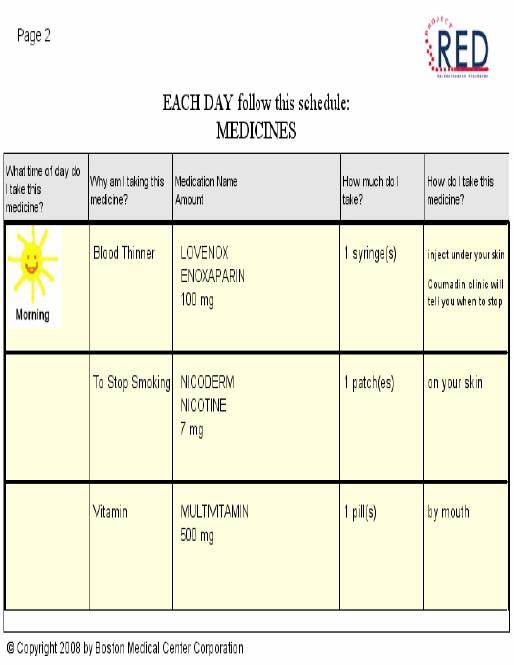
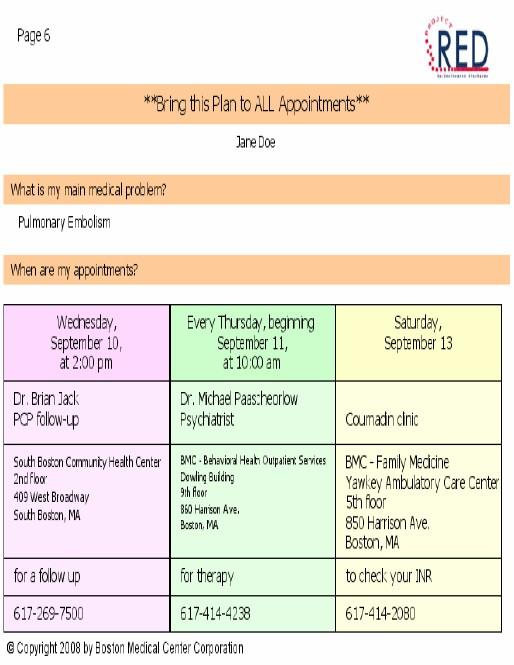
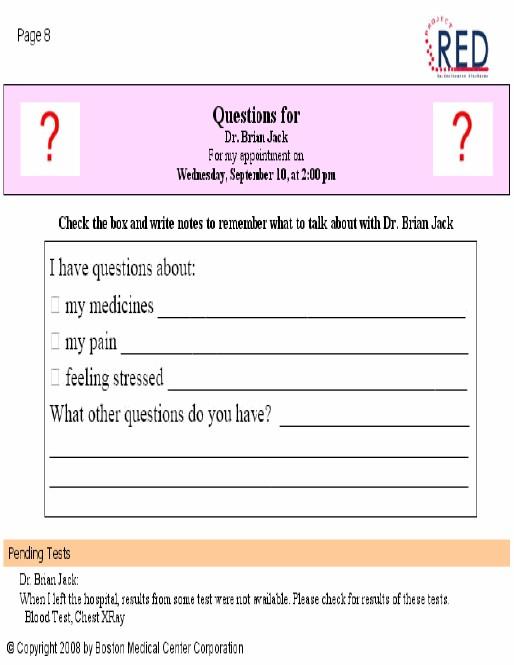
8 After Hospital Care Plan
9 Analysis Primary outcome: Total hospital utilization (readmissions plus ED visits) Intention-to-treat Poisson tests for significance Cumulative hazard curves generated for time to multiple events Secondary outcomes: PCP follow-up rate, identified dc diagnosis, identified PCP name, self-reported preparedness for discharge Proportions tests for significance
10 Primary Outcome: Hospital Utilization within 30d after discharge Usual Care (n=368) Intervention (n=370) P-value Hospital Utilizations * Total # of visits Rate (visits/patient/month) ED Visits Total # of visits Rate (visits/patient/month) Readmissions Total # of visits Rate (visits/patient/month) * Hospital utilization refers to ED + Readmissions
11 Usual care Intervention p = Cumulative Hazard Rate Cumulative Hazard Rate of Patients Experiencing Hospital Utilization 30 Days After Index Discharge Time After Index Discharge (days) 25 30
12 Self-Perceived Readiness for Discharge (30 days post-discharge) % Usual Care 40 RED Prepared Understand Appts Understand Meds Understand Dx Questions answ ered
13 50 60 Risk of hospital re-utilization by health literacy category 0 Risk of re-utilization P for trend=0.009 Grade33and and below below Grade Grade Grade Grade Grade REALM category Grade Grade 9+ 9+
14 60 Risk of hospital re-utilization by health literacy category p=0.06 p=0.59 p=0.38 p= Risk of re-utilization Usual Care Intervention Grade 3 and below Grade 4-6 Grade 7-8 REALM category Grade 9+
15 Conclusions or the RCT The Re-Engineered Discharge: Was successfully delivered using: RED protocols AHCP Improved Readiness for Discharge Improved PCP follow-up rate Decreased hospital use 30% overall reduction NNT = 7.3
16 Implications The components of the RED should be provided to all patients as recommended by the National Quality Forum, Safe Practice #11.

17 Introducing Project BOOST Funded by the John A Hartford Foundation Grant to the Society of Hospital Medicine Principle Investigator = Mark Williams, MD Implementation project
18 Project BOOST Developed a project team and national advisory board Developed a toolkit and implementation guide with web resources Rolled out via mentored implementation to 6 pilot sites across USA Now in phase 2: full roll out to 24 total sites

19
20
21
22 Principal BOOST Intervention Tool: The TARGET TARGET: Tool for Adjusting Risk: A Geriatric Evaluation for Transitions 7P Risk Scale Prior hospitalization Problem medications Punk (depression) Principal diagnosis Polypharmacy Poor health literacy Patient support Each associated with risk specific interventions
23 Universal Patient Discharge Checklist GAP assessment Medications reconciliation Medication use and side effects reviewed* Confirm understanding of prognosis, self-care, and symptoms requiring immediate medical attention* Best Practice guidelines assessment Discharge plan completed, taught, and provided to patient/caregiver Discharge communication provided to posthospitalization care provider Documented receipt of discharge information from principal care providers *Using Teach Back with patient/caregiver
24 The General Assessment of Preparedness: The GAP Caregivers and social support circle for patient Functional status evaluation completed Cognitive status assessed Abuse/neglect Substance abuse Advanced care planning addressed and documented On Admission Functional status Cognitive status Access to meds Responsible party for ensuring med adherence prepared Home preparation for patient s arrival Financial resources for care needs Transportation home Access (e.g. keys) to home Nearing Discharge Understanding of dx, treatment, prognosis, followup and postdischarge warning S/S (using Teach Back) Transportation to initial follow-up At Discharge
25

26 Teach Back Schillinger D et al. Closing the loop: physician communication... Arch Intern Med. 2003;163:83-90.


27
Roundtable on Health Literacy Institute of Medicine 17 March 2014
 Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Enhanced Assessment for Post Hospital Needs
 These presenters have nothing to disclose Enhanced Assessment for Post Hospital Needs Maureen Carroll September 28, 2015 Session Objectives Participants will be able to: Identify failures in current processes
These presenters have nothing to disclose Enhanced Assessment for Post Hospital Needs Maureen Carroll September 28, 2015 Session Objectives Participants will be able to: Identify failures in current processes
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Health Care Reform s BOOST to Reducing Readmissions
 Health Care Reform s BOOST to Reducing Readmissions Mark V. Williams, MD, FHM Professor & Chief, Division of Hospital Medicine Principal Investigator, Project BOOST Why the Focus on Care Transitions? n
Health Care Reform s BOOST to Reducing Readmissions Mark V. Williams, MD, FHM Professor & Chief, Division of Hospital Medicine Principal Investigator, Project BOOST Why the Focus on Care Transitions? n
Complex Care Management Protocols and Procedures
 Complex Care Management Protocols and Procedures December 2014 Version 3.0 1 Table of Contents I. Complex Care Management Program Staff Roles and Responsibilities... 4 II. Complex Care Management Program
Complex Care Management Protocols and Procedures December 2014 Version 3.0 1 Table of Contents I. Complex Care Management Program Staff Roles and Responsibilities... 4 II. Complex Care Management Program
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
6/10/2015. Adjusting your volume. Slides are available for download at Recording will be available in several days
 Wrestling Readmissions to the Mat: Evidence and Efforts LIVE in 5 Minutes Wrestling Readmissions to the Mat: Evidence and Efforts LIVE in 3 Minutes Adjusting your volume Select between two options: Telephone
Wrestling Readmissions to the Mat: Evidence and Efforts LIVE in 5 Minutes Wrestling Readmissions to the Mat: Evidence and Efforts LIVE in 3 Minutes Adjusting your volume Select between two options: Telephone
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007
 Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Medication Reconciliation as a Patient Safety Practice During Transitions of Care
 Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON
 Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON SCHOOL OF PHARMACY Conflicts of Interest I have no conflicts
Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON SCHOOL OF PHARMACY Conflicts of Interest I have no conflicts
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses
 The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
From Health Literacy Evidence and Tools to Patient Understanding, and Navigation: The Imperative to Take Action to Improve Health Care Outcomes
 From Health Literacy Evidence and Tools to Patient Understanding, and Navigation: The Imperative to Take Action to Improve Health Care Outcomes Cindy Brach Center for Delivery, Organization, and Markets
From Health Literacy Evidence and Tools to Patient Understanding, and Navigation: The Imperative to Take Action to Improve Health Care Outcomes Cindy Brach Center for Delivery, Organization, and Markets
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Effective Care Coordination
 Effective Care Coordination Coordinating Care for Adults with Multiple Chronic Illnesses: Searching for the Holy Grail National Health Policy Forum March 27, 2009 Randall Brown, Ph.D. Goals of Presentation
Effective Care Coordination Coordinating Care for Adults with Multiple Chronic Illnesses: Searching for the Holy Grail National Health Policy Forum March 27, 2009 Randall Brown, Ph.D. Goals of Presentation
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
Transition of Care Model for Inpatient & Observation Units
 V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
Medication Reconciliation for Older Adults Transitioning from. Long-Term Care to Home. Allison (Leverett) Kackman
 Kackman") Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Medication Trauma Crisis: Primary Care Innovations. Session Code: D25, E25
 Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Emergency Department Patient Navigation for Frequent Emergency Department Users: Findings from a Randomized Controlled Trial
 Emergency Department Patient Navigation for Frequent Emergency Department Users: Findings from a Randomized Controlled Trial Roberta Capp, MD, MHS Assistant Professor, Department of Emergency Medicine,
Emergency Department Patient Navigation for Frequent Emergency Department Users: Findings from a Randomized Controlled Trial Roberta Capp, MD, MHS Assistant Professor, Department of Emergency Medicine,
190 stroke patients were randomized to the intervention group and 190 were randomized to the control group. N=380
 Appendix 1: Summary of Evidence on Transitional Care (n=21) 1 Allen, et al., 2009 To evaluate whether comprehensive care management after discharge for stroke survivors is superior to stroke unit care
Appendix 1: Summary of Evidence on Transitional Care (n=21) 1 Allen, et al., 2009 To evaluate whether comprehensive care management after discharge for stroke survivors is superior to stroke unit care
SAFE PRACTICE 15: DISCHARGE SYSTEMS
 Safe Practices for Better Healthcare 2010 Update SAFE PRACTICE 15: DISCHARGE SYSTEMS The Objective Ensure that effective transfer of clinical information to the patient and ambulatory clinical providers
Safe Practices for Better Healthcare 2010 Update SAFE PRACTICE 15: DISCHARGE SYSTEMS The Objective Ensure that effective transfer of clinical information to the patient and ambulatory clinical providers
Improving the Discharge Process through Better Patient and Family Engagement
 Improving the Discharge Process through Better Patient and Family Engagement T A N Y A L O R D P H D, M P H D I R E C T O R, P A T I E N T A N D F A M I L Y E N G A G E M E N T A H A H R E T H E N P F
Improving the Discharge Process through Better Patient and Family Engagement T A N Y A L O R D P H D, M P H D I R E C T O R, P A T I E N T A N D F A M I L Y E N G A G E M E N T A H A H R E T H E N P F
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Reducing Readmissions: Care Transitions Toolkit
 Reducing Readmissions: Care Transitions Toolkit 2 nd Edition: February 26, 2014 Right Care at the Right Time in the Right Setting 1 P a g e Washington State Hospital Association - Partnership for Patients
Reducing Readmissions: Care Transitions Toolkit 2 nd Edition: February 26, 2014 Right Care at the Right Time in the Right Setting 1 P a g e Washington State Hospital Association - Partnership for Patients
Project RED (ReEngineering Discharge)
") Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Improving family experiences in ICU. Pamela Scott Senior Charge Nurse Forth Valley Royal Hospital ICU
 Improving family experiences in ICU Pamela Scott Senior Charge Nurse Forth Valley Royal Hospital ICU Family Burden in icu:- Incidence of anxiety symptoms range from 21% to 60.4% (median 40%) from ICU admission
Improving family experiences in ICU Pamela Scott Senior Charge Nurse Forth Valley Royal Hospital ICU Family Burden in icu:- Incidence of anxiety symptoms range from 21% to 60.4% (median 40%) from ICU admission
Communication with Surrogate Decision Makers. Shannon S. Carson, MD Associate Professor University of North Carolina
 Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6,
 Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
 Eastern Kentucky University Encompass Doctor of Nursing Practice Capstone Projects Baccalaureate and Graduate Nursing 2016 Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
Eastern Kentucky University Encompass Doctor of Nursing Practice Capstone Projects Baccalaureate and Graduate Nursing 2016 Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Patient and Family Engagement to Prevent Diagnostic Error
 Patient and Family Engagement to Prevent Diagnostic Error Martine Ehrenclou, MA Award-Winning Author, Healthcare Advocate Tejal Gandhi, MD MPH CPPS President National Patient Safety Foundation Kathryn
Patient and Family Engagement to Prevent Diagnostic Error Martine Ehrenclou, MA Award-Winning Author, Healthcare Advocate Tejal Gandhi, MD MPH CPPS President National Patient Safety Foundation Kathryn
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care
 Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Question Patient #1 Patient #2 Patient #3 Patient #4 Patient #5 Number of days between the last discharge and this readmission date?
 Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Promoting a Safe Transition from Hospital to Home Using the Teach-Back Process
 Promoting a Safe Transition from Hospital to Home Using the Teach-Back Process Cori Gibson, MSN, RN, CNL Cheryl Kornburger, BSN, RN Sandy Sadowski, RN Learning Objectives Describe how the teach-back process
Promoting a Safe Transition from Hospital to Home Using the Teach-Back Process Cori Gibson, MSN, RN, CNL Cheryl Kornburger, BSN, RN Sandy Sadowski, RN Learning Objectives Describe how the teach-back process