Major Incident Plan RHC. Women And Children s Directorate Risk Management Group LEAD CLINICIAN DIVISIONAL RESPONSIBILITY
|
|
|
- Miranda Gardner
- 5 years ago
- Views:
Transcription
1 RHC Major Incident Plan DIVISIONAL RESPONSIBILITY Women And Children s Directorate Risk Management Group LEAD CLINICIAN Dr Siobhan Sweeney IMPLEMENTATION DATE Nov 2016 NEXT REVIEW DATE annual ISSUE NUMBER 4 NUMBER OF PAGES 188
2 If and when a Major Incident is declared: Initial actions in the Emergency Department 1. Don t panic. Breathe! 2. Pull your senior team together and make a plan 3. Start a log of key decisions and actions 4. If you have a role in the emergency plan follow your action card 5. Clear the Emergency department 6. Plan breaks for your staff and standby other staff to take over 7. Identify a member of staff to call in the additional staff required-telephone numbers in ED secretaries office in MI folder 8. Establish triage at the ambulance doors 9. Ensure set up of Clinic 3 out-patients 10. Place staff / signage at front entrance of ED to divert patients to Clinic The relative waiting area is in the Therapies Hub, divert relatives here if necessary 12. If you have not read the plan do not do so now, follow your action card. 2
3 CONTENTS PAGE NUMBER 1. INTRODUCTION 5 2. DEFINITION 5 3. MAJOR INCIDENT ALERT PROCEDURE 6 4. STAFF NOTIFICATION PROCEDURE 8 5. HOSPITAL COORDINATION TEAM KEY ROLES ON SITE MEDICAL TEAM OUTLINE PROCESS TELEPHONE NUMBERS MAJOR INCIDENT DEBRIEFING REVIEW ACTION CARDS APPENDICES 118 3
4 APPENDICES PAGE NUMBER APPENDIX 1 MAJOR INCIDENT NOTIFICATION FORM 118 APPENDIX 2 SIGNPOSTING 119 APPENDIX 3 LOCATION OF TELEPHONE CONTACT LISTS 121 APPENDIX 4 LIST OF DESIGNATED AREAS AND TELEPHONE 122 NUMBERS APPENDIX 5 LIST OF EXTERNAL AGENCIES AND TELEPHONE 125 NUMBERS APPENDIX 6 MAJOR INCIDENT PATIENT REGISTRATION 126 APPENDIX 7 STRATHCLYDE POLICE CASUALTY BUREAU 130 ARRANGEMENTS APPENDIX 8 CHEMICAL AND RADIOLOGICAL INCIDENTS 131 APPENDIX 9 EMERGENCY VIP PATIENT POLICY 132 APPENDIX 10 POLICE FORMS USED TO HELP IDENTIFY 135 CASUALTIES 4
5 MAJOR INCIDENT PLAN 1. INTRODUCTION 1.1 The purpose of the Major Incident Plan is to ensure that the hospital is in a position to respond to incidents outside of its normal experience and of such a scale that special arrangements will be required. 1.2 There is an overarching Major Incident Plan for NHS Greater Glasgow and Clyde (NHSGGC) which sets out the overall health board response, the designation of receiving hospitals for specific major incidents and coordination with other Emergency Services. 1.3 The Royal Hospital for Children s (RHC) Major Incident Plan will be activated if it is known or anticipated that a significant number of paediatric casualties have resulted from a particular incident. 1.4 The Major Incident Plan follows an all hazards approach with a single plan intended to cope with all types of major incident. 1.5 The details of the Major Incident Plan should be known to all staff likely to be involved in the response to a major incident. The plan has been drawn up to make clear the procedures to be followed and actions to be taken by designated members of staff under these circumstances. 1.6 The Director of Women and Children s Services bears overall corporate responsibility for major incident planning for this hospital. 1.7 Regular review, updating and testing of the Major Incident Plan will be overseen through the Women and Children s Directorate Risk Management Group. 2. DEFINITION 2.1 A major incident is any event whose impact cannot be handled within routine service arrangements. With regard to health service planning, this would involve an event that owing to the number, severity, type or location of live casualties required an extraordinary response by the hospital. 5
6 3. MAJOR INCIDENT ALERT PROCEDURE 3.1 Major Incident Standby Notification The first notification of a potential major incident is likely to come from the Scottish Ambulance Service. When the ambulance service first suspects that a major incident might have occurred, the Scottish Ambulance Service Control Centre will identify all the hospitals potentially involved and alert them directly. This alert is the Major Incident- Standby. The ambulance service will then alert the GGC Contact centre who will activate the Confirmer call out system for all staff who will be involved in the response within the designated hospitals. Blue Light Services Ambulance Control Centre Contact GGC EDs GG&C Contact Centre Hospital staff 3.2 The first notification of a potential major incident may be received directly by the Emergency Department. In this case, the Nurse in Charge Emergency Department will contact the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770) to inform them of the information received. 6
7 3.3 It is the responsibility of the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770) to confirm the authenticity of any information received with the Scottish Ambulance Service or Police Scotland, contact details to be found in Appendix 5. The Major Incident Notification Form (Appendix 1) should be used to record the essential details. 3.4 If casualties begin arriving in the Emergency Department reporting that there has been a major incident, but prior to any official major incident alert, the Nurse in Charge Emergency Department will contact the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770) to inform them of the situation. They should assess whether the hospital Major Incident Plan should be activated in this case. 3.5 Following notification of a confirmed major incident from the Emergency Services, it is the responsibility of the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770) to confirm to GGC Contact Centre via 2222 call that a major incident has been declared and that the hospital Major Incident Plan is to be activated. 3.6 Major Incident Declared Notification If the Emergency services judge that the situation is deemed significant, they will revise the standby message to Major Incident Declared. This message will be sent to all the hospitals directly and then to the Contact Centre for further dissemination. The information relayed to the Contact Centre will be a METHANE message which will be passed on to the Emergency department. (See Action card Incident Log Sheet.) M- Major Incident declared/ standby E- Exact location T- Type of incident H- Hazards A- Access/Egress N- Number of casualties E- Emergency Services present/required The message that is received by pager, phone, text or will be a series of questions and options to select. The call lasts approximately 2 minutes. Confirmer will only cease attempting the other contact methods as long as ALL prompts during the call have been responded to positively. 3.7 Major Incident Stand down Procedure If the Emergency services decide that the situation is no longer significant, they will revise the message to Major Incident - Stand down and contact the emergency department red phone. This information should be communicated with the Hospital Coordinator who has the responsibility of verifying the information. 3.8 Major Incident Stand down at the end of a major incident The Hospital Coordinator will decide on the phasing of the stand down of the hospital major incident response and will communicate with staff accordingly. If GGC Contact Centre Operator receives a stand down call from the Scottish Ambulance Service Emergency Medical Dispatch Centre, or other External Agency, this information 7
8 must be communicated to the Hospital Coordinator in the first instance, as it is the Incident Controller who has responsibility for declaring any stand down of the hospital major incident response. 4. STAFF NOTIFICATION PROCEDURE 4.1 Major Incident Call-In Procedure The following entities will be called by the Confirmer system to notify them of the Major Incident status. The following entities will be contacted based on the contact information provided on Rota watch. Any additional staff will need to be contacted by each departments own major incident call-in list. RWRole Managers On Call North East Stobhill and Glasgow Royal Infirmary Senior Manager On Call RWRole Medical Consultant Rota Inverclyde Royal Hospital Consultant RWRole Medical Consultant Royal Alexandra or Vale Of Leven Consultant RWRole Medical Paediatric Consultant On Call Royal Hospital for Children Consultant RWRole Medical Receiving Consultants and Senior Staff Glasgow Royal Infirmary Consultant RWRole Orthopaedic On Call Glasgow Royal Consultant RWRole Orthopaedic On Call Queen Elizabeth University Hospital Consultant RWRole Orthopaedic On Call Royal Alexandra Consultant RWRole Orthopaedic On Call Royal Hospital for Children Consultant RWRole Press Officer Communications Press Officer On Call RWRole23 38 Public Health Medicine and Port Health Consultant or Specialist Registrar RWRole Public Health Medicine and Port Health Office Staff RWRole Surgical Consultant Glasgow Royal and Surgical Receiving Coordinator Duty Consultant Surgeon 8
9 RWRole Surgical Inverclyde Royal Consultant RWRole Surgical Receiving and Neonates Consultants and Registrar Royal Hospital for Children Consultant RWRole Surgical Receiving Consultant or Registrar Queen Elizabeth University Hospital Consultant RWRole Surgical Royal Alexandra Hospital Consultant RWRole Telecoms Manager On Call Telecoms Manager RWRole Test 1 Director Head RWRole A E Consultants On Call Glasgow Royal Infirmary Consultant RWRole A E Consultant on Call Queen Elizabeth University Hospital Consultant RWRole A E Consultant Royal Alexandra or Inverclyde Royal Consultant RWRole A E Consultants On Call Royal Hospital for Children Consultant RWRole37 64 Acute Executive Director On Call Acute Executive Director RWRole Acute Receiving Unit Queen Elizabeth University Hospital Clusters Consultant RWRole Anaesthetic senior trainee Queen Elizabeth University Hospital Senior trainee RWRole49 78 Anaesthetics Glasgow Royal Infirmary Consultant RWRole Anaesthetics Cardiac Consultant On Call Royal Hospital for Children Cardiac Consultant RWRole Anaesthetics Consultant On Call Royal Hospital for Children Consultant RWRole Anaesthetics General Consultant On Call Royal Hospital for Children General Consultant RWRole Anaesthetics Inverclyde Royal Consultant 9
10 RWRole Anaesthetics Queen Elizabeth University Hospital Consultant RWRole Anaesthetics Royal Alexandra Consultant RWRole Blood Transfusion Queen Elizabeth University Hospital Bio Medical Scientist RWRole Corporate Management Team City Wide Corporate Director RWRole Corporate Management Team City Wide Response Medical Director RWRole Department of Medicine for the Elderly Glasgow Royal Infirmary Stobhill and Lightburn Consultant RWRole Facilities Senior Manager On Call Senior Manager RWRole Major Incident I T 1 General I T RWRole Major Incident I T 2 General I T RWRole Major Incident I T 3 General I T RWRole Major Incident I T 4 General I T RWRole Manager On Call Queen Elizabeth University Hospital Manager on call RWRole Managers Clyde Royal Alexandra or Inverclyde Royal or Vale of Leven Duty Manager 4.2 Confirmer Test Calls Major Incident Test calls are held every month to ensure that the communication system works. The Emergency Red phone in the ED will also be included in the test calls but is not part of the confirmer system. 4.3 Secondary ED call out An updated list of contact numbers for individuals the ED department will contact following declaration of a major incident is kept in the ED secretaries office in the ED department. An appropriate member of staff will be allocated the call out role following declaration of an MI. 10
11 5. HOSPITAL COORDINATION TEAM 5.1 The hospital major incident response will be controlled by the Hospital Coordination Team. Hospital Co-ordinator Emergency Department Consultant Senior Nurse (8502) Site Facilities Manager 5.2 The Hospital Coordinator is in overall charge. This role Monday to Friday 9-5 will be filled the manager in RHSC holding page number Out of hours this role will be filled by the NHSGGC West Sector General Manager on call. In the unlikely event they are un-available the NHSGGC Executive Director on call will be contacted. The Senior Nurse on duty for the hospital (Page 8502/ DECT 85770) will, if necessary, assume this role until their arrival. 5.3 The Emergency Department Consultant has responsibility for organising the reception phase of the major incident. This role will be filled by the Emergency Department Consultant on call. The senior Emergency Department Specialty Trainee will, if necessary, assume this role until their arrival. 5.4 The Senior Nurse has responsibility for coordinating the nursing response within the hospital. This role will be filled by the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770). 5.5 The Site Facilities Manager has responsibility for coordinating the hospital support and non-clinical services response. 5.6 The Hospital Coordination Team will be based in the Seminar room in the Emergency Department. In a mixed adult and paediatric incident there will be a central control room in QEUH based in the meeting room on level 2 at the main atrium. Clear lines of communication must be established between RHC and QEUH, and the managers will have a role to play in both the adult and the paediatric response. 11
12 6. KEY ROLES 6.1 The duties and responsibilities of specific staff during a major incident are set out on individual action cards. 6.2 Members of staff fulfilling certain key roles may change according to the nature of the major incident - surgical/trauma versus medical type incidents. 6.3 All staff that are likely to play a key role in the hospital major incident response will have an action card. 6.4 Each action card tells an individual what their role will be and how they should achieve it. 6.5 Once informed that the hospital Major Incident Plan has been activated, staff should proceed to the staff reporting area in the HAN base and adjacent seminar room on the second floor to collect their action cards. 7. ON SITE MEDICAL TEAM 7.1 There is currently no role for RHC in the provision of on-site support at the scene of a major incident in the form of a Medical Incident Officer or Site Medical Team. 7.2 The Medical Incident Officer and Site Medical Team will be provided by EMRS. 7.3 If additional specialist paediatric skills are required on-site, these will be requested by the on-site Medical Incident Officer. RHC will respond as appropriate, through the pre-existing structure of the PICU Transport Service and this will include the capability to provide a Site Surgical Team. 12
13 8. OUTLINE PROCESS 8.1 Following activation of the hospital Major Incident Plan, the Senior Nurse on duty for the hospital will establish the Major Incident Control Room in the Seminar room in the Emergency Department. 8.2 Other members of the Hospital Coordination Team will proceed to the Major Incident Control Room in the Seminar room in the Emergency Department. 8.3 All members of staff who are designated in the hospital Major Incident Plan should proceed to the staff reporting area in the HAN base and adjacent seminar room on the second floor to collect their action card. 8.4 Staff members attending the hospital who do not have a designated action card, but may have a role to play in a major incident should attend the HAN base and adjacent seminar room on the second floor to give their name and designation to the senior nurse co-ordinating the staff reporting area, and remain in the seminar room to be called upon when required. 8.5 If extra staff are required during a major incident, in addition those specified on the action cards, they will be contacted. 9. TELEPHONE NUMBERS 9.1 It is essential that GGC Contact Centre is provided with up to date telephone contact details. This is achieved by ensuring that Rotawatch is accurately populated. Individual departments must maintain accurate and regularly updated telephone contact details for members of staff, so all necessary personnel can be contacted in the event of a major incident. 9.2 Telephone contact details for certain designated staff are held at the Contact Centre. More specific departmental telephone contact lists are held in various locations around the hospital as set out in Appendix Telephone numbers for key areas within the hospital that will play a designated role in a major incident are set out in Appendix Telephone numbers for relevant External Agencies are set out in Appendix MAJOR INCIDENT DEBRIEFING 10.1 Staff debriefing is essential following a major incident. Operational and psychological issues should be addressed The Hospital Coordinator will be responsible for ensuring a debriefing meeting is convened during the week following a major incident. 13
14 10.3 The Hospital Coordination Team will have responsibility for identifying those members of staff significantly involved in the major incident response and who should therefore attend. In addition to medical and nursing staff, hospital support services, medical records and the Contact Centre should also be represented The Hospital Coordinator will prepare a formal report based on the debriefing, which will be presented to the Director of Women and Children s Services and copied to the Civil Contingencies Planning Unit at NHSGGC All other staff involved should have the opportunity for a major incident debriefing, organised through their head of department There should be a formal and impartial audit carried out of the clinical care delivered to patients during the major incident and of the wider hospital response. This should be completed within a month of the incident. This will help identify any significant failures or successes and facilitate dissemination of lessons learned to a wider audience. 11. REVIEW 11.1 The Major Incident Plan will be subject to regular review and revised/updated as necessary through the Women and Children s Directorate Risk Management Group. 14
15 MAJOR INCIDENT ACTION CARDS ACTION CARD NUMBER ACTION CARD TITLE 1 HOSPITAL COORDINATOR 2 SENIOR NURSE ON DUTY PAGE , 3A-B EMERGENCY DEPARTMENT CONSULTANTS 4 NURSE IN CHARGE EMERGENCY DEPARTMENT 5 SITE FACILITIES MANAGER 6, 6A-E SENIOR EMERGENCY MEDICINE SPECIALTY TRAINEES 7,7A-E 8,8A-H 9,9A-E 10,10A-C EMERGENCY MEDICINE PAEDAITRIC AND GP STS EMERGENCY DEPARTMENT NURSES EMERGENCY DEPARTMENT HEALTH CARE ASSISTANTS ANAESTHETISTS, TRAINEE AND CONSULTANTS 11, 11A PICU, TRAINEE AND CONSULTANTS 12 NURSE IN CHARGE PICU 13, 13A-D CONSULTANT SURGEON ON CALL, SURGICAL TRAINEES 14, 14A ORTHOPAEDIC CONSULTANT ON CALL, ORTHO TRAINEE 15, 15 A-C CONSULTANT PAEDIATRICIAN, PAEDIATRIC TRAINEES 16 SENIOR NURSE 2A, holding page A SENIOR NURSE 1E, holding page
16 MAJOR INCIDENT ACTION CARDS ACTION CARD NUMBER ACTION CARD TITLE 17 SENIOR NURSE THEATRES 18 EMERGENCY DEPARTMENT RECEPTIONIST ON DUTY 18A 18B-D MEDICAL RECORDS MANAGER MEDICAL RECORDS STAFF 19 GENERAL SERVICES SUPERVISOR 20 POLICE LIAISON OFFICER 21 HOSPITAL ENQUIRIES OFFICER 21A HOSPITAL ENQUIRIES OFFICER ASSISTANT 22, 22A RELATIVE COORDINATORS 23, 23A PRESS OFFICER 24 HAEMATOLOGY AND BLOOD TRANSFUSION 25 BIOCHEMISTRY 26, 26A RADIOGRAPHER ON CALL, SENIOR RADIOGRAPHER 27 CONSULTANT RADIOLOGIST ON CALL 28 PHARMACIST ON CALL 28A PHARMACY MANAGER 29 DUTY SOCIAL WORKER 30,30A-C HOSPITAL CHAPLAINS 31 MORTUARY TECHNICIAN 32, 32 A-C PORTERS Decontamination Action cards RCH and QEUH 1-10 DECONTAMINATION ACTION CARDS Only use in the event of a decontamination incident. When a major incident is declared involving a decontamination incident these cards will be allocated to ED nursing and medical staff IN ADDITION to their Major Incident Action cards above 16
17 MAJOR INCIDENT ACTION CARD 1 Hospital Co-ordinator The Hospital Co-ordinator is in overall charge of the RHC hospital response to the major incident. Between 9-5, Monday to Friday the RHC manager holding page 8084 should be contacted. Out of hours this role will be taken by the NHSGGC South Sector General Manager on call. In the unlikely event they are un-available the NHSGGC Executive Director on call will be contacted. The Senior Nurse on duty (8502/ DECT 85770) for the hospital will act as Hospital Coordinator until he/she arrives on site. The Contact Centre Operator must be kept up to date on who is Hospital Coordinator. 1. Proceed to the Major Incident Control Room, which is located in the Seminar room in the Emergency Department. Access the Incident Information Sheet (appendix 1) and contact the Scottish Ambulance Service Emergency Medical Dispatch Centre to obtain and clarify information as to the nature, site and severity of the major incident. Telephone numbers to be found on appendix Confirm/allocate the following roles as soon as possible. There may be a significant delay out of hours: a) Police Liaison Officer (working hrs- Site Manager) b) Press Officer (contact no. appendix 5) c) Press Officer Assistant (working hrs- Play Staff member) d) Relative Coordinators x 2 (working hrs - Family Information and Play Staff) e) Hospital Enquiries Officer and Assistant (Main entrance receptionist and day surgery receptionist within hrs) f) Loggist / minute taker (working hours to be allocated by admin manager) 3. You have no role to play in direct clinical patient care. 4. Take an overall view of the hospital response to the major incident and liaise with the other members of the Hospital Coordination Team, namely: (a) (b) (c) The Emergency Department Consultant, who is in charge of the initial clinical response. The Senior Nurse (8502/ DECT 85770), who is responsible for the preparation of clinical areas and nursing provision. The Site Facilities Manager, who is responsible for ensuring the provision of support services. CONTINUED ON REVERSE 17
18 5. Liaise with 8502/ DECT page holder and page holding nurses from 1E and 2A to form an overarching view of activity in the hospital. Determine the number of vacant beds, intensive care beds and free ventilators. Update the Hospital Coordinator regularly. 6. Task medical staff with the discharge of any appropriate patients to maximise available bed spaces, with regular updates to the Hospital Coordinator as beds become available. 7. Terminate theatre and outpatients clinics as appropriate. Liaise with the surgeon and cardiac anaesthetist co-ordinating theatres 8. Authorise additional medical resources as required 9. Oversee dealings with relatives and the media. This will include working with the Press Officer to coordinate any VIP visits to the hospital. 10. Decide on the phasing of the stand down of the hospital major incident response and communicate with the Contact Centre Operator and staff accordingly. 11. Convene a debriefing meeting during the week following a major incident, liaising as necessary with the Women and Children s Directorate Management Team. With the help of the other members of the Hospital Coordination Team, identify those staff who were significantly involved and who should therefore be invited attend. In addition to medical and nursing staff, hospital support services, medical records and the Contact Centre should be represented. 12. Ensure the preparation of a report based on the debriefing meeting which should include: (a) A chronology of the major incident. (b) A summary of the hospital response to the incident. (c) Detail of any significant successes or failures in the hospital response. (d) An action plan outlining a timescale for further review and any necessary revision of the hospital Major Incident Plan. 13. The report should be presented to the Director of Women and Children s Services and copied to the Civil Contingencies Planning Unit at NHSGGC. 14. Ensure that all other staff involved in the hospital major incident response have the opportunity for a debriefing, organised through their head of department. 15. Coordinate a formal and impartial audit of the clinical care delivered to patients during the major incident and of the wider hospital response. This should be completed within a month of the incident. 16. Events, decisions and actions should be recorded on a Dictaphone in the absence of a Loggist. 18
19 MAJOR INCIDENT ACTION CARD 2 SENIOR NURSE ON DUTY PAGE 8502/ Dect Role Coordinate nursing part of the hospital major incident response It is the responsibility of the Senior Nurse on duty for the hospital (page 8502) to confirm to the Contact Centre via 2222 call that a major incident has been declared and that the hospital Major Incident Plan is to be activated. The Senior Nurse on duty for the hospital (page 8502/ Dect 85770) will assume the role of Hospital Coordinator until he / she arrives on site - follow Major Incident Action Card. 1. Help establish the Major Incident Control Room in the Seminar Room in the Emergency Department. 2. Ensure preparation and adequate nurse staffing of key clinical areas is in hand: (a) (b) (c) Emergency Department Clinic 3 Out-Patients Department PICU/Theatres 3. Liaise with the page holding Senior Nurses on Ward 1E (page 8345) and 2A (page 8399). With their assistance, alert all wards. In the process, establish bed status and the number of trained nurses and other ward staff who could be made available to assist elsewhere with the major incident response without jeopardising ward patient care. 4. If assuming the Senior Nurse role in the Hospital Coordination Team continue to follow Major Incident Action Card 3, if assuming a temporary Hospital Coordinator role follow Major Incident Action Card 2 and assign the senior nurse role in the hospital coordination team to a senior member of the nursing staff on shift. 6. Request the nursing staff on all wards, in conjunction with medical staff, to identify any patients who could be discharged to maximise available bed spaces. Collate this information as it becomes available and share with the Hospital Coordinator. 7. Nominate two runners to assist the Hospital Coordination Team. 8. Deploy additional available ward nurses and other staff as appropriate/necessary to the Emergency Department, Clinic 3 Out Patients Department, the Relatives Waiting Area (Therapies Hub) and the Patient Reunion/Discharge Area (Outpatient Clinic 5). CONTINUED ON REVERSE 19
20 9. Arrange contact of additional off duty nursing staff as required. Do not go through the Contact Centre operators - call directly using departmental/ward telephone call out lists. 10. After stand down of the hospital major incident response, ensure that all nursing staff involved participate in the debriefing process. 20
21 MAJOR INCIDENT ACTION CARD 3 EMERGENCY DEPARTMENT CONSULTANT 1 Roles 1. Coordinate clinical response in reception areas 2. Triage Doctor In the absence of the Emergency Department Consultant, the Senior Emergency Medicine Specialty Trainee will assume this role until the arrival on site of the Emergency Department Consultant on call. 1. Ensure that the Major Incident Control Room has been established in the Seminar Room, in the Emergency Department. In a mixed adult and paediatric MI the overarching control room is in QEUH. Ensure clear lines of communication have been established with this area. 2. Coordinate the process of clearing the Emergency Department of existing patients as follows: (a) (b) (c) Transfer those patients waiting for admission, or requiring a period of observation, to the wards. Transfer those patients who have been triaged as triage category 3 or above, or who are still to be triaged, to Clinic 3 Out-Patients Department. Send those patients waiting, who have been triaged as non-urgent, home with advice to contact their GP/NHS Work with the Nurse in Charge Emergency Department to ensure the preparation and equipping of all clinical areas for the reception of casualties. 4. Designate an appropriate number of Casualty Treatment Teams, each consisting of two doctors and one nurse. Allocate each Casualty Treatment Team to a specific treatment area. 5. Use the Senior Emergency Medicine Specialty Trainee to call in extra Emergency Department medical staff as deemed necessary. Do not go through Contact Centre operators - call directly using your departmental telephone contact list, located in the Major incident contact folder in the ED secretaries office. 6. Working together with the Triage Nurse, prepare to triage casualties as they arrive at the ambulance entrance. The availability/presence of a second Emergency Department Consultant would allow delegation of the Triage Doctor role - Major Incident Action Card 4A. 7. Coordinate and maintain an overview of all activity in the reception areas in conjunction with the Nurse in Charge Emergency Department. Liaise with radiology, theatres and PICU on a frequent basis. CONTINUED ON REVERSE 21
22 8. There should be regular contact with the Hospital Coordinator to allow accurate and timely clinical progress reports for relatives in the Relatives Waiting Area. Make use of the allocated runners to aid this communication process. 9. Once stand down of the hospital major incident response has been declared, ensure the offer of an immediate debrief for all Emergency Department staff before they leave the hospital. 22
23 MAJOR INCIDENT ACTION CARD 3A EMERGENCY DEPARTMENT CONSULTANT 2 Role Triage Doctor 1. Working together with the Triage Nurse, prepare to triage casualties as they arrive at the ambulance entrance. 2. Assess each patient on arrival and triage major incident casualties as follows: CATEGORY IMMEDIATE Casualties requiring immediate life saving treatment. CATEGORY URGENT Casualties requiring urgent surgical or other treatment intervention. CATEGORY DELAYED Casualties requiring non-urgent treatment. CATEGORY DEAD Casualties who are dead. CATEGORY EXPECTANT Consider making use of this category for those casualties who cannot survive treatment, or where the degree of intervention required is such that, in the context of a major incident, their treatment would severely compromise the provision of treatment for others. 3. Remain at the ambulance entrance and do not treat patients. 23
24 MAJOR INCIDENT ACTION CARD 3B EMERGENCY DEPARTMENT CONSULTANT 3 Role Assist coordinating clinical response in reception areas 1. Assist the Emergency Department Consultant on call in the coordination of all activity in the reception areas and in liaison with the Hospital Coordinator and other parts of the hospital. 24
25 MAJOR INCIDENT ACTION CARD 4 NURSE IN CHARGE EMERGENCY DEPARTMENT Role Coordinate nursing response in the Emergency Department The first notification of a major incident may be received directly by the Emergency Department. In this case, the Nurse in Charge Emergency Department will contact the Senior Nurse on duty for the hospital (Page 8502/ Dect 85770) to inform them of the information received. If casualties begin arriving in the Emergency Department reporting that there has been a major incident, but prior to any official major incident alert, the Nurse in Charge Emergency Department will contact the Senior Nurse on duty for the hospital (Page 8502) to inform them of the situation. They should assess whether the hospital Major Incident Plan should be activated in this case. 1. Set up the Major Incident Patient Board on the wall of the resus corridor between the ambulance doors and Majors in the Emergency Department. 2. Alert the Out-Patients Department. Out of hours, ensure you allocate the task of opening up the Out-Patients Department. 3. Work with the Emergency Department Consultant to coordinate the process of clearing the Emergency Department of existing patients as follows: (a) (b) (c) Transfer those patients waiting for admission, or requiring a period of observation, to the wards. Transfer those patients who have been triaged as triage category 3 or above, or who are still to be triaged, to Clinic 3 Out-Patients Department. Send those patients waiting, who have been triaged as non-urgent, home with advice to contact their GP/NHS Allocate appropriate/sufficient nursing staff to accompany those patients transferred round to Clinic 3 Out-Patients Department. 5. Work with the Emergency Department Consultant to ensure the preparation and equipping of all clinical areas for the reception of casualties. 6. Allocate a Triage Nurse, who will work with the Emergency Department Consultant to triage casualties as they arrive at the ambulance entrance. 7. Assist the Emergency Department Consultant to designate an appropriate number of Casualty Treatment Teams, each consisting of two doctors and one nurse. Allocate each Casualty Treatment Team to a specific treatment area. CONTINUED ON REVERSE 25
26 8. Organise the call in of extra Emergency Department nursing staff as deemed necessary. Do not go through the Contact Centre operator - call directly using your departmental telephone contact list located in the Major incident contact folder in the ED secretaries office. 9. Coordinate and maintain an overview of all activity in the reception area in conjunction with the Emergency Department Consultant. 10. Ensure re-supply of clinical areas as necessary. 11. Once stand down of the hospital major incident response has been declared, ensure the offer of an immediate debrief for all Emergency Department staff before they leave the hospital. 12. In a Major Incident involving hazardous materials requiring activation of the decontamination plan, the Nurse in Charge will allocate the role of Decontamination Supervisor, This person will the distribute the relevant action cards to the decontamination team. See Decontamination Action Cards Laminated decontamination action cards can be found in the Decontamination Unit storage area. 26
27 MAJOR INCIDENT ACTION CARD 5 SITE FACILITIES MANAGER Role Coordinate the support services part of the hospital major incident response 1. Proceed to the Major Incident Control Room in the Seminar Room in the Emergency Department. 2. Call on the following to assist in the non-clinical part of the hospital major incident response:- Deputy Site Manager Desk 69622, Dect mob Decontamination service (CSSD) / Assistant CSSD manager for escalation weekdays Assistant CSSD manager for escalation weekends Catering Lead- Desk 59619, Dect 82231, mob Facilities Duty Manager Do not go through the contact centre operator - call directly using the appropriate departmental telephone contact lists. 3. Ensure that the hospital site is locked down as directed and secure, to avoid any access to ALL clinical areas by non hospital staff. 4. Coordinate the involvement of, and liaise regularly with, all the hospital support services. 5. Ensure demands for clinical sterile and non-sterile supplies are met and organise Linen, Domestic and Catering services as necessary. 6. Liaise with Police Scotland and Parking Services to establish traffic flows and adequate access to parking for staff and parents/relatives. As per Action Card Assist the Hospital Coordinator as required. 27
28 MAJOR INCIDENT ACTION CARD 6 SENIOR EMERGENCY MEDICINE SPECIALTY TRAINEE Roles 1. Assist the Emergency Department Consultant on call 2. Casualty treatment In the absence of an Emergency Department Consultant, the Senior Emergency Medicine Specialty Trainee will assume their role until the arrival on site of the Emergency Department Consultant on call follow Major Incident Action Card Call in extra Emergency Department medical staff, as directed by the Emergency Department Consultant on call. The Contact Centre operator- call directly using your departmental telephone contact list. 2. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 3. Take the lead role in Casualty Treatment Team 1 allocated to the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 5. Summarise patient condition, treatment and management plan on Emergency Department card. 6. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 7. Prepare for the next patient. 28
29 MAJOR INCIDENT ACTION CARD 6A EMERGENCY MEDICINE SPECIALTY TRAINEE 2 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Take the lead role in Casualty Treatment Team 2 allocated to the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. Summarise patient condition, treatment and management plan on Emergency Department card. 5. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 6. Prepare for the next patient. 29
30 MAJOR INCIDENT ACTION CARD 6B EMERGENCY MEDICINE SPECIALTY TRAINEE 3 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Take the lead role in Casualty Treatment Team 5 allocated to Majors area, bays 1-4, where urgent category patients are being assessed. 3. Check that your treatment area is fully prepared and ready to receive a patient. 4. Summarise patient condition, treatment and management plan on Emergency Department card. 5. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and all patient documentation/property is on the trolley with the patient. 6. Prepare for the next patient. 7. When Bays 1-4 are full, bays 5-12, and the Minors area will be used to assess urgent category patients. 30
31 MAJOR INCIDENT ACTION CARD 6C EMERGENCY MEDICINE SPECIALTY TRAINEE 4 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Take the lead role in Casualty Treatment Team 6 allocated to Majors area, bays 1-4, where urgent category patients are being assessed. 3. Check that your treatment area is fully prepared and ready to receive a patient. 4. Summarise patient condition, treatment and management plan on Emergency Department card. 5. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 8. Prepare for the next patient. 9. When Bays 1-4 are full, bays 5-12, and the Minors area will be used to assess urgent category patients. 31
32 MAJOR INCIDENT ACTION CARD 6D EMERGENCY MEDICINE SPECIALTY TRAINEE 5 Role Casualty treatment 1. Go to the Clinical Decisions Unit. 2. Organise the treatment of the non-urgent patients triaged to this area. 32
33 MAJOR INCIDENT ACTION CARD 6E EMERGENCY MEDICINE SPECIALTY TRAINEE 6 Role Casualty treatment 1. Go to the Clinical Decisions Unit. 2. Organise the treatment of the non-urgent patients triaged to this area. 33
34 MAJOR INCIDENT ACTION CARD 7 EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 1 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 1 allocated to the Resuscitation Room, Bay 1. 34
35 MAJOR INCIDENT ACTION CARD 7A EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 2 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 2 allocated to the Resuscitation Room, Bay 2. 35
36 MAJOR INCIDENT ACTION CARD 7B EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 3 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 3 allocated to the Resuscitation Room, Bay 3. 36
37 MAJOR INCIDENT ACTION CARD 7C EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 4 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 4 allocated to the Resuscitation Room, Bay 4. 37
38 MAJOR INCIDENT ACTION CARD 7D EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 5 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 5 allocated to Majors area, Bays 1-4, where urgent category patients are being assessed. 38
39 MAJOR INCIDENT ACTION CARD 7E EMERGENCY DEPARTMENT PAEDIATRIC SPECIALTY TRAINEE 6 Role Casualty treatment 1. Assist the Emergency Department Consultant in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. Join Casualty Treatment Team 6 allocated to Majors area, bays 1-4, where urgent category patients are being assessed. 3. When Majors bays 1-4 are full, bays 5-12, and the Minors area will be used to assess urgent category patients. 39
40 MAJOR INCIDENT ACTION CARD 8 EMERGENCY DEPARTMENT NURSE 1 Role Triage Nurse assisting Triage Doctor 1. Collect Major Incident Packs and triage labels from the Major Incident Trolley. 2. Working together with the Triage Doctor, prepare to triage casualties as they arrive at the ambulance entrance. 3. On the arrival of each patient, affix an identification band and issue the corresponding Emergency Department card and numbered bag. These bags will be used as evidence by the police, and every item removed from a patient needs to be placed into the bag identified as belonging to a patient, and remaining with them. 4. On the instructions of the Triage Doctor, affix a colour coded triage label as follows: IMMEDIATE URGENT DELAYED DEAD (EXPECTANT RED YELLOW GREEN WHITE BLUE) 5. Allocate patients to the appropriate reception area according to their triage status as follows: IMMEDIATE RED RESUSCITATION ROOM THEN MAJORS 1-4 URGENT YELLOW MAJORS 5-12 AND MINORS 1-6 DELAYED GREEN CLINICAL DECISIONS UNIT DEAD WHITE MORTUARY (EXPECTANT BLUE CDU IF REQUIRED) 6. With the help of the Emergency Department receptionist, ensure that number/location details for each patient are recorded on the white board at the ambulance entrance. 7. Remain at the ambulance entrance and do not treat patients. 40
41 MAJOR INCIDENT ACTION CARD 8A EMERGENCY DEPARTMENT NURSE 2 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 1 in the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 41
42 MAJOR INCIDENT ACTION CARD 8B EMERGENCY DEPARTMENT NURSE 3 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 2 in the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 42
43 MAJOR INCIDENT ACTION CARD 8C EMERGENCY DEPARTMENT NURSE 4 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 3 in the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination, e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 43
44 MAJOR INCIDENT ACTION CARD 8D EMERGENCY DEPARTMENT NURSE 5 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 4 in the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 44
45 MAJOR INCIDENT ACTION CARD 8E EMERGENCY DEPARTMENT NURSE 6 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 5 in Majors area, bays 1-4, where urgent category patients are being assessed. 3. Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 10. When Majors bays 1-4 are full, bays 5-12, and the Minors area will be used to assess urgent category patients. 45
46 MAJOR INCIDENT ACTION CARD 8F EMERGENCY DEPARTMENT NURSE 7 Role Casualty treatment 1. Assist the Nurse in Charge Emergency Department in the formation of Casualty Treatment Teams, each consisting of two doctors and one nurse. 2. You are allocated to Casualty Treatment Team 6 in Majors Area, bays 1-4, where urgent category patients are being assessed. 3. Check that your treatment area is fully prepared and ready to receive a patient. 4. On the arrival of each patient, record vital signs and check that an identification band has been attached. 5. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 6. Assist medical staff with patient management and treatment as necessary. 7. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, of their intended destination e.g. Radiology/Theatres/PICU/Wards. They will book a bed space, arrange medical/nurse escorts as required and a porter. 8. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is on the trolley with the patient. 9. Update Major Incident Patient Board and prepare for the next patient. 10. When Majors bays 1-4 are full, bays 5-12, and the Minors area will be used to assess urgent category patients.. 46
47 MAJOR INCIDENT ACTION CARD 8G EMERGENCY DEPARTMENT NURSE 8 Role Casualty treatment 1. You are allocated to the Clinical Decisions Unit where non-urgent patients are being assessed. 2. Check that your treatment area is fully prepared and ready to receive patients. 3. On the arrival of each patient, record vital signs and check that an identification band has been attached. 4. Place any of the patient s clothing/property that is removed into the numbered plastic bag. 5. Assist medical staff with patient management and treatment as necessary. 6. Once the patient is ready to leave the Emergency Department, inform the Senior Nurse page holder on Ward 1E (page number 8345) based in the Training Room in ED, if they require admission to the wards. They will book a bed space, arrange a nurse escort and porter. 7. Once the escort team is available, ensure a verbal handover of important treatment/events and that all patient documentation/property is with the patient. 8. If a patient is ready for discharge home, ensure all documentation is completed and that discharge arrangements have been confirmed with an appropriate relative. Discharge can take place either directly from the Emergency Department, or via the Patient Reunion/Discharge Area in the Family Information and Support centre, Main Atrium. Check accurate contact details have been recorded for all patients discharged to ensure subsequent community follow up. 9. Update Major Incident Patient Board. 47
48 MAJOR INCIDENT ACTION CARD 8H EMERGENCY DEPARTMENT NURSE 9 Role Continue Emergency Department service for non-major incident patients 1. You are allocated to Clinic 3 Out-Patients Department, where non-major incident Emergency Department patients have been transferred/will continue to attend. 2. Take the Major Incident Airway, Circulation and Dressing trolleys to Clinic 3 in the Out-Patients Department. 3. Take Major Incident Drug box from Resus cupboard. 4. Check that the area is fully prepared and ready to receive patients. 5. Assist medical staff with patient assessment and treatment as necessary. 48
49 MAJOR INCIDENT ACTION CARD 9 EMERGENCY DEPARTMENT HEALTH CARE ASSISTANT 1 Role Assist with casualty treatment 1. You are allocated to the Resuscitation Room. 2. Assist the Casualty Treatment Teams in this area as required. 49
50 MAJOR INCIDENT ACTION CARD 9A EMERGENCY DEPARTMENT HEALTH CARE ASSISTANT 2 Role Assist with casualty treatment 1. You are allocated to Majors Area, bays 1-4, where urgent category patients are being assessed. 2. Assist the Casualty Treatment Teams in this area as required. 50
51 MAJOR INCIDENT ACTION CARD 9B HEALTH CARE ASSISTANT EMERGENCY DEPARTMENT 3 Role Assist with casualty treatment 1. You are allocated to the Clinical Decisions Unit where non-urgent patients are being assessed. 2. Assist with casualty treatment in this area as required. 51
52 MAJOR INCIDENT ACTION CARD 9C EMERGENCY DEPARTMENT HEALTH CARE ASSISTANT 4 Role Assist with casualty treatment 1. You are allocated to the Clinical Decisions Unit where non-urgent patients are being assessed. 2. Assist with casualty treatment in this area as required. 52
53 MAJOR INCIDENT ACTION CARD 9D EMERGENCY DEPARTMENT HEALTH CARE ASSISTANT 5 Role- Emergency Department service for non-major incident patients 1. You are allocated to Clinic 3 Out-Patients Department, where non-major incident Emergency Department patients have been transferred/will continue to attend. 2. Help take the Major Incident Airway, Circulation and Dressing trolleys and envelope marked Clinic 3 from the Major Incident Trolley round to Clinic 3, Out-Patients Department. 3. Check that the area is fully prepared and ready to receive patients. 4. Assist medical staff with patient assessment and treatment as necessary. 53
54 MAJOR INCIDENT ACTION CARD 10 SENIOR ANAESTHETIC SPECIALTY TRAINEE ON CALL Role Casualty treatment 1. Go to Emergency Department. 2. Take the lead role in Casualty Treatment Team 3 allocated to the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. Summarise patient condition, treatment and management plan on Emergency Department card. 5. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and all patient documentation/property is on the trolley with the patient. 6. Prepare for the next patient. 54
55 MAJOR INCIDENT ACTION CARD 10A CONSULTANT ANAESTHETIST ON CALL Role Casualty treatment supervision 1. Go to Emergency Department Resuscitation Room. 2. Work together with the Emergency Department/PICU Consultants on call to: (a) (b) (c) Assist Casualty Treatment Teams with resuscitation and stabilisation of patients. Coordinate transfer of patients to radiology, PICU, theatres and elsewhere. Organise anaesthetic support for patient transfers as required. 3. Decide on additional anaesthetic staff likely to be required in the Emergency Department and arrange for telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 55
56 MAJOR INCIDENT ACTION CARD 10B CONSULTANT CARDIAC ANAESTHETIST ON CALL Role Coordinate anaesthetic response in theatres 1. Go to theatres. 2. Decide on additional anaesthetic staff likely to be required in theatres and arrange for telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 3. Coordinate anaesthetic care of patients in theatres. This will involve close liaison with the Surgical Triage Officer based in the Emergency Department (Consultant Surgeon on call), the Senior Surgeon coordinating surgical care in theatres and Nurse in Charge theatres. 56
57 MAJOR INCIDENT ACTION CARD 10C JUNIOR ANAESTHETIC SPECIALTY TRAINEE ON CALL Role Assist with the anaesthetic management of casualties In the absence of the senior anaesthetic specialty trainee on call, you should assume that role until their arrival on site follow major incident action card 11. When/if senior trainee in hospital, you should follow junior anaesthetic trainee role: 1. Go to Theatres. 2. Check that theatres are fully prepared and ready to receive patients 3. Assist Consultant Cardiac Anaesthetist on call with anaesthetic management of casualties. 57
58 MAJOR INCIDENT ACTION CARD 11 SENIOR PICU SPECIALTY TRAINEE ON CALL Role Casualty treatment 1. Go to Emergency Department. 2. Take the lead role in Casualty Treatment Team 4 allocated to the Resuscitation Room, Bay Check that your treatment area is fully prepared and ready to receive a patient. 4. Summarise patient condition, treatment and management plan on Emergency Department card. 5. Once the patient is ready to leave the Emergency Department and an escort team is available, ensure a verbal handover of important treatment/events and all patient documentation/property is on the trolley with the patient. 6. Prepare for the next patient. 58
59 MAJOR INCIDENT ACTION CARD 11A PICU CONSULTANT ON CALL Role Casualty treatment supervision 1. Liaise with Nurse in Charge PICU to identify any patients who could be moved out of PICU/HDU and address staffing issues to maximise available PICU/HDU bed spaces. 2. Decide on additional PICU medical staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 3. Go to Emergency Department Resuscitation Room. 4. Work together with the Emergency Department Consultant/Consultant Anaesthetist on call to: (a) (b) Assist Casualty Treatment Teams with resuscitation and stabilisation of patients. Coordinate transfer of patients to radiology, PICU, theatres and elsewhere. 5. Be available to discuss possible requests for specialist paediatric skills needed nearer to/at the site of the major incident. RHC will respond as appropriate, through the pre-existing structure of the PICU transport service and this will include the capability to provide a Site Surgical Team. 6. Liaise with PICU RHSC Edinburgh. 59
60 MAJOR INCIDENT ACTION CARD 12 NURSE IN CHARGE PICU Role Preparation of PICU to receive casualties 1. Liaise with the PICU Consultant on call to identify any patients who could be moved out of PICU/HDU and address staffing issues to maximise available PICU/HDU bed spaces. 2. Decide on additional PICU nursing staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 3. Be aware of potential requests for specialist paediatric skills needed nearer to/at the site of the major incident. RHC will respond as appropriate, through the preexisting structure of the PICU transport service and this will include the capability to provide a Site surgical Team. 4. Liaise with PICU RHSC Edinburgh as required. 60
61 MAJOR INCIDENT ACTION CARD 13 CONSULTANT SURGEON ON CALL 1 Role Surgical Triage Officer oversees the surgical response to the major incident 1. Go to the Emergency Department. 2. Coordinate the surgical management of casualties. 3. Ensure that the right patients reach radiology and/or theatres at the right time with the right surgeon available liaise with the Senior Surgeon Theatres. 4. Decide on additional surgical staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 61
62 MAJOR INCIDENT ACTION CARD 13A CONSULTANT SURGEON ON CALL 2 Role Senior Surgeon Theatres 1. Ensure appropriate delegation of the task of liaising with the Surgical Wards to identify any patients who could be discharged to maximise available bed spaces. 2. Go to theatres. 3. Check with the Surgical Triage Officer (Consultant Surgeon on call) based in the Emergency Department on the additional surgical staff likely to be required in theatres and help arrange their telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 4. Coordinate the surgical care of patients in theatres. This will involve close liaison with the Surgical Triage Officer, Consultant Cardiac Anaesthetist (coordinating anaesthetic care in theatres) and Nurse in Charge theatres. 62
63 MAJOR INCIDENT ACTION CARD 13B SENIOR SURGICAL SPECIALTY TRAINEE ON CALL Role Assist with the surgical management of casualties In the absence of the Consultant Surgeon on call, the Senior Surgical Specialty Trainee on call will assume their role until the arrival on site of the Consultant Surgeon on call follow Major Incident Action Card Proceed to the surgical wards and identify any surgical patients who could be discharged to maximise available bed space. 2. Advise Contact centre to direct all GP receiving calls to extension to be dealt with by medical staff based in Clinic 3 in the Out Patients Department. 3. Call in additional surgical staff as directed by the Consultant Surgeons on call. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 4. Go to the Emergency Department. 5. Assist the Consultant Surgeon on call with the surgical management of casualties. 63
64 MAJOR INCIDENT ACTION CARD 13C BASIC SURGICAL TRAINEE Role If present to assist with the surgical management of casualties 1. Go to the Clinical Decisions Unit. 2. Help to organise the treatment of non-urgent patients triaged to this area. 64
65 MAJOR INCIDENT ACTION CARD 13D SURGICAL FY 1 Role Assist with the surgical management of patients 1. Go to Clinic 3 Out-Patients Department. 2. Help to organise the surgical treatment of existing/new non-major incident Emergency Department patients. 65
66 MAJOR INCIDENT ACTION CARD 14 ORTHOPAEDIC CONSULTANT ON CALL Role Coordinate the management of musculo-skeletal injuries 1. Go to the Emergency Department. 2. Coordinate the orthopaedic management of casualties. 3. Ensure that the right patients reach radiology and/or theatres at the right time with the right orthopaedic surgeon available. 4. Decide on additional orthopaedic staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 66
67 MAJOR INCIDENT ACTION CARD 14A ORTHOPAEDIC SPECIALTY TRAINEE ON CALL Role Assist with the management of musculo-skeletal injuries In the absence of the Orthopaedic Consultant on call, the Orthopaedic Specialty Trainee on call will assume their role until the arrival on site of the Orthopaedic Consultant on call follow Major Incident Action Card Proceed to the Acute Receiving Floor and identify any orthopaedic patients who could be discharged to maximise available bed space. 2. Advise Contact centre to direct all GP receiving calls to extension to be dealt with by medical staff based in Clinic 3 in the Out Patients Department. 3. Call in additional orthopaedic staff as directed by the Orthopaedic Consultant on call. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 4. Go to theatres. 5. Coordinate the orthopaedic care of patients in theatres. This will involve close liaison with the Orthopaedic Consultant on call, Consultant Cardiac Anaesthetist (coordinating anaesthetic care in theatres), Senior Surgeon Theatres and Nurse in Charge theatres. 67
68 MAJOR INCIDENT ACTION CARD 15 CONSULTANT PAEDIATRICIAN ON CALL Role Medical Triage Officer oversees the medical response to the major incident i.e. the treatment of non-surgical casualties 1. Go to the Emergency Department and contact the Hospital Coordinator. 2. If the major incident is not a surgical/trauma incident but a medical incident, help coordinate the medical management of casualties in the Emergency Department. 3. If the major incident is a surgical/trauma incident, liaise with the Clinical Decisions Unit and the Acute Receiving Floor to identify any patients who could be discharged to maximise available bed spaces. 4. Decide on additional paediatric medical staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 5. Continue to liaise with the Hospital Coordinator and the Emergency Department Consultant. 68
69 MAJOR INCIDENT ACTION CARD 15A SENIOR MEDICAL PAEDIATRIC SPECIALTY TRAINEE ON CALL Role To assist with the medical management of patients In the absence of the Consultant Paediatrician on call, the Senior Medical Paediatric Specialty Trainee on call will assume their role until the arrival on site of the Consultant Paediatrician on call follow Major Incident Action Card Go to Clinic 3, Out-Patients Department. 2. Coordinate the medical treatment of existing/new non-major incident Emergency Department patients. 3. Subsequently make yourself available to the Clinic 3 to assist in the treatment of non-urgent patients triaged to this area. 69
70 MAJOR INCIDENT ACTION CARD 15B JUNIOR MEDICAL PAEDIATRIC SPECIALTY TRAINEE ON CALL Role To assist with the medical management of patients 1. Provide a medical ward presence to assist the Consultant Paediatrician on call and the Senior Nurse Wards in identifying any medical patients who could be discharged to maximise available bed space. 2. Call in additional paediatric medical staff as directed by the Consultant Paediatrician on call. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 3. Advise Contact centre to direct all GP receiving calls to extension to be dealt with by medical staff based in Clinic 3 in the Out Patients Department.. 4. Subsequently make yourself available to the Clinical Decisions Unit to assist in the treatment of non-urgent patients triaged to this area. 70
71 MAJOR INCIDENT ACTION CARD 15C JUNIOR MEDICAL PAEDIATRIC SPECIALTY TRAINEE ON CALL Role To assist with the medical management of patients 1. Go to Clinic 3, Out-Patients Department. 2. Organise the medical treatment of existing/new non-major incident Emergency Department patients. 71
72 MAJOR INCIDENT ACTION CARD 16 SENIOR NURSE holding page 8399 on 2A Role Senior Nurse Medical Wards To prepare ward facilities for the reception of patients from the major incident 1. Go to the Major Incident Control Room in the Seminar Room in ED and contact the Senior Nurse on duty for the hospital (Page 8502/ DECT 85770). 2. Working from the Training Room in ED, assist the Senior Nurse on duty (Page 8502) in the task of alerting all wards. 3. In the process, establish bed status and the number of trained nurses and other ward staff who could be made available to assist elsewhere with the major incident response, without jeopardising ward patient care. 4. Request the nursing staff on all wards, in conjunction with medical staff, to identify any patients who could be discharged to maximise available bed spaces. Collate this information as it becomes available and share with the Hospital Coordinator. 5. Deploy additional available ward nurses and other staff as appropriate/necessary to the Emergency Department, Clinic 3 Out Patients Department, the Relatives Waiting Area (Therapies Hub) and the Patient Discharge/Reunion Area (Outpatient Clinic 5). 6. Allocate a member of nursing staff to the HAN base to record on an Action Card Pick Up list who has arrived to fulfil action card roles. Ensure this member of staff picks up a walkie talkie, and keeps a register of additional staff arriving, and where staff have been allocated too. The two page holding senior nurses need to be kept up to date with this information. Be aware of ongoing hospital staffing requirements. Any staff arriving that do not have an action card, and do not immediately need to be deployed should have their name and designation recorded and asked to wait in the Discharge lounge (Area 3D). As the need arises relevant staff can be deployed from this area. Close contact must be maintained with this staff member. 7. Arrange contact of additional off duty nursing staff as required. Do not call the Contact Centre operator - call directly using the appropriate departmental telephone contact lists. 8. Allocate Volunteer Coordinator. 9. Liaise with Duty Social Worker and Hospital Chaplin. 72
73 MAJOR INCIDENT ACTION CARD 16A SENIOR NURSE holding page 8345 on Ward 1E Role Senior Nurse Surgical Wards Help prepare ward facilities for the reception of patients from the major incident and coordinate their safe transfer from the Emergency Department 1. Go to the Major Incident Control Room and contact the Senior Nurse on duty for the hospital (Page 8502/ DECT 85770). 2. Working from the Training Room in ED, assist the senior nurse on duty (page 8502/ DECT 85770) in the task of alerting all wards. 3. Go to the HAN base AND ALLOCATE ANOTHER MEMBER OF STAFF to record on an Action Card Pick Up list who has arrived to fulfil action card roles. Ensure they pick up a walkie talkie, and keep a register of additional staff arriving, and where staff have been allocated too. The two page holding senior nurses need to be kept up to date with this information. Be aware of ongoing hospital staffing requirements. Any staff arriving that do not have an action card, and do not immediately need to be deployed should have their name and designation recorded and asked to wait in the Discharge lounge (Area 3D). As the need arises relevant staff can be deployed from this area. Close contact must be maintained with this staff member. 4. Return to the Training room in ED to assist with bed booking and allocation. 5. In the process, establish bed status and the number of trained nurses and other ward staff who could be made available to assist elsewhere with the major incident response without jeopardising ward patient care. 6. Request the nursing staff on all wards, in conjunction with medical staff, to identify any patients who could be discharged to maximise available bed spaces. Collate this information as it becomes available and share with the Hospital Coordinator. 7. All bed requests for patients being admitted will be channelled through you. During working hours the bed manager (8521) will assist in this role. Organise porters for patient transfers to Radiology/Theatres/PICU/Wards and, in conjunction with the Consultant Anaesthetist on call, arrange medical/nurse escort teams as required. 73
74 MAJOR INCIDENT ACTION CARD 17 SENIOR NURSE THEATRES page 8092 Role To prepare theatre suite for the reception of patients from the major incident requiring surgical intervention 1. Work together with the Surgical Triage Officer (Consultant Surgeon in the Emergency Department), the Consultant Cardiac Anaesthetist (coordinating anaesthetic care in theatres) and the Senior Surgeon Theatres to coordinate the surgical care of patients in theatres. 2. Allocate a member of nursing staff to contact theatre staff from major incident contact list starting from the most senior staff, anaesthetic team and scrub, floor staff 3. Ensure that the set up of adequate theatre space for emergency cases is underway. To facilitate this preparation, on receiving warning of major incident relating to RHC: - gain an estimate of casualties and the range of specialties required if known, from the major incident control room - set up theatres based on estimated number of patients - as staff arrive ensure staff reporting base aware, and that if they have a specific major incident action card this has been collected, and the designated role fulfilled - check in and allocate to theatre - If staff arrive that are not required in theatre direct them to the staff reporting area, then the staff holding area at the HAN base to be called upon when and where they are required Anaesthetic Nurses - prepare fluid warmer - prepare level 1 infuser - set up invasive monitoring - ensure ventilator checks are performed - increase environmental temperature in theatres - ensure adequate stock of blood sampling bottles Scrub/floor Nurses - gather surgical instruments required for range of specialties - locate specialist equipment 74
75 MAJOR INCIDENT ACTION CARD 18 EMERGENCY DEPARTMENT RECEPTIONIST ON DUTY Role To provide accurate and reliable administrative support to the reception area during a major incident 1. Identify the pre numbered MI packs in the filing cabinet at reception 2. Note the time of arrival of the first major incident casualty. 3. Assist the triage team in the issue of one Major Incident Pack per patient as each patient arrives, ensuring careful adherence to the number sequence. 4. See Major Incident Patient Registration process Appendix Record the number/location details for each patient on the white board at the ambulance entrance, as directed by the Triage Nurse. 6. Stay in position at the Ambulance Entrance until notified of major incident stand down. 75
76 MAJOR INCIDENT ACTION CARD 18A MEDICAL RECORDS PERSONNEL Responsibilities The Health Records Department are responsible for providing: A Health Records Documentation Team to register and process patients attending the ED Department following a Major Incident. Senior Health Records Information Officer to assist in the control room. To keep and maintain an Incident Register Initial Actions The ED clerical staff should inform a senior Health Records Officer that an Incident has occurred. This officer will act as the Incident Officer within the Department ensuring adequate staffing levels are provided during the Incident. Health Records Manager should be notified immediately. The Health Records Incident Officer should set up a clerical incident desk within ED Reception ensuring that the pre-numbered Major Incident packs are available prior to the arrival of the casualties The Health Records Incident Officer should allocate clerical staff to receive the casualties at the appropriate entrance. Clerical staff should transfer patients currently in ED who are not being discharged to Area 3 of the Out Patient department, and provide a member of staff to register patients attending Area 3 if possible. Upon arrival of the patients the ED clerical staff should: Register the casualties on to the Hospital Administration system using the unique patient identifier number included in the documentation pack provided for each casualty. After Registration provide the clinical staff with the Major Incident Documentation pack. Provide a copy of the patients Registration document to the Police Bureau which is based near the Hospital Control Room. Update and maintain the Major Incident Register as the Incident progresses Liaise with the Hospital Coordinator. Stand down 76
77 Update the Major Incident Register with all discharge locations ensuring that all patient identifiers have been merged or created. 77
78 MAJOR INCIDENT ACTION CARD 18 HEALTH RECORDS SENIOR Responsibilities To facilitate the provision of accurate and reliable administrative support during a major incident. Initial Actions 1. Review available medical records staff resources and ensure all key roles are filled. 2. Decide on additional medical records staff likely to be required and arrange for telephone call in. Do not contact operator call directly using departmental phone. 3. Liaise with incident controller as necessary. 78
79 MAJOR INCIDENT ACTION CARD 18D MEDICAL RECORDS STAFF 3 Role To provide accurate and reliable administrative support to the reception area during a major incident 1. Move around the Emergency Department to obtain accurate patient identification details where possible and at the convenience of medical and nursing staff. 2. Update major incident casualty list as information is collected. 79
80 MAJOR INCIDENT ACTION CARD 19 GENERAL SERVICES SUPERVISOR Role To coordinate portering services with reference to action cards 32, 32 A-C. Ensure that one porter is tasked with locking down and securing hospital entrances/exits as required. 1. Delegate the following tasks as a priority: (a) (b) Collection of the major incident emergency signs from the Major Incident Store cupboard in the Emergency Department and ensure that these are displayed as detailed in Appendix 2. Out-of-hours, open the Out-Patients Department, open up the Therapies Hub and Outpatient Clinic 5. Contact Security staff for assistance 2. Base yourself in the Training Room in the ED, to liaise with Senior Nurses from 2A (8399) and Ward 1E (8345) 3. Send a porter to the main hospital road entrance to direct: (a) (b) (c) (d) Major incident patients round to the Emergency Department ambulance entrance. Standby ambulance patients not involved in the Major Incident should also enter via the ED ambulance entrance. All other emergency patients not involved in the major incident should be directed to to Clinic 3 Out-Patients Department. Relatives to the Relatives Waiting Area, in the Adult OPD in a mixed MI, or the Therapies Hub in an incident affecting purely children, clarify with the MI Coordination team if unsure. Media/press representatives- discuss with on call press office re appropriate location. Staff Volunteers discuss with Hospital Coordinator. 4. Decide on additional portering staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 5. Maximise the number of wheelchairs and trolleys available in the trolley bay at the Emergency Department ambulance entrance. 6. Ensure that all available General Services Staff report to the HaN base to await allocation of further tasks. 7. Liaise with Hospital Coordinator as necessary. 80
81 MAJOR INCIDENT ACTION CARD 20 POLICE LIAISON OFFICER Role To liaise with Police Scotland Casualty Bureau Documentation Team 1. Ensure the establishment of the Police Control Room in the Adult Emergency Department. 2. Identify yourself to the Senior Police Officer on site. 3. Assist the police as required and with reference to the information set out in Appendix 7 of the Major Incident Plan. 81
82 MAJOR INCIDENT ACTION CARD 21 HOSPITAL ENQUIRIES OFFICER Role To provide appropriate information and directions to hospital visitors during a major incident 1. The Hospital Major Incident Enquiry Desk will be located at the front desk in the main hospital entrance. 2. The Enquiry Desk will act as a focus point for anyone who attends the hospital in person asking about casualties from the major incident. 3. Relatives up to the Relatives Waiting Area, in adult OPD in a mixed incident, and in the Therapies Hub in a paediatric incident. Liaise with on call press officer re press personnel, and Hospital Coordinator re volunteers. 4. You should be as satisfied as possible as to the identity of visitors and only admit bona fide enquirers through to clinical and relative waiting areas. Some form of escort should be provided if possible. 5. The Enquiry Desk will be updated as regularly as possible with relevant patient information via runners. 7. People attending the Enquiry Desk asking about individuals on whom you have no information should be advised to contact the Police Scotland Casualty Bureau. 8. Any staff reporting to the Enquiry Desk should be directed to the HaN room to register and await further instructions, non registered and unknown volunteers should be thanked for their offer of help but advised that they cannot assist. 82
83 MAJOR INCIDENT ACTION CARD 21A HOSPITAL ENQUIRIES OFFICER ASSISTANT Role To staff the Day Surgery Unit reception desk 1. The Therapies Hub and Outpatients Clinic 5 will be used as the Relatives Waiting Area and the Patient Reunion/Discharge Area respectively. 2. Base yourself at the reception desk at the ground floor entrance to monitor access to these areas. You should be as satisfied as possible as to the identity of visitors and only admit bona fide enquirers through to the relative waiting areas. 3. Provide assistance to the Relative Coordinators as required. 83
84 MAJOR INCIDENT ACTION CARD 22 RELATIVE COORDINATOR 1 Role To look after the relatives of casualties and provide as accurate and up-todate information as possible 1. The Relatives Waiting Area is located in the Adult Out Patient Department in a mixed incident, or the Therapies Hub in a paediatric incident. 2. An accurate record of attending relatives details should be established. 3. You should endeavour to keep relatives as fully informed as possible with regard to patients conditions and progress. The Relatives Waiting Area will be updated regularly with relevant patient information via runners. 4. As a general rule, parents and their children should be re-united as soon as is practicably possible. 5. Ensure availability of basic refreshments. 6. Patient reunions with relatives and subsequent discharge should be organised to take place in Outpatients Clinic Area 5. 84
85 MAJOR INCIDENT ACTION CARD 22A RELATIVE COORDINATOR 2 Role To coordinate patient reunions with relatives and subsequent discharge 4. The Patient Reunion Area is adjacent to the Relatives Waiting Area and is located in the Adult Out Patient Department in a mixed incident, or the Therapies Hub in a paediatric incident.. 2. Check accurate contact details have been recorded for all patients discharged from the Reunion/Discharge Area to ensure subsequent community follow up. 3. Ensure availability of basic refreshments. 4. Assist with arrangements for patient transport home as required. 85
86 MAJOR INCIDENT ACTION CARD 23 PRESS OFFICER Role To manage media handling of the major incident This role will be filled by the NHSGGC Press Officer on call, contactable through the Communications Department, NHSGGC HQ at JB Russell House. In their absence, it is the responsibility of the Hospital Coordinator to nominate an alternative. The following is guidance until the arrival of the NHSGGC Press Officer. 1. The Press Officer will be based in the Training Room adjacent to the Seminar Room in the Emergency Department. 2. Media representatives arriving on site will be directed to the Aroma Coffee shop to await instruction upon arrival of the NHSGGC Press Officer. 3. It should be made clear that under no circumstances should children be spoken to or photographed without the express consent of their parent or guardian. 4. Update media representatives on site on a regular basis and field any media phone calls. 5. Liaise with the Hospital Coordinator with regard to the content of any official press release and the organisation of any press conferences or interviews. Consider requests for access by press photographers and television cameras to clinical areas. Similarly, work together with the Hospital Coordinator to coordinate VIP visits to the hospital. 86
87 MAJOR INCIDENT ACTION CARD 23A PRESS OFFICER ASSISTANT Role To assist the Press Officer with media representatives 1. The Press Officer Assistant will be based in the Training Room adjacent to the Seminar Room in the Emergency Department. 2. Assist the Press Officer in providing regular updates to the media representatives on site. 3. Try to ensure that media representatives remain in the Aroma Coffee shop, or an alternative location as per the direction of the NHSGGC Press Officer, unless being escorted for approved access elsewhere in the hospital. 87
88 MAJOR INCIDENT ACTION CARD 24 Responsible Officer: Duty MLSO HAEMATOLOGY AND BLOOD TRANSFUSION Role To manage haematology major incident response 1. Contact Consultant Haematologist on call and Senior Chief MLSO. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 2. Contact Hospital Coordinator to ascertain the anticipated number and type of casualties. 3. Contact the Regional Blood Transfusion Centre and arrange additional supplies of blood products. 4. Ensure that adequate staff are available to coordinate the receipt of specimens and dissemination of results and blood products. 5. Liaise regularly with Emergency Department, operating theatres and PICU. 88
89 MAJOR INCIDENT ACTION CARD 25 Biochemistry RESPONSIBILITIES Responsible for the preparation and provision of biochemistry laboratory services. Mobilisation of additional staff as required. ACTIONS 1. If during core hours the reporting Biochemist who receives notification of a major incident will inform the Technical Services Manager (TSM) or Laboratory Sector Manager (LSM) that a major incident has occurred. 2. If outside core hours the Consultant Biochemist On-Call who receives notification of a major incident will inform one of the Biomedical Scientists working on shift that a major incident has occurred. 3. If the nature of the incident is such that a significant increase in urgent Biochemistry analysis is expected the TSM/LSM or Consultant Biochemist On-Call will inform the BMS staff working in core Biochemistry. 4. BMS staff will take steps to clear outstanding work. 5. BMS staff will ensure the Architect and blood gas analysers are ready to receive samples. PRIORITIES Informing the BMS staff working in core Biochemistry Preparing the analysers to receive samples. If outside core hours: 1. the on-call consultant biochemist will consider whether the expected workload requires additional BMS staff to attend the laboratory. If so they will arrange this by telephoning BMS staff at home. 2. If considered necessary the Consultant on call will make his/her way to the department, or if this is not immediately possible, arrange for a reporting biochemist to attend. 3. The consultant or reporting biochemist will then a) handle telephoned or paged requests for emergency analyses, and b) telephone results relating to patients 89
90 MAJOR INCIDENT ACTION CARD 26 Action Card Contact Telephone Number: EXT (once in hospital) Paediatric Radiographer RESPONSIBILITIES Responsible for co-ordinating and providing specialist radiological investigations in consultation with clinical staff. IMMEDIATE ACTIONS 1. Attend x-ray department. Arrange for on-call radiology Consultant to attend. 2. Check on call radiographer has been contacted and cascade has been initiated. 3. Radiology call-out using cascade. 4. Assess resources currently available and further staff required. 5. Arrange for consultant radiologist to attend emergency department. 6. Respond to requests for radiological referrals. 7. Liaise closely with Senior Emergency Physician on capacity for radiological investigations. 1. PRIORITIES Ensure adequate radiology and radiographer staffing. Liaise regularly with Senior Emergency Physician and Lead Consultant Radiologist 90
91 MAJOR INCIDENT ACTION CARD 26A SENIOR RADIOGRAPHER Role To initiate preparation for radiology major incident response 1. If not already informed, ensure Superintendent Radiographer is contacted. 2. Decide on additional radiology staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 2. Assess priority of work until arrival of Consultant Radiologist on call. 3. Arrange teams as necessary to cover workload in the Emergency Department and operating theatres in addition to the Radiology Department. 91
92 MAJOR INCIDENT ACTION CARD 27 CONSULTANT RADIOLOGIST ON CALL Role To oversee radiology major incident response 1. Go to Radiology Department. 2. Contact Hospital Coordinator in the ED Seminar room to ascertain the anticipated number and type of casualties. 3. Decide on additional radiology staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator - call directly using your departmental telephone contact list. 4. Assess and control priority of work. Liaise regularly with the Emergency Department Consultant and Surgical Triage Officer (Consultant Surgeon on call based in the Emergency Department) to inform this process. 5. Ensure hot reporting of imaging as appropriate. 92
93 MAJOR INCIDENT ACTION CARD 28 PHARMACIST ON CALL Role To manage pharmacy major incident response 1. Contact the Pharmacy Manager**. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. (Contact List in On-Call Bag and copy at front of Major Incident Plan ) 2. Go to Pharmacy. 3. Arrange for supplies of drugs and IV fluids as required by the Emergency Department, operating theatres and PICU/wards. 4. Dispense medicines as required for Emergency Department patients/in-patients being discharged from hospital. ** Pharmacy Managers:- Lead Clinical Pharmacist Stephen Bowhay Sector Chief Technician Joanne Barton 93
94 MAJOR INCIDENT ACTION CARD 28A PHARMACY MANAGER Role To manage pharmacy major incident response 1. Go to Pharmacy. 2. Contact Hospital Coordinator to assess likely demand for pharmacy services. 3. Decide on additional pharmacy staff likely to be required and arrange for telephone call in. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. (Contact List can be found in On-Call Bag and Front of Major Incident Plan) 4. Arrange for supplies of drugs and IV fluids as required by the Emergency Department, operating theatres and PICU/wards. 4. Dispense medicines as required for Emergency Department patients/in-patients being discharged from hospital. ** Pharmacy Managers:- Lead Clinical Pharmacist Stephen Bowhay Sector Chief Technician Joanne Barton 94
95 MAJOR INCIDENT ACTION CARD 29 DUTY SOCIAL WORKER Role To manage social work major incident response 1. Organise a social work team to attend the hospital. Do not call the Contact Centre operator- call directly using your departmental telephone contact list. 2. Social Work Team Leader to liaise with Senior Nurse page holders from 2A (8399) and Ward 1E (8345) to discuss social work support required for casualties and their families. 3. Contact Family Support Service to enlist their assistance. 4. Contact Department of Child and Family Psychiatry and Bereavement Service as appropriate. 5. Liaise with hospital chaplaincy service to ensure support tasks are allocated appropriately. 95
96 MAJOR INCIDENT ACTION CARD 30 HEALTHCARE CHAPLAINCY SERVICE ROLE The Healthcare Chaplaincy Service provides and facilitates spiritual care to patients, families and staff. Spiritual care may or may not include religious care. The resources of the service, spiritual care facilities and of faith / belief community representatives will be made available. 1. Healthcare Chaplain will assess needs and contact other Chaplains and faith representatives as required, as per Chaplaincy Service internal protocol. 2. Liaise with Emergency Department Relatives Coordinator in Therapies Hub (Ground Floor Atrium.) 3. The RHC Sanctuary (Ground floor) will be staffed for use by relatives and staff. 4. The service will ensure adequate cover to respond to requests for spiritual care services elsewhere on Hospital site. 5. The service will be available to provide staff support, before and after stand down, where appropriate. 6. Chaplaincy Service will ensure on-going Chaplaincy cover is available to provide follow-up support for patients and relatives transferred to wards. 96
97 MAJOR INCIDENT ACTION CARD 31 MORTUARY TECHNICIAN Role To provide mortuary services as required 1. Contact Consultant Pathologist on call. Do not call the Contact Centre operatorcall directly using your departmental telephone contact list. 2. Contact Hospital Coordinator to discuss any anticipated need for a temporary mortuary facility. 3. Open hospital mortuary and prepare to receive bodies of any fatalities. 4. Contact second mortuary technician. Do not call the Contact Centre operatoragain call directly using your departmental telephone contact list. 5. Maintain a register of dead patients according to details available, which may only be a numbered major incident identification band. 6. Second mortuary technician to alert other laboratory staff as required. 97
98 MAJOR INCIDENT ACTION CARD 32 PORTER 1 Role - Enact lockdown of hospital and non essential buildings in accordance with standard procedures or as directed by Site Facilities Manager/Major Incident Control 1. Lock down and secure hospital entrances/exits this involves the same security measures that are currently in place for the post 10pm and weekend shutdown. 2. Report to the Training Room in the ED, where the General Services Manager is based for further instructions 98
99 MAJOR INCIDENT ACTION CARD 32A PORTER 2 Role - To display external major incident signs at main roads and provide directions to persons arriving at hospital 1. Collect Major Incident In Progress and All Press enquiries to Main Entrance signs from the Major Incident cupboard in the Emergency Department and display at main traffic entrance to hospital 2. Remain at main traffic entrance and direct traffic / pedestrians as follows: a) Major incident patients to ED ambulance entrances b) All other emergency patients to Outpatients Department Clinic 3 c) Relatives of Major Incident patients to Relatives Waiting Area in the Therapies Hub in a paediatric incident, and the Adult Out Patient Department in a mixed MI d) Media / Press representatives to Aroma Coffee Shop e) Staff Volunteers to the HaN base on the second floor 99
100 MAJOR INCIDENT ACTION CARD 32B PORTER 3 Role: To display external major incident signs ED Department and provide directions to persons arriving at hospital 1. Collect Major Incident In Progress and All Press enquiries to Main Entrance signs from he Major Incident cupboard in the Emergency Department and display at Emergency Department Entrance 2 Collect Major Incident in Progress Ambulances Only Diversion for all other traffic sign and display at Govan Road entrances and Hardgate Road entrance 3. Remain at Emergency Department entrance and direct traffic / pedestrians as follows: a) Major incident patients to ED ambulance entrances b) All other emergency patients to Outpatients Department Clinic 3 c) Relatives of Major Incident patients to Relatives Waiting Area in the Therapies Hub in a paediatric incident, and the Adult Out Patient Department in a mixed MI d) Media / Press representatives to Aroma Coffee Shop e) Staff Volunteers to the HaN base on the second floor 100
101 MAJOR INCIDENT ACTION CARD 32C PORTER 4 Role: To display internal major incident signage as per guidance and Appendix 2 and open OPD, Day Surgery, Physiotherapy Gym and Major Incident Hub as required 1. On instruction ensure that relevant Major Incident signage is displayed correctly at the following locations: a) Seminar Room Emergency Department - on door Major Incident Control Room b) Training Room in Emergency Department- on door Senior Nurse /Press Officer c) HAN base and adjacent Seminar Room, 2 nd floor - on door Staff Reporting Base 2. Report to Training Room in the Emergency Department for further instructions 101
102 QEUH AND RHC Decontamination Plan Action Card 1 Senior Nurse Emergency Department Responsibilities: Actions: 1. Identify Decontamination Lead in conjunction with Senior Emergency Physician 2. Identify, if possible, the nature of the contamination. 3. Continue with Co-ordination of the Emergency Department 1. Inform security 2. Start and Maintain a log of incident/ decisions taken 3. Clear clinical areas as needed, e.g. by sending patients directly to wards. 4. Ensure contaminated casualties are kept out of the ED. If prior warning of a contamination incident is obtained, a member of staff should be allocated to meet the ambulance and ensure patients are not taken directly to ED. 5. If contaminated patients are in the ED, follow action card 3. Continue with duties as below. 6. Nominate the next most senior or appropriately trained member of staff to act as Decontamination Lead. If you are the most appropriately trained person on duty, hand the Nurse In-charge role over and manage the Hazmat/CBRN incident yourself. Ensure Radiation Protection Advisor contacted in a radiation incident. 7. Allocate staff for decontamination team (at least initially). If insufficient staff available call in decontamination trained staff from call-in sheets. 8. Inform Switchboard to place hospital on Major Incident Stand By (Hazmat/CBRN). 9. Call duty manager and ED consultant. 10. Continue to liaise with Decontamination Lead and the Hospital Control Team (if a Major Incident has been declared). 11. Continue with management of the Emergency Department. If Major Incident Not Declared: 1. Monitor staff resources and allocate someone to call in additional staff as required. If Major Incident Declared: Priorities: 1. Follow your action card in the Major Incident Plan. 1. Allocate staff for decontamination 2. Control entry into the emergency department 102
103 QEUH AND RHC Decontamination Plan Action Card 2 Senior Emergency Physician Responsibilities: 1. Identify Decontamination Lead. 2. Continue with Co-ordination of the Emergency Department. Initial Actions: 1. Start and maintain a log of activity/ decisions taken 2. Obtain a radio from staff area RCH ED to facilitate communication with the decontamination team. 3. Ensure contaminated casualties are kept out of the ED. 4. If contaminated patients are in the ED follow action card for this. Continue with duties as below. 5. Together with nurse in-charge, allocate staff for decontamination team (one or more medical staff may be needed for this depending on clinical condition of incoming contaminated patients). 6. Consider closing the Emergency Department, i.e. by phoning the ambulance service, and informing other local Emergency Departments. 7. Ensure hospital management are informed and are providing assistance. 8. Allocate medical staff duties, e.g. prepare for resuscitation cases. 9. Ensure on call public health consultant is contacted to inform them of incident and,if necessary, to ask their assistance in: a. accessing information on treatment b. advice on symptoms 10. Ensure that a Radiation Protection Advisor is contacted in a radiation incident, via switch. A back-up list of contact numbers is held in the Radiation Box in the decontamination unit storage area. Priorities: 1. Allocate staff for decontamination 2. Prepare emergency department for resuscitation cases 103
104 QEUH AND RHC Decontamination Plan Action Card 3 Contaminated patients inside the Emergency Department The ED must be closed in this eventuality. Senior Staff on duty should ensure the following is carried out: 1. Move the contaminated casualties outside the ED (or, if appropriate keep isolated from other persons in the ED): if a patient is a resuscitation case, balance the risks to the patient of being moved outside versus safety of staff and others within the ED, move the contaminated patients to an area away from the entrance of ED, down wind and away from others, stay away and up wind from these casualties, once staff are in PPE, they should approach the casualties to provide triage, decontamination, and treatment. In a radiation incident contamination level can be ascertained using the Geiger counter stored in the decontamination preparation room. 2. Cross Contamination: identify any staff or others who may have become contaminated as a result of exposure or contact with the contaminated casualties, move those who are at high risk of this outside ED, treat them as contaminated casualties, those less likely to be cross contaminated should have clothing changed (discarded clothes sealed in a bag), hands washed etc. If in doubt, move them outside as above. 3. Isolate the area affected: move all staff and patients outside the area, cordon off the area, using chairs, tape, and trolleys, place do not enter signs on cordon, keep all persons out of cordoned off area until declared safe by the appropriate authority, e.g. public health, radiation protection advisor. 4. Ventilate: (This applies to airborne contaminants, such as vapours and dusts.) open doors and windows to allow ventilation, taking care not to spread contaminant further into the building by taking account of wind direction and closing internal doors as appropriate. 5. Reduce Spread: close off all but one access route from ED into the hospital (e.g. lock doors), establish a cleaning station on the remaining access route, providing at the station: o a cordon using chairs, trolleys, and signs, o position a member of staff at the station, e.g. domestic supervisor or deputy, o clean patient trolleys to enable any patients coming from ED to be moved onto a clean trolley, then return the ED trolley back to ED, o plastic theatre overshoes, gloves and apron for staff to change into each time they pass the station, in either direction, o garbage bags. o reduce movement of personnel through this point to a minimum, o domestic staff: repeatedly clean the corridor floors on the hospital side of the station, using usual mop and bucket and on the ED side of the station using separate equipment. 6. Lockdown of other areas immediately adjacent. 104
105 QEUH AND RHC Decontamination Plan Action Card 4 Decontamination Lead Officer Locate yourself in the clean side of the area close to the decontamination module. There is no need to wear PPE. Responsibilities: 1. Assume command of the decontamination response (responsible for overall management including recovery). 2. Liaise with Senior Emergency Physician and Senior Nurse Emergency Department Initial Actions: 1. Direct facilities to undertake lockdown as an initial precautionary measure. It will be necessary to control the movement of public, patients & staff to ensure the Clean and dirty areas are clearly separated and to prevent contaminated patients entering the hospital (setting up barriers/cordons & directing traffic). 2. If sufficient warning of inbound contaminated patients is received set up a reception point outside of the hospital building in order to prevent cross contamination. Contaminated patients should then be directed to a suitable triage location and holding area. Patients known to be contaminated by radiation should remain in the ambulance until they are brought one by one to the decontamination facility entrance, located between the entrances to the paediatric and adult ED. 3. Communicate with decontamination team, senior ED physician and ED senior nurse via radio (available from staff area RCH ED). Source Dect phone also. 4. Assess the situation to determine the type of contaminant and method of decontamination required. 5. Seek expert advice and support in risk assessment and decision-making. Where possible, the following information should be obtained: Number of casualties? What are the signs and symptoms? Type of contaminant? Is it necessary to maintain Lockdown? If so is it the Emergency Department only or the entire hospital site? Is it likely that decontamination will be required? If so, what is the best method of decontamination? What level of PPE is likely to be required? Wind direction? Number of trained operators available? Number of suits available? 105
106 Information relating to the incident can be obtained from: Patients, SAS or NHS staff at the scene of incident, Local Police. REFER TO EXPERT ADVICE CONTACT LIST Specialist information can be obtained from: Fire & Rescue Service, SAS, Public Health Department, Health Protection Scotland, Radiation Protection Advisor, Health Protection Agency, National Poisons Information Service 6. Nominate members of decontamination team (or teams if first strike and clinical decontamination teams are required). If insufficient staff available call in decontamination trained staff from call-in sheets. 7. Arrange for the decontamination facility to be made operational. 8. Ensure Decontamination Team wear the correct PPE. 9. As waste water storage capacity is limited contact Scottish Water and advise of potential need to run to drain 10. Maintain effective communications (detail a member of staff as a runner if necessary) with: Hospital Control Room Emergency Department, Queen Elizabeth University Hospital +/- Royal Children s Hospital if paediatric cases involved. 11. Log all messages and actions taken (detail a member of staff as a scribe if available to assist with this). 12. Ensure decontaminated persons are clean. Radiation levels should be checked with a monitor at the point of exit from the dirty to the clean area to ensure no contamination of the ED department. 13. When monitoring and decontamination is compete all members of the team must be monitored, remove their protective clothing and decontaminated if necessary. 14. Ensure decontamination area is cleared of any waste and valuables and equipment which should be handled and stored appropriately. In radiation incidents waste disposal will be coordinated by the RPA. 15. Post incident, organise a hot debrief for members of the decontamination team and other staff involved in the incident. 16. Ensure Media/communications is handled appropriately 17. Ensure security is in place. 106
107 Priorities: 1. Take command of whole decontamination process 2. Maintain effective communication with emergency department, hospital control room and external agencies e.g. SAS, F&R 107
108 QEUH AND RHC Decontamination Plan Action Card 5 Decontamination Entry Control Officer Responsibilities: 1. Management of decontamination team, 2. Ensure the safety of all members of the decontamination team, 3. Management of the decontamination process (positioned in the Clean Zone), 4. Quality Assurance of patients exiting decontamination. Initial Actions: 1. Don theatre blues/greens. 2. Go to the toilet. 3. Have a soft drink. 4. Remove all jewellery. 5. Gather equipment: permanent marker pen, decontamination team monitoring board Patient Decontamination body map forms tuff cut scissors. 6. Consider if a separate team is required to set up the Clinical Decontamination equipment if another is involved in improvised/ interim decontamination. 7. Ensure safety team are in relevant PPE and ready to enter the Decontamination area should they be required 8. Number all staff as they enter the dirty zone and log the time on the board. 9. Scribe, or allocate a member of staff in clean area to scribe, upon the body map areas of contamination identified by the triage officer for each patient. Use TJ trakcare numbers to identify patients for the duration of the decontamination incident. 10. Monitor all personnel for signs of exhaustion, problems etc. 11. After maximum of one hour, arrange relief of personnel on the dirty side and assist out of suits. Log time on the board. 12. Ensure suits are bagged and tagged for decontamination. 13. Log all information from decontamination team board onto hard copy and give to Lead Nurse, Emergency Department. 14. Monitor the Health & Safety of all Staff within the dirty side. 15. Maintain effective communications with the Triage Officer, Decontamination Operators, and Decontamination Team Leader. Ensure staff in PPE use hands free radios, stored in Paediatric ED staff area, with staff in the clean area on hand held devices. Priorities: 1. Ensure safety of decontamination teams 2. Keep decontamination team monitoring board up to date 3. Liaise regularly with Triage Officer, Decontamination Operators and Decontamination Team Leader 108
109 QEUH AND RHC Decontamination Plan Action Card 6 Triage Officer Responsibilities: 1. Triage of contaminated patients using triage sieve. 2. To be the 1st member of the decontamination team into the dirty zone, 3. To start decontamination of casualties prior to formal decontamination in unit. Action: 1. Don theatre blues/greens. 2. Go to the toilet. 3. Have a soft drink. 4. Remove all jewellery. 5. Don appropriate PPE and enter dirty zone. 6. Gather equipment: 2 x buckets per person, 1 filled with tepid/warm, 1 filled with tepid/warm water and 20ml of detergent, Tuff cut scissors, Property bags, Disrobe packs, Marker pen, Sponges. Radiation monitor and patient decontamination forms in a radiation incident 7. Reassure casualties waiting for decontamination. (Issue instructions such as remove outer garments and rinse using buckets and sponges to assist in decontamination process). 8. Assess each of the casualties/self presenters to decide which, if any, require decontamination see algorithm 9. Triage patients using triage sieve for order of decontamination. 10. Carry out patient decontamination/treatments prior to formal decontamination in decontamination unit. 11. Inform decontamination team of order of priority. 12. Assist decontamination team in appropriate treatments and decontamination of patients. 13. Monitor the Health & Safety of all Staff within the dirty zone. 14. Liaise with Decontamination Entry Control Officer and Decontamination Lead Officer. Use hands free radios, stored in Paediatric ED staff area. 15. When monitoring and decontamination of patients is complete all members of the team must be monitored, remove their protective clothing and be decontaminated if necessary. This will occur within the dirty area, with a final check with a radiation monitor prior to entry into the clean area. Priorities: 1. Gather equipment required for use at triage 2. Use algorithm to determine need for decontamination 3. Use triage sieve to organise order of decontamination 109
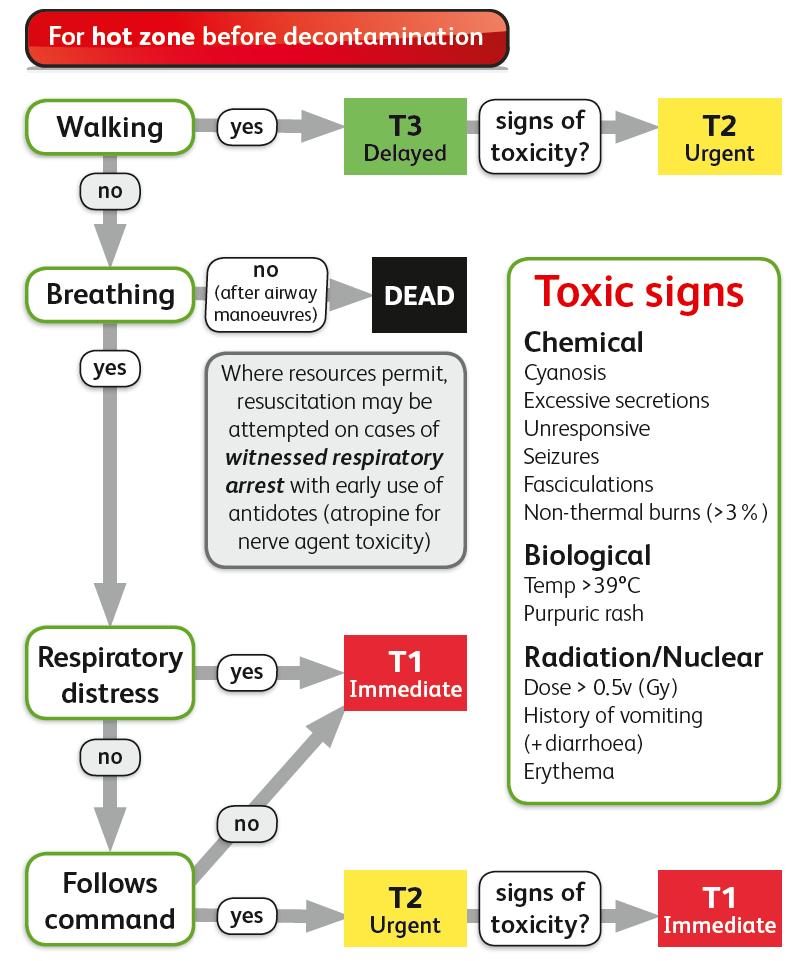
110 110
111 QEUH AND RHC Decontamination Plan Action Card 7 Staff member decontaminating patient Responsibilities: 1. Decontamination of casualties, 2. Manage and control contaminated casualties. Action: 1. Don theatre blues/greens. 2. Go to the toilet. 3. Have a soft drink. 4. Remove all jewellery. 5. Gather equipment: 2 x buckets per person, 1 filled with tepid/warm water, 1 filled with tepid/warm water and 20ml of detergent, Tuff cut scissors, Disrobe packs, Property bags, Marker pen, Sponges. 6. If time allows, deploy the decontamination unit. If time does not allow, prepare the area for use with buckets of water with 20ml detergent and sponges. (This responsibility may lie with a separate MDU team) 7. Don appropriate PPE. 8. Use hand free radio to communicate with decontamination team. Radios are stored in the staff area of the RCH ED. 9. Decontaminate patients in order that 1 st Out/Triage Officer states. 10. Instruct ambulatory patients to follow instructions for Ambulatory Rinse-Wipe-Rinse. Do not advise rinsing in a radiation contamination incident. 11. Decontaminate using the Rinse-Wipe-Rinse method, except in a radiation contamination incident where risk of splashes must be minimised, see specific instructions later on this card. 12. Communicate with Decontamination Entry Control Officer and follow their instructions. 13. Hand over decontaminated patients to clean team. Priorites: 1. If time allows deploy decontamination unit 2. Gather all equipment required 3. Decontaminate using rinse-wipe-rinse method, except in radiation incidents, see subsequent instructions. 111
112 RINSE-WIPE-RINSE PROCEDURE (N.B. Showering should be avoided in radiation contamination to avoid spread.) Equipment per person For effective application of the RINSE-WIPE-RINSE method of skin decontamination, the following is required: (i) Water, preferably warm/tepid. (ii) A bucket or other container (5 to 10 litre capacity) or a shower head with clean, preferably warm/tepid, running water. (iii) A second bucket (5 to 10 litre capacity) for use with a water (preferably warm/tepid) and detergent mix. (iv) Detergent. (v) A sponge or soft brush. Procedure 1. If walking casualties can self decontaminate then this is the best approach to take. Hospital personnel should supervise and assist as required. The recommended procedure for applying the RINSE-WIPE-RINSE method is as follows: (i) Make up a water/detergent solution of 0.5% detergent in warm/tepid water (5ml of detergent per litre of water or about three squirts of liquid detergent into a bucket of water). (ii) Having removed the contaminated person's clothes, RINSE the affected areas with clean water (no detergent) using showerheads or buckets. RINSE from the highest point downward, ensuring that any sponge or brush used does not come into contact with the casualty or their clothing. (iii) The RINSE should be applied to contaminated areas of skin only, to avoid spread to uncontaminated areas. (iv) Using the water/detergent mix detailed in point (i), WIPE the affected areas of skin with a wet sponge or soft brush. (v) RINSE the decontaminated casualty with clean warm/tepid water (no detergent) to remove the detergent and any residual chemicals. (vi) Dry the skin with a clean towel. (vii) This process should not take more than three to five minutes for an individual walking casualty. Repeat the RINSE-WIPE-RINSE procedure only if skin contamination remains obvious. (Persistent chemical warfare agents are poorly soluble in water and might require extended or repeated application.) Additional notes 2. It might not always be possible to guarantee that a casualty will be totally decontaminated at the end of this procedure. Remain cautious and observe for ill effects in the decontaminated person and in unprotected staff. 3. The rinse water itself will be contaminated, and therefore hazardous, and a source of further contamination spread. 4. Brushes and sponges used in this process will also be contaminated and should not be used on a new patient. 5. On average, stretcher casualty decontamination can take between 10 to 12 minutes to complete. 6. The risk from hypothermia should be considered when any form of decontamination is carried out. 7. The use of contamination/dose rate monitor may assist in determining if the decontamination of radio active material has been successful. Dry wipe may also be effective for radiation contamination. 112
113 Decontamination Techniques in Radiation Contamination 1. Any wounds that are not contaminated should first be protected with a waterproof dressing. 2. Contamination in wounds should be dealt with first. Following this any contamination in the nose, eyes, mouth or ears should be addressed before general decontamination of the skin is undertaken. 3. Materials used in decontamination must be collected in polythene bags for disposal as radioactive waste. Skin: Contaminated skin should be swabbed with absorbent pads dampened with mild soap and warm water. Gauze pads or small sponges may be suitable. Even a soft nail brush may be tried but damage to the outer horny layer of the skin must be avoided. The cleaning process should work from the edge of the contaminated area towards the centre. The area should be dried using disposable tissues and then monitored for residual contamination. Contaminated finger nails should be cut away as much as possible. Radioactive material lodged under or beside the nail may be removed by applying calamine lotion, which should be allowed to dry and then carefully brushed off. This procedure should be performed with the hand inside a plastic bag to avoid dispersing the powder into the atmosphere. If use of soap and water does not reduce contamination to an acceptable level, the skin may be swabbed with a solution of 1% Cetrimide and rinsed with water. A chelating agent (such as EDTA soap) may be used if advised by the Radiation Protection Adviser. A further measure that may be adopted is the application of 4% potassium permanganate solution. After a few minutes, when this is dry, the dark brown stains should be removed with 5% sodium bisulphite solution. This method should not be used on delicate skin such as the face as potassium permanganate is corrosive. Eyes: The eyes should be irrigated with sterile saline or water. Rolling back the eyelid will assist the irrigation procedures. This should only be carried out by a trained nurse or doctor. Contaminated washings should not be allowed to run into the nose, mouth or any wound. Mouth: If oral contamination is suspected, dentures should first be removed. The person should be told not to swallow and asked to wash their mouth thoroughly with repeated mouthwashes. The subjects should then be asked to brush their teeth, brushing away from the gums and carefully spitting out the water. Dentures should be scrubbed with a soft brush until free from contamination. Nose: If the nasal system is contaminated, the subjects should be asked to blow their nose into a disposable tissue, which should be collected for monitoring. If repeated nose blowing does not reduce the contamination to an acceptable level, nasal irrigation with saline or sterile water should be carried out under medical supervision. The head must be tilted forwards so that the bridge of the nasal septum is almost vertical in order that the contaminated liquid flows out of the nostril. The irrigation tube should be positioned just inside the nostril and the subject should be in a sitting position with a waterproof cover and absorbent material over their front and lap. 113
114 Ears: The opening of the ear may be cleaned with cotton swabs but caution must be exercised. If contamination has entered the ear, then trained nursing or medical staff should syringe the ears using water at body temperature. Hair: Do not shower the person if the scalp is contaminated. The person should be positioned with their head laid back over a sink and the hair washed carefully with shampoo. Care should be taken to ensure that contamination is not spread to other parts of the body especially the nose, mouth, ears and eyes. It may be necessary to wrap or cover some parts if spread of contamination cannot be avoided by other methods. The head should be dried with a clean towel and monitored to assess the level of residual contamination. If further decontamination is required, the hair may be treated with Cetrimide solution. If this still fails to remove the contamination then the hair should be trimmed, but the head must not be shaved. The clippings should be collected for assay and subsequent safe disposal. Wounds: The skin surrounding the wound should be cleaned carefully. The wound may be encouraged to bleed moderately and irrigated with sterile water to disperse the contamination, but this must not be spread to other parts of the body. The area should be dried by wiping away the liquid from the edge of the wound. Debridement of the wound may also assist the decontamination process. When the skin surrounding the wound has been decontaminated, the area should be sealed with a waterproof dressing. If fragments of radioactive metal have penetrated the wound, a wound probe may be required to assist in localisation of radioactive fragments. These should be removed with forceps, but may require surgical intervention. All fragments should be collected in plastic bags and retained for assessment. Following each decontamination attempt radiation levels must be rechecked and recorded upon Patient Decontamination body map form. It may be necessary to communicate the relevant information to a scribe with the form, via the hands free radio. When monitoring and decontamination is complete all members of the team must be monitored, remove their protective clothing and decontaminated if necessary. All staff in PPE should undergo this process in the dirty area and have a final radiation level check prior to exiting into the clean area. 114
115 QEUH AND RHC Decontamination Plan Action Card 8 Decontamination Team Members Responsibilities: 1. Decontamination of casualties, 2. Manage and control contaminated casualties. Immediate Actions: Priorities: 1. Don theatre blues/greens. 2. Go to the toilet. 3. Have a soft drink. 4. Remove all jewellery. 5. Don appropriate PPE. If respirator required, do not zip up and switch on respirator until ready to enter contaminated area or deal with potentially contaminated patients. 6. Use hand free radio from RCH ED staff area to communicate with decontamination team members. 7. Provide reassurance that decontamination will start as soon as possible for those waiting. 8. Prepare decontamination area and equipment. 9. Follow instructions of decontamination team leader. 1. Follow instructions from decontamination team leader. 115
116 QEUH AND RHC Decontamination Plan Action Card 9 Decontamination Dresser Responsibilities: 1. If required assist clean casualties in the re-robe area. 2. To assist staff in PRPS suits (who have self decontaminated) to remove protective clothing. Immediate Actions: 1. Don theatre blues/greens. 2. Go to the toilet. 3. Have a soft drink. 4. Remove all jewellery. 5. Don intermediate PPE. 6. Report to decontamination lead. 7. Ensure that there are sufficient re-robe kits for the numbers of decontaminated people coming through the unit. 8. If more re-robe kits are required inform the decontamination lead. 116
117 QEUH AND RHC Decontamination Plan Action Card 10 Emergency Department Receptionist Responsibilities: To notify Nurse in Charge of arrival at Emergency department if you are made aware of casualties that are potentially contaminated. Assign TJ numbers to casualties brought in via ambulance direct to the decontamination facility, to be used for the duration of the decontamination incident. Immediate Actions: 1. Tell potentially contaminated patient to avoid contact with other patients and remain where they are awaiting instruction. 2. Alert Nurse in Charge Emergency Department immediately. 3. Inform security. 4. Along with Nurse in Charge Emergency Department inform all persons in waiting room to vacate the area via ED front door and remain in ED drop off area for further instruction. 117
118 APPENDIX 1 MAJOR INCIDENT NOTIFICATION FORM MAJOR INCIDENT NOTIFICATION SHEET 1. TIME/DATE 2. NAME/ADDRESS OF INFORMANT 3. LOCATION OF INCIDENT 4. STATUS OF INCIDENT (POSSIBLE/CONFIRMED) 5. TIME OF INCIDENT 6. NATURE OF INCIDENT 7. POTENTIAL EXTENT OF PAEDIATRIC CASUALTIES 8. NOTES 118
119 APPENDIX 2 - SIGNPOSTING Location Sign EMERGENCY DEPARTMENT EMERGENCY DEPARTMENT Major Incident only All other casualties please report to Out Patients Department All press enquiries to Main Entrance MAIN ENTRANCE TO HOSPITAL SITE MAIN ENTRANCE TO HOSPITAL SITE Major Incident in Progress Temporary Accident and Emergency Area for all other Paediatric Casualties in Out Patients Department All press enquiries to Main Entrance EMERGENCY DEPARTMENT MAIN CORRIDOR ENTRY No Entry RADIOLOGY DEPARTMENT MAIN CORRIDOR ENTRY No Entry ON CORNER APPROACHING ED ENTRANCES Major Incident in Progress Ambulances Only Diversion for all other traffic 119
120 Location Sign Seminar Room, Emergency Department Incident Control Room Police Base Adult Emergency Department Police Control Room Training Room in Emergency Department General Services Supervisor / Senior Nurses/Press Officer 120
121 APPENDIX 3 LOCATION OF TELEPHONE CONTACT LISTS CONTACT LIST LOCATION 1. Contact Centre Contact Centre Hillington 2. Emergency Department Emergency Department Nurses Station 3. PICU PICU 4. Surgical/Orthopaedics/ENT Major Incident Box in Major Incident Store ED 5. Anaesthetics Major Incident Box in Major Incident Store ED 6. Theatres Theatre Manager s Office 7. Medical Major Incident Box in Major Incident Store ED 8. Radiology Via Rotawatch 9. Site / Facilities See Action Card Nursing Staff In SCN Office in each ward 11. Medical Records Medical Records Office / ED Reception 12. Haematology Haematology Laboratory Office 13. Biochemistry via Rotawatch 14. Pharmacy via Rotawatch For medical/surgical ward nursing staff, telephone contact lists are held / maintained locally on individual wards. It is the responsibility of Clinical Directors/Managers to ensure that up-to-date departmental telephone contact lists are maintained. It is the responsibility of Clinical Directors/Managers to ensure that up-to-date departmental telephone contact lists are provided to the Contact Centre Team Leaders. 121
122 APPENDIX 4 DESIGNATED AREA TELEPHONE NUMBERS AND MANAGEMENT NUMBERS 1. Major Incident Control Room Seminar Room, Emergency Department Police Control Room Police Base Adult Emergency Department Staff Reporting Area Han Base and adjacent Seminar Room nd Floor 4. Senior Nurses Wards 1C Ambulatory Care / D PICU / / E Cardiology / / A Oncology / Haematology / B Oncology / Haematology / C Acute Receiving / / A / / B / / C / / Psychiatry Emergency Department ED Minors Staff Base / ED Majors Staff Base / / ED Resuscitation Area Clinical Decisions Unit Staff Base / / Radiology Non Major Incident / Existing Emergency Department Patients Clinic 3 Out-Patients Department Relatives Waiting Area Therapies Hub in a paediatric incident / Adult Out Patient Department in a mixed Major Incident Patient Reunion /Discharge Area Outpatient Clinic Area Hospital Enquiry Desk Hospital Main Entrance / Main Entrance Adult Hospital
123 10. Theatre Areas Theatre Coordinator Page 8539 / ext Theatre Recovery Theatre / Theatre / Theatre / Theatre / Theatre / Theatre 6 (Emergency Theatre) / Theatre Theatre / Theatre / Cath Lab Interventional Radiology Mortuary Children s Management Team Bed manager Anne Douglas Lead Nurse Maureen Taylor / Lead Nurse Elaine Johnston Lead Nurse Melanie Hutton Lead Nurse Patricia Friel / Service Manager Lynne Robertson / Service Manager Heather Dawes / General Manager Jamie Redfern Clinical Director Phil Davies / Clinical Director Christine Gallacher Clinical Director Pam Cupples / Clinical Director Morag Campbell Chief of Medicine Alan Mathers Director Kevin Hill Facilities Management Facilities Duty Manager 7am-7pm Catering Services Manager 7am-7pm Domestic Services Department 24 hrs / / / Portering Department 24 hrs Estates Department page 7047 Emergency Duty Manager ( on call) FM General Manager Billy Hunter Site Manager Ronnie Clinton Site Manager Frank McGuire ( RCH) Deputy Site Manager Sharon Johnstone Deputy Site Manager Majorie McCulloch Deputy Site Manager Sheenagh Leighton (RCH) Professional Lead Portering Jim Magee Professional Lead Catering Jeanette Wilson / Professional Lead Domestic Pat Coyne / Duty Manager Tam Rae Duty Manager Barbara Speight
124 Duty Manager John Donaldson Duty Manager John Heron Duty Manager Adam Wright
125 APPENDIX 5 LIST OF EXTERNAL AGENCIES AND TELEPHONE NUMBERS 1. Police Scotland Headquarters 999 French Street, Dalmornock 2. Scottish Ambulance Service Emergency Medical Dispatch Centre West Caledonia House, Cardonald Park, Glasgow 3. Strathclyde Fire and Rescue Service Control Room South Thornhill, Johnstone 4. Social Work Department (Office hours) Ext: 80057/80058 Page: 8154 (Out of Hours Service) NHS Greater Glasgow and Clyde Press Officer (Office hours/out of Hours will automatically connect to Duty Officer) 6. Regional Blood Transfusion Centre Gartnavel General Hospital 7. Designated Major Incident Hospitals NHSGGC HOSPITAL CONTROL ROOM EMERGENCY DEPARTMENT Glasgow Royal Infirmary Southern General Hospital Royal Alexandra Hospital Paisley Inverclyde Hospital /2/ /

126 APPENDIX 6 Accident & Emergency Reception Registration Process Action Card Should a Major Incident take place, Health Records Accident & Emergency seniors should ensure Health Records processes for data recording are implemented. MI Patient Identifiers are as follows on Trakcare: All Major Incident patients are recorded with a unique TJ number and with the following same details: o Surname: Major Incident One (Through to Fifty) o Forename: Your site short code (i.e. VIC/SGH/IRH/RAH/ etc.) o DOB: 01/01/1901 Prior to Major Incidents Health Records Senior Staff should ensure the major incident cupboard is always fully stocked with 80 MI patient packs and packs now have all the up-to-date Major Incident patient identifiers. These should be in numerical order 1-80 Day of Major Incident Ensure a Health Records Major Incident basket is in place at reception. This basket will hold the completed MI Patient Form. This form is for Health Records use only and should not be removed from reception during the MI. Registration All patients who present during the Major Incident should be given the MI TJ number irrespective if they are identified or not. If a patient is identified (i.e. able to provide details) please update the TJ number with as many real patient details possible. Retain major Incident name as an alias. PLEASE ALWAYS RECORD THE GENDER EVEN IF THAT IS THE ONLY INFORMATION YOU HAVE. 126

127 On changing the surname & Forename you will be asked Please select OK The Major Incident surname/forename now become the alias names On updating all new details please print new patient labels and place these in the pack removing labels referring to patient name major incident Patients who are unknown i.e. where no patient details are provided will continue to be known as Major Incident one, two, three etc. Major Incident Patient Form Ensure the form has a patient label especially if you update with new details Complete as many details as possible before the patient is moved to another location Process patient details accordingly on Trak ED Reg and Move; please ensure to record MAJOR INCIDENT in the reason for attendance this will allow us to quickly identify MI patients using the ED Enquiry screen if possible record the true CHI number in the reason for attendance (time allowing) Once patient is recorded on Trak place the patient form in the Health Records MI basket 127
Inverclyde Royal Hospital Major Incident Plan. May 2016 Version 1.1
 Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
MAJOR INCIDENT PLAN Appendix and Action Cards
 MAJOR INCIDENT PLAN Appendix and Action Cards July 2012 A B Switchboard Record of Alert Call Control Centres - Site Specific Personnel C Distribution of Action Cards 1-54 D Action Cards APPENDIX A SWITCHBOARD
MAJOR INCIDENT PLAN Appendix and Action Cards July 2012 A B Switchboard Record of Alert Call Control Centres - Site Specific Personnel C Distribution of Action Cards 1-54 D Action Cards APPENDIX A SWITCHBOARD
MISSION IMMEDIATE ACTIONS RESPONSIBILITIES. Triage of patients in Emergency Centre according to protocol
 TRIAGE OFFICER Triage of patients in Emergency Centre according to protocol Get briefing from Emergency Centre Medical Commander Triage patients as they arrive, according to protocol Preparation of areas
TRIAGE OFFICER Triage of patients in Emergency Centre according to protocol Get briefing from Emergency Centre Medical Commander Triage patients as they arrive, according to protocol Preparation of areas
9.2 RESTRICTED NHS FORTH VALLEY. Major Emergency Plan
 RESTRICTED NHS FORTH VALLEY Major Emergency Plan IF A MAJOR INCIDENT HAS BEEN DECLARED DO NOT READ THIS PLAN NOW BUT REFER TO YOUR ACTION CARD Date of First Issue Circa 2004 Approved 31 / 01 / 2017 Current
RESTRICTED NHS FORTH VALLEY Major Emergency Plan IF A MAJOR INCIDENT HAS BEEN DECLARED DO NOT READ THIS PLAN NOW BUT REFER TO YOUR ACTION CARD Date of First Issue Circa 2004 Approved 31 / 01 / 2017 Current
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
REVIEW OF PAEDIATRIC INPATIENT SERVICES AT ROYAL ALEXANDRA HOSPITAL
 REVIEW OF PAEDIATRIC INPATIENT SERVICES AT ROYAL ALEXANDRA HOSPITAL 1. Introduction In 2012 there was a proposal by the Women and Children s Services Directorate to move the Paediatric Inpatient Services
REVIEW OF PAEDIATRIC INPATIENT SERVICES AT ROYAL ALEXANDRA HOSPITAL 1. Introduction In 2012 there was a proposal by the Women and Children s Services Directorate to move the Paediatric Inpatient Services
ACTION CARDS. Northern Devon Healthcare Trust. MAJOR INCIDENT PLAN: Appendix 1. Northern Devon Healthcare NHS Trust Major Incident Plan
 Northern Devon Healthcare Trust MAJOR INCIDENT PLAN: Appendix 1 ACTION CARDS NDHCT Major Incident Plan 2010 V1.1 1 Title MAJOR INCIDENT PLAN Action Cards Author Rowena Green, Divisional General Manager,
Northern Devon Healthcare Trust MAJOR INCIDENT PLAN: Appendix 1 ACTION CARDS NDHCT Major Incident Plan 2010 V1.1 1 Title MAJOR INCIDENT PLAN Action Cards Author Rowena Green, Divisional General Manager,
The impact of a flu or norovirus outbreak could have a significant impact on health and social services and could involve:
 NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
NHS GGC SGlas Campus_D.indd 1 31/03/ :06
 ESSENTIAL NHS INFORMATION ABOUT HOSPITAL CLOSURES AFFECTING YOU Key details about your brand-new South Glasgow University Hospital and new Royal Hospital for Sick Children NHS GGC SGlas Campus_D.indd 1
ESSENTIAL NHS INFORMATION ABOUT HOSPITAL CLOSURES AFFECTING YOU Key details about your brand-new South Glasgow University Hospital and new Royal Hospital for Sick Children NHS GGC SGlas Campus_D.indd 1
Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee
 The Delivery Suite Shift Co-ordinator: Roles and Responsibilities (GL819) This document forms appendix 4 of the Policy document Delivery Suite Staffing (Obstetric, Anaesthetic, Paediatric and Midwifery
The Delivery Suite Shift Co-ordinator: Roles and Responsibilities (GL819) This document forms appendix 4 of the Policy document Delivery Suite Staffing (Obstetric, Anaesthetic, Paediatric and Midwifery
NHS England South Escalation Framework
 NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
GLOSSARY. Access Overload Control (for mobile cellular radio telephones). ACCOLC
. ACCOLC") ACCOLC Ambulance control Ambulance Control Point (ACP) Ambulance Control Management Officer Ambulance Incident Commander (AIC) Ambulance Liaison Officer (ALO) Bronze control Cascade system Casualty Enquiry
ACCOLC Ambulance control Ambulance Control Point (ACP) Ambulance Control Management Officer Ambulance Incident Commander (AIC) Ambulance Liaison Officer (ALO) Bronze control Cascade system Casualty Enquiry
Number here HMIP/01 HOSPITAL MAJOR INCIDENT PLAN YSBYTY GWYNEDD
 Version: 0.1 Number here HMIP/01 HOSPITAL MAJOR INCIDENT PLAN YSBYTY GWYNEDD Date to be reviewed: July 2013 No of pages: 98 Author(s): Emma Binns Author(s) title: Business Continuity Manager Responsible
Version: 0.1 Number here HMIP/01 HOSPITAL MAJOR INCIDENT PLAN YSBYTY GWYNEDD Date to be reviewed: July 2013 No of pages: 98 Author(s): Emma Binns Author(s) title: Business Continuity Manager Responsible
Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK.
 Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK. Created: 13.9.16 Created by: Becca Robinson - Service Improvement Lead Bristol CCG Version: Draft v0.5 Last Review: Next Reviewed
Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK. Created: 13.9.16 Created by: Becca Robinson - Service Improvement Lead Bristol CCG Version: Draft v0.5 Last Review: Next Reviewed
St. Vincent s Health System Page 1 of 11. TITLE: Mass Casualty Plan Code Yellow 12/11/07 12/11/07
 St. Vincent s Health System Page 1 of 11 TITLE: Mass Casualty Plan Code Yellow FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Safety HOSPITAL SHARED POLICY? Yes No DOCUMENT NUMBER: 802 ORIGINATION
St. Vincent s Health System Page 1 of 11 TITLE: Mass Casualty Plan Code Yellow FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Safety HOSPITAL SHARED POLICY? Yes No DOCUMENT NUMBER: 802 ORIGINATION
NAME SPECIALTY PLEASE NOTE THAT THE CONSULTANT SURGEONS RUN A 4 WEEK ROLLING ROTA OF ACTIVITY. (HENCE THE 'BUSY' JOB PLAN)
") CONSULTANT CONTRACT JOB PLAN NAME SPECIALTY PLEASE NOTE THIS IS INTENDED AS A GUIDE ONLY. AN FORMAL JOB PLAN WILL BE DEVISED WITH THE SUCCESFUL CANDIDATE TO TAKE ACCOUNT OF PERSONAL INTERESTS AND SPECIALTY
CONSULTANT CONTRACT JOB PLAN NAME SPECIALTY PLEASE NOTE THIS IS INTENDED AS A GUIDE ONLY. AN FORMAL JOB PLAN WILL BE DEVISED WITH THE SUCCESFUL CANDIDATE TO TAKE ACCOUNT OF PERSONAL INTERESTS AND SPECIALTY
Unannounced Theatre Inspection Report
 Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Unannounced Follow-up Inspection Report
 Unannounced Follow-up Inspection Report Queen Elizabeth University Hospital NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in
Unannounced Follow-up Inspection Report Queen Elizabeth University Hospital NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in
UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN. Managing and Recovering from Major Incidents
 UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN Managing and Recovering from Major Incidents June 2017 MAJOR INCIDENT PLAN - June 2017 Title Primary author (name and title) UCL Major Incident Plan (public
UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN Managing and Recovering from Major Incidents June 2017 MAJOR INCIDENT PLAN - June 2017 Title Primary author (name and title) UCL Major Incident Plan (public
Infectious Diseases Protocol
 Infectious Diseases Protocol 1. The purpose of this document 1.1 This document outlines the response procedures that should be followed in cases where a member of the University is suspected or confirmed
Infectious Diseases Protocol 1. The purpose of this document 1.1 This document outlines the response procedures that should be followed in cases where a member of the University is suspected or confirmed
41 EC Emergency Planning Toolkit Action Cards
 41 EC Emergency Planning Toolkit Action Cards Policy number: 41 EC Version 2.1 Approved by Name of author/originator Owner (director) Executive Director Date of approval August 2014 Samantha Chalmers,
41 EC Emergency Planning Toolkit Action Cards Policy number: 41 EC Version 2.1 Approved by Name of author/originator Owner (director) Executive Director Date of approval August 2014 Samantha Chalmers,
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
SUP 08 Operational procedures for Medical Gas Pipeline Systems (MGPS) Unified procedures for use within NHS Scotland
 Unified procedures for use within NHS Scotland") SUP 08 Operational procedures for Medical Gas Pipeline Systems (MGPS) Unified procedures for use within NHS Scotland May 2015 Contents Page Acknowledgements... 4 Introduction... 5 1. Aim and scope... 6
SUP 08 Operational procedures for Medical Gas Pipeline Systems (MGPS) Unified procedures for use within NHS Scotland May 2015 Contents Page Acknowledgements... 4 Introduction... 5 1. Aim and scope... 6
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services
 It is essential to follow the EQIA Guidance in completing this form NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services Name of Current Service/Service Development/Service
It is essential to follow the EQIA Guidance in completing this form NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services Name of Current Service/Service Development/Service
Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010
 Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Register No: Status: Public on ratification
 Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
Patient Transfer Policy
 Patient Transfer Policy Policy Title: Executive Summary: Patient Transfer Policy All patients within East Cheshire NHS Trust that require transfer from one area to another either internally or externally
Patient Transfer Policy Policy Title: Executive Summary: Patient Transfer Policy All patients within East Cheshire NHS Trust that require transfer from one area to another either internally or externally
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE
 DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
JOB DESCRIPTION. Specialist Practitioner of Transfusion for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:-
 JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
Report to the Board of Directors 2015/16
 Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
HEALTH CARE PROFESSIONAL (HCP) ADMISSIONS
 ADMISSIONS") HEALTH CARE PROFESSIONAL (HCP) ADMISSIONS Information Booklet Contents Page No Content 1 Index 2 Introduction What is a HCP Admission? 3 Booking Transport Who is authorised to book HCP Admissions? Who
HEALTH CARE PROFESSIONAL (HCP) ADMISSIONS Information Booklet Contents Page No Content 1 Index 2 Introduction What is a HCP Admission? 3 Booking Transport Who is authorised to book HCP Admissions? Who
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
Policy for Clinical Supervision of Temporary or Locum Members of Junior Paediatric Medical Staff
 Policy for Clinical Supervision of Temporary or Locum Members of Junior Paediatric Medical Department / Service: Paediatrics Originator: Dr Andrew Gallagher Accountable Director: Dr Andrew Gallagher Approved
Policy for Clinical Supervision of Temporary or Locum Members of Junior Paediatric Medical Department / Service: Paediatrics Originator: Dr Andrew Gallagher Accountable Director: Dr Andrew Gallagher Approved
EMERGENCY PRESSURES ESCALATION PROCEDURES
 OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
SAFE CARE. Scottish Patient Safety Programme. SPSP Adult Acute
 SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
Unannounced Inspection Report
 Unannounced Inspection Report Stobhill Hospital Glasgow Royal Infirmary NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April
Unannounced Inspection Report Stobhill Hospital Glasgow Royal Infirmary NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April
Process and definitions for the daily situation report web form
 Process and definitions for the daily situation report web form November 2017 The daily situation report (sitrep) indicates where there are pressures on the NHS around the country in areas such as breaches
Process and definitions for the daily situation report web form November 2017 The daily situation report (sitrep) indicates where there are pressures on the NHS around the country in areas such as breaches
SUBJECT: Medical Staffing Update Report 1. PURPOSE
 Meeting of Lanarkshire NHS Board: Wednesday 25 March 2015 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk SUBJECT: Medical Staffing Update
Meeting of Lanarkshire NHS Board: Wednesday 25 March 2015 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk SUBJECT: Medical Staffing Update
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation
 Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE
 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE") NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services
 It is essential to follow the EQIA Guidance in completing this form Name of Current Service/Service Development/Service Redesign: Radiology Department at Glasgow Royal Infirmary NHS Greater Glasgow and
It is essential to follow the EQIA Guidance in completing this form Name of Current Service/Service Development/Service Redesign: Radiology Department at Glasgow Royal Infirmary NHS Greater Glasgow and
DOCUMENT TITLE: MAJOR INCIDENT PLAN. Version: V2.2. Date of Final Ratification: 15 th May 2017 Name of Ratifying Committee: Review Date: November 2019
 MAJOR INCIDENT PLAN DOCUMENT TITLE: MAJOR INCIDENT PLAN Originator/Author /Designation & Specialty: Sharon Walford - Emergency Planning & Capacity manager Director Lead: Paul Bytheway Chief Operating Officer
MAJOR INCIDENT PLAN DOCUMENT TITLE: MAJOR INCIDENT PLAN Originator/Author /Designation & Specialty: Sharon Walford - Emergency Planning & Capacity manager Director Lead: Paul Bytheway Chief Operating Officer
Severe Weather Plan V5.5 March 2018
 V5.5 March 2018 Table of Contents 1. Introduction 3 2. Purpose of this Plan. 3 3. Scope. 3 4. Ownership and Responsibilities. 3 5. Escalation Levels and Actions 5 6. Staffing Contingency and Guidance.
V5.5 March 2018 Table of Contents 1. Introduction 3 2. Purpose of this Plan. 3 3. Scope. 3 4. Ownership and Responsibilities. 3 5. Escalation Levels and Actions 5 6. Staffing Contingency and Guidance.
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and
 Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
POSITION DESCRIPTION. Position title: CSSD Supervisor Workflow processes
 POSITION DESCRIPTION Position title: CSSD Supervisor Workflow processes Date Produced/Reviewed: June 2014 Position Holder's Name: Position Holder's Signature:... Line Manager s Name: Line Manager s Signature:...
POSITION DESCRIPTION Position title: CSSD Supervisor Workflow processes Date Produced/Reviewed: June 2014 Position Holder's Name: Position Holder's Signature:... Line Manager s Name: Line Manager s Signature:...
PLANNED CARE THEATRE OPERATIONAL POLICY
 PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
REGISTERED NURSE Cohort Recruitment Band 5 Regional Sector
 REGISTERED NURSE Cohort Recruitment Band 5 Regional Sector Job Reference: 0000050985N Closing Date: 30 th March 2018 Dear applicant, Thank you for your interest in working for NHS Greater Glasgow and Clyde
REGISTERED NURSE Cohort Recruitment Band 5 Regional Sector Job Reference: 0000050985N Closing Date: 30 th March 2018 Dear applicant, Thank you for your interest in working for NHS Greater Glasgow and Clyde
NWL Pathology. Preparing Haematology and Blood Transfusion lab for a Major incident. Lorry Phelan MBE Site Manager Blood Sciences
 NWL Pathology Preparing Haematology and Blood Transfusion lab for a Major incident Lorry Phelan MBE Site Manager Blood Sciences NWL Pathology Definition of a major incident: A major incident or emergency
NWL Pathology Preparing Haematology and Blood Transfusion lab for a Major incident Lorry Phelan MBE Site Manager Blood Sciences NWL Pathology Definition of a major incident: A major incident or emergency
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
Board of Directors Meeting
 Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN
 CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN 12/13/2017 Fire Service, Emergency Management Division Schedule A to By-law 2017-236 Page 1 CONTENTS 1. INTRODUCTION... 3 2. PURPOSE... 3 3. SCOPE... 3
CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN 12/13/2017 Fire Service, Emergency Management Division Schedule A to By-law 2017-236 Page 1 CONTENTS 1. INTRODUCTION... 3 2. PURPOSE... 3 3. SCOPE... 3
ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline
 ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline 1.1. This guidance is designed to aid staff to monitor capacity and staffing in Child Health. 2. The Guidance 2.1. The majority
ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline 1.1. This guidance is designed to aid staff to monitor capacity and staffing in Child Health. 2. The Guidance 2.1. The majority
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
2. Scope. 3. Purpose
 1. Introduction This policy is developed to provide clear operational guidance for Escalation within UL Hospitals group. The policy describes the escalation status; bed capacity and Emergency Department(ED)
1. Introduction This policy is developed to provide clear operational guidance for Escalation within UL Hospitals group. The policy describes the escalation status; bed capacity and Emergency Department(ED)
Quality Indicator Local Use of Data
 Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
St. James s Hospital, Dublin.
 Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Safe staffing for nursing in A&E departments. NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015
 Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
ACUTE CARE BUSINESS UNIT THEATRE OPERATIONAL POLICY
 ACUTE CARE BUSINESS UNIT THEATRE OPERATIONAL POLICY Review date: October 2017 Mr U Khan : Clinical Director Mrs G Bird : Directorate Manager Critical Care Mr M Cawley : Theatre Manager Theatre Operational
ACUTE CARE BUSINESS UNIT THEATRE OPERATIONAL POLICY Review date: October 2017 Mr U Khan : Clinical Director Mrs G Bird : Directorate Manager Critical Care Mr M Cawley : Theatre Manager Theatre Operational
POSITION DESCRIPTION/RUN DESCRIPTION
 POSITION DESCRIPTION/RUN DESCRIPTION POSITION TITLE: FIRST YEAR HOUSE OFFICER DEPARTMENT/SERVICE: WHANGANUI HOSPITAL REPORTS TO: HEAD OF DEPARTMENT RESIDENT MEDICAL OFFICERS SPECIALIST CONSULTANT OF ASSIGNED
POSITION DESCRIPTION/RUN DESCRIPTION POSITION TITLE: FIRST YEAR HOUSE OFFICER DEPARTMENT/SERVICE: WHANGANUI HOSPITAL REPORTS TO: HEAD OF DEPARTMENT RESIDENT MEDICAL OFFICERS SPECIALIST CONSULTANT OF ASSIGNED
ADVANCED NURSE PRACTITIONER STRATEGY
 ADVANCED NURSE PRACTITIONER STRATEGY 2016-2020 Lead Manager: Chair, GG&C Advanced Practice Group Responsible Director: Board Nurse Director Approved by: NMAHP Group Date approved Date for review: September
ADVANCED NURSE PRACTITIONER STRATEGY 2016-2020 Lead Manager: Chair, GG&C Advanced Practice Group Responsible Director: Board Nurse Director Approved by: NMAHP Group Date approved Date for review: September
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Patient Flow Internal Escalation
 Trust Policy and Procedure Document Ref. No: PP(15) 304 Policy Name Internal Escalation For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff Trust Wide ECOO
Trust Policy and Procedure Document Ref. No: PP(15) 304 Policy Name Internal Escalation For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff Trust Wide ECOO
NHS Commissioning Board Core Standards for Emergency Preparedness, Resilience and Response (EPRR)
") NHS Commissioning Board NHS Commissioning Board Core Standards for Emergency Core Standards for Emergency Preparedness, Resilience and Preparedness, Resilience and Response (EPRR) Response (EPRR) 1 P a
NHS Commissioning Board NHS Commissioning Board Core Standards for Emergency Core Standards for Emergency Preparedness, Resilience and Preparedness, Resilience and Response (EPRR) Response (EPRR) 1 P a
Intensive Psychiatric Care Units
 NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
Paediatric Escalation Policy
 Paediatric Escalation Policy Specialty: Paediatrics Approval Body: WCH Quality and Safety Group Approval Date: 21 st January 2015 Date of Review: December 2018 PAEDIATRIC SERVICES ESCALATION POLICY FOR
Paediatric Escalation Policy Specialty: Paediatrics Approval Body: WCH Quality and Safety Group Approval Date: 21 st January 2015 Date of Review: December 2018 PAEDIATRIC SERVICES ESCALATION POLICY FOR
CARE DELIVERY TEAM NURSING GUIDELINES
 STANDARDS TO BE MET Team nursing is a model of care which utilises the resources within a nursing team on a shift by shift basis to deliver safe patient care within the clinical unit. The Bay of Plenty
STANDARDS TO BE MET Team nursing is a model of care which utilises the resources within a nursing team on a shift by shift basis to deliver safe patient care within the clinical unit. The Bay of Plenty
MAJOR INCIDENT RESPONSE
 HELICOPTER OPERATING PROCEDURE MAJOR INCIDENT RESPONSE HOP No: C/17 Issued: April 2012 Page: 1 of 7 Revision No: TRIM No: 09/300 Document No: D12/6739 Distribution: Sydney x Illawarra x Orange x Helicopter
HELICOPTER OPERATING PROCEDURE MAJOR INCIDENT RESPONSE HOP No: C/17 Issued: April 2012 Page: 1 of 7 Revision No: TRIM No: 09/300 Document No: D12/6739 Distribution: Sydney x Illawarra x Orange x Helicopter
REGISTERED NURSE Cohort Recruitment Band 5 Women & Children s Sector, Obstetrics and Gynaecology
 REGISTERED NURSE Cohort Recruitment Band 5 Women & Children s Sector, Obstetrics and Gynaecology Job Reference: 0000051650N Closing Date: 26 th July 2018 Dear applicant, Thank you for your interest in
REGISTERED NURSE Cohort Recruitment Band 5 Women & Children s Sector, Obstetrics and Gynaecology Job Reference: 0000051650N Closing Date: 26 th July 2018 Dear applicant, Thank you for your interest in
JOB DESCRIPTION NHS GREATER GLASGOW & CLYDE
 JOB DESCRIPTION NHS GREATER GLASGOW & CLYDE 1. JOB DETAILS Job Title: Managerially Responsible to: Professionally Responsible to: Services: Location: Head of Nursing, Neonatal, Children and Young People
JOB DESCRIPTION NHS GREATER GLASGOW & CLYDE 1. JOB DETAILS Job Title: Managerially Responsible to: Professionally Responsible to: Services: Location: Head of Nursing, Neonatal, Children and Young People
ACF(M)15/03 Minutes: GREATER GLASGOW AND CLYDE NHS BOARD
15/03 Minutes: GREATER GLASGOW AND CLYDE NHS BOARD") ACF(M)15/03 Minutes: 22-33 GREATER GLASGOW AND CLYDE NHS BOARD Minutes of a Meeting of the Area Clinical Forum held in Meeting Room A, J B Russell House, Corporate Headquarters, Gartnavel Royal Hospital,
ACF(M)15/03 Minutes: 22-33 GREATER GLASGOW AND CLYDE NHS BOARD Minutes of a Meeting of the Area Clinical Forum held in Meeting Room A, J B Russell House, Corporate Headquarters, Gartnavel Royal Hospital,
TRUST BOARD SEPTEMBER Surgical Services Reconfiguration
 def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON WEDNESDAY 20 TH JUNE 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST K EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON WEDNESDAY 20 TH JUNE 2012 Subject Supporting TEG Member Author Status 1 Emergency Preparedness,
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST K EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON WEDNESDAY 20 TH JUNE 2012 Subject Supporting TEG Member Author Status 1 Emergency Preparedness,
BUSINESS CONTINUITY PLAN
 BUSINESS CONTINUITY PLAN Version 1.4 Name of Director Lead Marie Price Name of author Lisa Wood Date issued September 2016 Review date October 2017 Target audience All BHR CCGs Staff To be read in conjunction
BUSINESS CONTINUITY PLAN Version 1.4 Name of Director Lead Marie Price Name of author Lisa Wood Date issued September 2016 Review date October 2017 Target audience All BHR CCGs Staff To be read in conjunction
Burton Hospitals NHS Foundation Trust. On: 24 October Review Date: October Corporate / Directorate. Clinical / Non Clinical
 POLICY DOCUMENT Burton Hospitals NHS Foundation Trust DISCHARGE POLICY Approved by: Trust Executive Committee On: 24 October 2017 Review Date: October 2020 Corporate / Directorate Clinical / Non Clinical
POLICY DOCUMENT Burton Hospitals NHS Foundation Trust DISCHARGE POLICY Approved by: Trust Executive Committee On: 24 October 2017 Review Date: October 2020 Corporate / Directorate Clinical / Non Clinical
Changes to Inpatient Disability Services in Clyde
 Changes to Inpatient Disability Services in Clyde Your chance to comment on the proposals This document explains proposed new arrangements for providing specialist inpatient physical disability services,
Changes to Inpatient Disability Services in Clyde Your chance to comment on the proposals This document explains proposed new arrangements for providing specialist inpatient physical disability services,
REVIEW OF WEST GLASGOW MINOR INJURIES SERVICES OPTION APPRAISAL INFORMATION
 REVIEW OF WEST GLASGOW MINOR INJURIES SERVICES OPTION APPRAISAL INFORMATION August 2017 1 CONTENTS Option appraisal process 3 Option appraisal flow chart 5 Options 6 Benefits criteria 7 Option appraisal
REVIEW OF WEST GLASGOW MINOR INJURIES SERVICES OPTION APPRAISAL INFORMATION August 2017 1 CONTENTS Option appraisal process 3 Option appraisal flow chart 5 Options 6 Benefits criteria 7 Option appraisal
NHS LANCASHIRE NORTH CCG MAJOR INCIDENT PLAN
 Agenda Item 12.0. NHS LANCASHIRE NORTH CCG MAJOR INCIDENT PLAN Version 2 Page 1 of 24 Version Control Version Reason for Date of Update by: Accountable NHS update update Emergency LNCCG Officer sign Governing
Agenda Item 12.0. NHS LANCASHIRE NORTH CCG MAJOR INCIDENT PLAN Version 2 Page 1 of 24 Version Control Version Reason for Date of Update by: Accountable NHS update update Emergency LNCCG Officer sign Governing
DISCHARGE LOUNGE OPERATIONAL GUIDELINES
 DISCHARGE LOUNGE OPERATIONAL GUIDELINES March 2014 Perfect Week Discharge Lounge Pilot Monday 24 th March 2014- Friday 4 th April 2014 Author: Acting Deputy Director of Operations Document Review date:
DISCHARGE LOUNGE OPERATIONAL GUIDELINES March 2014 Perfect Week Discharge Lounge Pilot Monday 24 th March 2014- Friday 4 th April 2014 Author: Acting Deputy Director of Operations Document Review date:
Membership and Public Engagement. Frequently Asked Questions
 Membership and Public Engagement Frequently Asked Questions Parking 1) Where can I park when visiting/attending the Central Site and Trafford Hospital sites? Central Site Grafton Street and Hathersage
Membership and Public Engagement Frequently Asked Questions Parking 1) Where can I park when visiting/attending the Central Site and Trafford Hospital sites? Central Site Grafton Street and Hathersage
62 days from referral with urgent suspected cancer to initiation of treatment
 Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
Unannounced Inspection Report. Aberdeen Maternity Hospital NHS Grampian. 9 October 2013
 Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
5.3: POLICY FOR THE MANAGEMENT OF REQUESTS FOR MEDICINES VIA PEER APPROVED CLINICAL SYSTEM (PACS) TIER 2
 TIER 2") NHS GREATER GLASGOW AND CLYDE POLICIES RELATING TO THE MANAGEMENT OF MEDICINES SECTION 5: NON-FORMULARY PROCESSES 5.3: POLICY FOR THE MANAGEMENT OF REQUESTS FOR MEDICINES VIA PEER APPROVED CLINICAL SYSTEM
NHS GREATER GLASGOW AND CLYDE POLICIES RELATING TO THE MANAGEMENT OF MEDICINES SECTION 5: NON-FORMULARY PROCESSES 5.3: POLICY FOR THE MANAGEMENT OF REQUESTS FOR MEDICINES VIA PEER APPROVED CLINICAL SYSTEM
Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian
 Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian Lead Author/Coordinator: Jeff Horn / Sarah Howlett Macmillan Haematology CNS/ Pharmacist Reviewer: Gavin Preston Consultant Haematologist
Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian Lead Author/Coordinator: Jeff Horn / Sarah Howlett Macmillan Haematology CNS/ Pharmacist Reviewer: Gavin Preston Consultant Haematologist
INVERCLYDE COMMUNITY HEALTH AND CARE PARTNERSHIP - DRAFT SCHEME OF ESTABLISHMENT
 EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
Incident Management Plan
 Incident Management Plan Document Control Version 2 Name of Document NHS Guildford and Waverley CCG Incident Management Plan Version Date 1st October 2016 Owner Director of Governance and Compliance [Accountable
Incident Management Plan Document Control Version 2 Name of Document NHS Guildford and Waverley CCG Incident Management Plan Version Date 1st October 2016 Owner Director of Governance and Compliance [Accountable
Borders NHS Board. Appendix NHS BORDERS 2012/13 WINTER PERIOD REPORT. Aim
 Borders NHS Board NHS BORDERS 2012/13 WINTER PERIOD REPORT Aim To update the Board on key activity relating to the 2012/13 winter period, specifically focussing on the festive period from 17 December to
Borders NHS Board NHS BORDERS 2012/13 WINTER PERIOD REPORT Aim To update the Board on key activity relating to the 2012/13 winter period, specifically focussing on the festive period from 17 December to
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool for Frontline Patient Services
 NHS Greater Glasgow and Clyde Equality Impact Assessment Tool for Frontline Patient Services Equality Impact Assessment is a legal requirement and may be used as evidence for referred cases regarding legislative
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool for Frontline Patient Services Equality Impact Assessment is a legal requirement and may be used as evidence for referred cases regarding legislative
Seven Day Working: in Practice Clinicians Perspective. Jonathan Vickers Consultant surgeon Dec 2015
 Seven Day Working: in Practice Clinicians Perspective Jonathan Vickers Consultant surgeon Dec 2015 Why me? Mr. Hunt argued that hospitals like Salford Royal and Northumbria have instituted seven-day working
Seven Day Working: in Practice Clinicians Perspective Jonathan Vickers Consultant surgeon Dec 2015 Why me? Mr. Hunt argued that hospitals like Salford Royal and Northumbria have instituted seven-day working
Barnes-Jewish Hospital Perioperative Services
 Page 1 of 13 Barnes-Jewish Hospital Perioperative Services TITLE: Perioperative Services Disaster Response Plan SUBMITTED/REVIEWED BY: Julie Nash, Trauma Services Manager David Watkins, Manager, Clinical
Page 1 of 13 Barnes-Jewish Hospital Perioperative Services TITLE: Perioperative Services Disaster Response Plan SUBMITTED/REVIEWED BY: Julie Nash, Trauma Services Manager David Watkins, Manager, Clinical
JOB DESCRIPTION. Pre-Assessment Senior Nurse. Band: Band 6. Pre-Assessment Team Leader. 1 Job Summary
 JOB DESCRIPTION Job Title: Pre-Assessment Senior Nurse Band: Band 6 Division / Department: Hours: Reports to: Accountable to: Perioperative Services 37.5 Hrs per week Pre-Assessment Team Leader Theatre
JOB DESCRIPTION Job Title: Pre-Assessment Senior Nurse Band: Band 6 Division / Department: Hours: Reports to: Accountable to: Perioperative Services 37.5 Hrs per week Pre-Assessment Team Leader Theatre
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national