PDPM Payment Model Dan Ciolek Associate Vice President, Therapy Advocacy American Health Care Association
|
|
|
- Charleen Craig
- 5 years ago
- Views:
Transcription
1 PDPM Payment Model Dan Ciolek Associate Vice President, Therapy Advocacy American Health Care Association
2 Agenda PDPM 101 Full version webinar on AHCA website Why PDPM is replacing RUGs on 10/1/2019 Overview of the PDPM Case-mix payment model PDPM payment drivers & impacts Getting Ready for PDPM Introduction to AHCA s PDPM Core Competencies AHCA Member Support Activities & Resources Questions or Suggestions PDPM@ahca.org
3 Why PDPM is replacing RUGs Implementation - October 1, 2019 (FY 2020)

4 DHHS/CMS Position on PDPM The PDPM would be a significant shift in how SNFs are paid and, we believe, a very positive one. It reflects our belief that we should not be paying providers in ways that drive overuse of services. Instead, we should pay providers based on the patients they treat, while assessing quality fairly. Secretary Alex M. Azar, Secretary of Health and Human Services, AHCA/NCAL Congressional Briefing. June 4, 2018
5 IMPACT Act of 2014 Outlined Intention of Creating Payment Systems Driven by Patient Characteristics The IMPACT Act requires standardized patient assessment data across post-acute care (PAC) settings to enable: Improvements in quality of care and outcomes Comparisons of quality across PAC settings Transparency in data reporting Information exchange across PAC settings Enhanced care transitions and coordinated care Person-centered and goals-driven care planning and discharge planning Payment modeling based on individual characteristics SNF PDPM, SNF QRP, and SNF VBP all advance the goals of the IMPACT Act


6 Primary Driver for Change: Therapy Utilization Bias RU: 57% days RU/RV 86% dollars
7 CMS Used a Payment Reform Framework CMS Framework Element Basis for Payment System Development Remain within Existing Statutory Authority Average Per Diem Payment Use Existing Data Develop a Readily Implementable System October 1, 2019 Shifts Away from Therapy as Basis for Payment Cost Report Data Claims, MDS 2006 Nursing Research Remains in Per Diem Builds on Existing Tools MDS, Claims Payment based on Patient Characteristics Minutes only Counted at Discharge
8 Overview of the PDPM Case-mix payment model
9 SNF Responsibilities That Remain Under PDPM SNF Responsibilities Need for Daily Skilled Care Nursing 7d and/or Therapy 5-7d Requirements of Participation Survey & Certification Annual Payment Rate Update Consolidated Billing SNF Quality Programs SNF Action Steps Maintain a Comprehensive Person-Centered Plan of Care Therapy & nursing delivery must align with patients needs Continue to Monitor for NPRM Payment Updates CMS will monitor quality of care and related outcomes
10 PDPM Replaces RUG-IV on October 1, 2019 Current RUG-IV Model 1. Payment is primarily determined by number of therapy minutes 2. Does not fully consider wide range of clinical characteristics that influence the relative resource use of SNF residents CMS Outlines Benefits of New Payment Model PDPM Criteria Removes therapy minutes as basis for payment Intended to enhance payment accuracy for therapy, nursing, NTA services by making payment dependent on a wide range of clinical characteristics Rather than primarily a function of therapy minutes/adl present in >90% of RUG days Intended to improve targeting of resources to beneficiaries with diverse care needs Designed to provide more equitable resources to facilities treating vulnerable populations Therapy minutes drive payment Patient characteristics drive payment



11 Important Features of PDPM Per Diem Payment *Budget-neutral Therapy Minutes No Longer Drive Payment Total Therapy Capped at 25% for Group and Concurrent Combined Admission Assessment Patient Characteristics Drive Payment Admission/IPA MDS Coding Timing & Accuracy Add Risk Key PDPM features impact all areas of operations and care delivery
12 Fewer Assessments Required Under PDPM RUG-IV Assessments RUG-IV Day 5 MDS Day 30 MDS Therapy OMRAs Day 90 MDS Day 14 MDS Day 60 MDS Discharge MDS PDPM Assessments 1. Elimination of RUGs MDS Schedule 2. Elimination of Other Medicare Required Assessment (OMRA) Day 5 MDS Discharge MDS with Therapy Codes PDPM OPTIONAL Interim Payment Assessment
13 PDPM Is Still a Per-diem Payment Model But Components Are Changed RUGs Therapy Non-Case-Mix Therapy Nursing Non-Case-Mix PDPM PT OT SLP Nursing NTAS Non-Case-Mix
14 PDPM Adds Variable Per-Diem Payment Adjustments PT PT Base Rate PT CMI PT Adjustment Factor OT OT Base Rate OT CMI OT Adjustment Factor SLP Nursing NTA SLP Base Rate Nursing Base Rate NTA Base Rate SLP CMI Nursing CMI NTA CMI NTA Adjustment Factor PDPM includes variable per-diem payment adjustments that modify payment based on changes in utilization of these services over a stay Non-Case Mix Non-Case-Mix Base Rate *RUGs HIV/AIDS add-on is replaced in PDPM with new 18% nursing component base rate adjustor and new NTA CMI factors (not shown)

15 - NEW - Variable Per-Diem Day 4 - NTAS rates drop 2/3 Day 21 and every 7 days after - PT and OT rates drop 2% Interim Payment Assessment Optional Variable Payments Do Not Reset to Day-One

 assigned for each component Patient characteristics for")
16 PDPM Admission Processes Are Critical Accuracy with Diagnosis & Coding Impact Payments and Compliance Risk Hospital Discharges Typical discharge information sufficient Surgery information not PCS codes for Section J2000 SNF Admits SNF clinician diagnoses Admission MDS assessment timing and accuracy MDS coordinator codes based on MDS items & ICD-10 codes PT OT SLP Nursing NTAS Payment Classification Case-Mix Group (CMG) assigned for each component Patient characteristics for component CMGs differ
17 Two New Provisions May Impact CMGs and Payment Rates: (1) Interim Payment Assessment (IPA) SNF Determines Triggering Event Does not return tapering to day-1 for PT/OT or NTAS While optional still requires monitoring Unclear how captured on claim Day 5 MDS CMG Changes Variable Per Diem Schedule Continues Optional IPA Discharge MDS

18 Two New Provisions May Impact CMGs and Payment Rates: (2) Interrupted Stay Policy Heightened CMS Scrutiny No new admission assessment If </= 3 days can use IPA New admission assessment required if away >3 days Does return to day day-1 PT/OT/NTAS tapering SNF VBP Impacts?
19 Therapy Time No Longer Impacts Payments But Must Still Be Reported Therapy services are only to be reported on SNF PPS discharge MDS The following PT/OT/SLP service delivery items are to be reported separately by discipline Start and end dates Total treatment days during entire stay Total individual 1:1 therapy minutes during entire stay Total concurrent therapy minutes during entire stay Total group therapy minutes during entire stay There is a 25% limit on the total amount of concurrent and or group therapy permitted per stay within each discipline CMS will issue a non-fatal warning edit on validation report if limit surpassed CMS will monitor and flag providers for audits, and revise policy if abused Focus is on Person- Centered Care and Care Planning
20 Other PDPM Considerations Many PDPM MDS items also impact SNF QRP 101 MDS items impact SNF QRP 2% adjustment for reporting How providers implement new PDPM IPA and Interrupted-Stay policies may impact SNF VBP hospital readmission ratings Uncertainty regarding whether, or how quickly, Medicaid, Medicare Advantage, ACO Conveners, CJR Bundle Holders, or other payers will transition to PDPM
21 PDPM Payment Drivers
22 Many More MDS Items Impact PDPM than Under RUGs Under RUGs Over 90% of resident days reported via Rehab RUGs Rehab RUG rates determined by 20 MDS item fields Therapy minutes/days 12 items ADLs 8 items Under PDPM All PDPM component rates independently determined 161 MDS item fields PT 14 MDS items OT 14 MDS items SLP 33 MDS items Nursing 129 MDS items NTAS 33 MDS items
23 PDPM Has More Case-Mix Adjusted Payment Components than RUGs Current RUG-IV Payment Model* Patient Driven Payment Model (PDPM)** Therapy Base Rate Therapy CMI PT PT Base Rate PT CMI PT Adjustment Factor Therapy O R Non-Case Mix Therapy Base Rate OT OT Base Rate OT CMI OT Adjustment Factor SLP SLP Base Rate SLP CMI Nursing Nursing Base Rate Nursing CMI Nursing Nursing Base Rate Nursing CMI Non- Case-Mix Non-Case-Mix Base Rate NTA NTA Base Rate NTA CMI NTA Adjustment Factor *Hierarchical CMG assignment in RUGs favors therapy Non- Case Mix Non-Case-Mix Base Rate **Independent CMG assignment for each PDPM component
24 Federal Unadjusted PDPM Component Base Rates FY 2019 estimate
25 PT and OT Component Drivers Primary reason for SNF care ICD-10-CM code Type of inpatient surgery Function* 4 functional score ranges 4 clinical categories 16 payment groups each *10 MDS Section GG items must be assessed days 1-3 (before treatment started)

26 PT/OT Classification Groups & Case-Mix Weights
27 SLP Component Drivers Primary reason for SNF care Presence of acute neurologic condition ICD-10 code SLP comorbidities MDS checklist & ICD-10 codes Cognitive impairment Mechanically altered diet Swallowing disorder 4 categories based on number of elements 3 categories based on number of elements 12 payment groups
28 SLP Classification Groups & Case-Mix Weights
29 Nursing Component Drivers Extensive Services Clinical Conditions Adjustors Depression Restorative nursing* Function** 3 base service categories 5 base clinical categories Used to modify extensive services and clinical conditions 25 payment groups * Restorative nursing requires a minimum of 6 days in a 7-day lookback (may impact ARD selection) ** 7 MDS Section GG items must be assessed days 1-3 (before treatment started)
30 Nursing Classification Groups & Case-Mix Weights

31 Nursing Classification Groups & Case-Mix Weights
32 NTAS Component Drivers High NTAS cost conditions High NTAS cost extensive services 6 payment groups Qualifying conditions and services assigned points: Sum of points for all conditions or services present will fall into one of 6 point ranges

33 Higher Point Value NTAS Conditions/Extensive Services (of 50)
34 Great! But what does that mean to my revenue?
35 PDPM Shifts Payment to Patients with Complex Clinical Needs Resident Population: $ Increase Residents who are dually enrolled Residents with longer prior inpatient stay Residents with complications in MS-DRG Residents who have high NTA costs & comorbidities Residents who receive extensive services (e.g., trach, ventilator) Residents who use IV medication Clinical categories: acute infections, cardiovascular, pulmonary, non-orthopedic surgery Vulnerable subpopulations: residents with addictions, bleeding disorders, behavioral issues, chronic neurological conditions, and bariatric care Residents whose most common therapy level is RU Residents with fewer comorbidities Longer SNF LOS Resident Population: $ Decrease
36 Example Resident Clinical Profile Admitted with stroke MDS Section G ADL score of 9 MDS Section GG function nursing score = 7, PT/OT score = 10 Moderate cognitive impairment Receives daily PT, OT, SLP = 730 minutes/week Resource-intensive nursing dialysis, IV meds, mechanically modified diet Comorbidities diabetes
37 Example Resident RUGs vs PDPM Drivers Resident Characteristics Resident A Details Rehab Received Yes Therapy Minutes 730 Extensive Services No ADL Score 9 PT, OT, and SLP Clinical Category Acute Neurologic PT and OT Function Score 10 SLP Cognitive Impairment Moderate SLP Mechanically Altered Diet Yes Nursing Serious Medical Conditions Dialysis Nursing Function Score 7 NTAS Condition/Extensive Services Score 7 (IV meds, diabetes) RUB RUG category determinants PDPM payment driver characteristics
38 Example Resident - RUGs Rate RUG Rate Calculation for RUB FY 2019 (Urban) Component Base Fed Rate Case-Mix Index Payment (per diem) Therapy $ x 1.87 = $ Non-case-mix therapy NA for RUB x = $0 Nursing $ x 1.56 = $ $ per diem x 30 day stay = $18, Non-case-mix nursing $92.63 x = $92.63 Total = $631.25
39 Example Resident - PDPM (Day 1-3) Component Base Fed Rate Case-Mix Index Special Adjustors Variable per diem Payment (per diem) PT $59.33 x 1.55 x x 1.00 = $91.96 OT $55.23 x 1.55 x x 1.00 = $85.61 SLP $22.15 x 2.85 x x = $63.13 NTA $78.05 x 1.85 x x 3.00 = $ Nursing $ x 1.43 x 1.00* x = $ Non-Case-Mix Component $92.63 x x x = $92.63 Total = $914.60* *Except when resident has HIV/AIDS, then variable per diem adjustment = 1.18 Note: Rates are for urban facilities, CMS estimated if program went into effect FY19 *PDPM per-diem days 1-3 = $ *RUGs per-diem all days = $631.25
40 Example Resident PDPM 30 Days Day 1-3 => 3 $ = $2, Day 4-20 => 17 $ = $10, Day => 7 $ = $4, Day => 3 $ = $1, Total = $19, Reminder: RUGs per-diem was $ and 30 day total was $18,937.50

41 Examples of PDPM stumbling blocks This Photo by Unknown Author is licensed under CC BY-SA-NC
42 What happens to my payment if I miss entering an MDS item that is a key driver of a PDPM payment component?
43 Example Resident: What happens to NTA casemix if the MDS IV medication item is not entered Failing to identify or incorrectly coding just one PDPM payment driver MDS item can have a significant impact on CMI *resident has 2 NTA points for diabetes
44 Example Resident 30 Day Stay RUGs PDPM PDPM (missing data) Days RUG-IV Per Diem Rate PDPM With Accurate MDS PDPM With Missing MDS IV Meds Data 1-3 $ $ $ $ $ $ $ $ $ $ $ $ Day Total $18, $19, $17,089.44
45 What happens if I don t pay attention to length of stay?
46 Example Resident - PDPM (Day ) Component Base Fed Rate Case-Mix Index Special Adjustors Variable per diem Payment (per diem) PT $59.33 x 1.55 x x 0.76 = $69.89 OT $55.23 x 1.55 x x 0.76 = $65.07 SLP $22.15 x 2.85 x x = $63.13 NTA $78.05 x 1.85 x x 1.00 = $ Nursing $ x 1.43 x 1.00* x = $ Non-Case-Mix Component $92.63 x x x = $92.63 Total = $583.41* *Except when resident has HIV/AIDS, then variable per diem adjustment = 1.18 Note: Rates are for urban facilities, CMS estimated if program went into effect FY19 *PDPM per-diem days 1-3 = $ *RUGs per-diem all days = $631.25

47 Per-Diem Rate Example resident full 100 day stay $950 $900 $850 $800 $750 $700 $650 $600 $550 $500 RUG-IV Correct PDPM MDS PDPM MDS Missing IV Meds
48 Getting Ready for PDPM & AHCA Resources
49 What Can Go Wrong If You Are Not Prepared for PDPM? If you deliver care that is not patient motivated or according to clinical needs, If you do not enter MDS and Claim information correctly, If you do not have appropriate staffing for case mix, If you do not optimize staffing and contracting resources appropriately, Audits Incorrect Payment/Audits Lower Quality Outcomes Budget Errors and Margin Shortfall! Your organization s compliance, quality, payment, and margins at risk
50 AHCA Membership Support Strategy in Transformational Era Rationale for Arriving at AHCA PDPM Readiness Toolbox & Core Competencies Therapy Driven Hierarchical CMG Assignment Clinical Coding Does Not Impact Payment RUGs Model Going Away PDPM Fundamentally Different Move Away from Therapy Minutes Clinical Care Management Focus Clinical Assessment & Coding Critical for Payment New Payment Drivers Clinical Information Collection Staff Role Changes Infrastructure Technology, Data and Vendor Relations AHCA PDPM Readiness Toolbox to Prepare for PDPM

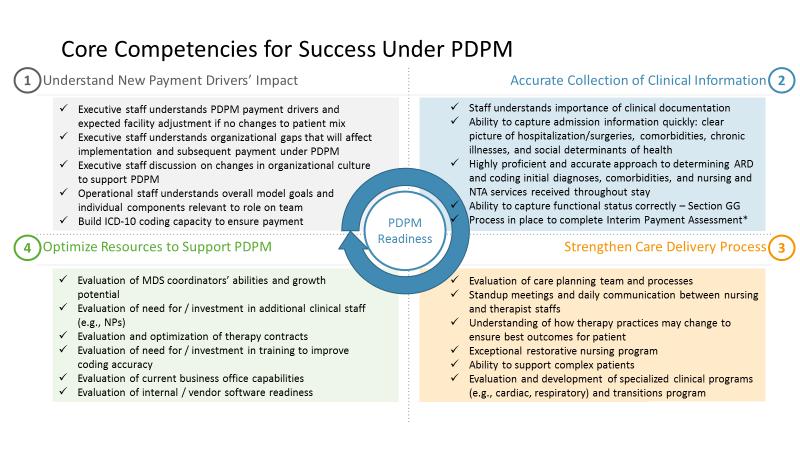
51 AHCA PDPM Readiness Tool & PDPM Core Competencies PDPM Analysis and Contractor Retained Member Interviews SNFs can be successful under PDPM, Four categories of must do s which AHCA refers to as the PDPM Core Competencies Resource Development AHCA PDPM Readiness Review Toolkit & Core Competencies to help members assess their current RUG-based operations Aid with determining what changes are needed to be successful under PDPM
52 Four Keys to Success Under PDPM
53 What To Be Doing Now Educate yourself about the new system Develop accurate diagnostic and MDS coding capabilities Evaluate and strengthen your ability to manage complex patients Align resources 53
54 1 Educate yourself about the new system 1. Download the AHCA PDPM Core Competencies and other tools 2. Attend AHCA webinars 3. Be able to answer these questions: What drives payment under the new system? What are my organization s operational and clinical gaps? What capabilities do I need to build or add? 54
55 2 Develop accurate diagnostic and MDS coding capabilities 1. Evaluate accuracy of current documentation for clinical diagnoses and ICD-10 codes 2. Develop plan for accurate and rapid collection of full clinical picture 3. Ensure organizational ability to accurately capture ICD-10 codes 4. Improve ability to accurately complete MDS, particularly section GG 55
56 3 Evaluate and strengthen your ability to manage complex patients 1. Enhance care planning capabilities and ability to substantiate 2. Evaluate who needs to be on the care team and how the team will communicate 3. Consider repurposing MDS coordinators to be care coordinators 4. Assess your ability to deliver NTA services and clinical care that addresses complex needs 56
57 4 Align resources 1. Adjust therapy contracts 2. Review technology needs 3. Consider hiring and training for new clinical capabilities 57
58 58
59 PDPM Next Steps AHCA Member Support Activities & Resources

60 CMS Schedule for PDPM Changes and Updates

61 Readiness Toolkit and Core Competencies Updates FY20 Notice of Proposed Rulemaking FY20 Final Rule Other PDPM Academy Toolkits AHCA PDPM MDS Accuracy Toolkit AHCA PDPM Hospital Discharge Toolkit AHCA PDPM Case-Mix Grouper Simulator Toolkit AHCA PDPM Compliance Guide and Best Practice Model Policies Toolkit AHCA PDPM Model Job Descriptions Toolkit AHCA PDPM Therapy Staffing/Contracting Considerations Toolkit Face to Face & Virtual PDPM Training Opportunities ICD-10 Virtual Training for AHCA Members State-by-State One-Day PDPM Workshops Monthly PDPM Webinars Webinars on How to Use PDPM Toolkits
62 Getting Started Form Interdisciplinary Team Download AHCA PDPM Readiness & Core Competencies Toolkit Develop Work Plan Based on Readiness Toolkit

63 Additional Questions or Suggestions address for questions AHCA PDPM Resource Center for updates, links, FAQs, and upcoming PDPM Academy educational offerings at: y_operations/medicare/pages/ PDPM-Resource-Center.aspx
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
Patient-Driven Payment Model
 Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Objectives 9/18/2018. Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018
 Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018") Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
2/20/2018. Resident Classification System RCS-1. CMS Proposal
 Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Goodbye PPS: Hello RCS!
 Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
The Shift is ON! Goodbye PPS, Hello RCS
 The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
SNF proposed rule revisions to case-mix methodology
 SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I ZIMMET HEALTHCARE 2018
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM)
") What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM) Presented by: Robin L. Hillier, CPA, STNA, LNHA, RAC-MT robin@rlh-consulting.com (330) 807-2850 PDPM Overview
What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM) Presented by: Robin L. Hillier, CPA, STNA, LNHA, RAC-MT robin@rlh-consulting.com (330) 807-2850 PDPM Overview
6/12/2017. The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group
 The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
CMS (Medicare), Patient Driven Payment Model PDPM. Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation
, Patient Driven Payment Model PDPM. Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation") CMS (Medicare), Patient Driven Payment Model PDPM Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation What is it? PDPM Released in Final Rule 7-31-18 Effective 10-1-19 Patient
CMS (Medicare), Patient Driven Payment Model PDPM Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation What is it? PDPM Released in Final Rule 7-31-18 Effective 10-1-19 Patient
& Reward. Opportunity, Risk. HealthPRO Heritage National healthcare solutions firm specializing in Care ReDesign for top of market clients 9/5/2018
 Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
June 26, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 RE: CMS 1696 Medicare Program; Prospective Payment
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 RE: CMS 1696 Medicare Program; Prospective Payment
Patient Driven Payment Model 101
 Patient Driven Payment Model 101 MARK MCDAVID, OTR, RAC-CT Presented by Why a New Payment Model? MedPAC has raised concerns about: Provider advantage Payment inequities for different patient types Patient
Patient Driven Payment Model 101 MARK MCDAVID, OTR, RAC-CT Presented by Why a New Payment Model? MedPAC has raised concerns about: Provider advantage Payment inequities for different patient types Patient
Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP
 Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP Objectives: What is RCS-1? Why the proposed change in payment system? Differences between RCS-1 and current PPS
Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP Objectives: What is RCS-1? Why the proposed change in payment system? Differences between RCS-1 and current PPS
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
CMS Requirements of Participation Facility Assessment
 HEALTHCARE I N S I G H T S May 2017 THE NEWSLETTER FROM LOEB & TROPER FOR NURSING HOMES AND HOME CARE AGENCIES CONTENTS CMS Requirements of Participation Facility Assessment Managed Care Contracts and
HEALTHCARE I N S I G H T S May 2017 THE NEWSLETTER FROM LOEB & TROPER FOR NURSING HOMES AND HOME CARE AGENCIES CONTENTS CMS Requirements of Participation Facility Assessment Managed Care Contracts and
Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD
 June 26, 2018 Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD 21244-1850 Re: CMS-1696-P Medicare Program; Prospective
June 26, 2018 Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD 21244-1850 Re: CMS-1696-P Medicare Program; Prospective
Pitch Perfect: Selling Your Services to LTC Facilities
 Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
June 22, Submitted electronically
 June 22, 2018 Seema Verma, MPH Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G Attn: CMS-1696-P Hubert Humphrey Building 200 Independence Ave,
June 22, 2018 Seema Verma, MPH Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G Attn: CMS-1696-P Hubert Humphrey Building 200 Independence Ave,
Development of Updated Models of Non-Therapy Ancillary Costs
 Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis
 Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis Part I: Update to the SNF VBP and QRP Programs Part II: Payment Updates Part III: Patient-Driven
Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis Part I: Update to the SNF VBP and QRP Programs Part II: Payment Updates Part III: Patient-Driven
Equalizing Medicare Payments for Select Patients in IRFs and SNFs
 Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Understanding the PEPPER
 Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
Fiscal Year 2014 Final Rule: Updates for LTCHs
 Fiscal Year 2014 Final Rule: Updates for LTCHs Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Mary Dalrymple Managing Director, LTRAX FY14 Final Rule & Impact Objectives Review updates to the FY14
Fiscal Year 2014 Final Rule: Updates for LTCHs Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Mary Dalrymple Managing Director, LTRAX FY14 Final Rule & Impact Objectives Review updates to the FY14
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
National Association for the Support of Long Term Care
 Seema Verma, Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW Washington, D.C. 20201
Seema Verma, Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW Washington, D.C. 20201
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
RCS-1. (Resident Classification System-Version 1) New Medicare payment system: What to Expect!
 New Medicare payment system: What to Expect!") RCS-1 (Resident Classification System-Version 1) New Medicare payment system: What to Expect! Presented by: Patricia J. Boyer Director of Clinical Services Wipfli LLP Wipfli LLP 10000 Innovation Drive,
RCS-1 (Resident Classification System-Version 1) New Medicare payment system: What to Expect! Presented by: Patricia J. Boyer Director of Clinical Services Wipfli LLP Wipfli LLP 10000 Innovation Drive,
Medicare Program; Prospective Payment System and Consolidated Billing for Skilled. AGENCY: Centers for Medicare & Medicaid Services (CMS), HHS.
, HHS.") This document is scheduled to be published in the Federal Register on 05/04/2017 and available online at https://federalregister.gov/d/2017-08519, and on FDsys.gov DEPARTMENT OF HEALTH
This document is scheduled to be published in the Federal Register on 05/04/2017 and available online at https://federalregister.gov/d/2017-08519, and on FDsys.gov DEPARTMENT OF HEALTH
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Proposed fy17 LTCH PPS: New rules for Quality & Referrals
 Proposed fy17 LTCH PPS: New rules for Quality & Referrals Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives Describe updates to the LTCH
Proposed fy17 LTCH PPS: New rules for Quality & Referrals Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives Describe updates to the LTCH
Outcomes Measurement in Long-Term Care (LTC)
") ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
What is CDI? 2016 HTH FL Boot Camp. HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race
 Race") HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Global Budget Revenue. October 8, 2015
 Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
IMAGES & ASSOCIATES O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT
 O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT The Prospective Payment System (PPS) for Inpatient Rehabilitation Facilities creates both opportunities and challenges for facilities that provide comprehensive
O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT The Prospective Payment System (PPS) for Inpatient Rehabilitation Facilities creates both opportunities and challenges for facilities that provide comprehensive
Medicare Inpatient Psychiatric Facility Prospective Payment System
 Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM
 MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM PAYMENT RULE BRIEF PROPOSED RULE Program Year: FFY 2019 OVERVIEW AND RESOURCES The Centers for Medicare & Medicaid Services released the
MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM PAYMENT RULE BRIEF PROPOSED RULE Program Year: FFY 2019 OVERVIEW AND RESOURCES The Centers for Medicare & Medicaid Services released the
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Value Based Purchasing 101. About Matt. Learning Objectives. Harmony Healthcare International (HHI)
") Value Based Purchasing 101 Matt Mc Garvey, MBA, VP of Business Development Harmony Healthcare International (HHI) We C.A.R.E. About Care Version 6.21.17 About Matt As Vice President of Business Development
Value Based Purchasing 101 Matt Mc Garvey, MBA, VP of Business Development Harmony Healthcare International (HHI) We C.A.R.E. About Care Version 6.21.17 About Matt As Vice President of Business Development
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT SEPTEMBER 2011 MELBOURNE, AUSTRALIA
 HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT 20 23 SEPTEMBER 2011 MELBOURNE, AUSTRALIA INTRODUCTION AND APPLICATION OF A CODING QUALITY TOOL PICQ JOE BERRY OPERATIONS AND PROJECT MANAGER, PAVILION HEALTH
HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT 20 23 SEPTEMBER 2011 MELBOURNE, AUSTRALIA INTRODUCTION AND APPLICATION OF A CODING QUALITY TOOL PICQ JOE BERRY OPERATIONS AND PROJECT MANAGER, PAVILION HEALTH
MANAGED CARE IS HERE
 MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
The Home Health Groupings Model (HHGM)
") The Home Health Groupings Model (HHGM) September 5, 017 PRESENTED BY: Al Dobson, Ph.D. PREPARED BY: Al Dobson, Ph.D., Alex Hartzman, M.P.A, M.P.H., Kimberly Rhodes, M.A., Sarmistha Pal, Ph.D., Sung Kim,
The Home Health Groupings Model (HHGM) September 5, 017 PRESENTED BY: Al Dobson, Ph.D. PREPARED BY: Al Dobson, Ph.D., Alex Hartzman, M.P.A, M.P.H., Kimberly Rhodes, M.A., Sarmistha Pal, Ph.D., Sung Kim,
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS)
") CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
January 10, Glenn M. Hackbarth, J.D Hunnell Road Bend, OR Dear Mr. Hackbarth:
 Glenn M. Hackbarth, J.D. 64275 Hunnell Road Bend, OR 97701 Dear Mr. Hackbarth: The Medicare Payment Advisory Commission (MedPAC or the Commission) will vote next week on payment recommendations for fiscal
Glenn M. Hackbarth, J.D. 64275 Hunnell Road Bend, OR 97701 Dear Mr. Hackbarth: The Medicare Payment Advisory Commission (MedPAC or the Commission) will vote next week on payment recommendations for fiscal
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm
 Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm Lisa Lyons Executive Director St. Josephs John Knox John M. Hehn, Jr. Executive Director Florida Presbyterian
Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm Lisa Lyons Executive Director St. Josephs John Knox John M. Hehn, Jr. Executive Director Florida Presbyterian
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10
 UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Objectives. Assisted Living. O 2 : Opportunities & Outcomes in Assisted Living. Presented by: Chief Clinical Officer
 O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
Proposed Rule Summary. Medicare Inpatient Psychiatric Facility Prospective Payment System: Federal Fiscal Year 2015
 Proposed Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Federal Fiscal Year 2015 June 2014 Table of Contents Overview and Resources 1 IPF Payment Rates 1 Effect of Sequestration
Proposed Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Federal Fiscal Year 2015 June 2014 Table of Contents Overview and Resources 1 IPF Payment Rates 1 Effect of Sequestration
Payment Rule Summary. Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013
 Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
2018 UDSmr Webinar Series
 May 17, 2:00 p.m. 3:15 p.m. Eastern Summary of the FY 2019 Proposed Rule FREE for subscribers, $79 for nonsubscribers This session will review CMS s FY 2019 proposed rule and highlight IRF PPS changes
May 17, 2:00 p.m. 3:15 p.m. Eastern Summary of the FY 2019 Proposed Rule FREE for subscribers, $79 for nonsubscribers This session will review CMS s FY 2019 proposed rule and highlight IRF PPS changes
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW
 MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Disclosure of Proprietary Interest
 HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Episode Payment Models Final Rule & Analysis
 Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Introduction 4/7/2015
 The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
Interdisciplinary Rehabilitation for Stroke
 Interdisciplinary Rehabilitation for Stroke Jessica Berry, MD Natasa Miljkovic, MD, PhD Antonette Murphy, RN, BSN, Clinician Kelly Vitti, PT, GCS, NCS Role of the PM&R Physician Consultation in acute care
Interdisciplinary Rehabilitation for Stroke Jessica Berry, MD Natasa Miljkovic, MD, PhD Antonette Murphy, RN, BSN, Clinician Kelly Vitti, PT, GCS, NCS Role of the PM&R Physician Consultation in acute care
Creating Value Based Home Health Programs for Improved Outcomes
 Creating Value Based Home Health Programs for Improved Outcomes HHSM Executive Clinical Director Melissa Couty BSN HH National Clinical Director HHSM Progressive HH Clinical/Operations Firm Founded by
Creating Value Based Home Health Programs for Improved Outcomes HHSM Executive Clinical Director Melissa Couty BSN HH National Clinical Director HHSM Progressive HH Clinical/Operations Firm Founded by
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance
 PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home