Spreading the success to an entire nation: tools for a successful Care Transitions project
|
|
|
- Conrad Norris
- 5 years ago
- Views:
Transcription
1 Spreading the success to an entire nation: tools for a successful Care Transitions project Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care This material was prepared by CFMC (PM CO 2012), the Medicare Quality Improvement Organization for Colorado under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy.
2 Objectives Outline the essential processes & milestones for a successful initiative Describe the need for impactful measurement strategies Display examples from around the nation 2
3
4 Every component is necessary 1. Expertise in an individual area, 2. Experts from different areas coming together to address a specific problem, but 3. Backbone Organization/Group is critical: Common agenda Common measures Structured collaboration 4

5 Community Coalition Building Information about Intervention Models Social Network Analysis Strategic Plan Develop and Formalize a Charter 5
6 Personal Narrative Strong commitment to the relationships Thanks to Marshall Ganz, NOI, OfH and others
7 En
8 Creating shared relational commitment Relationship as Interest Common Interests New Interests Interests Interests Resources Resources New Resources Common Resources Relationship as Resource

9 9 Creating shared structure

10 The roadmap again
11 A blown-up roadmap Root cause analysis What the intervention strategy should target What to measure Interventions The right intervention for the right target Who gets it, how much of it they get Measure What happens when the intervention reaches its intended target 11
12 Purpose of the Root Cause Analysis (RCA) Identify the root cause of readmissions within your community Identify patterns of readmissions specific to your community and its providers Use RCA results to guide targeting criteria and intervention selection 12
13 Community-Specific Root Cause Analysis Patient/family interviews Care coordinator interviews Medical record reviews Data Analysis Process mapping Cause-and-effect diagrams 5 Whys 13
14 Patient/Family Interviews Semi-structured telephone or face-to-face interviews with patients who were readmitted Helps to identify opportunities for improvement from the patient s perspective 14
15 Care Coordinator Interviews Conduct individual and/or group interviews with care coordinators Identify patterns, trends, and opportunities for improvement from the staff member s perspective Formulate groups across settings or within provider teams, organizations, or specialties 15
16 Medical Record Reviews Review randomly sampled hospital discharges and 30-day readmissions. Common finding: Patient education is completed and documented, but patients need more in-depth understanding to be compliant 16
17 Process Mapping Clarify specific roles and contributions of those involved in the process Observe discharge and admission processes directly, interview process owners, and map the processes Elicit staff perceptions about where communication issues and gaps may occur 17
18 Cause-and-Effect Diagram (Fishbone Diagram) Visually illustrates potential causes of high readmissions 18
19 5 Whys This is simple and easy to complete without statistical analysis. Start with asking why readmissions occur at your hospital and record the answer. If the answer provided does not directly identify the root cause of your readmissions problem, ask why again and record the answer. Continue this process until your team agrees the problem s root cause has been identified. 19
20 5 Whys Example Why are so many Medicare beneficiaries with heart failure being readmitted to our hospital? Because they do not understand or remember the red flags related to their condition after discharge. Why do they not understand the red flags? They do not have the correct documentation or reminder systems in place. 20
 or red flag magnet with")

21 5 Whys Example (cont d) Why do they not have the proper documentation or reminders? Because they did not receive a Personal Health Record (PHR) or red flag magnet with documentation of these red flags upon discharge. Why did they not receive the PHR or magnet? Distribution of these materials is not part of the current discharge process. 21
22 Building a Community-based Program Root Cause Analysis Did Intervention Address Driver ID Driver of Readmission Measure Intervention Select Intervention
23 Results from the community-specific root cause analysis Existing local programs and resources Funding resources Cost estimates of intervention implementation Estimates for intervention penetration Sustainability Intervention Selection & Implementation Plan Community preferences 23
24 Intervention Measurement Strategies Involves both process and outcome Measures Providers and CBOs collect most Process data QIOs can help link Outcome Measures from Medicare claims to interventions QIOs can create time series control charts to show intervention progress and to monitor potential effects
25 Suggested approach 1. Map out a detailed, community-level logic model of the intervention strategy. 2. Select and operationalize outcomes and processes from the logic model. 3. Develop and enforce the system for tracking implementation and outcome. 4. Effectively report time series data.
26 Logic model Visual representation, roadmap How a program is expected to work Context of the real world where the program is implemented Conceptual Utilized in program planning, management, evaluation and communication
27 Logic model components Inputs Resources, contributing factors Outputs Activities (interventions) Participation (processes) Outcomes Short-, medium, and long-term Assumptions External factors






28
29 Logic Model Outcomes Short-, medium-, and long-term changes and improvements Short-term Specific improvements in the targeted driver or root cause Medium-term Related outcomes along the causal path Long-term Improved care transitions Avoided readmission Improved health care utilization Implications of potential negative changes or non-changes
30 A few ideas CTI a) Pre- vs. post-coaching patient activation b) % coached patients with increased patient activation c) % coached patients who achieve 30-day health goal RED a) Percentage of RED patients reporting no problems at telephone follow-up b) Care Transitions Measure (CTM) BOOST a) Pre- vs. post-implementation patient satisfaction with discharge b) Rate of discharge summaries completed w/in 48h or discharge. INTERACT a) Pre- vs. post-implementation detection of acute change in condition using early warning and/or communication tools (re: "Stop and Watch" and care paths) 30
31 Business case for measurement Facilitate rapid cycle improvement See indicators of immediate, ground-level effect Make efficient, informed program decisions Do it without onerous data collection Leverage what s already being collected Incorporate new data elements into existing processes Demonstrate program effectiveness Tell the real story How people actually benefitted from the intervention That a goal was set and reached 31
32 Guiding the discussion What is the goal of the intervention? Are there multiple goals? How will you know the goal was achieved? Are there several observable components? What data would you need to show it? Is it something already being collected? Could you insert new data elements into an existing work process? How burdensome would it be to collect entirely new data? Who would be responsible? 32
33 Guiding the discussion, cont d What would improvement look like? A score or rate that changes over time People who get the intervention have a better outcome than those who don t People are better off after getting the intervention, compared to before getting it How large of a change would be needed to confidently say that improvement occurred? Over what time frame should this happen? 33

34 Aiming for SMART-ness SMART objectives dial in the measurement strategy Specific Measureable Quantify the amount of change expected. Provide a reference point for measuring change. Achievable Realistic Time-phased 34
35 Intervention How often did it happen? Process measure = number of times intervention occurred Is the intervention working? Interim/Proximal Outcome measure = Number of times the intervention did what it was intended to do Are we getting the expected outcome? Final Utilization measure = readmissions/1000 in the entire target population Is it enough to make a difference? Proximal Utilization Outcome measure = Utilization among those receiving the intervention
36 Let s see some real examples Examples of intervention measurement strategies Long-term outcomes Short-term outcomes Process / Reach measures Success stories Interim QIO Data 36

37 Lateral Cluster: 30day hospital readmission rate from SNFs in Harlingen
38 Short Term (% of HF patients who can TeachBack) 120 Percentage of CHF patients Who Can Teachback R² = Intervention began March Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12
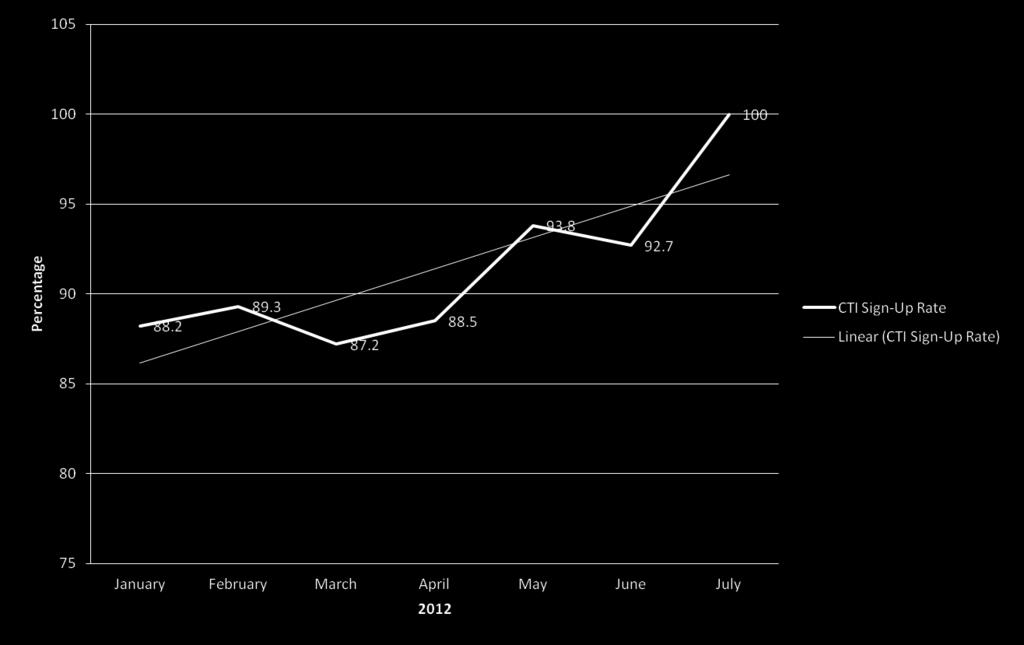
39 CTI Reach Process /Reach (CTI) Patient Referral Acceptance Percent 100.0% 90.0% 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% Completion Rates among Accepted Cases 39
40 A FEW STORIES OF SUCCESS ACROSS THE COUNTRY 40

41 41 Washington County, Rhode Island
42 Washington County, Rhode Island Intervention Send a complete communication document at the time of patient transfer (Transfer information sheet with reason for ER visit, current medication list, face sheet-demographics, DOB,PCP, Insurance, Emergency Contact, IC, Advance Directives) # Beneficiaries Touched 630 Schedule outpatient follow-up appointment prior to discharge 2600 Provide PCP with summary clinical information at discharge 2600
43 Percent of Patients with Communication Form that is 100% Complete 120% 100% 80% 88% 90% 77% 78% 75% 83% 92% 98% 86% 94% R² = % 60% 40% 20% 0% Feb 12 Mar 12 Apr 12 May 12 Jun 12 Jul 12 Aug 12 Sep 12 Oct 12 Nov 12 Dec 12
44 % Percent of Patients who have MD Appt Booked at Discharge
45 % Percent of patients whose summary info is provided to PCP
46 12.7%* 31.1%* * compared to


47 47 Lufkin, TX
48 Lufkin, Texas Intervention # Beneficiaries Touched Follow Up Appointment Scheduled for CHF Patients 151 Follow Up Appointments Scheduled for CHF, AMI, and PNE patients 190 Patient Education: Use of CHF Zone tool for CHF patients 50
49 Follow-up Appointments Scheduled for CHF Patients 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 75.0% 63.6% (12) 54.5% (7) (6) 43.8% 33.3% 40.0% (7) 30.8% 27.2% (3) (4) 27.8% (4) 20.0% 20.0% (3) (5) 12.5% (2) (2) (2) n=11 n=9 n=13 n=16 n=18 n=10 n=16 n=10 n=11 n=11 n=10 n=16 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12
50 30-day Readmission for CHF Patients 50.0% 40.0% 44.4% 30.0% 20.0% 10.0% 7.7% 16.7% 13.6% 0.0% Aug-12 Sep-12 Oct-12 Nov-12 Dec-12
51 Follow-up Appointments for CHF, AMI, PNE Patients 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 52.6% (10) 52.4% 40.0% (4) 57.7% (15) (11) 50.0% (5) 40.0% 40.0% (6) (6) 33.3% (7) 27.3% 26.3% (3) (5) n=19 n=10 n=21 n=15 n=21 n=26 n=11 n=19 n=15 n=10 n= % (10) Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12
52 8.9%* 5.3%* * compared to

53 53 San Francisco, CA
54 The San Francisco Transitional Care Program Intervention # Beneficiaries Touched Care Transitions Intervention (CTI) 201 Enrollment for In-Home Support Services (IHSS) 90 Provision of Meal Services 45 Provision of Transportation Services 26
55 CTI Enrollment Rate
56 In-home Support Services Enrollment Rate

57 Meal Services Enrollment Rate
58 5.5%* 13.3%* * compared to

59 59 The State of Montana

60 The State of Montana
61 Billings, Great Falls, Missoula-Rivalli, MT Community Intervention # Beneficiaries Touched Missoula/Ravalli Care Transitions Intervention (CTI) 661 Billings Check In 600 Billings Community coalition engagement intervention strategy ~2600 Billings End of Life Culture Change ~100 s Great Falls Safe Landing 89
62 % Accepting Check In % % 91.30% 93.10% 96.97% % 80.00% 82.35% 60.00% % Accepting Check In 40.00% Expon. (% Accepting Check In) 20.00% 0.00% Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Aug-12 Sep-12 Oct-12 Nov Dec % Accepting Check In 91.30% 82.35% 93.10% 96.97% % 62
63 Billings Level of Coalition Development Baseline 12/1/2011 Jun 2012 Jul 2012 Aug 2012 Oct
64 End of Life Culture Change Stage of development of Provider Education Tool Baldrige ADLI Linear (Stage of development of Provider Education Tool Baldrige ADLI)
65 Statewide Measures 7.6%* 15.2%* * compared to
66 Wisdom from A. Einstein Learn from yesterday, live for today, hope for tomorrow. The important thing is to not stop questioning. Not everything that counts can be counted, and not everything that can be counted counts If we knew what it was we were doing, it would not be called research, would it? Logic will get you from A to Z; imagination will get you everywhere.
67 Questions? Kimberly Irby, MPH Program Manager National Coordinating Center (NCC) Colorado Foundation for Medical Care (CFMC) Phone: x3026 If you want to go quickly, go alone. If you want to go far, go together. -African proverb
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Telligen. Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016
 Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Patient Safety in Ambulatory Care: Why Reporting Counts. August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH
 Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
3/24/2016. Value of Quality Management. Quality Management in Senior Housing: Back to the Basics. Objectives. Defining Quality
 Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Laguna Honda Lean Transformation. Laguna Honda Strategic Performance Management November 2017
 Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
thequalitypost in this issue Get Out of Your Comfort Zone Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone
 thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study
 Case Study") Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Compliance Division Staff Report
 Compliance Division Staff Report Polygraph Advisory Board Meeting Tuesday, September 26, 2017 Public Outreach Compliance Division routinely attends annual industry meetings held by TALEPI (Texas Association
Compliance Division Staff Report Polygraph Advisory Board Meeting Tuesday, September 26, 2017 Public Outreach Compliance Division routinely attends annual industry meetings held by TALEPI (Texas Association
TCLHIN Standardized Discharge Summary
 TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
Combining Nursing Power and Quality Metrics to Influence Policy Development
 Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY Introduction
 COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
UHF Quality Institute. Patient-Reported Outcomes in Primary Care New York PROPC-NY. Module 2 Webinar
 UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
Advancing Popula/on Health and Consumerism
 Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Avoiding the Cap Trap What Every Hospice Needs to Know. Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc.
 Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
HSAG the QIN-QIO NHQCC II and CDI Initiative Kick-off
 (HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
(HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes
 Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
National Trends Winter 2016
 National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
BOROUGH OF ROSELLE PUBLIC NOTICE ANNUAL NOTICE OF CALENDAR YEAR 2018 WORKSHOP SESSIONS, PRE-AGENDA MEETINGS AND REGULAR MEETINGS
 BOROUGH OF ROSELLE PUBLIC NOTICE ANNUAL NOTICE OF CALENDAR YEAR 2018 WORKSHOP SESSIONS, PRE-AGENDA MEETINGS AND REGULAR MEETINGS BE IT RESOLVED, by the Mayor and Borough Council of the Borough of Roselle,
BOROUGH OF ROSELLE PUBLIC NOTICE ANNUAL NOTICE OF CALENDAR YEAR 2018 WORKSHOP SESSIONS, PRE-AGENDA MEETINGS AND REGULAR MEETINGS BE IT RESOLVED, by the Mayor and Borough Council of the Borough of Roselle,
AI/AN Long Term Care Conference. Chronic Disease Management Through. Home Telehealth Monitoring. May 2, 2010 IHS. VA US Air Force US Army US Navy
 AI/AN Long Term Care Conference Chronic Disease Management Through Home Telehealth Monitoring May 2, 2010 Briefers: David T. Peters ANMC ANTHC IHS USCG VA US Air Force US Army US Navy Legal Authority --
AI/AN Long Term Care Conference Chronic Disease Management Through Home Telehealth Monitoring May 2, 2010 Briefers: David T. Peters ANMC ANTHC IHS USCG VA US Air Force US Army US Navy Legal Authority --
CHC-A Continuity Dashboard. All Sites Continuity - Asthma. 2nd Qtr-03. 2nd Qtr-04. 2nd Qtr-06. 4th Qtr-03. 4th Qtr-06. 3rd Qtr-04.
 PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
Performance Improvement Projects (PIP) Clinic May 13, 2016
 Clinic May 13, 2016") Behavioral Health Concepts, Inc. Performance Improvement Projects (PIP) Clinic May 13, 2016 Amy McCurry Schwartz, Esq., MHSA California EQRO Consultant OMB Approval No. 0938-0786 EQR PROTOCOL 3: VALIDATING
Behavioral Health Concepts, Inc. Performance Improvement Projects (PIP) Clinic May 13, 2016 Amy McCurry Schwartz, Esq., MHSA California EQRO Consultant OMB Approval No. 0938-0786 EQR PROTOCOL 3: VALIDATING
Discharge and Follow-Up Planning. Presented by the Clinical and Quality Team
 Discharge and Follow-Up Planning Presented by the Clinical and Quality Team After today s training you will be able to: Identify and summarize important information about discharge planning Have adequate
Discharge and Follow-Up Planning Presented by the Clinical and Quality Team After today s training you will be able to: Identify and summarize important information about discharge planning Have adequate
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Program Overview. Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series. June 12, 2018
 Series. June 12, 2018") Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series Program Overview June 12, 2018 2017 New York State, Department Of Health, Office of Health Insurance Programs.
Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series Program Overview June 12, 2018 2017 New York State, Department Of Health, Office of Health Insurance Programs.
Tarek & Sophie Inspiration (TSI) Grant Application Guide
 Grant Application Guide") Tarek & Sophie Inspiration (TSI) Grant Application Guide Dear Alumni! Students on Ice (SOI) is proud to offer Alumni of the Students on Ice 2016 Arctic expedition the opportunity to apply for a Tarek and
Tarek & Sophie Inspiration (TSI) Grant Application Guide Dear Alumni! Students on Ice (SOI) is proud to offer Alumni of the Students on Ice 2016 Arctic expedition the opportunity to apply for a Tarek and
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Increasing the Complexity of Emergency Preparedness Exercises to Satisfy Regulatory Requirements
 Increasing the Complexity of Emergency Preparedness Exercises to Satisfy Regulatory Requirements CHCANYS Statewide Conference & Clinical Forum Wednesday, October 24 th, 2012 Jean Paul Roggiero MPA, CEM
Increasing the Complexity of Emergency Preparedness Exercises to Satisfy Regulatory Requirements CHCANYS Statewide Conference & Clinical Forum Wednesday, October 24 th, 2012 Jean Paul Roggiero MPA, CEM
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral)
") Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Overview of a new study to assess the impact of hospice led interventions on acute use. Jonathan Ellis, Director of Policy & Advocacy
 Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
Working Together for a Healthier Washington
 Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Medicare Community-Based Care Transitions Program. Linda M. Magno Director, Medicare Demonstrations
 Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
2ab and 3cd. BTS Topic Selection:
 2ab and 3cd. BTS Topic Selection: Meet Your Colleagues PG Pg. 3 Topic Selection Objectives By the end of this session you should be able to: List the reasons that topic selection is a critical factor in
2ab and 3cd. BTS Topic Selection: Meet Your Colleagues PG Pg. 3 Topic Selection Objectives By the end of this session you should be able to: List the reasons that topic selection is a critical factor in
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
North Carolina Division of Medical Assistance
 North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events
 Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Issue 4: October 2014
 A trial to evaluate an extended rehabilitation service for stroke patients EXTRAS News Issue 4: October 2014 What has been happening since our last newsletter in March 2014.? 1. New study centres Four
A trial to evaluate an extended rehabilitation service for stroke patients EXTRAS News Issue 4: October 2014 What has been happening since our last newsletter in March 2014.? 1. New study centres Four
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Driving Quality Improvement in Managed Care. Toby Douglas, Director California Department of Health Care Services
 1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
1. March RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 13.8%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
Colorado Medical-Dental Integration Project (CO MDI)
") Colorado Medical-Dental Integration Project (CO MDI) Allison Cusick, MPA, CHES National Oral Health Conference April 2016 Colorado Medical-Dental Integration CO MDI Five-Year Initiative Launched in 2014
Colorado Medical-Dental Integration Project (CO MDI) Allison Cusick, MPA, CHES National Oral Health Conference April 2016 Colorado Medical-Dental Integration CO MDI Five-Year Initiative Launched in 2014
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
JANUARY 2018 (21 work days) FEBRUARY 2018 (19 work days)
 FEBRUARY 2018 (19 work days)") AND CORRESPONDING DATES FOR JANUARY AND FEBRUARY 2018 JANUARY 2018 ( work days) Deadline* 12-27 12-28 12-29 1-2 1-3 1-4 1-5 1-8 1-9 1-10 Benefit Hold ** 12-28 12-29 1-2 1-3 1-4 1-5 1-8 1-9 1-10 1-11 Mailing
AND CORRESPONDING DATES FOR JANUARY AND FEBRUARY 2018 JANUARY 2018 ( work days) Deadline* 12-27 12-28 12-29 1-2 1-3 1-4 1-5 1-8 1-9 1-10 Benefit Hold ** 12-28 12-29 1-2 1-3 1-4 1-5 1-8 1-9 1-10 1-11 Mailing
NSL LINCOLNSHIRE HEALTHWATCH PRESENTATION Ambulance NHS Trust Provision of Non- Emergency Patient Transport
 NSL LINCOLNSHIRE HEALTHWATCH PRESENTATION Ambulance NHS Trust Provision of Non- Emergency Patient Transport Agenda An introduction to NSL Lincolnshire Contractual Service KPI s & Current Performance Eligibility
NSL LINCOLNSHIRE HEALTHWATCH PRESENTATION Ambulance NHS Trust Provision of Non- Emergency Patient Transport Agenda An introduction to NSL Lincolnshire Contractual Service KPI s & Current Performance Eligibility
Enlisted Professional Military Education FY 18 Academic Calendar. Table of Contents COLLEGE OF DISTANCE EDUCATION AND TRAINING (CDET):
:") Enlisted Professional Military Education FY 18 Academic Calendar Table of Contents STAFF NON-COMMISSIONED OFFICER ACADEMIES: SNCO Academy Quantico SNCO Academy Camp Pendleton SNCO Academy Camp Lejeune
Enlisted Professional Military Education FY 18 Academic Calendar Table of Contents STAFF NON-COMMISSIONED OFFICER ACADEMIES: SNCO Academy Quantico SNCO Academy Camp Pendleton SNCO Academy Camp Lejeune
Santa Clara Care Coordination Collaborative Meeting. Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018
 June 8, 2018") Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Analysis of Incurred Claims Trend and Provider Payments
 Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Changes in the School Based Access Program (SBAP)
") Pennsylvania Association of School Business Officials Changes in the School Based Access Program (SBAP) April 23, 2013 Webcast (9:30-11:00 AM) Listen to audio over your computer speakers (If you prefer
Pennsylvania Association of School Business Officials Changes in the School Based Access Program (SBAP) April 23, 2013 Webcast (9:30-11:00 AM) Listen to audio over your computer speakers (If you prefer