One in Three Californians is a Medi-Cal Beneficiary. Is Your Organization Ready for the Next Steps in Drug Medi-Cal s ODS Waiver?
|
|
|
- Estella Moody
- 5 years ago
- Views:
Transcription




1 One in Three Californians is a Medi-Cal Beneficiary. Is Your Organization Ready for the Next Steps in Drug Medi-Cal s ODS Waiver? December 6, 2018
2 This presentation has been provided for informational purposes only and is not intended and should not be construed to constitute legal advice. Please consult your attorneys in connection with any fact-specific situation under federal, state, and/or local laws that may impose additional obligations on you and your company. Cisco WebEx can be used to record webinars/briefings. By participating in this webinar/briefing, you agree that your communications may be monitored or recorded at any time during the webinar/briefing. Attorney Advertising 2


3 Presented by Kathryn Edgerton Nelson Hardiman Kevin Malone Epstein Becker Green 3
4 Agenda 1. Background 2. Federal and National Landscape 3. DMC-ODS Waiver Authority 4. Core Elements i. Benefits ii. Beneficiary Eligibility 5. County, State, and Provider Responsibilities 6. Interim results and next steps 4
5 Background Medicaid is playing an increasingly important role as a payer for services provided to individuals with SUD in the United States. An estimated 12 percent of adult Medicaid beneficiaries ages have an SUD* and the federal government is strongly prioritizing SUD treatment as a focus of the Medicaid program. According to CMS: Nearly 12 percent of Medicaid beneficiaries over 18 have a SUD, and on average, 105 people die every day as result of a drug overdose. 6,748 individuals across the country seek treatment every day in the emergency department for misuse or abuse of drugs Drug overdose is the leading cause of injury death and has caused more deaths than motor vehicle accidents among individuals years old. The monetary costs and associated collateral impact to society due to SUDs are very high. *Substance Abuse and Mental Health Services Administration. Behavioral Health Treatment Needs Assessment Toolkit for States [online] Retrieved from: p.10. 5
6 Federal Landscape On July 27, 2015, the federal Centers for Medicare and Medicaid Services ( CMS ) announced a new opportunity to submit 1,115 demonstration projects for individuals with Substance Use Disorder (SUD). Largely in response to pressure from California The initiative allowed states, starting with California, to cover residential SUD treatment services that had previously excluded from coverage under federal Medicaid due to their classification as Institutions for Mental Diseases (IMD). In return, states are required to develop a comprehensive re-design of their SUD coverage and treatment system to ensure that a continuum of care is available to individuals with SUD and that the continuum is based on an independent, evidence based standard. 6

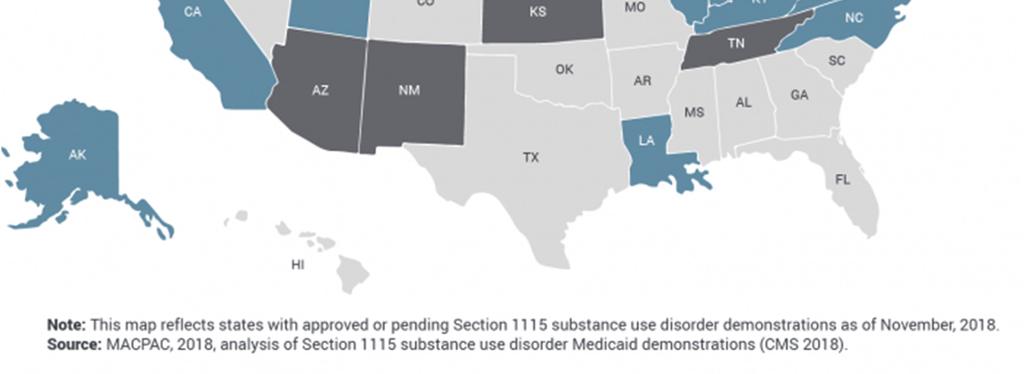
7 National Landscape 7
8 DMC-ODS Waiver Authority Organized Delivery System (ODS): Pilot program to demonstrate how organized SUD care increases beneficiary success while decreasing other health system costs Continuum of care based on ASAM Increased local control and accountability Utilization controls to improve care and efficiency Increased program oversight and integrity More intensive services for criminal justice population Evidence based practices requirements Increased coordination with other systems of care Authorized and financed under the authority of the state s Medi-Cal 2020 Waiver The DMC-ODS Pilot Program will be elective for 5 years at the county level, then mandatory. 8
9 Core Elements of the DMC-ODS - Benefits Standard DMC Benefits (available to beneficiaries in all counties) Outpatient Drug Free Treatment Intensive Outpatient Treatment Naltrexone Treatment (oral for opioid dependence or with TAR for other) Narcotic Treatment Program (methadone) Perinatal Residential SUD Services (limited by IMD exclusion) Detoxification in a Hospital (with a TAR) Pilot Benefits (only available to beneficiaries in pilot counties) Outpatient Services Intensive Outpatient Services Naltrexone Treatment (oral for opioid dependence or with TAR for other) Narcotic Treatment Program (methadone + additional medications) Residential Services (not restricted by IMD exclusion or limited to perinatal) Withdrawal Management (at least one level) Recovery Services Case Management Physician Consultation Partial Hospitalization (optional) Additional Medication Assisted Treatment (optional) 9
10 Core Elements of the DMC-ODS - Benefits Standard Residential (non-ods) State plan currently limits residential SUD services to perinatal beneficiaries only Federal matching funds are only available for services provided in facilities not considered IMDs (i.e. 16 bed max). Residential Under DMC-ODS Pilot Services are provided to non-perinatal and perinatal beneficiaries (all eligible adults and adolescents). No bed capacity limit (i.e. 16 bed IMD exclusion does not apply) Providers must be designated by DHCS to meet ASAM treatment criteria Counties must provide prior authorization for residential services within 24 hours of submission of the request. 10



11 Core Elements of the DMC-ODS - Benefits 11
12 Core Elements of the DMC-ODS - Eligibility No age restrictions Eligibility: Enrolled in Medi-Cal Reside in Participating County Meet Medical Necessity Criteria: o Adults: One DSM Diagnosis for substance-related and addictive disorders (with the exception of tobacco); meet ASAM criteria definition of medical necessity for services o Children: Be assessed to be at risk for developing a SUD and meet the ASAM adolescent treatment criteria (if applicable) 12
13 Core Elements of the DMC-ODS - Eligibility No age restrictions Eligibility: Enrolled in Medi-Cal Reside in Participating County Meet Medical Necessity Criteria: o Adults: One DSM Diagnosis for substance-related and addictive disorders (with the exception of tobacco); meet ASAM criteria definition of medical necessity for services o Children: Be assessed to be at risk for developing a SUD and meet the ASAM adolescent treatment criteria (if applicable) 13
14 County Responsibilities Access / Network Monitoring Care Coordination Selective Provider Contracting Beneficiary Protections Quality Assessment and Performance Improvement Utilization Management Authorization for Residential 14
15 County Responsibilities Managed Care Under managed care, beneficiaries receive part, or all, of their Medicaid services from providers who are paid by an organization (i.e. county) that is under contract with the State. Counties participating in the DMC-ODS Pilot Program are considered managed care plans. Prepaid Inpatient Health Plan. The State has entered into an intergovernmental agreement with counties to provide or arrange for the provision of DMC-ODS pilot services through a Prepaid Inpatient Health Plan (PIHP), as defined in federal law. Federal Managed Care Requirements. Accordingly, DMC-ODS Pilot PIHPs must comply with federal managed care requirements (with some exceptions). This is a new responsibility for counties and includes network adequacy, quality assurance and performance improvement, beneficiary rights and protections, and program integrity. 15
16 County Responsibilities Requirements Use a benefit design modeled after the American Society for Addiction Medicine (ASAM) criteria, covering a broad continuum of SUD treatment and support services Specify standards for quality and access Require providers to deliver evidence-based care Coordinate with physical and mental health services Act as a managed care plan for SUD treatment services 16
17 County Responsibilities Access Accessible Services. Each county must ensure that all required services are available and accessible to enrollees. Out of Network Coverage. If the county is unable to provide services, the county must adequately and timely cover these services out-of-network for as long as the county is unable to provide them. Appropriate and Adequate Network. The county shall maintain and monitor a network of appropriate providers that is supported by contracts with subcontractors, and sufficient to provide adequate access. Provider Selection. Access cannot be limited in any way when counties select providers. Timely Access. Hours of operation are no less than those offered to commercial enrollees or comparable Medi-Cal FFS, if the provider only services Medi-Cal. Includes 24/7 access, when medically necessary. Cultural Considerations. Pilot county participates in the State s efforts to promote the delivery of services in a culturally competent manner to all enrollees, including LEP and diverse cultural / ethnic backgrounds. Monitoring. Monitor providers regularly to determine compliance and take corrective action if there is a failure to comply. 17
18 County Responsibilities Network Adequacy In establishing and monitoring a network, pilot counties must consider: Timely Access Standards. Ability of providers to meet Department standards for timely access to care and services as specified in the county implementation plan and contract. Emergency and Crisis Care. Ability to assure that medical attention for emergency and crisis medical conditions be provided immediately. Number of Eligibles. The anticipated number of Medi-Cal eligible clients. Utilization. The expected utilization of services, taking into account the characteristics and SUD needs of beneficiaries. Number / Type of Providers. The expected utilization of services, taking into account the characteristics and SUD needs of beneficiaries. Providers Not Accepting New Patients. The number of network providers who are not accepting new beneficiaries. Geography. The geographic location of providers and their accessibility to beneficiaries, considering: Distance Travel Time Means of Transportation Ordinarily Used by Medi-Cal Beneficiaries Physical Access for Disabled Beneficiaries 18
19 County Responsibilities Selection Criteria Policies and Procedures. County should have written policy and procedures for selection and retention of providers that are applied equally Criteria. Counties will only select providers that have: A license and/or certification in good standing Enrolled / revalidated enrollment with DHCS as a DMC provider and have been screened as a high categorical risk A medical director who has enrolled with DHCS, has been screened as a limited categorical risk within a year prior, and has a signed Medicaid provider agreement with DHCS Contracting. Counties must enter into contracts with selected providers including: Cultural Competency. Provide culturally competent services, including translation services, as needed. Coordination. Procedures for coordination of care for enrollees receiving Medication Assisted Treatment (MAT) services. EBPs. Implement at least two (2) of the following Evidence Based Practices (EBPs): o Motivational Interviewing o Cognitive-Behavioral Therapy o Relapse Prevention o Trauma-Informed Treatment o Psycho-Education 19
20 County Responsibilities Contract Appeals Written Notification of Denial. County must serve providers that are not selected with a written decision and have a protest procedure for providers that are not selected. Local Protest Procedure. Providers may challenge the denial to DHCS only after the local protest procedure has been exhausted; must also have reason to believe that the county has an inadequate network State Appeal. Following submission of appeal and county response, DHCS will set a date for parties to discuss with a DHCS representative with subject matter knowledge. Final Determination. DHCS will make a final determination, which may result in no further action or a county corrective action plan (CAP). 20
21 State Responsibilities Monitoring Plan (EQRO, Program Integrity) Triennial Review Reporting of Activity ASAM Designation for Residential Provider Appeals Process 21
22 State Responsibilities Certified Public Expenditure. Counties will certify the total allowable expenditures incurred in providing DMC-ODS pilot services through county-operated or contracted providers. County-Specific Rates. Counties will develop proposed county-specific interim rates for each covered service (except for NTP) subject to state approval Realignment Provisions / BH Subaccount Realignment requirements related to the BH Subaccount will remain in place and the state will continue to assess and monitor county expenditures for the realigned programs. Federal Financial Participation (FFP). FFP will be available to contracting pilot counties who certify the total allowable expenditures incurred in delivering covered services. County-Operated Providers. County-operated providers will be reimbursed based on actual costs. Subcontracted Providers. Subcontracted fee-for-service providers will be reimbursed based on actual expenditures. CPE Protocol. Approved by CMS to allow FFP under the Pilot. Includes provisions related to: Inflation Factor Lower of Cost or Charge Cost Report 22
23 State Responsibilities Rates Annual Fiscal Plan. Counties are required to complete and submit an Annual County Fiscal Plan following DHCS guidance. DHCS Review and Approval. DHCS will review and approve the plan annually. Interim Rates. Proposed interim rates must be developed for each required and selected optional service specified in the waiver. Supporting Information. Counties must provide supporting information consistent with state and federal guidance for each proposed rate. Sources. Appropriate sources of information include filed cost reports, approved medical inflation factors, detailed provider direct and indirect service cost estimates, and verified charges made to other third party payers for similar programs. Residential Rates. Proposed residential rates must include clear differentiation between treatment and non-treatment room and board costs. Outpatient Rates. Proposed outpatient treatment rates should include all assessment, treatment planning and treatment provision direct and indirect costs consistent with coverage and program requirements outlined in state and federal guidance. Admin, QI, UR, etc. County administrative, quality improvement, authorization, and utilization review activities may be claimed separately consistent with state and federal guidance. 23

24 Overview of California s DMC-ODS Pilot Programs In California, 8.5% of residents age 12 and older (2.7 million people) met the criteria for having a SUD in the past year. Only 1 in 10 received treatment The goal of the DMC-ODS pilot program is to treat more people more effectively by reorganizing the delivery system for SUD treatment in Medi- Cal. *Source: California Health Care Foundation, Issue Brief, August
25 Overview of California s DMC-ODS Pilot Programs Forty California counties are taking part in the Drug Medi-Cal Organized Delivery System (DMC- ODS) pilot program under California s Medicaid Section 1115 waiver, which was approved in 2015 and will run through 2020 (see Figure 1). As of July 2018, 19 counties were providing services under the pilot and represent approximately 75% of the State s Medi-Cal population.* *Source: California Health Care Foundation, Issue Brief, August

26 Overview of California s DMC-ODS Pilot Programs When the remaining 21 counties that have submitted implementation plans begin services, over 97% of Medi-Cal enrollees will have access to DMC-ODS pilot programs The Tribal and Urban Indian Health Programs are scheduled to begin implementation in the summer of 2019 *Source: California Health Care Foundation, Issue Brief, August


27 Reframing of SUD Treatment Historically, SUD treatment has been associated more with criminal justice than healthcare. Under the DMC-ODS pilot program, SUD treatment has been brought into the larger health care landscape and addiction is being reframed as a chronic disease, which is a fundamental shift. *Source: California Health Care Foundation, Issue Brief, August

28 Standard Drug Medi-Cal vs. DMC-ODS *Source: California Health Care Foundation, Issue Brief, August

29 Keys to Success Provider Engagement Communications Plan Partnerships *Source: California Health Care Foundation, Issue Brief, August

30 Challenges Stigma Misconceptions about SUD and its treatment Some believe SUD is not a medical condition Public attitudes are evolving *Source: California Health Care Foundation, Issue Brief, August

31 Challenges Criminal Justice System Embedded patters have been disrupted Each individual has unique treatment needs Court-ordered treatment may not meet medical necessity criteria *Source: California Health Care Foundation, Issue Brief, August

32 Challenges Administrative Infrastructure Increased requirements for documentation, training, and coordination of care Expenses for new staff, technology, facility improvements, and training *Source: California Health Care Foundation, Issue Brief, August

33 Challenges High Demand, Low Supply Need a sufficient supply of qualified providers for high demand More residential providers needed More providers who serve the youth population needed *Source: California Health Care Foundation, Issue Brief, August

34 Challenges Predicting Costs Budgetary planning needed Increased demand for services *Source: California Health Care Foundation, Issue Brief, August

35 Generational Opportunity to Advance SUD Treatment This is a generational opportunity to advance SUD treatment, Everyone providers, patients, and plans should realize how important this is. It s a watershed moment for Medi-Cal. - John Connolly, PhD, who is leading the implementation of the Los Angeles County DMC-ODS pilot program. *Source: California Health Care Foundation, Issue Brief, August
36 Presented Questions? by Kathryn Edgerton Nelson Hardiman Kevin Malone Epstein Becker Green 36
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver
 Waiver") Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
Drug Medi-Cal Organized Delivery System Demonstration Waiver
 Drug Medi-Cal Organized Delivery System Demonstration Waiver All County Orientation to Standard Terms and Conditions & Fiscal Provisions Presentation by DHCS and Harbage September 28, 2015 Overview of
Drug Medi-Cal Organized Delivery System Demonstration Waiver All County Orientation to Standard Terms and Conditions & Fiscal Provisions Presentation by DHCS and Harbage September 28, 2015 Overview of
DRUG MEDI-CALWAIVER STAKEHOLDER FORUM
 October 27, 2015 DRUG MEDI-CALWAIVER STAKEHOLDER FORUM Patrick Zarate Division Manager, Alcohol & Drug Programs Objectives for Today Learn About the Drug Medi-Cal Organized Delivery System waiver Gain
October 27, 2015 DRUG MEDI-CALWAIVER STAKEHOLDER FORUM Patrick Zarate Division Manager, Alcohol & Drug Programs Objectives for Today Learn About the Drug Medi-Cal Organized Delivery System waiver Gain
Drug Medi-Cal (DMS) Organized Delivery System (ODS)
 Organized Delivery System (ODS)") Drug Medi-Cal (DMS) Organized Delivery System (ODS) Stanislaus County BHRS Substance Use Disorder (SUD) System of Care Stakeholder Meetings April 21 and May 4, 2017 Welcome and Introductions Rick DeGette,
Drug Medi-Cal (DMS) Organized Delivery System (ODS) Stanislaus County BHRS Substance Use Disorder (SUD) System of Care Stakeholder Meetings April 21 and May 4, 2017 Welcome and Introductions Rick DeGette,
SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery. o--,-.m-a----,laa~-d-c~~~~~~~~~~-
 Page 11 of 8 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Policy and Procedure Section Sub-section Alcohol and Drug Program (ADP) Policy Drug Medi-Cal
Page 11 of 8 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Policy and Procedure Section Sub-section Alcohol and Drug Program (ADP) Policy Drug Medi-Cal
Drug Medi-Cal Organized Delivery System
 Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) PERFORMANCE METRICS. (version 6/23/17)
 PERFORMANCE METRICS. (version 6/23/17)") 1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
California Medi-Cal 2020 Demonstration Page 89 of 307 Approved December 30, 2015 through December 31, 2020
 X. DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM 127. Drug Medi-Cal Eligibility and Delivery System. The Drug Medi-Cal Organized Delivery System (DMC-ODS) is a Pilot program to test a new paradigm for the organized
X. DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM 127. Drug Medi-Cal Eligibility and Delivery System. The Drug Medi-Cal Organized Delivery System (DMC-ODS) is a Pilot program to test a new paradigm for the organized
Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services. Uma K. Zykofsky, LCSW Behavioral Health Director
 Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services April 24, 2017 Presentation to Geographic Managed Care Providers Uma K. Zykofsky, LCSW Behavioral Health
Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services April 24, 2017 Presentation to Geographic Managed Care Providers Uma K. Zykofsky, LCSW Behavioral Health
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) YEAR 1 PERFORMANCE METRICS (version 10/24/17)
 YEAR 1 PERFORMANCE METRICS (version 10/24/17)") 1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
DMC-ODS. System Transformation. Presented at DHCS 2017 Annual Conference. Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW
 DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
The Addiction Treatment Landscape:
 The Addiction Treatment Landscape: The California Transformation to a Managed Care Model California Association of Collaborative Courts September 12, 2018 Elizabeth Stanley-Salazar, MPH Consultant, Project
The Addiction Treatment Landscape: The California Transformation to a Managed Care Model California Association of Collaborative Courts September 12, 2018 Elizabeth Stanley-Salazar, MPH Consultant, Project
Behavioral Wellness A System of Care and Recovery
 ., SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery P a g e \ 1 of 6 Departmental Policy and Procedure Section Sub-section Policy Alcohol and Drug Program (ADP) Drug
., SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery P a g e \ 1 of 6 Departmental Policy and Procedure Section Sub-section Policy Alcohol and Drug Program (ADP) Drug
Behavioral Health Services
 Behavioral Health Services Substance Use Disorder Services and RFP 26-2016: Substance Abuse Disorder Treatment Services and Support. February 6, 2018 1 Introduction Today is the fourth in a series of overview
Behavioral Health Services Substance Use Disorder Services and RFP 26-2016: Substance Abuse Disorder Treatment Services and Support. February 6, 2018 1 Introduction Today is the fourth in a series of overview
The CMS Medicaid Managed Care Final Rule An Overview for Behavioral Health Directors. Linnea Koopmans Senior Policy Analyst December 14, 2016
 The CMS Medicaid Managed Care Final Rule An Overview for Behavioral Health Directors Linnea Koopmans Senior Policy Analyst December 14, 2016 Presentation Outline CMS Background Medicaid Managed Care (MMC)
The CMS Medicaid Managed Care Final Rule An Overview for Behavioral Health Directors Linnea Koopmans Senior Policy Analyst December 14, 2016 Presentation Outline CMS Background Medicaid Managed Care (MMC)
Departm. The Department of. Stakeholder. Delivery Bridge to. ion Waiver. CMS. Delivery. Phone: (916) TOBY DOUGLAS DIRECTOR
 TOBY DOUGLAS DIRECTOR") State of California Health and Human Services Agency Departm ment of Health Care Services TOBY DOUGLAS DIRECTOR EDMUNDD G. BROWN JR. GOVERNOR Date: October 3, 2014 To: Stakeholder rs and Interested Parties
State of California Health and Human Services Agency Departm ment of Health Care Services TOBY DOUGLAS DIRECTOR EDMUNDD G. BROWN JR. GOVERNOR Date: October 3, 2014 To: Stakeholder rs and Interested Parties
Any time of the day or night, seven days a
 August 2018 Medi-Cal Moves Addiction Treatment into the Mainstream: Early Lessons from the Drug Medi-Cal Organized Delivery System Pilots Issue Brief Any time of the day or night, seven days a week, residents
August 2018 Medi-Cal Moves Addiction Treatment into the Mainstream: Early Lessons from the Drug Medi-Cal Organized Delivery System Pilots Issue Brief Any time of the day or night, seven days a week, residents
Contra Costa County. Drug Medi-Cal Organized Delivery System (DMC-ODS) Program BENEFICIARY HANDBOOK
 Program BENEFICIARY HANDBOOK") Contra Costa County Drug Medi-Cal Organized Delivery System (DMC-ODS) Program BENEFICIARY HANDBOOK DMC-ODS Beneficiary Handbook 1 TABLE OF CONTENTS Table of Contents GENERAL INFORMATION... 4 Emergency
Contra Costa County Drug Medi-Cal Organized Delivery System (DMC-ODS) Program BENEFICIARY HANDBOOK DMC-ODS Beneficiary Handbook 1 TABLE OF CONTENTS Table of Contents GENERAL INFORMATION... 4 Emergency
Drug Medi-Cal Organized Delivery System Implementation Plan
 California Department of Health Care Services Drug Medi-Cal Organized Delivery System Waiver NEVADA COUNTY BEHAVIORAL HEALTH Drug Medi-Cal Organized Delivery System Implementation Plan Submitted July 14,
California Department of Health Care Services Drug Medi-Cal Organized Delivery System Waiver NEVADA COUNTY BEHAVIORAL HEALTH Drug Medi-Cal Organized Delivery System Implementation Plan Submitted July 14,
Title 22 Background & Updated Information State Plan Amendments Roles and Responsibilities Provider SUD Medical Director Physician Department of
 Title 22 Background & Updated Information State Plan Amendments Roles and Responsibilities Provider SUD Medical Director Physician Department of Health Care Services (DHCS) County DMC Substance Use Disorder
Title 22 Background & Updated Information State Plan Amendments Roles and Responsibilities Provider SUD Medical Director Physician Department of Health Care Services (DHCS) County DMC Substance Use Disorder
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
Mental Health Board Member Orientation & Training
 1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
Drug Medi-Cal Organized Delivery System Implementation Plan
 Drug Medi-Cal Organized Delivery System Implementation Plan For Yolo County Health and Human Services Agency Submitted by: Ian Evans, LMFT HHSA Approved: December 2016 PART I PLAN QUESTIONS This part is
Drug Medi-Cal Organized Delivery System Implementation Plan For Yolo County Health and Human Services Agency Submitted by: Ian Evans, LMFT HHSA Approved: December 2016 PART I PLAN QUESTIONS This part is
MEDICAID MENTAL HEALTH PARITY AND ADDICTION EQUITY ACT COMPLIANCE PLAN
 State of California Health and Human Services Agency Department of Health Care Services MEDICAID MENTAL HEALTH PARITY AND ADDICTION EQUITY ACT COMPLIANCE PLAN October 2, 2017 This page is left intentionally
State of California Health and Human Services Agency Department of Health Care Services MEDICAID MENTAL HEALTH PARITY AND ADDICTION EQUITY ACT COMPLIANCE PLAN October 2, 2017 This page is left intentionally
Mental Health Parity Implementation: Are We There Yet?
 Mental Health Parity Implementation: Are We There Yet? March 22, 2016 2016 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com This presentation has been provided for informational purposes only
Mental Health Parity Implementation: Are We There Yet? March 22, 2016 2016 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com This presentation has been provided for informational purposes only
Substance Use Disorder Treatment Provider Manual
 Substance Use Disorder Treatment Provider Manual February 2017 This page intentionally left blank. 1 Substance Use Disorder Treatment Provider Manual Contents SUBSTANCE USE DISORDER TREATMENT PROVIDER
Substance Use Disorder Treatment Provider Manual February 2017 This page intentionally left blank. 1 Substance Use Disorder Treatment Provider Manual Contents SUBSTANCE USE DISORDER TREATMENT PROVIDER
Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act
 October 2018 Issue Brief Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act MaryBeth Musumeci and Jennifer Tolbert On October 3, 2018, the Senate overwhelmingly passed
October 2018 Issue Brief Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act MaryBeth Musumeci and Jennifer Tolbert On October 3, 2018, the Senate overwhelmingly passed
Drug Medi-Cal Organized Delivery System Evaluation: Baseline
 Drug Medi-Cal Organized Delivery System Evaluation: Baseline Darren Urada, Ph.D., Cheryl Teruya, Ph.D., Valerie P. Antonini, M.P.H., Elise Tran, B.A., David Huang, Ph.D., Howard Padwa, Ph.D., June Lim,
Drug Medi-Cal Organized Delivery System Evaluation: Baseline Darren Urada, Ph.D., Cheryl Teruya, Ph.D., Valerie P. Antonini, M.P.H., Elise Tran, B.A., David Huang, Ph.D., Howard Padwa, Ph.D., June Lim,
Drug Medi-Cal Waiver Evaluation Planning
 Drug Medi-Cal Waiver Evaluation Planning Darren Urada, Ph.D. UCLA Integrated Substance Abuse Programs January 5, 2015 The author s views and recommendations do not necessarily represent those of the funders,
Drug Medi-Cal Waiver Evaluation Planning Darren Urada, Ph.D. UCLA Integrated Substance Abuse Programs January 5, 2015 The author s views and recommendations do not necessarily represent those of the funders,
UTILIZATION MANAGEMENT POLICIES AND PROCEDURES. Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08
 SALISH BHO UTILIZATION MANAGEMENT POLICIES AND PROCEDURES Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08 Reference: WAC 388-877B, Contract requirements DSM-5, ASAM, SBHO
SALISH BHO UTILIZATION MANAGEMENT POLICIES AND PROCEDURES Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08 Reference: WAC 388-877B, Contract requirements DSM-5, ASAM, SBHO
Overview of California External Quality Review Activities
 Overview of California External Quality Review Activities CBHDA Fiscal Administrator Conference Rama Khalsa, Director Drug Medi-Cal EQRO Bill Ullom, Information Systems Chief December 11, 2017 Review Activities
Overview of California External Quality Review Activities CBHDA Fiscal Administrator Conference Rama Khalsa, Director Drug Medi-Cal EQRO Bill Ullom, Information Systems Chief December 11, 2017 Review Activities
Notice of Adverse Benefit Determination Training
 Notice of Adverse Benefit Determination Training Santa Cruz County Behavioral Health Quality Improvement Mental Health Plan / Drug Medi-Cal Plan From here-out to be referred to as Plans 05/1/18 Goal Training
Notice of Adverse Benefit Determination Training Santa Cruz County Behavioral Health Quality Improvement Mental Health Plan / Drug Medi-Cal Plan From here-out to be referred to as Plans 05/1/18 Goal Training
Drug Medi Cal Organized Delivery System Member Handbook
 Behavioral Health Services A Division of Health Care Services Agency Tony Vartan, MSW, LCSW, BHS Director Substance Abuse Services Drug Medi Cal Organized Delivery System Member Handbook SJC BHS SAS 5/30/2018
Behavioral Health Services A Division of Health Care Services Agency Tony Vartan, MSW, LCSW, BHS Director Substance Abuse Services Drug Medi Cal Organized Delivery System Member Handbook SJC BHS SAS 5/30/2018
Drug Medi-Cal Organized Delivery System Implementation Plan. Imperial County Behavioral Health Services
 Drug Medi-Cal Organized Delivery System Implementation Plan Behavioral Health Services Contents Page Number Part I Plan Questions 2 Part II Plan Description: Narrative Description of the County s Plan
Drug Medi-Cal Organized Delivery System Implementation Plan Behavioral Health Services Contents Page Number Part I Plan Questions 2 Part II Plan Description: Narrative Description of the County s Plan
MARIN BEHAVIORAL HEALTH AND RECOVERY SERVICES Department Update
 MARIN BEHAVIORAL HEALTH AND RECOVERY SERVICES Department Update P R E S E N T E D B Y : S U Z A N N E T A V A N O, P H D B E H A V I O R A L H E A L T H A N D R E C O V E R Y S E R V I C E S D I R E C
MARIN BEHAVIORAL HEALTH AND RECOVERY SERVICES Department Update P R E S E N T E D B Y : S U Z A N N E T A V A N O, P H D B E H A V I O R A L H E A L T H A N D R E C O V E R Y S E R V I C E S D I R E C
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
9/13/2016. ASAM Criteria and Levels of Care. Why a Continuum of Care. and. Substance Use. Co-Occurring Disorders. Guiding Principles
 ASAM Criteria and Levels of Care Substance Use and Co-Occurring Disorders Why a Continuum of Care 1.To help clients/patients to receive the most appropriate and highest quality treatment services, 2.To
ASAM Criteria and Levels of Care Substance Use and Co-Occurring Disorders Why a Continuum of Care 1.To help clients/patients to receive the most appropriate and highest quality treatment services, 2.To
Medicaid Fundamentals. John O Brien Senior Advisor SAMHSA
 Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
Health Services. Purpose. Major Budget Changes. F-12 County of San Joaquin Proposed Budget. Health Care Services Director
 Greg Diederich, Health Care Services Director Mental Health & 2013-14 2014-15 2015-16 2015-16 Increase/ Substance Abuse Fund Actual Approved Requested Recommended (Decrease) Expenditures Salaries & Benefits
Greg Diederich, Health Care Services Director Mental Health & 2013-14 2014-15 2015-16 2015-16 Increase/ Substance Abuse Fund Actual Approved Requested Recommended (Decrease) Expenditures Salaries & Benefits
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Drug/Medi-Cal Organized Delivery System (DMC-ODS) Waiver County Implementation Plan. Submitted By: Ventura County Behavioral Health Department
 Waiver County Implementation Plan. Submitted By: Ventura County Behavioral Health Department") Drug/Medi-Cal Organized Delivery System (DMC-ODS) Waiver County Implementation Plan Submitted By: Ventura County Behavioral Health Department June 2016 1 Drug Medi-Cal Organized Delivery System Implementation
Drug/Medi-Cal Organized Delivery System (DMC-ODS) Waiver County Implementation Plan Submitted By: Ventura County Behavioral Health Department June 2016 1 Drug Medi-Cal Organized Delivery System Implementation
California Drug Medi-Cal. Organized Delivery System: Proposed Evaluation for California s Section 1115 Demonstration Waiver
 California Drug Medi-Cal Organized Delivery System: Proposed Evaluation for California s Section 1115 Demonstration Waiver Approved by CMS June 20, 2016 Table of Contents California s Drug Medi-Cal Organized
California Drug Medi-Cal Organized Delivery System: Proposed Evaluation for California s Section 1115 Demonstration Waiver Approved by CMS June 20, 2016 Table of Contents California s Drug Medi-Cal Organized
ODS Waiver SUD Treatment Documentation. A high level overview of DMC-Organized Delivery System (ODS) Waiver documentation requirements
 Waiver documentation requirements") ODS Waiver SUD Treatment Documentation A high level overview of DMC-Organized Delivery System (ODS) Waiver documentation requirements 1 Overview Expanded Service Delivery Definition of LPHA Intake Physical
ODS Waiver SUD Treatment Documentation A high level overview of DMC-Organized Delivery System (ODS) Waiver documentation requirements 1 Overview Expanded Service Delivery Definition of LPHA Intake Physical
Stanislaus County Drug Medi-Cal Organized Delivery System (DMC- ODS)
") Stanislaus County Drug Medi-Cal Organized Delivery System (DMC- ODS) BHRS Vision Our vision is to continue to be a leader in behavioral health and to be recognized for excellence in our community, state,
Stanislaus County Drug Medi-Cal Organized Delivery System (DMC- ODS) BHRS Vision Our vision is to continue to be a leader in behavioral health and to be recognized for excellence in our community, state,
California County Administrator Survey 2015 Preliminary Results
 California County Administrator Survey 2015 Preliminary Results September 24, 2015 CBHDA SAPT+ Committee Meeting Elise Tran, Darren Urada, Ph.D., Valerie Antonini, MPH, Cheryl Teruya, Ph.D., Kate Lovinger,
California County Administrator Survey 2015 Preliminary Results September 24, 2015 CBHDA SAPT+ Committee Meeting Elise Tran, Darren Urada, Ph.D., Valerie Antonini, MPH, Cheryl Teruya, Ph.D., Kate Lovinger,
California s Drug Medi-Cal Organized Delivery System
 California s Drug Medi-Cal Organized Delivery System FY 2015 2016 Report Evaluation of California s Section 1115 Demonstration Waiver Prepared for the Department of Health Care Services California Health
California s Drug Medi-Cal Organized Delivery System FY 2015 2016 Report Evaluation of California s Section 1115 Demonstration Waiver Prepared for the Department of Health Care Services California Health
EQRO Year 1 Toolkit for Counties Participating in the DMC-ODS Waiver
 Website: www.caleqro.com Ph.: 855-385-3776 5901 Christie Avenue, Suite 502 Emeryville, CA 94608 EQRO Year 1 Toolkit for Counties Participating in the DMC-ODS Waiver TABLE OF CONTENTS INTRODUCTION... 3
Website: www.caleqro.com Ph.: 855-385-3776 5901 Christie Avenue, Suite 502 Emeryville, CA 94608 EQRO Year 1 Toolkit for Counties Participating in the DMC-ODS Waiver TABLE OF CONTENTS INTRODUCTION... 3
I. Coordinating Quality Strategies Across Managed Care Plans
 Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Managed Medi-Cal Behavioral Health Benefits. Alliance Board Meeting October 23, 2013
 Managed Medi-Cal Behavioral Health Benefits Alliance Board Meeting October 23, 2013 Purpose Discuss role of ACA in expanding benefits Review philosophy of integrated health care Review State policy process
Managed Medi-Cal Behavioral Health Benefits Alliance Board Meeting October 23, 2013 Purpose Discuss role of ACA in expanding benefits Review philosophy of integrated health care Review State policy process
Volume 26 No. 05 July Providers of Behavioral Health Services For Action Health Maintenance Organizations For Information Only
 Newsletter Published by the N.J. Dept. of Human, Div. of Medical Assistance & Health & the Division of and Volume 26 No. 05 July 2016 TO: SUBJECT: Providers of Behavioral Health For Action Health Maintenance
Newsletter Published by the N.J. Dept. of Human, Div. of Medical Assistance & Health & the Division of and Volume 26 No. 05 July 2016 TO: SUBJECT: Providers of Behavioral Health For Action Health Maintenance
Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016
 Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016 # Category Agency Issue Description/Analysis Next Steps Timeframe/Target Date 1 BH-BHO BHA Require BHOs to
Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016 # Category Agency Issue Description/Analysis Next Steps Timeframe/Target Date 1 BH-BHO BHA Require BHOs to
Drug Medi-Cal Organized Delivery System Implementation Plan
 Drug Medi-Cal Organized Delivery System Implementation Plan Santa Barbara County Department of Behavioral Wellness Alcohol and Drug Programs countyofsb.org/behavioral-wellness 805-681-5220 Prepared by:
Drug Medi-Cal Organized Delivery System Implementation Plan Santa Barbara County Department of Behavioral Wellness Alcohol and Drug Programs countyofsb.org/behavioral-wellness 805-681-5220 Prepared by:
California s Current Section 1115 Waiver & Its Impact on the Public Hospital Safety Net
 February 2010 California s Current Section 1115 Waiver & Its Impact on the Public Hospital Safety Net Executive Summary The current Section 1115 Medicaid waiver, which was intended to stabilize California
February 2010 California s Current Section 1115 Waiver & Its Impact on the Public Hospital Safety Net Executive Summary The current Section 1115 Medicaid waiver, which was intended to stabilize California
Short-term Intensive Residential Remediation Treatment
 Short-term Intensive Residential Remediation Treatment LETTER OF INTENT Signal Behavioral Health Network 6130 GREENWOOD PLAZA BLVD, #150, GREENWOOD VILLAGE, CO 80111 1 LETTER OF INTENT SCOPE This Letter
Short-term Intensive Residential Remediation Treatment LETTER OF INTENT Signal Behavioral Health Network 6130 GREENWOOD PLAZA BLVD, #150, GREENWOOD VILLAGE, CO 80111 1 LETTER OF INTENT SCOPE This Letter
DHCS Update: Major Initiatives and Strategies Towards Standardization
 DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
Vermont Hub and Spoke Model
 Vermont Hub and Spoke Model John R. Brooklyn, MD Assistant Clinical Professor of Family Medicine and Psychiatry Medical Director Substance Abuse Treatment Center University of Vermont Impetus for Developing
Vermont Hub and Spoke Model John R. Brooklyn, MD Assistant Clinical Professor of Family Medicine and Psychiatry Medical Director Substance Abuse Treatment Center University of Vermont Impetus for Developing
North Carolina s Transformation to Managed Care
 North Carolina s Transformation to Managed Care Jay Ludlam, Assistant Secretary Department of Health and Human Services December 2017 My background Only 10+ years of experience in Medicaid Assistant Attorney
North Carolina s Transformation to Managed Care Jay Ludlam, Assistant Secretary Department of Health and Human Services December 2017 My background Only 10+ years of experience in Medicaid Assistant Attorney
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL
 PROVIDER MANUAL") THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
California s Coordinated Care Initiative
 California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
MassHealth Restructuring Overview
 1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
Division of Mental Health, Developmental Disabilities & Substance Abuse Services NC Mental Health and Substance Use Service Array Survey
 Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Beacon Health Strategies Primary Care Provider Training
 Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Transition Period. Parallel Paths to Purchasing Transformation 2020: RSAs. Fully Integrated Managed Care System
 2 Parallel Paths to Purchasing Transformation 2020: Fully Integrated Managed Care System Transition Period 2014 Legislative Action: SSB 6312 By January 1, 2020, the community behavioral health program
2 Parallel Paths to Purchasing Transformation 2020: Fully Integrated Managed Care System Transition Period 2014 Legislative Action: SSB 6312 By January 1, 2020, the community behavioral health program
I. General Instructions
 Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
~,, Behavioral Wellness ~ ' ~ A System of Care and Recovery
 SANTA BARBARA COUNT Y ~ DEPARTMENT OF ~,, Behavioral Wellness ~ ' ~ A System of Care and Recovery Page 11 of 7 Departmental Policy and Procedure Section Sub-section Policy Policy# Office of Strategy Management
SANTA BARBARA COUNT Y ~ DEPARTMENT OF ~,, Behavioral Wellness ~ ' ~ A System of Care and Recovery Page 11 of 7 Departmental Policy and Procedure Section Sub-section Policy Policy# Office of Strategy Management
Expanded Coverage For Addiction Treatment: Finding The Opportunities With The Drug Medi-Cal Organized Delivery System
 Expanded Coverage For Addiction Treatment: Finding The Opportunities With The Drug Medi-Cal Organized Delivery System The 2016 OPEN MINDS California Management Best Practices Institute August 24, 2016
Expanded Coverage For Addiction Treatment: Finding The Opportunities With The Drug Medi-Cal Organized Delivery System The 2016 OPEN MINDS California Management Best Practices Institute August 24, 2016
Medicaid Transformation
 JOINT LEGISLATIVE COMMITTEE ON MEDICAID AND NC HEALTH CHOICE Medicaid Transformation Dr. Mandy Cohen, Dave Richard, Jay Ludlam Department of Health and Human Services Nov. 14, 2017 Recap: Where We Are
JOINT LEGISLATIVE COMMITTEE ON MEDICAID AND NC HEALTH CHOICE Medicaid Transformation Dr. Mandy Cohen, Dave Richard, Jay Ludlam Department of Health and Human Services Nov. 14, 2017 Recap: Where We Are
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
Coordinated Care Initiative (CCI) ADVANCED I: Benefit Package and Consumer Protections
 ADVANCED I: Benefit Package and Consumer Protections") July 29, 2014 Coordinated Care Initiative (CCI) ADVANCED I: Benefit Package and Consumer Protections Amber Cutler, Staff Attorney National Senior Citizens Law Center www.nsclc.org 1 The National Senior
July 29, 2014 Coordinated Care Initiative (CCI) ADVANCED I: Benefit Package and Consumer Protections Amber Cutler, Staff Attorney National Senior Citizens Law Center www.nsclc.org 1 The National Senior
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION
 -OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
MEDI-CAL MANAGED CARE OVERVIEW
 MEDI-CAL MANAGED CARE OVERVIEW July 2018 Sandy Damiano, PhD Deputy Director DHS Primary Health Eligibility & Enrollment Apply for Medi-Cal year round: County Department of Human Assistance (DHA) Online,
MEDI-CAL MANAGED CARE OVERVIEW July 2018 Sandy Damiano, PhD Deputy Director DHS Primary Health Eligibility & Enrollment Apply for Medi-Cal year round: County Department of Human Assistance (DHA) Online,
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo.
 This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
Improving Health Status through Behavioral Health Interventions
 Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward
 The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
MEDICAL ASSISTANCE BULLETIN
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER September 8, 1995 September 8, 1995 1153-95-01 SUBJECT Accessing Outpatient Wraparound
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER September 8, 1995 September 8, 1995 1153-95-01 SUBJECT Accessing Outpatient Wraparound
The County of Sonoma Department of Health Services Behavioral Health Division
 The County of Sonoma Department of Health Services Behavioral Health Division Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Implementation Plan August 2016 Prepared by: Sonoma County Behavioral
The County of Sonoma Department of Health Services Behavioral Health Division Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Implementation Plan August 2016 Prepared by: Sonoma County Behavioral
Draft Children s Managed Care Transition MCO Requirements
 Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
COMPLIANCE. Behavioral Health Compliance Office Compliance Corner. October Defining Healthcare Compliance. A culture that promotes:
 Behavioral Health Compliance Office Compliance Corner October 2018 COMPLIANCE Defining Healthcare Compliance Healthcare compliance can be defined as the ongoing A culture that promotes: process of meeting
Behavioral Health Compliance Office Compliance Corner October 2018 COMPLIANCE Defining Healthcare Compliance Healthcare compliance can be defined as the ongoing A culture that promotes: process of meeting
Draft Meeting Minutes August 3 rd, :00 P.M. to 5:00 P.M. Pea Soup Andersen s Pavilion Room, Buellton, CA
 SANTA BARBARA COUNTY ADVISORY BOARD ON ALCOHOL & DRUG PROBLEMS 300 North San Antonio Road, Santa Barbara, CA 93110 Phone (805) 681-5440 / Fax (805) 681-5413 http://www.countyofsb.org/admhs/ Draft Meeting
SANTA BARBARA COUNTY ADVISORY BOARD ON ALCOHOL & DRUG PROBLEMS 300 North San Antonio Road, Santa Barbara, CA 93110 Phone (805) 681-5440 / Fax (805) 681-5413 http://www.countyofsb.org/admhs/ Draft Meeting
Provider Relations Training
 Cal MediConnect Provider Relations Training Presented by Victor Gonzalez and George Scolari Provider Relations Training Agenda Overview of Cal MediConnect Eligibility & Exclusions Enrollment & Disenrollment
Cal MediConnect Provider Relations Training Presented by Victor Gonzalez and George Scolari Provider Relations Training Agenda Overview of Cal MediConnect Eligibility & Exclusions Enrollment & Disenrollment
1. SMHS Section of CCR Title 9 (Division 1, Chapter 11): this is the regulation created by the California Department of Health Care Services (DHCS).
: this is the regulation created by the California Department of Health Care Services (DHCS).") Clinical Documentation Tool This tool compares the definitions of outpatient Specialty Mental Health s (SMHS) that appear in two different sources: 1. SMHS Section of CCR Title 9 (Division 1, Chapter 11):
Clinical Documentation Tool This tool compares the definitions of outpatient Specialty Mental Health s (SMHS) that appear in two different sources: 1. SMHS Section of CCR Title 9 (Division 1, Chapter 11):
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s)
") Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
LOUISIANA MEDICAID PROGRAM ISSUED: 08/24/17 REPLACED: 07/06/17 CHAPTER 2: BEHAVIORAL HEALTH SERVICES APPENDIX B GLOSSARY/ACRONYMS PAGE(S) 5 GLOSSARY
 5 GLOSSARY") GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
Behavioral health provider overview
 Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Leveraging FQHCs in California s Behavioral Health Care Continuum
 Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
IME Training Phase II
 1 IME Training Phase II 2 IME Phase II Training Phase II of IME to include Full Utilization Management of Managed Initiatives by the IME Significant Changes in NJSAMS Changes in Claims Conversion of Slot
1 IME Training Phase II 2 IME Phase II Training Phase II of IME to include Full Utilization Management of Managed Initiatives by the IME Significant Changes in NJSAMS Changes in Claims Conversion of Slot
MHP Work Plan: 4-Behavioral health clinical care
 PROGRAM INFORMATION: Program Title: School Based Metro (MHSA) Provider: Department of Behavioral Health The Department of Behavioral Health (DBH) Metro School Based Team (MSBT) is designed to deliver outpatient
PROGRAM INFORMATION: Program Title: School Based Metro (MHSA) Provider: Department of Behavioral Health The Department of Behavioral Health (DBH) Metro School Based Team (MSBT) is designed to deliver outpatient
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Optum/OptumHealth Behavioral Solutions of California Facility Network Request Form / Credentialing Application
 Optum/OptumHealth Behavioral Solutions of California Is the facility currently in the Optum network? Yes No Acceptance into the Optum/OptumHealth Behavioral Solutions of California (Optum) provider network
Optum/OptumHealth Behavioral Solutions of California Is the facility currently in the Optum network? Yes No Acceptance into the Optum/OptumHealth Behavioral Solutions of California (Optum) provider network
California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process. Peter Harbage President Harbage Consulting
 California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process Peter Harbage President Harbage Consulting 1 Today s Agenda 1. California Context 1. California s Stakeholder Engagement
California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process Peter Harbage President Harbage Consulting 1 Today s Agenda 1. California Context 1. California s Stakeholder Engagement
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training
 Santa Clara County Behavioral Health provider training") Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
The Current Medi-Cal Landscape: Overview of Mild-to-Moderate Mental Health Coverage and System Organization
 Advancing innovations in health care delivery for low-income Americans The Current Medi-Cal Landscape: Overview of Mild-to-Moderate Mental Health Coverage and System Organization December 1, 2016 For Audio
Advancing innovations in health care delivery for low-income Americans The Current Medi-Cal Landscape: Overview of Mild-to-Moderate Mental Health Coverage and System Organization December 1, 2016 For Audio
Major Dimensions of Managed Behavioral Health Care Arrangements Level 3: MCO/BHO and Provider Contract
 Introduction To understand how managed care operates in a state or locality it may be necessary to collect organizational, financial and clinical management information at multiple levels. For instance,
Introduction To understand how managed care operates in a state or locality it may be necessary to collect organizational, financial and clinical management information at multiple levels. For instance,
Drug Medi-Cal Billing Manual. Substance Use Disorder Program, Policy, and Fiscal Division Fiscal Management and Accountability Branch
 Drug Medi-Cal Billing Manual Substance Use Disorder Program, Policy, and Fiscal Division Fiscal Management and Accountability Branch June 2017 Table of Contents INTRODUCTION... 3 1.1... Definitions of
Drug Medi-Cal Billing Manual Substance Use Disorder Program, Policy, and Fiscal Division Fiscal Management and Accountability Branch June 2017 Table of Contents INTRODUCTION... 3 1.1... Definitions of
Recovery Homes: Recovery and Health Homes under Health Care Reform
 Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Quality Improvement Work Plan Evaluation. Fiscal Year
 Quality Improvement Work Plan Evaluation Fiscal Year 2016-2017 Evaluation of FY 16-17 Quality Improvement Committee Goals For fiscal year 2016-2017, the SBCMHP QI Committee focused on five key areas. The
Quality Improvement Work Plan Evaluation Fiscal Year 2016-2017 Evaluation of FY 16-17 Quality Improvement Committee Goals For fiscal year 2016-2017, the SBCMHP QI Committee focused on five key areas. The
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD,
 econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
Affordable Care Act: Medi Cal Opportunities and Challenges An analysis for the Conrad N. Hilton Foundation s four domestic programs
 Affordable Care Act: Medi Cal Opportunities and Challenges An analysis for the Conrad N. Hilton Foundation s four domestic programs By Andrea Jones Domestic Programs Intern, The Conrad N. Hilton Foundation
Affordable Care Act: Medi Cal Opportunities and Challenges An analysis for the Conrad N. Hilton Foundation s four domestic programs By Andrea Jones Domestic Programs Intern, The Conrad N. Hilton Foundation