Meaningful Use Stage 2
|
|
|
- Barrie Armstrong
- 5 years ago
- Views:
Transcription
1 An Overview
2 Meaningful Use Stage 2 Today we will review what Stage 2 of Meaningful Use has in store for us. Please Fasten your seatbelts and make sure your seat backs and tray tables are in the full and upright position. Take a Deep Breath
3 17 Core and 6 Menu Measures We must either MEET or be Exempt from each of the 17 Core Measures We must MEET 3 of the 6 Menu Measures We can no longer claim an exemption from a Menu Measure and get credit for it.
4 CPOE
5 Laboratory Order Order for any service provided by a laboratory that could not be provided by a non-laboratory.
6 Laboratory A facility for the biological, microbiological, serological, chemical, immunohematological, hematological, biophysical, cytological, pathological, or other examination of from the human body for the purpose of providing information for the diagnosis, prevention, or treatment of any disease or impairment of, or the assessment of the health of, human beings. These examinations also include procedures to determine, measure, or otherwise describe the presence or absence of various substances or organisms in the body. Facilities only collecting or preparing specimens (or both) or only serving as a mailing service and not performing testing are not considered laboratories.
7 Radiology Order Order for any imaging services that uses electronic product radiation. YOU can include orders for other types of imaging services that do not rely on electronic product radiation in this definition as long the policy is consistent across all patient and for the entire EHR reporting period.
8 Electronic Product Radiation Any ionizing or nonionizing electromagnetic or particulate radiation, or [a]nysonic, infrasonic, or ultrasonic wave that is emitted from an electronic product as the result of the operation of an electronic circuit in such product. X Rays CT MRI Foot Scanners
9 Unique Patient If a patient is seen by an you more than once during the EHR reporting period, then for purposes of measurement that patient is only counted once in the denominator for the measure.
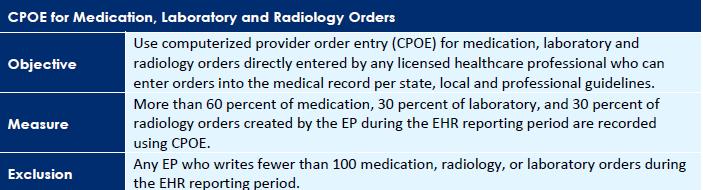
10 Part 1: Medication Orders DENOMINATOR: Number of medication orders created during the EHR reporting period. NUMERATOR: The number of orders in the denominator recorded using CPOE. THRESHOLD: The resulting percentage must be more than 60 percent in order to meet this measure. EXCLUSION: If you write fewer than 100 medication orders during the EHR reporting period.
11 Part 2: Imaging Orders DENOMINATOR: Number of imaging orders created during the EHR reporting period. NUMERATOR: The number of orders in the denominator recorded using CPOE. THRESHOLD: The resulting percentage must be more than 30 percent in order for you to meet this measure. EXCLUSION: If you write fewer than 100 imaging orders during the EHR reporting period.
12 Part 3: Laboratory Orders DENOMINATOR: Number of laboratory orders created during the EHR reporting period. NUMERATOR: The number of orders in the denominator recorded using CPOE. THRESHOLD: The resulting percentage must be more than 30 percent in order for you to meet this measure. EXCLUSION: If you write fewer than 100 laboratory orders during the EHR reporting period.
13 Additional Information You are permitted, but not required, to limit the measure of this objective to those patients whose records are maintained using certified EHR technology (CEHRT). Nursing Homes??? The CPOE function must be used to create the first record of the order that becomes part of the patient's medical record and before any action can be taken on the order to count in the numerator.
14 However, in some situations it may be impossible or inadvisable to wait to initiate an intervention until a record of the order has been created. For example, situations where an intervention is identified and immediately initiated by the provider, or initiated immediately after a verbal order by the ordering provider to a licensed healthcare professional under his/her direct supervision. Therefore in these situations, so long as the order is entered using CPOE by a licensed healthcare professional or certified medical assistant to create the first record of that order as it becomes part of the patient s medical record, these orders would count in the numerator of the CPOE measure.
15 Any licensed healthcare professionals and credentialed medical assistants, can enter orders into the medical if they can originate the order per state, local and professional guidelines. Credentialing for a medical assistant must come from an organization other than the organization employing the medical assistant.
16 Electronic transmittal of the medication order is not a requirement for meeting the measure of this objective. CPOE is the entry of the order into the patient's EHR that uses a specific function of CEHRT. It is not how that order is filled or otherwise carried out.
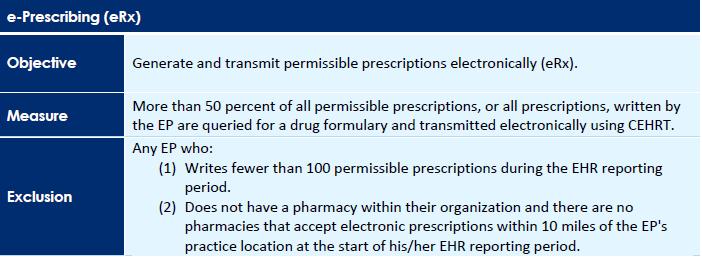
17 E- Prescribing
18 Definition of Terms Permissible Prescriptions The concept of only permissible prescriptions refers to the current restrictions established by the Department of Justice on electronic prescribing for controlled substances in Schedule II-V. (The substances in Schedule II-V can be found at ngebook/e_cs_sched.pdf). Any prescription not subject to these restrictions would be permissible.
19 Prescription The authorization by you to a pharmacist to dispense a drug that the pharmacist would not dispense to the patient without such authorization. AKA OTC Meds DO NOT COUNT.
20 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of prescriptions written for drugs requiring a prescription in order to be dispensed other than controlled substances during the EHR reporting period; or Number of prescriptions written for drugs requiring a prescription in order to be dispensed during the EHR reporting period. NUMERATOR: The number of prescriptions in the denominator generated, queried for a drug formulary and transmitted electronically using CEHRT. THRESHOLD: The resulting percentage must be more than 50 percent in order for you to meet this measure.
21 EXCLUSIONS: (1) If you write fewer than 100 permissible prescriptions during the EHR reporting period; or (2) If you do not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of your practice location at the start of the EHR reporting period.
22 Additional Information Authorizations for items such as durable medical equipment, or other items and services that may require your authorization before the patient could receive them, are not included in the definition of prescriptions. These are excluded from the numerator and the denominator of the measure.
23 As electronic prescribing of controlled substances is now possible, providers can choose to include all prescriptions or only permissible prescriptions as long as the decision applies to all patients and for the entire EHR reporting period. The determination of whether a prescription is a ''permissible prescription'' for purposes of this measure should be made based on the guidelines for prescribing Schedule II-V controlled substances in effect on or before January 13, 2010.
24 If you dispense the medication from your office, and enter the Rx into CPOE it IS considered electronic transmission. If the pharmacy clearing house takes the electronic transmission and converts it to fax it is still considered electronic transmission
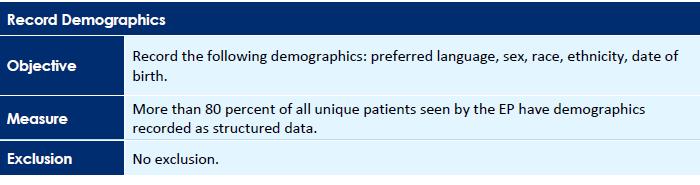
25 Record Demographics
26 Definition of Terms Preferred Language The language by which the patient prefers to communicate. You are NOT required to communicate with the patient in their preferred language.
27 DENOMINATOR/ NUMERATOR /THRESHOLD DENOMINATOR: Number of unique patients seen by you during the EHR reporting period. NUMERATOR: The number of patients in the denominator who have all the elements of demographics (or a specific notation if the patient declined to provide one or more elements or if recording an element is contrary to state law) recorded as structured data. THRESHOLD: The resulting percentage must be more than 80 percent in order to meet this measure.
28 Additional Information Race and ethnicity codes should follow current federal standards published by the Office of Management and Budget ( licy/#dr). So your EHR vendor did not make these up.
29 If a patient declines to provide all or part of the demographic information, or if capturing a patient s ethnicity or race is prohibited by state law, Or if patients who do not know their ethnicity, You should treat these patients the same way as patients who decline to provide race or ethnicity identify in the patient record that the patient declined to provide this information. These all count towards meeting the measure

30 Record Vital Signs
31 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of unique patients seen during the EHR reporting period. NUMERATOR: Number of patients in the denominator who have at least one entry of their height/length and weight (all ages) and/or blood pressure (ages 3 and over) recorded as structured data. THRESHOLD: The resulting percentage must be more than 80 percent in order for you to meet this measure.
32 EXCLUSIONS: Any EP who sees no patients 3 years or older is excluded from recording blood pressure. Any EP who believes that all 3 vital signs of height/length, weight, and blood pressure have no relevance to their scope of practice is excluded from recording them. Any EP who believes that height/length and weight are relevant to their scope of practice, but blood pressure is not, is excluded from recording blood pressure. Any EP who believes that blood pressure is relevant to their scope of practice, but height/length and weight are not, is excluded from recording height/length and weight.
33 Additional Information If you meet exclusion (3) or exclusion (4) you must both attest to the exclusion and report the numerator and denominator for the remaining elements of the measure. The only information required to be inputted by you is the height and weight, and/or blood pressure of the patient. The certified EHR technology will calculate BMI and the growth chart if applicable to patient based on age.
34 Height, weight, and blood pressure do not have to be updated at every patient encounter. You can make the determination based on the patient s individual circumstances as to whether height, weight, and blood pressure need to be updated.
35 Vital sign information can be entered into the patient's medical record in a number of ways including: direct entry by the you; entry by a designated individual from the your staff; data transfer from another provider electronically, through an HIE or through other methods; or data entered directly by the patient through a portal or other means. Some of these methods are more accurate than others, and it is up to the you to determine the level of accuracy needed to care for their patient and how best to obtain this information.

36 Record Smoking Status
37 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of unique patients age 13 or older seen during the EHR reporting period. NUMERATOR: The number of patients in the denominator with smoking status recorded as structured data. THRESHOLD: The resulting percentage must be more than 80 percent in order for you to meet this measure.
38 EXCLUSION: If you neither see nor admit to a hospital any patients 13 years old or older.
39 This is a check of the medical record for patients 13 years old or older. If this information is already in the medical record available through certified EHR technology, an inquiry does not need to be made every time a provider sees a patient 13 years old or older. The frequency of updating this information is left to the provider and guidance is provided already from several sources in the medical community.
40 To Be Continued. Questions

41 Clinical Decision Support
42 Definition of Terms Clinical Decision Support HIT functionality that builds upon the foundation of an EHR to provide persons involved in care processes with general and person-specific information, intelligently filtered and organized, at appropriate times, to enhance health and health care.
43 Attestation Requirements YES/NO You must attest YES to implementing five clinical decision support interventions and enabling and implementing functionality for drug-drug and drug-allergy interaction to meet this measure.
44 EXCLUSION: (Drug / Allergy Checks) If you write fewer than 100 medication orders during the EHR reporting period. There is NO exclusion for the 5 other CDS rules you must implement. (part 1 of the measure)
45 Additional Information Your Clinical Decision Support Rules must relate to a Clinical Quality Measure published by CMS. If none of the CQMs are applicable to your scope of practice, You should implement CDS interventions that you believe will to drive improvements in the delivery of care for the highpriority health conditions relevant to your patient population..
46 The need for inclusion of attributes for each CDS intervention also applies to drug-drug and drugallergy interventions as well as interventions based on self-generated evidence. Drug-drug and drug-allergy interaction alerts are separate from the 5 clinical decision support interventions and do not count towards the 5 required for this first measure.
47 CDS is tied to Evidence Based Medicine. You are required to select (i.e., activate) one or more electronic clinical decision support interventions (in addition to drug-drug and drug-allergy contraindication checking) based on each one and at least one combination of the following data: (A) Problem list; (B) Medication list; (C) Medication allergy list; (D) Demographics; (E) Laboratory tests and values/results; and (F) Vital signs.
48 The CDS Rule must be Linked Point to the EBM or Clinical Guideline that supports the CDS Rule

49 Patient Electronic Access
50 Definition of Terms Access When a patient possesses all of the necessary information needed to view, download, or transmit their information. This could include providing patients with instructions on how to access their health information, the website address they must visit for online access, a unique and registered username or password, instructions on how to create a login, or any other instructions, tools, or materials that patients need in order to view, download, or transmit their information.
51 View The patient (or authorized representative) actually uses the steps in the previous slide to access their health information online.
52 Transmission and Download Any means of electronic transmission Using physical electronic media (for example, USB, CD) does not qualify as transmission. The movement of the information from online to the physical electronic media will be a download. This means patients will need to be able to do BOTH Transmit and Download
53 Business Days Business days are defined as Monday through Friday excluding federal or state holidays on which the you or your respective administrative staffs are unavailable.
54 DENOMINATOR/NUMERATOR/ THRESHOLD Measure 1: DENOMINATOR: Number of unique patients seen during the EHR reporting period. NUMERATOR: The number of patients in the denominator who have timely (within 4 business days after the information is available to the you) online access to their health information. THRESHOLD: The resulting percentage must be more than 50 percent in order for you to meet this measure.
55 Measure 2: DENOMINATOR: Number of unique patients seen by the you during the EHR reporting period. NUMERATOR: The number of unique patients (or their authorized representatives) in the denominator who have viewed online, downloaded, or transmitted to a third party the patient's health information. THRESHOLD: The resulting percentage must be more than 5 percent in order for you to meet this measure.
56 EXCLUSIONS: (1) If you neither orders nor creates any of the information listed for inclusion as part of both measures, except for "Patient name" and "Provider's name and office contact information," may exclude both measures. <fuggedaboutit> (2) If 50 percent or more of your patient encounters are in a county that does not have 50 percent or more of its housing units with 3Mbps broadband availability according to the latest information available from the FCC on the first day of the EHR reporting period may exclude only the second measure.

57 Clinical Summaries
58 What is in a Clinical Summary Clinical Summary An after-visit summary that provides a patient with relevant and actionable information and instructions containing in no particular order: Patient name. Provider's name and office contact information. Date and location of the visit. Reason for the office visit. Current problem list. Current medication list. Current medication allergy list. Procedures performed during the visit. Immunizations or medications administered during the visit. Vital signs taken during the visit (or other recent vital signs). Laboratory test results. List of diagnostic tests pending. Clinical instructions. Future appointments. Referrals to other providers. Future scheduled tests. Demographic information maintained within certified electronic health record technology (CEHRT) (sex, race, ethnicity, date of birth, preferred language). Smoking status. Care plan field(s), including goals and instructions. Recommended patient decision aids (if applicable to the visit).
59 What is NOT in a Clinical Summary Your Chart Notes
60 Office Visit Office visits include separate, billable encounters that result from evaluation and management services provided to the patient and include: (1) Concurrent care or transfer of care visits, (2) Consultant visits, or (3) Prolonged Physician Service without Direct (Face-To-Face) Patient Contact (tele-health). A consultant visit occurs when a provider is asked to render an expert opinion/service for a specific condition or problem by a referring provider.
61 DENOMINATOR/ NUMERATOR/THRESHOLD DENOMINATOR: Number of office visits conducted during the EHR reporting period. NUMERATOR: Number of office visits in the denominator where the patient or a patientauthorized representative is provided a clinical summary of their visit within one (1) business day. THRESHOLD: The resulting percentage must be more than 50 percent in order for you to meet this measure.
62 EXCLUSION: If You have no office visits during the EHR reporting period.
63 Additional Information You are permitted, but not required, to limit the measure of this objective to those patients whose records are maintained using certified electronic health record technology (CEHRT). The provision of the clinical summary is limited to the information contained within CEHRT.
64 The clinical summary can be provided through a PHR patient portal on the web site secure electronic media such as CD or USB fob or printed copy. If you choose electronic media, You are required to provide the patient a paper copy upon request. You may also default to providing paper copies, in which case an electronic form of YOUR choice would need to be provided upon request
65 If you believe that substantial harm may arise from the disclosure of particular information, you may choose to withhold that particular information from the clinical summary. You may not charge patients a fee to provide this information. When a patient visit lasts several days or a patient is seen by multiple EPs, a single clinical summary at the end of the visit should be counted only once in both the numerator and denominator.
66 In the event that a clinical summary is offered to and subsequently declined by the patient, that patient may still be included in the numerator of the measure.

67 Patient Electronic Health Info
68 Attestation Requirements YES/NO You must attest YES to conducting or reviewing a security risk analysis and implementing security updates as needed to meet this measure. The most common cause for providers to fail Meaningful Use Audits is failure to meet this measure.
69 Additional Information You must conduct or review a security risk analysis of CEHRT including addressing encryption/security of data, and implement updates as necessary at least once prior to the end of the EHR reporting period and attest to that conduct or review. The testing could occur prior to the beginning of the first EHR reporting period. However, a new review would have to occur for each subsequent reporting period.
70 The parameters of the security risk analysis are defined 45 CFR (a)(1) which was created by the HIPAA Security Rule. Meaningful use does not impose new or expanded requirements on the HIPAA Security Rule nor does it require specific use of every certification and standard that is included in certification of EHR technology. More information on the HIPAA Security Rule can be found at ative/securityrule/.

71 Clinical Lab Test Results
72 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of lab tests ordered during the EHR reporting period by you whose results are expressed in a positive or negative affirmation or as a number. NUMERATOR: Number of lab test results which are expressed in a positive or negative affirmation or as a numeric result which are incorporated in CEHRT as structured data. THRESHOLD: The resulting percentage must be more than 55 percent in order for you to meet this measure.
73 EXCLUSION: If you do not order any lab tests where results are either in a positive/negative affirmation or numeric format during the EHR reporting period.

74 Patient Lists
75 Criteria Select, sort, access, and create patient lists by: date and time; and based on each one and at least one combination of the following data: (i) Problems; (ii) Medications; (iii) Medication allergies; (iv) Demographics; (v) Laboratory tests and values/results; and (vi) Ambulatory setting only - Patient communication preferences.
76 Attestation Requirements You must attest YES to having generated at least one report listing patients with a specific condition to meet this measure
77 Additional Information This objective does not dictate the report(s) which must be generated; therefore you or a member of the your staff could generate the list and meet this measure. You are best positioned to determine which reports are most useful to your care efforts.
78 The report generated could cover every patient whose records are maintained using certified EHR technology (CEHRT) or a subset of those patients at your discretion. Each EHR reporting period should be identified with a different report. Reports generated in past EHR reporting periods cannot be used to satisfy this measure in the current EHR reporting period.
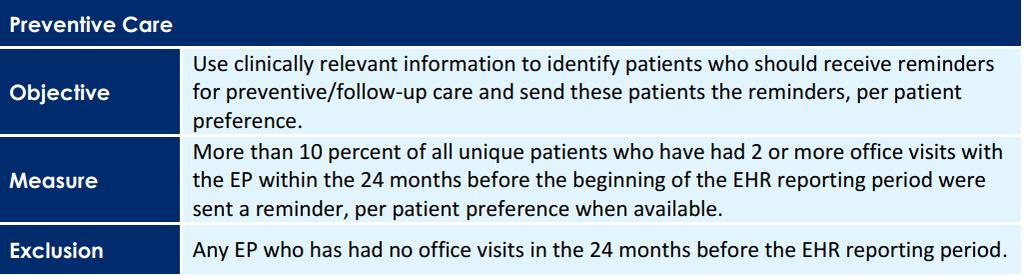
79 Preventive Care
80 Certification Criteria Select, sort, access, and create patient lists by: date and time; and based on each one and at least one combination of the following data: (i) Problems; (ii) Medications; (iii) Medication allergies; (iv) Demographics; (v) Laboratory tests and values/results; and (vi) Patient communication preferences.
81 Definition of Terms Patient Preference The method of communication that patients prefer to receive their reminders such as (but not limited to) by mail, by phone or by secure messaging. Active Patients Patients with at least two office visits in the last 24 months.
82 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of unique patients who have had two or more office visits in the 24 months prior to the beginning of the EHR reporting period. NUMERATOR: Number of patients in the denominator who were sent a reminder per patient preference when available during the EHR reporting period. THRESHOLD: The resulting percentage must be more than 10 percent in order for you to meet this measure.
83 EXCLUSION: Any EP who has had no office visits in the 24 months before the EHR reporting period.
84 Additional Information EPs meet the aspect of per patient preference of this objective if they are accommodating known reasonable requests in accordance with the HIPAA Privacy Rule, as specified at 45 CFR (b), which is the guidance established for accommodating patient requests.
85 You should use clinically relevant information stored within the CEHRT to identify patients who should receive reminders. To count for the measure, reminders for preventive/follow-up care must be for care that the patient is not already scheduled to receive. Reminders for referrals or to engage in certain activities are also included in this objective and measure.
86 Reminders must be sent using the preferred communication medium only when it is known by the provider. This is limited to the type of communication (phone, mail, secure messaging, etc.) and does not extend to other constraints like time of day. Patients may decline to provide their preferred communication medium in which case the provider may select the communication medium. A patient may also decline to receive reminders.

87 Patient Specific Education
88 DENOMINATOR / NUMERATOR / THRESHOLD DENOMINATOR: Number of unique patients with office visits seen during the EHR reporting period. NUMERATOR: Number of patients in the denominator who were provided patient-specific education resources identified by the Certified EHR Technology. THRESHOLD: The resulting percentage must be more than 10 percent in order for you to meet this measure.
89 EXCLUSION: Any EP who has no office visits during the EHR reporting period.
90 Education resources or materials do not have to be stored within or generated by the certified EHR. However, the provider should utilize certified EHR technology (CEHRT) in a manner where the technology suggests patient -specific educational resources based on the information stored in the CEHRT. The provider can make a final decision on whether the education resource is useful and relevant to a specific patient.
91 You may use these elements or additional elements within CEHRT to identify educational resource s specific to patients' needs. You can then provide these educational resources to patients in a useful format for the patient electronic copy printed copy electronic link to source materials through a patient portal or PHR.
92 If resources or topic area of resources are not identified by CEHRT and provided to the patient then it will not count in the numerator. The education resources will need to be provided
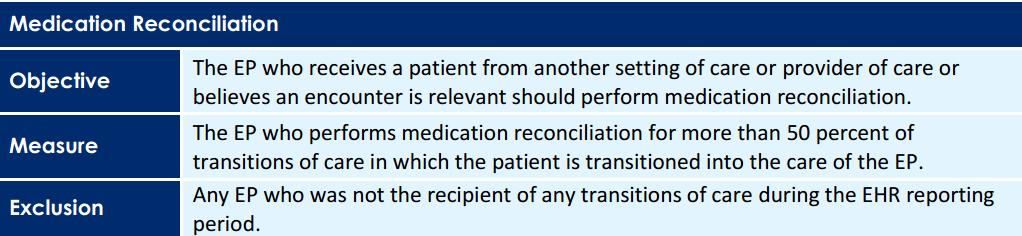
93 Medication Reconciliation
94 Criteria Electronically reconcile the data that represent a patient s active medication, problem, and medication allergy list as follows. For each list type: (i) Electronically and simultaneously display (i.e., in a single view) the data from at least two list sources in a manner that allows a user to view the data and their attributes, which must include, at a minimum, the source and last modification date. (ii) Create a single reconciled list of medications, medication allergies, or problems. (iii) Review and validate the accuracy of a final set of data and, upon a user s confirmation, automatically update the list.
95 Definition of Terms Medication Reconciliation The process of identifying the most accurate list of all medications that the patient is taking, including name, dosage, frequency, and route, by comparing the medical record to an external list of medications obtained from a patient, hospital, or other provider. Relevant Encounter An encounter during which the you perform a medication reconciliation due to new medication or long gaps in time between patient encounters or for other reasons determined appropriate by you. Essentially an encounter is relevant if you judges it to be so. Note: Relevant encounters may included in the numerator and denominator of the measure for this objective.
96 Transition of Care The movement of a patient from one clinical setting (inpatient, outpatient, physician office, home health, rehab, long-term care facility, etc.) to another or from one EP to another. At a minimum, transitions of care include first encounters with a new patient and encounters with existing patients where a summary of care record (of any type) is provided to the receiving provider. The summary of care record can be provided either by the patient or by the referring/transiting provider or institution.
97 DENOMINATOR/NUMERATOR/ THRESHOLD DENOMINATOR: Number of transitions of care during the EHR reporting period for which You are the receiving party of the transition. NUMERATOR: The number of transitions of care in the denominator where medication reconciliation was performed. THRESHOLD: The resulting percentage must be more than 50 percent in order for you to meet this measure.
98 EXCLUSION: Any EP who was not the recipient of any transitions of care during the EHR reporting period.
99 The electronic exchange of information is not a requirement for medication reconciliation. The measure of this objective does not dictate what information must be included in reconciliation. Information included in the process of reconciliation is appropriately determined by the provider and patient.

100 Summary of Care Pt 1

101 Summary of Care Pt 2
102 Definition of Terms Transition of Care The movement of a patient from one setting of care (hospital, ambulatory primary care practice, ambulatory, specialty care practice, long-term care, home health, rehabilitation facility) to another. At a minimum this includes all transitions of care and referrals that are ordered by you.
103 Summary of Care Record A summary of care record must include the following elements: Patient name. Referring or transitioning provider's name and office contact information (EP only). Procedures. Encounter diagnosis Immunizations. Laboratory test results. Vital signs (height, weight, blood pressure, BMI). Smoking status. Functional status, including activities of daily living, cognitive and disability status Demographic information (preferred language, sex, race, ethnicity, date of birth). Care plan field, including goals and instructions. Care team including the primary care provider of record and any additional known care team members beyond the referring or transitioning provider and the receiving provider. Reason for referral Current problem list (EPs may also include historical problems at their discretion). Current medication list, and Current medication allergy list.
104 Problem List At a minimum a list of current, active and historical diagnoses. We do not limit the EP to just including diagnoses on the problem list. Active/current medication list A list of medications that a given patient is currently taking. Active/current medication allergy list A list of medications to which a given patient has known allergies.
105 Allergy An exaggerated immune response or reaction to substances that are generally not harmful. Care Plan The structure used to define the management actions for the various conditions, problems, or issues. A care plan must include at a minimum the following components: problem (the focus of the care plan), goal (the target outcome) and any instructions that the provider has given to the patient. A goal is a defined target or measure to be achieved in the process of patient care (an expected outcome).
106 MEASURE 1: DENOMINATOR: Number of transitions of care and referrals during the EHR reporting period for which you were the transferring or referring provider. NUMERATOR: The number of transitions of care and referrals in the denominator where a summary of care record was provided. THRESHOLD: The percentage must be more than 50 percent in order for you to meet this measure.
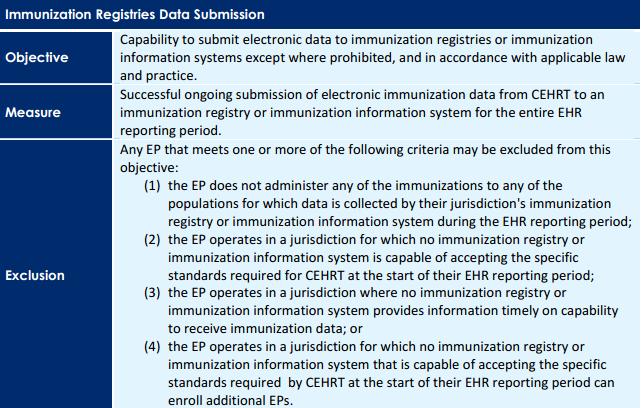
107 EXLCUSION: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the EHR reporting period is excluded from all three measures
108 MEASURE 2: DENOMINATOR: Number of transitions of care and referrals during the EHR reporting period for which you were the transferring or referring provider. NUMERATOR: The number of transitions of care and referrals in the denominator where a summary of care record was a) electronically transmitted using CEHRT to a recipient or b) where the recipient receives the summary of care record via exchange facilitated by an organization that is a NwHIN Exchange participant or in a manner that is consistent with the governance mechanism ONC establishes for the nationwide health information network. The organization can be a thirdparty or the sender's own organization. THRESHOLD: The percentage must be more than 10 percent in order for you to meet this measure.
109 EXCLUSION: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the EHR reporting period is excluded from all three measures
110 Measure 3 Lots of words there.. but. It means that you must at least test the exchange with another provider who has a different EHR than you. This is important if you work in an integrated setting where all docs have the same EHR program.
111 EXCLUSION: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the EHR reporting period is excluded from all three measures
112 If you refer a patient to a provider who uses THE SAME EHR as you. (Shared database) and they have access to your records you do not have to send a Summary of Care. To count in the numerator of any measure, you must verify these three fields are not blank for current problem list, current medication list, and current medication allergy list
113 To count in the numerator of measure 2, the summary of care record must be received by the provider to whom the sending provider is referring or transferring the patient.
114 Immunization Registry
115 Attestation Requirements YES/NO You must attest YES to meeting one of the following criteria under the umbrella of ongoing submission. Ongoing submission was already achieved for an EHR reporting period in a prior year and continues throughout the current EHR reporting period
116 Registration with the PHA or other body to whom the information is being submitted of intent to initiate ongoing submission was made by the deadline (within 60 days of the start of the EHR reporting period) and ongoing submission was achieved. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is still engaged in testing and validation of ongoing electronic submission. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is awaiting invitation to begin testing and validation
117 EXCLUSIONS : If you meet one or more of the following criteria you may be excluded from this objective: (1) Does not administer any of the immunizations to any of the populations for which data is collected by their jurisdiction's immunization registry or immunization information system during the EHR reporting period; (2) Operates in a jurisdiction for which no immunization registry or immunization information system is capable of accepting the specific standards required for CEHRT at the start of their EHR reporting period
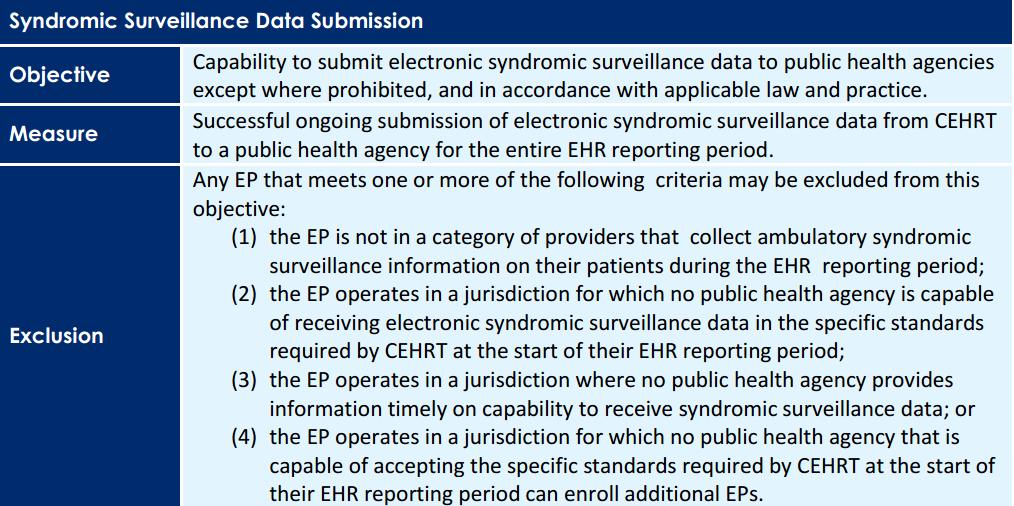
118 (3) Operates in a jurisdiction where no immunization registry or immunization information system provides information timely on capability to receive immunization data; or (4) Operates in a jurisdiction for which no immunization registry or immunization information system that is capable of accepting the specific standards required by CEHRT at the start of their EHR reporting period can enroll additional EPs

119 Secure Messaging
120 Definition of Terms Secure Message Any electronic communication between a provider and patient that ensures only those parties can access the communication. This electronic message could be the electronic messaging function of a PHR an online patient portal or any other electronic means
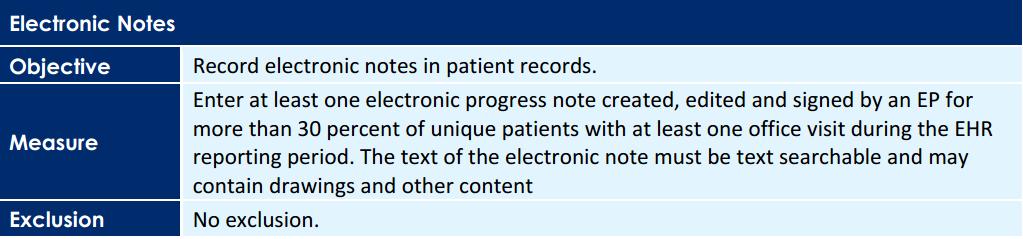
121 DENOMINATOR/ NUMERATOR/ THRESHOLD DENOMINATOR: Number of unique patients seen during the EHR reporting period. NUMERATOR: The number of patients or patientauthorized representatives in the denominator who send a secure electronic message to you that is received using the electronic messaging function of CEHRT during the EHR reporting period. THRESHOLD: The resulting percentage must be more than 5 percent in order for you to meet this measure.
122 EXCLUSION: If you have no office visits during the EHR reporting period, or you conduct 50 percent or more of your patient encounters in a county that does not have 50 percent or more of its housing units with 3Mbps broadband availability according to the latest information available from the FCC on the first day of the EHR reporting period.
123 The Menu Measures Yes there is more!!! And you can not claim an exemption you must meet 3 of these.
124 Syndromic Surveillance
125 Attestation Requirements YES / NO You must attest YES to successful ongoing submission of electronic syndromic surveillance data from CEHRT to a public health agency for the entire EHR reporting period. Ongoing submission was already achieved for an EHR reporting period in a prior year and continues throughout the current EHR reporting period. Registration with the PHA or other body to whom the information is being submitted of intent to initiate ongoing submission was made by the deadline (within 60 days of the start of the EHR reporting period) and ongoing submission was achieved. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is still engaged in testing and validation of ongoing electronic submission. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is awaiting invitation to begin testing and validation
126 EXCLUSIONS: Any EP that meets one or more of the following criteria may be excluded from this objective: (1) the EP is not in a category of providers that collect ambulatory syndromic surveillance information on their patients during the EHR reporting period; (2) the EP operates in a jurisdiction for which no public health agency is capable of receiving electronic syndromic surveillance data in the specific standards required by CEHRT at the start of their EHR reporting period; (3) the EP operates in a jurisdiction where no public health agency provides information timely on capability to receive syndromic surveillance data; or (4) the EP operates in a jurisdiction for which no public health agency that is capable of accepting the specific standards required by CEHRT at the start of their EHR reporting period can enroll additional EPs.
127 Sorry. You probably wont be able to meet Syndromic Survellience.
128 Electronic Notes
129 Definition of Terms Electronic Notes Defined as electronic progress notes. CMS will rely on providers own determinations and guidelines defining when progress notes are necessary to communicate individual patient circumstances and for coordination with previous documentation of patient observations, treatments and/or results in the electronic health record
130 DENOMINATOR /NUMERATOR/ THRESHOLD DENOMINATOR: Number of unique patients with at least one office visit during the EHR reporting period NUMERATOR: The number of unique patients in the denominator who have at least one electronic progress note from an eligible professional recorded as text searchable data. THRESHOLD: The resulting percentage must be more than 30 percent in order for you to meet this measure
131 Additional Information An EP or authorized provider may author, edit and sign the note in any manner including dictation, conversion of written notes to text searchable notes, direct entry into the EHR or any other method as long as the end result is a text searchable note that is the information that the EP or authorized provider wanted to note.
132 Non-searchable notes do not qualify, but this does not mean that all of the content has to be character text. Drawings and other content can be included with searchable text notes under this measure
133 Ok that is 1 Meanure Measure you can meet. 2 to go.

134 Imaging Results
135 Definition of Terms Imaging The description of radiology services from the Stage 2 CPOE objective is the minimum description of imaging.
136 Electronic Product Radiation Any ionizing or nonionizing electromagnetic or particulate radiation, or [a]nysonic, infrasonic, or ultrasonic wave that is emitted from an electronic product as the result of the operation of an electronic circuit in such product. X Rays CT MRI Foot Scanners
137 Accessible through Either incorporation of the image and accompanying information into CEHRT or an indication in CEHRT that the image and accompanying information are available for a giving patient in another technology and a link to that image and accompanying information. Incorporation of the I mage The image and accompanying information is stored by the CEHRT
138 DENOMINATOR / NUMERATOR / THRESHOLD DENOMINATOR: Number of tests whose result is one or more images ordered by you during the EHR reporting period. NUMERATOR: The number of results in the denominator that are accessible through CEHRT. THRESHOLD : The resulting percentage must be more than 10 percent in order to meet this measure.
139 EXCLUSION : Any EP who orders less than 100 tests whose result is an image during the EHR reporting period; or any EP who has no access to electronic imaging results at the start of the EHR reporting period Do you ever receive any MRI or CT on a disk? Can you view digital x rays over the internet?
140 Additional Information There are no limitations on the resolution of the image. Storing the images natively in CEHRT is one way to make them accessible through CEHRT, but there are many other ways and native storage is not required by the objective and measure. Images and imaging results that are scanned into the CEHRT may be counted in the numerator of this measure.
141 May be difficult But not impossible So that is 2 of 3 And yes you do need to do this one because There is really only 1 more you can count on being able to do.

142 Family Health History
143 Definition of Terms First Degree R elative A family member who shares about 50 percent of their genes with a particular individual in a family. First degree relatives include parents, offspring, and siblings.
144 DENOMINATOR / NUMERATOR / THRESHOLD DENOMINATOR: Number of unique patients seen by you during the EHR reporting period. NUMERATOR: The number of patients in the denominator with a structured data entry for one or more first-degree relatives. THRESHOLD: The resulting percentage must be more than 20 percent in order to meet this measure.
145 EXCLUSION: Any EP who has no office visits during the EHR reporting period
146 Additional Information This measure is a minimum and not a limitation on the health history that can be recorded. For patients who are asked about their family health history, but do not know their family history, it is acceptable for the provider to record the patient's family history as "unknown."
147 3 of 3 This is a relatively easy one. This gives you 3 menu measures you can meet.

148 Cancer Registry
149 Attestation Requirements YES/NO You must attest YES to successful ongoing submission of cancer case information from certified electronic health record technology ( CEHRT ) to a public health central cancer registry for the entire EHR reporting period. Ongoing submission was already achieved for an EHR reporting period in a prior year and continues throughout the current EHR reporting period. Registration with the PHA or other body to whom the information is being submitted of intent to initiate ongoing submission was made by the deadline (within 60 days of the start of the EHR reporting period) and ongoing submission was achieved.
150 Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is still engaged in testing and validation of ongoing electronic submission. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is awaiting invitation to begin testing and validation.
151 EXCLUSIONS: Any EP that meets at least 1 of the following criteria may be excluded from this objective: (1) The EP does not diagnose or directly treat cancer; (2) t he EP operates in a jurisdiction for which no public health agency is capable of receiving electronic cancer case information in the specific standards required for CEHRT at the beginning of their EHR reporting period; (3) the EP operates in a jurisdiction where no PHA provides information timely on capability to receive electronic cancer case information; or (4) the EP operates in a jurisdiction for which no public health agency that is capable of receiving electronic cancer case information in the specific standards required for CEHRT at the beginning of their EHR reporting period can enroll additional EPs
152 Why Bother? Lots of text explaining our exclusions but We can not claim an exclusion to a menu measure. We can not count on being able to meet the cancer registry measure.
153 Other Registries
154 Definition of Terms Specialized Registry Sponsored by national specialty societies and specialized registries maintained by public health agencies.
155 Attestation Requirements YES/NO You must attest YES to successfully submitting specific case information from CEHRT to a specialized registry for the entire reporting period to meet this measure. Ongoing submission was already achieved for an EHR reporting period in a prior year and continues throughout the current EHR reporting period.
156 Registration with the PHA or other body to whom the information is being submitted of intent to initiate ongoing submission was made by the deadline (within 60 days of the start of the EHR reporting period) and ongoing submission was achieved. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is still engaged in testing and validation of ongoing electronic submission. Registration of intent to initiate ongoing submission was made by the deadline and the EP or hospital is awaiting invitation to begin testing and validation.
157 EXCLUSIONS: Any EP that meets at least 1 of the following criteria may be excluded from this objective: (1) The EP does not diagnose or directly treat any disease associated with a specialized registry sponsored by a national specialty society for which the EP is eligible, or the public health agencies in their jurisdiction; (2) The EP operates in a jurisdiction for which no specialized registry sponsored by a public health agency or by a national specialty society for which the EP is eligible is capable of receiving electronic specific case information in the specific standards required by CEHRT at the beginning of their EHR reporting period ;
158 (3) The EP operates in a jurisdiction where no public health agency or national specialty society for which the EP is eligible provides information timely on capability to receive information into their specialized registries; or (4) The EP operates in a jurisdiction for which no specialized registry sponsored by a public health agency or by a national specialty society for which the EP is eligible that is capable of receiving electronic specific case information in the specific standards required by CEHRT at the beginning of their EHR reporting period can enroll additional EPs
159 Are they KIDDING? Other Registries?? We can not count on this either.
160 An Now for Something Completely Different Changes to Stage 1 Yes there have been some
161 Computerized Provider Order Entry (CPOE) Beginning in 2013, CMS is adding an optional alternate measure to the objective for computerized provider order entry (CPOE). The current measure for CPOE is based on the number of unique patients with a medication in their medication list that was entered using CPOE. The new, alternate measure is based on the total number of medication orders created during the EHR reporting period.
162 An EP, eligible hospital, or CAH may select either measure for this objective in Stage 1 in order to achieve meaningful use. (Note that this alternative measure will be required for all providers in Stage 2.) Alternate Measure: More than 30 percent of medication orders created by the EP or authorized providers of the eligible hospital's or CAH's inpatient or emergency department (POS 21 or 23) during the EHR reporting period are recorded using CPOE
163 Electronic Prescribing Beginning in 2013, CMS is adding an additional exclusion to the objective for electronic prescribing for providers who are not within a 10 mile radius of a pharmacy that accepts electronic prescriptions.
164 New Additional Exclusion: Any EP who: does not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR reporting period.
165 Record and Chart Changes in Vital Signs CMS is changing the measure of the objective for recording and charting changes in vital signs for EPs, eligible hospitals, and CAHs. The current measure specifies that vital signs must be recorded for more than 50 percent of all unique patients ages 2 and over. The new measure amends that age limit to recording blood pressure for patients ages 3 and over and height and weight for patients of all ages.
166 The exclusions for this objective for EPs are also changing. The current exclusions only allow an EP to claim the exclusion if all three vital signs (height, weight, blood pressure) are not relevant to their scope of practice or if the EP sees n o patients 2 years or older. However, under the new Stage 1 changes, an EP can claim an exclusion if the EP sees no patients 3 years or older (the EP would not have to record blood pressure), if all three vital signs are not relevant to their scope of practice (the EP would not record any vital signs), if height and weight are not relevant to their scope of practice (the EP would still record blood pressure), or if blood pressure is not relevant to their scope of practice (the EP would still record height and weight).
167 This new measure and these new exclusions are optional in 2013 but will be required in 2014 and beyond
168 New Measure: More than 50 percent of all unique patients seen by the EP or admitted to the eligible hospital's or CAH's inpatient or emergency department (POS 21 or 23) during the EHR reporting period have blood pressure (for patients age 3 and over only) and height and weight (for all ages) recorded as structured data
169 New Exclusion: Any EP who 1. Sees no patients 3 years or older is excluded from recording blood pressure; 2. Believes that all three vital signs of height, weight, and blood pressure have no relevance to their scope of practice is excluded from recording them; 3. Believes that height and weight are relevant to their scope of practice, but blood pressure is not, is excluded from recording blood pressure; or 4. Believes that blood pressure is relevant to their scope of practice, but height and weight are not, is excluded from recording height and weight
170 Electronic Exchange of Key Clinical Information Beginning in 2013, the objective for electronic exchange of key clinical information will no longer be required for Stage 1 for EPs, eligible hospitals, and CAHs. Providers faced numerous challenges in understanding the requirements for this objective, so we are moving instead to a more robust requirement for electronic health information exchange as a part of the Stage 2 objective for providing a summary of care record following a transition of care or referral.
171 Report Clinical Quality Measures Beginning in 2013, there will no longer be a separate objective for reporting ambulatory or hospital clinical quality measures as a part of meaningful use. It is important to note, however, that EPs, eligible hospitals, and CAHs will still be required to report on clinical quality measures in order to achieve meaningful use. CMS is simply removing the standalone objective that requires providers to attest that they plan to report on clinical quality measures because it is redundant.
172 Electronic Copy of and Electronic Access to Health Information In order to better align Stage 1 objectives with the new 2014 capabilities of Certified EHR Technology, CMS is replacing several Stage 1 objectives for providing electronic copies of and electronic access to health information with objectives to provide patients the ability to view, download, or transmit their health information or hospital admission information online. The capability to provide patients online access to this information will be a part of Certified EHR Technology beginning in 2014, therefore the new Stage 1 objectives will be required beginning in
173 Public Health Reporting Objectives Beginning in 2013, all of the Stage 1 public health objectives (submitting data to an immunization registry, submitting data to a syndromic surveillance database, or submitting reportable lab results to a public health agency) will require that providers perform at least one test of their Certified EHR Technology s capability to send data to public health agencies, except where prohibited. The intent of this modification is to encourage all EPs, eligible hospitals, and CAHs to submit public health data, even when not required by State/local law. Therefore, if providers are authorized to submit the data, they should do so even if it is not required by either law or practice. If the test of submission is successful, provider should institute regular reporting with the entity with whom the successful test was conducted.

174 Questions Presented By Michael L. Brody, DPM Sponsored By ICS Software, Ltd.
during the EHR reporting period.
 CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1
 STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 2
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Qualifying for Medicare Incentive Payments with Crystal Practice Management. Version 1.0
 Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016
 Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Final Meaningful Use Objectives for
 Final Meaningful Use Objectives Modified Stage 2 All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition CEHRT. Stage 2 Objective Protect Health Information Clinical Decision
Final Meaningful Use Objectives Modified Stage 2 All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition CEHRT. Stage 2 Objective Protect Health Information Clinical Decision
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Final Meaningful Use Objectives for
 Final Meaningful Use Objectives All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition CEHRT. Stage 2 Objective Protect Health Information Clinical Decision Support Stage 2
Final Meaningful Use Objectives All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition CEHRT. Stage 2 Objective Protect Health Information Clinical Decision Support Stage 2
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
Final Meaningful Use Objectives for 2017
 Final Meaningful Use Objectives Modified Stage 2 All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition or a combination of 2014 & 2015 CEHRT. Stage 2 Objective Protect Health
Final Meaningful Use Objectives Modified Stage 2 All Eligible Professionals (EP) must attest to all objectives using a 2014 Edition or a combination of 2014 & 2015 CEHRT. Stage 2 Objective Protect Health
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 1
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Meaningful Use - Modified Stage Alternate Exclusions and/or Specifications
 Objectives Measures for EPs in 2016 Objective 1: Protect Patient Health Information Measure: Conduct or review a security risk analysis in accordance with the requirements in 45 CFR 164.308(a)(1), including
Objectives Measures for EPs in 2016 Objective 1: Protect Patient Health Information Measure: Conduct or review a security risk analysis in accordance with the requirements in 45 CFR 164.308(a)(1), including
Stage 2 Eligible Professional Meaningful Use Core and Menu Measures. User Manual/Guide for Attestation using encompass 3.0
 Stage 2 Eligible Professional Meaningful Use Core and Menu Measures User Manual/Guide for Attestation using encompass 3.0 Prepared By: Arête Healthcare Services, LLC Document Version: V1.0 9/02/2015 Eligible
Stage 2 Eligible Professional Meaningful Use Core and Menu Measures User Manual/Guide for Attestation using encompass 3.0 Prepared By: Arête Healthcare Services, LLC Document Version: V1.0 9/02/2015 Eligible
Stage 2 Meaningful Use Objectives and Measures
 Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures
 CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures Stage 2 MU Objectives and Measures for EHs - Core More than 60 percent of medication, 1. Use CPOE for medication,
CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures Stage 2 MU Objectives and Measures for EHs - Core More than 60 percent of medication, 1. Use CPOE for medication,
FINAL Meaningful Use Objectives for
 Meaningful Use s All Eligible Professionals (EP) and Eligible Hospitals (EH) must attest to all objectives using a 2014 Edition CEHRT. Protect Electronic Health Information Protect electronic health information
Meaningful Use s All Eligible Professionals (EP) and Eligible Hospitals (EH) must attest to all objectives using a 2014 Edition CEHRT. Protect Electronic Health Information Protect electronic health information
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013
 Summary of Care Objective Measure Exclusion Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013 The eligible hospital or CAH who transitions
Summary of Care Objective Measure Exclusion Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013 The eligible hospital or CAH who transitions
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE. Angel L. Moore, MAEd, RHIA Eastern AHEC REC
 THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet
 EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet CMS published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet CMS published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and
EHR Incentive Programs: 2015 through 2017 (Modified Stage 2) Overview
 Overview") EHR Incentive Programs: 2015 through (Modified Stage 2) Overview CMS recently released a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and critical access hospitals
EHR Incentive Programs: 2015 through (Modified Stage 2) Overview CMS recently released a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and critical access hospitals
Stage 1 Meaningful Use Objectives and Measures
 Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
MEANINGFUL USE STAGE FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
Meaningful Use - Modified Stage 2. Brett Paepke, OD David Wolfson Marni Anderson
 Meaningful Use - Modified Stage 2 Brett Paepke, OD David Wolfson Marni Anderson Wait! Where did Stage 1 and Stage 2 go? Traditional stages eliminated in late 2015 in order to: 1. reduce reporting requirements
Meaningful Use - Modified Stage 2 Brett Paepke, OD David Wolfson Marni Anderson Wait! Where did Stage 1 and Stage 2 go? Traditional stages eliminated in late 2015 in order to: 1. reduce reporting requirements
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Stage 2 Eligible Professional Meaningful Use Core Measures Measure 15 of 17 Last Updated: November 2013
 Summary of Care Objective Measures Exclusion Table of Contents Stage 2 Eligible Professional Meaningful Use Core Measures Measure 15 of 17 Last Updated: November 2013 The EP who transitions their patient
Summary of Care Objective Measures Exclusion Table of Contents Stage 2 Eligible Professional Meaningful Use Core Measures Measure 15 of 17 Last Updated: November 2013 The EP who transitions their patient
Stage 1 Changes Tipsheet Last Updated: August, 2012
 Stage 1 Changes Tipsheet Last Updated: August, 2012 Overview CMS recently announced some changes to the Stage 1 meaningful use objectives, measures, and exclusions for eligible professionals (EPs), eligible
Stage 1 Changes Tipsheet Last Updated: August, 2012 Overview CMS recently announced some changes to the Stage 1 meaningful use objectives, measures, and exclusions for eligible professionals (EPs), eligible
Eligible Professional Core Measure Frequently Asked Questions
 Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)*
*") 2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)* n In order for an EP to be considered a meaningful electronic health record (EHR) user, at least 50 percent of the EP s patient
2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)* n In order for an EP to be considered a meaningful electronic health record (EHR) user, at least 50 percent of the EP s patient
Practice Director Modified Stage MU Guide 03/17/2016
 Table of Contents General Info & Meaningful Use Report....4-7 Measures..........8-62 Objective 1: Protect Electronic Health Information 8 Conduct or Review a security risk analysis Objective 2: Clinical
Table of Contents General Info & Meaningful Use Report....4-7 Measures..........8-62 Objective 1: Protect Electronic Health Information 8 Conduct or Review a security risk analysis Objective 2: Clinical
Meaningful Use CHCANYS Webinar #1
 Meaningful Use 2016 CHCANYS Webinar #1 Ekem Merchant -Bleiberg, Director of Implementation Services Alliance of Chicago Wednesday February 24, 2016 Agenda 2016 Meaningful Use Guidelines Timelines & Deadlines
Meaningful Use 2016 CHCANYS Webinar #1 Ekem Merchant -Bleiberg, Director of Implementation Services Alliance of Chicago Wednesday February 24, 2016 Agenda 2016 Meaningful Use Guidelines Timelines & Deadlines
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Core Measure Set. Status. MU1 Increase from 30% New. Computerized Physician Order Entry Use computerized provider order. NextGen EHR Medication Module
 Bridge to Meaningful Use: Stage 2 Our Bridge to Meaningful Use connects the various measurements of the EHR Incentives to their respective counterparts in the EHR system. By utilizing the software and
Bridge to Meaningful Use: Stage 2 Our Bridge to Meaningful Use connects the various measurements of the EHR Incentives to their respective counterparts in the EHR system. By utilizing the software and
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use What You Need to Know for December 6, 2016
 Meaningful Use What You Need to Know for 2016-2017 December 6, 2016 Agenda Overview of Programs Eligibility Requirements Timeframes & Reporting Periods When you need to Upgrade Measures to Meet 2016 &
Meaningful Use What You Need to Know for 2016-2017 December 6, 2016 Agenda Overview of Programs Eligibility Requirements Timeframes & Reporting Periods When you need to Upgrade Measures to Meet 2016 &
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Meaningful Use and PCC EHR. Tim Proctor Users Conference 2017
 Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011
 Meaningful Use Final Objectives and Measures for Stage 1, 2011") Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
Meaningful Use Stage 2. Physician Office October, 2012
 Meaningful Use Stage 2 Physician Office October, 2012 Why are we here? Meaningful Use overview NOT Stage 1 requirements NOT Interesting facts Stage 1 - The Moving Target Stage 2 Final Rule Penalties Audits
Meaningful Use Stage 2 Physician Office October, 2012 Why are we here? Meaningful Use overview NOT Stage 1 requirements NOT Interesting facts Stage 1 - The Moving Target Stage 2 Final Rule Penalties Audits
EHR/Meaningful Use
 EHR/Meaningful Use 2015-2017 The requirements for Meaningful Use attestation have changed due to the recently released Medicare and Medicaid Programs: Electronic Health Record Incentive Program Stage 3
EHR/Meaningful Use 2015-2017 The requirements for Meaningful Use attestation have changed due to the recently released Medicare and Medicaid Programs: Electronic Health Record Incentive Program Stage 3
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
INTERGY MEANINGFUL USE 2014 STAGE 2 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 2 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 2 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
of 23 Meaningful Use 2015 PER THE CMS REVISION TO THE FINAL RULE RELEASED OCTOBER 6, 2015 CHARTMAKER MEDICAL SUITE
 1 Meaningful Use 2015 PER THE CMS REVISION TO THE FINAL RULE RELEASED OCTOBER 6, 2015 CHARTMAKER MEDICAL SUITE WHEN WE ARE FINISHED TODAY YOU SHOULD KNOW THE FOLLOWING. 2 EHR reporting periods Amended
1 Meaningful Use 2015 PER THE CMS REVISION TO THE FINAL RULE RELEASED OCTOBER 6, 2015 CHARTMAKER MEDICAL SUITE WHEN WE ARE FINISHED TODAY YOU SHOULD KNOW THE FOLLOWING. 2 EHR reporting periods Amended
The History of Meaningful Use
 A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
How to Participate Today 4/28/2015. HealthFusion.com 2015 HealthFusion, Inc. 1. Meaningful Use Stage 3: What the Future Holds
 Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Meaningful Use Roadmap Stage : Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Stage 2 requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Stage 2 requirements,
Meaningful Use Participation Basics for the Small Provider
 Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Virtual Office Hours Webinar for Eligible Providers and Hospitals
 Meaningful Use Virtual Office Hours Webinar for Eligible Providers and Hospitals Patti Kritzberger, RHIT, CHPS Tracey Regimbal, RHIT HIT-Quality Improvement Specialists Jane Stotts, BSN Quality Improvement
Meaningful Use Virtual Office Hours Webinar for Eligible Providers and Hospitals Patti Kritzberger, RHIT, CHPS Tracey Regimbal, RHIT HIT-Quality Improvement Specialists Jane Stotts, BSN Quality Improvement
MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE
 MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE *Please note, the below guidelines are currently proposed. ASCRS will let you know if and when they are finalized through regulatory alerts
MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE *Please note, the below guidelines are currently proposed. ASCRS will let you know if and when they are finalized through regulatory alerts
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage
 PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
Meaningful Use 2016 and beyond
 Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
Beyond Meaningful Use: Driving Improved Quality. CHCANYS Webinar #1: December 14, 2016
 Beyond Meaningful Use: Driving Improved Quality CHCANYS Webinar #1: December 14, 2016 Agenda The Current State Measuring Monitoring & Reporting Quality. Meaningful Use 2018 and Beyond The New Quality Payment
Beyond Meaningful Use: Driving Improved Quality CHCANYS Webinar #1: December 14, 2016 Agenda The Current State Measuring Monitoring & Reporting Quality. Meaningful Use 2018 and Beyond The New Quality Payment
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Travis Broome AMIA
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Medicaid Provider Incentive Program
 Medicaid Provider Incentive Program The Road to Meaningful Use Ohio Association of Community Health Centers 2013 Spring Conference March 6, 2013 Presenters: Elbony McIntyre, Project Manager Emma Esmont,
Medicaid Provider Incentive Program The Road to Meaningful Use Ohio Association of Community Health Centers 2013 Spring Conference March 6, 2013 Presenters: Elbony McIntyre, Project Manager Emma Esmont,
Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care
 Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period
 Advancing Care Information Performance Category Transition Measure 2018 Performance Period") Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Exclusion: Measure Exclusion ID: Health
Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Exclusion: Measure Exclusion ID: Health
GE Healthcare. Meaningful Use 2014 Prep: Core Part 1. Ramsey Antoun, Training Operations Coordinator December 12, 2013
 GE Healthcare Meaningful Use 2014 Prep: Core Part 1 Ramsey Antoun, Training Operations Coordinator December 12, 2013 2013 General Electric Company All rights reserved. This does not constitute a representation
GE Healthcare Meaningful Use 2014 Prep: Core Part 1 Ramsey Antoun, Training Operations Coordinator December 12, 2013 2013 General Electric Company All rights reserved. This does not constitute a representation
Medicaid EHR Incentive Program What You Need to Know about Program Year 2016
 Medicaid EHR Incentive Program What You Need to Know about Program Year 2016 February 2017 Carrie Ortega, Health IT Project Manager Imeincentives@dhs.state.ia.us 1 Attestation Reminders 2016 Dates to Remember
Medicaid EHR Incentive Program What You Need to Know about Program Year 2016 February 2017 Carrie Ortega, Health IT Project Manager Imeincentives@dhs.state.ia.us 1 Attestation Reminders 2016 Dates to Remember
Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information
 2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
EHR Meaningful Use Guide
 EHR Meaningful Use Guide for Stage I (2011) HITECH Attestation Version 2.0 Updated May/June 2014 in partnership with 1-866-611-5428 herfert@medicfusion.com www.medicfusion.com/herfert Medicfusion EMR V1.1
EHR Meaningful Use Guide for Stage I (2011) HITECH Attestation Version 2.0 Updated May/June 2014 in partnership with 1-866-611-5428 herfert@medicfusion.com www.medicfusion.com/herfert Medicfusion EMR V1.1
A complete step by step guide on how to achieve Meaningful Use Core Set Measures in Medgen EHR.
 Medgen EHR A complete step by step guide on how to achieve Meaningful Use Core Set Measures in Medgen EHR. Contents Important information regarding Meaningful Use... 2 How to generate your measure report
Medgen EHR A complete step by step guide on how to achieve Meaningful Use Core Set Measures in Medgen EHR. Contents Important information regarding Meaningful Use... 2 How to generate your measure report
Meaningful Use Reporting period for 2017: Change: Any consecutive 90 days in 2017 for Medicaid customers only.
 Meaningful Use 2017 Reporting period for 2017: Change: Any consecutive 90 days in 2017 for Medicaid customers only. Who needs to report on Meaningful Use for 2017? Medicaid customers who have 30 % Medicaid
Meaningful Use 2017 Reporting period for 2017: Change: Any consecutive 90 days in 2017 for Medicaid customers only. Who needs to report on Meaningful Use for 2017? Medicaid customers who have 30 % Medicaid
CMS Meaningful Use Proposed Rules Overview May 5, 2015
 CMS Meaningful Use Proposed Rules Overview May 5, 2015 Elisabeth Myers Center for Clinical Standards and Quality Centers for Medicare & Medicaid Services Disclaimer» CMS must protect the rulemaking process
CMS Meaningful Use Proposed Rules Overview May 5, 2015 Elisabeth Myers Center for Clinical Standards and Quality Centers for Medicare & Medicaid Services Disclaimer» CMS must protect the rulemaking process
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
Meaningful Use Stage 2 For Eligible and Critical Access Hospitals
 Meaningful Use Stage 2 For Eligible and Critical Access Hospitals Eileen Colen This material was prepared by HealthInsight, the Medicare Quality Improvement Organization for Nevada and Utah, under contract
Meaningful Use Stage 2 For Eligible and Critical Access Hospitals Eileen Colen This material was prepared by HealthInsight, the Medicare Quality Improvement Organization for Nevada and Utah, under contract
ecw and NextGen MEETING MU REQUIREMENTS
 ecw and NextGen MEETING MU REQUIREMENTS ecw version 9.0 is Meaningful Use certified and will be upgraded in Munson hosted practices. Anticipated to be released the end of February. NextGen application
ecw and NextGen MEETING MU REQUIREMENTS ecw version 9.0 is Meaningful Use certified and will be upgraded in Munson hosted practices. Anticipated to be released the end of February. NextGen application
Measure: Patient name. Referring or transitioning healthcare provider's name and office contact information (MIPS eligible clinician only) Procedures
 Procedures") Objective: Measure: Health Information Exchange Health Information Exchange The MIPS eligible clinician that transitions or refers their patient to another setting of care or health care clinician (1)
Objective: Measure: Health Information Exchange Health Information Exchange The MIPS eligible clinician that transitions or refers their patient to another setting of care or health care clinician (1)
CMS EHR Incentive Programs Overview
 CMS EHR Incentive Programs Overview Elizabeth Holland and Robert Anthony Session 20, Room 320 Monday, February 24 at 11:30 AM DISCLAIMER: The views and opinions expressed in this presentation are those
CMS EHR Incentive Programs Overview Elizabeth Holland and Robert Anthony Session 20, Room 320 Monday, February 24 at 11:30 AM DISCLAIMER: The views and opinions expressed in this presentation are those
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal. Lori Hack & Val Tuerk, Object Health
 Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA
 REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
HIE Implications in Meaningful Use Stage 1 Requirements
 s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
HIE Implications in Meaningful Use Stage 1 Requirements
 HIE Implications in Meaningful Use Stage 1 Requirements HIMSS 2010-2011 Health Information Exchange Committee November 2010 The inclusion of an organization name, product or service in this publication
HIE Implications in Meaningful Use Stage 1 Requirements HIMSS 2010-2011 Health Information Exchange Committee November 2010 The inclusion of an organization name, product or service in this publication
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals
 The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
Sevocity v Advancing Care Information User Reference Guide
 Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
Meaningful Use for 2014 Stag St e ag 1 Or Or Stag St e ag e 2 For Fo r 2014? Meaningful Meaningful Use: Stag St e ag e 1 1 Fo r Fo 2014
 Meaningful Use for 2014 Gerald E. Meltzer MD MSHA Medical Director imedicware Stage 1 Or Stage 2 For 2014? Meaningful Use: Stage 1 For 2014 1 Key Changes for 2014 Patient Electronic Access Clinical Quality
Meaningful Use for 2014 Gerald E. Meltzer MD MSHA Medical Director imedicware Stage 1 Or Stage 2 For 2014? Meaningful Use: Stage 1 For 2014 1 Key Changes for 2014 Patient Electronic Access Clinical Quality
HITECH Act American Recovery and Reinvestment Act (ARRA) Stimulus Package. HITECH Act Meaningful Use (MU)
 Stimulus Package. HITECH Act Meaningful Use (MU)") Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
Meaningful use glossary and requirements table
 Meaningful use glossary and requirements table 2011 2012 Glossary...2 Requirements table...3. Exclusions...12 Meaningful use glossary The following spreadsheet describes the requirements an eligible professional
Meaningful use glossary and requirements table 2011 2012 Glossary...2 Requirements table...3. Exclusions...12 Meaningful use glossary The following spreadsheet describes the requirements an eligible professional
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs. September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto
 2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
HIE and Meaningful Use Stage 2 Matrix
 HIE and Meaningful Use Matrix December 2012 Healthcare Information Exchange An HIE Overview HIE and Meaningful Use Matrix Health Information Exchange (HIE) can be defined in a number of ways. In its most
HIE and Meaningful Use Matrix December 2012 Healthcare Information Exchange An HIE Overview HIE and Meaningful Use Matrix Health Information Exchange (HIE) can be defined in a number of ways. In its most
MEANINGFUL USE BASICS
 MEANINGFUL USE BASICS Medicare $44,000 Medicaid $63,000 What is Meaningful Use? Meaningful Use is an umbrella term for rules and regulations that health care providers can meet to qualify for federal incentive
MEANINGFUL USE BASICS Medicare $44,000 Medicaid $63,000 What is Meaningful Use? Meaningful Use is an umbrella term for rules and regulations that health care providers can meet to qualify for federal incentive
Meaningful Use Stage 1 and 2 Your Survival Guide!
 Thank You to Our Sponsors! Meaningful Use Stage 1 and 2 Your Survival Guide! Dr. Henry and Dr. Gross are affiliated with EHRGURU.NET and have lectured for numerous companies including Topcon, First Insight,
Thank You to Our Sponsors! Meaningful Use Stage 1 and 2 Your Survival Guide! Dr. Henry and Dr. Gross are affiliated with EHRGURU.NET and have lectured for numerous companies including Topcon, First Insight,
Alaska Medicaid Program
 Alaska Medicaid Program ALASKA ELECTRONIC HEALTH RECORDS Incentive Program Updated January 2018 Provider Manual 1 Background... 4 2 How Do I use this manual?... 6 3 How do I get help?... 7 4 Eligible provider
Alaska Medicaid Program ALASKA ELECTRONIC HEALTH RECORDS Incentive Program Updated January 2018 Provider Manual 1 Background... 4 2 How Do I use this manual?... 6 3 How do I get help?... 7 4 Eligible provider
CHCANYS NYS HCCN ecw Webinar
 CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
Meaningful Use Roadmap
 Meaningful Use Roadmap Copyright SOAPware, Inc. 2011 1 Introduction 1.1 2 3 Introduction 6 Registration and Attestation 2.1 1. Request the "CMS EHR Certification ID" for SOAPware 9 2.2 2. Register for
Meaningful Use Roadmap Copyright SOAPware, Inc. 2011 1 Introduction 1.1 2 3 Introduction 6 Registration and Attestation 2.1 1. Request the "CMS EHR Certification ID" for SOAPware 9 2.2 2. Register for
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Southwest Regional Health Care Compliance Association Conference February 18, 2011 Travis Broome, Special Assistant for Quality Improvement and Survey & Certification
Medicare & Medicaid EHR Incentive Programs Southwest Regional Health Care Compliance Association Conference February 18, 2011 Travis Broome, Special Assistant for Quality Improvement and Survey & Certification
Understanding Your Meaningful Use Report
 Understanding Your Meaningful Use Report Distributed by Kowa Optimed EMRlogic activehr Understanding Your Meaningful Use Report, version 2.1 Publication Date: May 8, 2012 OD Professional and activehr OD
Understanding Your Meaningful Use Report Distributed by Kowa Optimed EMRlogic activehr Understanding Your Meaningful Use Report, version 2.1 Publication Date: May 8, 2012 OD Professional and activehr OD
Eligible Professionals. How can the West Virginia Health Information Network (WVHIN) assist you in meeting Meaningful Use requirements?
 assist you in meeting Meaningful Use requirements?") Eligible Professionals How can the West Virginia Health Information Network (WVHIN) assist you in meeting Meaningful Use requirements? The charts below define Stage 1 & Stage 2 Meaningful Use objectives
Eligible Professionals How can the West Virginia Health Information Network (WVHIN) assist you in meeting Meaningful Use requirements? The charts below define Stage 1 & Stage 2 Meaningful Use objectives
2015 Meaningful Use and emipp Updates (for Eligible Professionals)
") 2015 Meaningful Use and emipp Updates (for Eligible Professionals) Kai-Yun Kao Department of Health and Mental Hygiene Presented to: Maryland Medicaid Providers Date: February 18, 2016 Webinar Agenda 2
2015 Meaningful Use and emipp Updates (for Eligible Professionals) Kai-Yun Kao Department of Health and Mental Hygiene Presented to: Maryland Medicaid Providers Date: February 18, 2016 Webinar Agenda 2