Post-Acute Care Work Group. January 30, 2017
|
|
|
- Darren Hicks
- 5 years ago
- Views:
Transcription
1 Post-Acute Care Work Group January 30,
2 Agenda 9:00 - Call to Order and Roll Call Greg Banaszynski, Chair 9:05 - Welcoming Remarks Eric Borgerding 9:15 - Work Group Member Introductions All Work Group Members 9:25 - Background on Post-Acute Care Laura Rose 10:15 - Post-Acute Care Survey Results Laura Leitch 10:30 - Identification of Issues All Work Group Members 11:30 - Next Steps; Plans for Future Meetings Greg Banaszynski 11:45 - Adjournment Lunch Immediately following adjournment 2
3 Work Group Purpose and Goal Purpose: To explore how WHA can help hospitals and health systems address their post-discharge challenges and opportunities. Goal: To develop a package of achievable policy initiatives aimed at improving the ability of hospitals and health systems to provide or locate post-acute care for their patients. 3
4 Post-Acute Care and Hospitals Medicare reimbursement for P-AC is trending away from site of service, each with their own reimbursement formula, and towards reimbursement based on patient characteristics. Use of common patient assessment data across P-AC providers may help with appropriate P-AC placement. (IMPACT Act) Greater integration of providers is essential as alternative payment models become more prevalent; hospitals increasingly responsible for outcomes over an episode of care. Discharge planning rule - proposed rule issued 11/2015. Not finalized yet. 4
5 Post-Acute Provider Types Long-term care hospitals (LTCH): A hospital that furnishes extended medical and rehabilitative care to individuals with clinically complex problems, such as multiple acute or chronic conditions, that need hospital-level care for relatively extended periods. To qualify as an LTCH for Medicare payment, a facility must meet Medicare's conditions of participation for acute care hospitals and have an average inpatient length of stay greater than 25 days. Medicare recognized 436 LTCHs in Inpatient Rehabilitation Facilities (IRF): Freestanding rehabilitation hospitals and rehabilitation units in acute care hospitals. They provide an intensive rehabilitation program and patients who are admitted must be able to tolerate three hours of intense rehabilitation services per day. IRFs are paid under Medicare s IRF Prospective Payment System (PPS) which went into effect 1/1/
6 Post-Acute Provider Types Skilled Nursing Facility (SNF): An institution that is primarily engaged in providing: o Skilled nursing care and related services for residents who require medical or nursing care, or rehabilitation services for the rehabilitation of injured, disabled, or sick persons, and is not primarily for the care and treatment of mental diseases; o Has in effect a transfer agreement with a hospital. (Medicare will reimburse for SNF stays following hospital discharge only if the patient had at least a 3 day stay in the hospital.) o Meets the requirements for a skilled nursing facility described in 42 U.S.C. 1395i 3. 6
7 Post-Acute Provider Types Home health agency (HHA): An agency that: o Is primarily engaged in providing skilled nursing and other therapeutic services; o Has policies established by a professional group including at least one physician and at least one registered nurse to govern services, and provides for supervision of these services by a physician or a registered nurse; and o Maintains clinical records on all patients 7
8 Post-Acute Provider Types Swing bed hospital: A hospital or critical access hospital (CAH) participating in Medicare that CMS approves to provide post-hospital SNF care and meets the SNF requirements set out in federal regulations. CAHs that offer swing bed services are exempt from the SNF PPS. These CAHs are paid for their SNF-level services based on 101 percent of the reasonable cost of the services. Non-CAH hospitals offering swing bed services are paid for their SNF-level services under the SNF PPS. 8
9 Numbers of P-AC Providers, Wisconsin LTCH: 5 hospitals; 255 beds IRF: 3 facilities; 121 beds SNF: 372 facilities; 32,854 beds HHA: Approx. 154 agencies Swing bed hospitals: 58 hospitals 9
10 Post-Acute Care Discharges In 2013, 22.3% of all inpatient hospital discharges (7.96 million) were to a post-acute setting. Patients whose payer is Medicare have, by far, the greatest percentage of discharges to post-acute care: o Medicare: 41.7% of discharges are to P-AC o Private insurance: 11.7% o Medicaid: 8.1% o Uninsured: 4.8% *AHRQ Healthcare Cost and Utilization Project, Statistical Brief #205, An All-Payer View of Hospital Discharge to Post-Acute Care, 2013, May
11 Medicare Spending on Post- Acute Care P-AC is fastest growing major Medicare spending category. P-AC Medicare spending grew from $29 billion in 2001 to $59 billion in *MedPAC, Report to the Congress: Medicare Payment Policy, Ch. 7; 3/
12 Medicaid Spending on Long-term Care, Wisconsin, 2015 FY 2015 expenditures, Medicaid FFS, all funds, o Nursing homes: $608,800,000* o Home health AND personal care: $966,312,508** Source: *Wisconsin Legislative Fiscal Bureau, Informational Paper #41, Medical Assistance and Related Programs, January **Kaiser Family Foundation, State Health Facts: Distribution of Fee-for-Service Medicaid Spending on Long Term Care, published 12/

13 Payer Mix by Discharge Disposition 13
14 Medicare Payment Policies: LTCHs To qualify as an LTCH for Medicare payment, a facility must meet Medicare s conditions of participation for acute care hospitals and have an average length of stay greater than 25 days for certain Medicare patients. The 25% Rule : Only 25% of an LTCH s patients may be admitted to the LTCH from a single referring acute care hospital during a cost-reporting period without being subject to a negative payment adjustment. 14
15 Medicare Payment Policies: IRFs To qualify as an IRF, a facility must meet Medicare s conditions of participation for acute care hospitals. In addition, the facility must be primarily focused (e.g., no less than 60% of the IRF s patient population) on treating one of 13 conditions that typically require intensive rehabilitation therapy. 15
16 Medicare Payment Policies: SNFs Beneficiaries who need short-term skilled care (nursing or rehabilitation services) on an inpatient basis following a hospital stay of at least three days are eligible to receive covered services in skilled nursing facilities(snfs). Medicare covers up to 100 days of SNF care per spell of illness. A spell of illness begins with the first day of a hospital or SNF stay and ends when there has been 60 consecutive days during which a patient was not in a hospital or a SNF. 16
17 Medicare Payment Policies: HHAs CMS has a prospective payment system (PPS) that pays HHAs a predetermined rate for each 60-day episode of home health care, on patients conditions and service use, and adjusted to reflect the level of market input prices in the geographical service area. The patient must be homebound. 17
18 Regulatory Issues Key Medicare regulations : o LTCHs: 25 day average length of stay rule; reduced payment for certain patients transferred to an LTCH from a particular general acute care hospital. o IRFs: 3 hours of therapy/5 days a week minimum; 60% rule o SNFs: SNF 3 day stay requirement. o HHAs: Requirement that patients be homebound in order to qualify for services 18
19 MedPAC Observations on Post-Acute Care Medicare payments to P-AC providers are too generous. System encourages providers to increase payments by making certain patient care decisions. Biases in payments systems make certain patients and services provided to them more profitable than others. Despite increased costs, quality of care had not improved. The need for P-AC is not well defined. Medicare per capita spending on P-AC varies more than any other covered services. High Medicare margins relative to other settings. MedPAC Report to Congress, March 2015, ch
20 Value-Based Purchasing Important for P-AC because payments are tied to value rather than volume; measures in VBP initiatives include episodes of care that extend beyond the hospitalization period into the P- AC setting. VBP refers to a broad set of performance-based payment strategies that link financial incentives to a provider s performance on a set of defined measures in an effort to achieve better value by driving improvements in quality and slowing the growth in health care spending. Hospital value based purchasing ties a small % of a hospital s payments to quality metrics (75%) and Medicare spending per episode (25%). 20

21 VBP, P-AC, and Hospitals 21
22 VBP Initiatives Affecting Post- Acute Care Landscape Bundled Payments (such as Comprehensive Care for Joint Replacement; Bundled Payments for Care Improvement) ACOs Hospital Readmission Reduction Program IMPACT Act 22
23 Bundled Payments Initiatives Important for P-AC because the expressed goals of bundled approaches to payment are to improve coordination across the providers engaged in caring for a patient during an episode of care and, in turn, improve cost efficiencies or savings. Important for P-AC because payment to providers is based on predetermined expected costs for a group of related health care services, including P-AC. Medicare goal: 30 % of all Medicare fee-for-service payments should be made via alternative payment models by 2016 and 50 % by
24 Comprehensive Joint Replacement (CJR) Initiative CJR tests bundled payment and quality measurement for an episode of care associated with hip and knee replacements (the most common surgeries for Medicare beneficiaries) to encourage hospitals, physicians, and post-acute care providers to work together to improve the quality and coordination of care from the initial hospitalization through recovery. CMS has implemented the CJR model in 67 geographic areas across the U.S. Wisconsin mandatory participants (except for certain BPCI participants): o Madison, WI: Columbia, Dane, Green, Iowa Counties o Milwaukee-Waukesha-West Allis, WI: Milwaukee, Ozaukee, Washington, Waukesha Counties 24
25 Bundled Payments for Care Improvement (BPCI) Initiative The three-year initiative (which may be extended by up to two years) links payments for services related to an episode of care that is triggered by a hospitalization. BPCI participants may benefit financially from providing services in the bundle more efficiently and are at risk if their costs for the bundle are higher than a historical benchmark. Conditions tested: o Acute Myocardial Infarction (AMI) Model; o Coronary Artery Bypass Graft (CABG) Model; o Surgical Hip and Femur Fracture Treatment (SHFFT) Model; and o Cardiac Rehabilitation (CR) Incentive Payment Model 25
26 Accountable Care Organizations Accountable Care Organizations (ACOs) are groups of doctors, hospitals, and other health care providers, who come together voluntarily to give coordinated high quality care to the Medicare patients they serve. When an ACO succeeds in both delivering high-quality care and spending health care dollars more wisely, it shares in the savings it achieves for the Medicare program. 4 MSSP ACOs in Wisconsin. Important for P-AC because ACOs hold providers financially responsible for the total cost of care and a set of quality measures, which may potentially incentivize post-acute care management. 26
27 Hospital Readmission Reduction Program Requires CMS to reduce payments to IPPS hospitals with excess readmissions, effective for discharges beginning on October 1, One in 5 Medicare patients admitted to skilled nursing facilities from hospitals is readmitted to the hospital within 30 days, Important for P-AC because hospitals (except CAHs) may be penalized for readmissions that happen 30 days post-discharge for certain conditions. Hospitals activities that may lower readmission rate include: clarifying patient discharge instructions; coordinating with post-acute care providers and patients primary care physicians; and reducing medical complications during patients initial hospital stays. 27
28 Literature Review and Recent Study RAND Corporation, Measuring Success in Health Care Value- Based Purchasing Programs, 2016 Recent JAMA Study: o During a time period in which Medicare payments for joint replacement episodes increased by 5%, bundled payment for procedures at a 5 hospital system in Texas was associated with substantial hospital savings and reduced Medicare payments. o Decreases in P-AC spending occurred only when it was included in the bundle. Source: January 03, 2017: Cost of Joint Replacement Using Bundled Payment Models (JAMA Intern Med. doi: /jamainternmed ) 28
29 IMPACT* Act of 2014 Attempts to implement standardized assessment data across all P-AC settings, rather than the current system. PAC providers must submit patient assessment data using uniform tool beginning in 2018; HHS Secretary must recommend a uniform payment system for P- AC based on two years of uniform patient assessment data; probably not until * Improving Medicare Post-Acute Care Transformation (IMPACT) Act of
30 Selected State Policies Affecting Post-Acute Care Post-acute provider Medicaid reimbursement rates. Other Medicaid policies. Potentially Preventable Readmissions (PPR). SNF statewide bed limit; construction moratorium. Workforce issues. 30
31 Medicaid Pay-for- Performance (P4P) Currently: Potential for recoupment of payment if the external quality review organization determines a discharge from a hospital was medically inappropriate and patient needed to be readmitted. Readmission within 30 days used as a measure for FFS P4P. 31
32 Potentially Preventable Readmissions New PPR policy will replace the current FFS P4P program; PPR output will provide actionable data for providers to drive improvement. In CY 2017, DHS will evaluate the PPR model results in collaboration with WHA and report to hospitals and HMO plans. 32
33 Medicaid Reimbursement of Post-Acute Providers IRFs: Rehabilitation hospitals are reimbursed for inpatient services on a per diem basis. The rate is set at 85% of the average daily cost of serving Medicaid patients. SNFs: Nursing homes are reimbursed on a daily rate for care provided to Medicaid recipients according to a prospective payment system that DHS must update annually. Rate incorporates case-mix and consideration of 5 cost centers. 33
34 Medicaid Reimbursement of Post-Acute Providers HHAs: DHS establishes maximum allowable fees for all covered home health services provided to Wisconsin Medicaid members. Providers are required to bill their usual and customary charges for services provided. For each covered service, the DHS shall pay the lesser of a provider s usual and customary charge or the maximum allowable fees established by the DHS (is almost always the latter). 34
35 Medicaid Certification Requirements In addition to federal Medicaid regulations, providers must meet additional state-level regulations for Medicaid certification: o Rehabilitation hospitals: approved as a general hospital under s , Stats., and ch. DHS 124, including the requirements for rehabilitation services under s. DHS o Nursing homes: licensed pursuant to s , Stats., and ch. DHS 132. o Home health agencies: licensed under DHS 133, and meet additional requirements in DHS
36 Requirements for Prior Authorization or Physician s Order Prior authorization, generally: DHS (3) Prior authorization, Home health agencies: DHS (3) Services requiring a physician's order or prescription: Skilled nursing services in a SNF; Home health agencies services: (2m) 36
37 SNF bed availability SNFs are a primary location for post-acute care, but: o The number of skilled nursing home beds in Wisconsin has declined between July 2003 and July 2013 by 6,577 beds, or 16 percent. o A moratorium on nursing home bed construction has existed since

38 Nursing Home Census Trends 38
39 Post-Acute Provider Workforce Issues The median hourly starting wage for personal caregivers is $10.75, compared to $12.00 for local, non-health care employers seeking unskilled, entry-level workers. Nursing facilities vacancy rates, 2016: o 12.6% for registered nurses (RN), o 12.1% for licensed practical nurses (LPN), o 14% for certified nurse aides (CNA), the primary caregivers in nursing facilities. Source: LeadingAge, WHCA, RSA and WALA; The Long Term Care Workforce Crisis;

40 Post-Acute Provider Workforce Issues: Nurses 40
41 Creation of Preferred Post-Acute Networks : Preferred Criteria Easy access for hospital patient discharges: o Geographic access for all patients. o Admissions allowed 24/7. o Start of home care within 24 hours of hospital discharge. Source: AHA Trendwatch, December
42 Preferred Criteria Compliance with federal and state regulations. Lower than average survey deficiencies: o For SNFs: at least a 3 start quality rating o Separate unit for P-AC patients with ACO or health system physician serving in the SNF o 24/7 RN care provider and 1:15 RN/P-AC patient ratio. o Use of INTERACT 3.0 tools 42
43 Preferred Criteria Common outcomes measures that may be collected monthly, and may be aggregated for comparison purposes: o 30 day hospital readmission rates. o Patient/family satisfaction ratings. o ED visits, especially within 3 days of admission to P-AC venue. 43
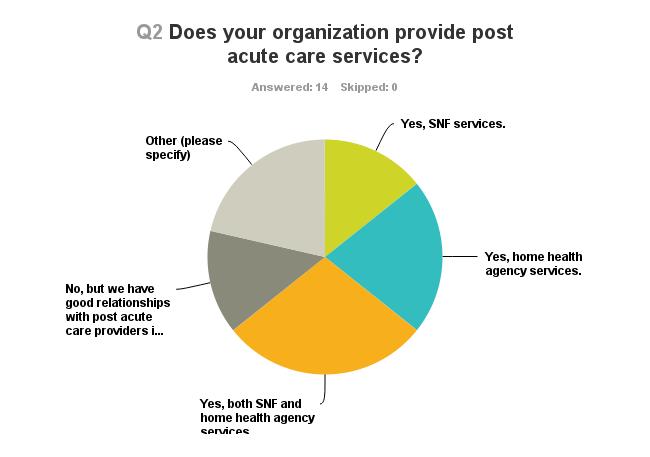
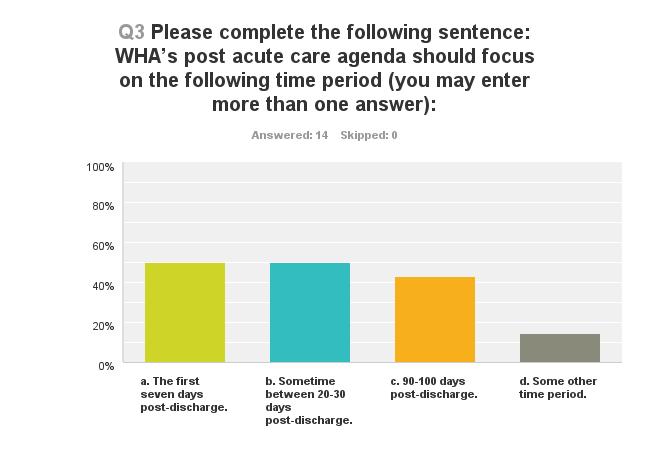
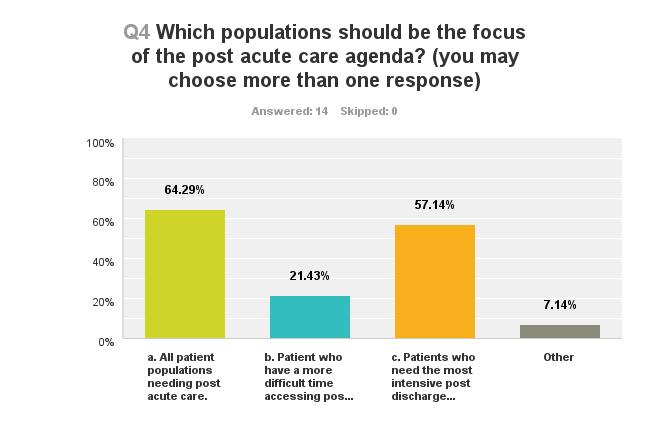
44 WHA Post-Acute Care Survey Results Fall,
45
46
47
48
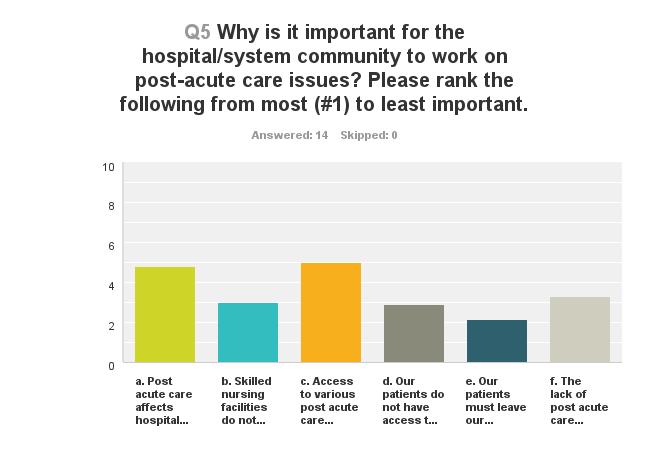
49 Why is it important? 5. Access to various P-AC options is key to our discharge planning Post acute care affects hospital reimbursement through bundled payments, penalties and incentives The lack of P-AC options results in people overusing inpatient and outpatient hospital services.
50 Why is it important? 3. SNFs do not necessarily provide the level or frequency of services patients need post-discharge Our patients do not have access to PAC that allows them to stay in their home even when home care should be an option. 2.5 Our patients must leave our community to receive care in a SNF.
51
52 Other barriers Volume of regulations across settings. Lack of understanding of cost effectiveness of P-AC. EHR connectivity. Better incentives for SNFs to work with hospitals. Physicians don t understand or lack familiarity with P-AC services.
53 Challenges next 5 years Providing appropriate care for difficult populations. Reimbursement and staffing. Regulatory environment. Mega rule. Home care not available or affordable. Align hospital and SNF incentives. Management structure to manage bundled payments.

54 54
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Episode Payment Models:
 Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Advancing Care Coordination Proposed Rule
 Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
Episode Payment Models Final Rule & Analysis
 Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
PAYMENT INNOVATION: Real Examples of Client Implementation. Craig Tolbert & Michael Wolford
 PAYMENT INNOVATION: Real Examples of Client Implementation Craig Tolbert & Michael Wolford 2 PINNACLE SPEAKER PROFILE CRAIG TOLBERT Principal DHG Healthcare Birmingham, AL PINNACLE SPEAKER PROFILE MICHAEL
PAYMENT INNOVATION: Real Examples of Client Implementation Craig Tolbert & Michael Wolford 2 PINNACLE SPEAKER PROFILE CRAIG TOLBERT Principal DHG Healthcare Birmingham, AL PINNACLE SPEAKER PROFILE MICHAEL
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Alternative Payment Models: Trends and Tactics for Success
 Alternative Payment Models: Trends and Tactics for Success James Michel Senior Director, Medicare Reimbursement & Policy American Health Care Association November 15, 2016 Discussion Review CMS priorities
Alternative Payment Models: Trends and Tactics for Success James Michel Senior Director, Medicare Reimbursement & Policy American Health Care Association November 15, 2016 Discussion Review CMS priorities
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
2013 Health Care Regulatory Update. January 8, 2013
 2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future
 Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
Regulatory Advisor Volume Eight
 Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
CRS Report for Congress Received through the CRS Web
 CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
3/19/2013. Medicare Spending Per Beneficiary: The New Link Between Acute and Post Acute Providers
 The New Link Between Acute and Post Acute Providers Carol Quiring, RN President and CEO, Home Care and Hospice Saint Luke s Health System Shauna Thompson, RHIT Senior Director, Quality & Patient Safety
The New Link Between Acute and Post Acute Providers Carol Quiring, RN President and CEO, Home Care and Hospice Saint Luke s Health System Shauna Thompson, RHIT Senior Director, Quality & Patient Safety
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
What 2017 Holds for Medicare Value-Based Transformation: Finalization of the Advancing Care Coordination Rule and Much More
 January 19, 2017 What 2017 Holds for Medicare Value-Based Transformation: Finalization of the Advancing Care Coordination Rule and Much More HDG Webinar Series Brian Ellsworth, MA, Director, Payment Transformation
January 19, 2017 What 2017 Holds for Medicare Value-Based Transformation: Finalization of the Advancing Care Coordination Rule and Much More HDG Webinar Series Brian Ellsworth, MA, Director, Payment Transformation
Distribution of Post-Acute Care under CJR Model of Lower Extremity Joint Replacements for MS-DRG 470
 Distribution of Post-Acute Care under CJR Model of Lower Extremity Joint Replacements for MS-DRG 470 Introduction The goal of the Medicare Comprehensive Care for Joint Replacement (CJR) payment model is
Distribution of Post-Acute Care under CJR Model of Lower Extremity Joint Replacements for MS-DRG 470 Introduction The goal of the Medicare Comprehensive Care for Joint Replacement (CJR) payment model is
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.
 Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.") MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
Furthering the agency s stated intention to pay for value over volume,
 in the news Health Care September 2016 The Future Is Now: CMS Proposes Broad Bundled Payment Expansion for Cardiac Care Episodes In this Issue: Episode Payment Models... 2 Cardiac Rehabilitation Incentives...
in the news Health Care September 2016 The Future Is Now: CMS Proposes Broad Bundled Payment Expansion for Cardiac Care Episodes In this Issue: Episode Payment Models... 2 Cardiac Rehabilitation Incentives...
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Partnerships: Developing an Elective Joint Replacement Program
 Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY
 VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
Submission #1. Short Description: Medicare Payment to HOPDs, Section 603 of BiBA 2015
 Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
(202) or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays
 or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships
 MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
The Future of Healthcare Delivery; Are we ready?
 The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
Leslie Demaree Goldsmith
 LESLIE DEMAREE GOLDSMITH Shareholder is a shareholder in Baker Donelson's Baltimore office. Overview Ms. Goldsmith brings more than 25 years of experience to her practice, representing health care providers
LESLIE DEMAREE GOLDSMITH Shareholder is a shareholder in Baker Donelson's Baltimore office. Overview Ms. Goldsmith brings more than 25 years of experience to her practice, representing health care providers
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Facing the Post-Acute Care Acuity Challenge
 Post-Acute Care Collaborative Facing the Post-Acute Care Acuity Challenge Adjusting to the New Post-Acute Population Julia Burgdorf Senior Analyst burgdorj@advisory.com Road Map A Changing Population Sector
Post-Acute Care Collaborative Facing the Post-Acute Care Acuity Challenge Adjusting to the New Post-Acute Population Julia Burgdorf Senior Analyst burgdorj@advisory.com Road Map A Changing Population Sector
Framework for Post-Acute Care: Current and Future Issues for Providers
 Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
paymentbasics Defining the inpatient acute care products Medicare buys Under the IPPS, Medicare sets perdischarge
 Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
September 22, 2017 VIA ELECTRONIC SUBMISSION
 September 22, 2017 VIA ELECTRONIC SUBMISSION The Honorable Seema Verma Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services 7500 Security Boulevard Baltimore,
September 22, 2017 VIA ELECTRONIC SUBMISSION The Honorable Seema Verma Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services 7500 Security Boulevard Baltimore,
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
CJR Final Rule: Policy Changes and Strategies for Bundled Payment Success
 CJR Final Rule: Policy Changes and Strategies for Bundled Payment Success Melinda Hancock, Edward Stall, Craig Tolbert, Michael Wolford Friday, November 20, 2015 1 Agenda 1) Overview of CJR Model 2) Policy
CJR Final Rule: Policy Changes and Strategies for Bundled Payment Success Melinda Hancock, Edward Stall, Craig Tolbert, Michael Wolford Friday, November 20, 2015 1 Agenda 1) Overview of CJR Model 2) Policy
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
New Models in Payment: Joint Replacements. Sharon Eloranta, MD February 18, 2016
 New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
WHERE DO WE GO FROM HERE?
 INTEGRATING ACUTE TO POST-ACUTE CARE SETTINGS: WHERE DO WE GO FROM HERE? HEALTHCARE LANDSCAPE February 23, 2018 WHAT IS POST-ACUTE CARE? what comes after an acute care stay Goals are to expedite the recovery
INTEGRATING ACUTE TO POST-ACUTE CARE SETTINGS: WHERE DO WE GO FROM HERE? HEALTHCARE LANDSCAPE February 23, 2018 WHAT IS POST-ACUTE CARE? what comes after an acute care stay Goals are to expedite the recovery
Pay-for-Performance. GNYHA Engineering Quality Improvement
 Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A
 Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
April 26, Ms. Seema Verma, MPH Administrator Centers for Medicare & Medicaid Services. Dear Secretary Price and Administrator Verma:
 April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
September 16, The Honorable Pat Tiberi. Chairman
 1201 L Street, NW, Washington, DC 20005 T: 202-842-4444 F: 202-842-3860 www.ahcancal.org September 16, 2016 The Honorable Kevin Brady The Honorable Ron Kind Chairman U.S. House of Representatives House
1201 L Street, NW, Washington, DC 20005 T: 202-842-4444 F: 202-842-3860 www.ahcancal.org September 16, 2016 The Honorable Kevin Brady The Honorable Ron Kind Chairman U.S. House of Representatives House
What s Next for CMS Innovation Center?
 What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Making CJR Work for You. A Roadmap for Successful Implementation of Medicare Bundles
 December 10, 2015 Making CJR Work for You A Roadmap for Successful Implementation of Medicare Bundles https://innovation.cms.gov/initiatives/cjr Sheldon Hamburger shamburger@thearistonegroup.com (248)
December 10, 2015 Making CJR Work for You A Roadmap for Successful Implementation of Medicare Bundles https://innovation.cms.gov/initiatives/cjr Sheldon Hamburger shamburger@thearistonegroup.com (248)
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
September 6, RE: CY 2017 Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems Proposed Rule
 September 6, 2016 VIA E-MAIL FILING Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1656-P P.O. Box 8013 Baltimore, MD 21244-1850 RE: CY 2017 Hospital Outpatient
September 6, 2016 VIA E-MAIL FILING Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1656-P P.O. Box 8013 Baltimore, MD 21244-1850 RE: CY 2017 Hospital Outpatient
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
HOME DIALYSIS REIMBURSEMENT AND POLICY. Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation
 HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
CMS in the 21 st Century
 CMS in the 21 st Century ICE 2013 ANNUAL CONFERENCE David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco November 15, 2013 The strategy is to concurrently pursue
CMS in the 21 st Century ICE 2013 ANNUAL CONFERENCE David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco November 15, 2013 The strategy is to concurrently pursue
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
A1600 A1800: Most Recent Admission/Entry or Reentry into this Facility
 A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Critical Access Hospital Quality
 Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR)
") Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,