Linda Gibson, President & CEO
|
|
|
- Hector French
- 5 years ago
- Views:
Transcription

1 Linda Gibson, President & CEO


2
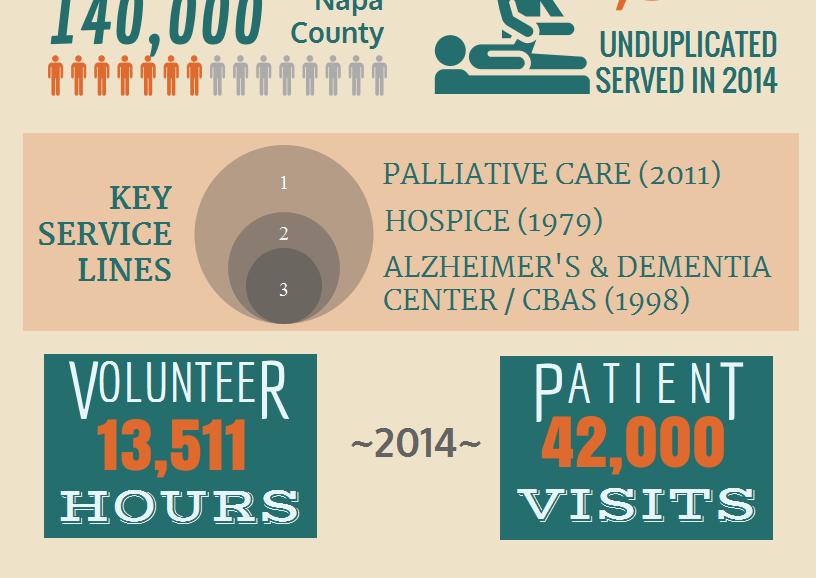
3 Topics Community-based palliative care the unfunded approach Partners in Palliative Care Pilot with Partners in Palliative Care Pilot with Partnership Health Plan of California (PHC) the funded approach
4 Why Start an Unfunded Palliative Care Program? To promote Hospice program growth and improve length of stay To fill care delivery gaps in the community To reach the Latino population A Warm hand-off for discharged Hospice patients To control the message about Hospice A new way to engage Physicians and other referral sources
5 Eligibility Progressive advanced illness and Significant and complex symptoms Multiple recent hospitalizations In need of advance care planning Uncertainly regarding goals of care In need of support in end-of-life decision making May be receiving curative therapy May be in a skilled nursing facility Would you be surprised if your patient died in the next year?
6 Care Delivery Model Services Staffing Setting Initial Assessment RN Home * Pain / symptom management Advance Care Planning / POLST RN PrimaryCare, Medical Director, RN Home Telephone Home Coordination of Care RN Home Telephone Monday Friday (8 a.m. 5 p.m.) Telephonic Support RN / Volunteer RN Telephone Care Management Plan RN Home Telephone Help with practical needs Volunteers Home Reimbursement: Fee-for-service, $60.00 / month & sliding fee * Home, Skill Nursing Facility, Board & Care, Assisted Living, Retirement
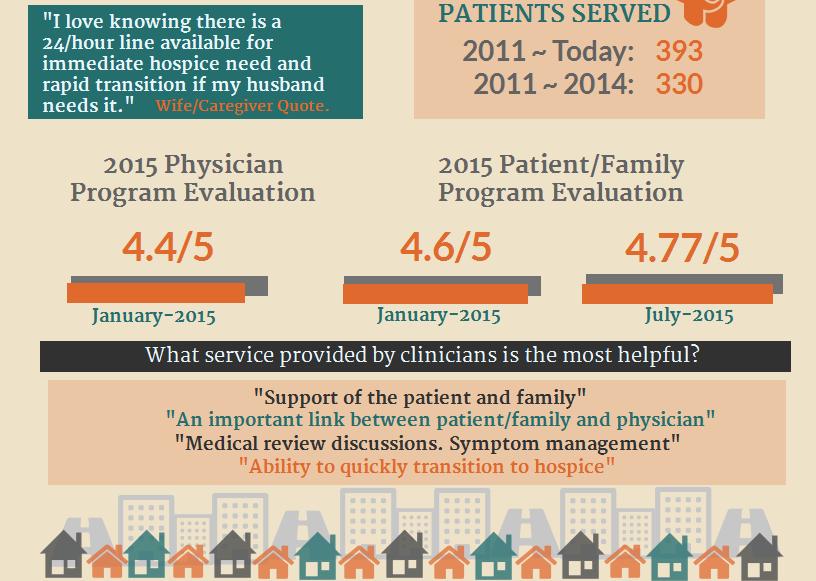
7 Other Considerations Need to be very clear about scope of services and frequency of visits: Monthly visits Weekly telephone calls Occasional social work and spiritual care consultation Focus is on education, coordination and consultation Use of volunteers helps to control costs and provides a richer patient experience RN case load = patients Requires surprisingly little marketing and outreach
8 Lessons Learned Exceedingly well received in the community Physicians, families love the program Need to have a plan to move patients to Hospice when eligible Improves ability to keep discharged Hospice patients in the fold Allowing volunteers to stay with the patient during transitions from / to Hospice facilitates continuity Has helped Hospice LOS ROI improves every year
9 60 Transitions Palliative Care Average Daily Census Comparison = August 2014 YTD
10 Transitions Transfers to Hospice -MLOS MLOS Hospice
11 Transitions Transfers to Revenue ,084,626 1,290, , ,415 Expense - $206,


12
13 Napa Valley Hospice & Adult Day Services Partnership Health Plan of California


14 Partnership HealthPlan of California Mission: To help our members, and the communities we serve, be healthy Membership: 540,000 in 14 counties Model: Not-for-profit, Community Organized Health System Primary Care: 77% at FQHC, RHC or Native Health Center
15 Offering and Honoring Choices TM Partnership HealthPlan s Initiative to promote Advance Care Planning and Palliative Care. 14 Projects Purpose: Ensure that our members and their families are knowledgeable about healthcare treatment options, empowered to define their treatment goals, and able to make informed choices about the interventions they prefer during the last years of life.


16 Offering and Honoring Choices TM Projects
17 PHC Palliative Care Pilot CHCF planning grant (2014) Working group of hospice agencies and palliative care physicians contributed to proposed plan PHC awarded CHCF implementation grant (2015) Four pilot sites selected: Resolution Care (Humboldt County) Napa Valley Hospice and Adult Day Services (Napa County) Hospice of Yolo (Yolo County) Interim HealthCare (Shasta County)
18 PHC Pilot Eligible Patients Life expectancy less than 2 years Advanced severity (when not decompensated ) Any of six diagnoses: Congestive Heart Failure COPD Cirrhosis Dementia Frailty Syndrome Stage IV Cancer
19 Partners in Palliative Care Service Model
20 Partners in Palliative Care: Payment Model Global Payment Per enrolled member, per month One rate if resident of SNF or if skilled nursing services not included Another rate if in-home nursing included Bonus Payments: Quality: Bonus per Quarter for Meeting Quality Metrics Shared Savings: Bonus per month if no Emergency Department visits or Hospitalizations during the month
21 Engaging the Health Plan A history of working together successfully Hospice Services CBAS services Lead agency for community ACP project Partner together to put on an annual palliative care educational conference Planning Partner, then Pilot for testing a palliative care benefit
22 What You Need From the Health Plan Mission alignment Mutual respect Common focus on quality Appreciation for importance of financial sustainability Collaborative approach Innovative practices willingness to try new approaches
23 What You Need From the Health Plan Access to data Provider lists Eligible members (frequent flyers) Cost data Flexibility In care model design and implementation In eligibility requirements
24 What You Need From the Health Plan Simplified enrollment and billing processes Limit data submission requirements PMPM works well (we think ) Promotional assistance Joint press releases Letters to providers announcing benefit
25 Evaluating Payment Models Must be financially sustainable for the provider: Costs of building a new program Financial modeling of assumptions Balancing risk and likelihood of success Importance of baseline financial stability

26 Contact Information Linda J. Gibson President & CEO Napa Valley Hospice & Adult Day Services
27 Ann Hablitzel, RN, BSN, MBA Hospice Care of California
28 Objectives You will learn to: Identify and speak to the priorities and challenges of payer sources Describe the core components of a Community based Palliative Program

29
30 Mission Statement for Palliative Program To advance, support and provide a Community based Palliative Care Program. We envision a seamless, less fragmented and more coordinated care system, that also addresses effective stewardship of resources.
31 Focus of Program Provide symptom management and emotional support to patient/family Assist with EOL discussions/decisions Promote a smooth transition to Hospice. Implement Palliative Care Program to a targeted population in order to reduce ER visits and inpatient hospitalizations Promote appropriate utilizations of resources to reduce unnecessary costs Promote transition to Hospice when appropriate Improve patient care
32 Program Goals To address physical, psychological, social, spiritual, practical expectations and needs To reduce or eliminate Emergency Room visits (especially for pain/symptom management) and total care costs To reduce or eliminate (unplanned) hospital admission and/or readmission To promote a seamless transition from curative to Palliative to Hospice for patients and their families. To address goals of care and advance care planning To assess the individual primary care physicians and subspecialists preferences in communicating to members of the team To assist family members emotional adjustments to the changing role in relation to the patient and within the family system through support and education
33 Structure and Process Identification of patients who would benefit from Palliative Care Program Develop Criteria for evaluation and admission Referral process Fax sheet MD order Authorization process Letter of explanation - to family (English and Spanish) -to PCP
34 Basic Disease Process Criteria Cancer (metastatic/recurrent) Advanced COPD Stroke (with decreased function by at least 50%) End-stage Renal Disease Advanced Cardiac Disease i.e.; CHF, Severe CAD, CM (LVEF less than 25%) Frail Elderly with Multiple Diagnosis Other Life-limiting Illness
35 Criteria Concomitant Disease Process Liver Disease Moderate Renal Disease Moderate COPD Moderate CHF Other Condition Complicating Care Other Criteria to consider in Screening Team/patient/family needs help with complex decision making and determination of goals of care Patient has frequent visit to emergency department (greater than 1 time a month for same diagnosis) Patient has more than 1 hospital admission for the same diagnosis in the last 30 days
36 Interdisciplinary Team Based Care Communication Provide purpose and explanation of Palliative Program Provide purpose and explanation of Palliative Program to Clinical Team focus on communication, authorization process and utilization of resources
37 Evidence Based Outcome Data Data Collected Demonstrating Cost Avoidance or Improved Resource Utilization Measuring Quality Pain and symptom management Patient/family satisfaction Advanced care planning Improved utilization outcomes Hospitalizations Hospital readmission rate Emergency room visits
38 Summary & Lessons Learned California is a highly capitated and competitive market with diverse population urban and rural Culture Economic affluent and extreme poverty Healthcare Payer sources (IPA s, Medical Groups, Hospitals Cancer Center Insurance Plans) Medicare Advantage Plans Full risk or shared risk Needs Assessment of Payer Source Identify their goals and outcomes Reduction of costs with high quality patient care

39 Thank you
40 Jeff Hammond Sea Crest Home Health Services Inc. November 9&
41 MCCM Details The model is designed to: Increase access to supportive care services provided by hospice; Improve quality of life and patient/family satisfaction; Inform new payment systems for the Medicare and Medicaid programs. Number of Participants: 141 California Participants: 4 Assisted HomeCare Inc. dba Assisted Hospice Care(Los Angeles, California) Assisted Home Hospice(Los Angeles, California) Sea Crest Hospice Services, Inc. (Orange County, California) CareChoices Hospice and Palliative Care Services, Inc. (Orange County, California) Hospice of Saddleback Valley(Orange County, California) 5 year pilot The model will be phased in over 2 years. Participating hospices will be randomly assigned to Phase 1 or Phase 2. Services will begin starting January 1, 2016 for the first phase of participating hospices and in January 2018 for the remaining participating hospices. Participating hospices will receive payment under the model through the standard Medicare claims process
42 How does MCCM operate? The hospices will be paid a $400 per beneficiary per month (PBPM) fee for providing services under the model for 15 or more calendar days per month. If services are provided under the model for fewer than 15 calendar days per month during the first month that the beneficiary is in the model, the hospices will be paid $200 PBPM. As the beneficiary is not electing the Medicare hospice benefit, hospices participating in this model will not receive the Medicare Hospice Benefit per diem rates Services provided under the model are not subject to a copay
43 Target Population The target population for the Medicare Care Choices Model is: Medicare beneficiaries who are eligible for the Medicare Hospice Benefit and dually eligible beneficiaries who are enrolled in traditional Medicare and eligible for the Medicaid hospice benefit. Medicare and dually eligible beneficiaries must not have elected the Medicare Hospice Benefit (or the Medicaid hospice benefit) within the last 30 days prior to participating in the model and satisfy all the eligibility criteria listed in the Request for Applications. The model provides Medicare beneficiaries who qualify for coverage under the Medicare hospice benefit and dually eligible beneficiaries who qualify for the Medicaid hospice benefit the option to elect to receive supportive care services typically provided by hospice while continuing to receive curative services Participation is limited to beneficiaries with: advanced cancers chronic obstructive pulmonary disease congestive heart failure human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS).
44 The Sea Crest Care Pathways Program Goals Promote the highest quality of life by controlling symptoms such as pain, shortness of breath, nausea, vomiting, fatigue and anxiety. Provide psychological, spiritual and relational support for patients, families and staff. Facilitate communication about the illness process and options for care. Educate community hospitals, physicians, skilled nursing facilities, families, patients, and our staff about palliative care practices and philosophies. Conduct research and promote community efforts to continuously improve the quality of care for people with serious and life-threatening illnesses. Program advantages and benefits: Improved quality of life that allows patients the time to live every moment. Intensive symptom and comfort management (alleviate pain, fatigue, anxiety, nausea, loss of appetite, sleeplessness, depression and other complex medical care issues). 24-hour phone access to RN Program Managers and/or triage nurses that coordinate medical, psychological, and related support and communication services. Trusted care coordination for intelligently navigating the health care system. Education regarding all care options. Guidance regarding complex treatment, emergency room admission or re-hospitalization choices. Physical, emotional and spiritual support to encourage complete well-being throughout the care continuum.
45 Anastasia Dodson, Associate Director Department of Health Care Services
46 Medi-Cal Palliative Care Program Development SB 1004 (Hernandez) Enacted in 2014 DHCS has been consulting with palliative care experts and stakeholders: Develop a shared understanding of palliative care Review data findings Consider performance measures Review October 2, 2015 Medi-Cal Palliative Care Paper
47 DHCS Goals for Medi-Cal Palliative Care 1. Establish standards and provide technical assistance for Medi-Cal managed care plans to ensure delivery of palliative care services. 2. Establish guidance on the medical conditions and prognoses that render a [Medi-Cal] beneficiary eligible for the palliative care services. 3. Develop a Medi-Cal palliative care policy that, to the extent practicable, is cost-neutral to the General Fund on an ongoing basis. 4. Define Medi-Cal palliative care services, to include but are not limited to those types of services that are available through the Medi-Cal hospice benefit. 5. Provide access to both hospice-type services and curative care at the same time, to the extent the services are not duplicative, for beneficiaries eligible for Medi-Cal palliative care.
48 Medi-CalPalliativeCareScope Medi-Cal palliative care will use specific definitions of eligible conditions, services, and providers Specificity is needed: To meet the requirements of SB 1004 Long- term success is more likely through an incremental approach
49 Delivery System and Dual-Eligible Considerations Initial focus on managed care; further analysis needed for fee-for-service Medi-Cal Initial focus on Medi-Cal only beneficiaries (not dually eligible for Medicare) Considering policy options for beneficiaries in HCBS waiver programs, nursing facilities, and potentially Cal Medi-Connect.
50 Proposed EligibleCondition for Medi-Cal Palliative Care Late-Stage/High Grade Cancer with significant functional decline or limitations Should DHCS provide more specific standardized clinical criteria on this condition? Allow Medi-Cal Managed Care Organizations (MCO) to use one of several existing screening protocols?
51 AdditionalConditions Existing palliative care programs generally include additional conditions, such as advanced Congestive Heart Failure or end-stage pulmonary disease. Managed care plans that currently (or in future) authorize palliative care consults and services for patients with other medical conditions may continue to do so.
52 ProposedPalliativeCareServices When reasonable and necessary for the palliation or management of a qualified serious illness and related conditions, and when provided by qualified personnel: Hospice-Type Services (DHCS All-Plan Letter ) Additional Services: Palliative Care Consultation, Advance Care Planning Care Coordination, Assessment, Interdisciplinary care team, Care Plan * Curative Care *
53 ProviderQualifications Consider full range of inpatient, outpatient, community-based providers. DHCS is considering options: Palliative Care Training Palliative Care Certification, Accreditation Health Plan Credentialing Add Palliative Care component to existing provider qualifications
54 PerformanceMeasures DHCS developing performance measures DHCS considering linking payment to performance DHCS considering linking payment to performance measures, particularly in fee-for-service
55 Questions and Contact Info DHCS Palliative Care Website: vpart/pages/palliative- Care- and-sb-1004.aspx Contact:
Variables that impact the cost of delivering SB 1004 palliative care services. Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017
 Variables that impact the cost of delivering SB 1004 palliative care services Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017 SB 1004 Palliative Care SB 1004 (Hernandez, Chapter 574, Statutes
Variables that impact the cost of delivering SB 1004 palliative care services Kathleen Kerr, BA Kerr Healthcare Analytics September 28, 2017 SB 1004 Palliative Care SB 1004 (Hernandez, Chapter 574, Statutes
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Providing Hospice Care in a SNF/NF or ICF/IID facility
 Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
hospic Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals.
 Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
(f) Department means the New Hampshire department of health and human services.
 Department means the New Hampshire department of health and human services.") Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
HOSPICE IN MINNESOTA: A RURAL PROFILE
 JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways
 Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways") Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
National Hospice and Palliative Care OrganizatioN. Facts AND Figures. Hospice Care in America. NHPCO Facts & Figures edition
 National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Kathleen Kerr, BA Kerr Healthcare Analytics July 18, 2017
 Estimating the number of individuals eligible for SB1004 palliative care and appreciating baseline utilization patterns and costs toward the end of life Kathleen Kerr, BA Kerr Healthcare Analytics July
Estimating the number of individuals eligible for SB1004 palliative care and appreciating baseline utilization patterns and costs toward the end of life Kathleen Kerr, BA Kerr Healthcare Analytics July
Understanding and Leveraging Continuity of Care
 Understanding and Leveraging Continuity of Care Cal MediConnect Providers Summit January 21, 2015 Moderator: Jane Ogle, Consultant, Harbage Consulting www.chcs.org An Overview of Continuity of Care in
Understanding and Leveraging Continuity of Care Cal MediConnect Providers Summit January 21, 2015 Moderator: Jane Ogle, Consultant, Harbage Consulting www.chcs.org An Overview of Continuity of Care in
Special Needs Plan Provider Education
 Special Needs Plan Provider Education Learning Goals What is a Special Needs Plan (SNPs) What differentiates a SNP from other MA plans What SNPs are offered by Freedom Health and Optimum Healthcare 2 Care
Special Needs Plan Provider Education Learning Goals What is a Special Needs Plan (SNPs) What differentiates a SNP from other MA plans What SNPs are offered by Freedom Health and Optimum Healthcare 2 Care
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
CAL MEDICONNECT: Understanding the Health Risk Assessment. Physician Webinar Series
 CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
California s Health Homes Program
 California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
Coordinated Care Initiative Frequently Asked Questions for Physicians
 What is the Coordinated Care Initiative? California's Coordinated Care Initiative (CCI) changes the focus and delivery of health care for seniors and people with disabilities. Coordinated care offers participants
What is the Coordinated Care Initiative? California's Coordinated Care Initiative (CCI) changes the focus and delivery of health care for seniors and people with disabilities. Coordinated care offers participants
California s Pediatric Palliative Care. Jill Abramson, MD, MPH November 1, 2012
 California s Pediatric Palliative Care Jill Abramson, MD, MPH November 1, 2012 Outline How a program can change a life Pediatric Palliative Care PFC Overview PFC Results Challenges PFC in the future Case
California s Pediatric Palliative Care Jill Abramson, MD, MPH November 1, 2012 Outline How a program can change a life Pediatric Palliative Care PFC Overview PFC Results Challenges PFC in the future Case
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012
 Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Lessons Learned from the Dual Eligibles Demonstrations. Real-Life Takeaways from California and Other States
 Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
History of Patient Navigation 8/26/17. Cancer Navigation September 26, Agenda
 Cancer Navigation September 26, 2017 Eric T. Kimchi, MD, MBA Medical Director, Ellis Fischel Cancer Center Agenda History of Patient Navigation Principles of Patient Navigation UAB Experience EFCC Initiative
Cancer Navigation September 26, 2017 Eric T. Kimchi, MD, MBA Medical Director, Ellis Fischel Cancer Center Agenda History of Patient Navigation Principles of Patient Navigation UAB Experience EFCC Initiative
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance
 Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
08-16 FORM CMS
 08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Programs and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance Program
 s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Health Policy Brief. Better Outcomes, Lower Costs: Palliative Care Program Reduces Stress, Costs of Care for Children With Life-Threatening Conditions
 Health Policy Brief August 2012 Better Outcomes, Lower Costs: Palliative Care Program Reduces Stress, Costs of Care for Children With Life-Threatening Conditions Daphna Gans, Gerald F. Kominski, Dylan
Health Policy Brief August 2012 Better Outcomes, Lower Costs: Palliative Care Program Reduces Stress, Costs of Care for Children With Life-Threatening Conditions Daphna Gans, Gerald F. Kominski, Dylan
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
HOMECARE AND HOSPICE REIMBURSEMENT
 Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions
 Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016
 8/19/2016 IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016 Susan Campbell, Community Liaison Crystal Godfrey, RN, BSN, Director of Clinical Services Premier
8/19/2016 IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016 Susan Campbell, Community Liaison Crystal Godfrey, RN, BSN, Director of Clinical Services Premier
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Database Profiles for the ACT Index Driving social change and quality improvement
 Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)
 DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)") SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Common Questions Asked by Patients Seeking Hospice Care
 Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
2015 National Training Program. History of Modern Hospice. Hospice Legislative History. Medicare s Coverage of Hospice Services
 2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Wow ADVANCE CARE PLANNING The continued Frontier. Kathryn Borgenicht, M.D. Linda Bierbach, CNP
 Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
ENVISIONING THE FUTURE OF THE CALIFORNIA CHILDREN S SERVICES PROGRAM (CCS) IMPROVING CARE COORDINATION WHILE PRESERVING ACCESS TO HIGH QUALITY CARE
 IMPROVING CARE COORDINATION WHILE PRESERVING ACCESS TO HIGH QUALITY CARE") ENVISIONING THE FUTURE OF THE CALIFORNIA CHILDREN S SERVICES PROGRAM (CCS) IMPROVING CARE COORDINATION WHILE PRESERVING ACCESS TO HIGH QUALITY CARE California Children s Hospital Association March 2015
ENVISIONING THE FUTURE OF THE CALIFORNIA CHILDREN S SERVICES PROGRAM (CCS) IMPROVING CARE COORDINATION WHILE PRESERVING ACCESS TO HIGH QUALITY CARE California Children s Hospital Association March 2015
New York State Medicaid Value Based Payment: Data Driven Strategies. Bundled Payment Summit June 27, 2017
 New York State Medicaid Value Based Payment: Data Driven Strategies Bundled Payment Summit June 27, 2017 Panelists Moderator Paloma Hernandez Anthony Thompson Marc Berg President and CEO Urban Health Plan
New York State Medicaid Value Based Payment: Data Driven Strategies Bundled Payment Summit June 27, 2017 Panelists Moderator Paloma Hernandez Anthony Thompson Marc Berg President and CEO Urban Health Plan
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Overview of the Hospice Proposed Rule
 HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
Health Home Program (HHP)
") Comparison of California s, Whole Person Care Pilot, Program, and March 16, 2016 This document summarizes and compares four major California initiatives: 1) the Health Homes for Patients with Complex Needs
Comparison of California s, Whole Person Care Pilot, Program, and March 16, 2016 This document summarizes and compares four major California initiatives: 1) the Health Homes for Patients with Complex Needs
Heart of Hope Asian America Hospice Care 希望之 心安寧醫護關懷中 心
 Heart of Hope Asian America Hospice Care 希望之 心安寧醫護關懷中 心 Teleconference 2017.01.19 Prepared by: Che-Fai Au (fai@mac.com) Hospice Care through Medicare, Medi-Cal, and Private Insurance Hospice care is a
Heart of Hope Asian America Hospice Care 希望之 心安寧醫護關懷中 心 Teleconference 2017.01.19 Prepared by: Che-Fai Au (fai@mac.com) Hospice Care through Medicare, Medi-Cal, and Private Insurance Hospice care is a
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Minnesota Rural Palliative Care Initiative
 Minnesota Rural Palliative Care Initiative Janelle Shearer, RN, BSN, MA 2010 Minnesota Gerontological Society Annual Spring Conference - Pushing the Envelope: Innovative Models for Aging Populations April
Minnesota Rural Palliative Care Initiative Janelle Shearer, RN, BSN, MA 2010 Minnesota Gerontological Society Annual Spring Conference - Pushing the Envelope: Innovative Models for Aging Populations April
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Other languages and formats
 Dear member, We re glad you re part of our health plan! It s important to us that you have the most up-to-date information about your benefits. We re sending you the following notices with this letter:
Dear member, We re glad you re part of our health plan! It s important to us that you have the most up-to-date information about your benefits. We re sending you the following notices with this letter:
Breathing Easy: A Case Study on Asthma Prevention
 Breathing Easy: A Case Study on Asthma Prevention Bob Morrow, MD, MBA Market President, Houston & Southeast Texas Blue Cross and Blue Shield of Texas @DrBobMorrow A Division of Health Care Service Corporation,
Breathing Easy: A Case Study on Asthma Prevention Bob Morrow, MD, MBA Market President, Houston & Southeast Texas Blue Cross and Blue Shield of Texas @DrBobMorrow A Division of Health Care Service Corporation,
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training
 Santa Clara County Behavioral Health provider training") Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
California s Coordinated Care Initiative
 California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
DHCS Update: Major Initiatives and Strategies Towards Standardization
 DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
Cal MediConnect (CMC) Model of Care
 Model of Care") Cal MediConnect (CMC) Model of Care CMC MOC Annual Training Presentation for Providers and Health Net Associates Presentation by Health Net Medical Management Training Department Herminia Escobedo Health
Cal MediConnect (CMC) Model of Care CMC MOC Annual Training Presentation for Providers and Health Net Associates Presentation by Health Net Medical Management Training Department Herminia Escobedo Health
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual
 HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual Issued April 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10 diagnosis
HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual Issued April 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10 diagnosis
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s)
") Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Reference Guide for Hospice Medicaid Services
 Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Model Of Care: Care Coordination Interdisciplinary Care Team (ICT)
") Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Molina Medicare Model of Care
 Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Administrative Guide. KanCare Program Chapter 11: Hospice. Physician, Health Care Professional, Facility and Ancillary. UHCCommunityPlan.
 KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
Hospice 101. Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati
 Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
Toolkit Development for a Community-Based Palliative Care Program
 Grand Valley State University ScholarWorks@GVSU Doctoral Projects Kirkhof College of Nursing 3-30-2017 Toolkit Development for a Community-Based Palliative Care Program Tanya A. Rowerdink Grand Valley
Grand Valley State University ScholarWorks@GVSU Doctoral Projects Kirkhof College of Nursing 3-30-2017 Toolkit Development for a Community-Based Palliative Care Program Tanya A. Rowerdink Grand Valley
PCQN Forum. Steven Pantilat, MD Kara Bischoff, MD Angela Marks, MSEd. PCQN Conference May 3, 2018
 PCQN Forum Steven Pantilat, MD Kara Bischoff, MD Angela Marks, MSEd PCQN Conference May 3, 2018 PCQN 111 Member Organizations 69 Community Hospitals 14 Academic Hospitals 11 Public Hospitals 17 Community-Based
PCQN Forum Steven Pantilat, MD Kara Bischoff, MD Angela Marks, MSEd PCQN Conference May 3, 2018 PCQN 111 Member Organizations 69 Community Hospitals 14 Academic Hospitals 11 Public Hospitals 17 Community-Based
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015
 PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015 HENRY R. DESMARAIS, MD, MPA HEALTH POLICY ALTERNATIVES, INC. A POSSIBLE OPTION MENU QUALITY Ø Add palliative
PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015 HENRY R. DESMARAIS, MD, MPA HEALTH POLICY ALTERNATIVES, INC. A POSSIBLE OPTION MENU QUALITY Ø Add palliative
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,