Not so Trivial Pursuit - PCMH Edition. Chris Espersen, MSPH Mandy May, MPH
|
|
|
- Darrell James
- 5 years ago
- Views:
Transcription
1 Not so Trivial Pursuit - PCMH Edition Chris Espersen, MSPH Mandy May, MPH
2 Learning Objectives Apply best practices to become a true medical home Understand the new 2017 NCQA PCMH standards Adapt tools to organize, maintain, and sustain your medical home transformation
3 Our time together today Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
4

 Enroll in")
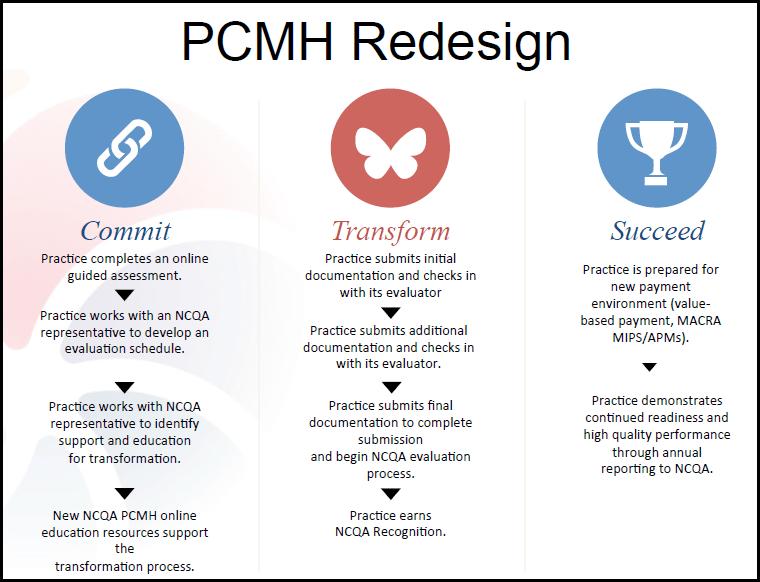
5 Commit Get buy-in Review standards, get trained Determine eligible clinicians Determine sites and fee schedule HRSA Notice of Intent (PAL ) Enroll in QPASS
6


7 Transform Get buy-in Identify current state and ideal state Implement new workflows, policies and procedures Gather documentation for evidence Introductory call Up to 3 virtual check-ins Peer Review Committee
8
9 Project Management Tools for Success Agile project management methodology Kick off Bi-weekly sprints Project Charter Communication Tools
 within 8 Sprints. The 9th Sprint was not needed as such.")

10 1 0 Sprint Effort The team completed the PCMH Standards review and subsequent work required (policies, workflows, reports, etc.) within 8 Sprints. The 9th Sprint was not needed as such. A small subset of the Project Team involved in the NCQA Check In Calls and related efforts continued to meet and work outside the Sprint format. Number of Sprints to Complete Items Items Completed per Sprint

11 Succeed Maintain transformation Enhance model Annual reporting
12 Maintaining and sustaining

13 Keeping organized 2 hour task
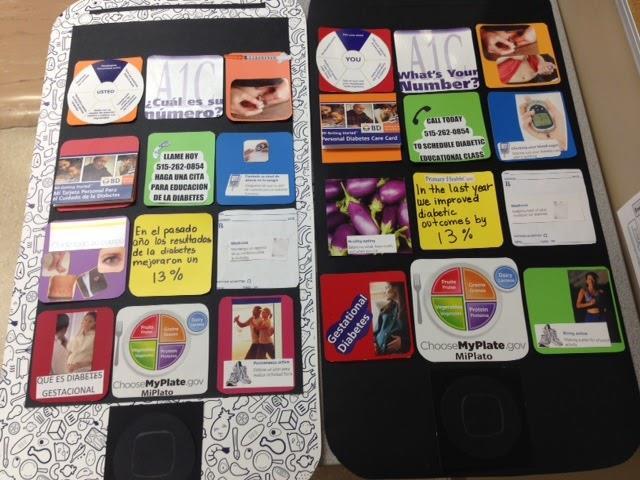
14 Data Engagement



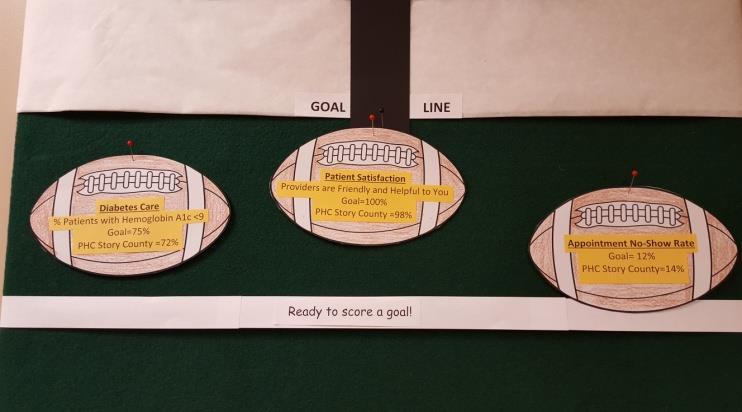
15 Patient and Staff Engagement Goal # 5 Improve Patient Experience
16 Dashboards


17 Insatiable thirst for data 100% 95% I get called back quickly Staff questionnaire on phone note process 90% 85% 80% 75% 70% 65% 60% QTR QTR QTR QTR QTR QTR QTR Patient Satisfaction Data QTR QTR Phone note chart audit
18 Team Based Care & Practice Organization The practice provides continuity of care, communicates roles and responsibilities of the medical home to patients/families/caregivers, and organizes and trains staff to work to the top of their license and provide effective team-based care. Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
19 Team Based Care & Practice Organization Competency A: The practice is committed to transforming the practice into a sustainable medical home. Members of the care team serve specific roles as defined by the practice s organizational structure and are equipped with the knowledge and training necessary to perform those functions. Competency B: Communication among staff is organized to ensure that patient care is coordinated, safe and effective. TC 01 (Core): Designates a clinician lead of the medical home and a staff person to manage the PCMH transformation and medical home activities. TC 03 (1 Credit): The practice is involved in external PCMH-oriented collaborative activities (e.g., federal/state initiatives, health information exchanges). TC 04 (2 Credits): Patients/families/caregivers are involved in the practice s governance structure or on stakeholder committees. TC 08 (2 Credits) Has at least one care manager qualified to identify and coordinate behavioral health needs.
20 TC Community Focused Criteria TC 03 (1 Credit): The practice is involved in external PCMH-oriented collaborative activities (e.g., federal/state initiatives, health information exchanges). TC 04 (2 Credits): Patients/families/caregivers are involved in the practice s governance structure or on stakeholder committees.
21 Knowing and Managing Your Patients The practice uses information about the patients and community it serves to deliver evidence-based care that supports population needs and provision of culturally and linguistically appropriate services. Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
22 Knowing and Managing Your Patients KM 02 (Core): Comprehensive health assessment includes (all items required): F. Social functioning. G. Social determinants of health. KM 05 (1 Credit): Assesses oral health needs and provides necessary services during the care visit based on evidence-based guidelines or coordinates with oral health partners. KM 07 (2 Credits): Understands social determinants of health for patients, monitors at the population level and implements care interventions based on these data. KM 11 (1 Credit): Identifies and addresses population-level needs based on the diversity of the practice and the community (at least two): A. Target population health management on disparities in care. C. Educate practice staff in cultural competence. KM 18 (1 Credit): Reviews controlled substance database when prescribing relevant medications. KM 21 (Core): Uses information on the population served by the practice to prioritize needed community resources. KM 04 (1 Credit): Conducts behavioral health screenings and/or assessments using a standardized tool. (Implement two or more.) A. Anxiety. B. Alcohol use disorder. C. Substance use disorder. D. Pediatric behavioral health screening. E. Post-traumatic stress disorder. F. Attention deficit/hyperactivity disorder. G. Postpartum depression. KM 06 (1 Credit): Identifies the predominant conditions and health concerns of the patient population. KM 08 (1 Credit): Evaluates patient population demographics/communication preferences/health literacy to tailor development and distribution of patient materials. KM 13 (2 Credits): Demonstrates excellence in a benchmarked/ performance-based recognition program assessed using evidencebased care guidelines. KM 19 (2 Credits): Systematically obtains prescription claims data in order to assess and address medication adherence. KM 23 (1 Credit): Provides oral health education resources to patients. KM 25 (1 Credit): Engages with schools or intervention agencies in the KM 28 (2 Credits): Has regular case conferences involving parties community. outside the practice team (e.g., community supports, specialists)
23 KM Community focused criteria KM 07 (2 Credits): Understands social determinants of health for patients, monitors at the population level and implements care interventions based on these data. KM 10 (Core): Assesses the language needs of its population. KM 19 (2 Credits): Systematically obtains prescription claims data in order to assess and address medication adherence. KM 21 (Core): Uses information on the population served by the practice to prioritize needed community resources. KM 22 (1 Credit): Provides access to educational resources, such as materials, peer-support sessions, group classes, online self-management tools or programs. KM 25 (1 Credit): Engages with schools or intervention agencies in the community. KM 26 (1 Credit): Routinely maintains a current community resource list based on the needs identified in KM 21. KM 27 (1 Credit): Assesses the usefulness of identified community support resources. KM 28 (2 Credits): Has regular case conferences involving parties outside the practice team (e.g., community supports, specialists).
24 Patient Centered Access and Continuity The practice provides 24/7 access to clinical advice and appropriate care facilitated by their designated clinician/care team, considers the needs and preferences of the patient population when modeling standards for access. Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
25 Patient Centered Access and Continuity Competency Competency A: The practice seeks to enhance access by providing appointments and clinical advice based on patients needs Competency B: Practices support continuity through empanelment and systematic access to the patient s medical record Core Criteria AC 01 (core) Assess the access needs and preferences of the patient population AC 09 (1 Credit): Uses information about the population served by the practice to assess equity of access that considers health disparities. AC 13 (1 credit) Reviews and actively manages panel sizes. AC 14 (1 credit) Reviews and reconciles panels based on health plan or other outside patient assignments.
26 AC Community Focused Criteria AC 03 (core) Appointments Outside Business Hours: Provides routine and urgent appointments outside regular business hours to meet identified patient needs. *May arrange for patients to schedule appointments with other facilities or clinicians. AC 14 (1 credit) External Panel Review and Reconciliation: Reviews and reconciles panels based on health plan or other outside patient assignments
27 Care Coordination and Transitions The practice systematically tracks tests and coordinates care across specialty care, facility-based care and community organizations Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
28 Care Coordination and Care Transitions Competency Competency A: The practice effectively tracks and manages laboratory and imaging tests important for patient care and informs patients of the result. Competency B: The practice provides important information in referrals to specialists and tracks referrals until the report is received. Competency C: The practice connects with health care facilities to support patient safety throughout care transitions. The practice received and shares necessary patient treatment information to coordinate comprehensive patient care. Core Criteria CC 03 (2 Credits): Uses clinical protocols to determine when imaging and lab tests are necessary. CC 05 (2 Credits): Uses clinical protocols to determine when a referral to a specialist is necessary. CC 06 (1 Credit): Identifies the specialists/specialty types frequently used by the practice. CC 11 (1 Credit): Monitors the timeliness and quality of the referral response. CC 13 (2 Credits): Engages with patients regarding cost implications of treatment options. CC 17 (1 Credit): Systematic ability to coordinate with acute care settings after office hours through access to current patient information.
29 CC Community Focused Criteria CC 04 (Core) Practice systematically manages referrals. CC05 (2 credits) Uses clinical protocols to determine when a referral to a specialist is necessary. CC 06 (1 credit) Identifies the specialist/specialty types frequently used by the practice. CC 07 (2 credits) Considers available performance information on consultants/specialists when making referrals. CC 08 (1 credit) Works with nonbehavioral healthcare specialists to whom the practice frequently refers to set expectations for information sharing and patient care. CC 09 (2 credits) Works with behavioral healthcare providers to whom the practice frequently refers to set expectations for information sharing and patient care. CC 11 (1 credit) Monitors the timeliness and quality of the referral response. CC 15 (Core) Shares clinical information with admitting hospitals and emergency departments CC 17 (1 Credit) Systematic ability to coordinate with acute care settings after office hours through access to current patient information.
30 Care Management and Support The practice systematically tracks tests, referrals, and care transitions to achieve high quality care coordination, lower costs, improve patient safety and ensure effective communication with specialists and other providers in the medical neighborhood. Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
31 Care Management and Support Competency A: The practice systematically identifies patients who may benefit from care management. Competency B: For patients identified for care management, the practice consistently uses patient information and collaborates with patients/families/ caregivers to develop a care plan that addresses barriers and incorporates patient preferences and lifestyle goals documented in the patient s chart. CM 03 (2 Credits): Applies a comprehensive riskstratification process for the entire patient panel in order to identify and direct resources appropriately. CM 09 (1 Credit): Care plan is integrated and accessible across settings of care.
32 CM Community Focused Criteria CM 01 (Core): Considers the following when establishing a systematic process and criteria for identifying patients who may benefit from care management (practice must include at least three in its criteria): A. Behavioral health conditions. B. High cost/high utilization. C. Poorly controlled or complex conditions. D. Social determinants of health. E. Referrals by outside organizations (e.g., insurers, health system, ACO), practice staff, patient/ family/caregiver. CM 07 (1 Credit): Identifies and discusses potential barriers to meeting goals in individual care plans. CM 09 (1 Credit): Care plan is integrated and accessible across settings of care.
33 Performance Measurement and Quality Improvement The practice establishes a culture of data-driven performance improvement on clinical quality, efficiency, and patient experience, and engages staff and patients/families/caregivers in quality improvement activities. Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
34 Performance Measurement and Quality Improvement Competency Competency A: The practice measures to understand current performance and to identify opportunities for improvement Competency B: The practice evaluates its performance against goals or benchmarks and uses the results to prioritize and implement improvement strategies Competency C: The practice is accountable for performance. The practice shares performance data with the practice, patients and/or publicly for the measures and patient populations identified in the previous section Core Criteria QI 01 (Core) Monitors at least 5 clinical quality measures across the 4 categories (includes behavioral health measure) QI 08 (Core) Sets goals and acts to improve performance upon at least 3 measures across 3 of 4 categories (includes behavioral health measure) QI 14 (2 credits) Achieves improved performance on at least 1 measure of disparities in care or service. QI 19 (max 2 credits) Is engaged in value based agreement (upside risk contract or two-sided risk contract)
35 QI Community Focused Criteria QI 16 (1 credit) Reports practice-level or individual clinician performance results publicly or with patients for measures reported by the practice. QI 18 (2 credits) Reports clinical quality measures to Medicare or Medicaid agency. QI 19 (Max 2 credits Is engaged in Value-Based Agreement (upside risk contract = 1 credit, two-sided risk contract = 2 credits).
36 Good Luck in Your Pursuits! Chris Espersen (919) Mandy May (303) Team Based Care & Practice Org Patient Centered Access & Continuity Care Coordination & Transitions Knowing & Managing Patients Care Management & Support PM & QI
Introduction to PCMH 2017
 Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
QI ROUNDTABLE. NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA
 QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
NCQA PCMH 2017 Standard Two 4/11/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017
 Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
NCQA PCMH 2017 Standards Intro 3/29/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
PCMH Standards and Guidelines
 PCMH Standards and Guidelines Team-Based Care and Practice Organization (TC)... 31 Competency A... 31 TC 01 PCMH Transformation Leads... 31 TC 02 Structure and Staff Responsibilities... 31 TC 03 External
PCMH Standards and Guidelines Team-Based Care and Practice Organization (TC)... 31 Competency A... 31 TC 01 PCMH Transformation Leads... 31 TC 02 Structure and Staff Responsibilities... 31 TC 03 External
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
PCMH Standards and Guidelines
 PCMH Standards and Guidelines Team-Based Care and Practice Organization (TC)... 31 Competency A... 31 TC 01 PCMH Transformation Leads... 31 TC 02 Structure and Staff Responsibilities... 31 TC 03 External
PCMH Standards and Guidelines Team-Based Care and Practice Organization (TC)... 31 Competency A... 31 TC 01 PCMH Transformation Leads... 31 TC 02 Structure and Staff Responsibilities... 31 TC 03 External
PCMH 2017 Performance Measurement and Quality Improvement
 PCMH 2017 Performance Measurement and Quality Improvement Performance Measurement and Quality Improvement If you are PCMH 2011 practice or PCMH 2014 Level 1: you are not eligible for annual reporting If
PCMH 2017 Performance Measurement and Quality Improvement Performance Measurement and Quality Improvement If you are PCMH 2011 practice or PCMH 2014 Level 1: you are not eligible for annual reporting If
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State
 Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Patient Centered Medical Home 2017 Redesign
 Patient Centered Medical Home 2017 Redesign Patient-Centered Medical Home Objectives for today: 2017 Redesign Why the redesign? Discussion of the 2017 Redesign Understand core criteria and menu criteria
Patient Centered Medical Home 2017 Redesign Patient-Centered Medical Home Objectives for today: 2017 Redesign Why the redesign? Discussion of the 2017 Redesign Understand core criteria and menu criteria
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Patient Centered Medical Home (PCMH) Training. August 11, 2017
 Training. August 11, 2017") Patient Centered Medical Home (PCMH) Training August 11, 2017 Wi-Fi Network Name: attwifi Promo Code: rmhp Overview: What is a Patient-Centered Medical Home? Anna Messinger, MHA, PCMH CCE August 11, 2017
Patient Centered Medical Home (PCMH) Training August 11, 2017 Wi-Fi Network Name: attwifi Promo Code: rmhp Overview: What is a Patient-Centered Medical Home? Anna Messinger, MHA, PCMH CCE August 11, 2017
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Appendix 4. PCMH Distinction in Behavioral Health Integration
 Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Clinical Medical Standing Orders (PCMH 1G) Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)
 Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)") Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs
 The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Behavioral and Mental Health: High-Weighted. Behavioral and Mental Health: Medium-Weighted. Implementation of co-location PCP and MH services
 Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Practice Transformation Networks
 Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard
 April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
URAC Patient Centered Medical Home
 URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Improvement Activities Data Validation Criteria
 Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F
 Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers
: Strategies to Overcome Implementation Barriers") Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
2014 PCMH STANDARDS. Renewals & Annual Data Requirements
 2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Chapter 4 Health Care Management Unit 5: Quality Management
 Chapter 4 Health Care Management Unit 5: Quality Management In This Unit Topic See Page Unit 5: Quality Management Quality Management Program 2 Prevention and Wellness 4 Clinical Quality 5 Network Quality
Chapter 4 Health Care Management Unit 5: Quality Management In This Unit Topic See Page Unit 5: Quality Management Quality Management Program 2 Prevention and Wellness 4 Clinical Quality 5 Network Quality
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
URAC Patient Centered Health Care Home (PCHCH) Education, Evaluation, and Recognition
 Education, Evaluation, and Recognition") URAC Patient Centered Health Care Home (PCHCH) Education, Evaluation, and Recognition PRESENTER: Michelle Phipps, RN, PhD Sr. Director of Clinical Education and Conferences DATE: March 13, 2013 Focus On
URAC Patient Centered Health Care Home (PCHCH) Education, Evaluation, and Recognition PRESENTER: Michelle Phipps, RN, PhD Sr. Director of Clinical Education and Conferences DATE: March 13, 2013 Focus On
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet
 Cohort 3 Request for Application (RFA) Packet") Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD
 MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
National Committee for Quality Assurance
 National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Community Health Centers: Medical Homes in the Safety Net. Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health
 Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions
 Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Accountable Care Organizations. What the Nurse Executive Needs to Know. Rebecca F. Cady, Esq., RNC, BSN, JD, CPHRM
 JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
I. OPERATIONAL CHARACTERISTIC: PATIENT-CENTEREDNESS
 I. OPERATIONAL CHARACTERISTIC: PATIENT-CENTEREDNESS A. FOCUS AREA: INFORMATION TO PATIENTS ABOUT PCMH 1. The organization provides information to the patient about: (indicate Yes or No to each item) Yes
I. OPERATIONAL CHARACTERISTIC: PATIENT-CENTEREDNESS A. FOCUS AREA: INFORMATION TO PATIENTS ABOUT PCMH 1. The organization provides information to the patient about: (indicate Yes or No to each item) Yes
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee