High Cost Users for LHINs & Health Links. Health Analytics Branch, HSIMI September 2013
|
|
|
- Lucy Chapman
- 5 years ago
- Views:
Transcription
1 High Cost Users for LHINs & Health Links Health Analytics Branch, HSIMI September 2013

2 Distribution of Costs, 2010/11 Proportion of Ontario Patients Proportion of Costs 2
3 Defining the high cost user In the following analyses, high cost users are the 10% of patients with the highest combined cost in 2010/11 for the following health care services: Acute Care Day Surgery Emergency Rooms Inpatient Rehabilitation Inpatient Mental Health Complex Continuing Care Home Care Long-Term Care Physician Claims These sectors account for approximately 74% of the Ministry/LHIN operating expenses The analysis is based on cost alone. This group of patients may include those with a single very expensive event (e.g. transplants) or multiple events with high combined cost (e.g., care for chronic conditions). 3
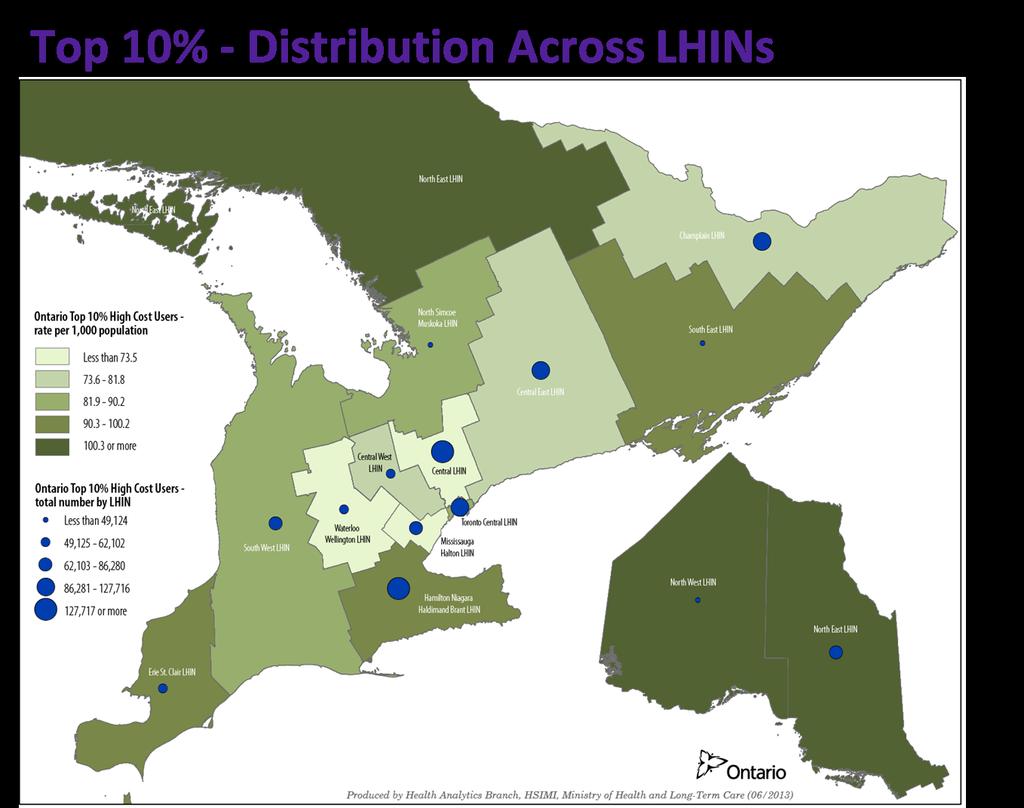
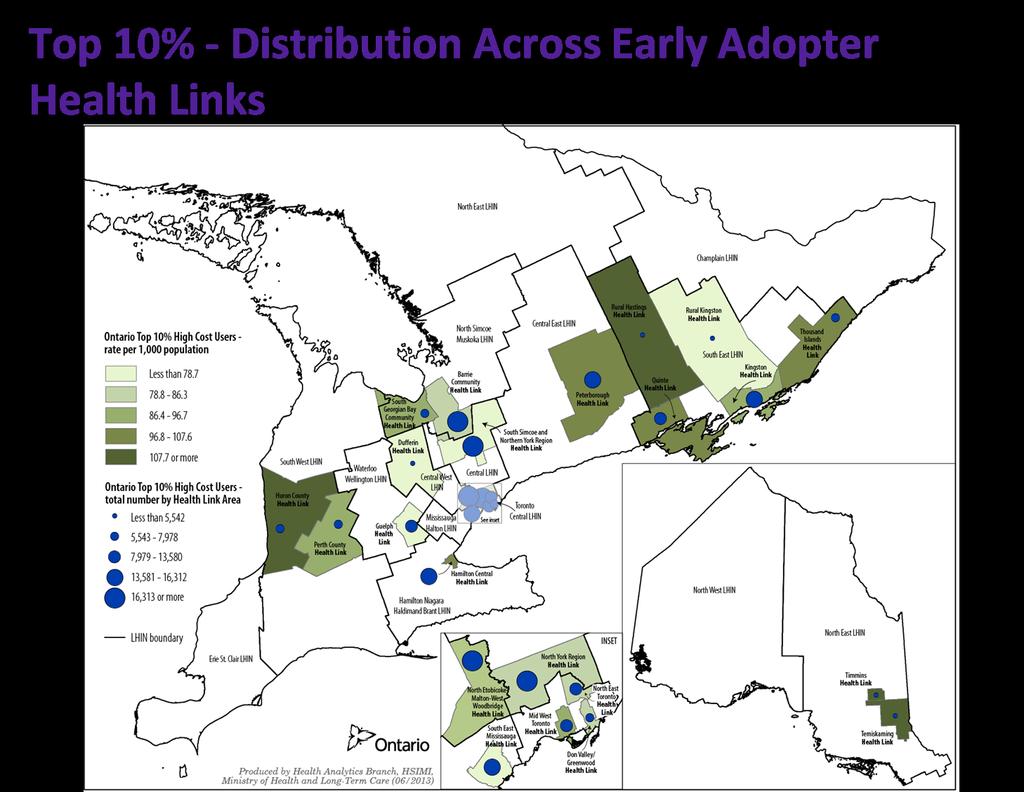
4 Purpose of Current Analyses Upon the establishment of the Early Adopter Health Links, the ministry received requests for high cost user analyses for these areas. The following describes analyses of the high cost users at the LHIN and Health Link levels (22 Health Links approved as of February 2013); the analysis focuses on the 10% of patients who reside within each Health Link area who had the highest combined cost in 2010/11. Due to the small size of some Health Link areas the analysis has been done only for the Top 10% patients. The analysis was done separately for each geographic area. Note that LHIN/Health Link High Cost Users may not be within the Ontario high cost users. 4
5 5
6 6
7 Key Findings Regardless of whether we focus on the high cost users at the Health Link, LHIN or provincial level, the following key findings are applicable: 1. A patient who is a high cost user in one fiscal year may not continue to be a high cost user in future years. 2. Rare conditions, such as transplants, low birth weight babies, and burns have the highest average acute care cost, while chronic conditions, hip fracture, hip replacement and palliative care have the highest total cost. Health Links have the potential to impact certain groups of high cost users. 3. High cost users are a diverse group, but typically have two key characteristics: They receive treatment from multiple health care sectors and/or have long lengths of stay in inpatient settings. 7
8 Key Findings (continued) 4. For most sectors, the average number of episodes and cost per episode is similar for high cost users and all users. However, high cost users access a larger number of health care sectors. 5. The characteristics of patients and patterns of health care utilization among high cost users are similar across geographic areas. Seniors represent the largest percentage of patients/expenses and have the highest average cost per patient. Acute care, physician visits, and long-term care represent the largest percentage of expenses. 6. The profile of high cost users is consistent with the population structure of the area. Areas with more seniors will have more seniors among the high cost user patients. Areas with more young families will have more children and young adults among the high cost user patients. 8
9 Understanding the High Cost User, 2010/11 9
10 High Cost User Patients Example Profiles High cost users access multiple types of care and have long lengths of stay Female, age yrs (cost: $1 million) Acute inpatient care : 5 discharges 190 acute days + 60 ALC days Male, age yrs (cost: $570,000) Male, age 80+ yrs (cost: $240,000) Acute inpatient care: 2 discharges 70 acute days + 90 ALC days Acute inpatient care: 3 discharges 75 acute days Emergency: 5 visits Day surgery: 1 visit CCC: 1 episode, 340 days Homecare: 62 services Nursing, physiotherapy, OT and personal support Physician visits\claims: 105 Problems\Conditions: Heart transplant, congestive heart failure, digestive symptoms, cellulitis, cardiovascular screening, transplant rejection CCC: 1 admission, 80 days Inpatient Rehab: 1 discharge, 130 days Physician visits\claims: 170 Problems\Conditions: Respiratory failure, traumatic brain injury, craniofacial bone intervention Emergency Dept: 3 visits Day Surgery: 2 visits Homecare: 12 services Nursing, Physiotherapy Physician visits\claims: 105 Problems\Conditions: AMI\angina, AMI\shock arrest\with cardiac cath., respiratory intervention, gastrointestinal intervention, screening exam, cardiac study, endoscopic inspection digestive tract 10

11 Once a high cost user not necessarily always a high cost user 11
12 Conditions in Acute Care Highest Average Cost Case Mix Group Separations/ Discharges Top 10% Patient Segment Total Expense ($) Average Expense ($) 160 Heart or Lung Transplant 65 $ 11,360,000 $ 169, Extensive Burn with Skin Graft 35 $ 5,320,000 $ 161, Newborn/Neonate gm with Major 145 $ 20,830,000 $ 145,700 Cardiovascular Intervention 110 Lung Transplant 60 $ 7,520,000 $ 121, Newborn/Neonate <750 grams 200 $ 21,420,000 $ 108, Failure/Rejection Lung Transplant 10 $ 890,000 $ 98, Newborn/Neonate gm with Major 170 $ 16,420,000 $ 95,500 Gastrointestinal/Diaphragm Intervention 579 Newborn/Neonate grams, Gestational 305 $ 27,720,000 $ 90,900 Age <29 Weeks 270 Liver/Pancreas/Duodenum Transplant 195 $ 15,910,000 $ 81, Newborn/Neonate grams, Gestational Age <29 Weeks 375 $ 25,420,000 $ 68,100 List includes relatively rare events with very high acute care cost. 12
13 Conditions in Acute Care Highest Total Cost Case Mix Group Separations/ Discharges Top 10% Patient Segment Total Expense ($) Average Expense ($) 139 Chronic Obstructive Pulmonary Disease 23,520 $ 187,110,000 $ 8, Vaginal Delivery, No Other Intervention 64,505 $ 179,670,000 $ 2, Heart Failure without Cardiac Catheter (CHF) 19,100 $ 170,380,000 $ 8, Unilateral Knee Replacement 19,335 $ 163,560,000 $ 8, Viral/Unspecified Pneumonia 19,220 $ 142,940,000 $ 7, Palliative Care 12,660 $ 134,050,000 $ 10, Colostomy/Enterostomy 4,315 $ 127,420,000 $ 29, Cardiac Valve Replacement 3,150 $ 119,620,000 $ 38, Percutaneous Coronary Intervention with MI/Shock/Arrest/Heart Failure (Angioplasty) 9,410 $ 118,920,000 $ 12, Fixation/Repair Hip/Femur (Hip Fracture) 7,285 $ 115,300,000 $ 15,800 List includes chronic conditions with moderate to high acute care costs. Patients with vaginal delivery are among the high cost users because they have numerous physician visits, and other types of care in addition to the cost of the birth. 13

14 Number of Sectors Used Top 10% patients for Ontario Top 10% patients by Health Link Health Link Area of Residence Average # of Sectors Used 3% used a single sector. 89% used 2-4 sectors. 7% used 5 or more sectors. The average number of sectors used was 3.0. The average number of sectors used by LHIN of patient residence ranged from 2.8 to 3.4. Perth County 3.3 Huron 3.4 Guelph 3.0 Hamilton Central 3.3 N. Etobicoke-Malton-W. Woodbridge 2.9 Dufferin 3.1 South East Mississauga 2.9 Mid Toronto West 2.8 Don Valley/Greenwood 2.8 North Toronto East 2.8 S. Simcoe and Northern York 2.9 North York Region 2.9 Peterborough 3.3 Rural Hastings 3.3 Quinte 3.3 Rural Kingston 3.0 Kingston 3.1 Thousand Islands 3.3 Barrie Community 3.0 South Georgian Bay 3.2 Temiskaming 3.4 Timmins 3.4 The average number of sectors used ranged from 2.8 to
15 Proportion of patients by sector type If we compare all Ontario users to the top 10% : Nearly 100% of patients had a physician visit. 26% of all users and 63% of high cost users had an emergency visit 7% of all users and 61% of high cost users had an acute care discharge 9% of all users and 33% of high cost users had a day surgery visit 4% of all users and 27% of high cost users received a homecare service 1% of all users and 9% of high cost users spent time in long-term care While the magnitude varied, the patterns of utilization for both groups were similar at the Health Link and LHIN of residence level. 15
16 Event Frequency by Sector Among the Ontario top 10% patients: 96% had 6 or more physician visits in 2010/11. For all other sectors, among the patients with activity, the largest proportion had a single event. 26% of patients had 1 emergency visit, while 21% had 3 or more visits. Less than 10% of patients received treatment in mental health, rehabilitation, CCC, or LTC. 27% of patients received homecare with an average of 77 visits/hours per patient. 16
17 Total Length of Stay (LOS) Patients in the top 10% in Ontario: Account for % of the total LOS for all Ontario users within each sector. Have 6.3 million total days in acute care, including 1 million ALC and 720,000 special care unit days. Have 718,000 days in inpatient rehabilitation. Have 1.4 million days in inpatient mental health. Have 1.7 million days in complex continuing care. Have 27.4 million days in long-term care. 17
18 Comparison of Analyses /10 vs. 2010/11 All Users Top 10% 2009/ /11 Total Patients 3,901,620 11,160,290 Total Expense (Billions) $14.2 $25.2 Average Cost per Patient $3,500 $2,300 Patients 390,160 1,116,030 Total Expense (Billions) $10.6 $19.4 Average Cost per Patient $27,000 $17,400 % of Total Expense 75% 77% With the addition of LTC and Physician visits, the number of patients and the expense increased among all users and high cost users; however the average cost per patient declined. However, regardless of the method, 10% of patients account for just over 75% of the included health care expenditures. 18
19 Expense Summary Early Adopter Health Links The top 10% patients account for 74-81% of the total expenses for Health Link residents and 74-78% of expenses for LHIN residents, indicating that the proportion of total expenses for high cost users is consistent across Health Links and LHINs. All Users Health Link Area of Residence Total Patients Expense (Millions) Perth County 61, Huron 51, Guelph 119, Hamilton Central 123, N. Etobicoke-Malton-W. Woodbridge 189, Dufferin 57, South East Mississauga 159, Mid Toronto West 123, Don Valley/Greenwood 68, North Toronto East 100, S. Simcoe and Northern York 224, North York Region 554,125 1,258 Peterborough 118, Rural Hastings 33, Quinte 106, Rural Kingston 27, Kingston 113, Thousand Islands 63, Barrie Community 168, South Georgian Bay 49, Temiskaming 28, Timmins 36, Patients Total Expense (Millions) Top 10% % of Total Expense for All Users Average Expense $ 6,105 $ $ 18,300 $ 5,185 $ $ 20,800 $ 11,975 $ $ 15,900 $ 12,385 $ $ 27,100 $ 18,950 $ $ 15,200 $ 5,720 $ $ 15,600 $ 15,990 $ $ 14,800 $ 12,320 $ $ 22,700 $ 6,810 $ $ 20,100 $ 10,060 $ $ 17,200 $ 22,500 $ $ 14,700 $ 55,415 $ $ 17,300 $ 11,840 $ $ 21,400 $ 3,390 $ $ 20,800 $ 10,660 $ $ 20,200 $ 2,740 $ $ 17,200 $ 11,345 $ $ 23,300 $ 6,305 $ $ 23,100 $ 16,845 $ $ 15,600 $ 4,980 $ $ 19,000 $ 2,820 $ $ 26,300 $ 3,685 $ $ 19,800 19
20 Average Cost Per Event Sector Average Cost/Event All Users Top 10% Average Cost/ Inpatient Day Average Cost/Event Average Cost/ Inpatient Day Acute Separation $ 7,678 $ 1,875 $ 8,150 $ 2,026 Rehabilitation Discharge $ 17,944 $ 898 $ 17,913 $ 888 CCC Episode $ 35,775 $ 584 $ 37,133 $ 589 Mental Health Episode $ 18,111 $ 554 $ 21,662 $ 575 LTC Episode $ 20,750 $ 99 $ 24,044 $ 99 Day Surgery Visit $ 981 $ 1,407 Emergency Visit $ 249 $ 391 Physician Visit $ 69 $ 135 Home Care Service (Hour/Visit) $ 54 $ 75 Among all users and Ontario patients in the top 10%: Acute and rehabilitation have the highest average cost per day. Homecare, physician and ED visits have relatively low costs per event. The difference in the average cost for the top 10% vs. all users is relatively small, suggesting that the higher cost is due to a greater number of events rather than more expensive events. 20

 combined account for 58% of the population and 33% of high cost user patients.")
21 Patients and Cost by Age Group If we compare the Ontario population to patients in the top 10%: Seniors account for 41% of high cost user patients, but only 14% of the population. Although infants represent 1% of the population they account for 2.5% of high cost users. Children and young adults (age years) combined account for 58% of the population and 33% of high cost user patients. Seniors and infants have the highest average health care costs, while young adults have the lowest. 21
 reveals that: Peterborough and South Georgian Bay have greater proportions of seniors amongst their high cost users")
22 High Cost User Profile is Consistent with Population Age Structure A comparison of Health Links with larger proportions of seniors (Peterborough, South Georgian Bay) to those with smaller proportions of seniors but larger proportions of children/young adults (Guelph, Dufferin) reveals that: Peterborough and South Georgian Bay have greater proportions of seniors amongst their high cost users (areas above the red lines top 10% bars). In contrast, Guelph and Dufferin have smaller proportions of seniors (areas above the red lines top 10% bars), but larger proportions of children/young adults (areas below the green lines) amongst their high cost users. The profile of high cost users is consistent with the age structure of the population. 22

23 Average Costs are Similar for LHINs and Health Links Among the top 10% patients for LHIN and Health Link residents: North West and North East LHINs had the highest average cost, while Mississauga Halton and Central LHINs residents had the lowest. Hamilton Central and Temiskaming Health Links had the highest average cost, while residents of South Simcoe and Northern York and South East Mississauga Health Links had the lowest. The average cost for the top 10% within a Health Link is similar to the average cost for the top 10% for the LHIN of residence. 23
24 Health Links vs. LHINs Per Cent of Total Expense Health Link/LHIN of Residence Perth County Huron South West LHIN Mid Toronto West Per Cent of Total Expense Don Valley/ Greenwood North Toronto East Toronto Central LHIN Temiskaming Timmins Sector Acute Long-Term Care Physician Visits CCC Inp. Mental Health Homecare Emergency Day Surgery Inp. Rehabilitation North East LHIN Among patients in the top 10% for select Health Links/LHINs: Although there is variation in the magnitude, the per cent of total expense by sector for the Health Links is consistent with the overall values for the LHIN. Acute care accounted for the largest per cent of the expense for all LHINs/Health Links. Long-term care was the 2 nd highest proportion for the South West and North East LHINs and Health Links, while physician visits accounted for the 2 nd highest proportion of expenses for the Toronto Central LHIN and Health Links. 24
25 Health Links vs. LHINs Average number of events Health Link/LHIN of Residence Perth County Huron South West LHIN Mid Toronto West Average Number of Events Don Valley/ Greenwood North Toronto East Toronto Central LHIN Temiskaming Timmins Sector Homecare Physician Visits Emergency Acute Day Surgery Inp. Mental Health Long-Term Care Inp. Rehabilitation CCC North East LHIN Among patients in the top 10% for select Health Links/LHINs: Although there is variation in the magnitude, the average number of events by sector for the Health Links is consistent with the overall values for the LHIN. Homecare and physician visits had the largest average number of events. Homecare services showed the greatest variation within and between LHIN areas. This may be due to the differences in the age structure of the population and/or different service delivery patterns. 25
26 Summary and Conclusions: High cost users are a small, but diverse group; however, their patterns of health care utilization are relatively consistent across geographic areas. The top 10% account for approximately 75% of all health care expenditures. They access an average of 3 different health care sectors. They account for % of the total LOS in each sector. Acute care represents the largest proportion of their expenses. Seniors are more likely to be high cost users than those in other age groups. Only 44% of patients who were high cost users in one fiscal (2009/10) year were still high cost users the following fiscal year (2010/11). The high cost user analyses will always be retrospective. The analysis demonstrates that there is a spectrum of high cost users (from transplant patients to patients with multiple chronic diseases). Health Links have the potential to impact certain groups of high cost users and improve patient care coordination. It is important to focus on the features (patient demographics, diagnoses, utilization trends) that are associated with being identified as a high cost user in order to target populations and assist with planning and service coordination for LHINs and Health Links. 26
27 Appendix 27
28 Changes to the High Cost User Methodology /10 vs. 2010/11 Addition of Long-Term Care and Physician Claims Increases the # of patients from 3.9 million in 2009/10 to 11.1 million in 2010/11 Increases the total expense from $14.2 billion in 2009/10 to $25.2 billion in 2010/11 Inclusion of activity and costs from private, federal, and specialty facilities that receive provincial funding Increases the total hospital expense by $103 million 28
29 Acute Care by Location of Service - LHIN Nearly half, of acute care expenses for Central (49%) and Central West (48%) LHIN residents were for care provided in hospitals outside the LHIN of residence. Only 3% of acute care expenses for Champlain residents were incurred in other LHINs. 29
30 Acute Care by Location of Service Health Link Among the Top 10% of patients by Health Link: 58% of the acute expense for North York residents was for care provided outside Central LHIN. 53% of the acute expenses for North Etobicoke-Malton-West Woodbridge and 48% of the expenses for Dufferin residents were incurred in hospitals outside the Central West LHIN. The large expense for residents of North York Region is due to the large population size of that Health Link. 30
31 Limitations: 31 The ministry is unable to provide the following information: 1. A summary of health care utilization for actual health card numbers. 2. A summary of information for small geographic areas (postal code, FSA). 3. A summary information for specific health care providers. 4. Information for Top 1% and 5% patient segments. 5. Information for all planned areas. 31
Assessing Value in Ontario Health Links. Part 3: Measures of System Performance in Ontario s Health Links
 Assessing Value in Ontario Health Links. Part 3: Measures of System Performance in Ontario s Health Links Applied Health Research Question Series Volume 4.3 Health System Performance Research Network Report
Assessing Value in Ontario Health Links. Part 3: Measures of System Performance in Ontario s Health Links Applied Health Research Question Series Volume 4.3 Health System Performance Research Network Report
Health System Transformation. Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC
 Health System Transformation Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC The Need for Change Historic levels of 6% investment are not sustainable The cost of care
Health System Transformation Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC The Need for Change Historic levels of 6% investment are not sustainable The cost of care
This profile provides an overview of the services provided at the Royal Inland Hospital in the areas of:
 Facility Profile This profile provides an overview of the services provided at the in the areas of: Inpatient Cases & Days Inpatient Surgery & Surgical Day Care Emergency Department The information provided
Facility Profile This profile provides an overview of the services provided at the in the areas of: Inpatient Cases & Days Inpatient Surgery & Surgical Day Care Emergency Department The information provided
Supporting Best Practice for COPD Care Across the System
 Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
2015 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators
 215 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
215 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
Understanding and Identifying Target Populations for Integrated Care
 Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
2016 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators
 216 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
216 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
Waterloo Wellington Community Care Access Centre. Community Needs Assessment
 Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Indicator description
 Patients with a primary care visit within 7 days of acute discharge for Quality Improvement Plans - Primary Care Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term
Patients with a primary care visit within 7 days of acute discharge for Quality Improvement Plans - Primary Care Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term
Provincial Dialysis Capacity Assessment Executive Summary. April 2012
 Provincial Dialysis Capacity Assessment 2011-2020 Executive Summary April 2012 Table of Contents Introduction... 2 Planning Process... 2 Methodology... 3 Dialysis Planning Support Model... 3 Data... 3
Provincial Dialysis Capacity Assessment 2011-2020 Executive Summary April 2012 Table of Contents Introduction... 2 Planning Process... 2 Methodology... 3 Dialysis Planning Support Model... 3 Data... 3
Causes and Consequences of Regional Variations in Health Care Resources in Ontario
 Causes and Consequences of Regional Variations in Health Care Resources in Thérèse A. Stukel, Ph.D. DA Alter, R Saskin, DM Rothwell Institute for Clinical Evaluative Sciences, Health Services Restructuring
Causes and Consequences of Regional Variations in Health Care Resources in Thérèse A. Stukel, Ph.D. DA Alter, R Saskin, DM Rothwell Institute for Clinical Evaluative Sciences, Health Services Restructuring
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
2006 SURVEY OF ORTHOPAEDIC SURGEONS IN ONTARIO
 ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network 2006 SURVEY OF ORTHOPAEDIC SURGEONS IN ONTARIO MARCH 2007 Prepared by: Elizabeth Badley Paula Veinot Jeanette Tyas Mayilee
ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network 2006 SURVEY OF ORTHOPAEDIC SURGEONS IN ONTARIO MARCH 2007 Prepared by: Elizabeth Badley Paula Veinot Jeanette Tyas Mayilee
Health Economics Program
 Health Economics Program Issue Brief 2006-02 February 2006 Health Conditions Associated With Minnesotans Hospital Use Health care spending by Minnesota residents accounts for approximately 12% of the state
Health Economics Program Issue Brief 2006-02 February 2006 Health Conditions Associated With Minnesotans Hospital Use Health care spending by Minnesota residents accounts for approximately 12% of the state
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Developmental /Category III Explanatory/Category II Not Defined Explanatory/Category II Defined Proposed Priority
 The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Northeastern Ontario Clinical Services Review
 Northeastern Ontario Clinical Services Review FINAL PROJECT REPORT Hay Group Health Care Consulting March, 2014 2014 Hay Group Limited. All rights reserved Contents 1.0 EXECUTIVE SUMMARY... 1 1.1 BACKGROUND
Northeastern Ontario Clinical Services Review FINAL PROJECT REPORT Hay Group Health Care Consulting March, 2014 2014 Hay Group Limited. All rights reserved Contents 1.0 EXECUTIVE SUMMARY... 1 1.1 BACKGROUND
Trenton Memorial Hospital. Presentation to
 Our TMH Resource Committee Trenton Memorial Hospital Facts and Figures Presentation to Quinte West Council 12 August 2015 1 Overview OurTMH Resource Committee projects: Provincial Organization of Health
Our TMH Resource Committee Trenton Memorial Hospital Facts and Figures Presentation to Quinte West Council 12 August 2015 1 Overview OurTMH Resource Committee projects: Provincial Organization of Health
Hospital Service Accountability Agreements
 2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Health System Funding Reform New Directions
 Health System Funding Reform New Directions Melissa Farrell, Assistant Deputy Minister, Health System Quality and Funding Division, MOHLTC Fredrika Scarth, Director, HQO Liaison and Program Development
Health System Funding Reform New Directions Melissa Farrell, Assistant Deputy Minister, Health System Quality and Funding Division, MOHLTC Fredrika Scarth, Director, HQO Liaison and Program Development
What does the Patients First Act mean for Rural Communities?
 What does the Patients First Act mean for Rural Communities? Michael Barrett, CEO South West Local Health Integration Network (LHIN) ROMA Conference January 30, 017 Overview of Today s Presentation 1.
What does the Patients First Act mean for Rural Communities? Michael Barrett, CEO South West Local Health Integration Network (LHIN) ROMA Conference January 30, 017 Overview of Today s Presentation 1.
Do-not-Resuscitate/Do-not- Hospitalize Orders in Nursing Homes: Are they being done and do they make a Difference?
 Do-not-Resuscitate/Do-not- Hospitalize Orders in Nursing Homes: Are they being done and do they make a Difference? Peter Tanuseputro MHSc (CH&E), MD, CCFP, FRCPC (PHPM) Mathieu Chalifoux MSc Acknowledgements
Do-not-Resuscitate/Do-not- Hospitalize Orders in Nursing Homes: Are they being done and do they make a Difference? Peter Tanuseputro MHSc (CH&E), MD, CCFP, FRCPC (PHPM) Mathieu Chalifoux MSc Acknowledgements
Health-Based Allocation Model (HBAM) Overview
 Overview") HBAM Overview Presentation Low Health-Based Allocation Model (HBAM) Overview June 29, 2010 Ontario Ministry IPM/HSIMI of Health and Long-Term Care Health System Information Management and Investment Division
HBAM Overview Presentation Low Health-Based Allocation Model (HBAM) Overview June 29, 2010 Ontario Ministry IPM/HSIMI of Health and Long-Term Care Health System Information Management and Investment Division
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017
 is made as of the 1 st day of July, 2017") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND University of Ottawa
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND University of Ottawa
March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan
 BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
Executive Compensation Policy and Framework BLUEWATER HEALTH
 Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Benchmarking variation in coding across hospitals in Canada: A data surveillance approach
 Benchmarking variation in coding across hospitals in Canada: A data surveillance approach Lori Kirby Canadian Institute for Health Information October 11, 2017 lkirby@cihi.ca cihi.ca @cihi_icis Outline
Benchmarking variation in coding across hospitals in Canada: A data surveillance approach Lori Kirby Canadian Institute for Health Information October 11, 2017 lkirby@cihi.ca cihi.ca @cihi_icis Outline
H-SAA AMENDING AGREEMENT B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND
 AND") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
LHIN Regional Summaries 2016
 College of Nurses of Ontario LHIN Regional Summaries 2016 Mississauga Halton VISION Leading in regulatory excellence MISSION Regulating nursing in the public interest LHIN Regional Summary 2016 Mississauga
College of Nurses of Ontario LHIN Regional Summaries 2016 Mississauga Halton VISION Leading in regulatory excellence MISSION Regulating nursing in the public interest LHIN Regional Summary 2016 Mississauga
PCFHC STRATEGIC PLAN
 PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
Integrated Health Services Plan
 Integrated Health Services Plan 3 2013-2016 02 IHSP 3 Central West LHIN Contents i ii iii Contents Executive Summary Strategic Directions 1 Section A: Today s Health Care Environment 1 Why LHINs? 2 Planning
Integrated Health Services Plan 3 2013-2016 02 IHSP 3 Central West LHIN Contents i ii iii Contents Executive Summary Strategic Directions 1 Section A: Today s Health Care Environment 1 Why LHINs? 2 Planning
Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association
 Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association April 2014 Ministry of Health and Long-Term Care V2.4 (2014-04-28) Session Objectives
Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association April 2014 Ministry of Health and Long-Term Care V2.4 (2014-04-28) Session Objectives
Neighbourhood HEALTH PROFILE A PEEL HEALTH STATUS REPORT. M. Prentice, Mississauga Ward 3 Councillor
 Neighbourhood HEALTH PROFILE 2005 A PEEL HEALTH STATUS REPORT MISSISSAUGA WARD 3 M. Prentice, Mississauga Ward 3 Councillor Mississauga, Ward 3 This report provides an overview of the health status of
Neighbourhood HEALTH PROFILE 2005 A PEEL HEALTH STATUS REPORT MISSISSAUGA WARD 3 M. Prentice, Mississauga Ward 3 Councillor Mississauga, Ward 3 This report provides an overview of the health status of
ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION
 ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION March 2007 Prepared by: Laura Passalent Emily Borsy
ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION March 2007 Prepared by: Laura Passalent Emily Borsy
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 2016
 is made as of the 1 st day of October, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
2006 Strategy Evaluation
 Continuing Care 2006 Strategy Evaluation Executive Summary June 2015 Introduction In May 2006, the Department of Health and Wellness (DHW) released the Continuing Care Strategy entitled Shaping the Future
Continuing Care 2006 Strategy Evaluation Executive Summary June 2015 Introduction In May 2006, the Department of Health and Wellness (DHW) released the Continuing Care Strategy entitled Shaping the Future
LHIN Regional Summaries 2016
 College of Nurses of Ontario LHIN Regional Summaries 2016 Central West VISION Leading in regulatory excellence MISSION Regulating nursing in the public interest LHIN Regional Summary 2016 Central West
College of Nurses of Ontario LHIN Regional Summaries 2016 Central West VISION Leading in regulatory excellence MISSION Regulating nursing in the public interest LHIN Regional Summary 2016 Central West
Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All
 Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
 AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2010 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) - and - MUSKOKA ALGONQUIN
AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2010 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) - and - MUSKOKA ALGONQUIN
MINISTRY OF HEALTH AND LONG-TERM CARE
 THE ESTIMATES, 1 The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life for all Ontarians.
THE ESTIMATES, 1 The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life for all Ontarians.
H-SAA AMENDING AGREEMENT
 H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
Dr. JoAnn Harrold, Site Chief, Neonatology, Children s Hospital of Eastern Ontario Charlotte Etue, Clinical Nurse Specialist Childbirth/NICU, Grand
 Dr. JoAnn Harrold, Site Chief, Neonatology, Children s Hospital of Eastern Ontario Charlotte Etue, Clinical Nurse Specialist Childbirth/NICU, Grand River Hospital 1 1) Goals of Quality-Based Procedures
Dr. JoAnn Harrold, Site Chief, Neonatology, Children s Hospital of Eastern Ontario Charlotte Etue, Clinical Nurse Specialist Childbirth/NICU, Grand River Hospital 1 1) Goals of Quality-Based Procedures
Bundled Payment Primer
 Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
Potentially Avoidable Hospitalizations in Tennessee, Final Report. May 2006
 The Methodist LeBonheur Center for Healthcare Economics 312 Fogelman College of Business & Economics Memphis, Tennessee 38152-3120 Office: 901.678.3565 Fax: 901.678.2865 Potentially Avoidable Hospitalizations
The Methodist LeBonheur Center for Healthcare Economics 312 Fogelman College of Business & Economics Memphis, Tennessee 38152-3120 Office: 901.678.3565 Fax: 901.678.2865 Potentially Avoidable Hospitalizations
Health Links: Meeting the needs of Ontario s high needs users. Presentation to the Canadian Institute for Health Information January 27, 2016
 Health Links: Meeting the needs of Ontario s high needs users Presentation to the Canadian Institute for Health Information January 27, 2016 Agenda Items Health Links: Overview and successes to date Critical
Health Links: Meeting the needs of Ontario s high needs users Presentation to the Canadian Institute for Health Information January 27, 2016 Agenda Items Health Links: Overview and successes to date Critical
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016
 is made as of the 1 st day of April, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Pembroke Regional Hospital
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Pembroke Regional Hospital
Retrospective Bundles
 Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Telemedicine in Central East LHIN
 Telemedicine in Central East LHIN Status Report May 28, 2014 Jeanne Thomas, Lead System Design Shelley Morris, Regional Coordinator, OTN What is OTN Telemedicine? OTN is one of the largest Telemedicine
Telemedicine in Central East LHIN Status Report May 28, 2014 Jeanne Thomas, Lead System Design Shelley Morris, Regional Coordinator, OTN What is OTN Telemedicine? OTN is one of the largest Telemedicine
Revisiting the inpatient rehabilitation case-mix and funding model in Ontario, Canada: lessons learned
 Revisiting the inpatient rehabilitation case-mix and funding model in Ontario, Canada: lessons learned Kristen Pitzul, Emitis Moshirzadeh, Jan Walker, Kevin Yu, Sandro Serino, Imtiaz Daniel Quick Facts
Revisiting the inpatient rehabilitation case-mix and funding model in Ontario, Canada: lessons learned Kristen Pitzul, Emitis Moshirzadeh, Jan Walker, Kevin Yu, Sandro Serino, Imtiaz Daniel Quick Facts
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators. November 29, 2013
 and Small Dot (Sector Specific) Indicators. November 29, 2013") TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
The Regional Cardiac Care Program at Southlake
 The Regional Cardiac Care Program at Southlake The Future Vision of Regional Cardiac Services Serving the Populations of York, Simcoe, Muskoka, and Dufferin Regions Copyright 2009. Southlake Regional Health
The Regional Cardiac Care Program at Southlake The Future Vision of Regional Cardiac Services Serving the Populations of York, Simcoe, Muskoka, and Dufferin Regions Copyright 2009. Southlake Regional Health
Infrastructure of Rural Vitality:
 Infrastructure of Rural Vitality: The Future of Rural Health Services Jim Whaley Rural Vitality Conference (May 23, 2008) Presentation Overview Rural Health Reality Hard Infrastructure: E-health Soft Infrastructure:
Infrastructure of Rural Vitality: The Future of Rural Health Services Jim Whaley Rural Vitality Conference (May 23, 2008) Presentation Overview Rural Health Reality Hard Infrastructure: E-health Soft Infrastructure:
Home care clients with complex needs who received personal support service within five days
 Home care clients with complex needs who received personal support service within five days Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator
Home care clients with complex needs who received personal support service within five days Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017
 is made as of the 1 st day of April, 2017") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Deep River and District
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Deep River and District
GREATER VICTORIA Local Health Area Profile 2015
 GREATER VICTORIA Local Health Area Profile 215 Greater Victoria LHA is one of 14 LHAs in Island Health and is located in Island Health s South Island Health Service Delivery Area (HSDA). The LHA is at
GREATER VICTORIA Local Health Area Profile 215 Greater Victoria LHA is one of 14 LHAs in Island Health and is located in Island Health s South Island Health Service Delivery Area (HSDA). The LHA is at
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
Chronic Obstructive Pulmonary Disease in Ontario
 Chronic Obstructive Pulmonary Disease in Ontario 1996/97 to 2014/15 October 2017 ii Chronic Obstructive Pulmonary Disease in Ontario, 1996/97 to 2014/15 Authors Andrea S. Gershon Graham Mecredy Sujitha
Chronic Obstructive Pulmonary Disease in Ontario 1996/97 to 2014/15 October 2017 ii Chronic Obstructive Pulmonary Disease in Ontario, 1996/97 to 2014/15 Authors Andrea S. Gershon Graham Mecredy Sujitha
Deaths by care setting
 Deaths by care setting Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator description RIS indicator name Deaths by care setting Other names
Deaths by care setting Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator description RIS indicator name Deaths by care setting Other names
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost
 Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Toronto Central LHIN 2016/2017 QIP Snapshot Report. Health Quality Ontario The provincial advisor on the quality of health care in Ontario
 Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
The Movement Towards Integrated Funding Models
 The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
The Re-ACT Program. Remote Access to Care Technology
 w w w.w E C A R E. C A The Re-ACT Program Remote Access to Care Technology January 2011 Introduction Almost 80% of Canadian adults over the age of 65 have some form of chronic disease. Treating and caring
w w w.w E C A R E. C A The Re-ACT Program Remote Access to Care Technology January 2011 Introduction Almost 80% of Canadian adults over the age of 65 have some form of chronic disease. Treating and caring
Appendix H. Community Profile. Hamilton Niagara Haldimand Brant Local Health Integration Network
 Appendix H Community Profile Hamilton Niagara Haldimand Brant Local Health Integration Network August 2006 ISBN 1-4249-2806-0 Table of Contents Executive Summary... 1 Characteristics of the Population
Appendix H Community Profile Hamilton Niagara Haldimand Brant Local Health Integration Network August 2006 ISBN 1-4249-2806-0 Table of Contents Executive Summary... 1 Characteristics of the Population
New York Metro Chapter
 New York Metro Chapter Business Intelligence & Predictive Analytics in the Healthcare Environment Paul Savage; Director Center for Health Analytics Iona College, Hagan School of Business, Healthcare Management
New York Metro Chapter Business Intelligence & Predictive Analytics in the Healthcare Environment Paul Savage; Director Center for Health Analytics Iona College, Hagan School of Business, Healthcare Management
RECOMMENDATION STATUS OVERVIEW
 Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Rehabilitative Care Alliance Capacity Planning and System Evaluation Task Group Capacity Planning Framework March 2015
 The Capacity Planning and System Evaluation (CP&SE) Initiative was established in October 2014 as one of four priority initiatives within the Rehabilitative Care Alliance s first mandate (April 2013-).
The Capacity Planning and System Evaluation (CP&SE) Initiative was established in October 2014 as one of four priority initiatives within the Rehabilitative Care Alliance s first mandate (April 2013-).
Report on Provincial Wait Time Strategy
 Hôpital régional de Sudbury Regional Hospital Report on Provincial Wait Time Strategy May 2007 Provincial Wait-time Strategy Announced by Minister of Health in November 2004 Focus is to increase access
Hôpital régional de Sudbury Regional Hospital Report on Provincial Wait Time Strategy May 2007 Provincial Wait-time Strategy Announced by Minister of Health in November 2004 Focus is to increase access
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017
 South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Factors that Impact Readmission for Medicare and Medicaid HMO Inpatients
 The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
COURTENAY Local Health Area Profile 2015
 COURTENAY Local Health Area Profile 215 Courtenay Local Health Area (LHA) is one of 14 LHAs in Island Health and is located in Island Health s North Island Health Service Delivery Area (HSDA). Courtenay
COURTENAY Local Health Area Profile 215 Courtenay Local Health Area (LHA) is one of 14 LHAs in Island Health and is located in Island Health s North Island Health Service Delivery Area (HSDA). Courtenay
Preoperative Consultations: OHTAC Recommendation
 Preoperative Consultations: OHTAC Recommendation Ontario Health Technology Advisory Committee March 2014 Preoperative Consultations: OHTAC Recommendation. March 2014; pp. 1 11 Suggested Citation This report
Preoperative Consultations: OHTAC Recommendation Ontario Health Technology Advisory Committee March 2014 Preoperative Consultations: OHTAC Recommendation. March 2014; pp. 1 11 Suggested Citation This report
2017/18 PERSONAL SUPPORT WORKER (PSW) TRAINING FUND FOR HOME AND COMMUNITY CARE PROGRAM DESCRIPTION
 TRAINING FUND FOR HOME AND COMMUNITY CARE PROGRAM DESCRIPTION") 2017/18 PERSONAL SUPPORT WORKER (PSW) TRAINING FUND FOR HOME AND COMMUNITY CARE PROGRAM DESCRIPTION 1 Table of Contents 1. Introduction and Background... 3 a) Introduction b) Eligible Organizations c)
2017/18 PERSONAL SUPPORT WORKER (PSW) TRAINING FUND FOR HOME AND COMMUNITY CARE PROGRAM DESCRIPTION 1 Table of Contents 1. Introduction and Background... 3 a) Introduction b) Eligible Organizations c)
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE
 IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE GTA Rehab Network Charissa Levy, Sharon Ocampo-Chan, Donna Renzetti October 2016
IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE GTA Rehab Network Charissa Levy, Sharon Ocampo-Chan, Donna Renzetti October 2016
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Nursing Practice In Rural and Remote Ontario: An Analysis of CIHI s Nursing Database
 Nursing Practice In Rural and Remote Ontario: An Analysis of CIHI s Nursing Database www.ruralnursing.unbc.ca Highlights In the period between 2003 and 2010, the regulated nursing workforce in Ontario
Nursing Practice In Rural and Remote Ontario: An Analysis of CIHI s Nursing Database www.ruralnursing.unbc.ca Highlights In the period between 2003 and 2010, the regulated nursing workforce in Ontario
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard /10 Q3
 MLAA Performance Assessment Dashboard /10 Q3") MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ
 Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
How BC s Health System Matrix Project Met the Challenges of Health Data
 Big Data: Privacy, Governance and Data Linkage in Health Information How BC s Health System Matrix Project Met the Challenges of Health Data Martha Burd, Health System Planning and Innovation Division
Big Data: Privacy, Governance and Data Linkage in Health Information How BC s Health System Matrix Project Met the Challenges of Health Data Martha Burd, Health System Planning and Innovation Division
Hospital Report. A joint initiative of the Ontario Hospital Association and the Government of Ontario
 Hospital Report A C U T E C A R E A joint initiative of the Ontario Hospital Association and the Government of Ontario CONTENTS PAGE This report is brought to you by the Government of Ontario in partnership
Hospital Report A C U T E C A R E A joint initiative of the Ontario Hospital Association and the Government of Ontario CONTENTS PAGE This report is brought to you by the Government of Ontario in partnership
Partnerships: Developing an Elective Joint Replacement Program
 Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL
 Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL Front Page for Ministry Submission: Organization (Full Name): Last Name: Job Title: Address:
Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL Front Page for Ministry Submission: Organization (Full Name): Last Name: Job Title: Address:
Health and Wellness. Business Plan to restated. Accountability Statement
 Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
Hamilton Niagara Haldimand Brant LHIN. Appendix XII: Strategic Health System Plan: Current State Synopsis
 Hamilton Niagara Haldimand Brant LHIN Appendix XII: Strategic Health System Plan: Current State Synopsis Table of Contents Introduction... 4 Environmental Scan Summary... 5 Provider Survey Summary...
Hamilton Niagara Haldimand Brant LHIN Appendix XII: Strategic Health System Plan: Current State Synopsis Table of Contents Introduction... 4 Environmental Scan Summary... 5 Provider Survey Summary...
1/14/2013. Emerging Healthcare Issues: How Will They Impact Hospital Reimbursement? EMERGING HEALTHCARE TOPICS FOR DISCUSSION
 2013 University of California Compliance & Audit Symposium Lori Laubach, Partner Sharon Hartzel, Director Health Care Consulting Moss Adams LLP Emerging Healthcare Issues: How Will They Impact Hospital
2013 University of California Compliance & Audit Symposium Lori Laubach, Partner Sharon Hartzel, Director Health Care Consulting Moss Adams LLP Emerging Healthcare Issues: How Will They Impact Hospital
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM
 Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers