Fylde & Wyre CCG New Interim Care Home Service. Amanda Lomas F&W CCG Commissioner
|
|
|
- Rodney Arnold
- 5 years ago
- Views:
Transcription


1 Fylde & Wyre CCG New Interim Care Home Service Amanda Lomas F&W CCG Commissioner

2 Care Homes Model Overview Background Four new care home models piloted on the Fylde coast. One in BCCG area, three in Fylde and Wyre. In summary, these models all centre on improving the triage and assessment of patients, increasing home staff s access to advice/support from healthcare professionals and medical optimisation.




3 Care Home Service 3
4 Introduction Aim of the presentation Alison Ricchiuti- Operation Manager Michelle Dicks- Deputy Manager, Alexandra Nursing Home
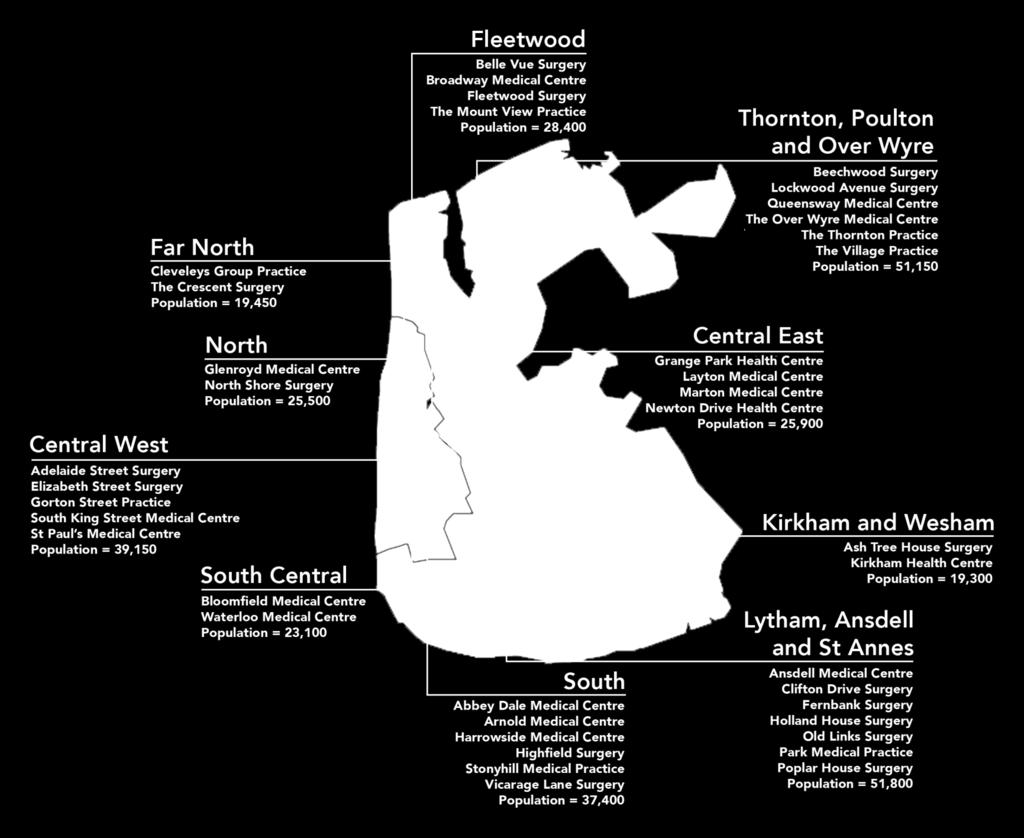
5 Background Wyre Integrated Neighbourhood (WIN) 6 practices, Thornton, Poulton, Over Wyre All practices wanted to develop services for care home patient with ambitions of extending this service out to household patients and recognised an underserviced population 25 homes, Cohort of 415 residents Primary Care not set up to service Chronic Disease Management in residential care Currently reactive service
6 Why? Ageing population, increasing burden of illness Dementia 1 in 5 >80 yrs, set to double in next 30 years. Complex health and social care needs and fragmented services. Residential Home 24 months avg. life expectancy High rates of unplanned admissions distressing & costly
7 Aims Improve health care for residents. Improve patient experience & Quality of life. Improve communication. Improve medicines management. Patient centred anticipatory care. Building on collaborative working with care homes. Identify learning needs and skills gaps for teaching and training. Reduce hospital inappropriate admissions.
8 Neighbourhood engagement 2014/15 - Two very successful formal engagement events involving care home managers, practices and CCG and wider stakeholders ( mental health, social services Age UK Dementia UK, Trinity etc.)prior to service going live Informal feedback Formal Questionnaires
9 Stakeholders Care Home Staff WIN Team Practices Mental Heath Third Sector Patient OOH Services Social Services Family Community Services
10 Feedback following engagement Sharing of information. A greater understanding of the barriers to effective communications for optimum care between practices and care homes. Communication across the board identified inconsistences between practices e.g Medications. Discharge information. Local champions from care homes that took part in the original pre 2014 pilot to promote uptake across all the care homes.




11 Meet the team
12 WIN care home team Service commenced in December 2015 Initially challenges with recruitment and staffing capacity Initial "hump" of workload in 1st round of assessments and care planning Initial assessment, 3 mthly review now 6 monthly Individual holistic care Co-ordination plans New residents within 14 days Within 72 hrs of hospital discharge Chronic Disease Management Medication review Advance care planning /end of life Care home staff training NOT an acute service

13 New resident visit Harry is scheduled for a visit in 6 months time to review his health plan Home inform of Harry s admission to the care home. Care home Team visit Speak with Harry Care staff and Family Care Coordination plan shared with GP and FCMS Assess holistically Chronic disease 6- CIT review, check MaRR against GP records.encourage discussion around advanced care planning. Care co-ordination plan produced given to home and asked to call appropriated numbers, EpaCCs recorded Pharmacist review sometimes face to face

14 Admission to hospital Lessons learned Harry admitted Service makes contact with the Hospital & works with the home to reduce LOS Admission discussed at MDT with clinical lead to identify if considered avoidable or not. Outcome shared with home Action plan completed and Care Coordination plan reviewed and shared with GP and FCMS Pharmacist will review medications checked Assessment and discussion with the resident, home and family as to why the resident went in and RCA form filled in. Marr Comparison made. Team contact the home following day of discharge and visit within 72 hours
15 GSF ward rounds Care home team will update FCMS and GP Care home team call Care Home to arrange a monthly meeting Care staff and link care home team nurse go through all the residents in the home Actions identified discussed jointly for resident who have moved along the coding scale including med review Discuss DNARCPR protocols and Just In case Advanced care planning discussion will be confirmed including if the resident has a shared EpACCs Each resident will be discussed as to where they sit on the GSF prognosis scale
16 GSF ward rounds Lead nurse identified for each home Each resident s discussed monthly in a virtual ward round Just in case drugs DNACPR protocol Named link in each practice and information shared across Common and consistent processes and clinical coding across all practices. Medication reviews Involvement in practice palliative care meetings Involvement of Trinity and EOL care home group


17 Pharmacist interventions Medication reviews Visit home, review MARs, carers concerns, suitable patients to review with them. Look at indication, suitability, dosage, formulation, usage, risk scores of prescribed medications. Best practice prescribing, following local and national guidance. Advise GPs on suggestions, implement with agreement and notify homes. 72hr discharge and new patient reviews. Dealing with specific queries that come in from homes that may otherwise be directed to GP. Support & advice for team. Neighbourhood given pharmacist authority to make cost effective changes to certain medications where appropriate.
18 Two years on 91% Med reviews completed (March 17) Admissions reduction of 74% 100% 100% PPC/ PPD and DNARCPR discussed New residents seen within two weeks Care plans completed = = 161 Total cost savings 280,901 Of which 68,818 medication savings Length of stay reduction by 1,118 days (2,916 days) (1,798 days)

19 Two years on Care Home feedback Primrose Bank would like to thank care home team for all their hard work and support. Gave us a bunch of flowers. Just wanted to take some time out to thank you and the WIN team on behalf of Pilling Nursing home for all your help and support during our ongoing development since opening. Worth their weight in gold Alexandra Nursing Home. Family feedback Thank you for getting my Mum home sooner post discharge and checking everything has been OK. You ve been a great support. Thank you for your kindness and support in helping us make Mum s last few days comfortable and in the right place. You went above and beyond to ensure, Mum got the best care and for that we ll be forever grateful.
20 Initial reflection on the new service Alexandra Nursing Home: Initial Barriers Staff trust nervous about who the team were and constructive comments not taken easily Vision unclear not communicated Short term increased work load care plan writing and collection of resident information weights ect. My own previous experience of care plans and no explanations given How did you overcome them? Reflection and recognition of lack of services out there to support Vision became clear Building relationships Easy access to other MDT Quicker and smoother response Able to bounce ideas of each other having a mutual respect Preventing unnecessary admissions and placement breakdown
21 Case study Chris 81years old. History of Frailty, dementia, stroke and diabetes. Chris had been very independent up until 2011 when he suffered memory loss. Diagnosed in 2011 with Dementia. Family struggling to cope Admitted to Rest home section of the Nursing Home following an admission from a fall and fracture Wandered frequently and high risk of falls. Home and wife would always be feeding him finger foods. WIN Team when visiting would witness him singing Let it go Disney classic from Frozen and that he would often dance. He would sometimes be mischievous and creep up behind you whilst having conversations with others but was like a gentle giant.
22 Case study Home WIN 5/2016 Home Informed WIN new resident 5/2016 Chris seen on initial chronic disease review and care plan completed. Discussed need for advanced care planning with home and offer of support 7/2016 Home discussed with family and requested DNARCPR along with PPC/ PPD 4/2017 GSF ward round +continued care 5/2017 GSF Ward round + continued care 7/2016 Care plan updated following Advanced care planning 11/2016 Joanna pharmacist med review 5/2017 Chronic disease review and advise around fortification 5/2017 Fall in home and admission 5/2017 Visit by WIN Identification of drug changes when comparing MaR against discharge letter Referral made to falls team and Dietician. Green months years prognosis EPaCCS notified 6/2017 GSF ward round and continue monthly 9/17 Fall in home and admission 9/17 Care home identify EOL weeks (Yellow) and inform WIN and GP 10/17 Care home confident in looking after Chris in EOL 9/10/17 Chris died peacefully in the home 6/2017 Med review following admission. Updated EMIS records of changes 9/17 Visit by WIN discussion around deterioration EOL and falls to highlight with safeguard team Care plan completed 9/17 WIN update EPaCCS and change care plan. Request 4 core meds 10/17 Continue to support home with EOL 10/10 WIN and surgery informed
23 Lessons learned 1. Inconsistencies surrounding completion of DNRCPR s 2. RCA s MDT 3. Understanding of common themes in admissions i.e falls 4. Managing family expectations - important to involve family 5. Safeguarding can increase LOS 6. Sometimes gaps in key skills and competences ( such as wound and EoLC) in nursing homes 7. Acute hospitals understanding of frail patients once admitted 8. Advanced care planning and using consistent sharing processes. 9. What can be achieved through a shared vision and desire to collaborate for a common goal.
24 Success Provides a conduit to support better communication Shared Vision Neighbourhood and care home relationships and trust. Increased EOL recognition Quality of care for residents and families Team professional satisfaction and neighbourhood pride in achievement Further possibilities in streamlining neighbourhood protocols to improve quality and flow Chronic disease protocols Wound care protocols for ordering Shared protocols in covert medications Common homely remedies agreement




25 Success A future service across the Fylde and Wyre based on national evidence and local success.

26 Thank you!
 Nurse Practitioners Health Care Assistants Pharmacist GP Neighbourhood Support Integrated Falls Service Enhanced Primary Care (EPC) Future Integrated Neighbourhood Team District Nursing")
27 Fylde & Wyre CCG Interim Care Home Service 2 Interim Care Home Teams between 1 st November st March 2019 Fylde - (Kirkham & Wesham and Lytham Neighbourhood) Interim Workforce ( Nov 2017 Mar 2019) Nurse Practitioners Health Care Assistants Pharmacist GP Neighbourhood Support Integrated Falls Service Enhanced Primary Care (EPC) Future Integrated Neighbourhood Team District Nursing Community Matron Therapy Services Mental Health Services Social Services Extensivist Service (ECS) Wyre (Fleetwood and WIN)




28 Future Vision Integrated Neighbourhoods Patients and professionals refer into a neighbourhood hub including care homes. Triage Assess Signpost Community consultants Patient activation Care coordination Primary care Therapy Community nursing Mental health Social care Diagnostics and specialist acute care Wellbeing support 1 Improved outcomes and experiences of care for patients 2 Better utilisation of the local health and care workforce 3 Improved utilisation and sustainability of local services
29

30 Interventions include: Medication reviews and optimisation Care planning Advanced care planning GSF Nurse Ward Rounds Dementia screening Post discharge review within 72 hours Urgent clinical triage via telehealth MDT









31 Virtual Care Homes MDT GP Neighbourhood Support Pharmacist Nurse Practitioners Integrated Neighbourhood Team Health Care Assistants Community Matron MDT Social services Integrated Falls Service Therapy Services Mental Health Services District Nursing In-Reach Geriatrician

32 Technology Utilisation 2017/18 secured funding via vanguard programme to provide telecare in all care homes across the Fylde Coast. The IT project teams have worked alongside the Care Home team to roll this out and provide support. Care Homes will link to: Fylde & Wyre Care Home Teams Out of hours services (Care Coordination) Primary Care ongoing roll-out during Working with other Community Services (Dietetics and SaLT).
 Initial surveys completed: 100% (52/52) Broadband commissioned: 79% (41/52) Wi-Fi commissioning complete: 62% (32/52) ipads deployed and training complete: 48%")
33 Care Home Connect Update 100% engagement with 69 care homes in Fylde & Wyre CCG. Care Homes refused service: 25% (17/69) Initial surveys completed: 100% (52/52) Broadband commissioned: 79% (41/52) Wi-Fi commissioning complete: 62% (32/52) ipads deployed and training complete: 48% (25/52) The process is to: Engage Visit and explain the project further Survey any existing network Complete installations Issue ipad and training Sign and return MoU

34 Directory of Services Now launched across the Fylde coast: Provides a comprehensive resource for patients and professionals to access health, social and third/voluntary sector service information. Fylde coast care homes listed on the site enabling families to review. Please take a look at your own listings you can manage these yourself!
Transforming End of Life Care at Blackpool Teaching Hospitals
 Transforming End of Life Care at Blackpool Teaching Hospitals Dr Harriet Preston Palliative Medicine Consultant & Clinical lead for End of Life Care Blackpool Teaching Hospitals NHS Foundation Trust Palliative
Transforming End of Life Care at Blackpool Teaching Hospitals Dr Harriet Preston Palliative Medicine Consultant & Clinical lead for End of Life Care Blackpool Teaching Hospitals NHS Foundation Trust Palliative
Nurse Led End of Life Care. Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough
 Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
PRIMARY CARE COMMISSIONING COMMITTEE MEETING
 PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
The Symphony Programme an example from the UK of integrated working between primary and secondary care. Jeremy Martin, Symphony Programme Director
 The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
End of Life Care Commissioning Strategy. NHS North Lincolnshire - Adding Life to Years and Years to Life
 End of Life Care Commissioning Strategy NHS North Lincolnshire - Adding Life to Years and Years to Life END OF LIFE CARE 1. Background NHS North Lincolnshire End of Life Care Commissioning Strategy The
End of Life Care Commissioning Strategy NHS North Lincolnshire - Adding Life to Years and Years to Life END OF LIFE CARE 1. Background NHS North Lincolnshire End of Life Care Commissioning Strategy The
West Kent CCG Emergency Health Care Plan
 West Kent CCG Emergency Health Care Plan 20 October 2015 Bruno Capone Local situation 11486 Elderly 85+ 3800 Care home residents in West Kent area Average life expectancy of nursing home residents is 6-9
West Kent CCG Emergency Health Care Plan 20 October 2015 Bruno Capone Local situation 11486 Elderly 85+ 3800 Care home residents in West Kent area Average life expectancy of nursing home residents is 6-9
Integrated Care in North Central London
 Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018
 A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018 ENCLOSURE 7 PROPOSAL FOR ENHANCED MEDICAL SUPPORT TO BROMLEY CARE HOMES SUMMARY: Bromley CCG gained agreement at the CCG Clinical
A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018 ENCLOSURE 7 PROPOSAL FOR ENHANCED MEDICAL SUPPORT TO BROMLEY CARE HOMES SUMMARY: Bromley CCG gained agreement at the CCG Clinical
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy
 Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Building Partnerships and Reducing Demand through Telemedicine
 Building Partnerships and Reducing Demand through Telemedicine Alex Blake TANP Digital Care Airedale NHS Foundation Trust Telemedicine Right care, right place, right time What is telemedicine? How does
Building Partnerships and Reducing Demand through Telemedicine Alex Blake TANP Digital Care Airedale NHS Foundation Trust Telemedicine Right care, right place, right time What is telemedicine? How does
EPaCCS in Greater Manchester
 EPaCCS in Greater Manchester Developments of integrated End-of-life Care Services/EPaCCS Over the past 8 years the NHS has proactively supported developments in integrated care services across service
EPaCCS in Greater Manchester Developments of integrated End-of-life Care Services/EPaCCS Over the past 8 years the NHS has proactively supported developments in integrated care services across service
Mid Powys Cluster Plan
 Mid Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
Mid Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
Integrated Care theme / Long Term Conditions priority
 Integrated Care theme / Long Term Conditions priority Professor Ruth Chambers OBE Clinical lead for LTC priority/clinical lead for Flo telehealth exemplar of Integrated Care WMAHSN Integrated Care & other
Integrated Care theme / Long Term Conditions priority Professor Ruth Chambers OBE Clinical lead for LTC priority/clinical lead for Flo telehealth exemplar of Integrated Care WMAHSN Integrated Care & other
SYMPHONY. The Symphony Programme. 7 June Person-Centred, Co-ordinated Care
 SYMPHONY Person-Centred, Co-ordinated The Symphony Programme 7 June 2016 Programme Structure: Overview Advisory Group Symphony Programme Board PMO Cross- Model Forum Identify themes and quick wins across
SYMPHONY Person-Centred, Co-ordinated The Symphony Programme 7 June 2016 Programme Structure: Overview Advisory Group Symphony Programme Board PMO Cross- Model Forum Identify themes and quick wins across
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes. Camden Clinical Commissioning Group. Care Home LES Spec v1
 Local Enhanced Service Clinical Lead Commissioner Reporting Mechanism/Frequency Payment Frequency Payment Contact This Version GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes Dr
Local Enhanced Service Clinical Lead Commissioner Reporting Mechanism/Frequency Payment Frequency Payment Contact This Version GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes Dr
LOCALITY SUMMARIES: September 2017
 LOCALITY SUMMARIES: September 2017 Appendix B LOCALITY: BURNLEY KEY AREAS OF DISCUSSION & ACTIONS: Burnley Community Health and Wellbeing Partnership Development Burnley Learning Partnership Small Grants
LOCALITY SUMMARIES: September 2017 Appendix B LOCALITY: BURNLEY KEY AREAS OF DISCUSSION & ACTIONS: Burnley Community Health and Wellbeing Partnership Development Burnley Learning Partnership Small Grants
Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan Improving Through Change
 Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan 2015-2018 Improving Through Change Trust Board 22 nd October 2015 1 Contents Section 1: Why have we produced
Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan 2015-2018 Improving Through Change Trust Board 22 nd October 2015 1 Contents Section 1: Why have we produced
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
A collaborative approach to Specialist Palliative Care and the difference this is making in Dudley
 A collaborative approach to Specialist Palliative Care and the difference this is making in Dudley Dr Joanne Bowen, Dudley Foundation Trust Nicole Woodyatt, Macmillan Cancer Support The Midhurst Macmillan
A collaborative approach to Specialist Palliative Care and the difference this is making in Dudley Dr Joanne Bowen, Dudley Foundation Trust Nicole Woodyatt, Macmillan Cancer Support The Midhurst Macmillan
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Leeds West CCG Business Case for Recurrent or Non Recurrent Funding request.
 Leeds West CCG Business Case for Recurrent or Non Recurrent Funding request. Proposal Title: Proposal to commission enhanced clinical services for people in care homes Transformation Workstream: NHS Leeds
Leeds West CCG Business Case for Recurrent or Non Recurrent Funding request. Proposal Title: Proposal to commission enhanced clinical services for people in care homes Transformation Workstream: NHS Leeds
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
SALFORD TOGETHER TRANSFORMING HEALTH AND SOCIAL CARE
 SALFORD TOGETHER TRANSFORMING HEALTH AND SOCIAL CARE Our Challenges Our Aims Improved Health and Social Care outcomes for people Improved experience of health and social care Making better use of limited
SALFORD TOGETHER TRANSFORMING HEALTH AND SOCIAL CARE Our Challenges Our Aims Improved Health and Social Care outcomes for people Improved experience of health and social care Making better use of limited
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Transforming musculoskeletal and orthopaedic elective care services
 Transforming musculoskeletal and orthopaedic elective care services Case studies About these Further Equality and health inequalities Promoting equality and addressing health inequalities are at the heart
Transforming musculoskeletal and orthopaedic elective care services Case studies About these Further Equality and health inequalities Promoting equality and addressing health inequalities are at the heart
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
One Chance to Get it Right:
 One Chance to Get it Right: Implementing the new priorities of Care for the Dying Person Dr Susan Salt, Medical Director Trinity Hospice, Blackpool Outline of the talk Brief look at what led to this point..
One Chance to Get it Right: Implementing the new priorities of Care for the Dying Person Dr Susan Salt, Medical Director Trinity Hospice, Blackpool Outline of the talk Brief look at what led to this point..
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Gold Standards Framework in Care Homes Programme
 Gold Standards Framework in Care Homes Programme Re Accreditation Round 11 (016) Quality Hallmark Award Final Report Care Home Details Name of Home & Coordinator St Dominics Care Home Registration Number
Gold Standards Framework in Care Homes Programme Re Accreditation Round 11 (016) Quality Hallmark Award Final Report Care Home Details Name of Home & Coordinator St Dominics Care Home Registration Number
The Suffolk Marie Curie Delivering Choice Programme
 The Suffolk Marie Curie Delivering Choice Programme Phase III A report on progress and achievements Date: April 2012 Author: Sandy Barron Project Lead Manager Design and Development - MCDCP 1 Table of
The Suffolk Marie Curie Delivering Choice Programme Phase III A report on progress and achievements Date: April 2012 Author: Sandy Barron Project Lead Manager Design and Development - MCDCP 1 Table of
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
Making Health and Care services for for an aging population- End of Life care
 Making Health and Care services for for an aging population- End of Life care Prof Keri Thomas The National GSF Centre in End of Life Care Hon Professor End of Life Care Birmingham University www.goldstandardsframework.org.uk
Making Health and Care services for for an aging population- End of Life care Prof Keri Thomas The National GSF Centre in End of Life Care Hon Professor End of Life Care Birmingham University www.goldstandardsframework.org.uk
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
Clinical Case Manager for Older Persons. Elaine Dunne
 Clinical Case Manager for Elaine Dunne According to the World Health Organisations World Report on ageing (2015) the numbers of older people worldwide are dramatically increasing. In their Global Strategy
Clinical Case Manager for Elaine Dunne According to the World Health Organisations World Report on ageing (2015) the numbers of older people worldwide are dramatically increasing. In their Global Strategy
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Frail Elderly Assessment Unit (FEAU)
") Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP).
 Centre in End of Life care on use of the Liverpool Care Pathway (LCP).") Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP). April 2013 Contents 1. Summary of submission from GSF Centre 2. About
Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP). April 2013 Contents 1. Summary of submission from GSF Centre 2. About
Champions for learning disabilities
 Champions for learning disabilities Enable Care and Home Support End of Life Project Developing training for end of life care has led to an empowered staff team and more engaged residents and people who
Champions for learning disabilities Enable Care and Home Support End of Life Project Developing training for end of life care has led to an empowered staff team and more engaged residents and people who
End of Life Care A Single Point of Access
 End of Life Care A Single Point of Access Stakeholder meeting report Oct 2014 Single Point of Access project Stakeholder meeting report V2.1 FINAL Page 1 1. Background End of life care is about caring
End of Life Care A Single Point of Access Stakeholder meeting report Oct 2014 Single Point of Access project Stakeholder meeting report V2.1 FINAL Page 1 1. Background End of life care is about caring
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
WOLVERHAMPTON CCG. Governing Body Meeting 9 th September 2014
 WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
Telehealth for Acute and Urgent Care
 Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Connected Palliative Care Partnership End of Year Report
 where everyone matters Sandwell and West Birmingham Hospitals NHS Trust Connected Palliative Care Partnership End of Year Report 2016 2017 Sandwell and West Birmingham Clinical Commissioning Group Contents
where everyone matters Sandwell and West Birmingham Hospitals NHS Trust Connected Palliative Care Partnership End of Year Report 2016 2017 Sandwell and West Birmingham Clinical Commissioning Group Contents
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
End of Life Care Review Case Review Audit
 Case Review Audit : : Version: 1 NHS Wales (Intranet) / Public Health Wales (Intranet) Purpose and summary of document: This document is for use by general practices who are engaged in providing services
Case Review Audit : : Version: 1 NHS Wales (Intranet) / Public Health Wales (Intranet) Purpose and summary of document: This document is for use by general practices who are engaged in providing services
Contents. Care Homes Admissions Avoidance Schemes. Leeds West Clinical Commissioning Group. Dec Final Version
 Contents Care Homes Admissions Avoidance Schemes Leeds West Clinical Commissioning Group Dec 2014 Page 1 of 33 Final Version Contents Con VERSION CONTROL 3 SUMMARY 4 BACKGROUND 6 EVIDENCE 8 LEEDS ENHANCED
Contents Care Homes Admissions Avoidance Schemes Leeds West Clinical Commissioning Group Dec 2014 Page 1 of 33 Final Version Contents Con VERSION CONTROL 3 SUMMARY 4 BACKGROUND 6 EVIDENCE 8 LEEDS ENHANCED
RM Partners Palliative Care Stakeholder Event
 RM Partners Palliative Care Stakeholder Event Remember to check out the London Hospices Choir The Living Years - Xmas No.1??? https://www.youtube.com/watch?v=xblgzikvm3u Thursday 15 th December 2016 Broadway
RM Partners Palliative Care Stakeholder Event Remember to check out the London Hospices Choir The Living Years - Xmas No.1??? https://www.youtube.com/watch?v=xblgzikvm3u Thursday 15 th December 2016 Broadway
practice. A Health Board education campaign? To be launched
 W95045 Tony Pandy Health Centre Practice Development Plan Services Priority The issues Aims and objectives How will this be done? ( Practice; GP Cluster; Health Board) Access DNA rates on To reduce the
W95045 Tony Pandy Health Centre Practice Development Plan Services Priority The issues Aims and objectives How will this be done? ( Practice; GP Cluster; Health Board) Access DNA rates on To reduce the
NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74
 Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Proactive Anticipatory Care (PACe) in Guildford & Waverley. Shaping healthcare for you and your family
 in Guildford & Waverley. Shaping healthcare for you and your family") Proactive Anticipatory Care (PACe) in Guildford & Waverley Introduction Sian Jones Clinical Lead End of Life Care & Cancer Guildford & Waverley CCG Sharing our learning Background Putting it into practice
Proactive Anticipatory Care (PACe) in Guildford & Waverley Introduction Sian Jones Clinical Lead End of Life Care & Cancer Guildford & Waverley CCG Sharing our learning Background Putting it into practice
Integrating Telemedicine into mental Health Care
 Integrating Telemedicine into mental Health Care learning from a Care Homes Vanguard Rachel Binks Nurse Consultant Digital & Acute Care Airedale NHS Foundation Trust Chris North Care Home Liaison Team
Integrating Telemedicine into mental Health Care learning from a Care Homes Vanguard Rachel Binks Nurse Consultant Digital & Acute Care Airedale NHS Foundation Trust Chris North Care Home Liaison Team
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY. (for use by Health and Social Care Trusts)
") REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
top Tips guide To supportive and palliative
 top Tips guide To supportive and palliative care meetings Patients value care that is high quality and co ordinated. Efficient meetings in a Primary Care setting are of great importance in ensuring that
top Tips guide To supportive and palliative care meetings Patients value care that is high quality and co ordinated. Efficient meetings in a Primary Care setting are of great importance in ensuring that
Merton Integration & Better Care Fund Plan 2017/19
 Merton Better Care Fund Programme Merton Clinical Commissioning Group Merton Integration & Better Care Fund Plan 2017/19 Area London Constituent Health and Wellbeing Boards Merton Constituent CCGs Merton
Merton Better Care Fund Programme Merton Clinical Commissioning Group Merton Integration & Better Care Fund Plan 2017/19 Area London Constituent Health and Wellbeing Boards Merton Constituent CCGs Merton
RUH End of Life Care Working Group Annual Report. April 2013 March 2014
 RUH End of Life Care Working Group Annual Report April 2013 March 2014 Agenda Item: 11 Page 1 of 11 Contents 1. Introduction page 3 2. End of Life Care Working Group page 3 3. End of Life Care Work Plan
RUH End of Life Care Working Group Annual Report April 2013 March 2014 Agenda Item: 11 Page 1 of 11 Contents 1. Introduction page 3 2. End of Life Care Working Group page 3 3. End of Life Care Work Plan
End of Life Care in the Acute Hospital Setting. Dr Adam Brown Consultant in Palliative Medicine
 End of Life Care in the Acute Hospital Setting Dr Adam Brown Consultant in Palliative Medicine Learning objectives Understanding a patient's priorities for end of life care How to work with the 5 priorities
End of Life Care in the Acute Hospital Setting Dr Adam Brown Consultant in Palliative Medicine Learning objectives Understanding a patient's priorities for end of life care How to work with the 5 priorities
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on
 A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on the phone and even go out to their houses if needed
A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on the phone and even go out to their houses if needed
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
What do we want? Common purpose: ONE BED, ONE OUTCOME
 What do we want? Common purpose: ONE BED, ONE OUTCOME What do we want? Common Vision: Develop a sustainable, high quality New Care Model for people in community-beds and receiving home-based care services
What do we want? Common purpose: ONE BED, ONE OUTCOME What do we want? Common Vision: Develop a sustainable, high quality New Care Model for people in community-beds and receiving home-based care services
Cluster Network Action Plan Neath Cluster. Abertawe Bro Morgannwg University Health Board Neath Cluster Action Plan
 Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
Developing Integrated Care in Hertfordshire. Chris Badger Operations Director, Older People Hertfordshire County Council
 Developing Integrated Care in Hertfordshire Chris Badger Operations Director, Older People Hertfordshire County Council Hertfordshire s Approach A system that delivers the right care and support at the
Developing Integrated Care in Hertfordshire Chris Badger Operations Director, Older People Hertfordshire County Council Hertfordshire s Approach A system that delivers the right care and support at the
Right place, right time, right team
 Right place, right time, right team Thurrock Rapid Response Assessment Service A joint Thurrock social care and South West Essex Community Services initiative helps residents in Thurrock get a rapid response
Right place, right time, right team Thurrock Rapid Response Assessment Service A joint Thurrock social care and South West Essex Community Services initiative helps residents in Thurrock get a rapid response
Annex 3 Cluster Network Action Plan South Ceredigion and Teifi Valley Cluster Plan
 Annex 3 Network Action Plan 06-7 South Ceredigion and Teifi Valley Plan The Network Development Domain supports GP Practices to work to collaborate to: Understand local needs and priorities. Develop an
Annex 3 Network Action Plan 06-7 South Ceredigion and Teifi Valley Plan The Network Development Domain supports GP Practices to work to collaborate to: Understand local needs and priorities. Develop an
Wolverhampton Clinical Commissioning Group - Care Home Document
 Wolverhampton Clinical Commissioning Group - Care Home Document 1 Contents Page 1. Purpose 2. Workstreams Completed 3. 2014/15 Workstreams 4. Future Workstreams 2 1. Purpose 1.1. Introduction 1.1.1. This
Wolverhampton Clinical Commissioning Group - Care Home Document 1 Contents Page 1. Purpose 2. Workstreams Completed 3. 2014/15 Workstreams 4. Future Workstreams 2 1. Purpose 1.1. Introduction 1.1.1. This
SERVICE SPECIFICATION
 SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
Sheffield: using co-design & technology to deliver person-centred care Learning from the NHS England Test Bed Programme
 Sheffield: using co-design & technology to deliver person-centred care Learning from the NHS England Test Bed Programme www.ppptestbed.nhs.uk Philippa Hedley-Takhar @Perfect_Pathway #PerfectPathway Sheffield
Sheffield: using co-design & technology to deliver person-centred care Learning from the NHS England Test Bed Programme www.ppptestbed.nhs.uk Philippa Hedley-Takhar @Perfect_Pathway #PerfectPathway Sheffield
Introducing the Single Point of Access (SPA)
") Intermediate Care Staff Newsletter Welcome to the fourth edition of CONNECTED, the staff newsletter for Intermediate Care Services in Doncaster. The aim is to keep staff informed of developments in the
Intermediate Care Staff Newsletter Welcome to the fourth edition of CONNECTED, the staff newsletter for Intermediate Care Services in Doncaster. The aim is to keep staff informed of developments in the
Annual Report Summary 2016/17
 Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Please find below the response to your recent Freedom of Information request regarding Continence Services within NHS South Sefton CCG.
 Our ref: FOI ID 5544 2 6 th August 2015 southseftonccg.foi@nhs.net NHS South Sefton CCG Merton House Stanley Road Bootle Merseyside L20 3DL Tel: 0151 247 7000 Re: Freedom of Information Request Please
Our ref: FOI ID 5544 2 6 th August 2015 southseftonccg.foi@nhs.net NHS South Sefton CCG Merton House Stanley Road Bootle Merseyside L20 3DL Tel: 0151 247 7000 Re: Freedom of Information Request Please
1. Introduction. Cllr Maurice Jones Chair Central Bedfordshire Health and Wellbeing Board
 Contents: 1. Introduction 2. The Vision for Integrated Care 3. The Case for Change 4. BCF Plans 16/17 Delivery 5. Agreed approach to financial risk share and contingency 6. The National Conditions 7. BCF
Contents: 1. Introduction 2. The Vision for Integrated Care 3. The Case for Change 4. BCF Plans 16/17 Delivery 5. Agreed approach to financial risk share and contingency 6. The National Conditions 7. BCF
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
NHS RightCare scenario: The variation between standard and optimal pathways
 NHS RightCare scenario: The variation between standard and optimal pathways Sarah s story: Parkinson s Appendix 1: Summary slide pack January 2018 Sarah s story This is the story of Sarah s experience
NHS RightCare scenario: The variation between standard and optimal pathways Sarah s story: Parkinson s Appendix 1: Summary slide pack January 2018 Sarah s story This is the story of Sarah s experience
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
NHS 111 specification
 NHS 111 specification Contents NHS 111 Specification introduction 2 Vision/aims of NHS 111 3 NHS 111: The basics 3 Who is NHS 111 for? 3 What patients can expect the new service to do: 3 Basic service
NHS 111 specification Contents NHS 111 Specification introduction 2 Vision/aims of NHS 111 3 NHS 111: The basics 3 Who is NHS 111 for? 3 What patients can expect the new service to do: 3 Basic service
Supporting people who need Palliative and End of Life Care in the Community. Giving people a choice
 Supporting people who need Palliative and End of Life Care in the Community Giving people a choice Introduction People who are terminally ill or at the end of their life need excellent nursing and medical
Supporting people who need Palliative and End of Life Care in the Community Giving people a choice Introduction People who are terminally ill or at the end of their life need excellent nursing and medical
The Community Based Target Model
 1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
All clinical areas of the Trust All clinical Trust staff All adults with limited prognosis Palliative care team Approved. Purpose of this document
 Trust Policy and Procedure Document Ref. No: PP(15)310 End of Life Care For use in: For use by: For use for: Document owner: Status: All clinical areas of the Trust All clinical Trust staff All adults
Trust Policy and Procedure Document Ref. No: PP(15)310 End of Life Care For use in: For use by: For use for: Document owner: Status: All clinical areas of the Trust All clinical Trust staff All adults
Ladydale Care Home. Aegis Residential Care Homes Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement
 Aegis Residential Care Homes Limited Ladydale Care Home Inspection report 9 Fynney Street Leek Staffordshire ST13 5LF Tel: 01538386442 Website: www.pearlcare.co.uk Date of inspection visit: 10 May 2017
Aegis Residential Care Homes Limited Ladydale Care Home Inspection report 9 Fynney Street Leek Staffordshire ST13 5LF Tel: 01538386442 Website: www.pearlcare.co.uk Date of inspection visit: 10 May 2017
We need to talk about Palliative Care. The Care Inspectorate
 We need to talk about Palliative Care The Care Inspectorate Introduction The Care Inspectorate is the official body responsible for inspecting standards of care in Scotland. That means we regulate and
We need to talk about Palliative Care The Care Inspectorate Introduction The Care Inspectorate is the official body responsible for inspecting standards of care in Scotland. That means we regulate and