Central New York Care Collaborative Primary Care Transformation Project Implementation Collaborative Kickoff Meeting. Friday, February 26, 2016
|
|
|
- Kelley Porter
- 5 years ago
- Views:
Transcription


1 Central New York Care Collaborative Primary Care Transformation Project Implementation Collaborative Kickoff Meeting Friday, February 26, 2016
2 Welcome and Introductions CNYCC Team Karen Joncas-Project Manager for Primary Care Transformation (and CVDM) PIC Moderator Lauren Wetterhahn-Director of Program Operations PIC Facilitator Liz Fowler-Operations Coordinator Scribe
3 Learning Objectives
4 Learning Objectives Topics What is the Delivery System Reform Payment Program(DSRIP) What is the Central New York Care Collaborative (CNYCC) Project Implementation Collaborative (PIC)-Who, What, When DSRIP Primary Care Transformation Requirements Overview Patient-Centered Medical Home (PCMH) Readiness Assessment Overview Getting Started with PCMH Transformation A Word about Advanced Primary Care (APC) A Word about PCMH 2017 Redesign CNYCC Partner Support Resources Q & A and Next Steps
5 Introduction to DSRIP and the CNYCC
6 DSRIP - Delivery System Reform Incentive Payment Program Created in 2014 allowing NYS to re-invest federal savings generated by the Medicaid Redesign Team (MRT) Funding provided to support hospitals and other service provides to change how healthcare is provided to Medicaid beneficiaries Provides incentives to promote community-level collaborations through Performing Provider Systems (PPSs) $6.42 billion for payments to all state PPSs to meet DSRIP goals of system reform and cost reduction Goals of DSRIP Reduce avoidable hospital readmissions and emergency department use by 25% over the next 5 years Preserve and transform the State s fragile health care safety net system
7 performance CNYCC Central New York Care Collaborative Mission: Working together for better health Vision: To improve the health of our community by coordinating services and building partnerships throughout the healthcare system Guiding Principles: Better Integrate Services Collaborate on Patient Care Improve Healthcare Quality Lower Cost of Healthcare


8 CNYCC: At a Glance 6 COUNTIES Cayuga, Lewis, Madison, Oneida, Onondaga, and Oswego 170 Partner Organizations 9,700 SQUARE MILES Nearly 200,000 MEDICAID SUBSCRIBERS New Corporation PPS Lead Agency 1,400 HEALTHCARE AND COMMUNITY- BASED SERVICE PROVIDERS
9 CNYCC Governance Corporate Members (4 Co-Leads) Board of Directors (22 Members) Executive Project Advisory Committee (EPAC) RPAC Cayuga County RPAC Lewis County Board Committees Executive Committee Finance Committee RPAC Madison County RPAC Oneida County Clinical Governance Committee Nominating Committee RPAC Onondaga County Compliance Committee IT/Data Governance Committee RPAC Oswego County




10 Partner Engagement Structures Inform
11 Project Implementation Collaborative (PIC) Overview
12 Project Implementation Collaborative (PIC) Purpose The PIC will develop, update, and guide the CNYCC s project implementation plans over time with an eye toward meeting state project requirements, implementation of best practice, and broad system transformation
13 Project Implementation Collaborative (PIC) Who-Roles and Responsibilities All partner organizations who have signed up to participate in projects are encouraged to actively participate (Remember: Our joint success is based on individual partners meeting goal). Participants will have a voice in the full PIC meetings and may volunteer to participate in smaller, targeted cohorts or work groups that meet more often and report back to full PIC CNYCC Project Manager is the PIC facilitator ensuring that information flows between smaller groups and full PIC and monitors partner project plans against goals
14 Project Implementation Collaborative (PIC) What Primary Care Transformation is integral to the Integrated Delivery System project Primary Care Transformation PIC purpose is to assist all eligible partners in achieving NCQA PCMH 2014 Recognition Assist in identifying and sharing best practices Support project monitoring and quality improvement processes Promote/Celebrate project success and the system transformation
15 Project Implementation Collaborative (PIC) When Primary Care Transformation PIC will begin monthly meetings by Webinar Primary Care Transformation PIC will periodically meet jointly with the Health Information Technology PIC to discuss common goals
16 Primary Care Transformation PIC Partner Member Role Actively Participate in the Meetings Share expertise (best practices) with other Members Share concerns or risks in meeting project goals Achieve success in meeting project goals and deadlines Project Manager Role PIC moderator ensuring that information flows between all partner members Educate Partners in project requirements Mitigate project risks Monitor Partner Plans to ensure meeting NYS Project Implementation Plan Deadlines
17 Primary Care Transformation PIC Purpose Work together to ensure the success of the collaborative integrated delivery system and all eligible partners achieve transformation validated by NCQA PCMH 2014 Recognition What Collaborative venue for sharing best practices across the partner network Communication link for updates/issues to partner organizations Who Partner organization s Project Leadership, Clinical Leadership, HIT Leadership, Quality Leadership, Administrative Leadership Partner organization s DSRIP Coordinator





18 Relationship Between PICs HIT PIC Exploration, Vetting and Development Of Technical Solutions Clinical & Operational Requirements Development Project & Primary Care Transformation PICs
19 PCMH and DSRIP
20 PCMH and DSRIP PCMH required across multiple DSRIP projects including: Integrated Delivery System (2ai) DSRIP Care Management (2aiii) ED Care Triage (2biii) Primary Care/Behavioral Health Integration (3ai) Cardiovascular Disease Management (3bi) Palliative Care PCMH Integration (3gi) Implement strategies for contracted projects into your PCMH plan.
21 Introduction to PCMH
22 What is PCMH? Patient-centered medical home (PCMH), is a team-based health care delivery model led by a health care provider that is intended to provide comprehensive and continuous medical care to patients with the goal of obtaining maximized health outcomes. The evidence indicates how the medical home inspires quality in care, cultivates more engaging patient relationships, and captures savings through expanded access and delivery options that align patient preferences with payer and provider capabilities.
23 Readiness Assessment & Planning Process Overview
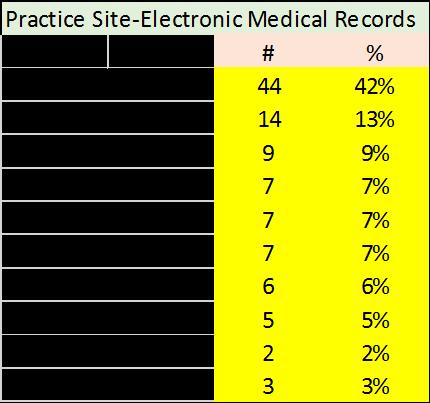
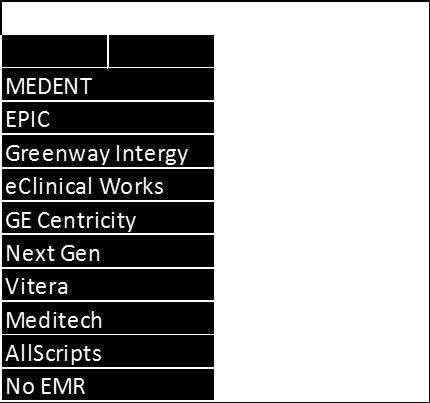
24 PPS PCMH and MU Readiness Assessment Goals Identified current state including PCMH recognition, MU attestation, readiness to transform practice to PCMH Final Reports On-site or telephone assessments of each practice Summary of PPS Partner recognition status and EMR platform Cohort strategy for small workgroups and learning collaborative sessions

25 PPS PCMH Readiness Assessment
26 Planning for Transformation

27
28 Educate
29 Educate Practice Eligibility Practice provides coordinated, team-based whole-person care at outpatient primary care sites Personal clinician (MD, DO, APRN, PA) with their own patient panel and provides first contact, continuous, comprehensive care for at least 75% of its patients Does not include urgent care clinics or those offering seasonal care Provides scheduled routine and urgent care appointments icalhomepcmh/beforelearnitpcmh/pcmheligibility.aspx
30 Educate Determine Type of Submission Single Site(s) submission Confirm Eligibility for submitting a multi site application Three or more eligible sites Use same EMR system Operate under the same policies and procedures Telephone Consultation with NCQA Project Leader for mulit-site application Process.aspx
31 Educate NCQA PCMH 2014 Standards Obtain a copy of PCMH 2014 Recognition Standards and Guidelines ( NCQA offers recorded trainings Community Health Care Association of NYS (CHCANYS) PCMH resources Patient Centered Primary Care Collaborative ( Download the PCMH 2014 Self- Assessment tool
32 Already PCMH 2011 Recognized? Conversion vs Renewal
33 Educate Conversion to PCMH 2014 Documentation required for six standards Must complete the full survey tool All positive survey responses subject to audit Submission of Record Review not Required-Sample care plan only Does not extend recognition expiration date Must have achieved PCMH 2011 Level 3 Option if 2 years of quality data is not available
34 Educate Renewal to PCMH 2014 Documentation required for eleven standards Must complete the full survey tool All positive survey responses subject to audit Extends recognition expiration date for three years Must have achieved PCMH 2011 Level 2 or 3
35 Plan
36 Project Planning Payment Policy Planning Develop and Submit a Project Charter including Names and Contact Information and Defined roles of Project Team Members Complete Project Plan Documentation Template (Under Development) Complete and Submit Planning Questions in Appendix B/Payment Mechanism 3 Complete Provided Excel Template with Provider Information
37 Components of a Project Charter
38 Project Charter Suggested Components Determine the Project Mission and Objectives Determine the Project Deliverables and Timeline Develop a Project Team Determine a communication plan and decision making process Determine Frequency and Location of Project Meetings Determine if outside resources will be used Determine where project documentation will be kept
39 Establish a Project Team
40 PCMH Project Team Suggested Team Members Physician Champion Project Leader Clinical Leader Administrative Leader Quality Leader HIT Leader Scribe Some team members could take on multiple roles or share roles with multiple staff. Team Members should always strive for sustainable change with the goal to improve care for all patients.
41 Project Team Roles
42 Project Team Members Physician Champion Should have passion for and be able to define organizational values and facilitate culture change to patient-centered team based care. Develop the strategic vision and drive the necessary investment in infrastructure change in people, process and technology. Manage resistance and set a positive tone for the project Embrace performance measurement and partner with project team to communicate quality initiatives and evidence best practices to providers and staff
43 Project Team Members Project Leader Responsible for the facilitation of the project plan development and project management. Communicates status throughout the team and organization. Ensures the project team and staff completes all aspects of transformation and submission Makes sure that success is continually celebrated with the team and all staff. Communicates with CNYCC Project Manager regarding status of the project and any risks or issues to meeting project goals.
44 Project Team Members Clinical Leader Responsible for managing and overseeing all clinical functions within the practice including: clinical advice, team based care, population health management, evidence-based decision support, care management and support, medication management. This role is typically held by a physician or mid-level provider. The functions may be assisted by a Clinical Nurse Manager.
45 Project Team Members Administrative Leader Responsible for supervising and directing all administrative functions within the practice including policy and workflow updates for PCMH topics such as patient access and scheduling, patient orientation and transitions, collecting demographic information, communicating medical home responsibilities, language services and care coordination. A practice manager or administrative director is ideal for this role
46 Project Team Members Quality Team Leader Leads the practice or organization s Quality Improvement(QI) Team. Works with the QI team to assign roles and responsibilities for quality improvement for all functions in the practice and all QI committee roles Works with the practice/organization to identify performance measures and quality improvement initiatives
47 Project Team Members HIT Leader Responsible for all Health Information Technology requirements including assessment of capability of systems to meet PCMH (including Meaningful Use) requirements, building of required EMR templates to facilitate the delivery of consistent evidence based medicine; building and running reports (and/or training others). Interfaces with EMR Vendor as required. Interfaces with CNYCC on interoperability capabilites
48 Project Team Members Scribe Responsible for taking notes at all scheduled and ad-hoc planning meetings. The organization can decide how these will be distributed or stored for easy access by all team members.
49 Implement
50 Implementation Early Steps Begin with the steps (standards) that will have multiple impact on culture and where focus will enhance sustainability These should be implemented with buy-in from staff and with the support of practice/organizational leadership Prepare PCMH self-assessment to identify opportunities Develop Care Team Strategy Develop communication strategy to include all team members in PCMH transformation and all quality initiatives Develop Quality Improvement Strategy NCQA Focus: Standard 2D and 6
51 Implementation Early Steps Assess where new policies, documented processes will be needed Assess PCMH standard alignment with planning strategies Training Strategy Health Information Technology Strategy Prepare Baseline Reporting for QI and Gaps in Care (when available) NCQA Focus: Multiple standards, Standards 2D, 6 and 3D
52 Implementation Early Steps Determine Patient Engagement Strategy Patient experience measurement Patient Advisory Council; Patients on QI team Care management strategy and workflows Shared decision making aids Self-management support Home monitoring for chronic conditions NCQA Focus: Multiple standards, Standard 2D, 4B, 4E, 6C
53 Implementation Patient Access Develop understanding of patient access supply and demand Provider patient panels Demand vs. Supply of Same Day Access Appointments Develop minimum standards for wait times for appointments Determine how supply and demand of appointments will be monitored Consider alternative visits Determine baseline no-show rates and review policies to mitigate this affect on patient access NCQA Focus: Standard 1
54 Implementation Integrated and Coordinated Care Develop/update/tighten strategies for care coordination and care transitions Tracking and follow-up on all tests and referrals Manage all care transitions (hospitals, palliative care, referrals, new patients) Behavioral Health Strategy Co-management agreements with specialty care providers Build relationships with community based organizations Engage in the RHIO NCQA Focus: Standards 5 and 2A
55 Implementation Communication Plan Develop strategy to communicate the roles and responsibilities of a medical home Develop strategy to Communicate Performance Results externally Develop strategy to effectively communicate to patients with consideration to cultural competency and health literacy. Develop strategy for patient education and self-management support Internal communication plans- team huddles, practice process, quality performance results NCQA Focus: Standards: Multiple including 1B, 1C, 2, 4B, 4E,6F
56 Implementation Evidence-Based Medicine Develop patient safety strategies including: Consistent evidence-based medicine Implement Clinical Decision Support tools Care Coordination NCQA Focus: Standards 3E, 5
57 Implementation Documentation Gaps Complete Mock Audit-Chart Review using NCQA Record Review Workbook to identify documentation gaps Complete health assessments Medication Care plan Revise workflows as needed NCQA Focus: Standards 3C, 4B, 4C
58 Implementation Execute Policy, Documented Process, Workflow and Procedure Evidence-based Medicine Clinical Decision Support Quality Initiative Action Plan Population Health Management- Gaps in Care Patient Engagement Plan Internal and External Communication Plans Integrated and Coordinated Care Training Strategies NCQA Focus: Standards: Multiple and 1, 2B, 2D,3D,3E,5, 6
59 Implementation Execute Care Management Strategy Patient Identification Workflows Care Team Members-Internal Resources vs. External Resources Care Plan Templates Motivational Interviewing Self-Management Support Care Coordination Community Based Resources NCQA Focus: Standards 4B and 5
60 Implementation Execution of NCQA Application and Survey Final Report Run Complete final Record Review Complete Quality Improvement Worksheet Complete NCQA On-line Application (and fees) Prepare Final Survey tool Final Quality Check of all Documents to be Submitted Upload Documents to NCQA Document Library Submit NCQA ISS Tool and Document Library CELEBRATE
61 Sustain A Word on Sustaining the Transformation Build process audits into policies Maintain accountability to patients Maintain quality improvement team with continued measurement CONTINUE to CELEBRATE SUCCESS
62 PCMH Suggested Timeline
63 Timeline Considerations Current PCMH Recognition Status and Expiration Date EMR Implementation or Upgrade Readiness Multi-site vs. Single Site submissions Organization Mission and Objectives Transformation Process could take 1 year or more PPS to have Staggered Timelines No NCQA submissions in PPS after October 1, 2017
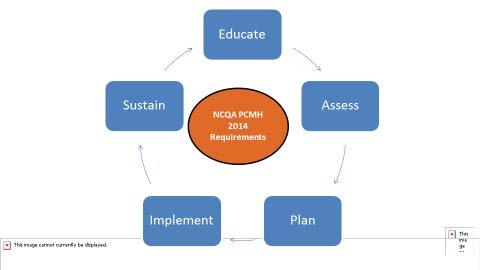
64 Assessment and Planning Process Timeline Educate, Assess, Plan Care Team Strategy Behavioral Health Strategy and implementation Quality Improvement Strategy Communication Plan-Internal and External HIT Cohort Assistance/Baseline Reporting Training Strategy and Implementation Patient Engagement Strategy Determine and communicate QI plan Execute population health and other QI action plans Patient Access Strategy and Implementation Execute Internal and External Communications Update and Implement Policies and Procedures and workflows Care Coordination and Transitions Monitoring Execute Care Management Strategy Finalize Documentation for Submission Complete On-Line NCQA application Final Document Audit and Sign off Load documents to Document Library and Submit NCQA Survey Tool 31-Mar May Jul Sep Nov Jan Mar May May Jul Sep-17 This graphic display is a sample project plan meant to show how educate, assess, plan and implement are often not linear. Also, in order for transformation to be sustainable, transformation and quality improvement continue.
65 NYS Advance Primary Care Model
66 Advanced Primary Care Model New York State Innovation Model: Comprehensive, patient-centered care Coordinated care between primary care and other clinical care and community-based services Greater usage of HIT including EHR, Population Health and data analytics Financial support for primary care practices for transformation A shift from encounter based payment to alternative payments supporting services and infrastructure Multi-payer participation and alignment
67 Advanced Primary Care Model New York State Innovation Model: Meaningful Performance Measures consistent with existing standards and measures (NCQA, CPCI, etc.)-measured on improvement in Core Measures Requires ability to identify high-risk patients and have plan for care coordination Drive change over time instead of one-time certification Be tied to outcomes and facilitated by innovative payment systems State goal is for 80% of care to be paid under a value-based financial arrangement within 5 years Timeline fluid Preliminary Launch scheduled January 2017
68 Advanced Primary Care Model PCMH or APC? State Project Implementation Plan requires one or the other Recommendation is for PPS practices to pursue PCMH State APC Model has delayed launch date Those with PCMH Recognition with demonstrated transformation will be eligible for earlier access to care coordination payments and/or outcome based payments Measure metrics to be aligned with PCMH and other quality initiatives Existing Medicaid PMPM payments Additional information forthcoming
69 NCQA PCMH 2017 Re-design
70 NCQA PCMH 2017 NCQA PCMH Redesign Role out Spring PCMH 2014 Retires December Earlier for corporate application. No survey tool purchases after June Overarching objective is to enhance the value of the recognition for all stakeholders Reduce the burden of non-value added work More focus on outcomes instead of structure and process More support for transforming practices
71 NCQA PCMH 2017 NCQA PCMH Redesign Two pathways Those with first time recognition will complete an assessment to determine readiness. If more work is needed practice would be directed to additional educational materials. Second pathway-engagement phase-match practice with a facilitator and reviewer, identify education needed, facilitate check-ins with a reviewer where practice would know where they stand during process. Engaging practices in a streamlined annual check-in rather than three year documentation burden Watch for more information on NCQA blog
72 CNYCC Partner Support Resources Learning Collaborative Sessions

73 CNYCC Learning Collaborative Sessions

74 CNYCC Learning Collaborative Sessions
75 CNYCC Partner Support Resources Health Information Technology Support
76 Readiness Assessment-Health Information Technology Goals Identify current state of health information technology availability and capability including: Access to RHIO and usage of Direct Messaging EMR certification for Stage 2 Meaningful Use Provide Clinical Decision Support to facilitate evidence based care Access to reporting required for PCMH and other quality performance measurements Format Series of surveys indicating technology capability of each organization Summary of PPS Partner status
77 Integrated Delivery Network-HIT Support Goals Vendor Engagement to Implement/Optimize EMR Platforms EMR Vendor Selection Toolkit Create clinically integrated networks Build the technical infrastructure including a shared platform to enable care coordination and population health management Develop Project/Reporting Specific HIT requirements Technical Assistance Technical Cohort Development
78 CNYCC Partner Support Resources Funds Flow
79 CNYCC Integrated Delivery System Funds Flow Project Activity Description Eligible Partners DY1 Payments 2.a.i Category 1. Regional Health Information Organization (RHIO) Payment 1: Payment for signing a participation agreement and implementing a consent management policy/procedure All Partners Total: $870,349 Per Partner: $2,500 Assumption: 350 responding partner sites 2.a.i Category 2. Electronic Medical Records (EMR) Payment 1: Current State Assessment (Documented plan for upgrading to, or implementing new MU Certified EMR that meets DSRIP requirements; documented plan for making required system changes to meet DSRIP requirements) MU eligible; BH Providers; SNFs; Non- PCPs Total: $1,450,582 Per EMR: $10,000 Assumption: 145 completed assessments 2.a.i Category 3. Patient-Centered Medical Home Payment 1: Per practice site payment for PMCH 2014 Level 3 recognition plan PCPs Total: $1,740,699 Per PCP Site: $10,000 Assumption: 145 responding PCP sites

80 Questions & Answers
81 CNYCC Primary Care Transformation PIC: Feedback Do you feel you have a good understanding of the goals of Primary Care Transformation? What type of support would be most useful to you? What topics would you like to see brought to this PIC or learning collaborative sessions? What success stories do you have to share? How have you celebrated success with your staff?
82 Next Steps & Wrap Up
83 Next Steps & Wrap Up Next Steps Complete Project Planning Templates Assist CNYCC IT Team in identification of needed IT reports and other technology upgrades to meet NCQA PCMH 2014 Site visits with Project Leaders to review planning process, assess needed support Learning collaborative sessions plan
84 Next Steps & Wrap Up Next Meeting PIC meeting 3/25/16, 10:00 AM 12:00 PM Joint meeting with HIT PIC with DSRIP IT leads and other PCMH Project Team Leaders and DSRIP Coordinators
Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016
 Oneida County Health Coalition Meeting June 30, 2016") Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016 Agenda 1. Overview of the NYS DSRIP Program 2. History of Performing Provider Systems in Central New York
Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016 Agenda 1. Overview of the NYS DSRIP Program 2. History of Performing Provider Systems in Central New York
Primary Care/Behavioral Health Integration (3ai)
") Primary Care/Behavioral Health Integration (3ai) Standards of Care Summary Opportunity for PIC Input Standards of Care - Workgroup Workgroup Charge It is expected that standards of care be developed around
Primary Care/Behavioral Health Integration (3ai) Standards of Care Summary Opportunity for PIC Input Standards of Care - Workgroup Workgroup Charge It is expected that standards of care be developed around
DSRIP 2017: Lessons Learned and Paving the Way for Success
 DSRIP 2017: Lessons Learned and Paving the Way for Success Greg Allen, MSW (Moderator) Director, Division of Program Development and Management Office of Health Insurance Programs, New York State Department
DSRIP 2017: Lessons Learned and Paving the Way for Success Greg Allen, MSW (Moderator) Director, Division of Program Development and Management Office of Health Insurance Programs, New York State Department
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
Building the Oncology Medical Home. Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc.
 Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information. As of October 28, 2015
 Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information As of October 28, 2015 10/28/2015 2 General Guidance regarding Domain 1 Active Engagement The Independent Assessor
Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information As of October 28, 2015 10/28/2015 2 General Guidance regarding Domain 1 Active Engagement The Independent Assessor
Using Healthix to Support DSRIP: Opportunities and Challenges. February 25, 2016
 Using Healthix to Support DSRIP: Opportunities and Challenges February 25, 2016 Contents 1. Community Care of Brooklyn Overview (2 5) 2. Healthix Enablement of CCB IT Strategy (6-13) 3. Challenges (slide
Using Healthix to Support DSRIP: Opportunities and Challenges February 25, 2016 Contents 1. Community Care of Brooklyn Overview (2 5) 2. Healthix Enablement of CCB IT Strategy (6-13) 3. Challenges (slide
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State
 Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
OneCity Health Partner Webinar
 1 OneCity Health Partner Webinar Past, Present, and Looking Ahead December 13, 2016 Today s Presenter 2 Richard Bernstock, Bronx Hub Executive Director Topics for Today s Webinar 3 OneCity Health Partner
1 OneCity Health Partner Webinar Past, Present, and Looking Ahead December 13, 2016 Today s Presenter 2 Richard Bernstock, Bronx Hub Executive Director Topics for Today s Webinar 3 OneCity Health Partner
Task for Partner PCMH Standard APC Requirement TCPI Milestone
 Page 2/ Question 1 2aiM4D1* 2aiiiM3D1* Submit last page of signed participation agreement with HealthLinkNY or other Qualified Entity (QE). Standard 5B - Referral Tracking and Follow-up 5.B.7. Has the
Page 2/ Question 1 2aiM4D1* 2aiiiM3D1* Submit last page of signed participation agreement with HealthLinkNY or other Qualified Entity (QE). Standard 5B - Referral Tracking and Follow-up 5.B.7. Has the
Patient-Centered Medical Home Assessment & Roadmap
 11/30/2016 Patient-Centered Medical Home Assessment & Roadmap Population Health Management Workstream Milestone 1 Table of Contents 1) Executive Summary 2) Overview of Primary Care Providers 3) PCMH Timeline
11/30/2016 Patient-Centered Medical Home Assessment & Roadmap Population Health Management Workstream Milestone 1 Table of Contents 1) Executive Summary 2) Overview of Primary Care Providers 3) PCMH Timeline
# Topic Responsible Person Document
 NYPQ DSRIP PPS PCMH Committee Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: September 5, 2017 Conference Line: 877-594-8353 Code: 79706143# Location:
NYPQ DSRIP PPS PCMH Committee Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: September 5, 2017 Conference Line: 877-594-8353 Code: 79706143# Location:
Performing Provider System (PPS) CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK
 CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK") Performing Provider System (PPS) Westchester Medical Center Health Network CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK 7 SKYLINE DRIVE, SUITE 385 HAWTHORNE, NY 10532 914.326.4200
Performing Provider System (PPS) Westchester Medical Center Health Network CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK 7 SKYLINE DRIVE, SUITE 385 HAWTHORNE, NY 10532 914.326.4200
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
REQUEST FOR PROPOSAL PROJECT 3AII: BEHAVIORAL HEALTH CRISIS STABILIZATION CRISIS STABILIZATION SERVICES EXPANSION
 REQUEST FOR PROPOSAL PROJECT 3AII: BEHAVIORAL HEALTH CRISIS STABILIZATION CRISIS STABILIZATION SERVICES EXPANSION DATE: MARCH 9 TH, 2016 UPDATED: MARCH 30, 2016 UPDATED: APRIL 11, 2016 CNY CARE COLLABORATIVE
REQUEST FOR PROPOSAL PROJECT 3AII: BEHAVIORAL HEALTH CRISIS STABILIZATION CRISIS STABILIZATION SERVICES EXPANSION DATE: MARCH 9 TH, 2016 UPDATED: MARCH 30, 2016 UPDATED: APRIL 11, 2016 CNY CARE COLLABORATIVE
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Behavioral Health Integration in the Primary Care Setting
 Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Meeting Title. Facilitator. Conference Line
 DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
SIM Cohort 3 Application Instructions and Questions
 SIM Cohort 3 Application Instructions and Questions Overview, Instructions & Resources: SIM Cohort 3 Application Overview: Thank you for your interest in the Colorado State Innovation Model (SIM) Initiative
SIM Cohort 3 Application Instructions and Questions Overview, Instructions & Resources: SIM Cohort 3 Application Overview: Thank you for your interest in the Colorado State Innovation Model (SIM) Initiative
Westchester Medical Center PPS Project Advisory Committee. April 15, 2015 Via Webinar: 10:00 am 11:30 am
 Westchester Medical Center PPS Project Advisory Committee April 15, 2015 Via Webinar: 10:00 am 11:30 am Agenda Discussion Topic Welcome & Status Update Finalizing the Implementation Plan DSRIP Year 1:
Westchester Medical Center PPS Project Advisory Committee April 15, 2015 Via Webinar: 10:00 am 11:30 am Agenda Discussion Topic Welcome & Status Update Finalizing the Implementation Plan DSRIP Year 1:
NCQA PCMH 2017 Standards Intro 3/29/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Part 1: NCQA PCMH 2014 Standards
 Part 1: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health Objectives Examine the requirements for NCQA PCMH 2014 Standards Review project
Part 1: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health Objectives Examine the requirements for NCQA PCMH 2014 Standards Review project
NewYork-Presbyterian/Queens PPS Clinical Integration Strategy
 NewYork-Presbyterian/Queens PPS Clinical Integration Strategy Document Title: NYP/Q PPS Clinical Integration Strategy Version 1.0 Purpose: Approving Committee: This document outlines the needs for a clinically
NewYork-Presbyterian/Queens PPS Clinical Integration Strategy Document Title: NYP/Q PPS Clinical Integration Strategy Version 1.0 Purpose: Approving Committee: This document outlines the needs for a clinically
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
NY State initiatives for Primary Care Practices: CPC plus - Webinar
 NY State initiatives for Primary Care Practices: CPC plus - Webinar Marcus Friedrich, MD, MBA, FACP Medical Director NYSDOH - Office of Quality and Patient Safety August 30, 2016 August 30, 2016 2 Primary
NY State initiatives for Primary Care Practices: CPC plus - Webinar Marcus Friedrich, MD, MBA, FACP Medical Director NYSDOH - Office of Quality and Patient Safety August 30, 2016 August 30, 2016 2 Primary
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017
 Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
CLINICAL INTEGRATION STRATEGY
 CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
# Topic Responsible Person Document
 Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: August 1, 2017 Conference Line: 877-594-8353 Code: 79706143# Location: Meeting Purpose: NYPQ 56-45
Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: August 1, 2017 Conference Line: 877-594-8353 Code: 79706143# Location: Meeting Purpose: NYPQ 56-45
University of Rochester Medical Center Community Advisory Council
 December 8, 2015 University of Rochester Medical Center Community Advisory Council FLPPS and DSRIP Carol Tegas Executive Director 1 Agenda DSRIP in NYS FLPPS Implementation of DSRIP Vision: Create a Regional
December 8, 2015 University of Rochester Medical Center Community Advisory Council FLPPS and DSRIP Carol Tegas Executive Director 1 Agenda DSRIP in NYS FLPPS Implementation of DSRIP Vision: Create a Regional
Nicole Harmon, MBA, PCMH CCE Senior Director HANYS Solutions Practice Advancement Strategies
 Nicole Harmon, MBA, PCMH CCE Senior Director HANYS Solutions Practice Advancement Strategies HANYS Healthcare Solutions Association Practice of Advancement New York State Strategies www.hanys.org 9/28/2017
Nicole Harmon, MBA, PCMH CCE Senior Director HANYS Solutions Practice Advancement Strategies HANYS Healthcare Solutions Association Practice of Advancement New York State Strategies www.hanys.org 9/28/2017
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
A. PCMH Service Site: 1. Co-locate behavioral health services at primary care practice sites. All participating primary
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
QUALITY IMPROVEMENT ROUNDTABLE
 QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Cayuga County Regional Project Advisory Committee
 Cayuga County Regional Project Advisory Committee Welcome and Introductions Cayuga EPAC Representative Liz Smith Value Based Payment and the Year Ahead https://youtu.be/jqfipbmg2rs Goals of DSRIP There
Cayuga County Regional Project Advisory Committee Welcome and Introductions Cayuga EPAC Representative Liz Smith Value Based Payment and the Year Ahead https://youtu.be/jqfipbmg2rs Goals of DSRIP There
NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014
 NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014 Present: D. Johansson-ACMH, L. Capitelli-NY Psychiatric Institute, K. Meyer-Community Healthcare Network, E. Eng-ArchCare,
NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014 Present: D. Johansson-ACMH, L. Capitelli-NY Psychiatric Institute, K. Meyer-Community Healthcare Network, E. Eng-ArchCare,
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Meeting Title. Facilitator. Conference Line. Corporation)
") DSRIP Meeting Agenda 5/29/15 NYP PPS Date and Time Meeting Title Committee Location 45 Wadsworth Street, 9 th Floor Facilitator Dr. Emilio Carrillo Go to Meeting https://global.gotomeeting.com/ join/158738573
DSRIP Meeting Agenda 5/29/15 NYP PPS Date and Time Meeting Title Committee Location 45 Wadsworth Street, 9 th Floor Facilitator Dr. Emilio Carrillo Go to Meeting https://global.gotomeeting.com/ join/158738573
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD
 MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Patient Centered Specialty Practice: Are We Ready for. Course Schedule
 Patient Centered Specialty Practice: Are We Ready for MACRA? Xiaoyan Huang, MD, MHCM, FACC Providence Heart Clinic December 5 th, 2016 28 th IHI National Forum Course Schedule Morning: Introduction Xiaoyan
Patient Centered Specialty Practice: Are We Ready for MACRA? Xiaoyan Huang, MD, MHCM, FACC Providence Heart Clinic December 5 th, 2016 28 th IHI National Forum Course Schedule Morning: Introduction Xiaoyan
NYS Value Based Payments (VBP):
:") NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
NYS DSRIP Overview. Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO. November 2016
 NYS DSRIP Overview Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO November 2016 DSRIP: A Mechanism to Transform Medicaid Delivery Delivery System Reform Incentive Payment (DSRIP) programs are a key mechanism
NYS DSRIP Overview Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO November 2016 DSRIP: A Mechanism to Transform Medicaid Delivery Delivery System Reform Incentive Payment (DSRIP) programs are a key mechanism
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Moving into DSRIP Year 4 What Do We Need To Do. Peggy Chan DSRIP Program Director
 Moving into DSRIP Year 4 What Do We Need To Do Peggy Chan DSRIP Program Director 2 DSRIP Implementation Timeline and Key Benchmarks We are here Focus on Infrastructure Development/System Design Focus on
Moving into DSRIP Year 4 What Do We Need To Do Peggy Chan DSRIP Program Director 2 DSRIP Implementation Timeline and Key Benchmarks We are here Focus on Infrastructure Development/System Design Focus on
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use
 Welcome! Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use Presented by: Larry Katzovitz & Judy Triano Elmhurst Memorial Healthcare Kay Jackson (978) 805-3104 Kay.Jackson@iatric.com
Welcome! Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use Presented by: Larry Katzovitz & Judy Triano Elmhurst Memorial Healthcare Kay Jackson (978) 805-3104 Kay.Jackson@iatric.com
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Albany Medical Center. AMCH PPS Clinical & Quality Affairs Committee. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH PPS August 26, 2015
 Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH PPS August 26, 2015 AMCH PPS: Clinical & Quality Affairs (CQA) Committee Presentation
Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH PPS August 26, 2015 AMCH PPS: Clinical & Quality Affairs (CQA) Committee Presentation
Delivery System Reform Incentive Payment (DSRIP)
") Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
Health System Transformation Overview of Health Systems Transformation in New York State. July 23, 2015
 Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
Report of the Connecticut State Medical Society-IPA, Inc. to the Connecticut State Medical Society House of Delegates September 30, 2015
 Report of the Connecticut State Medical Society-IPA, Inc. to the Connecticut State Medical Society House of Delegates September 30, 2015 Each year the Connecticut State Medical Society IPA (CSMS-IPA) provides
Report of the Connecticut State Medical Society-IPA, Inc. to the Connecticut State Medical Society House of Delegates September 30, 2015 Each year the Connecticut State Medical Society IPA (CSMS-IPA) provides
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers. LeadingAge New York Webinar
 Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
Michigan Primary Care Association
 Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Introduction to PCMH 2017
 Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
NCQA Recognition Programs Redesign Work in Progress
 NCQA Recognition Programs Redesign Work in Progress March 2016 Mina Harkins, MBA, BSMT, PCMH CCE NCQA Assistant Vice President Recognition Programs Policy and Resources Re-use without permission is prohibited
NCQA Recognition Programs Redesign Work in Progress March 2016 Mina Harkins, MBA, BSMT, PCMH CCE NCQA Assistant Vice President Recognition Programs Policy and Resources Re-use without permission is prohibited