TRANSITIONS: Improving Care for High-Risk Medicaid Beneficiaries in Tompkins County
|
|
|
- Anissa Johnson
- 5 years ago
- Views:
Transcription
1 TRANSITIONS: Improving Care for High-Risk Medicaid Beneficiaries in Tompkins County Aging Concerns Unite Us Conference June 7, 2016 Lisa Holmes, Tompkins County Office for the Aging Sue Ellen Stuart, Visiting Nurse Services of Ithaca and Tompkins County 1

2 Why Care Transitions? 2
3 National Data on Hospital Readmissions New England Journal of Medicine (2009): Nationally, 1 in 5 Medicare beneficiaries are readmitted within 30 days following hospitalization Medicare cost of over $17 billion annually Heart failure, pneumonia, COPD were among most frequent medical diagnoses of patients readmitted Half of patients readmitted had no physician contact within 30 days post- discharge 3
4 National Data on Hospital Readmissions Medicaid patients have readmission rates as high or higher than Medicare patients 25% of Medicare patients with CHF returned to hospital in 30 days; 33% Medicaid patients. Medicaid readmission patterns: more behavioral health conditions, socio-economic factors affecting access, substance abuse. Agency for Healthcare Research and Quality 4
5 Tompkins County s Previous Care Transitions Experience CMS Community Based Care Transitions Program (CCTP) Goal: To reduce hospital readmissions among Medicare FFS beneficiaries by 20% Strategy: Collaboration of multiple community agencies facilitated and led by Tompkins County Office for the Aging: including VNS, Hospice, Cayuga Medical Center 5
6 CCTP Partners Tompkins County Office for the Aging: lead agency, coordination, reporting, billing Cayuga Medical Center community hospital Visiting Nurse Services coaching Hospicare coaching 6
7 Care Transitions Intervention Developed by Dr. Eric Coleman of the University of Colorado Designed to encourage older patients and their caregivers to assert a more active role during care transitions Low cost Low intensity Easily adaptable Short 30 days with 1 home visit and 3 phone calls 7
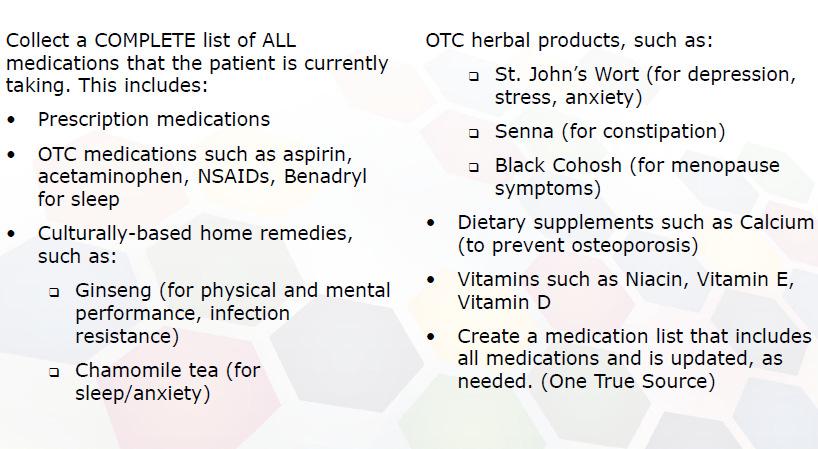
8 The Four Pillars of CTI 1. Medication self-management 2. Follow-up with PCP/Specialist 3. Knowledge of red flags or warning signs/symptoms and how to respond 4. Patient-centered medical record Transitions Coach is used to build skills, confidence and to provide tools to support self-management Model behavior for common problems Practice or role play for health care encounters Create an accurate medication list 8
9 Tompkins CCTP: Challenges and Lessons Learned Challenge: Low patient volume Smallest CCTP site in nation, small rural hospital Could only bill for Medicare FFS inservice patients (no Medicare Advantage or observation stays) Restrictive eligibility based on patient diagnosis: originally CHF, COPD, Pneumonia; later CMS granted permission to broaden criteria to include additional diagnoses, age, polypharmacy and social factors Lesson Learned: Cast a wide net Broaden targeting criteria to be all-inclusive 9
10 Tompkins CCTP: Challenges and Lessons Learned Challenge: Patient identification and referral Few referrals among hospital discharge planners Turnover among key hospital staff and leadership No direct access to charts/ medical records Communication of protected health information between partners a challenge Lesson Learned: Embed transitions staff in hospital system Staff credentialing at hospital (this took a champion ) Daily rounds Access to electronic medical records 10
11 Tompkins CCTP: Challenges and Lessons Learned Challenge: Too many cooks Two agencies involved in hospital case finding and inhome coaching Complex communication, information dropped Paid per coaching session: agencies losing money on staff time in rounds Lessons Learned: Streamline Right-size program to one agency 11
12 Tompkins CCTP: Challenges and Lessons Learned Challenge: Patient acceptance of intervention Patients declining intervention in hospital Patients accepting in hospital, declining when home Lesson Learned: Present program as standard part of discharge Schedule home visit while in hospital if possible Utilize same person to introduce program to patient to conduct home visit when possible 12
13 Tompkins CCTP Results Goal: reduce hospital readmissions of Medicare patients by 20% in 2 years Program served 85 patients total Though good results for individual patients, not enough volume to create impact CCTP contract period ended 5/31/14 13
14 14
15 From CCTP to BIP BIP Innovations Fund: NYSDOH Target: Medicaid beneficiaries Goal: To increase access to community-based care options over institutional settings Tompkins submitted application: May, 2014 Notification of grant award: July, 2014 Start of service: Sept
16 Structure of BIP Transitions Program Tompkins County Office for the Aging: lead organization, coordination, reporting. Cayuga Medical Center community hospital Visiting Nurse Service coaching CAP CONNECT clinical integration organization, marketing, outreach, data analytics 16
17 Structure of BIP Transitions Program Studied hospital data on Medicaid readmission patterns In addition to chronic diseases, behavioral health issues, substance abuse, health literacy issues, barriers in accessing community supports Modified model to suit needs of Medicaid patients 17
18 Structure of BIP Transitions Program Modified Coleman approach: 1 or more home visits by an RN with physician s order Importance of medication reconciliation by RN Medicaid-reimbursable service: sustainable after grant period ends Available to ALL Medicaid patients who could benefit Including behavioral health patients Including patients discharged home from 2 large skilled nursing facilities Referrals accepted from community physicians 18
19 Goals of BIP Transitions Program 1) Raise awareness of Transitions Program among clinical partners/referral sources Outreach through CAP Connect 2) Foster case finding and patient introduction to Transitions Program Active involvement at daily rounds by VNS 19
20 Goals of BIP Transitions Program 3) Improve health outcomes and reduce avoidable 30 and 90 day ED visits and inpatient admissions Serve Medicaid beneficiaries with 1+ home visits by Transitions nurse, using modified Coleman approach 4) Ensure program stability beyond grant period Establish referral patterns to ensure program is regularly utilized beyond grant period 20
21 BIP Transitions Program Marketing 21
22 BIP Transitions Program Marketing 22


23 BIP Transitions Program Marketing 23



24 Patient Testimonials Vaness Joanne Andrew Martha 24
25 BIP Transitions Program Implementation 25
26 BIP Transitions Program Results ED Utilization: Number of ED Visits Per Enrollee Through December Days Prior 30 Days Prior 30 Days Post 90 Days Post
27 BIP Transitions Program Results Inpatient Utilization: Number of Inpatient Stays Per Enrollee Through December 90 Days Prior 30 Days Prior 30 Days Post 90 Days Post
28 BIP Transitions Program Results Estimated program savings through December 31st, 2015 ED visits per patient 90 days prior to enrollment = 2.31 ED visits per patient 90 days post enrollment = 1.28 Estimated ED visits prevented = 1.03 visits Number of patients enrolled = 137 Average charges for a Medicaid ED visit* = $ Estimated program savings related to preventable ED visits = $49, *This number based on the average charges for a Medicaid ED visit based on the 2013 Medicaid fee schedule 28
29 BIP Transitions Program Results Estimated program savings through December 31st, 2015 Inpatient admissions per patient 90 days prior to enrollment = 1.24 Inpatient admissions per patient 90 days post enrollment = 0.45 Estimated Inpatient admissions prevented per patient = 0.79 Number of patients enrolled = 137 Average charges for a Medicaid inpatient visit* = $3, Estimated program savings related to preventable inpatient admissions = $324, *This number based on the average charges for a Medicaid inpatient visit based on the 2013 Medicaid fee schedule 29
30 BIP Transitions Program Results Estimated total cost savings from September 2014 through December 31st, 2015: $374,
31 The Future of the Transitions Program Program infrastructure and procedures remain in place Transitions will be the model used for DSRIP Care Transitions project in Tompkins County Program details shared with Care Compass Network for consideration throughout DSRIP PPS. 31
32 VNS Role 1. Pt. Identification & Hospital Visit 2. Home Visits 3. Follow up Phone Calls 4. Referrals to other agencies 5. Integrating techniques to enhance results such as motivational interviewing 32
33 Identification of Medicaid Recipients Access & Review Hospital Census each morning Identify all newly admitted Medicaid patients Review identified patients at hospital rounds and discuss with discharge planning team to identify patients appropriate for the program. 33
34 Approach Medicaid Patient in the hospital about the program It has been determined through the Coleman project that the program is more successful if the same person making the home visits also approaches the patient in the hospital. This begins to develop trust in the relationship and more success in ensuring the home visit. There is usually a 50% acceptance rate. 34
35 Transitions Nurse called discharged patient and set up visit within 3 days of discharge This has been a challenge for the program! Medicaid recipients tend to be more mobile and not as likely to answer their phones or to be reached (or found) after discharge. Early in the program, Transitions RN would visit even if not reached on the phone first usually without success and this practice was stopped. Saw on average, 39% of patients that accepted the program in the hospital. 35
36 Home Visit Based on Four Pillars of CTI 1. Medication self-management 2. Follow-up with PCP/Specialist 3. Knowledge of red flags or warning signs/symptoms and how to respond 4. Patient-centered medical record 36
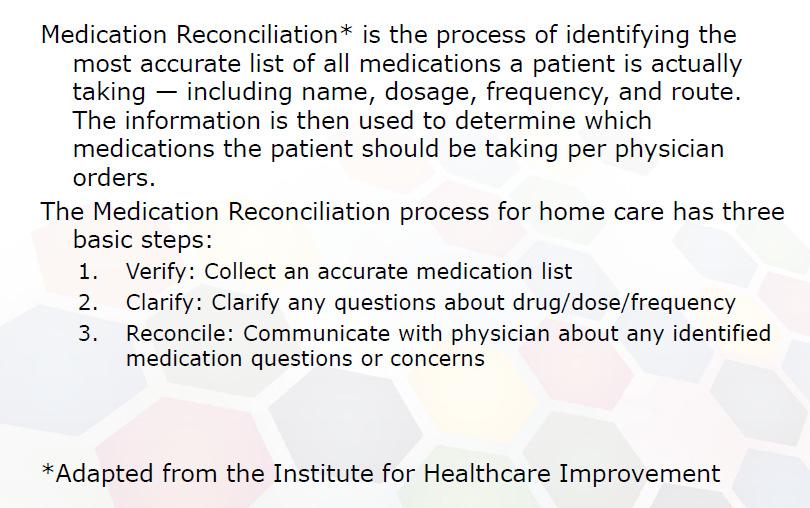
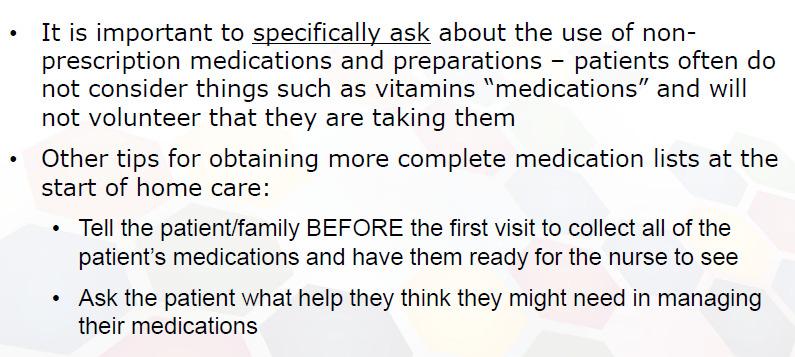
37 MEDICATION RECONCILIATION The key for our project was medication reconciliation by an RN which differed from the Coleman Model which did not require an RN for the coach. 37
38 38
39 39
40 40
41 41
42 42

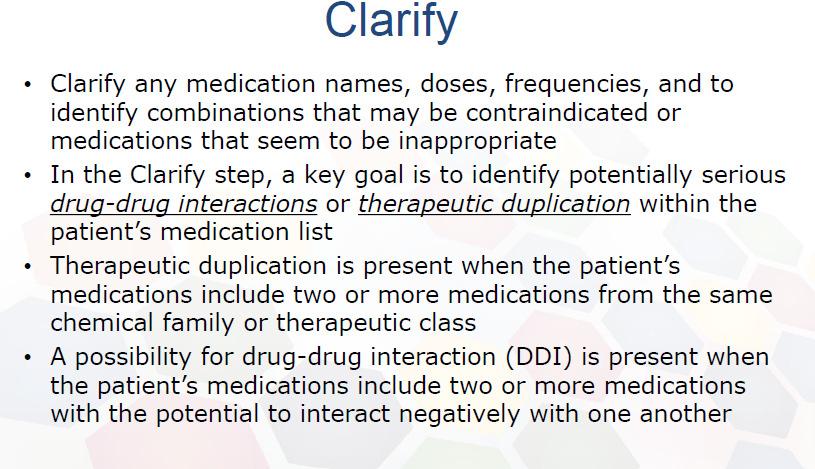
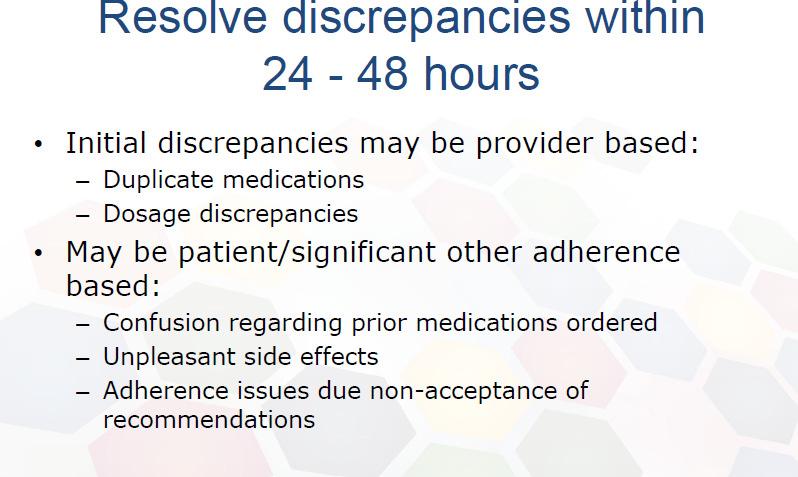
43 used. It is the responsibility of the nurse to Call the physician to reconcile any discrepancies 43
44 44
45 45
46 46
47 47
48 48
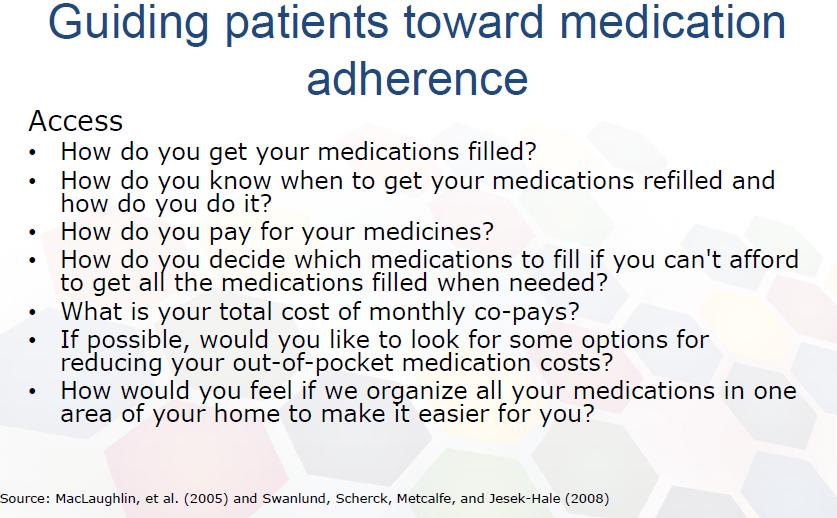
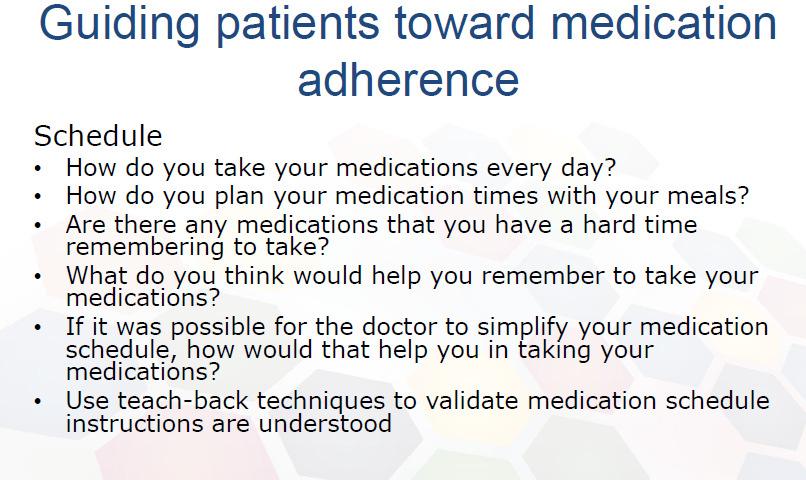
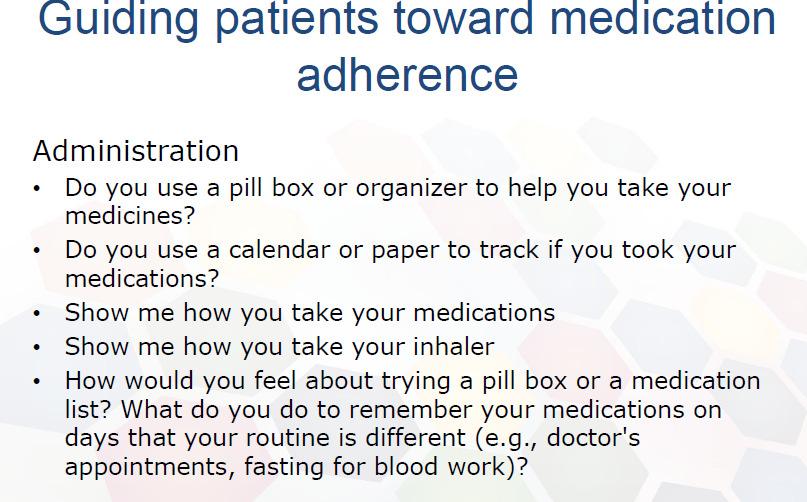
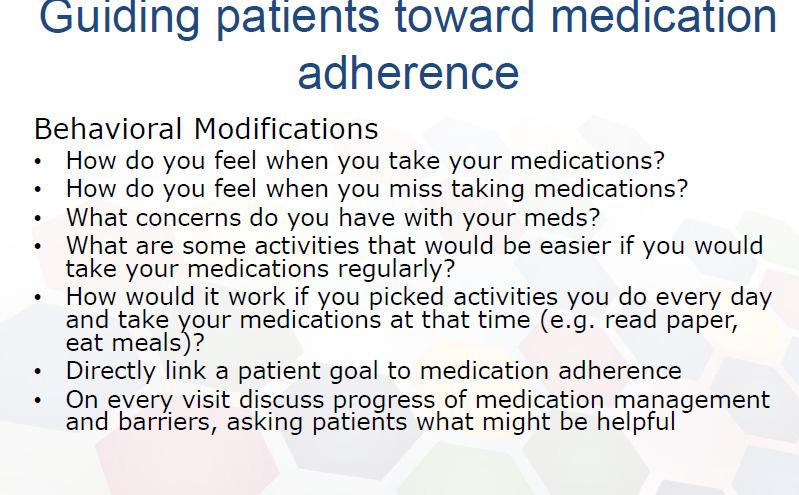
49 Medication Tools for the Patient 49
50 50
51 Steps to assure MD appointment Ascertain whether patient has a follow-up appointment with MD Confirm appropriate MD responsible managing patients Work with patient to schedule the appointment Discuss barriers to appointment including transportation and scheduling with family member, caregiver or friend Confirm/assist with transportation arrangements Provide appointment reminders and work with patient to put appointment information in a convenient place Confirm patient s use of personal health record Use coaching to encourage patient/caregiver to understand importance of scheduling the appointment Confirm that patient understands to take medication list 51


52 Physician Visit 52
53 Knowledge of red flags or warning signs/symptoms and how to respond Red Flags worksheets are disease specific Many free resources to find Red Flags including : 53
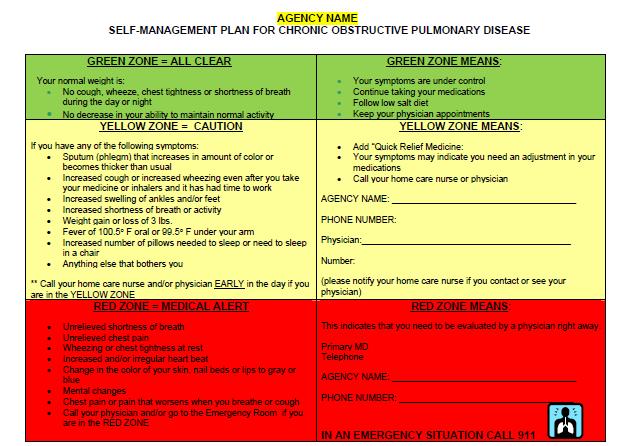
54 Red Flags-COPD 54

55 Red Flags Heart Disease 55

56 Red Flags- High Blood Pressure 56
57 Personal Health Record Booklet given to Patient to take to MD visits. Coach Provides Assistant to complete 57

58 Personal Health Record 58
59 Personal Health Record 59
60 Personal Health Record 60
61 Personal Health Record 61
62 Personal Health Record 62
63 Patient Activation 63

64 Follow Up Phone Calls 64
65 Important Components incorporated into the Program Teach Back Motivational Interviewing Health Literacy 65

66 Teach Back 66
67 Motivational Interviewing Designed to enhance client motivation to change Especially effective for patients that are stuck not making recommended health related behavior changes MI is a directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence MI helps activate the patient s own motivations to change 6 Source: Rollnick, Miller, and ButlerInterview: Motivational ing in Healthcare
68 Motivational Interviewing Collaboration through COACHING: An approach of partnering with patients to enhance self-management strategies for the purpose of preventing exacerbations of chronic illness and supporting lifestyle change (Huffman, 2007, p. 271). 68

69 Motivational Interviewing 69

70 Motivational Interviewing 70

71 Motivational Interviewing 71

72 Health Literacy 72

73 Health Literacy 73

74 Health Literacy 74
75 Resources List of websites to access resources :

76 Questions? 76
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
The Metro Care Transitions Program (CCTP)
") The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
1/11/2016. The Metro Care Transitions Program (CCTP) OUR GOAL OUR HISTORY
 OUR GOAL OUR HISTORY") The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings.
 Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Care Transition Coach
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Thinking Differently about Hospital Readmissions
 Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Exacerbation of Condition. VNAA Best Practice for Home Health
 Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
University of Rochester Medical Center Community Advisory Council
 December 8, 2015 University of Rochester Medical Center Community Advisory Council FLPPS and DSRIP Carol Tegas Executive Director 1 Agenda DSRIP in NYS FLPPS Implementation of DSRIP Vision: Create a Regional
December 8, 2015 University of Rochester Medical Center Community Advisory Council FLPPS and DSRIP Carol Tegas Executive Director 1 Agenda DSRIP in NYS FLPPS Implementation of DSRIP Vision: Create a Regional
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012
 Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
MHS Care Management Program 1017.PR.P.PP.1 10/17
 MHS Care Management Program 1017.PR.P.PP.1 10/17 Sample Integrated Transitional Care Model Inpatient Admission Process Admission thru discharge and beyond Goals: Ensure safe and timely transitions of care
MHS Care Management Program 1017.PR.P.PP.1 10/17 Sample Integrated Transitional Care Model Inpatient Admission Process Admission thru discharge and beyond Goals: Ensure safe and timely transitions of care
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Webinar. Reducing Readmissions with BI and Analytics. 23 March 2018 Copyright 2016 AAJ Technologies All rights reserved.
 Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Evidence Summary for the Care Transitions Program
 Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Transition of Care Model for Inpatient & Observation Units
 V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Recommendations for Transitions of Care in North Carolina
 Recommendations for Transitions of Care in North Carolina FINAL REPORT June 30, 2014 Revised, July 31, 2014 Submitted to: North Carolina Office of Rural Health and Community Care 311 Ashe Avenue Raleigh,
Recommendations for Transitions of Care in North Carolina FINAL REPORT June 30, 2014 Revised, July 31, 2014 Submitted to: North Carolina Office of Rural Health and Community Care 311 Ashe Avenue Raleigh,
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Assessment. SMP Foundations Training Kit. Table of Contents
 SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Hospice Discharges. Legacy Hospice
 Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
THE UTILIZATION OF MODELS OF CARE TRANSITION TO REDUCE MEDICARE BENEFICIARIES HOSPITAL READMISSION RATES IN KENTUCKY: A CASE STUDY
 THE UTILIZATION OF MODELS OF CARE TRANSITION TO REDUCE MEDICARE BENEFICIARIES HOSPITAL READMISSION RATES IN KENTUCKY: A CASE STUDY CAPSTONE PROJECT PAPER A paper submitted in partial fulfillment of the
THE UTILIZATION OF MODELS OF CARE TRANSITION TO REDUCE MEDICARE BENEFICIARIES HOSPITAL READMISSION RATES IN KENTUCKY: A CASE STUDY CAPSTONE PROJECT PAPER A paper submitted in partial fulfillment of the
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
Collaborative Care- Bridging the Gap in Healthcare
 Collaborative Care- Bridging the Gap in Healthcare Ron Emerson RN BSN, Global Director of Healthcare Polycom, Inc. All rights reserved. Unnecessary Hospital Readmissions The Accountable Care Act mandated
Collaborative Care- Bridging the Gap in Healthcare Ron Emerson RN BSN, Global Director of Healthcare Polycom, Inc. All rights reserved. Unnecessary Hospital Readmissions The Accountable Care Act mandated
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Chronic Care Management INFORMATION RESOURCE
 Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER
 PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no
 None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no commercial support for this CME activity RIVERSIDE COUNTY
None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no commercial support for this CME activity RIVERSIDE COUNTY
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
kaiser medicaid and the uninsured commission on O L I C Y
 P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Community Health Needs Assessment Three Year Summary
 Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.