The journey of RAID through evolution
|
|
|
- Hannah Katherine Snow
- 5 years ago
- Views:
Transcription
1 The journey of RAID through evolution George Tadros Consultant in Old Age Liaison Psychiatry, RAID Lead Clinician, Birmingham, UK Professor of Old Age Liaison Psychiatry, Warwick Medical School, University of Warwick Visiting Professor of Mental Health and Ageing, Staffordshire University Vice-Chair, faculty of Old Age Psychiatry, Royal College of Psychiatry
2 Recent evidence: Older People Up to 70% of hospital beds are occupied by older people. 70% of older people referrals to liaison services are not under the care of mental health services. 500beds hospital would have 5,000 admissions/annum, of whom 3,000 will have or will develop a mental disorders , hospital stay for increased by 50%, over 75 by 66%. In a typical acute hospital (500 beds), failure to organize dementia liaison services leads to excess cost of 6m/year The majority of mental co-morbidity in acute hospital affecting older people is due to three disorders: Dementia, Depression and Delirium. Dementia CQUIN (FAR) Mental disorder in older adults is a predictor of: Increased LOS Increased readmissions Increased Institutionalism (impacting on performance and efficiency) Other poorer outcomes
3 Evidence for need: Alcohol and Substance Misuse 88% of adults in the UK drink alcohol, with 38% of men and 16% of women recognized as having an alcohol use disorder 12% of A&E attendances are alcohol related 7-20% acute admissions have alcohol problems Annual healthcare cost of 1.7 billion RAID Research at Hospital front door (AMU) April 2013 Used MUST-G Findings: Hospital identify that 1% of elderly admissions have alcohol related problems, using FAST. Our research team using MUST-G identified 18% of older people coming to AMU have alcohol related problems
4 Evidence for Need: General Psychiatry 25% of patients with a physical illness also have a mental health condition. 60% of over 60s A&E work is primarily with younger people coming with DSH, Alcohol problems and acute psychosis. Depression & Anxiety - 2 to 3 times more common in those with physical long-term illness. Neuropsychiatry Postnatal psychiatry Eating disorders MUPS: long term disability and dissatisfaction. Present in most hospital specialities. Care costs estimated at 3.1 billion per annum
5 Traditional Models of Liaison Psychiatry Consultant led, consultant sessions Nurse led service Service provided from mental health base. Outward referrals 9:00 5:00, 8:00 8:00!! services Weekdays, weekends!! Out of hours support Food for thoughts. Is RAID Liaison psychiatry? How RAID is different from Liaison Psychiatry?
6 The product: Rapid Assessment Interface Discharge 24x7 Service BOUNDARY FREE RAPID RESPONSE TRAINING RAID SINGLE POINT OF CONTACT COMMUNITY FOCUS EARLY INTERVENTION
7 The upgraded RAID service (cost 1.4m) Consultant Psychiatrist Mental Health of Older People Consultant Psychologist Mental Health of Older People RAID Team Manager Consultant Liaison Psychiatrist Currently Funded Consultant Psychiatrist Substance Misuse Band 7 Nurse MHOP Currently Funded Specialist Doctor Specialist Doctor Band 7 Social Worker Currently Funded Band 7 Nurse Liaison Currently Funded Lead Nurse Substance Misuse Band 6 Nurse MHOP Currently Funded Band 6 Nurse MHOP Currently Funded Band 6 Nurse MHOP Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Substance misuse Currently Funded Assistant Research Psychologist Admin Band4 Admin Band4
8 The upgraded RAID service (cost 1m) Consultant Psychiatrist Mental Health of Older People Consultant Liaison Psychiatrist Clinical psychologist/ Band 8 or above Team Manager Band 8a Band 7 Nurse MHOP Currently Funded Physician Assistance FY1 or CT1 or SpR Band 7 Nurse Liaison Currently Funded Band 6 Nurse MHOP Currently Funded Band 6 Nurse MHOP Currently Funded Band 6 Nurse MHOP Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Liaison Currently Funded Band 6 Nurse Substance misuse Assistant Research Psychologist Admin Band4 Admin Band4
9 RAID evaluation RESPONSE QUALITY COST
10 Referrals Origin of referral Number of referrals years 65 years + Mean age Accident and Emergency (A&E) Poisons Unit Wards % 4% 36.4 years % 4% 34.6 years % 59% 65.6 years Steadily increasing referrals 350+ monthly referrals (goes up to 700 referral/month at QEHB) Only 30% patients known prior to RAID.


11 Top 7 reasons for referral Drug misuse 4% Dementia/ Confusion 18% Anxiety 6% Deliberate self harm 32% Psychosis 9% Alcohol misuse 13% Depression 18% Deliberate self harm Depression Alcohol misuse Psychosis Dementia/ Confusion Drug misuse Anxiety


12 A&E Response Not Assessed; 3% Not Recorded; 17% Targets Met Targets Not Met Not Assessed Not Recorded Targets Not Met; 7% Targets Met; 73%

13 Ward Response Target Not Met; 10% Not Assessed; 1% Not Recorded; 6% Target Met Target Not Met Not Assessed Not Recorded Target Met; 83%


14 Teaching and evaluation 158 hospital staff trained: All completed the evaluation Very poor; 0% Poor; 0% Neutral; 3% Good; 36% Very poor Poor Neutral Good Excellent Excellent; 61% A lovely insight from a very experienced practitioner


15 Patient satisfaction: Feedback Very poor to poor rating; 8% Neither poor nor good rating; 8% Very poor to poor rating Neither poor nor good rating Good to excellent rating Good to excellent rating; 84% Range Mode Median Mean 0 to


16 Staff satisfaction: Feedback Referral to other services; 8% Other; 5% Liaison with other services; 7% Providing information to patient; 10% Advice on managing patients; 12% Advice on medication; 11% Support to family/carers; 17; 8.17% Support of staff; 11% Education; 7% Information sharing; 7% Support to patient; 10% Signposting; 4% Range Mode Median Mean 2.5 to
17 Savings and wider financial Benefits Potential Benefits of RAID Social care Outcomes Considered in this Study Complaints Patient satisfaction Staff sickness Staff satisfaction Acute staff confidence in dealing with MH conditions 1. Inpatient LoS A&E savings Demand for community MH services 2. Readmission rates 3. Admission avoidance Discharge destination MH outcomes SUIs Quality Acute staff training Security Referring / Signposting to community MH services
18 3 Groups for the study!! 1. Pre- RAID group (control group) December July 2009 No changes/confounders between pre and post!! 2. RAID_ influence group December July 2010 RAID did not see patients, but had influence through training and support 3. RAID group December July 2010 RAID patients Matched groups: Matched age, gender, mental health code, medical diagnosis, healthcare resource group (HRG) RAID patients were the most complex RAID: average 9 different diagnostic codes RAID_ influence 3 different diagnostic codes

 Mean: 9.")
19 case-by-case Matched Control Study Sub Control mean: 8.4 Sub RAID Inf mean: 5.2 Sub Control mean: 10.3 Sub RAID mean: cases 72 cases Control (2873 Patient) Mean: 9.3 days RAID Influence (2654 Patient) Mean: 4.74 RAID (886 Patient) Mean: 17.6

20 Length of stay: Comparing the groups P value= 0.01
21 Cost savings: LOS/ all age groups All ages: Saving over 8 months= ,493 = 9,290 bed days Saving over 12 months= 13,935 bed days Per day= 13, = 38 beds per day Older people only: Saving over 8 months= ,220 = 8,634 bed days Saving over 12 months= 12,951 bed days Per day= 12, = 35 beds per day
22 2. Admission Avoidance at MAU: Cohort control study All ages Control group; 30% of avoided admission at MAU. RAID and RAID influence group; 33% avoided admission at MAU Increase of 9% Older people Control group; 17% of avoided admission at MAU. RAID and RAID influence group; 25% avoided admission at MAU Increase of 47% Average LOS= 9.3 days 240X9.3= 2,232 bed days = 6 beds/ day Average LOS= 22 days 111 X 22= 2442 bed days = 6 beds/ day


23 3. Elderly Patient Discharge Destination 30% of elderly patients who come to acute hospitals from their own homes are discharged to care homes (national figures) LSE estimated savings to our wider economy of 60,000/week (Social care cost).
24 4. Savings: Re-admission Group Re-admission per 100 patients Retrospective (3500) 15 (505) Partial RAID (3200) 12 (408) RAID (850) 4 (42)
25 Savings: through increasing survival The savings calculated from survival assumes patients readmission at same rate of retrospective patients Over 8 months 1200 admissions saved. Over 12 months 1800 admissions saved. Saving 22 beds per day = one ward Saving 20 beds per day comes out of elderly care wards.
26 Combined total savings: beds/day On reduced LOS saved bed days/12 months= 13,935 bed days 365 = 38 days/day (35 beds/day for the elderly) Saved bed days through avoiding admissions at MAU Saved bed days = 6 beds / day Elderly.. = 6 beds Increasing survival before another readmission Admissions saved over 12 months =1800 admissions Average LOS 4.5 days = 8100 saved bed days 365 = 22 beds/day 20 for the elderly Total Saved beds every day = = 66 bed/ day (Maximum) {Elderly: 59 beds/day} = = 49 bed days (minimum) {Elderly: 42 beds/ day} 2010: City Hospital has already closed 60 beds.
27 London school of Economics, August 2011 Very thorough, detailed and vigorous review but conservative estimation Total savings: 3.55 million to NHS At least 44 beds/day 60,000/week to social care cost Money value Cost : return = 1: 4 Recommended the model to NHS confederation RAID expanded in Birmingham to 5 acute hospitals across three acute Trust, 3600 beds Now RAID is being implemented in over 20 trusts across the country.
28 RAID+ Vs RAID A New RAID Model at MAU 1. What if we move RAID to the hospital front doors? 2. Does early screening improve patients outcomes? 3. Is RAID early intervention (RAID+) more cost effective than RAID? MAU Discharge effect Comparing current RAID with RAID+ MAU screening LOS, RA rates, Discharge destination
29 Number of patients with a Mental Health Diagnosis Dementia Delirium and Depression (Retrospective case notes and Screened patients

30 RAID Screening - Groups Screened ve Screened ve Screened 421 Clinical Filter + ve Filter ~ ve Filter ~200 Referred to RAID 135 Not Referred to RAID ~86 + ve RAID ~105 - ve RAID ~30

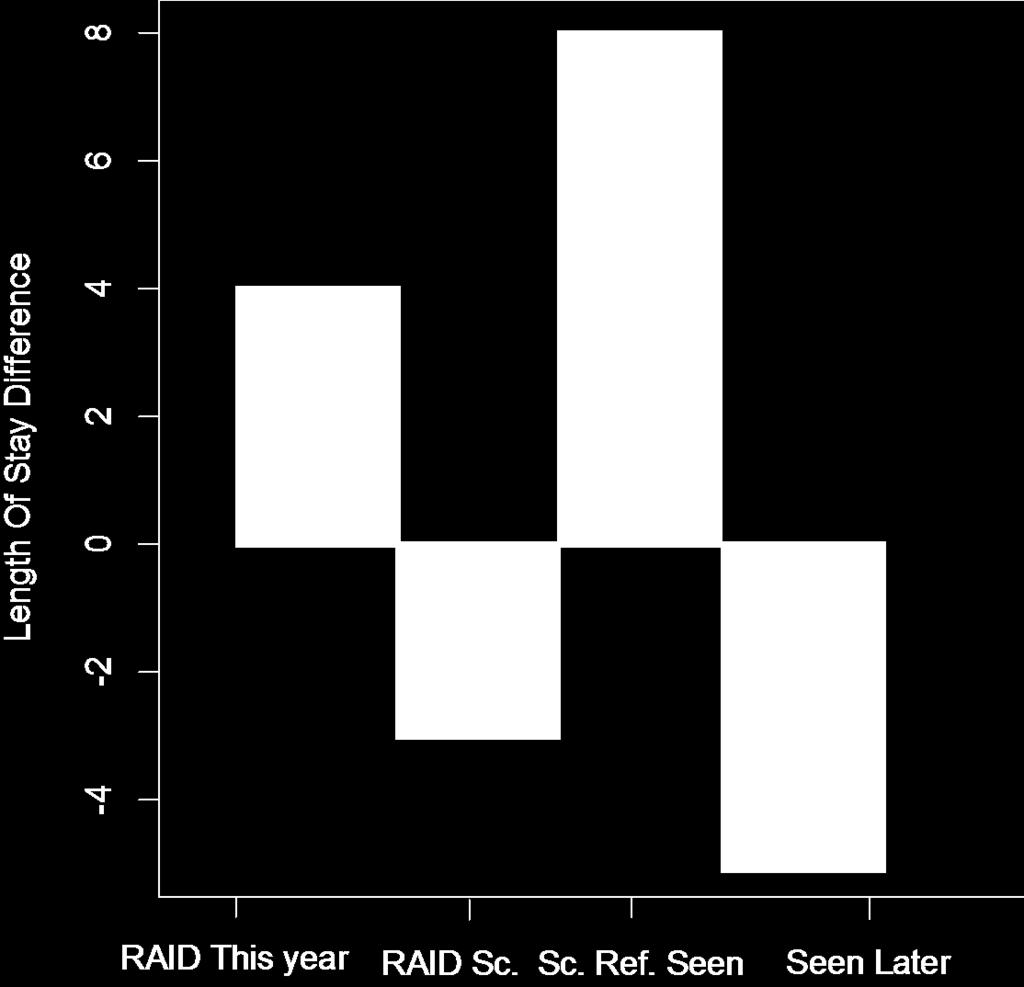
31 Length of Stay
32
33 New RAID research findings Length of stay: Screened by RAID+ at MAU reduces LOS on average by extra 4 days comparing to RAID Readmissions: Hazard Ratio for Referred patients is 0.64, p-value Patients referred and seen by RAID stays in the community 35% more than patient not referred by RAID Creating new screening tool
34 Independent RAID Financial Evaluation by Central Midlands CSU Led by : Steven Wyatt Rapid Assessment Interface And Discharge Liaison Economic Evaluation of the Birmingham and Solihull Roll-Out October 2012
35 Data Sources and Data Flows BSMHFT CM CSU Collate data on RAID contacts*; NHS Number Date Setting Match to SUS A&E and IP tables and collate identifiers (not PI) of relevant attendances and admissions Locate these attendances and admissions in local SUS and national HES tables
36 Wider Potential Benefits Potential Benefits of RAID Outcomes Considered in this Study Inpatient LoS A&E reattendance rates Time in A&E Readmission rates Admission rates fro A&E Time to readmission Acute Prov / Comm Social care Security Complaints Patient satisfaction Staff sickness Discharge destination Quality Staff satisfaction Acute staff confidence in dealing with MH conditions Demand for community MH services SUIs Acute staff training Referring / Signposting to community MH services MH outcomes
37 A&E Activity Outcomes Concurrent Controls Outcome Cases Controls Admission from A&E 13.7% 22.4% Difference (95% CI) 8.7% (6.8% %) Notes Sig. at 99% Average Duration in A&E 4h 20m 2h 43m 97m (83m 111m) Sig. at 99% Average Number of Reattendances within 28 days* (0.40 to 0.61) Sig. at 99% Average Number of Reattendances within 90 days* (0.57 to 0.78) Sig. at 99% * Applies to subset of cases seen between July 2012 and November 2012
38 A&E Financial Outcomes Concurrent Controls Commissioner Cost Provider Cost Cases Controls Cases Controls All % 22% 14% 22% Admitted % 91% 90% 90% Located & Costed ,615 Cost 286, , , , Grossed -Up Cost 319, , , ,505 Difference -498, ,875
39 Inpatient Activity Outcomes Concurrent Controls Outcome Cases Controls Difference (95% CI) Notes Average Length of Stay Days (0.5 to 0.7) Sig. at 99% Average Number of Readmissions within 28 days* (-0.01 to -0.05) Sig. at 99% Average Number of Readmissions within 90 days* (0.04 to 0.13) Sig. at 99% * Applies to subset of cases seen between July 2012 and November 2012.
40 Inpatient Financial Outcomes Concurrent Controls Commissioner Cost Provider Cost Cases Controls Cases Controls All* 33,750 33,750 33,750 33,750 93,1% 93.1% 93.1% 93.1% Matched 31,414 31,414 31,414 31, % 99.0% 99.6% 99.6% Located & Costed 31,093 31,093 31, ,238 Cost 50,656,320 52,162,644 65,110,245 70,042,352 Difference 1,506,323 4,923, Grossed-Up Difference 1,635,107 5,318,846 * To avoid double counting, this number excludes cases seen by RAID in AE and then admitted
41 Financial Outcomes Summary Concurrent Controls Full Tariff / Average Cost ( 000s) A&E Inpatient Grossed- Up Total* Savings Share Marginal ( 000s) Commissioner Saving 498 1,635 2,133 36% 640 Provider Spend ,319-5,892 Income ,635-2,133 Saving 74 3,684 3,758 64% 1,127 Total Saving 5,892 1,768 Full Costs 3,295 Incremental Cost 1,976 Saving / Incremental Cost
42 Activity Outcomes by Site Site Admission via A&E Length of Stay cases controls diff cases controls diff Heartlands 14.3% 28.7% -14.4% Good Hope 19.4% 29.2% -9.8% Solihull 20.2% 11.2% +9.0% City 11.4% 17.3% -5.9% UHB 10.9% 19.1% -8.2% All 13.7% 22.4% -8.7%
43 Financial Outcomes by Site ( 000s) All HoEFT City UHB Full Cost 3,295 1, Incremental Cost 1, Commissioner Savings AE Provider Savings AE Commissioner Savings IP -1,635-1, Provider Savings IP -3,684-3,161-1, Total Savings -5,892-5,008-1, Net Savings (@ full cost) -2,597-3, ,347 Net Savings (@ incremental cost) -3,916-4, ,062 Savings / Full Cost Savings / Incremental Cost
44 Conclusions - Activity Primary Activity Outcomes Patients seen by RAID in A&E were significantly less likely to be admitted than controls. Patients seen by RAID on inpatient wards had a significantly lower average length of stay than controls. Secondary Activity Outcomes Patients seen by RAID in A&E spent significantly more time in the department than controls and were more likely to reattend with 28 and 90 days. Financial savings: Savings associated with reduced acute utilisation were 3 times greater than the incremental cost of the RAID Service if commissioner costs are calculated at full tariffs and providers costs are calculated at the average reference costs. 64% of these savings fell to providers and 36% to commissioners. Most of the savings came as a result of reducing lengths of stay rather than admission avoidance.
The. British Psychological. Society. Society. Prof Jamie Hacker Hughes CPsychol CSci FBPsS. President, British Psychological Society
 British Psychological Society The British Psychological Society Prof Jamie Hacker Hughes CPsychol CSci FBPsS President, British Psychological Society Psychology and Psychiatry in Liaison Numbers with LTCs
British Psychological Society The British Psychological Society Prof Jamie Hacker Hughes CPsychol CSci FBPsS President, British Psychological Society Psychology and Psychiatry in Liaison Numbers with LTCs
The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class
 Driving Improvement along Emergency Care Pathways: A Master Class") The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class WORKSHOP INFORMATION Morning Workshops (Workshops 1-4) Delegates have a choice of two
The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class WORKSHOP INFORMATION Morning Workshops (Workshops 1-4) Delegates have a choice of two
Liaison Can Improve The Care In Care Homes And General Hospitals. Joanne Hirst
 Liaison Can Improve The Care In Care Homes And General Hospitals Joanne Hirst Service Model Older Peoples Liaison Service Care Homes General Hospital The case for Need 1/3 of people with dementia live
Liaison Can Improve The Care In Care Homes And General Hospitals Joanne Hirst Service Model Older Peoples Liaison Service Care Homes General Hospital The case for Need 1/3 of people with dementia live
The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond
 The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond Thames Valley Strategic Clinical Networks February 2015 Table of Contents Introduction & Context pp 3-11 SCN recommendations
The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond Thames Valley Strategic Clinical Networks February 2015 Table of Contents Introduction & Context pp 3-11 SCN recommendations
Review of Mental Health Liaison Services in the South West of England. June 2013
 Review of Mental Health Liaison Services in the South West of England June 2013 1 Strategic Clinical Network (South West) Mental Health, Dementia, Neurological Conditions Commissioning Liaison Psychiatry/Mental
Review of Mental Health Liaison Services in the South West of England June 2013 1 Strategic Clinical Network (South West) Mental Health, Dementia, Neurological Conditions Commissioning Liaison Psychiatry/Mental
briefing Liaison psychiatry the way ahead Background Key points November 2012 Issue 249
 briefing November 2012 Issue 249 Liaison psychiatry the way ahead Key points Failing to deal with mental and physical health issues at the same time leads to poorer health outcomes and costs the NHS more
briefing November 2012 Issue 249 Liaison psychiatry the way ahead Key points Failing to deal with mental and physical health issues at the same time leads to poorer health outcomes and costs the NHS more
PACT Patient experience and Anticipatory Care Planning Team. Dr Eleanor Halloran Consultant Liaison Psychiatrist Edinburgh
 PACT Patient experience and Anticipatory Care Planning Team Dr Eleanor Halloran Consultant Liaison Psychiatrist Edinburgh Project proposers Dr David Caesar Dr Carl Bickler Clinical Director GP Clinical
PACT Patient experience and Anticipatory Care Planning Team Dr Eleanor Halloran Consultant Liaison Psychiatrist Edinburgh Project proposers Dr David Caesar Dr Carl Bickler Clinical Director GP Clinical
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
PRISM: GPs - your questions answered
 PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
2015/16 CQUIN Schemes
 Barnet, Enfield & Haringey Mental Health Trust 2015/16 CQUIN Schemes Version: 3.0 Version Date Revision Author 1.0 30/03/15 Excel to Word Document A Bland 2.0 01/04/15 1 st Discussion with BEHMHT A Bland
Barnet, Enfield & Haringey Mental Health Trust 2015/16 CQUIN Schemes Version: 3.0 Version Date Revision Author 1.0 30/03/15 Excel to Word Document A Bland 2.0 01/04/15 1 st Discussion with BEHMHT A Bland
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
A New Model of Urgent and Emergency Mental Health Care
 A New Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Dr Paul Brown- Consultant Psychiatrist, Sunderland
A New Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Dr Paul Brown- Consultant Psychiatrist, Sunderland
Mental Health: What The Data Tells Us. Stephen Watkins and Zoë Page
 1 Mental Health: What The Data Tells Us Stephen Watkins and Zoë Page Overview NHS Benchmarking Network Acute pathway Community based care Workforce Economics Discussion points NHS Benchmarking Network
1 Mental Health: What The Data Tells Us Stephen Watkins and Zoë Page Overview NHS Benchmarking Network Acute pathway Community based care Workforce Economics Discussion points NHS Benchmarking Network
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
GE1 Clinical Utilisation Review
 GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
Academic Health Science Network for the North East and North Cumbria Mental Health Programme. Elaine Readhead AHSN NENC Mental Health Programme Lead
 Academic Health Science Network for the North East and North Cumbria Mental Health Programme Elaine Readhead AHSN NENC Mental Health Programme Lead Background No health without mental health Five Year
Academic Health Science Network for the North East and North Cumbria Mental Health Programme Elaine Readhead AHSN NENC Mental Health Programme Lead Background No health without mental health Five Year
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Managing deliberate self-harm in young people
 Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE OVER A SIX YEAR PERIOD ( )
") The British Journal of Developmental Disabilities Vol. 54, Part 2, JULY 2008, No. 107, pp. 89-99 A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE
The British Journal of Developmental Disabilities Vol. 54, Part 2, JULY 2008, No. 107, pp. 89-99 A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE
PICU and Acute Services Psychiatric Intensive Care and Acute services
 PICU and Acute Services Psychiatric Intensive Care and Acute services All of our services have 24 hour medical cover and admissions can occur 24-hours-a-day Introduction As a national provider of specialist
PICU and Acute Services Psychiatric Intensive Care and Acute services All of our services have 24 hour medical cover and admissions can occur 24-hours-a-day Introduction As a national provider of specialist
Background to HoNOS (extract from Trust website) Page 2. How to Rate HoNOS Page 2. The Mental Health Clustering Tool Page 3
 Page 2. How to Rate HoNOS Page 2. The Mental Health Clustering Tool Page 3") HOW TO..HoNOS and RiO Contents: Background to HoNOS (extract from Trust website) Page 2 How to Rate HoNOS Page 2 The Mental Health Clustering Tool Page 3 How to use HoNOS process flow For teams using RiO
HOW TO..HoNOS and RiO Contents: Background to HoNOS (extract from Trust website) Page 2 How to Rate HoNOS Page 2 The Mental Health Clustering Tool Page 3 How to use HoNOS process flow For teams using RiO
New Savoy Conference Psychological Therapies in the NHS
 New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
Commissioning for quality and innovation (CQUIN): 2014/15 guidance. February 2014
: 2014/15 guidance. February 2014") Commissioning for quality and innovation (CQUIN): 2014/15 guidance February 2014 1 NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning
Commissioning for quality and innovation (CQUIN): 2014/15 guidance February 2014 1 NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning
The Community Crisis House model
 An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
OUTLINE PROPOSAL BUSINESS CASE
 OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE
 DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
Frail Elderly Assessment Unit (FEAU)
") Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
Improving Mental Health Services in South Gloucestershire
 Improving Mental Health Services in South Gloucestershire Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers Information
Improving Mental Health Services in South Gloucestershire Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers Information
Mental Health Crisis Care: The Five Year Forward View. Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust
 Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
Liaison Psychiatry Services National Overview of Services 2010
 Liaison Psychiatry Services National Overview of Services 2010 The Royal College of Psychiatrists has described Liaison psychiatry as the subspecialty which provides psychiatric treatment to patients attending
Liaison Psychiatry Services National Overview of Services 2010 The Royal College of Psychiatrists has described Liaison psychiatry as the subspecialty which provides psychiatric treatment to patients attending
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals. The Pennine Acute Hospitals NHS Trust
 Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
A Model of Urgent and Emergency Mental Health Care
 A Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Kate Chartres, Nurse Consultant, Psychiatric Liaison,
A Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Kate Chartres, Nurse Consultant, Psychiatric Liaison,
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
Statement of purpose. Health and Social Care Act 2008
 Statement of purpose Health and Social Care Act 2008 Registered address Bethlem Royal, Monks Orchard Road, Beckenham BR3 3BX Contact details Switchboard t: 020 3228 6000 Patient Advice and Liaison Service
Statement of purpose Health and Social Care Act 2008 Registered address Bethlem Royal, Monks Orchard Road, Beckenham BR3 3BX Contact details Switchboard t: 020 3228 6000 Patient Advice and Liaison Service
Actions Required. Page 1 of 7
 Action Plan Mr A Rec Summary of Report Recommendation 1 and the future commissioning body responsible should ensure that any patient with epilepsy who has a psychotic episode, irrespective of apparent
Action Plan Mr A Rec Summary of Report Recommendation 1 and the future commissioning body responsible should ensure that any patient with epilepsy who has a psychotic episode, irrespective of apparent
Ambulatory emergency care Reimbursement under the national tariff
 HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Urgent and emergency mental health care pathways
 Urgent and emergency mental health care pathways Initial guidance for improving data quality in the Mental Health Services Dataset (MHSDS) Published August 2018 Copyright 2018 NHS Digital Contents Who
Urgent and emergency mental health care pathways Initial guidance for improving data quality in the Mental Health Services Dataset (MHSDS) Published August 2018 Copyright 2018 NHS Digital Contents Who
Welcome to. Northern England and the Five Year Forward View for Mental Health. Thursday 2 February 2017 at the Radisson Blu, Durham
 Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Long-Stay Alternate Level of Care in Ontario Mental Health Beds
 Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
A&E Clinical Quality Indicators June 2013
 A&E Clinical Quality Indicators June 2013 (RJE) Initial Assessment Treatment Total time in A&E Patient arrives in A&E 1.1 95% of patients waited under 17 minutes from arrival to initial assessment 1.2
A&E Clinical Quality Indicators June 2013 (RJE) Initial Assessment Treatment Total time in A&E Patient arrives in A&E 1.1 95% of patients waited under 17 minutes from arrival to initial assessment 1.2
Secure care services: Medium secure services for men and women at Ardenleigh, Reaside Clinic and Tamarind Centre
 Birmingham and Solihull Mental Health NHS Foundation Trust Secure care services: Medium secure services for men and women at Ardenleigh, Reaside Clinic and Tamarind Centre Secure care services Commissioners
Birmingham and Solihull Mental Health NHS Foundation Trust Secure care services: Medium secure services for men and women at Ardenleigh, Reaside Clinic and Tamarind Centre Secure care services Commissioners
Key facts and trends in acute care
 Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB)
") ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB) NOTICE OF INTENT TO CONTRACT (NIC) FOR ADMINISTRATIVE SERVICES ONLY (ASO) FOR HEALTH MAINTENANCE ORGANIZATION PLAN
ADDENDUM #1 STATE OF LOUISIANA DIVISION OF ADMINISTRATION OFFICE OF GROUP BENEFITS (OGB) NOTICE OF INTENT TO CONTRACT (NIC) FOR ADMINISTRATIVE SERVICES ONLY (ASO) FOR HEALTH MAINTENANCE ORGANIZATION PLAN
Worcestershire Early Intervention Service. Operational Policy
 Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Our Journey to Discharge to Assess (D2A)
") Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg
Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Suicide Among Veterans and Other Americans Office of Suicide Prevention
 Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
Mental Health Supported Housing Context and Analysis. 30 th March 2015
 Mental Health Supported Housing Context and Analysis 30 th March 2015 Overview Background and context Supported Housing provision Acute mental health demand Community mental health services demand Costs
Mental Health Supported Housing Context and Analysis 30 th March 2015 Overview Background and context Supported Housing provision Acute mental health demand Community mental health services demand Costs
Process and definitions for the daily situation report web form
 Process and definitions for the daily situation report web form November 2017 The daily situation report (sitrep) indicates where there are pressures on the NHS around the country in areas such as breaches
Process and definitions for the daily situation report web form November 2017 The daily situation report (sitrep) indicates where there are pressures on the NHS around the country in areas such as breaches
PSYCHIATRY OF OLDER ADULTS
 GP Specialty Training Programme PSYCHIATRY OF OLDER ADULTS GP Curriculum As this forms part of a GP Specialty Training Programme it is important that GPStRs work towards the learning objectives of the
GP Specialty Training Programme PSYCHIATRY OF OLDER ADULTS GP Curriculum As this forms part of a GP Specialty Training Programme it is important that GPStRs work towards the learning objectives of the
Seven day hospital services: case study. University Hospital Southampton NHS Foundation Trust
 Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
PHFT Building Voluntary working with the Voluntary Sector. Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset
 PHFT Building Voluntary working with the Voluntary Sector Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset WE ARE ALL BUSY! Emergency Attendances Emergency Admissions GP Admissions
PHFT Building Voluntary working with the Voluntary Sector Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset WE ARE ALL BUSY! Emergency Attendances Emergency Admissions GP Admissions
The future of mental health: the Taskforce 5 year forward view and beyond
 The future of mental health: the Taskforce 5 year forward view and beyond May 2016 Content Mental Health Taskforce Overview Achieving Better Access Safe, Effective and Compassionate Care Integrating Physical
The future of mental health: the Taskforce 5 year forward view and beyond May 2016 Content Mental Health Taskforce Overview Achieving Better Access Safe, Effective and Compassionate Care Integrating Physical
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Integrated Intelligence and system modelling in Kent
 Integrated Intelligence and system modelling in Kent Dr Abraham P George Consultant / Asst Dir in Public Health abraham.george@kent.gov.uk Today s presentation Context and objectives Public Health Kent
Integrated Intelligence and system modelling in Kent Dr Abraham P George Consultant / Asst Dir in Public Health abraham.george@kent.gov.uk Today s presentation Context and objectives Public Health Kent
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Next Steps on the NHS Five Year Forward View
 Next Steps on the NHS Five Year Forward View easy read About this document This document uses easy words and pictures. You might want to read through it with someone else to help you to understand it more.
Next Steps on the NHS Five Year Forward View easy read About this document This document uses easy words and pictures. You might want to read through it with someone else to help you to understand it more.
Getting the Right Response In A Mental Health Crisis
 Getting the Right Response In A Mental Health Crisis Imagine someone you knew suddenly experienced a mental health crisis What response are you able to provide at the moment? What are the barriers in your
Getting the Right Response In A Mental Health Crisis Imagine someone you knew suddenly experienced a mental health crisis What response are you able to provide at the moment? What are the barriers in your
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Compassionate Carers / Compassionate Employers
 Compassionate Carers / Compassionate Employers H E F T IN PARTNERSHIP W I T H THE D Y I N G M A T T E R S C O A L I T I O N D R D A W N C H A P L I N - H E A D N U R S E P A T I E N T E X P E R I E N C
Compassionate Carers / Compassionate Employers H E F T IN PARTNERSHIP W I T H THE D Y I N G M A T T E R S C O A L I T I O N D R D A W N C H A P L I N - H E A D N U R S E P A T I E N T E X P E R I E N C
5. ADULT MENTAL HEALTH PLANNING FRAMEWORK. 5.1 Analysis of Local Position
 5. ADULT MENTAL HEALTH PLANNING FRAMEWORK 5.1 Analysis of Local Position 5.1.1 The Joint Planning, Performance & Implementation Group (JPPIG) in Renfrewshire has lead responsibility for planning of Adult
5. ADULT MENTAL HEALTH PLANNING FRAMEWORK 5.1 Analysis of Local Position 5.1.1 The Joint Planning, Performance & Implementation Group (JPPIG) in Renfrewshire has lead responsibility for planning of Adult
Transforming the Discharge Process Carol Jagpal Clinical Manager Complex Discharge Team QEHB
 Transforming the Discharge Process Carol Jagpal Clinical Manager Complex Discharge Team QEHB Background Queen Elizabeth Hospital Birmingham has 1400 beds, 32 operating theatres and a100 bed critical care
Transforming the Discharge Process Carol Jagpal Clinical Manager Complex Discharge Team QEHB Background Queen Elizabeth Hospital Birmingham has 1400 beds, 32 operating theatres and a100 bed critical care
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Seven Day Working: in Practice Clinicians Perspective. Jonathan Vickers Consultant surgeon Dec 2015
 Seven Day Working: in Practice Clinicians Perspective Jonathan Vickers Consultant surgeon Dec 2015 Why me? Mr. Hunt argued that hospitals like Salford Royal and Northumbria have instituted seven-day working
Seven Day Working: in Practice Clinicians Perspective Jonathan Vickers Consultant surgeon Dec 2015 Why me? Mr. Hunt argued that hospitals like Salford Royal and Northumbria have instituted seven-day working
Paediatric Observation and Assessment Unit Operational Policy
 Paediatric Observation and Assessment Unit Operational Policy 1 Policy Title: Paediatric Observation and Assessment Unit Operational Policy Executive Summary: Supersedes: Description of Amendment(s): This
Paediatric Observation and Assessment Unit Operational Policy 1 Policy Title: Paediatric Observation and Assessment Unit Operational Policy Executive Summary: Supersedes: Description of Amendment(s): This
Inclement Weather Plan. Controlled Document Number: Version Number: 004. Controlled Document Sponsor: Controlled Document Lead: On: October 2017
 Inclement Weather Plan CATEGORY: CLASSIFICATION: Plan Emergency planning CONTROLLED DOCUMENT PURPOSE Controlled Document Number: This plan is designed to provide actions for the Trust to undertake to ensure
Inclement Weather Plan CATEGORY: CLASSIFICATION: Plan Emergency planning CONTROLLED DOCUMENT PURPOSE Controlled Document Number: This plan is designed to provide actions for the Trust to undertake to ensure
Provider Payment: highlights from the evidence
 Provider Payment: highlights from the evidence Anita Charlesworth Chief Economist Nuffield Trust September, 2012 17 October 2013 Provider Payment systems Activity based Not linked to activity Prospective
Provider Payment: highlights from the evidence Anita Charlesworth Chief Economist Nuffield Trust September, 2012 17 October 2013 Provider Payment systems Activity based Not linked to activity Prospective
Two Years On The Five Year Forward View for Mental Health
 Two Years On The Five Year Forward View for Mental Health Tim Kendall National Clinical Director for Mental Health, NHS England and NHS Improvement 15 May 2018 Mental Health Five Year Forward View: priorities
Two Years On The Five Year Forward View for Mental Health Tim Kendall National Clinical Director for Mental Health, NHS England and NHS Improvement 15 May 2018 Mental Health Five Year Forward View: priorities
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification
 Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
APPENDIX 7C BENEFITS REALISATION PLAN
 APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
Clinical. Financial. Integrated.
 Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Patients Experience of Emergency Admission and Discharge Seven Days a Week
 Patients Experience of Emergency Admission and Discharge Seven Days a Week Abstract Purpose: Data from the 2014 Adult Inpatients Survey of acute trusts in England was analysed to review the consistency
Patients Experience of Emergency Admission and Discharge Seven Days a Week Abstract Purpose: Data from the 2014 Adult Inpatients Survey of acute trusts in England was analysed to review the consistency
Inequalities Sensitive Practice Initiative
 Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
THE FIVE YEAR FORWARD VIEW FOR MENTAL HEALTH
 THE FIVE YEAR FORWARD VIEW FOR MENTAL HEALTH A Policy Unit briefing on the findings of the independent Mental Health Taskforce and the implications for psychiatrists and the wider NHS workforce Holly Taggart
THE FIVE YEAR FORWARD VIEW FOR MENTAL HEALTH A Policy Unit briefing on the findings of the independent Mental Health Taskforce and the implications for psychiatrists and the wider NHS workforce Holly Taggart
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Avon & Wiltshire Mental Health Partnership NHS Trust Commissioning for Quality and Innovation (CQUIN) Schedule 2015/16
 Schedule 2015/16") Avon & Wiltshire Mental Health Partnership NHS Trust Commissioning for Quality and Innovation (CQUIN) Schedule 2015/16 4A Nationally Mandated CQUIN IMPROVING PHYSICAL HEALTHCARE TO REDUCE PREMATURE MORTALITY
Avon & Wiltshire Mental Health Partnership NHS Trust Commissioning for Quality and Innovation (CQUIN) Schedule 2015/16 4A Nationally Mandated CQUIN IMPROVING PHYSICAL HEALTHCARE TO REDUCE PREMATURE MORTALITY
Liaison Service Psychiatry of Old Age, North Tyneside General Hospital Profile of Learning Opportunities
 Liaison Service Psychiatry of Old Age, North Tyneside General Hospital Profile of Learning Opportunities DATE LAST UPDATED :- July 2012 by Lynne Harrison and Joanne Leck Contents 1. Area Profile 2. Learning
Liaison Service Psychiatry of Old Age, North Tyneside General Hospital Profile of Learning Opportunities DATE LAST UPDATED :- July 2012 by Lynne Harrison and Joanne Leck Contents 1. Area Profile 2. Learning
Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper
 1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
Numerator. Denominator Rationale for inclusion
 Goal number Goal name Indicator number Indicator name Goal weighting (% of CQUIN scheme Indicator weighting (% of goal Description of indicator Numerator Denominator Rationale for inclusion Data source
Goal number Goal name Indicator number Indicator name Goal weighting (% of CQUIN scheme Indicator weighting (% of goal Description of indicator Numerator Denominator Rationale for inclusion Data source
NHS Information Standards Board
 DSC Notice: 29/2002 Date of Issue: September 2002 NHS Information Standards Board Subject: Data Standards: Mental Health Minimum Data Set Implementation Date: 1 st April 2003 DATA SET CHANGE CONTROL PROCEDURE
DSC Notice: 29/2002 Date of Issue: September 2002 NHS Information Standards Board Subject: Data Standards: Mental Health Minimum Data Set Implementation Date: 1 st April 2003 DATA SET CHANGE CONTROL PROCEDURE
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.
 MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.") CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire
 Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Clinical Case Manager for Older Persons. Elaine Dunne
 Clinical Case Manager for Elaine Dunne According to the World Health Organisations World Report on ageing (2015) the numbers of older people worldwide are dramatically increasing. In their Global Strategy
Clinical Case Manager for Elaine Dunne According to the World Health Organisations World Report on ageing (2015) the numbers of older people worldwide are dramatically increasing. In their Global Strategy
17. Dementia: John s Campaign
 17. Dementia: John s Campaign name weighting (% of CQUIN scheme available) Description of indicator Numerator Implementing a policy on welcoming carers and family members of people with dementia according
17. Dementia: John s Campaign name weighting (% of CQUIN scheme available) Description of indicator Numerator Implementing a policy on welcoming carers and family members of people with dementia according