Making Hospital Readmissions RARE in Minnesota
|
|
|
- Prudence Franklin
- 5 years ago
- Views:
Transcription

1 Making Hospital Readmissions RARE in Minnesota Minnesota Rural Health Conference June 24, Duluth MN Karla Weng, MPH, Stratis Health












2

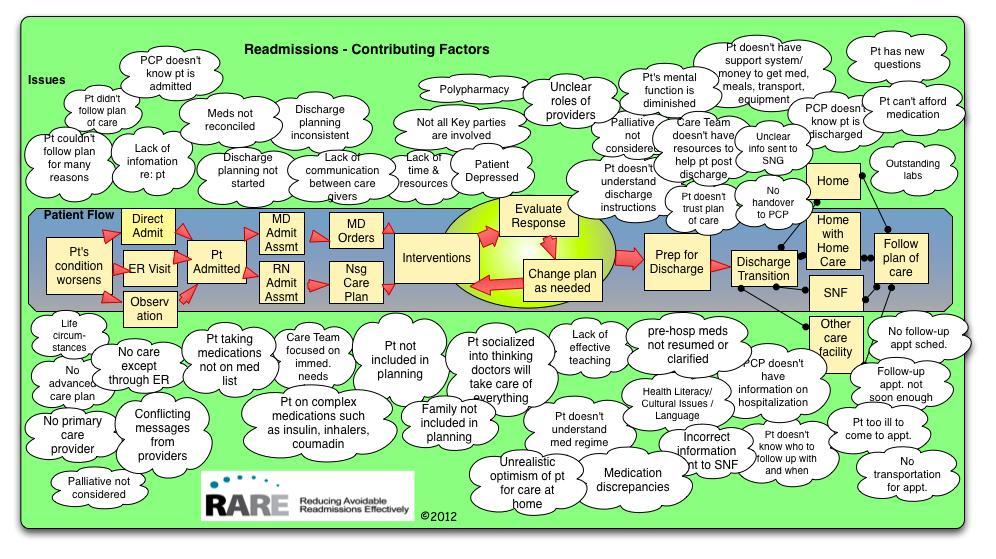
3 What is happening?
4
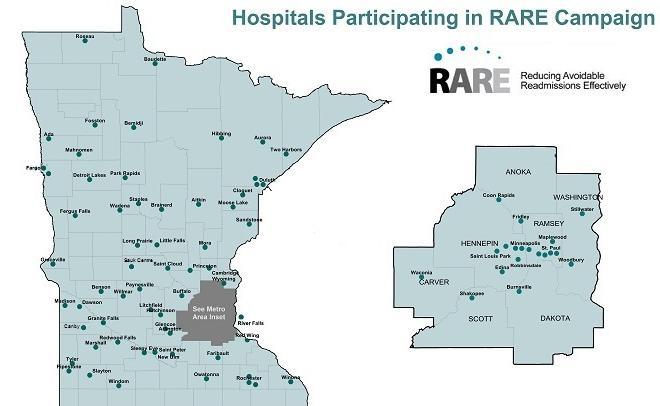
5 What is the RARE Campaign? A campaign across the continuum of care to reduce avoidable hospital readmissions across Minnesota and surrounding areas Regional approach, supported by hospitals, providers, health plans, other key stakeholders Campaign is engaging other care providers, acknowledging that readmissions are the result of a fragmented health care system



6 Triple Aim Goals Population health Prevent 4,000 avoidable readmissions within 30 days of discharge, OR in other words, Reduce overall readmissions rate by 20% from 2009 base by December 31, 2012 Care experience Recapture 16,000 nights of patients sleep in their own beds instead of in the hospital Improve by 5% on HCAHPS discharge survey questions Affordability of care Save an estimated $30 million for commercially insured patients; additional savings for Medicare patients

 Stratis")
7 Broad Community Support Operating Partners: Institute for Clinical Systems Improvement (ICSI) Minnesota Hospital Association (MHA) Stratis Health

8 Broad Community Support Supporting Partners: Minnesota Medical Association MN Community Measurement VHA Upper Midwest
9 Broad Community Support Community Partners: Endorse and actively support the campaign A growing list of providers, health plans, state health agencies, home health agencies, nursing homes, patient advocacy groups, and other community organizations Complete list on
10

11 Campaign Design
12 Five Focus Areas Patient and Family Engagement Transition Communication Comprehensive Discharge Plan Medication Management Transition Support
13 Patient Family Engagement and Activation 1. Use Teach Back to assess patient s understanding of any instructions 2. Ensure caregivers are engaged in developing the plan of care 3. Use health literacy standards such as AHRQ Health Literacy Universal Precautions
14 Comprehensive Discharge Planning A written patient centered plan must include: 1. Reason for hospitalization, including information on disease in terms patient can understand 2. Medications to be taken post transition: Purpose, dosage, when and how to take, and how to obtain refills 3. Self-care activities 4. Durable medical equipment 5. Symptom recognition and management 6. Coordination and planning for follow-up appointments
15 Medication Management 1. Medication reconciliation at each patient transition with date 2. Medication list should contain purpose for each medication 3. Pre/post hospital medication changes should be made clear to the patient 4. Medication discrepancies must be evaluated and acted upon 5. Use Teach Back when instructing patients on medication use
16 Care Transition Support 1. Follow-up appointment within 5 business days 2. Available appointment slots 3. Follow-up arranged with ancillary services, such as PT, OT, RT 4. Within 72 hours a purpose contact is made with patient by a care team member

17 Follow-up visit should focus on: 1. Patient s goals for the visit 2. Patient s needs for medication adjustment, test results, advance directives 3. Instruction on self management 4. Explanation of warning signs and how to respond 5. Instructions for seeking emergency and nonemergency after hours care
18 Transition Communication 1. PCP notified when patient is admitted or discharged 2. Patients know who is responsible for care and how to contact them 3. Concise transfer forms with key elements must be sent with the patient in every transfer 4. Direct reports between nursing staff 5. Complete discharge summaries should be received by the accepting facilities within 3 business days
19 Supporting Work Groups Medication Management Mental Health Epic Users Measurement Long Term Care
20 Potentially Preventable Readmissions Data source Minnesota Hospital Association database All-payer inpatient claims for all Minnesota hospitals But, can only look at readmit to same facility 22% readmits to different facility Software 3M Potentially Preventable Readmissions 3M s clinical experts developed methodology Each record designated as admission or readmission Calculates severity-adjusted PPR rates by condition and by hospital
21 Actual to Expected Ratio 1.05 Potentially Preventable Readmissions in Minnesota, RARE Hospitals represent 87% of discharges in Minnesota % decrease = 1,000 fewer readmissions RARE Campaign Launch RARE Hospitals Target Target is a 20% reduction by the end of 2012, using 2009 as a baseline q q q q 2011

22 16,000 Nights At Home Will Make Our Day.



23 Thank You For Helping Everyone Sleep More Peacefully.

, an agency of the U.S. Department of Health and Human Services.")
24 This material was prepared by Stratis Health, the Minnesota Medicare Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The materials do not necessarily reflect CMS policy. 10SOW-MN-C
Project RED (ReEngineering Discharge)
") Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
Care Coordination is More Than a Care Coordinator
 Care Coordination is More Than a Care Coordinator Jennifer P. Lundblad, PhD, MBA CA State Rural Health Association November 7, 2013 Objectives As a result of this session, participants will: Understand
Care Coordination is More Than a Care Coordinator Jennifer P. Lundblad, PhD, MBA CA State Rural Health Association November 7, 2013 Objectives As a result of this session, participants will: Understand
About Minnesota s hospitals
 2017 About Minnesota s hospitals Minnesota s 142 hospitals and health systems have earned a national reputation for delivering safe, high-quality care and for meeting the needs of our communities. It takes
2017 About Minnesota s hospitals Minnesota s 142 hospitals and health systems have earned a national reputation for delivering safe, high-quality care and for meeting the needs of our communities. It takes
Webinar Objectives. Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar
 Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar February 14, 2018 Webinar Objectives Discuss the analysis findings for home health referrals, post hospital discharge,
Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar February 14, 2018 Webinar Objectives Discuss the analysis findings for home health referrals, post hospital discharge,
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Care Transitions Success Stories and Lessons Learned
 Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Learning Session 4: Required Infection Reporting for Minnesota CAH
 Learning Session 4: Required Infection Reporting for Minnesota CAH Presenters: Vicki Tang Olson Program Manager, Stratis Health Janet Lilleberg Quality Data Specialist, Stratis Health Marilyn Grafstrom,
Learning Session 4: Required Infection Reporting for Minnesota CAH Presenters: Vicki Tang Olson Program Manager, Stratis Health Janet Lilleberg Quality Data Specialist, Stratis Health Marilyn Grafstrom,
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural
 Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural Jennifer P. Lundblad, PhD, MBA Washington University PCOR Symposium April 5-6, 2016 Washington University 2016
Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural Jennifer P. Lundblad, PhD, MBA Washington University PCOR Symposium April 5-6, 2016 Washington University 2016
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Medicare Community-Based Care Transitions Program. Linda M. Magno Director, Medicare Demonstrations
 Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Hospital IQR and VBP Programs: Reviewing Your Claims-Based Measures Hospital-Specific Reports Questions and Answers Speakers Tamara Mohammed, MHA, PMP Measure Implementation and Stakeholder Communication
Hospital IQR and VBP Programs: Reviewing Your Claims-Based Measures Hospital-Specific Reports Questions and Answers Speakers Tamara Mohammed, MHA, PMP Measure Implementation and Stakeholder Communication
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Strategies for Reducing Readmissions to the Inpatient Psychiatric Setting
 Strategies for Reducing Readmissions to the Inpatient Psychiatric Setting Kay E. Jewell, MD Tara Center LLC Sue Abderholden, MPH Executive Director NAMI Minnesota April 25, 2017 1 Objectives Identify elements
Strategies for Reducing Readmissions to the Inpatient Psychiatric Setting Kay E. Jewell, MD Tara Center LLC Sue Abderholden, MPH Executive Director NAMI Minnesota April 25, 2017 1 Objectives Identify elements
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Hospital Compare Quality Measures: 2008 National and Florida Results for Critical Access Hospitals
 Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Preventing Avoidable Readmissions: Collaborative Measurement. July 24, 2013
 Preventing Avoidable Readmissions: Collaborative Measurement July 24, 2013 Collaborative Goals Reduce readmission rates by 20% Increase the number of patients in the pilot unit or population who undergo
Preventing Avoidable Readmissions: Collaborative Measurement July 24, 2013 Collaborative Goals Reduce readmission rates by 20% Increase the number of patients in the pilot unit or population who undergo
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Minnesota Rural Palliative Care Initiative
 Minnesota Rural Palliative Care Initiative Janelle Shearer, RN, BSN, MA 2010 Minnesota Gerontological Society Annual Spring Conference - Pushing the Envelope: Innovative Models for Aging Populations April
Minnesota Rural Palliative Care Initiative Janelle Shearer, RN, BSN, MA 2010 Minnesota Gerontological Society Annual Spring Conference - Pushing the Envelope: Innovative Models for Aging Populations April
Best Practices: Access Case Management
 Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Decrease in Hospital Uncompensated Care in Michigan, 2015
 Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Implementing QAPI: Translating Data into Action. Objectives
 Implementing QAPI: Translating Data into Action Jane C Pederson, MD, MS April 16, 2013 Objectives Prioritize improvement opportunities based on data Identify a baseline measure for an improvement project
Implementing QAPI: Translating Data into Action Jane C Pederson, MD, MS April 16, 2013 Objectives Prioritize improvement opportunities based on data Identify a baseline measure for an improvement project
Appendix B: Formulae Used for Calculation of Hospital Performance Measures
 Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
NNHQI Campaign. Safely Reduce Hospitalizations Tracking Tool Getting Started!
 NNHQI Campaign Safely Reduce Hospitalizations Tracking Tool Getting Started! This material was prepared by Telligen, National Nursing Home Quality Improvement Campaign contractor, under contract with the
NNHQI Campaign Safely Reduce Hospitalizations Tracking Tool Getting Started! This material was prepared by Telligen, National Nursing Home Quality Improvement Campaign contractor, under contract with the
Medicare Beneficiary Quality Improvement Project (MBQIP)
") Medicare Beneficiary Quality Improvement Project (MBQIP) Karla Weng, MPH, CPHQ November 14, 2017 Nebraska CAH Conference on Quality Kearney, NE Stratis Health Independent, nonprofit, Minnesota-based organization
Medicare Beneficiary Quality Improvement Project (MBQIP) Karla Weng, MPH, CPHQ November 14, 2017 Nebraska CAH Conference on Quality Kearney, NE Stratis Health Independent, nonprofit, Minnesota-based organization
Medicare: 2017 Model of Care Training 4/13/2017
 Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
2 nd Annual PPS Quality and Patient Safety Conference
 2 nd Annual PPS Quality and Patient Safety Conference Jointly Sponsored by MHA and Stratis Health Welcome and Introduction Jennifer Lundblad, PhD, MBA, President & CEO, Stratis Health Healthcare-Centric
2 nd Annual PPS Quality and Patient Safety Conference Jointly Sponsored by MHA and Stratis Health Welcome and Introduction Jennifer Lundblad, PhD, MBA, President & CEO, Stratis Health Healthcare-Centric
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE
 STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M. D., M.P.H. Jack C. Keane Bernadette C.
STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M. D., M.P.H. Jack C. Keane Bernadette C.
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
A Battelle White Paper. How Do You Turn Hospital Quality Data into Insight?
 A Battelle White Paper How Do You Turn Hospital Quality Data into Insight? Data-driven quality improvement is one of the cornerstones of modern healthcare. Hospitals and healthcare providers now record,
A Battelle White Paper How Do You Turn Hospital Quality Data into Insight? Data-driven quality improvement is one of the cornerstones of modern healthcare. Hospitals and healthcare providers now record,
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
2015 Executive Overview
 An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Home Health Quality Improvement Campaign
 Home Health Quality Improvement Campaign Description of Monthly Report for Improvement in Oral Medications Monthly Report for Improvement in Management of Oral Medications All data displayed illustrate
Home Health Quality Improvement Campaign Description of Monthly Report for Improvement in Oral Medications Monthly Report for Improvement in Management of Oral Medications All data displayed illustrate
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Discharge Information
 Discharge Information Yes, patients were given information about what to do during their recovery Vikki Choate, MSN, RN, CCM, RN-BC, CPHQ Nashville, TN May 14-15, 2013 Learning Objectives At the end of
Discharge Information Yes, patients were given information about what to do during their recovery Vikki Choate, MSN, RN, CCM, RN-BC, CPHQ Nashville, TN May 14-15, 2013 Learning Objectives At the end of
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
New Models for Rural Post-Acute Care. Mark Lindsay MD Assistant Professor Mayo Clinic College of Medicine
 New Models for Rural Post-Acute Care Mark Lindsay MD Assistant Professor Mayo Clinic College of Medicine Objectives Understand Post-acute Transitional Care as a tremendous opportunity for critical access
New Models for Rural Post-Acute Care Mark Lindsay MD Assistant Professor Mayo Clinic College of Medicine Objectives Understand Post-acute Transitional Care as a tremendous opportunity for critical access
Database Profiles for the ACT Index Driving social change and quality improvement
 Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Product and Network Innovation: Strategies to Achieve Triple Aim Success. Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013
 Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
THE BRIDGE MODEL. Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging
 THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Clinical Quality Payment Policies Impact to Finance and Operations
 Clinical Quality Payment Policies Impact to Finance and Operations Kristen Geissler, MS, PT, MBA, CPHQ Director Berkeley Research Group December 4, 2014 What s the Buzz? Cost Efficient VALUE Effective
Clinical Quality Payment Policies Impact to Finance and Operations Kristen Geissler, MS, PT, MBA, CPHQ Director Berkeley Research Group December 4, 2014 What s the Buzz? Cost Efficient VALUE Effective
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes
 Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Hi-Tech Software and the Triple Check Process
 Hi-Tech Software and the Triple Check Process Contents How Hi-Tech Software Assists the Triple Check Process... 1 Census... 1 Stay Tables... 2 Hi-Tech Helps you Avoid Incorrect Assessments... 3 Diagnosis
Hi-Tech Software and the Triple Check Process Contents How Hi-Tech Software Assists the Triple Check Process... 1 Census... 1 Stay Tables... 2 Hi-Tech Helps you Avoid Incorrect Assessments... 3 Diagnosis
Team Building Storyboard Template
 Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient
Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient
Transitional Care and Preventing Readmissions in San Francisco
 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
The Link Between Patient Experience and Patient and Family Engagement
 The Link Between Patient Experience and Patient and Family Engagement Powerful Partnerships: Improving Quality and Outcomes Mission to Care Florida Hospital Association Hospital Improvement Innovation
The Link Between Patient Experience and Patient and Family Engagement Powerful Partnerships: Improving Quality and Outcomes Mission to Care Florida Hospital Association Hospital Improvement Innovation
Recommendations for Transitions of Care in North Carolina
 Recommendations for Transitions of Care in North Carolina FINAL REPORT June 30, 2014 Revised, July 31, 2014 Submitted to: North Carolina Office of Rural Health and Community Care 311 Ashe Avenue Raleigh,
Recommendations for Transitions of Care in North Carolina FINAL REPORT June 30, 2014 Revised, July 31, 2014 Submitted to: North Carolina Office of Rural Health and Community Care 311 Ashe Avenue Raleigh,
Care Transitions: What Does It Really Look Like?
 Care Transitions: What Does It Really Look Like? Selena Bolotin, LICSW Director WA Patient Safety & Care Transitions June 5, 2014 Qualis Health is one of the nation s leading healthcare consulting organizations,
Care Transitions: What Does It Really Look Like? Selena Bolotin, LICSW Director WA Patient Safety & Care Transitions June 5, 2014 Qualis Health is one of the nation s leading healthcare consulting organizations,
Coordination of Care Initiative Mora Area Community
 Coordination of Care Initiative Mora Area Community Community Meeting October 9, 2018 FirstLight Health System Download meeting agenda and slide handout: Agenda Presentation handout 2 1 Welcome Introductions
Coordination of Care Initiative Mora Area Community Community Meeting October 9, 2018 FirstLight Health System Download meeting agenda and slide handout: Agenda Presentation handout 2 1 Welcome Introductions
Population health and potentially preventable events 3M solutions for population health, patient safety and cost-effective care
 3M Health Information Systems Population health and potentially preventable events 3M solutions for population health, patient safety and cost-effective care Challenge: Shifting the financial risk The
3M Health Information Systems Population health and potentially preventable events 3M solutions for population health, patient safety and cost-effective care Challenge: Shifting the financial risk The
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
Quality Measures for CAH Swing Bed Patients
 Quality Measures for CAH Swing Bed Patients Ira Moscovice, PhD Michelle Casey, MS Henry Stabler, MPH Division of Health Policy and Management University of Minnesota NRHA Annual Meeting New Orleans, LA
Quality Measures for CAH Swing Bed Patients Ira Moscovice, PhD Michelle Casey, MS Henry Stabler, MPH Division of Health Policy and Management University of Minnesota NRHA Annual Meeting New Orleans, LA
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Health Literacy: A Crisis In Health Care Minnesota Rural Health Conference July 19, 2005 Duluth, MN
 Health Literacy: A Crisis In Health Care Minnesota Rural Health Conference July 19, 2005 Duluth, MN Developed by Stratis Health with the Permission of the American Medical Association Foundation and the
Health Literacy: A Crisis In Health Care Minnesota Rural Health Conference July 19, 2005 Duluth, MN Developed by Stratis Health with the Permission of the American Medical Association Foundation and the
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
PRE-DECISIONAL SURVEYOR WORKSHEET. Assessing Hospital Compliance with the. Condition of Participation for Discharge Planning
 PRE-DECISIONAL SURVEYOR WORKSHEET Assessing Hospital Compliance with the Condition of Participation for Discharge Planning Pilot Program Draft Version Name of State Agency: Instructions: The following
PRE-DECISIONAL SURVEYOR WORKSHEET Assessing Hospital Compliance with the Condition of Participation for Discharge Planning Pilot Program Draft Version Name of State Agency: Instructions: The following
Volume to Value Based Healthcare Dr. Thilo Koepfer, VP International, 3M Health Information Systems
 Volume to Value Based Healthcare Dr. Thilo Koepfer, VP International, 3M Health Information Systems Learning Objectives 1. Explain the Triple Aim as developed by the Institute of Healthcare Improvement
Volume to Value Based Healthcare Dr. Thilo Koepfer, VP International, 3M Health Information Systems Learning Objectives 1. Explain the Triple Aim as developed by the Institute of Healthcare Improvement
HOSPITAL PATIENT SAFETY INITIATIVE (PSI)
") HOSPITAL PATIENT SAFETY INITIATIVE (PSI) DRAFT RISK EVALUATION TOOL Discharge Planning Name of State Agency: Instructions: The following is a list of items that must be assessed during the on-site survey,
HOSPITAL PATIENT SAFETY INITIATIVE (PSI) DRAFT RISK EVALUATION TOOL Discharge Planning Name of State Agency: Instructions: The following is a list of items that must be assessed during the on-site survey,
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of