Damage Control Surgery
|
|
|
- Erik Pitts
- 5 years ago
- Views:
Transcription
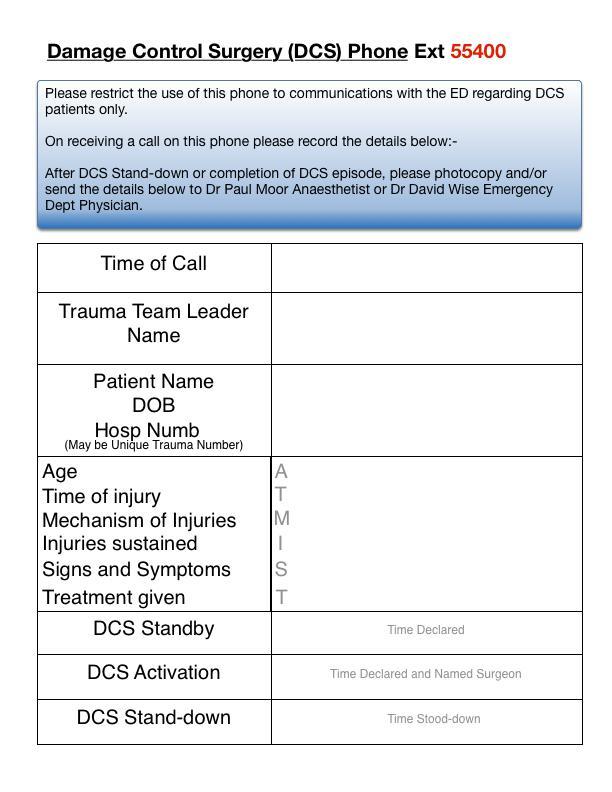
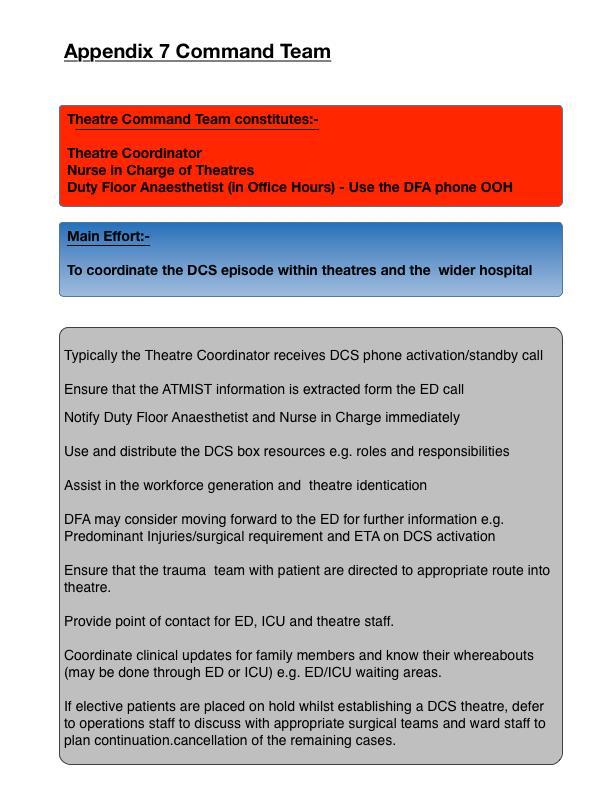
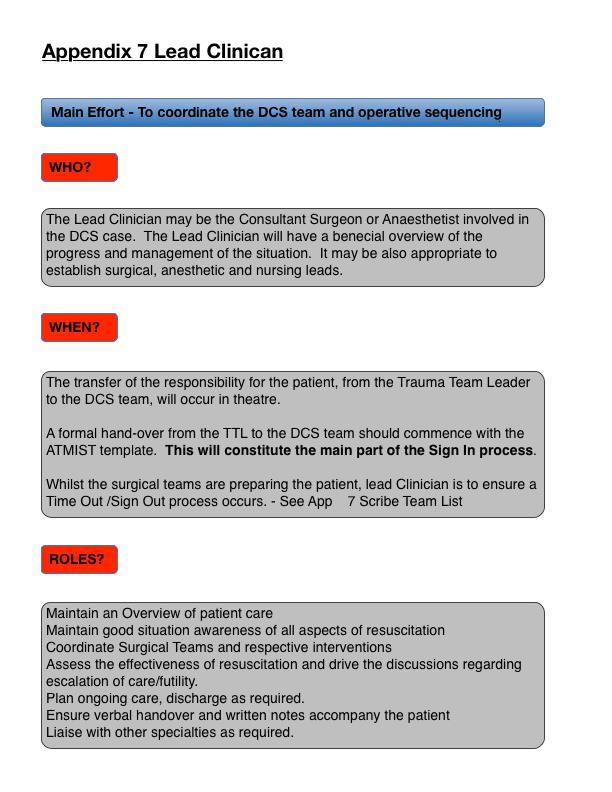
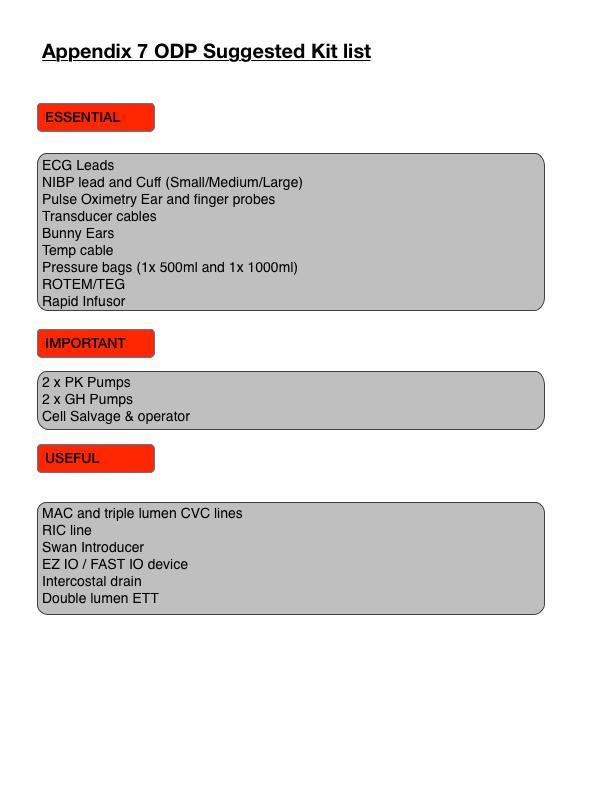
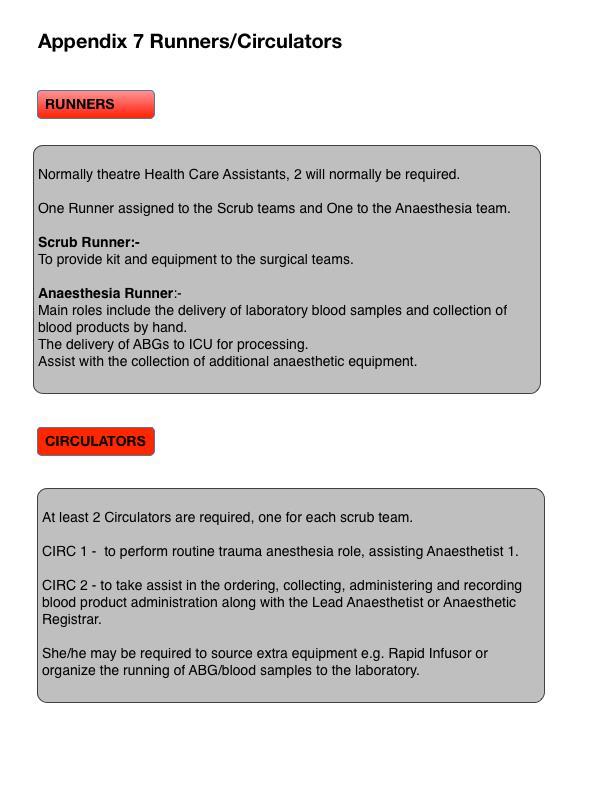
1 Damage Control Surgery Tactics, Techniques and Procedures Trauma Team Members ITU Consultants and Middle Grades Action: Anaesthetic Consultants, Middle Grades General Surgery Consultants and Middle Grades T&O Consultants and Middle grades Theatre Staff Info: MTCCs Related documents: Trauma Call SOP, Paeds Trauma Call and DCS SOP Publication date: Feb 16 Review date: Aug 19 Version 2 Authors: Paul Moor, Sarah Droog, Scott Adams Contents 1. Introduction & Purpose 2 2. The Guideline 2 3. Application 2 4. Damage Control Surgery Guideline Triggers 2 5. Actions on activation 3 6. Patient Transfer Arrangements 4 7. Trauma Team Reception 4 8. Surgery/Anaesthesia Conduct 5 9. Intensive Care Medicine Debrief Audit Guideline Summary Appendices 1 DCS Phone Audit Form/Response Flowchart 7/8 2 DCS Guideline Escalation/De-escalation 9 3 DCS Activation Box Contents 10 4 Actions on DCS Activation 11 5 Staff Generation Matrix 12/13 6 Theatre Identification Matrix 14 7 DCS Team Member Roles and Responsiblities Command Team 15 Scribe/Team List 16/17 Lead Clinician 18 Surgical Team 19 Anaesthesia Team 20 Scrub/ODP Team 21 ODP Suggested Kit list 22 Runners/circulators 23 8 Blood Product Template/10 Minute Brief 24 9 Theatre Equipment Theatre Layout DCS WHO Surgical Checklist Debrief Template Equipment Packing Lists 29 1
2 1. INTRODUCTION/PURPOSE 1.1 Plymouth Hospitals NHS Trust is a Major Trauma Centre and as a result, is mandated to provide high quality care to the severely injured trauma patients. Traumatic injury requiring immediate or Damage Control Surgery (DCS) is rare, but when encountered it best served by a unified and swift institutional response. Such actions will help to maximise patient safety and minimize patient morbidity/mortality. The World Health Organisation suggests that this is best served by the generation of clinical guidelines and standard operating procedures (SOP). 1.2 This SOP will enable and encourage the safe and effective provision of DCS, through mobilizing the correct personnel, equipment and real estate. Emphasis will be placed on clear and effective lines of communication, mutual role awareness, good team behaviours and clear escalation and de-escalation features. 1.3 This SOP is not intended to replace the clinical decision making of senior clinicians. It serves to provide approved guidance to all care providers. It aims to assist in how best identify and prepare the trauma patient, staff, laboratory and theatre suite for their DCS. 1.4 For further clinical guidance please refer to Trauma Call and Traumatic Cardiac Arrest SOP dated July For the specific management of Paediatric patients requiring DCS see the guideline listed above. 2. THE STANDARD OPERATING PROCEDURE 2.1 This SOP aims to assist with the safe and effective transfer to theatre and provision of DCS to the complex multiply injured patient. 3. APPLICATION: TO WHOM THIS SOP APPLIES 3.1 This Guideline will relate to all patients, identified in the ED or prior to hospital arrival, who have been identified to be at risk of life threatening haemorrhage, requiring contamination control or restoration of perfusion and have a subsequent requirement for DCS. 3.2 This SOP applies to all Hospital Trauma Call Team members and level 4 Theatre team members within PHNT. All T&O and General surgeons should be familiar with the guideline; other sub specialties may be called on for definitive surgery or collaboration and subsequent decision-making regarding the patient s care. 3.3 The policy will be implemented by personnel in ED, main theatres, Anaesthesia and Intensive Care departments. 4. DAMAGE CONTROL SURGERY - GUIDELINE TRIGGERS 4.1 This guideline will be triggered when there is a need to transfer patients to an operating theatre for DCS to arrest life-threatening haemorrhage, reduce contamination or restore perfusion. This surgery should follow DCS principles and may include surgery for proximal haemorrhage control, packing, or a combination of both. See Appendix Likely activation may be predictable and should be anticipated from prehospital notification of patient injuries and physiology (ATMIST). Activation may also be made at any stage of the patients Trauma Bay treatment. See Trauma Call SOP. 4.3 This guideline can be activated in part ( DCS Standby ), via Trauma Team Leader (TTL) communications with Theatre Reception/Coordinator (Ext 55400) see Appendix 2. Full activation ( DCS DECLARED ) usually requires discussions with the relevant single specialty 2
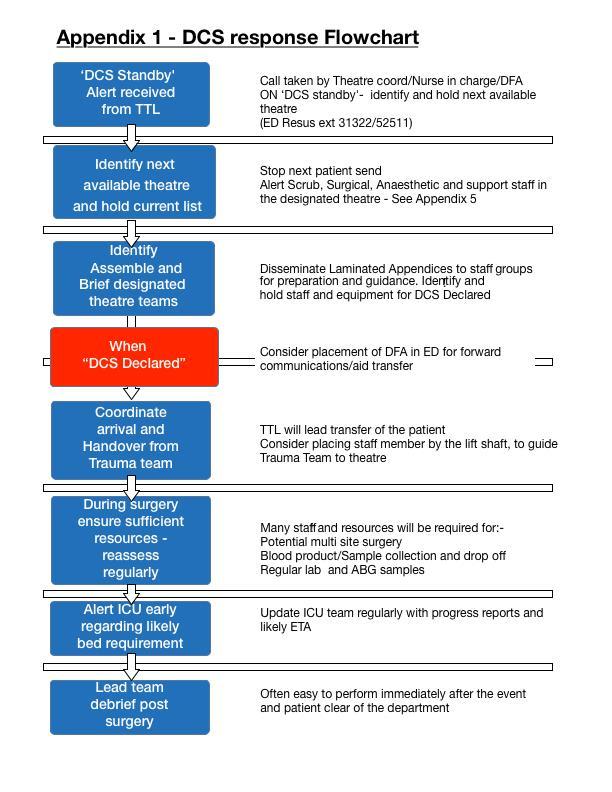
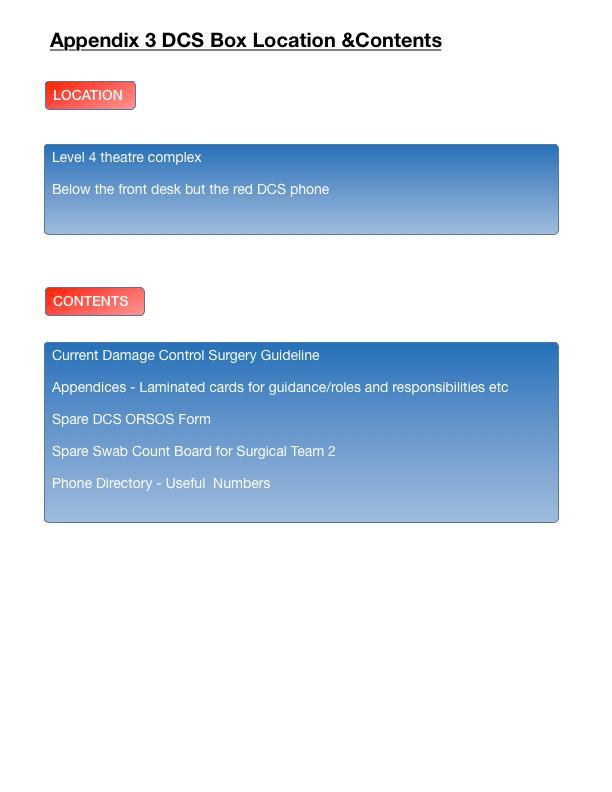
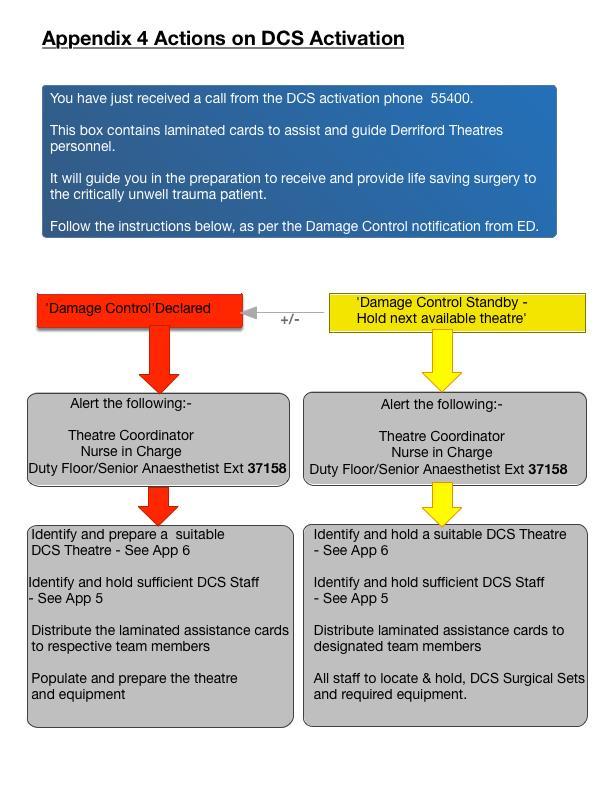
3 Consultant, however DCS DECLARED can be activated by the TTL. DCS phone ext should be notified of named speciality. 4.4 Standard triggers for ACTIVATION OF DCS GUIDELINE include:- i/ ED Thoracotomy/Traumatic Cardiac Arrest ii/ Urgent Abdominal, Chest or Pelvic Surgery iii/ Exsanguinating Haemorrhage requiring proximal control iv/ Non responder to Haemostatic resuscitation and MTP with suspected solid visceral injury 4.5 TTL and the assembled team are encouraged to consider as part of their initial assessment, do we need to action or standby the DCS Guideline or do theatres need to be made aware?. This may be done as part of the 10 minute trim. 4.6 DCS STANDBY is encouraged if the TTL suspects that surgery may be required. When STANDBY is called, a theatre will be made available as quickly as possible This situation may be STOODDOWN at a later time. Triggers for DCS STANDBY include:- i/ A likely requirement for time critical/life saving surgery after CT scanning has been completed. 4.7 Staff are reminded that when the guideline is in STANDBY, the theatre coordinator (ext 55400) will require regular updates regarding ETD from ED/CT. This is more important during silent hours. 4.8 Be advised that activation and implementation of this guideline differs in and out of office hours. Trauma Team Members and Leaders are encouraged to consider the activation of this guideline early, outside of the normal working day, to enable sufficient staff generation. 5. ACTIONS ON ACTIVATION See Appendix Activation will occur via ext (DCS Phone) Theatre Coordinator and Duty Floor Anaesthetist ext (on call Anaesthetists outside Office hours). Please reserve ext for essential DCS communications only. As a key part of the DCS Standby or DCS Declared an ATMIST statement is required, with the proposed surgery and site detailed. It is useful to use this comprehensive list to describe the surgery to aid communication. Resuscitative Thoracotomy Resuscitative Laparotomy Pelvic Packing Junctional Control Upper Limb Lower Limb Neck Complex Airway Management Craniotomy Thoracotomy Laparotomy Vascular Shunt Fasciotomy External Fixation Debridement Splint 5.2 Theatre Coordinator will locate and open the DCS Guideline Box and action it s contents. 3
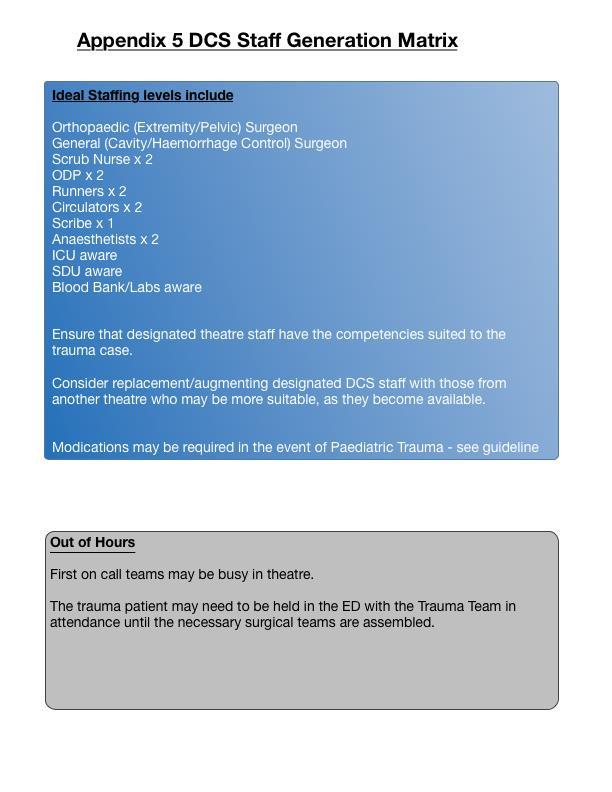
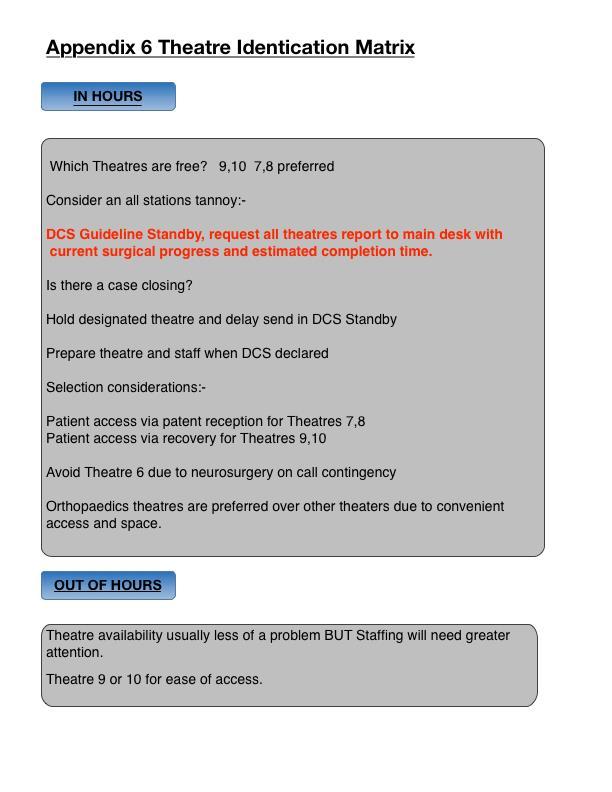
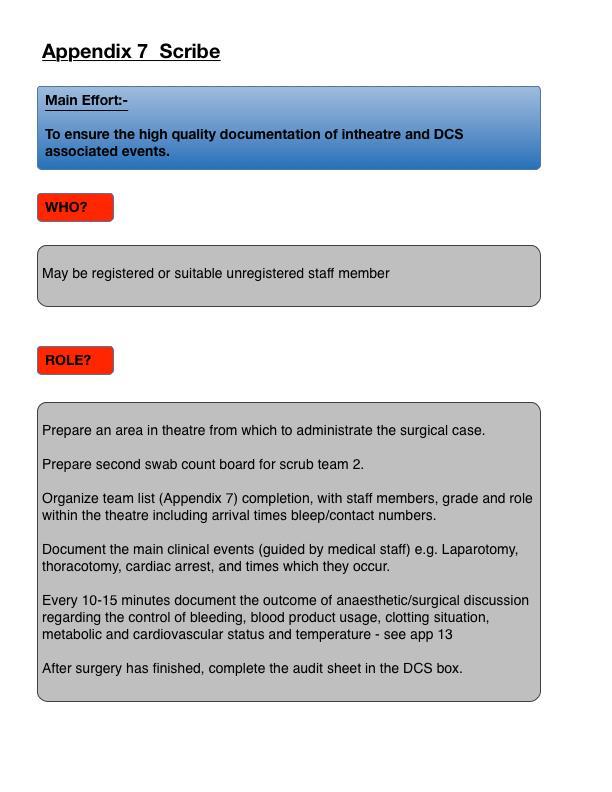
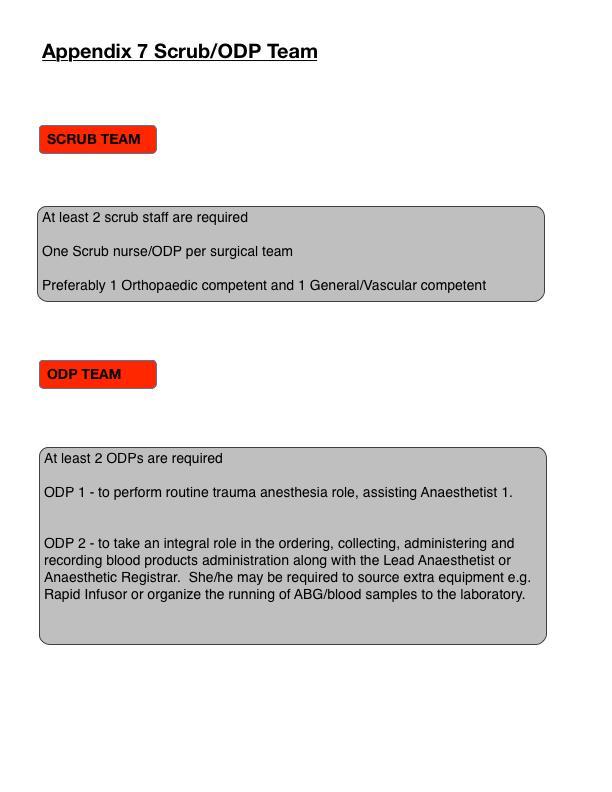
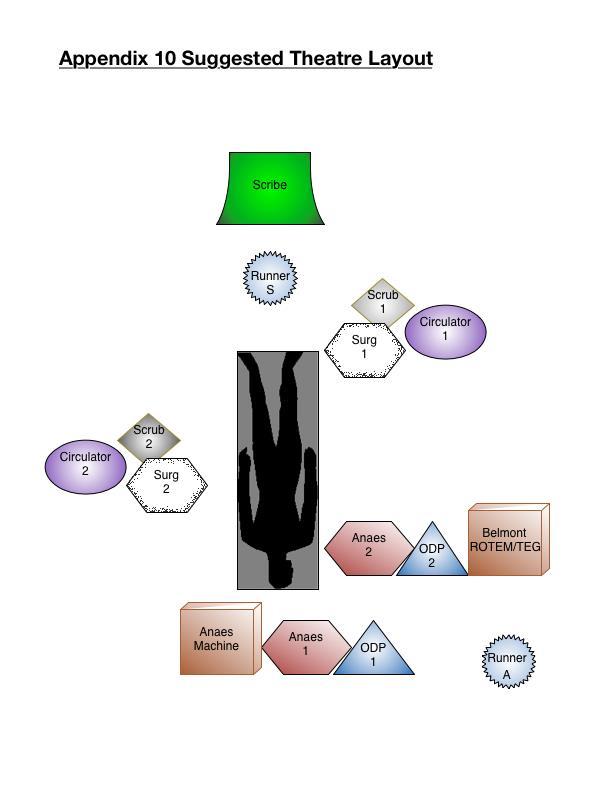
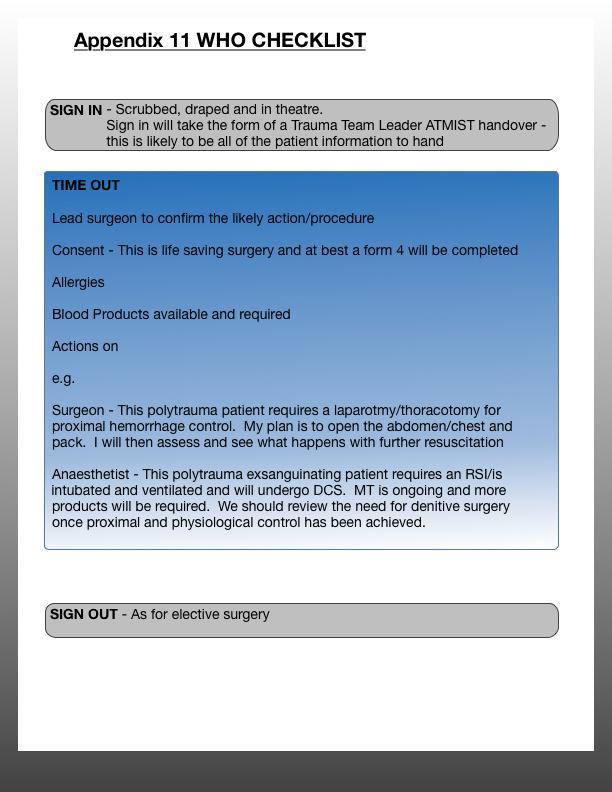
4 5.3 Theatre Coordinator and Senior Nurse will identify the next available theatre and hold for potential use. See Appendix 5. The designated theatre team will be alerted and all efforts made to deliver the Guideline Box and administration to that designated theatre. 5.4 Designated theatre teams will obtain respective Role and Responsibility cards and liaise regarding equipment requirements, surgical set requirements etc See Appendix 7. Absent team members as designated by Appendix 5 should be sought as a matter of urgency. 5.5 Out of hours, theatre team generation may well be delayed, due to off site team members. As a result efforts should be made to notify these personnel early. See Appendix 5 staff generation matrix. 5.6 The receiving theatre should be configured in a way that will allow at least two surgical teams access to the patient, see appendix 10 for a suggested layout. 5.7 All subteams should acquire the appropriate equipment as per appendix 9 and assist other sub teams as appropriate. The scribe will require assistance with the placement of blood usage, swab count and team list; the Runners may be suitably placed to assist with this. 5.8 Nurse in charge is well placed to liaise with Theatre Coordinator regarding estimated time of arrival of the casualty. One or more members of staff should be tasked to wait in the level 4 corridor to receive the mobile Trauma Team and direct to the designated theatre. 6. PATIENT TRANSFER ARRANGEMENTS 6.1 The assembled Trauma Team having activated the DCS Guideline will call Theatres on Ext Movements to theatre may occur direct from ED or from CT. Patient movements will require sufficient portering staff and only after pre move checklists have been completed in line with the trauma call SOP. 6.3 The patient transfer should involve all Trauma Team Members with coordination from TTL and attending Anaesthetist. Consideration of maintaining rapid infusion device use in transit should be given, certainly in the transient and non-responder. Transit considerations include:- i/ Designated staff member to depart in advance and hold lift. ii/ Infusion teams to continue manual infusion methods if rapid infusers are removed. iii/ Lift Holder heads straight to theatres when relieved, ahead of the remainder of the team, down the stairs, to identify Theatres POC. iv/ Theatres must direct the inbound trauma team to the identified theatre. Direction will be required via the appropriate route in. ie Via patient reception for Th 7, Via Recovery for Th TRAUMA TEAM RECEPTION 7.1 Trauma team will arrive in theatre with the patient, who should be allowed to transfer the patient directly to the operating table and establish adequate ventilation. 7.2 All receiving staff will remain hands off the trauma patient and ensure a Silent Cockpit whilst the Trauma Team Leader delivers their ATMIST handover to the surgery team; this process will serve as an effective WHO surgical checklist Sign in - See Appendix 11. The Scribe will require all documentation from the TTL, including details of all individuals present. 4
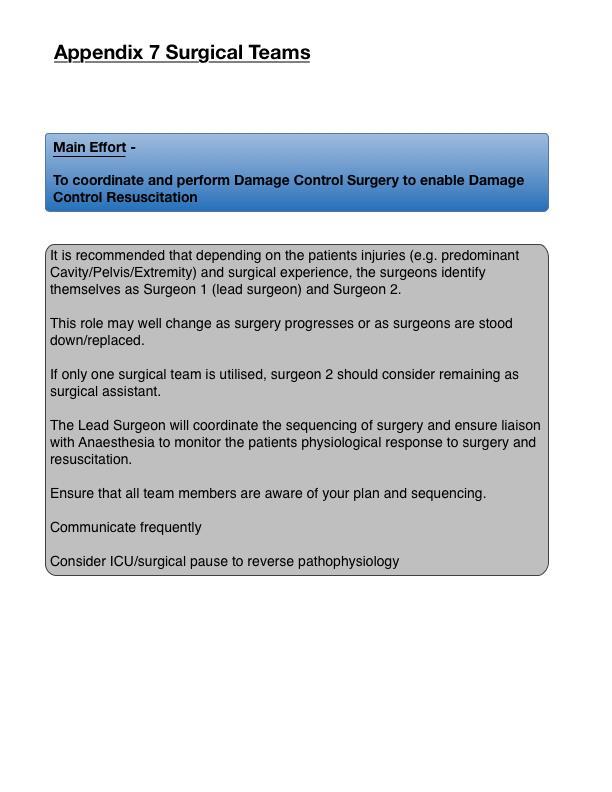
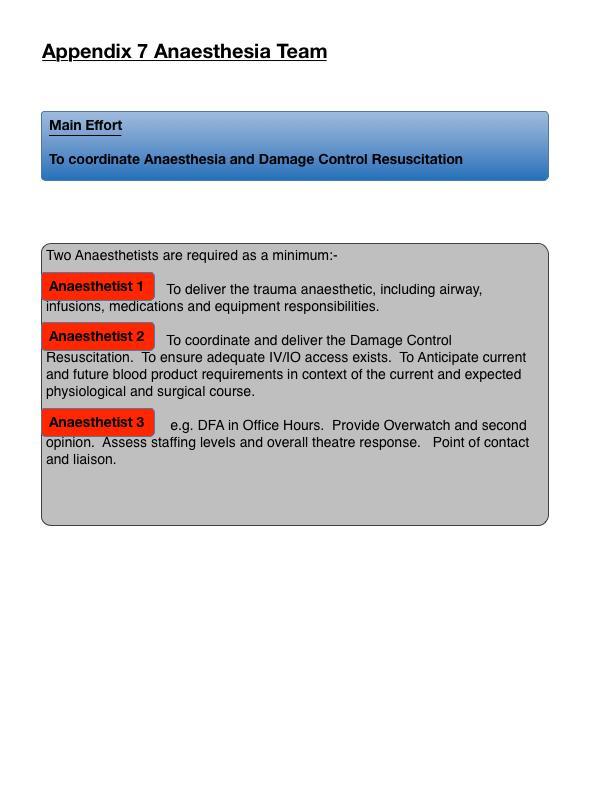
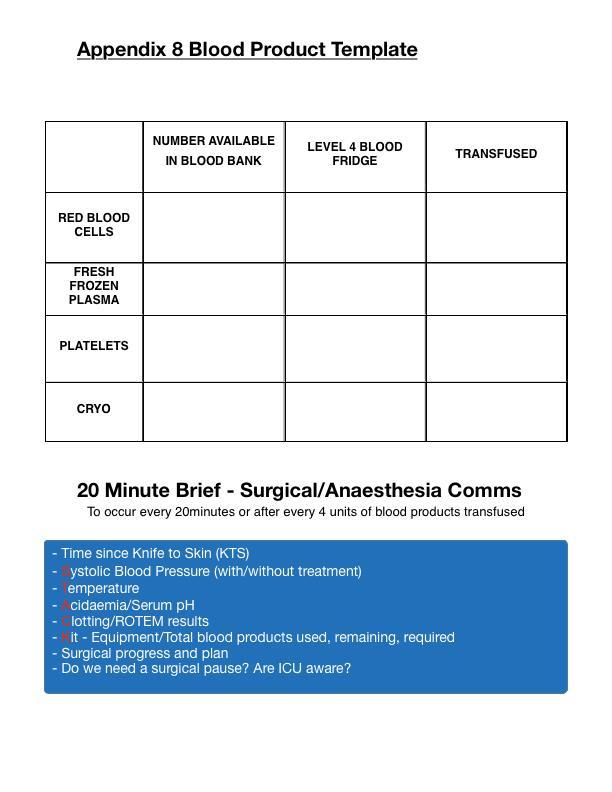
5 7.3 The Trauma Team should remain in theatre until stood down by the lead clinician a suitable time for this is on establishment of haemorrhage/proximal control. 7.4 The designated lead surgeon should adhere to the WHO checklist for Time Out and also utilize this as a way of delivering information regarding the surgical sequencing to the wider team. The WHO checklist needs to be abbreviated in this patient population, enabling the maintenance of patient safety, team focus and pragmatism. See appendix Liaison with Intensive Care Medicine must occur to inform them of likely organ support requirements and estimated length of surgery/post operative ICM requirements. 7.6 Surgeons, Anaesthetists and Intensivists should be encouraged to discuss treatment options, estimated time lines, prognosis and futility at earliest possibility. 8. SURGERY/ANAESTHESIA CONDUCT 8.1 By the very nature of DCS, Surgery Teams are encouraged to pursue a Damage Control approach i.e. the completion of surgical procedures to prevent exsanguination, control contamination and restore perfusion, in order to achieve physiological stability. This often means that surgery is abbreviated to allow the acidaemic, coagulopathic and hypothermic patient s physiology to be normalized. It is anticipated that the entire surgical episode should not last longer than an hour. 8.2 Within the surgical episode patients may require a Surgical Pause, where the surgical teams will temporarily cease surgery allowing the anaesthesia team to address acidaemia, coagulopathy and hypothermia. The Surgical Pause, serves as a useful break in the proceedings and may allow all specialties to discuss the care delivered, assess efficacy, prognosticate, discuss futility, boundaries to care and brief families. The 20 minute Brief will help to identify this requirement See appendix Major trauma patients requiring DCS will be recipients of Massive Transfusion. Up to 40% of these patients may be coagulopathic. To that end, the Anaesthesia teams are encouraged to maintain regular blood sample provision and good communications with laboratory staff and Haematology/Transfusion physicians. Utilisation of point of care coagulation testing eg ROTEM or TEG, to fine tune blood product replacement is encouraged. Appendix 8 Blood Product Template is designed to provide all team members an update on blood products used and pending. Blood Bank Haematology/Transfusionists can be reached through switchboard. 8.4 Anaesthetists are encouraged to prompt the surgical teams on a 20 minute basis, as a minimum or after every RBC and FFP. Communications back and forth are encouraged to establish:- Time since surgical start/knife to Skin Systolic BP Temperature Acidaemia/Serum ph Coagulation/ROTEM results Kit Equipment/Blood products used, remaining and required. Plan Surgical and Anaesthetic It is hoped that the brief above, in the context of anaesthesia, resuscitation and surgical progress will allow physicians to establish the trajectory of a patients condition, the requirement for a Surgical Pause, likely physiological trajectory and prognosis. It may also prompt discussions regarding the appropriateness of current treatment, staging or potential futility of care. See Appendix 8. 5
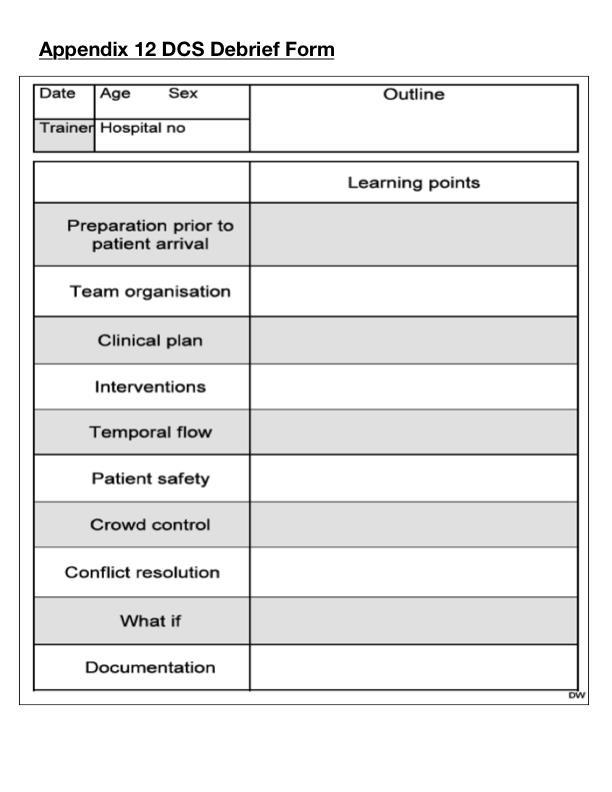
6 9. INTENSIVE CARE MEDICINE 9.1 At all times, early communication is key to success. Effective communications with ICU to keep them fully informed of the situation in theatre and estimated surgery length/progress, will be useful. ICU can be reached through switchboard, bleep 0110 or ext DEBRIEF 10.1 An effective debrief will enable the development and improvement of this guideline. After each DCS episode, all staff members are encouraged to perform a debrief process using the Appendix 12 template. This will serve to identify areas of excellence and/or those requiring further attention and improvement. 11. AUDIT 11.1 Activation of this guideline will be audited in both Stand by and Declared states. The impact of Damage Control Standby on level 4 efficiency will be monitored along with every Damage Control Declared patient. 12. SUMMARY OF THE POLICY 12.1 Improving the ED/Theatres interface, with a DCS guideline aims to improve the patient outcome through informed decision-making and optimized team behaviours of all attending staff This guideline promotes and encourages a safe, organized and measured institutional response, to physiologically unstable patients, undergoing potentially hazardous movements around the hospital Provision of a guideline and common trajectory serves to improve team behaviours and formulate a distributed situation awareness, on which to base sound decision making. 6
7 7
8 8
9 9
10 10
11 11
12 12
13 13
14 14
15 15
16 16
17 17
18 18
19 19
20 20
21 21
22 22
23 23
24 24
25 25
26 26
27 27
28 28
29 APPENDIX 13 Top Metal Bucket Plaster Trolley Packing List Tactics, Techniques and Procedures Sister Osborn 01 Aug 16 Synthetic Undercast Padding 7.5 cm X 10 Plaster of Paris Slabs 10 cm X cm X cm X 1 Box 15 cm X 1 Box Plaster of Paris Roll 5 cm X cm X 1 Box 7.5 cm X cm X cm X 10 Synthetic Roll 5 cm X cm X cm X 10 Top Drawer Crepe Bandage 5 cm X 10 Narrow Plaster spreaders X 1 10 cm X 10 Broad Plaster spreaders X 1 15 cm X 10 Tough Cut Scissors X 2 Transpore Tape X 2 Bottom Drawer Fleecy Web Roll (5 cm X 3m) X 2 rolls Fleecy Web Sheets (22.5 cm X 40 cm) X 2 packs Stockinette 5 cm X 2 rolls 7.5 cm X 2 rolls 10 cm X 2 rolls Bottom Rolls of Bags for Bucket Inco pads X 10 Props X 2 In Department Plaster saw To be restocked daily by Theatre 9 HCA during morning theatre set up 29
30 DCS Trolley Packing List Tactics, Techniques and Procedures 30
MISSION IMMEDIATE ACTIONS RESPONSIBILITIES. Triage of patients in Emergency Centre according to protocol
 TRIAGE OFFICER Triage of patients in Emergency Centre according to protocol Get briefing from Emergency Centre Medical Commander Triage patients as they arrive, according to protocol Preparation of areas
TRIAGE OFFICER Triage of patients in Emergency Centre according to protocol Get briefing from Emergency Centre Medical Commander Triage patients as they arrive, according to protocol Preparation of areas
Anaesthetic Trainees- The Trauma Call at SMH
 Anaesthetic Trainees- The Trauma Call at SMH Anaesthetic staff at a trauma call Bleep Grade Times 1201 Consultant 08:00 18:00 SpR on-call for theatres 18:00 08:00 6348 Extra SpR 08:00 17:00 Obstetric SpR
Anaesthetic Trainees- The Trauma Call at SMH Anaesthetic staff at a trauma call Bleep Grade Times 1201 Consultant 08:00 18:00 SpR on-call for theatres 18:00 08:00 6348 Extra SpR 08:00 17:00 Obstetric SpR
Time-Critical Transfer of the Sick or Injured Child (<16 years)
") LRI Emergency Department Standard Operating Procedure for: Time-Critical Transfer of the Sick or Injured Child (
LRI Emergency Department Standard Operating Procedure for: Time-Critical Transfer of the Sick or Injured Child (
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Summary of Significant Changes. Policy. Purpose. Responsibilities. Definitions
 This Management Process Description replaces MPD880/5 Copy Number Summary of Significant Changes Effective 22/09/17 Reformatting of document numbering and bullet points. Update with the new 5 hour rule
This Management Process Description replaces MPD880/5 Copy Number Summary of Significant Changes Effective 22/09/17 Reformatting of document numbering and bullet points. Update with the new 5 hour rule
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
Inverclyde Royal Hospital Major Incident Plan. May 2016 Version 1.1
 Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
TRAUMA UNIT OPERATIONAL POLICY
 TRAUMA UNIT OPERATIONAL POLICY Document Author Written By: TARN Co-ordinator Authorised Authorised By: Chief Executive Date: 28/08/2016 Date: 13 th December 2016 Lead Director: Medical Director Effective
TRAUMA UNIT OPERATIONAL POLICY Document Author Written By: TARN Co-ordinator Authorised Authorised By: Chief Executive Date: 28/08/2016 Date: 13 th December 2016 Lead Director: Medical Director Effective
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Procedure for the Application of a Cast and its subsequent care V1.3
 Procedure for the Application of a Cast and its subsequent care V1.3 May 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary...
Procedure for the Application of a Cast and its subsequent care V1.3 May 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary...
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Wales Critical Care & Trauma Network (North)
") Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Clinical Guideline Trauma Care: Accessing Trauma Services
 Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Consultation Paper. Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network
 Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Sample Template Operational Policy
 Operational Delivery s Sample Template Operational Policy October 2014 Document MTN-OP-03-10-14 Classification: General Organisation Document Purpose Title Author Operational Delivery s Guidance Sample
Operational Delivery s Sample Template Operational Policy October 2014 Document MTN-OP-03-10-14 Classification: General Organisation Document Purpose Title Author Operational Delivery s Guidance Sample
Alabama Trauma Center Designation Criteria
 2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
A. Hospital demographics
 A. Hospital demographics 1. Contact details Name of the Hospital Last name of person in charge First name of person in charge City Country 2. Demographics # of inpatient beds # of operating rooms # of
A. Hospital demographics 1. Contact details Name of the Hospital Last name of person in charge First name of person in charge City Country 2. Demographics # of inpatient beds # of operating rooms # of
Implementation of the 10 minute meeting: a user s guide
 Implementation of the 10 minute meeting: a user s guide How a short daily meeting can save lives by helping emergency teams work together more effectively. What s the issue? A critical care outreach team
Implementation of the 10 minute meeting: a user s guide How a short daily meeting can save lives by helping emergency teams work together more effectively. What s the issue? A critical care outreach team
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large
? Provision and mobilisation of large") RCH Massive Transfusion Protocol medical Dr. Helen Savoia Nicole vander Linden Mary Comande What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large amounts of blood product
RCH Massive Transfusion Protocol medical Dr. Helen Savoia Nicole vander Linden Mary Comande What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large amounts of blood product
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
DETERIORATING PATIENT & RESUSCITATION POLICY
 DETERIORATING PATIENT & RESUSCITATION POLICY Version Number: 2.3 Version date: December 2015 Policy Owner Author First approval or date last reviewed Staff/Groups Consultant Discussed by Policy Group Director
DETERIORATING PATIENT & RESUSCITATION POLICY Version Number: 2.3 Version date: December 2015 Policy Owner Author First approval or date last reviewed Staff/Groups Consultant Discussed by Policy Group Director
Organisational Audit Questions - Links to recommendations, standards and evidence
 Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Having a staging laparoscopy
 Information for patients Having a staging laparoscopy Turnberg Building Upper GI General Surgery 0161 206 5062 Page 1 of 5 This booklet has four aims: l To help you and your family become better informed
Information for patients Having a staging laparoscopy Turnberg Building Upper GI General Surgery 0161 206 5062 Page 1 of 5 This booklet has four aims: l To help you and your family become better informed
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
The impact of a flu or norovirus outbreak could have a significant impact on health and social services and could involve:
 NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
STAG TRAUMA. Quality Indicators
 STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
Implementation of Surgical Safety Checklist
 Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
ISOLATED HEAD INJURY. MODULE: Intensive Care Medicine / Trauma ALL ANAESTHETISTS, INTENSIVISTS & ED PHYSICIANS BACKGROUND:
 ISOLATED HEAD INJURY MODULE: Intensive Care Medicine / Trauma TARGET: ALL ANAESTHETISTS, INTENSIVISTS & ED PHYSICIANS BACKGROUND: Head injuries are a major cause of morbidity and mortality in children
ISOLATED HEAD INJURY MODULE: Intensive Care Medicine / Trauma TARGET: ALL ANAESTHETISTS, INTENSIVISTS & ED PHYSICIANS BACKGROUND: Head injuries are a major cause of morbidity and mortality in children
9.2 RESTRICTED NHS FORTH VALLEY. Major Emergency Plan
 RESTRICTED NHS FORTH VALLEY Major Emergency Plan IF A MAJOR INCIDENT HAS BEEN DECLARED DO NOT READ THIS PLAN NOW BUT REFER TO YOUR ACTION CARD Date of First Issue Circa 2004 Approved 31 / 01 / 2017 Current
RESTRICTED NHS FORTH VALLEY Major Emergency Plan IF A MAJOR INCIDENT HAS BEEN DECLARED DO NOT READ THIS PLAN NOW BUT REFER TO YOUR ACTION CARD Date of First Issue Circa 2004 Approved 31 / 01 / 2017 Current
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50
 Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Equivalence Guidance for GMP Domain 1
 Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
Implementation of the National Safety and Quality Health Service Standards
 Implementation of the National Safety and Quality Health Service Standards The Experience and Lessons Learnt by the Australian Council on Healthcare Standards July 2012 Introduction and overview This information
Implementation of the National Safety and Quality Health Service Standards The Experience and Lessons Learnt by the Australian Council on Healthcare Standards July 2012 Introduction and overview This information
Prone Ventilation of the Critically Ill Patient
 Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition
 Nursing Competency Workbook 6th Edition") Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee
 The Delivery Suite Shift Co-ordinator: Roles and Responsibilities (GL819) This document forms appendix 4 of the Policy document Delivery Suite Staffing (Obstetric, Anaesthetic, Paediatric and Midwifery
The Delivery Suite Shift Co-ordinator: Roles and Responsibilities (GL819) This document forms appendix 4 of the Policy document Delivery Suite Staffing (Obstetric, Anaesthetic, Paediatric and Midwifery
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
Base Hospital Advanced Life Support Program for Durham Region
 Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Mrs. Ursula McCollum Lead Resuscitation Officer Contact via Resuscitation Department extension
 RESUSCITATION POLICY August 2016 Policy Title : Author: Ownership: Mrs. Ursula McCollum Lead Resuscitation Officer Contact via Resuscitation Department extension 213901 Executive Director of Nursing /
RESUSCITATION POLICY August 2016 Policy Title : Author: Ownership: Mrs. Ursula McCollum Lead Resuscitation Officer Contact via Resuscitation Department extension 213901 Executive Director of Nursing /
North York General Hospital Policy Manual
 ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The How to Guide for Reducing Surgical Complications
 The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
Wrong site interventions
 Publication Ref: I2017/004/1 Wrong site interventions 27 November 2017 This interim bulletin contains facts which have been determined up to the time of issue. It is published to inform the NHS and the
Publication Ref: I2017/004/1 Wrong site interventions 27 November 2017 This interim bulletin contains facts which have been determined up to the time of issue. It is published to inform the NHS and the
Emergency Blood Management Plan For Blood Component Shortages. Toolkit
 Emergency Blood Management Plan For Blood Component Shortages Toolkit TABLE OF CONTENTS Terms of Reference...3 Roles and Responsibilities...5 Provincial Emergency Blood Management Plan Flowchart 7 Contingency
Emergency Blood Management Plan For Blood Component Shortages Toolkit TABLE OF CONTENTS Terms of Reference...3 Roles and Responsibilities...5 Provincial Emergency Blood Management Plan Flowchart 7 Contingency
ATLS International Promulgation Guidelines. Guidelines for International Promulgation of Advanced Trauma Life Support ATLS Course Site Visit
 Guidelines for International Promulgation of Advanced Trauma Life Support ATLS Course Site Visit Contents Front Cover Contents of guidelines 2 Definition International Promulgation 3 Selecting an appropriate
Guidelines for International Promulgation of Advanced Trauma Life Support ATLS Course Site Visit Contents Front Cover Contents of guidelines 2 Definition International Promulgation 3 Selecting an appropriate
Unannounced Theatre Inspection Report
 Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
JOB DESCRIPTION 1. JOB IDENTIFICATION
 JOB DESCRIPTION 1. JOB IDENTIFICATION Job Title: Anaesthetic/Recovery Nurse Practitioner/Operating Department Practitioner Responsible to: Theatre Senior Charge Nurse Department(s): Theatre and Recovery
JOB DESCRIPTION 1. JOB IDENTIFICATION Job Title: Anaesthetic/Recovery Nurse Practitioner/Operating Department Practitioner Responsible to: Theatre Senior Charge Nurse Department(s): Theatre and Recovery
NWL Pathology. Preparing Haematology and Blood Transfusion lab for a Major incident. Lorry Phelan MBE Site Manager Blood Sciences
 NWL Pathology Preparing Haematology and Blood Transfusion lab for a Major incident Lorry Phelan MBE Site Manager Blood Sciences NWL Pathology Definition of a major incident: A major incident or emergency
NWL Pathology Preparing Haematology and Blood Transfusion lab for a Major incident Lorry Phelan MBE Site Manager Blood Sciences NWL Pathology Definition of a major incident: A major incident or emergency
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services
 Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
Addressing ambulance handover delays: actions for local accident and emergency delivery boards
 Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
Pre Assessment Policy. Trust Policy Forum March 2004
 Policy No: OP19 Version 1.0 Name of Policy: Pre Assessment Policy Effective From: March 2004 Approved by: Trust Policy Forum March 2004 Next Review Date: March 2005 Reviewed by: This policy supercedes
Policy No: OP19 Version 1.0 Name of Policy: Pre Assessment Policy Effective From: March 2004 Approved by: Trust Policy Forum March 2004 Next Review Date: March 2005 Reviewed by: This policy supercedes
The 2013 Boston Marathon Bombings
 The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
MAJOR INCIDENT PLAN Appendix and Action Cards
 MAJOR INCIDENT PLAN Appendix and Action Cards July 2012 A B Switchboard Record of Alert Call Control Centres - Site Specific Personnel C Distribution of Action Cards 1-54 D Action Cards APPENDIX A SWITCHBOARD
MAJOR INCIDENT PLAN Appendix and Action Cards July 2012 A B Switchboard Record of Alert Call Control Centres - Site Specific Personnel C Distribution of Action Cards 1-54 D Action Cards APPENDIX A SWITCHBOARD
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy
 Policy") Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description
 National Clinical Programme Integrated Care Programme Patient Flow Job Description") TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description Mater Misericordiae University Hospital 39 hours National Rehabilitation
TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description Mater Misericordiae University Hospital 39 hours National Rehabilitation
Serious Incident Report Public Board Meeting 26 November 2015
 Serious Incident Report Public Board Meeting 26 November 2015 Presented for: Presented by: Author Previous Committees Governance Yvette Oade, Chief Medical Officer Craig Brigg, Director of Quality None
Serious Incident Report Public Board Meeting 26 November 2015 Presented for: Presented by: Author Previous Committees Governance Yvette Oade, Chief Medical Officer Craig Brigg, Director of Quality None
Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital
 Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital Name: Start Date:. Mentor:. Introduction My name is Helen McCallum; I am the Clinical Skills Facilitator for St Marys Theatres. I would
Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital Name: Start Date:. Mentor:. Introduction My name is Helen McCallum; I am the Clinical Skills Facilitator for St Marys Theatres. I would
Guidelines on the Handover of Responsibility of an. Anaesthesiologist
 The Hong Kong College of s Page 1 of 5 Guidelines on the Handover of Responsibility of an Version Effective Date 1 MAY 1994 (reviewed Feb 2002) 2 JUL 2013 Document No. HKCA P12 v2 Prepared by College Guidelines
The Hong Kong College of s Page 1 of 5 Guidelines on the Handover of Responsibility of an Version Effective Date 1 MAY 1994 (reviewed Feb 2002) 2 JUL 2013 Document No. HKCA P12 v2 Prepared by College Guidelines
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Register No: Status: Public
 Care of the Critically Ill Child Clinical Guideline Register No: 16025 Status: Public Developed in response to: Best practice Contributes to CQC Fundamental Standard 9, 12 Consulted With Post/Committee/Group
Care of the Critically Ill Child Clinical Guideline Register No: 16025 Status: Public Developed in response to: Best practice Contributes to CQC Fundamental Standard 9, 12 Consulted With Post/Committee/Group
Trauma Care Network News. West Midlands Major Trauma Clinical Lead appointed. Inside Issue 3. Issue 3
 Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Level 3 Trauma Hospital Criteria
 Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Morton s neuroma. If you have any further questions, please speak to a doctor or nurse caring for you.
 Morton s neuroma This leaflet aims to answer your questions about having surgery for Morton s neuroma. It explains the benefits, risks and alternatives, as well as what you can expect when you come to
Morton s neuroma This leaflet aims to answer your questions about having surgery for Morton s neuroma. It explains the benefits, risks and alternatives, as well as what you can expect when you come to
Mediastinal Venogram and Stent Insertion
 Mediastinal Venogram and Stent Insertion Radiology Department Patient information leaflet This leaflet tells you about the procedure known as a mediastinal venogram. It explains what is involved and the
Mediastinal Venogram and Stent Insertion Radiology Department Patient information leaflet This leaflet tells you about the procedure known as a mediastinal venogram. It explains what is involved and the
Pre-operative categorization (triaging) of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency
 of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency") Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Returning to work after a period of absence
 Introduction Doctors may be away from their normal working environment for many reasons and these periods can extend from months to years. This guidance is directed at anaesthetists returning to anaesthesia
Introduction Doctors may be away from their normal working environment for many reasons and these periods can extend from months to years. This guidance is directed at anaesthetists returning to anaesthesia
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Resuscitation Council (UK) Guidelines for the use of Automated External Defibrillators SUPERSEDED
 Guidelines for the use of Automated External Defibrillators SUPERSEDED") Page 1 of 7 Resuscitation Council (UK) Guidelines for the use of Automated External Defibrillators Resuscitation Guidelines 2000 Contents 1. Introduction 2. The 'chain of survival' concept 3. Recommendations
Page 1 of 7 Resuscitation Council (UK) Guidelines for the use of Automated External Defibrillators Resuscitation Guidelines 2000 Contents 1. Introduction 2. The 'chain of survival' concept 3. Recommendations
Roles and responsibilities of adult/paediatric cardiac arrest bleep holders: QMC/City Campus
 Roles and responsibilities of adult/paediatric cardiac arrest bleep holders: QMC/City Campus Who should attend a 2222 cardiac arrest call? There are 2 types of responders to adult/paediatric cardiac arrest
Roles and responsibilities of adult/paediatric cardiac arrest bleep holders: QMC/City Campus Who should attend a 2222 cardiac arrest call? There are 2 types of responders to adult/paediatric cardiac arrest
Nursing Practice Committee
 Nursing Practice Committee Standard Operating Procedure on Patient preparation and Admission to Operating Theatre Author: Emma Cooney CNM 3 & Rosemary Clerkin CNF Issue Date: March 2010 Review Date: March
Nursing Practice Committee Standard Operating Procedure on Patient preparation and Admission to Operating Theatre Author: Emma Cooney CNM 3 & Rosemary Clerkin CNF Issue Date: March 2010 Review Date: March
Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI Section 4.13 INCIDENT COMMAND MANAGEMENT
 Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI 49646 Section 4.13 INCIDENT COMMAND MANAGEMENT The purpose of an Incident Command Management System
Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI 49646 Section 4.13 INCIDENT COMMAND MANAGEMENT The purpose of an Incident Command Management System
Z: Perioperative Nursing Specialty
 Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
ANTERIOR RESECTION WHAT ARE THE BENEFITS OF HAVING AN ANTERIOR RESECTION?
 WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
PLANNED CARE THEATRE OPERATIONAL POLICY
 PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units
 Page 1 of 7 Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units Version Effective Date 1 Oct 1992 (reviewed Feb 02) 2 Nov 2011 3 Dec 2016 Document No. HKCA T3 v3 Prepared
Page 1 of 7 Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units Version Effective Date 1 Oct 1992 (reviewed Feb 02) 2 Nov 2011 3 Dec 2016 Document No. HKCA T3 v3 Prepared
Severn & Peninsula Major Trauma Networks
 Severn & Peninsula Major Trauma Networks Paediatric Major Trauma Centre Acceptance Policy May 2014, V3 REVIEW DISTRIBUTION APPROVAL/ADOPTED 6 months after formal approval and then annually Severn major
Severn & Peninsula Major Trauma Networks Paediatric Major Trauma Centre Acceptance Policy May 2014, V3 REVIEW DISTRIBUTION APPROVAL/ADOPTED 6 months after formal approval and then annually Severn major
Committees / Group Date Consultation: Risk Management Sub Committee Nov 2016
 Title of Standard Operation Procedure: ocedure: Person(s) responsible for the production of report First Aid at Work Procedure Health and Safety Manager Reference Number: H&S Procedure 22 Version No: 2
Title of Standard Operation Procedure: ocedure: Person(s) responsible for the production of report First Aid at Work Procedure Health and Safety Manager Reference Number: H&S Procedure 22 Version No: 2
Acutely ill patients in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
41 EC Emergency Planning Toolkit Action Cards
 41 EC Emergency Planning Toolkit Action Cards Policy number: 41 EC Version 2.1 Approved by Name of author/originator Owner (director) Executive Director Date of approval August 2014 Samantha Chalmers,
41 EC Emergency Planning Toolkit Action Cards Policy number: 41 EC Version 2.1 Approved by Name of author/originator Owner (director) Executive Director Date of approval August 2014 Samantha Chalmers,
ADMINISTRATION OF FIRST AID POLICY
 ADMINISTRATION OF FIRST AID POLICY Mandatory Quality Area 2 PURPOSE This policy will provide guidelines for the administration of first aid at DNMK. POLICY STATEMENT 1. VALUES DNMK is committed to: providing
ADMINISTRATION OF FIRST AID POLICY Mandatory Quality Area 2 PURPOSE This policy will provide guidelines for the administration of first aid at DNMK. POLICY STATEMENT 1. VALUES DNMK is committed to: providing
Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN
 Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN Adopted January 2000 Revised February 2008 TABLE OF CONTENTS 1.0 Purpose 2.0 Policy 3.0 Definitions 4.0 Organizations Affected 5.0 Standard
Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN Adopted January 2000 Revised February 2008 TABLE OF CONTENTS 1.0 Purpose 2.0 Policy 3.0 Definitions 4.0 Organizations Affected 5.0 Standard
Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients
 UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
Your Child is having an Operation
 Department of Paediatrics Your Child is having an Operation Patient Information Leaflet This information leaflet explains what to expect when your child comes into hospital to have an operation or investigation
Department of Paediatrics Your Child is having an Operation Patient Information Leaflet This information leaflet explains what to expect when your child comes into hospital to have an operation or investigation