|
|
|
- Clifford Dalton
- 5 years ago
- Views:
Transcription
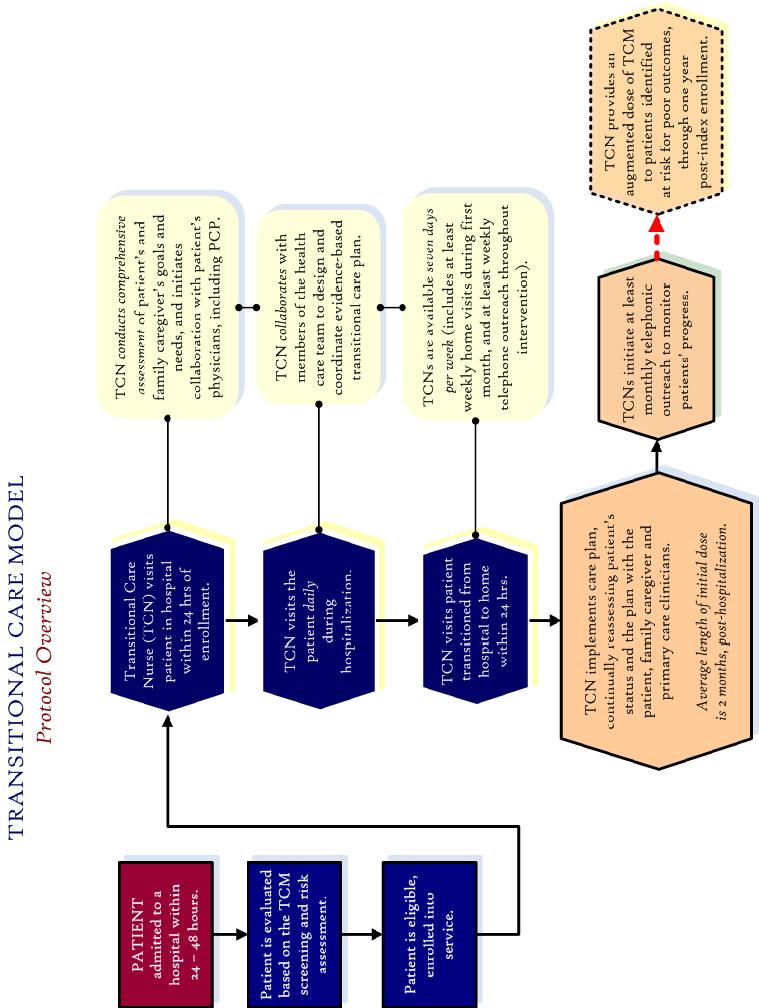
1 OVERVIEW The Transitional Care Model (TCM) provides comprehensive in-hospital planning and home follow-up for chronically ill high-risk older adults hospitalized for common medical and surgical conditions. For the millions of Americans who suffer from multiple chronic conditions and complex therapeutic regimens, TCM emphasizes coordination and continuity of care, prevention and avoidance of complications, and close clinical treatment and management all accomplished with the active engagement of patients and their family and informal caregivers and in collaboration with the patient s physicians. Because TCM focuses on individualized, multidisciplinary evidence-based clinical protocols that prevent decline and reduce readmission for an extended period, TCM complements primary care provided by regular physicians, telephonic case management programs or disease management programs that focus only on one health conditions. Promoting the use of TCM by a health care system is achieved through the following: 1) effectively communicating the value of the model to key stakeholders; 2) integrating and adapting the model to fit the mission and goals of each organization; 3) recruiting, orienting and preparing transitional care nurses and patient recruiter to implement the model; 4) providing ongoing clinical and technical support to these staff; 5) quality monitoring and quality improvement; and 6) conducting a comprehensive evaluation.
2
3 TRANSITIONAL CARE NURSE (TCN) CARE PROTOCOL Schedule of TCN Visits Findings from our three completed RCT s have informed the development of the TCN schedule: patients will be visited within 24 hours of study enrollment; at least daily throughout hospitalization (using clinical judgment for visits on Sundays and for those with long length of hospital stays, as needed); within 24 hours of discharge to home (from hospital or from skilled nursing facility [SNF]); at least weekly during the first month post-discharge from hospital to SNF (if applicable); and, at least semi-monthly through the duration of the intervention. Hospital visits are expected to range from 15 to 60 minutes, home care visits 30 to 60 minutes, and telephone contacts 5 to 20 minutes, with initial hospital and home visits lasting longest. While the proposed schedule defines minimal expectations, TCNs will use their clinical judgment to determine the frequency (number) and intensity (length) of patient and caregiver visits and telephone contacts. Hospital Component The primary purposes of hospital contacts are to: establish a trusting relationships with the patient and caregiver, develop individualized plans of care in collaboration with the patient and caregiver and the patient s physician, and initiate implementation of the individualized, collaborative plans. Post-discharge Component The home component will begin immediately following hospital discharge to home. Based on prior work, it is estimated that about 10% of patients may be discharged to a nursing home or rehabilitation center for short-term post-acute services (one to three weeks). TCNs will continue to implement the protocol with the patient while in the SNF setting and on transfer to home. The length intervention will not extend due to a SNF stay. Home Follow-up Visit: In addition to assessing the effects of transition from hospital to home on the overall health status of the patient and the emotional status of the caregiver, TCNs will assure that patients/caregivers understand and have access to all prescribed post-discharge therapies and are environmentally safe. Patients should be seen within 24 hours of discharge from hospital to home, or from SNF to home, with any variation documented in the patient chart. TCNs will play a major role in coordinating care provided by others and promoting access to health and community resources. During the intervention, TCNs will promote patients adaptation by focusing on: managing risk factors to prevent further decline;
4 managing problem behaviors; assessing and managing physical symptoms; preventing functional decline; managing depression; promoting adherence to therapies; assuring proper medical management; validating knowledge and skills; and reducing caregiver burden. SNF Visit (when applicable): In addition to assessing the effects of transition from hospital to SNF and improve the management of the overall health of the patient, TCNs will work actively to ensure that patients/caregivers understand and have access to all prescribed post-discharge therapies and are environmentally safe. Patients should be seen within 24 hours of discharge from hospital to SNF. TCNs will work actively to establish a productive working relationship with the SNF staff providing care for the patient (e.g., nursing staff, social worker, physician, nutritionist, etc.) to provide input and assist in coordinating the transition from the hospital to the SNF and to home. TCNs will be in contact with the SNF staff and the patient and/or caregiver via telephone or visit at least weekly during the SNF stay. Frequency of actual visits is expected to increase during the time of transition from the hospital to the SNF and at the time of transition from the SNF back to the patient s home. During the intervention time at the SNF, TCNs will promote patients adaptation by focusing on: managing risk factors to prevent further decline; managing problem behaviors; assessing and managing physical symptoms; preventing functional decline; managing depression; promoting adherence to therapies; advocating to implement proper medical management; validating knowledge and skills; and reducing caregiver burden. Weekend Coverage: Weekend coverage consists minimally of 4 hours of telephonic coverage on Saturday and Sunday. Each TCN is responsible for signing off to the covering TCN on Friday. The TCN covering the weekend will follow up on any patient needs and use their clinical judgment to determine if any visits need to occur. Any patients discharged on Friday or Saturday will be seen within 24 hours of discharge. If a patient is discharged to a SNF/rehab the first visit can be delayed to Monday of the next week. Hospitalized patients are to be seen minimally one day of the weekend, with the TCN exercising their clinical judgment if a second weekend visit is necessary.
5 Prior to the weekend, each TCN s should visit all high risk patients on Friday as late in the day as possible. Any major issues or concerns for high risk patients should be documented and communicated to the weekend covering TCN. Telephone Availability: Daily telephone availability of the TCNs will extend from the index hospital admission through the duration of the intervention. TCNs will be available from 8AM to 8PM Mondays through Fridays and 8AM to noon (or alternative 4 hour segments on each day) on weekends to respond to patients /caregivers needs and concerns. Patients and caregivers will be provided with a written plan with instructions for emergency care. Phone contacts will be made by the TCN during any week that a patient is not visited at home. The purposes of these calls will range from monitoring patient s health status to reinforcing caregiver s skill acquisition. Discharging the Patient and Caregiver TCNs will use their clinical judgment to determine the length of intervention for each patient. Based on prior research with a similar population, termination of the intervention will be guided by the following criteria: goals identified by patients and caregivers and related to managing the acute episode of illness and transitioning to home are met; the patient is medically stable; the caregiver is able to identify early symptoms that require intervention; and the caregiver knows how to intervene to prevent poor outcomes. By the completion of the intervention, the TCN will have arranged for any necessary follow-up care in consultation with the patient/caregiver and patient s physician. A discharge letter will be written to the physician formally discharging the patient, stating attained goals, general impression, discharge medications, recommendations and issues requiring follow-up (if needed) with additional providers copied to assure continuity of care. A separate patient/caregiver discharge letter will be written reinforcing goals attained, strategies developed, emergency plan and reminders to patient re: agreed plan of care.
6 SCREENING CRITERIA & RISK ASSESSMENT Are the following statements true for the patient: Admitted to hospital within the last hours? 65 years of age or older? English speaking? Reachable by telephone? Alert and cognitively intact? (see Instruments, SPMSQ >6) Documented history of a primary cardiovascular, respiratory, endocrine, or orthopedic health problem? Does not have end-stage renal disease? Does not have primary neurological diagnosis? Does not have major psychiatric illness? Does not have a primary diagnosis of cancer? Lives within 30 miles of the admitted facility? Returning home after discharge (SNF/rehab stay < 3 weeks)? If yes to all of the above, does the patient have two (or more) of the following risk factors: Age 80 or older Moderate to severe functional deficits History of mental/emotional illness Four or more active co-existing health conditions Six or more prescribed medications Two or more hospitalizations within past 6 months Hospitalization in the past 30 days Inadequate support system Poor self-rating of health Documented history of non-adherence to therapeutic regimen PATIENT DATA Patient data is collected from patients, caregivers (as identified by the patient), or medical records, including: sociodemographics caregiver involvement and availability physical data general health status severity of illness illness specific data number of prescribed daily medications health resources (utilization activity prior to hospitalization)
7 ASSESSMENT TOOLS Short Portable Mental Status Questionnaire (SPMSQ): The SPMSQ measures intellectual function by assessing response to 10 items. The questionnaire is scored correct or incorrect. Scores range from 0-10 with a higher number indicating higher intellectual function. Adjustment for educational attainment can be made to allow one more error for a subject with only a grade school education, and allow one less error for a subject with education beyond high school. Geriatric Depression Scale (GDS): Fifteen item self-report instrument in a "yes" or "no" format that takes 5-10 minutes to administer. Developed specifically for the elderly and standardized on elderly samples. Contains few somatically-based items and has had extensive psychometric testing. Validity was established by correlation with both diagnostic clinical ratings and other self-report measures of depression. Scores of 0-5 are normal for non depressed responders; scores of 6-10 indicate mild depression; and 11-15, moderate to severe depression. Instrumental Activities of Daily Living (Lawton s IADL): Lawton's IADL is used to measure ability to perform money and medication management, shopping, and household chores. On completion, a lower score equates with worsening function. Katz Activities of Daily Living (Katz ADL): Katz ADL index measures ability to conduct selfcare. This six-item instrument assesses independence or dependence in the activities of bathing, dressing, toileting, transferring, continence and feeding. Scores range from 0-6, with lower scores indicating more disability. Overall Quality of Life (QoL): Overall QoL is measured by a respondent s self-report of current quality of life in answer to the question: "How would you rate your quality of life? Response choices are "excellent", "very good", "good", "fair", or "bad". High correlation has been demonstrated between perceived and actual quality of life and outcomes. Subjective Health Rating: Self assessment of health measures the respondent s perception of his/her overall health using a single item question: "How would you rate your overall health at the present time?" Responses are recorded as "excellent", "good", "fair", or "poor". Highly significant correlations have been reported between self-reports and physician ratings of health status. Symptom Bother Scale: Measures the presence and severity of 13 physical symptoms typically associated with aging and chronic illness (e.g., pain, aches, itching). Patients will rate the absence or presence of a specific symptom. If a symptom is present, they will further rank the degree to which they were bothered by each symptom on a 1 to 3 scale, with higher scores indicating worse symptoms. Symptom bother was positively associated with difficulty with ADLs and depression, and negatively associated with subjective health, providing support for the validity of the scale. The Mini Mental State Exam (MMSE): MMSE is a widely used tool that measures orientation to time and place, recall ability, short-term memory and arithmetic ability in elderly patients. It consists of 30 questions. The MMSE total score ranges from 0 to 30 and reflects the number of correct responses. In general, scores > 23 indicate intact cognition, mild CI, moderate CI and < 12 severe CI. However, cutoff scores will be modulated according to educational level. This instrument is easily administered, well tolerated and can be completed within 5-10 minutes. It is a useful adjunct to the SPMSQ if the score lower than expected, or contradicts other assessment data.
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO
 FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
STROKE REHAB PROGRAM
 STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Guidelines for Physiatric Practice and Inpatient Review Criteria
 Guidelines for Physiatric Practice and Inpatient Review Criteria Table of Contents PART I: GUIDELINES Guidelines for Physiatric Practice PART II: INPATIENT REVIEW Instructions: Pre-admission or Admission
Guidelines for Physiatric Practice and Inpatient Review Criteria Table of Contents PART I: GUIDELINES Guidelines for Physiatric Practice PART II: INPATIENT REVIEW Instructions: Pre-admission or Admission
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
The Use of interrai scales- ways of summarizing interrai data
 The Use of interrai scales- ways of summarizing interrai data Katherine Berg PhD PT Chair, Department of Physical Therapy Chair, Graduate Department of Rehabilitation Science University of Toronto K Berg
The Use of interrai scales- ways of summarizing interrai data Katherine Berg PhD PT Chair, Department of Physical Therapy Chair, Graduate Department of Rehabilitation Science University of Toronto K Berg
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Caregiving: Health Effects, Treatments, and Future Directions
 Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SKILLED NURSING SERVICES
 DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
Evidence Based Practice. Dorothea Orem s Self Care Deficit Theory
 Evidence Based Practice Dorothea Orem s Self Care Deficit Theory Self Care Deficit Theory Theory Overview The question What is the condition that indicates that a person needs nursing care? was the basis
Evidence Based Practice Dorothea Orem s Self Care Deficit Theory Self Care Deficit Theory Theory Overview The question What is the condition that indicates that a person needs nursing care? was the basis
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE
 Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 09 MEDICAL CARE PROGRAMS Chapter 07 Medical Day Care Services Authority: Health-General Article, 2-104(b), 15-103, 15-105, and 15-111, Annotated
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 09 MEDICAL CARE PROGRAMS Chapter 07 Medical Day Care Services Authority: Health-General Article, 2-104(b), 15-103, 15-105, and 15-111, Annotated
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
11/13/2017. Thank You to Our Sponsors. Evaluations & CE Credits. University at Albany School of Public Health. New York State Department of Health
 Thank You to Our Sponsors University at Albany School of Public Health New York State Department of Health NYSACHO Evaluations & CE Credits Nursing Contact Hours, CME, CHES and Social Work credits are
Thank You to Our Sponsors University at Albany School of Public Health New York State Department of Health NYSACHO Evaluations & CE Credits Nursing Contact Hours, CME, CHES and Social Work credits are
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Attending Physician Statement- Total and Permanent Disability
 Instruction to doctor: This patient is insured with us against the happening of certain contingent events associated with his health. A claim has been submitted in connection with Total and Permanent Disability
Instruction to doctor: This patient is insured with us against the happening of certain contingent events associated with his health. A claim has been submitted in connection with Total and Permanent Disability
PPS Therapy. Medicare 2/28/ year Home Health clinician/contractor. 30 years Geriatric Rehab. Home Health consultant, author, speaker
 PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
Documentation. The learner will be able to :
 Functional Decline in Hospice Assessment, Intervention, & Objectives The learner will be able to : Assess functional decline utilizing appropriate evidence based tools Document functional indicators and
Functional Decline in Hospice Assessment, Intervention, & Objectives The learner will be able to : Assess functional decline utilizing appropriate evidence based tools Document functional indicators and
UNIT DESCRIPTIONS. 2 North Musculoskeletal Rehabilitative Care
 UNIT DESCRIPTIONS 2 North Musculoskeletal Rehabilitative Care Musculoskeletal Rehabilitation The Musculoskeletal Service provides rehabilitation following multiple trauma, or orthopaedic surgery (primarily
UNIT DESCRIPTIONS 2 North Musculoskeletal Rehabilitative Care Musculoskeletal Rehabilitation The Musculoskeletal Service provides rehabilitation following multiple trauma, or orthopaedic surgery (primarily
GROUP LONG TERM CARE FROM CNA
 GROUP LONG TERM CARE FROM CNA Valdosta State University Voluntary Plan Pays benefits for professional treatment at home or in a nursing home GB Table of Contents Thinking Long Term in a Changing World
GROUP LONG TERM CARE FROM CNA Valdosta State University Voluntary Plan Pays benefits for professional treatment at home or in a nursing home GB Table of Contents Thinking Long Term in a Changing World
Behavioral Health Initial Review Form
 Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
Exhibit A. Part 1 Statement of Work
 Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Long Term Care (LTC) Facility Authorization Request
 Facility Authorization Request") State of Alaska Department of Health and Social Services Senior and Disabilities Services Long Term Care (LTC) Facility Authorization Request This form may be completed by hospital discharge staff or a
State of Alaska Department of Health and Social Services Senior and Disabilities Services Long Term Care (LTC) Facility Authorization Request This form may be completed by hospital discharge staff or a
Statistical Portrait of Caregivers in the US Part III: Caregivers Physical and Emotional Health; Use of Support Services and Technology
 Statistical Portrait of Caregivers in the US Part III: Caregivers Physical and Emotional Health; Use of Support Services and Technology [Note: This fact sheet is the third in a three-part FCA Fact Sheet
Statistical Portrait of Caregivers in the US Part III: Caregivers Physical and Emotional Health; Use of Support Services and Technology [Note: This fact sheet is the third in a three-part FCA Fact Sheet
UTILIZATION MANAGEMENT AND CARE COORDINATION Section 8
 Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
An Initiative to Improve Patient Discharge Satisfaction
 An Initiative to Improve Patient Discharge Satisfaction Speaker Disclosure Statement Sally Strong, RN, APN-CNS, CNRN, CRRN Clinical Nurse Specialist Marianjoy Rehabilitation Hospital Adjunct Faculty Elmhurst
An Initiative to Improve Patient Discharge Satisfaction Speaker Disclosure Statement Sally Strong, RN, APN-CNS, CNRN, CRRN Clinical Nurse Specialist Marianjoy Rehabilitation Hospital Adjunct Faculty Elmhurst
MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY
 OPTUM MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY Guideline Number: Effective Date: June, 2017 INTRODUCTION
OPTUM MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY Guideline Number: Effective Date: June, 2017 INTRODUCTION
Today s educational presentation is provided by. The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE
 Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Dialectical Behavioral Therapy (DBT) Level of Care Guidelines
 Level of Care Guidelines") Page 1 of 5 Category: Code: Subject: Purpose: Policy: Utilization Management Dialectical Behavioral Therapy () Level of Care Guidelines The purpose of this policy is to describe the criteria used by BHP
Page 1 of 5 Category: Code: Subject: Purpose: Policy: Utilization Management Dialectical Behavioral Therapy () Level of Care Guidelines The purpose of this policy is to describe the criteria used by BHP
Guidelines for Psychiatric Practice in Public Sector Psychiatric Inpatient Facilities RESOURCE DOCUMENT
 Guidelines for Psychiatric Practice in Public Sector Psychiatric Inpatient Facilities RESOURCE DOCUMENT Approved by the Board of Trustees, December 1993 The findings, opinions, and conclusions of this
Guidelines for Psychiatric Practice in Public Sector Psychiatric Inpatient Facilities RESOURCE DOCUMENT Approved by the Board of Trustees, December 1993 The findings, opinions, and conclusions of this
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Key points. Home Care agency structures. Introduction to Physical Therapy in the Home Care Setting. Home care industry
 Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Test Content Outline Effective Date: December 23, 2015
 Board Certification Examination There are 200 questions on this examination. Of these, 175 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Board Certification Examination There are 200 questions on this examination. Of these, 175 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
A1600 A1800: Most Recent Admission/Entry or Reentry into this Facility
 A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab
 Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
DoDNA WOUNDED, ILL, AND INJURED SENIOR OVERSIGHT COMMITTEE 4000 DEFENSE PENTAGON WASHINGTON, DC 20301
 DoDNA WOUNDED, ILL, AND INJURED SENIOR OVERSIGHT COMMITTEE 4000 DEFENSE PENTAGON WASHINGTON, DC 20301 orc 1 0 2008 MEMORANDUM FOR SECRETARIES OF THE MILITARY DEPARTMENTS UNDERSECRETARY FOR HEALTH (VETERANS
DoDNA WOUNDED, ILL, AND INJURED SENIOR OVERSIGHT COMMITTEE 4000 DEFENSE PENTAGON WASHINGTON, DC 20301 orc 1 0 2008 MEMORANDUM FOR SECRETARIES OF THE MILITARY DEPARTMENTS UNDERSECRETARY FOR HEALTH (VETERANS
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Care for Older Adults (COA)
") Q: Which members are included in the sample? Adults 66 years and older who had each of the following in 2016: ; Advance care planning ; Medication review ; Functional status assessment ; Pain assessment
Q: Which members are included in the sample? Adults 66 years and older who had each of the following in 2016: ; Advance care planning ; Medication review ; Functional status assessment ; Pain assessment
CGS Administrators, LLC Clinical Hospice Documentation from CGS Missouri Hospice & Palliative Care Assoc. October 3, 2016
 Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Needs-based population segmentation
 Needs-based population segmentation David Matchar, MD, FACP, FAMS Duke Medicine (General Internal Medicine) Duke-NUS Medical School (Health Services and Systems Research) Service mismatch: Many beds filled
Needs-based population segmentation David Matchar, MD, FACP, FAMS Duke Medicine (General Internal Medicine) Duke-NUS Medical School (Health Services and Systems Research) Service mismatch: Many beds filled
Medication Management: Therapy Scope Versus Comfort Level
 Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
8/1/2017. Services and Description
 Index of CPT Codes for Medical Home The following index was originally published in November 2003 in Medical Home Crosswalk To Reimbursement. The information was developed by Margaret McManus, Alan Kohrt,
Index of CPT Codes for Medical Home The following index was originally published in November 2003 in Medical Home Crosswalk To Reimbursement. The information was developed by Margaret McManus, Alan Kohrt,
Pain Transition Planning. University of Illinois at Chicago
 Pain Transition Planning University of Illinois at Chicago Purpose To present a transition plan for a participant with pain. Included examples of a plan that can be adapted for participants with pain.
Pain Transition Planning University of Illinois at Chicago Purpose To present a transition plan for a participant with pain. Included examples of a plan that can be adapted for participants with pain.
Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey -
 Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT
 JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT 1. INITIAL CREDENTIALING, PSYCHIATRISTS Completion
JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT 1. INITIAL CREDENTIALING, PSYCHIATRISTS Completion
LONG TERM CARE SETTINGS
 LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Telehealth. Administrative Process. Coverage. Indications that are covered
 Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Community Health Services in Bristol Community Learning Disabilities Team
 Community Health Services in Bristol 2014 Community Learning Disabilities Team This provides specialist community based services for adults with learning difficulties and help to promote equal access to
Community Health Services in Bristol 2014 Community Learning Disabilities Team This provides specialist community based services for adults with learning difficulties and help to promote equal access to
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Szanton, S. L., Thorpe, R. J., Boyd, C., Tanner, E. K., Leff, B., Agree, E., & Gitlin, L. N. (2011). Community aging in place, advancing better living for elders: A bio-behavioralenvironmental
CRITICALLY APPRAISED PAPER (CAP) Szanton, S. L., Thorpe, R. J., Boyd, C., Tanner, E. K., Leff, B., Agree, E., & Gitlin, L. N. (2011). Community aging in place, advancing better living for elders: A bio-behavioralenvironmental
Hospice Discharges. Legacy Hospice
 Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
NJ Level of Care and Assessment Process
 NJ Level of Care and Assessment Process CODING GUIDELINES AND LEVEL OF CARE Cheryl Hogan Division of Aging Services NJ Department of Human Services 1 5/28/2014 Goals To understand the assessment process
NJ Level of Care and Assessment Process CODING GUIDELINES AND LEVEL OF CARE Cheryl Hogan Division of Aging Services NJ Department of Human Services 1 5/28/2014 Goals To understand the assessment process
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Home Health Eligibility Requirements
 Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists
 DECLINE Facility Assessment Checklists") ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program
 INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
Palliative and Hospice Care In the United States Jean Root, DO
 Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Reference materials are provided with the criteria and should be used to assist in the correct interpretation of the criteria.
 InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
Care Model for Tufts Health Plan Senior Care Options
 Care Model for Tufts Health Plan Senior Care Options Tufts Health Plan Core Principles The overarching construct for the Tufts Health Plan Senior Care Options (SCO-SNP) is to improve access to medical,
Care Model for Tufts Health Plan Senior Care Options Tufts Health Plan Core Principles The overarching construct for the Tufts Health Plan Senior Care Options (SCO-SNP) is to improve access to medical,
2018 PROVIDER TOOLKIT
 1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medications: Defining the Role and Responsibility of Physical Therapy Practice
 This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
This article is based on a presentation by Matt Janes, PT, DPT, MHS, OCS, CSCS, Division AVP, Therapy Practice and Quality, Kindred at Home, and Diana Kornetti, PT, MA, HCS-D, President, Home Health Section
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Supplementary Online Content
 Supplementary Online Content Buurman BM, Parlevliet JL, Allore HG, et al. Comprehensive geriatric assessment and transitional care in acutely hospitalized patients: the Transitional Care Bridge Randomized
Supplementary Online Content Buurman BM, Parlevliet JL, Allore HG, et al. Comprehensive geriatric assessment and transitional care in acutely hospitalized patients: the Transitional Care Bridge Randomized
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Chapter 6: Nursing Process in Mental Health. Multiple Choice Identify the choice that best completes the statement or answers the question.
 Instant download and all chapters Test Bank Neebs Fundamentals of Mental Health Nursing 4th Edition Linda M. Gorman https://testbanklab.com/download/test-bank-neebs-fundamentals-mental-health-nursing-4thedition-linda-m-gorman/
Instant download and all chapters Test Bank Neebs Fundamentals of Mental Health Nursing 4th Edition Linda M. Gorman https://testbanklab.com/download/test-bank-neebs-fundamentals-mental-health-nursing-4thedition-linda-m-gorman/
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service
 WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
OUTPATIENT SERVICES. Components of Service
 OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
10/3/2016 PALLIATIVE CARE WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION. What, Who, Where and When
 PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
Personal Support Worker
 PROGRAM OBJECTIVES The Personal Support Worker program prepares students to deliver appropriate short or longterm care assistance and support services in either a long-term care facility, acute care facility,
PROGRAM OBJECTIVES The Personal Support Worker program prepares students to deliver appropriate short or longterm care assistance and support services in either a long-term care facility, acute care facility,
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
CARE FOR OLDER ADULTS (COA)
") CARE FOR OLDER ADULTS (COA) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE HEDIS (Hybrid) To assess the percentage of adults ages 66 years and
CARE FOR OLDER ADULTS (COA) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE HEDIS (Hybrid) To assess the percentage of adults ages 66 years and
Overview of the Prior Authorization Process for Home Health Aide Services. June 27, 2018
 Overview of the Prior Authorization Process for Home Health Aide Services June 27, 2018 Objectives Understand the HUSKY Health program s Prior Authorization (PA) process for home health aide (HHA) services
Overview of the Prior Authorization Process for Home Health Aide Services June 27, 2018 Objectives Understand the HUSKY Health program s Prior Authorization (PA) process for home health aide (HHA) services
Oxford Condition Management Programs:
 Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Basic Covered Benefits and Services
 Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
Michelle P Waiver Training
 Michelle P Waiver Training Presented by Department for Medicaid Services and Department for Mental Health, Developmental Disabilities and Addiction Services 1 Workshop Outline I. History and Overview of
Michelle P Waiver Training Presented by Department for Medicaid Services and Department for Mental Health, Developmental Disabilities and Addiction Services 1 Workshop Outline I. History and Overview of
INSTRUCTIONS FOR SUBMITTING EXPERT TESTIMONY BY ANSWERS TO WRITTEN DEPOSITION
 INSTRUCTIONS FOR SUBMITTING EXPERT TESTIMONY BY ANSWERS TO WRITTEN DEPOSITION To establish incapacity, the petitioner must present testimony from an individual qualified by training and experience in evaluating
INSTRUCTIONS FOR SUBMITTING EXPERT TESTIMONY BY ANSWERS TO WRITTEN DEPOSITION To establish incapacity, the petitioner must present testimony from an individual qualified by training and experience in evaluating
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified