Definition of Seclusion
|
|
|
- Deirdre Freeman
- 5 years ago
- Views:
Transcription
1 Definition of Seclusion The involuntary confinement of a patient ALONE in a room or area from which the patient is physically prevented from leaving This now must be ordered for patients confined to a room by a one to one, unless for suicide observation.

2 Definition of Chemical Restraints Medications are Chemical Restraints when They are used as a restriction to manage the patient s freedom of movement and is NOT a standard treatment or dosage for the patient s condition
3 When is a Restraint Appropriate? To ensure the immediate physical safety of the patient, a staff member or others When less restrictive interventions have been determined to be ineffective to protect the patient, staff member or other from harm in accordance with a written modification to the patient s plan of care when the type or technique is the least restrictive intervention that will be effective to protect the patient or others from harm in accordance with safe and appropriate restraint techniques as determined by the hospital policy
4 Involving family When appropriate, discuss with family when restraints are or maybe needed Invite their ideas for ways the prevent the need for restraints
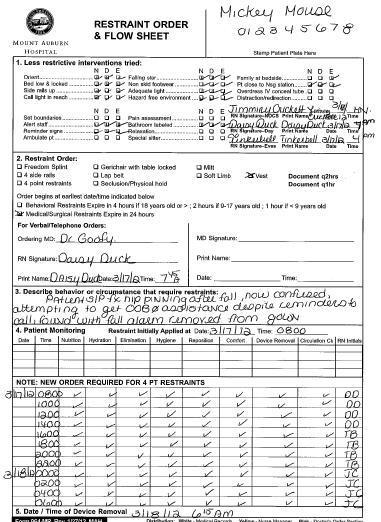
5 Med Surg Safety Restraint Orders obtain the order BEFORE applying a restraint orders must be written prior to the restraint and Q 24hrs Monitoring Q2hrs when used in NON-Violent/Non Self-destructive patients Nutrition Elimination Repositioning Device removal Hydration Hygiene Comfort Circulation
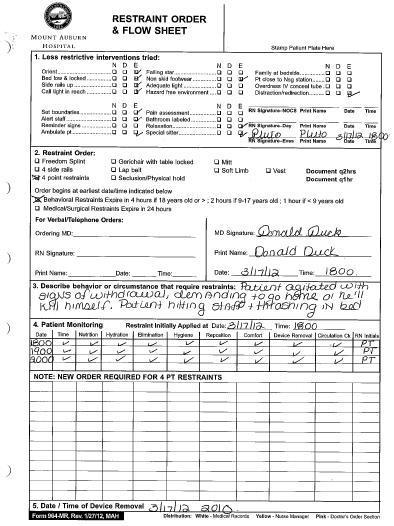
6 Behavioral Restraints Orders For Violent Patients: Restraints can be initiated prior to getting an order ONLY when there is a clear and immediate danger to a patient or staff. (as in the case of a violent/self destructive patient) An order must be obtained as soon as possible and a face to face evaluation of the patient must occur within 1 hour For Violent /Self Destructive Patients: The Licensed independent practitioner MUST see the patient within 1 hour to: Evaluation the immediate situation Patients reaction to the intervention Evaluation their medical and behavioral condition Determine the need to continue or terminate the restraint
7 Behavioral Restraints The order is good for only 4 hours for an adult, 2 hours for ages 9-17 and 1 hour for under the age of 9 There must be a FACE to FACE reevaluation of the patient at least every 8 hours Q15min for Violent/Self Destructive patients Signs of injury Nutrition Hydration Circulation ROM Hygiene Elimination By Observation worker The nurse must assess the patient as often as necessary but the above assessments, the patients physical and psychological status, and readiness for discontinuation of restraints must be made Q1hr
8 Restraint Orders May be ordered by a licensed independent practitioner who is responsible for the patient s care The attending physician must be consulted as soon as possible if they did not write the order Restraints can be initiated (before receiving an order (as determined by hospital policy) when there is a clear danger and immediate risk of harm to the patient or staff member PRN or standing orders for restraints ARE NOT permitted
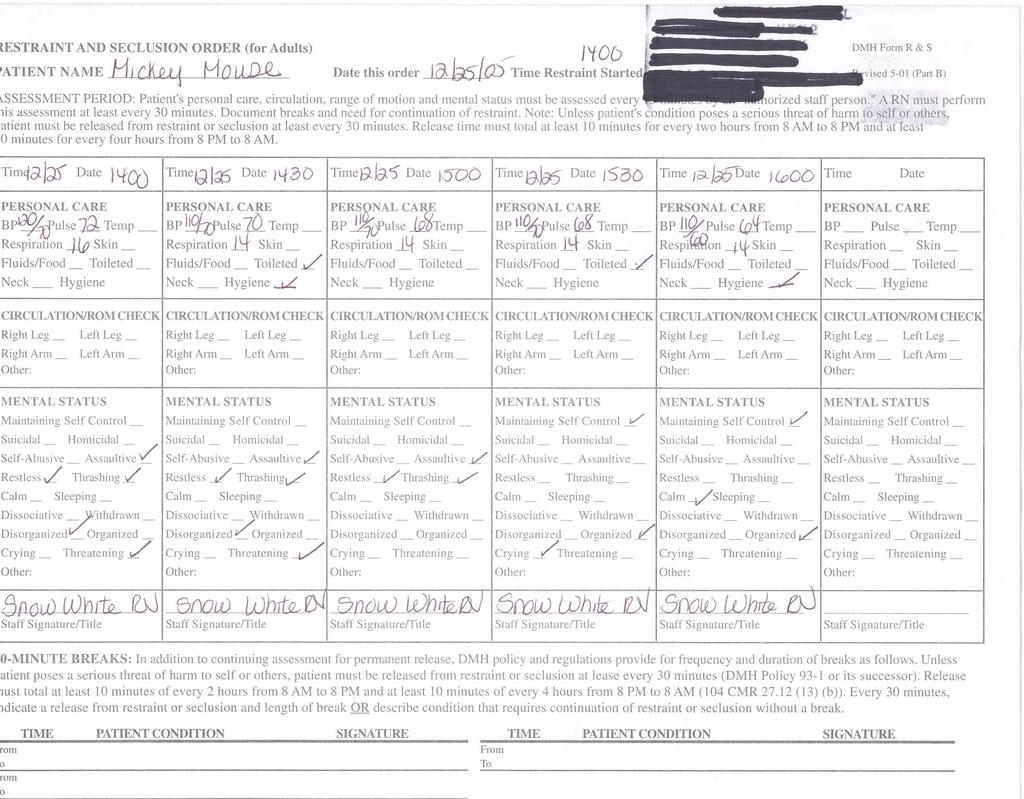
9 Importance of vital signs with restraints Heart rate: is the heart rate > 100? This can show an added stress on the heart, can be a sign of fear and agitation Respiratory rate: is the respiratory rate> 28? This can be a sign of anxiety, panic, or could be caused by tightness of the restraint around the chest or neck. Blood pressure: Is the blood pressure more than 15 points higher than the persons baseline?? BP can rise with agitation and fear


10 Signs of distress while in restraints Edema of the extremity: Check for a pulse, color, sensation and motion of the extremity restrained. If edema is restraint related, remove/loosen restraint, if no pulse or change in CSM, notify MD Discolor of the extremity: Either paleness or a blue discoloration of the extremity must be reported Change in sensation of the extremity: Can the person feel you touch the restrained extremity Change in movement of the extremity: Can the patient move their fingers and toes


11 Signs of distress while in restraints Difficulty breathing: Ensure restraint is not restricting the patient anyway between the neck to the hips Assist patient to an upright position, check 02 sat Skin irritation: Check the skin under the restraint, if redness or skin tear noted, loosen restraint, consider padding the restraint with ABD pads, if skin broken, consult skin care nurse Bleeding: If a patient begins to bleed, while wearing gloves apply pressure to the bleeding area and elevate it. Choking: Monitor patients ability to cough and clear their lungs. If unable to speak, perform Heimlich maneuver Pain: Notify the nurse of any complaints of pain. Patients fighting in restraints can injure joints and muscles

12 Signs of Distress while in Restraints: Psychological Increased anxiety: pressured and rapid speech. Restlessness and agitation Anger Frustration Misunderstanding the rationale for the restraint as something other than a safety measure Despondent Non communicative Depressed Post traumatic stress disorder
13
14
15 When is it time to remove the restraint? Patient demonstrates calm behavior and is able to listen to and follow instructions The behavior that stimulated the use of the restraint is no longer demonstrated Patient is able to contract with staff that they will not harm themselves or others if restraint removed The device we were trying to protect the patient from harming for their medical-surgical healing is no longer needed
16 Mental Health Patients Refers to a patient whose primary need for care is psychological in nature Restraints requires an MD order which must take place within 1 hour of the restraint and is validate for 3 hours The patient must be evaluated by the MD within 1 hour of the restraint and every 6 hours as long as the restraint is in use After 3 hours, the nurse can take a verbal order to renew the order for another 3 hours Use the DMH forms: # 1 MD order # 2 Monitoring form # 3 Patient comment form There is also a team debriefing form
17 Rationale Alternatives tried MD order
18
19

20 Update the Patient s Plan of Care Individualize the Safety Risk problem with either the Extubation Fall Wandering or Agitation Protocols
21 When the worse happens. If the patient aspirates: assist the patient to an upright position monitor their ability to cough and clear lungs, if unable to clear lungs; consider suctioning. If unable to cough or speak, utilize the Heimlich manuever If the patient becomes unresponsive and pulseless while in restraints, remove the restraints (noting their position at the time of arrest) implement BLS measures: Airway, Breathing, Circulation Complete an incident report in RL. If the patient dies, call Quality and Safety as well as this is a reportable death
22 Death Reporting The practitioner will report to the Department of Quality and Safety any patient death that occurs: During a restraint or seclusion episode within 24hrs after removal from restraint or seclusion Within one week after a restraint or seclusion where it is reasonable to assume that the use of restraint or seclusion directly or indirectly contributed to a death When a member of Quality and Safety notifies CMS of the death, they will document the date and time of the call in the medical record
Restraint Update 2016
 Restraint Update 2016 For questions contact: Weddy Balmaceda, MSN, RN-BC, CCRN, CCDS Professional Development Ext. 5241 Source: RBMC policy and procedures Objectives Review types of restraints Review RBMC
Restraint Update 2016 For questions contact: Weddy Balmaceda, MSN, RN-BC, CCRN, CCDS Professional Development Ext. 5241 Source: RBMC policy and procedures Objectives Review types of restraints Review RBMC
Site: Lovelace Health System Title: PATIENT CARE - Restraints Approved Date: 08/28/2015 Effective Date: TBD
 Approved Date: 08/28/2015 Effective Date: TBD 08/01/2018 Document Number P-NS-1063.6 Document Type: Policy Page 1 of 11 1. Policy: All patients have the right to be free from physical or mental abuse,
Approved Date: 08/28/2015 Effective Date: TBD 08/01/2018 Document Number P-NS-1063.6 Document Type: Policy Page 1 of 11 1. Policy: All patients have the right to be free from physical or mental abuse,
Institutional Handbook of Operating Procedures Policy Responsible Vice President: Executive Vice President and CEO, Health System
 Section: Clinical Subject: General Policies Institutional Handbook of Operating Procedures Policy 09.13.06 Responsible Vice President: Executive Vice President and CEO, Health System Responsible Entity:
Section: Clinical Subject: General Policies Institutional Handbook of Operating Procedures Policy 09.13.06 Responsible Vice President: Executive Vice President and CEO, Health System Responsible Entity:
POLICY AND PROCEDURE RESTRAINT/SECLUSION, MEDICAL CENTER PATIENT CARE Effective Date: March 2010
 Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Restraint Education Program JHS Annual Mandatory Clinical Education
 Restraint Education Program 2017 JHS Annual Mandatory Clinical Education Program Goals Prevent, reduce and eliminate use of restraints Initiate restraint only when other less restrictive measures have
Restraint Education Program 2017 JHS Annual Mandatory Clinical Education Program Goals Prevent, reduce and eliminate use of restraints Initiate restraint only when other less restrictive measures have
Comparison of Violent or Self Destructive vs. Non-Violent Restraints
 Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Appendix E: Minimizing Restraining Staff Training Presentation. Least Restraint, Last Resort
 Appendix E: Minimizing Restraining Staff Training Presentation Least Restraint, Last Resort Audience: Registered Staff Release Date: December 3, 2010 Adapted from educational materials provided by Belmont
Appendix E: Minimizing Restraining Staff Training Presentation Least Restraint, Last Resort Audience: Registered Staff Release Date: December 3, 2010 Adapted from educational materials provided by Belmont
The policy applies to all SHS employees involved in direct patient care and medical staff.
 Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Restraints and Seclusion Use Training
 Restraints and Seclusion Use Training Table of Content TOPIC PAGE NUMBER OBJECTIVES 2 WHAT ARE RESTRAINTS? 3 INTRODUCTION 4 WHAT IS A RESTRAINT? 6 A RESTRAINT FREE ENVIRONMENT 8 THE MOST COMMON REASONS
Restraints and Seclusion Use Training Table of Content TOPIC PAGE NUMBER OBJECTIVES 2 WHAT ARE RESTRAINTS? 3 INTRODUCTION 4 WHAT IS A RESTRAINT? 6 A RESTRAINT FREE ENVIRONMENT 8 THE MOST COMMON REASONS
Subacute Care. 1. Define important words in the chapter. 2. Discuss the types of residents who are in a subacute setting
 175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE
 NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
RESTRAINTS TABLE OF CONTENTS. 1. Purpose Scope Definitions 2 to Policy Statements 6 to Procedures 7 to 14
 PAGE: 1 of 18 TABLE OF CONTENTS Section Page Numbers 1. Purpose 2 2. Scope 2 3. Definitions 2 to 6 4. Policy Statements 6 to 7 5. Procedures 7 to 14 Cross References; Owner; References; Prior Version Dates
PAGE: 1 of 18 TABLE OF CONTENTS Section Page Numbers 1. Purpose 2 2. Scope 2 3. Definitions 2 to 6 4. Policy Statements 6 to 7 5. Procedures 7 to 14 Cross References; Owner; References; Prior Version Dates
SETHS STANDARDIZED USE OF RESTRAINT AND/OR SECLUSION. Date Adopted: 07/09 Date Revised: 03/18 Supersedes: Date Reviewed: 03/18
 CHRISTUS Southeast Texas Health System ADMINISTRATIVE POLICY TITLE: I. KEY WORDS: Restraint, Chemical Restraint, Seclusion, Non-Violent/Non-Self Destructive Restraints, Violent/Self-Destructive Restraints
CHRISTUS Southeast Texas Health System ADMINISTRATIVE POLICY TITLE: I. KEY WORDS: Restraint, Chemical Restraint, Seclusion, Non-Violent/Non-Self Destructive Restraints, Violent/Self-Destructive Restraints
Patient Rights. Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR
 CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 Patient Rights Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR Objectives: Patients will be able to understand
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 Patient Rights Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR Objectives: Patients will be able to understand
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
Chapter 11 Assessment of the Medical Patient DOT Directory
 Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
1/8/2018. Chapter 55. End-of-Life Care
 Chapter 55 End-of-Life Care Some deaths are sudden; others are expected. Health team members see death often. Death and dying mean helplessness and failure to cure. Your feelings about death affect the
Chapter 55 End-of-Life Care Some deaths are sudden; others are expected. Health team members see death often. Death and dying mean helplessness and failure to cure. Your feelings about death affect the
RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES
 RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES CHAPTER 0940-3-9 USE OF ISOLATION, MECHANICAL RESTRAINT, AND PHYSICAL HOLDING RESTRAINT TABLE OF CONTENTS
RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES CHAPTER 0940-3-9 USE OF ISOLATION, MECHANICAL RESTRAINT, AND PHYSICAL HOLDING RESTRAINT TABLE OF CONTENTS
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
for the Wilderness CHECK: Check the Scene, the Resources and the Person person, other members of the group and any bystanders.
 Check Call Care for If you find yourself in an emergency, you should follow three basic emergency action principles: CHECK CALL CARE. These principles will help guide you in caring for the patient and
Check Call Care for If you find yourself in an emergency, you should follow three basic emergency action principles: CHECK CALL CARE. These principles will help guide you in caring for the patient and
Recognizing and Reporting Acute Change of Condition
 Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
When Your Loved One is Dying at Home
 When Your Loved One is Dying at Home What can I expect? What can I do? Although it is impossible to totally prepare for a death it may be easier if you know what to expect. Hospice Palliative Care aims
When Your Loved One is Dying at Home What can I expect? What can I do? Although it is impossible to totally prepare for a death it may be easier if you know what to expect. Hospice Palliative Care aims
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - ACUTE CARE INPATIENT - PEDIATRIC SCOPE Provincial: Acute Care Inpatient Pediatric APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating
TITLE RESTRAINT AS A LAST RESORT - ACUTE CARE INPATIENT - PEDIATRIC SCOPE Provincial: Acute Care Inpatient Pediatric APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating
Emergency Use of Manual Restraints Policy
 Emergency Use of Manual Restraints Policy It is the policy of this DHS licensed provider, Companion Linc, to promote the rights of persons served by this program and to protect their health and safety
Emergency Use of Manual Restraints Policy It is the policy of this DHS licensed provider, Companion Linc, to promote the rights of persons served by this program and to protect their health and safety
Effective: Revised: April 15, 2016 SUCTIONING, MODIFIED STERILE TRACHEAL
 SUCTIONING, MODIFIED STERILE TRACHEAL Purpose: Tracheal suctioning is performed to remove secretions and maintain a patent airway. Additional Authority: Nevada Revised Statute, Nevada Nurse Practice Act,
SUCTIONING, MODIFIED STERILE TRACHEAL Purpose: Tracheal suctioning is performed to remove secretions and maintain a patent airway. Additional Authority: Nevada Revised Statute, Nevada Nurse Practice Act,
Interim Final Interpretive Guidelines Version 1.1
 Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Standard Operating Procedures
 Standard Operating Procedures Purdue University Stadium Rescue Squad Last Updated: October 26, 2012 Introduction: Liability: Contact: This document serves as the standard operating procedures (SOP) for
Standard Operating Procedures Purdue University Stadium Rescue Squad Last Updated: October 26, 2012 Introduction: Liability: Contact: This document serves as the standard operating procedures (SOP) for
MANAGEMENT OF DYSPHAGIA POLICY
 MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
Revised 08/07/2014 BEHAVIORAL MANAGEMENT I-59 New 07/2013
 3195 Neil Armstrong Blvd. Eagan, MN 55121 651-686-0405 204 Mississippi Ave. Red Wing, MN 55066 651-388-7108 224 Main Street Zumbrota, MN 55992 507-732-7888 1202 Beaudry Blvd Hudson, WI 54016 715-410-4216
3195 Neil Armstrong Blvd. Eagan, MN 55121 651-686-0405 204 Mississippi Ave. Red Wing, MN 55066 651-388-7108 224 Main Street Zumbrota, MN 55992 507-732-7888 1202 Beaudry Blvd Hudson, WI 54016 715-410-4216
Effective Date: August 31, 2006 SUBJECT: TRACHEOSTOMY CARE: CLEANING OF INNER CANNULA
 COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 418 Effective Date: August 31, 2006 SUBJECT: TRACHEOSTOMY CARE: CLEANING OF INNER CANNULA 1. PURPOSE: To
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 418 Effective Date: August 31, 2006 SUBJECT: TRACHEOSTOMY CARE: CLEANING OF INNER CANNULA 1. PURPOSE: To
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION
 RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION CHAPTER 0940-5-20 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-20-.01 Policies and Procedures for Adult
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION CHAPTER 0940-5-20 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-20-.01 Policies and Procedures for Adult
Returned Missionary Study Guide
 Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Your Results for: "NCLEX Review"
 Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
New OSU Hospital Policy on the Use of Restraints and Seclusion
 University Hospitals Office of the Medical Director 130 Doan Hall 410 West 10 th Avenue Columbus, OH 43210-1228 Phone: (614) 293-8158 FAX: (614) 293-4989 MEMORANDUM DATE: February 7, 2000 TO: FROM: RE:
University Hospitals Office of the Medical Director 130 Doan Hall 410 West 10 th Avenue Columbus, OH 43210-1228 Phone: (614) 293-8158 FAX: (614) 293-4989 MEMORANDUM DATE: February 7, 2000 TO: FROM: RE:
Caring for Patients at Risk for Aspiration
 Nursing Assistants Sample Peak Development Resources, LLC P.O. Box 13267 Richmond, VA 23225 Phone: (804) 233-3707 Fax: (804) 233-3705 After reading the newsletter, the nursing assistant should be able
Nursing Assistants Sample Peak Development Resources, LLC P.O. Box 13267 Richmond, VA 23225 Phone: (804) 233-3707 Fax: (804) 233-3705 After reading the newsletter, the nursing assistant should be able
BED RAIL SAFETY 9/15/2015. A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
RN - Skilled Nursing Visit
 Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0154) Direct skilled services of
Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0154) Direct skilled services of
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
does staff intervene; used? If not, describe.
 Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
9/17/2015. Bed Rail Safety A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline. Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES
 2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES SKILL CHECKLIST Cardiac Arrest NAME PRINT NAME EMS # DATE Objective: Given a multi-person company, BLS/ALS equipment and manikin: demonstrate
2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES SKILL CHECKLIST Cardiac Arrest NAME PRINT NAME EMS # DATE Objective: Given a multi-person company, BLS/ALS equipment and manikin: demonstrate
[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.
![[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.](/thumbs/78/78464102.jpg "[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.") Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
FALLS RISK REDUCTION & MANAGEMENT OF INPATIENT FALLS - STANDARDS
 STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
Preparing for Death: A Guide for Caregivers
 Preparing for Death: A Guide for Caregivers Preparing for Death As a person is dying, their body will go through a number of physical changes as it slows down and moves toward the final stages of life.
Preparing for Death: A Guide for Caregivers Preparing for Death As a person is dying, their body will go through a number of physical changes as it slows down and moves toward the final stages of life.
Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene If the First Person On-Scene is able to proceed
Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene If the First Person On-Scene is able to proceed
Iowa Department of Inspections and Appeals Health Facilities Division Citation
 : Survey s: 56.12 481 56.12 (135C) I violation as a result of multiple lesser violations. The director of the department of inspections and appeals may issue a citation for a class I violation when a physical
: Survey s: 56.12 481 56.12 (135C) I violation as a result of multiple lesser violations. The director of the department of inspections and appeals may issue a citation for a class I violation when a physical
OAR Changes. Presented by APD Medicaid LTC Policy
 OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
Score Sheet for Patient #1 - "Crushed Arm"
 CYCLE # TEAM # 5001 5002 5003 5004 5005 5006 5007 Did the team ASK for SITUATION HISTORY? 5008 Did the team DETERMINE the NUMBER OF CASUALTIES? 2 5009 Did the team ID SELF and OBTAIN CONSENT? 5010 5011
CYCLE # TEAM # 5001 5002 5003 5004 5005 5006 5007 Did the team ASK for SITUATION HISTORY? 5008 Did the team DETERMINE the NUMBER OF CASUALTIES? 2 5009 Did the team ID SELF and OBTAIN CONSENT? 5010 5011
Cygnet Schools. First Aid Policy
 Cygnet Schools First Aid Policy Table 1 Related Policies CARDIAC ARREST (CP 12) DFE GUIDANCE ON SUPPORTING PUPILS WITH MEDICAL CONDITIONS (2014) GUIDANCE ON FIRST AID IN SCHOOLS (2014) HEALTH AND SAFETY
Cygnet Schools First Aid Policy Table 1 Related Policies CARDIAC ARREST (CP 12) DFE GUIDANCE ON SUPPORTING PUPILS WITH MEDICAL CONDITIONS (2014) GUIDANCE ON FIRST AID IN SCHOOLS (2014) HEALTH AND SAFETY
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE
 RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE CHAPTER 0940-5-24 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-24-.01 Health,
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE CHAPTER 0940-5-24 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-24-.01 Health,
INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )
 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )") County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE
County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE
Anaphylactic Reaction Emergency Treatment Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Anaphylactic Reaction Emergency Treatment Reference Number: NHSCT/12/551 Target audience: Nursing Staff Groups included are:
This is an official Northern Trust policy and should not be edited in any way Anaphylactic Reaction Emergency Treatment Reference Number: NHSCT/12/551 Target audience: Nursing Staff Groups included are:
M: Maternal/ Newborn Care
 M: Maternal/ Newborn Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 113 Competency: M-1 Maternal/Newborn Nursing M-1-1 M-1-2 M-1-3 Demonstrate knowledge
M: Maternal/ Newborn Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 113 Competency: M-1 Maternal/Newborn Nursing M-1-1 M-1-2 M-1-3 Demonstrate knowledge
Policy Review Sheet. Review Date: 14/10/16 Policy Last Amended: 19/10/17. Next planned review in 12 months, or sooner as required.
 Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Standards of proficiency for nursing associates
 Standards of proficiency for nursing associates DRAFT April 2018 www.nmc.org.uk Contents Introduction 3 Standards of proficiency for nursing associates 5 Platform 1: Being an accountable professional 5
Standards of proficiency for nursing associates DRAFT April 2018 www.nmc.org.uk Contents Introduction 3 Standards of proficiency for nursing associates 5 Platform 1: Being an accountable professional 5
To be completed by healthcare provider
 Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Residential Assisted Living Procedure Development
 Revised: 04-10-17 Residential Assisted Living Procedure Development WHEN TO CALL 911 POCATELLO FIRE DEPARTMENT 408 E. Whitman, Pocatello, Idaho, 83201 Revised: 04-10-17 Table of Contents Purpose of this
Revised: 04-10-17 Residential Assisted Living Procedure Development WHEN TO CALL 911 POCATELLO FIRE DEPARTMENT 408 E. Whitman, Pocatello, Idaho, 83201 Revised: 04-10-17 Table of Contents Purpose of this
Occupational First Aid Minor Wound Care Refresher Instructors Guide
 Occupational First Aid Minor Wound Care Refresher Instructors Guide Policies Occupational First Aid Minor Wound Care Refresher Instructor Guide This review course is a one day, or two four hour session
Occupational First Aid Minor Wound Care Refresher Instructors Guide Policies Occupational First Aid Minor Wound Care Refresher Instructor Guide This review course is a one day, or two four hour session
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Tube Feeding Status Critical Element Pathway
 Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015
 PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth
 Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
EMS Safety Test Handout
 1. Why is body substance isolation important? Page 1 of 5 It is a requirement of OSHA. It demonstrates a professional attitude. It prevents the patient from obtaining an infection. It reduces the risk
1. Why is body substance isolation important? Page 1 of 5 It is a requirement of OSHA. It demonstrates a professional attitude. It prevents the patient from obtaining an infection. It reduces the risk
All about Your Implanted Venous Access Device (IVAD, Port )
") All about Your Implanted Venous Access Device (IVAD, Port ) Your doctor has chosen an Implanted Venous Access Device (IVAD) for you based on your treatment needs. Because the IVAD can remain in place for
All about Your Implanted Venous Access Device (IVAD, Port ) Your doctor has chosen an Implanted Venous Access Device (IVAD) for you based on your treatment needs. Because the IVAD can remain in place for
Resident/Fellow Training Orientation Policies
 Resident/Fellow Training Orientation Policies Restraint or Seclusion: Violent Behavior Prevention and Reporting of Patient Abuse Blood Component Indications & Critical Tests HIPAA Privacy and Security
Resident/Fellow Training Orientation Policies Restraint or Seclusion: Violent Behavior Prevention and Reporting of Patient Abuse Blood Component Indications & Critical Tests HIPAA Privacy and Security
LOS ALAMITOS UNIFIED SCHOOL DISTRICT
 LOS ALAMITOS UNIFIED SCHOOL DISTRICT Seizure Action Plan Student Name: DOB: School: Grade/Teacher: Parent/Guardian: Phone # Printed Name of Treating Neurologist: Treating Neurologist s Phone # Fax# Seizure
LOS ALAMITOS UNIFIED SCHOOL DISTRICT Seizure Action Plan Student Name: DOB: School: Grade/Teacher: Parent/Guardian: Phone # Printed Name of Treating Neurologist: Treating Neurologist s Phone # Fax# Seizure
Carotid Endarterectomy
 P A T IENT INFORMAT ION Carotid Endarterectomy Please bring this book to the hospital on the day of your surgery. CP 16 B (REV 06/2012) THE OTTAWA HOSPITAL Disclaimer This is general information developed
P A T IENT INFORMAT ION Carotid Endarterectomy Please bring this book to the hospital on the day of your surgery. CP 16 B (REV 06/2012) THE OTTAWA HOSPITAL Disclaimer This is general information developed
Entry Level Assessment Blueprint Home Health Aide
 Entry Level Assessment Blueprint Home Health Aide Test Code: 4048 / Version: 01 Specific Competencies and Skills Tested in this Assessment: First Aid and Basic Emergency Measures Administer first aid for
Entry Level Assessment Blueprint Home Health Aide Test Code: 4048 / Version: 01 Specific Competencies and Skills Tested in this Assessment: First Aid and Basic Emergency Measures Administer first aid for
SKILLS CHECKLIST FOR RECERTIFICATION
 NAME BLS-2017-Altered Mental States EMERGENCY MEDICAL SERVICES (11/10 MH) Objective: Given a partner, appropriate equipment and an altered mental status, demonstrate appropriate assessment and treatment
NAME BLS-2017-Altered Mental States EMERGENCY MEDICAL SERVICES (11/10 MH) Objective: Given a partner, appropriate equipment and an altered mental status, demonstrate appropriate assessment and treatment
Decreasing Seclusion and Increasing Restraint and Seclusion Documentation Compliance using LEAN. Sheppard Pratt Health System
 Decreasing Seclusion and Increasing Restraint and Seclusion ation Compliance using LEAN Rick Wallace MSN, RN Associate Director of Clinical Services Jacqueline Williams Porter MBA, RN Unit Director Sheppard
Decreasing Seclusion and Increasing Restraint and Seclusion ation Compliance using LEAN Rick Wallace MSN, RN Associate Director of Clinical Services Jacqueline Williams Porter MBA, RN Unit Director Sheppard
Management of Assaultive Behavior Workplace Violence in the Hospital
 Management of Assaultive Behavior Workplace Violence in the Hospital What is workplace violence? Definitions Workplace is any place where an employee performs job duties. Violence is any act that causes
Management of Assaultive Behavior Workplace Violence in the Hospital What is workplace violence? Definitions Workplace is any place where an employee performs job duties. Violence is any act that causes
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES. By Maureen Kroning EdD, RN
 A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Mental Health Commission
 Code of Practice Code of Practice on the Use of Physical Restraint in Approved Centres Issued Pursuant to Section 33(3)(e) of the Mental Health Act 2001. October 2009 VISION Working Together for Quality
Code of Practice Code of Practice on the Use of Physical Restraint in Approved Centres Issued Pursuant to Section 33(3)(e) of the Mental Health Act 2001. October 2009 VISION Working Together for Quality
Wound Care Program for Nursing Assistants- Prevention 101
 Wound Care Program for Nursing Assistants- Prevention 101 Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion of this webinar,
Wound Care Program for Nursing Assistants- Prevention 101 Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion of this webinar,
Skilled skin care should be provided by an agency licensed to provide home health
 8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
Christian Brothers Risk Management Services. Nursing Home & Health Care Ministry Documentation: Are you open for a lawsuit?
 2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
Course Title: Emergency Medical Responder 3 Course Number: Course Credit: 1. Course Description:
 Course Title: Emergency Medical Responder 3 Course Number: 8417171 Course Credit: 1 Course Description: This course prepares students to be employed as Emergency Medical Responders. Content includes, but
Course Title: Emergency Medical Responder 3 Course Number: 8417171 Course Credit: 1 Course Description: This course prepares students to be employed as Emergency Medical Responders. Content includes, but
TECUMSEH PUBLIC SCHOOLS Medical Emergency Response Team (MERT)
") Action Effective, efficient communication throughout campus Coordinate and practice your emergency response plan TECUMSEH PUBLIC SCHOOLS Medical Emergency Response Team (MERT) Specifics Establish a rapid
Action Effective, efficient communication throughout campus Coordinate and practice your emergency response plan TECUMSEH PUBLIC SCHOOLS Medical Emergency Response Team (MERT) Specifics Establish a rapid
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy
 Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
NM DDSD Intensive Medical Living Services Eligibility Parameter Tool A. MEDICATION ADMINISTRATION SEVERE 4 SIGNIFICANT 3 MODERATE 2 LOW 1 NONE - 0
 FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
Effective: September, 2011 Revised: August 17, 2016 TRACHEOSTOMY TUBE REPLACEMENT
 TRACHEOSTOMY TUBE REPLACEMENT Purpose: Emergency tracheostomy tube replacement occurs when the tube becomes blocked, dislodged or has been unintentionally removed. Additional Authority: Nevada Revised
TRACHEOSTOMY TUBE REPLACEMENT Purpose: Emergency tracheostomy tube replacement occurs when the tube becomes blocked, dislodged or has been unintentionally removed. Additional Authority: Nevada Revised
First Aid, CPR and AED
 First Aid, CPR and AED Training saves lives! If you observe someone who requires medical attention as a result of an accident, injury or illness, it is very important for you to understand your options.
First Aid, CPR and AED Training saves lives! If you observe someone who requires medical attention as a result of an accident, injury or illness, it is very important for you to understand your options.
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Next Gen Training. Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups
 Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Indications for Calling A Code Blue or Pediatric Medical Emergency
 Code Blue/Pediatric Medical Emergency Code Blue is a term used to alert the Code Team and hospital staff of the significant deterioration in an individual s status (e.g. unresponsiveness, absence of blood
Code Blue/Pediatric Medical Emergency Code Blue is a term used to alert the Code Team and hospital staff of the significant deterioration in an individual s status (e.g. unresponsiveness, absence of blood
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Goals & Objectives 4/17/2014 UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN. Why would someone need to do this?
 By Maureen Kroning, EdD, RN. Why would someone need to do this?") UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
RESIDENT CARE AND SERVICES MANUAL SECTION: RESIDENT SAFETY INDEX I.D.: E-25. APPROVED BY: REVISED DATE: April 30, 2010
 SUBJECT: RESTRAINTS PAGE: 1 OF 6 STANDARD: 1. The decision to use restraints is based on the principle that least restraint can only be considered after the interdisciplinary team had tried alternatives
SUBJECT: RESTRAINTS PAGE: 1 OF 6 STANDARD: 1. The decision to use restraints is based on the principle that least restraint can only be considered after the interdisciplinary team had tried alternatives
Patient Restraint 1. INTRODUCTION
 Patient Restraint Supersedes: 09-13-13 Effective: 12-14-15 1. INTRODUCTION 1.1. Patients have the right to refuse treatment and/or transport if they are of legal age and are competent. Competence is defined
Patient Restraint Supersedes: 09-13-13 Effective: 12-14-15 1. INTRODUCTION 1.1. Patients have the right to refuse treatment and/or transport if they are of legal age and are competent. Competence is defined
Rowan Court. Avery Homes (Nelson) Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement
 Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement") Avery Homes (Nelson) Limited Rowan Court Inspection report Silverdale Road Newcastle under Lyme Staffordshire ST5 2TA Tel: 01782622144 Website: www.averyhealthcare.co.uk Date of inspection visit: 16 May
Avery Homes (Nelson) Limited Rowan Court Inspection report Silverdale Road Newcastle under Lyme Staffordshire ST5 2TA Tel: 01782622144 Website: www.averyhealthcare.co.uk Date of inspection visit: 16 May
Mental Health/Substance Abuse SECLUSION AND RESTRAINT USE IN PSYCHIATRIC CRISIS MANAGEMENT
 FLORIDA STATE HOSPITAL OPERATING PROCEDURE NO. 155-22 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES CHATTAHOOCHEE, August 28, 2017 Mental Health/Substance Abuse SECLUSION AND RESTRAINT USE IN PSYCHIATRIC
FLORIDA STATE HOSPITAL OPERATING PROCEDURE NO. 155-22 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES CHATTAHOOCHEE, August 28, 2017 Mental Health/Substance Abuse SECLUSION AND RESTRAINT USE IN PSYCHIATRIC