To-Do List Functional Medicine (COMPREHENSIVE) patients UNDER 10 YEARS OLD
|
|
|
- Jonah Simmons
- 5 years ago
- Views:
Transcription
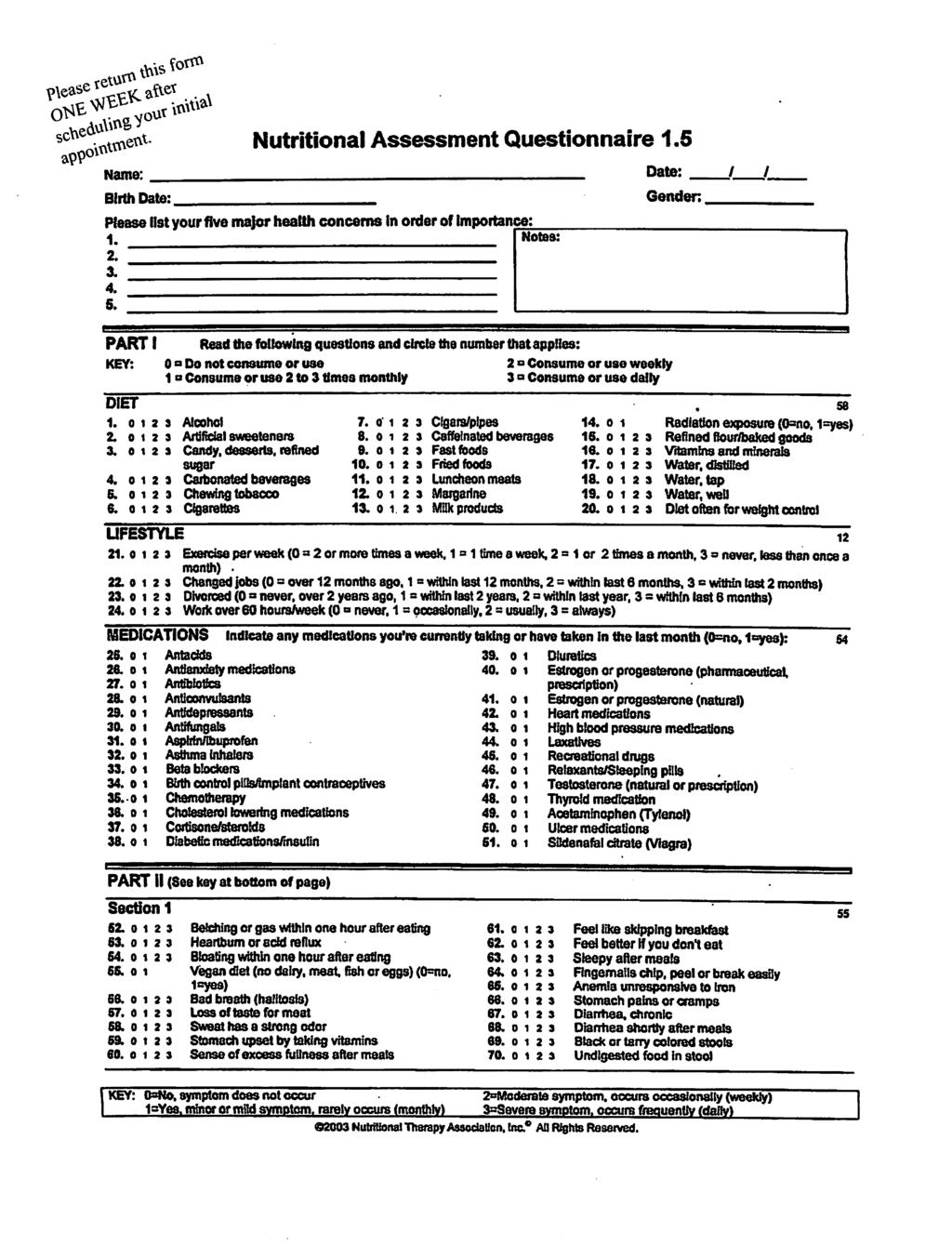
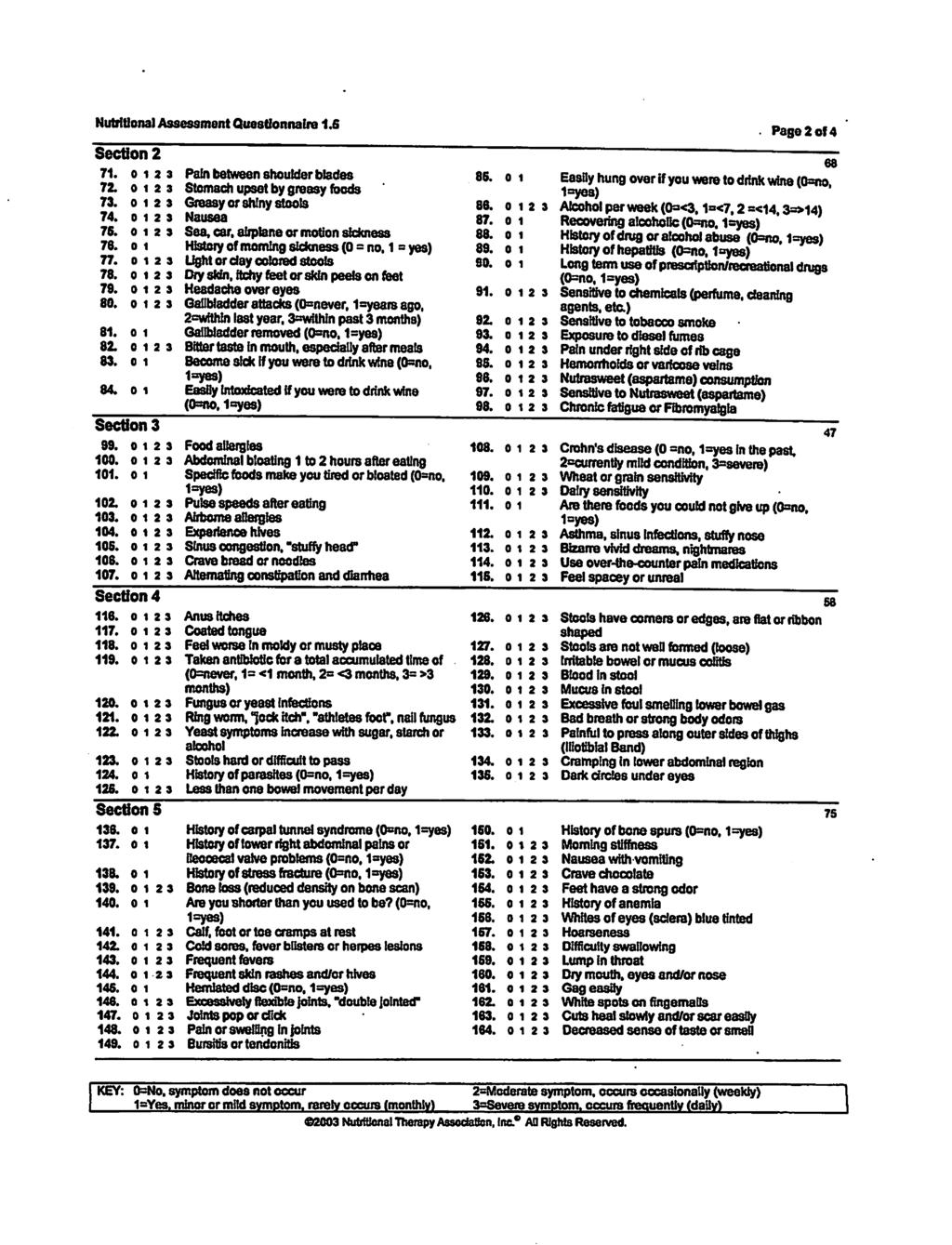
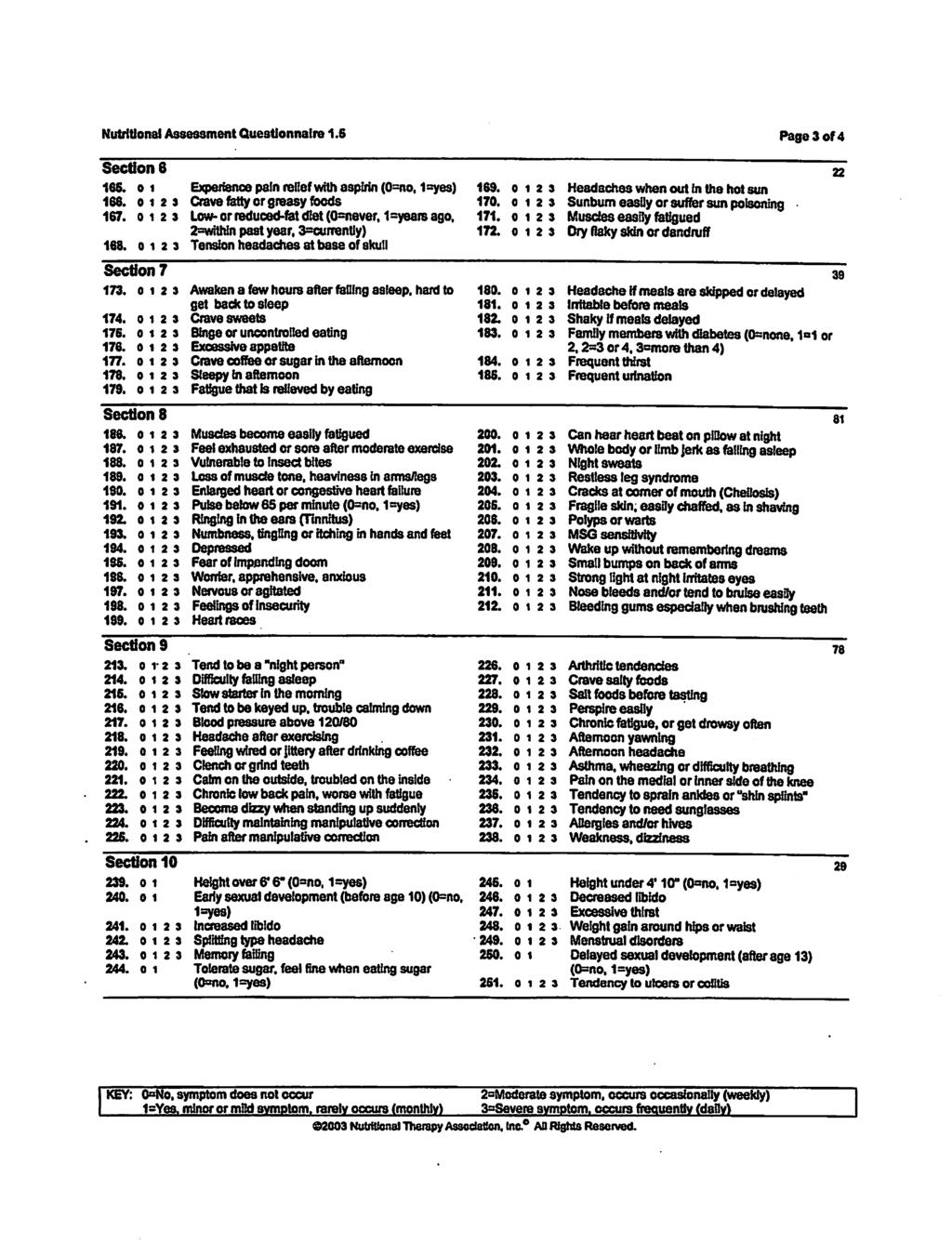
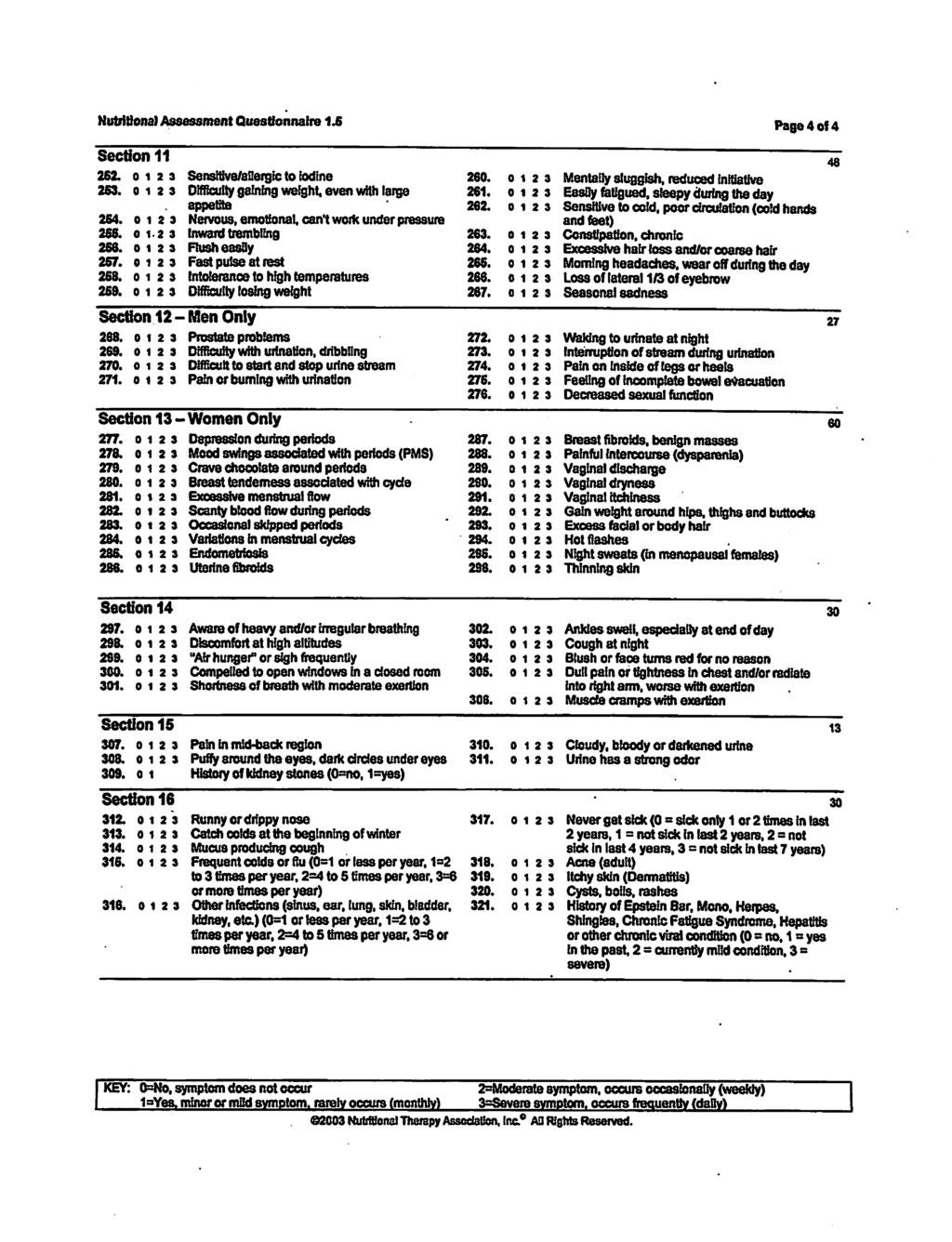
1 To-Do List Functional Medicine (COMPREHENSIVE) patients UNDER 10 YEARS OLD A SUMMARY OF THE FORMS YOU WILL NEED TO COMPLETE BEFORE YOUR INITIAL FUNCTIONAL MEDICINE APPOINTMENT WITH DR. FENSKE, AND WHEN SHE WILL NEED TO RECEIVE THEM IN ORDER TO FULLY PREPARE FOR YOUR APPOINTMENT. FORM: DUE: Medical Record Request (separate download from other forms) Patient Acceptance Form Within TWO DAYS of scheduling your initial appointment. Within ONE WEEK of scheduling your initial appointment. Weekly Symptom Checklist Within ONE WEEK of scheduling your initial appointment. Nutritional Assessment Questionnaire Within ONE WEEK of scheduling your initial appointment. Diet Diary Within ONE WEEK of scheduling your initial appointment. Health Goals Within ONE WEEK of scheduling your initial appointment tel fax Info@DrFenske.com Terrace Ave. Ste 2 Middleton, WI 53562
2 Patient Acceptance Policy Functional Medicine (COMPREHENSIVE) patients (608) Name (last, first) Date: Address City, State, Zip Phone (home) Phone (cell) Sex Age Date of Birth Spouse/Partner s Name Children (ages, names) Occupation Employer/School Whom may we thank for referring you to our office? In order to best serve you, the Patient Acceptance Policy should be carefully reviewed. It is Dr. Fenske s opinion that you should be well informed on our expectations and clinical procedures. To prevent any misunderstandings or confusion on what to expect, Dr. Fenske would appreciate that you read the below steps and provide your signature. This would simply imply that you have read the Patient Acceptance Policy and understand what is expected of you. PRIOR TO FIRST APPOINTMENT: 1. Completion of the following forms: Patient Acceptance Policy, Patient Health History, Nutritional Assessment Questionnaire, Diet and Lifestyle Diary, Health Goals, Request for Records. These forms were developed to gather important information about your body. They will help Dr. Fenske more quickly zero in on the probable causes of your health problems. It is VERY important for you to carefully and thoroughly complete all of these forms and questionnaires prior to your first consultation with Dr. Fenske. 2. Medical Records and Lab Reports (see Request for Records form) Obtain medical records and lab reports from all physicians since you were first diagnosed with your health condition. We MUST receive these prior to your initial appointment. FIRST APPOINTMENT: 3. At your initial appointment Dr. Fenske will review your case with you and provide a detailed written report based on the information you have provided. The cost for the 60 to 75 minute appointment as well as Dr. Fenske s time for studying your forms / medical records is $ Based on your initial appointment and review of all your medical information Dr. Fenske may recommend various labs. These labs help uncover underlying weaknesses in the body that may result in disease. You will be presented with detailed information on the specific tests recommended. Because it varies case by case, the cost for your initial laboratory tests will be discussed at that time. SECOND APPOINTMENT: 5. The time it takes to receive the results of your tests varies based on individual test processing time as well as on when you choose to initiate the test. When results are available our staff will call to schedule your second appointment. This appointment usually takes approximately one hour. You will be presented with the possible causes of your health problem and the recommended treatment protocol. The fee for this second appointment is typically $120 to $ for approximately 30 to 60 minutes.
3 6. Your recommendations may consist of personalized dietary and lifestyle changes as well as nutritional supplements. 7. After this second appointment, you may meet with our patient educator to discuss implementation of specific recommendations. SUBSEQUENT APPOINTMENTS: 8. Follow-up consultations will be scheduled every 3, 6 or 12 weeks allowing you the opportunity to discuss your progress and any concerns with Dr. Fenske. Dr. Fenske will at this time determine what direction to take to help you continue your progress. Your cooperation in taking personal responsibility in your health care will go a long way in getting better. Consultations may be conducted either by phone or in person at our office. The fee for follow-up consultations is based on the time required for the appointment (typically $ to $240). 9. Abnormal laboratory tests will need to be re-evaluated. The success of your treatment will not only be measured on the reduction or elimination of your physical symptoms, but on abnormal laboratory tests returning to a normal status. Laboratory fees can vary depending on what needs to be re-tested. Our goal at Fenske Holistic Healthcare Center is to provide high quality, personal service that is responsive to the healthcare needs of our patients. We require payment for services at the time they are provided. Insurance companies do not cover Functional Medicine consultations, nutritional supplements, or preventative lab services. Any specific questions you may have about coverage for our services should be directed to your insurance provider. Note: prices are subject to change without notice, the duration of each visit is approximate, and 24-hour notice is required to cancel an appointment without incurring a charge. Prices not only reflect the time spent with each patient but also the time studying your case between visits and the advanced training, expertise, and effort required to treat complex health conditions. We accept payment by cash, check, or credit card (Mastercard and Visa). I have read and fully understand the Patient Acceptance Policy. Patient (Parent/Guardian) Signature Date (The signature of Parent/Guardian hereby authorizes Dr. Nicole Fenske to provide care for the minor child listed as Patient). Fenske Holistic Healthcare Center 2 Patient Acceptance Policy (FM Comprehensive)
4 Fenske Holistic Healthcare Center WEEKLY SYMPTOM CHECKLIST FOR CHILDREN Name Date Date of Birth Age Height Weight Blood Type Rate each of the following symptoms based on your child s current health profile Point Scale 0 - Never or almost never has the symptom 1 - Occasionally has symptoms 2 - Frequently has symptoms HEAD Headaches Difficulty falling asleep Wakes up during the night Total EYES Watery or itchy eyes Dark circles under eyes Bags under eyes Swollen eyelids Total EARS Reddening of ears Itchy ears Earaches/Ear infections (circle which apply) Drainage from ear Hearing loss Frequent pulling on ears Total NOSE Runny nose Stuffy nose Sneezing Allergic Salute (rubs, itches, wipes nose frequently with hands) Total MOUTH/THROAT Swollen or red lips Gagging, frequent need to clear throat Sore throat, hoarseness, loss of voice Swollen or sore or discolored tongue Swollen or sore gums or lips Canker sores Total SKIN Easy bruising Hives Rash Dry or flaky skin Flushing Cold hands or feet Eczema Total
5 LUNGS Coughing Sneezing Difficulty breathing Wheezing Total DIGESTIVE TRACT Nausea Vomiting Diarrhea Constipation Bloated feeling Belching Passing gas (flatulence) Heartburn Tummy ache Poor appetite Refusal to eat Total JOINTS/MUSCLE Coordination problems Pain in muscles (e.g., leg ache) Pain in joints ( e.g., knee ache) Total ENERGY Fatigue, sluggishness Apathy, lethargy Hyperactivity Restlessness Sleeping problems Total MIND/EMOTIONS Inattentiveness or poor concentration Mood swings Anxiety, nervousness Fear Anger Irritability Aggressiveness (e.g. hitting, kicking, biting) Crying or weepiness Tantrums Hyperactivity Total OTHER Frequent urination Itching of anus or genitals Bed wetting Wetting or soiling of clothes Total GRAND TOTAL TOTAL Fenske Holistic Healthcare Center 2 Weekly Symptom Checklist
6
7
8
9
10
11
12 Establishing Your Health Goals Functional Medicine (COMPREHENSIVE) patients (608) Name Date: Personal Message Before You Begin Before you begin our journey together, I would like to discuss something very important that will have a major impact on your ability to recover and achieve maximum improvement. After many years in private practice, I have had the opportunity to work with thousands of patients and have seen many patients achieve significant improvement while others have become frustrated and failed in their attempt to get well. After careful review, I have discovered the reasons why some people succeed and why others fail. This questionnaire is about much more than eliminating your symptoms it s about living a life of vibrant health. I ve discovered that any discussion of the correct way to achieve health and stay healthy is, in actuality, a discussion of how you have lived your life up to this point and how you will live it in the future. Therefore, to help you make significant changes in your present health, I want to ask you a few very important questions. I want you to be honest with yourself and really dig deep inside yourself for the answers. 1. Have you made the decision to change? To do what it takes to get well? Yes No I have read something interesting: The definition of insanity is to keep doing the same thing and expecting different results. If you keep following the same course of treatment you have been following will your results really change? Have you ever wondered if you are on the right path to achieving optimal health? Sometimes it requires taking a new and improved road to reach your destination. Most people I ask tell me they have made the decision to change. But how many people have truly decided to change? Very few! Why? Because there is a big difference between deciding something and having reasons to actually do it. When you have made a decision to make a change and you know your reasons, you create an internal power that can propel you to achieve health and wellness. So now I ask: 2. List up to 5 things that you have been unable to do as a result of your present symptoms. Please be specific. (Use extra pages if necessary)
13 3. List up to 5 things that you plan to do once you are feeling better. Please be specific. (Use extra pages if necessary) 4. Please check off the following that you would like to achieve with my help: o Increase energy o Sleep better o Have better digestion o Be able to eat more foods o Get rid of my allergies o Have a better immune system (i.e. less colds /coughs) o Not be dependent on laxatives or stool softeners o Be able to work out again o Have better muscle tone o Be in less pain o No longer use pain medication o No longer use allergy medication o No longer use sleep medication o To feel less sleepy in the afternoon o Lose weight o Increase my sex drive o Increase my metabolism to burn more fat o Increase my flexibility o Reduce my stress o Improve my memory o Improve my focus o Improve my mood o Reduce my risk of developing a chronic disease o I want to work on an anti-aging program o I want to detoxify my body o I want to improve my diet o I want to clear up my skin 5. Are there any other health goals you want to achieve? Fenske Holistic Healthcare Center 2 Health Goals (FM Comprehensive)
Address City, State Zip Code Phone
 Email Correspondence Authorization Patient Name Date of Birth Address City, State Zip Code Phone By signing this form, I authorize Angela Pifer, Certified Nutritionist and 28 Day Health Solutions Co. (Angela
Email Correspondence Authorization Patient Name Date of Birth Address City, State Zip Code Phone By signing this form, I authorize Angela Pifer, Certified Nutritionist and 28 Day Health Solutions Co. (Angela
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Hello and Welcome! I truly look forward to working with you and your child on the journey towards optimal health. Warmly, Amanda H.
 Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION SHEET:
 PATIENT INFORMATION SHEET: LAST NAME: FIRST NAME/MI: ADDRESS: CITY: STATE: ZIP CODE: SOCIAL SECURITY #: HOME: CELL: WORK: SEX: M F BIRTHDATE: MARITAL STATUS: SINGLE MARRIED WIDOWED OTHER EMPLOYER NAME:
PATIENT INFORMATION SHEET: LAST NAME: FIRST NAME/MI: ADDRESS: CITY: STATE: ZIP CODE: SOCIAL SECURITY #: HOME: CELL: WORK: SEX: M F BIRTHDATE: MARITAL STATUS: SINGLE MARRIED WIDOWED OTHER EMPLOYER NAME:
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
GENERAL PATIENT INFORMATION
 1460 Drew Ave, Suite 300, Davis, CA 95618 PH: (530) 758-4IRH (4474) FAX: (530) 758-1880 www.4irh.com GENERAL PATIENT INFORMATION NAME DOB: / / SSN - - LAST, FIRST, MIDDLE INTIAL ADDRESS CITY STATE ZIP
1460 Drew Ave, Suite 300, Davis, CA 95618 PH: (530) 758-4IRH (4474) FAX: (530) 758-1880 www.4irh.com GENERAL PATIENT INFORMATION NAME DOB: / / SSN - - LAST, FIRST, MIDDLE INTIAL ADDRESS CITY STATE ZIP
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES
 HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 445 W. Main Street Clarksburg, WV 26301 (304) 326-7690 FAX (304) 326-7691 Dear Parent, Date Please complete the enclosed forms and return them to your
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 445 W. Main Street Clarksburg, WV 26301 (304) 326-7690 FAX (304) 326-7691 Dear Parent, Date Please complete the enclosed forms and return them to your
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely)
") SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
Naturopathic Wellness Center
 Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
PATIENT INFORMATION & CONDITION FORM
 PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
Tube Feeding at Home A Guidebook for Patients and Caregivers
 Tube Feeding at Home A Guidebook for Patients and Caregivers This manual provides information on the following: What is Tube Feeding? How to Flush Your Feeding Tube Problems That May Occur With Tube Feeds
Tube Feeding at Home A Guidebook for Patients and Caregivers This manual provides information on the following: What is Tube Feeding? How to Flush Your Feeding Tube Problems That May Occur With Tube Feeds
Last Name First Middle. Mailing Address. City State Zip Phone. Date of Birth Age Soc. Sec# Cell. Employer Work Phone
 Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
APPLICATION FOR CARE AT FAMILY WELLNESS AT TERAVISTA
 APPLICATION FOR CARE AT FAMILY WELLNESS AT TERAVISTA Today s Date: Patient Demographics Name: Address: City: State: Zip: Cell Ph: Work Ph: E-mail: Preferred method of communication: (Check one) Email Phone
APPLICATION FOR CARE AT FAMILY WELLNESS AT TERAVISTA Today s Date: Patient Demographics Name: Address: City: State: Zip: Cell Ph: Work Ph: E-mail: Preferred method of communication: (Check one) Email Phone
Glastonbury Family YMCA. CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET
 2018 Glastonbury Family YMCA CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET CAMP LOCATION 30 High Street South Glastonbury, CT 06073 860-541-1812 STEP STEP one REGISTRATION Done online,
2018 Glastonbury Family YMCA CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET CAMP LOCATION 30 High Street South Glastonbury, CT 06073 860-541-1812 STEP STEP one REGISTRATION Done online,
DEMOGHRAPHICS INSURANCE INFORMATION
 DEMOGHRAPHICS Name: Date of Birth: / / AGE: Street Address: City: State: Zip: Home Phone #: ( ) Cellular Phone :( ) Social Security Number: E-mail: Marital Status: Single Married Divorced Widowed Employer:
DEMOGHRAPHICS Name: Date of Birth: / / AGE: Street Address: City: State: Zip: Home Phone #: ( ) Cellular Phone :( ) Social Security Number: E-mail: Marital Status: Single Married Divorced Widowed Employer:
NEWSPAPER SIGN YELLOW PAGES COMMUNITY EVENT MAILING DOCTOR S NAME: PLEASE EXPLAIN: DOCTOR S NAME: RESULTS:
 ABOUT THE CHILD CHIROPRACTIC EXPERIENCE NAME: WHO REFERRED YOU TO OUR OFFICE? ADDRESS: CITY: HOME PHONE: STATE/ZIP CODE: HOW DID YOU HEAR ABOUT OUR OFFICE (ALL THAT APPLY): NEWSPAPER SIGN YELLOW PAGES
ABOUT THE CHILD CHIROPRACTIC EXPERIENCE NAME: WHO REFERRED YOU TO OUR OFFICE? ADDRESS: CITY: HOME PHONE: STATE/ZIP CODE: HOW DID YOU HEAR ABOUT OUR OFFICE (ALL THAT APPLY): NEWSPAPER SIGN YELLOW PAGES
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care
 Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
Temporary Exclusion for Health Reasons (Including Medications and Special Diets) Policy
 Policy") Temporary Exclusion for Health Reasons Policy Rationale: Head Start Performance Standard 45 CFR Section 1304.22 (b)(i) Policy: To ensure the health and safety of our children, staff and volunteers, children
Temporary Exclusion for Health Reasons Policy Rationale: Head Start Performance Standard 45 CFR Section 1304.22 (b)(i) Policy: To ensure the health and safety of our children, staff and volunteers, children
Allergies Drug Food Environmental. Previous Surgeries & Hospitalizations (Please list date, reason, and hospital)
") Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
MARATHON HEALTH CENTER a benefit of CHG Health and Wellness
 Health & Wellness MARATHON HEALTH CENTER a benefit of CHG Health and Wellness WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE PEOPLE TO LEAD HEALTHIER LIVES. CHG Healthcare Services
Health & Wellness MARATHON HEALTH CENTER a benefit of CHG Health and Wellness WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE PEOPLE TO LEAD HEALTHIER LIVES. CHG Healthcare Services
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease
 Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Immunization Requirements as Mandated by the Georgia Department of Public Health
 Dear Parents, As we prepare for the upcoming school year, it is time to begin preparing mandatory health forms for the upcoming school year. Our procedures closely align with other private schools in the
Dear Parents, As we prepare for the upcoming school year, it is time to begin preparing mandatory health forms for the upcoming school year. Our procedures closely align with other private schools in the
Bellevue Neurology PATIENT DEMOGRAPHIC FORM
 PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital
PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital
PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT.
 PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: 516-354-8597 ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT. THANK YOU - 1 - NEW PATIENT MEDICAL INFORMATION Steven J.
PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: 516-354-8597 ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT. THANK YOU - 1 - NEW PATIENT MEDICAL INFORMATION Steven J.
Camp Echoing Hills Annual Respite Participant Application
 Camp Echoing Hills Annual Respite Participant Application Application must be completed in full, signed and mailed or faxed to Camp office prior to attending. Incomplete applications will be returned.
Camp Echoing Hills Annual Respite Participant Application Application must be completed in full, signed and mailed or faxed to Camp office prior to attending. Incomplete applications will be returned.
Emergency Care for Blood and Marrow Transplant Patients
 PATIENT EDUCATION patienteducation.osumc.edu Emergency Care for Blood and Marrow Transplant Patients General Guidelines for Emergency Care Use these guidelines to know when and how to report any problems
PATIENT EDUCATION patienteducation.osumc.edu Emergency Care for Blood and Marrow Transplant Patients General Guidelines for Emergency Care Use these guidelines to know when and how to report any problems
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
2.. The two persons trained shall be regular members of the school staff, which ensures at least one of the two being present during school hours.
 STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cetuximab (+/- Chemotherapy) PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier)
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cetuximab (+/- Chemotherapy) PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier)
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Gemcitabine-Doxorubicin PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Gemcitabine-Doxorubicin PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with?
 Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Gemcitabine-Cisplatin PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Gemcitabine-Cisplatin PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM CHOP 21 + RITUXIMAB
 Patient identifier/label: Page 1 of 6 FORM CHOP 21 + RITUXIMAB Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas Hospital King s College Hospital
Patient identifier/label: Page 1 of 6 FORM CHOP 21 + RITUXIMAB Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas Hospital King s College Hospital
5121 Forest Drive Suite E New Albany, OH
 5121 Forest Drive Suite E New Albany, OH 43054 614-524-4527 WELCOME! Dear _, Welcome to Kanodia MD. Thank you for choosing us for your health care needs. In order to allow our staff and physicians to focus
5121 Forest Drive Suite E New Albany, OH 43054 614-524-4527 WELCOME! Dear _, Welcome to Kanodia MD. Thank you for choosing us for your health care needs. In order to allow our staff and physicians to focus
Julie Gussenhoven, OD 3416 Bechelli Lane Redding, CA 96002
 Julie Gussenhoven, OD OCULAR AND MEDICAL HISTORY QUESTIONNAIRE Name: M F Date: Date of Birth: Home Phone: Social Security #: Cell Phone: Address: Work Phone: City: Zip: Email: Please complete all personal
Julie Gussenhoven, OD OCULAR AND MEDICAL HISTORY QUESTIONNAIRE Name: M F Date: Date of Birth: Home Phone: Social Security #: Cell Phone: Address: Work Phone: City: Zip: Email: Please complete all personal
NPM INTAKE FORM. Home Phone No.: Work Phone No.: Cell Phone:
 NPM INTAKE FORM INFORMATION: Name: Chosen Name (What would you like to be called?): Address: Date: Age: City/State/Zip: Home Phone No.: Work Phone No.: Cell Phone: Email Address: Date of Birth: Occupation:
NPM INTAKE FORM INFORMATION: Name: Chosen Name (What would you like to be called?): Address: Date: Age: City/State/Zip: Home Phone No.: Work Phone No.: Cell Phone: Email Address: Date of Birth: Occupation:
Recognizing and Reporting Acute Change of Condition
 Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM PAZOPANIB. Patient s first names.
 Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM PAZOPANIB Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM PAZOPANIB Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas
 ADVANCED DIRECTIVES ACKNOWLEDGEMENT FORM Patient Name: Date: I do have an Advanced Directive / Living Will / Durable Power of Attorney for medical or health care decisions. I do not have an Advanced Directive
ADVANCED DIRECTIVES ACKNOWLEDGEMENT FORM Patient Name: Date: I do have an Advanced Directive / Living Will / Durable Power of Attorney for medical or health care decisions. I do not have an Advanced Directive
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Lenvatinib PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL NAME/STAMP:
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Lenvatinib PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL NAME/STAMP:
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
Dear Parent/Guardian:
 Dear Parent/Guardian: If it is necessary for your child to receive Epinephrine during school hours, school health policy requires that you provide a written request for the administration of the prescribed
Dear Parent/Guardian: If it is necessary for your child to receive Epinephrine during school hours, school health policy requires that you provide a written request for the administration of the prescribed
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM DOCETAXEL + PREDNISOLONE. Patient s first names
 Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM DOCETAXEL + PREDNISOLONE Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM DOCETAXEL + PREDNISOLONE Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s
Abdominal Surgery. Beyond Medicine. Caring for Yourself at Home. ilearning about your health
 ilearning about your health Abdominal Surgery Caring for Yourself at Home www.cpmc.org/learning Beyond Medicine. Table of Contents Your Checklist for Going Home...3 Arranging Transportation Home...3 Making
ilearning about your health Abdominal Surgery Caring for Yourself at Home www.cpmc.org/learning Beyond Medicine. Table of Contents Your Checklist for Going Home...3 Arranging Transportation Home...3 Making
SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE. Student Name: Current Date: Date of Birth: Grade:
 SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE Student Name: Current Date: Date of Birth: Grade: 1. Describe in detail what your child is allergic to: 2. How often does your child have a severe
SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE Student Name: Current Date: Date of Birth: Grade: 1. Describe in detail what your child is allergic to: 2. How often does your child have a severe
2200 Northern Boulevard, Suite 133 East Hills, NY Fax (516) Transitional Care
 Transitional Care") 2200 Northern Boulevard, Suite 133 East Hills, NY 11548 855-670-6077 Fax (516) 918-9039 Transitional Care Dear New Patient: We welcome you to our practice as a transitional patient. We will be managing
2200 Northern Boulevard, Suite 133 East Hills, NY 11548 855-670-6077 Fax (516) 918-9039 Transitional Care Dear New Patient: We welcome you to our practice as a transitional patient. We will be managing
College of Sequoias Physical Therapist Assistant Program Student Health Release Form
 Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
MANDATORY HEALTH FORMS
 MANDATORY HEALTH FORMS All forms must be completed prior to enrollment Contact Information: School Nurse: nurse@grandriver.org Admissions: admissions@grandriver.org Checklist of Required Forms & Items:
MANDATORY HEALTH FORMS All forms must be completed prior to enrollment Contact Information: School Nurse: nurse@grandriver.org Admissions: admissions@grandriver.org Checklist of Required Forms & Items:
TALK. Health. The right dose. May is Mental Health Month. 4 tips for people who use antidepressants
 VOLTEE PARA ESPAÑOL! SPRING 2016 Health THE KEY TO A GOOD LIFE TALK IS A GREAT PLAN May is Mental Health Month. Everyone deserves good mental health. Whether you have a minor mental health condition that
VOLTEE PARA ESPAÑOL! SPRING 2016 Health THE KEY TO A GOOD LIFE TALK IS A GREAT PLAN May is Mental Health Month. Everyone deserves good mental health. Whether you have a minor mental health condition that
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
Integrative Therapies 7E Oak Branch Drive Greensboro, NC
 Integrative Therapies 7E Oak Branch Drive Greensboro, NC 27407 www.integrativetherapies.net 336-294-0910 Hello! Welcome to Integrative Therapies and Integrative Pain Medicine, We are very happy that you
Integrative Therapies 7E Oak Branch Drive Greensboro, NC 27407 www.integrativetherapies.net 336-294-0910 Hello! Welcome to Integrative Therapies and Integrative Pain Medicine, We are very happy that you
Rosati Family Chiropractic Intake Form
 Patient Data Date Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name I prefer to be called by Address City State Zip Code Home Phone ( ) - Work Phone ( ) - Cell Phone (
Patient Data Date Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name I prefer to be called by Address City State Zip Code Home Phone ( ) - Work Phone ( ) - Cell Phone (
PHONE: (813) FAX:
 FAX:") Welcome to Natural Healing of Tampa Bay! We look forward to meeting you and also working with you towards your wellness goal. We have enclosed a new patient packet which should be filled out prior to your
Welcome to Natural Healing of Tampa Bay! We look forward to meeting you and also working with you towards your wellness goal. We have enclosed a new patient packet which should be filled out prior to your
Subacute Care. 1. Define important words in the chapter. 2. Discuss the types of residents who are in a subacute setting
 175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
HEALTH. CENTER Main St NE, Suite 101 PO Box 507 Duvall, WA ph fax Dr. Jeffrey P. Metcalf
 Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
When Your Loved One is Dying at Home
 When Your Loved One is Dying at Home What can I expect? What can I do? Although it is impossible to totally prepare for a death it may be easier if you know what to expect. Hospice Palliative Care aims
When Your Loved One is Dying at Home What can I expect? What can I do? Although it is impossible to totally prepare for a death it may be easier if you know what to expect. Hospice Palliative Care aims
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cabozantinib PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL NAME/STAMP:
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cabozantinib PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH: NHS NUMBER: (or other identifier) HOSPITAL NAME/STAMP:
Age: Birthdate: Date of Last Physical exam:
 Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Congestive Heart Failure
 TM Nightingale Congestive Heart Failure Do you or someone you know have any of the following symptoms? 1. Shortness of breath (dyspnea) when you exert yourself or when you lie down 2. Swelling in your
TM Nightingale Congestive Heart Failure Do you or someone you know have any of the following symptoms? 1. Shortness of breath (dyspnea) when you exert yourself or when you lie down 2. Swelling in your
James M. Wilson, M.D. - Medical Information to (fax to ) PATIENT INFORMATION Last name: First: D.O.
 PATIENT INFORMATION Last name: First: D.O.") James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
Symptoms and Ill Health (Present State)
") Name Date Address City State Zip Home Phone ( ) Work Phone ( ) Cell ( ) Date of Birth Age ( ) Referred by Friend/Family Yelp Google Other Search Engine Facebook Instagram Groupon Event PhoneBook Occupation
Name Date Address City State Zip Home Phone ( ) Work Phone ( ) Cell ( ) Date of Birth Age ( ) Referred by Friend/Family Yelp Google Other Search Engine Facebook Instagram Groupon Event PhoneBook Occupation
Entrance Case History (Please write or print clearly)
") Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
Patient Information: Last Name First Name MI. Address Apt/Room # City Zip. Community name (if not at home) Martial Status: S M W D
 Martial Status: S M W D") HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
ALASKA COMMUNITY HEALTH AIDE/PRACTITIONER PROGRAM Standing Orders
 CHA/P Name: Village: Tribal Health Organization: is authorized to treat patients with the CHAM ASSESSMENTS that are initialed below according to the PLAN listed in the 2006 Alaska Community Health Aide/Practitioner
CHA/P Name: Village: Tribal Health Organization: is authorized to treat patients with the CHAM ASSESSMENTS that are initialed below according to the PLAN listed in the 2006 Alaska Community Health Aide/Practitioner
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD
 Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
MARATHON HEALTH CENTER AND HEALTH COACHING a benefit of CHG Health and Wellness for our North Carolina office
 Health & Wellness MARATHON HEALTH CENTER AND HEALTH COACHING a benefit of CHG Health and Wellness for our North Carolina office WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE
Health & Wellness MARATHON HEALTH CENTER AND HEALTH COACHING a benefit of CHG Health and Wellness for our North Carolina office WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE
Food / Insect Allergy Action Plan
 Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Tennessee Neurology Specialists Affiliated with Baptist Healthcare Group
 Tennessee Neurology Specialists Affiliated with Baptist Healthcare Group Oscar E. Mendez, M.D. Rejane Lisboa, M.D. Williamson Medical Center Tower 4323 Carothers Pkwy, Suite 303 Franklin, TN 37067 Phone:
Tennessee Neurology Specialists Affiliated with Baptist Healthcare Group Oscar E. Mendez, M.D. Rejane Lisboa, M.D. Williamson Medical Center Tower 4323 Carothers Pkwy, Suite 303 Franklin, TN 37067 Phone:
Making the Most of the Ambulance Service
 Making the Most of the Ambulance Service ~ When do we need an ambulance? ~ In recent years, we have seen an increase in both the number of times ambulances get called out, and
Making the Most of the Ambulance Service ~ When do we need an ambulance? ~ In recent years, we have seen an increase in both the number of times ambulances get called out, and
Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, Patient Data Sheet
 Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, 63119 314.484.0690 Patient Data Sheet Date Name: Address: City: State: Zip: Social Security Number: - - Email: Home Phone: ( ) Cell Ph.: ( ) Work Ph.:
Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, 63119 314.484.0690 Patient Data Sheet Date Name: Address: City: State: Zip: Social Security Number: - - Email: Home Phone: ( ) Cell Ph.: ( ) Work Ph.:
WELCOME TO USF HEALTH
 WELCOME TO USF HEALTH We appreciate you choosing USF Health for your healthcare needs. When you come to see a new healthcare provider, you may have questions about what to expect at your first visit. We
WELCOME TO USF HEALTH We appreciate you choosing USF Health for your healthcare needs. When you come to see a new healthcare provider, you may have questions about what to expect at your first visit. We
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY:
 PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cetuximab (+/- platinum-based chemotherapy) HOSPITAL NAME/STAMP: PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH:
PATIENT AGREEMENT TO SYSTEMIC ANTI- CANCER THERAPY: Cetuximab (+/- platinum-based chemotherapy) HOSPITAL NAME/STAMP: PATIENT DETAILS PATIENT S SURNAME/FAMILY NAME: PATIENT S FIRST NAME(S): DATE OF BIRTH:
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet
 Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
Before and After Hospital Admission for Surgery. Dartmouth General Hospital
 2015 Before and After Hospital Admission for Surgery Dartmouth General Hospital Before and After Hospital Admission for Surgery Dartmouth General Hospital Welcome. This pamphlet will give you some information
2015 Before and After Hospital Admission for Surgery Dartmouth General Hospital Before and After Hospital Admission for Surgery Dartmouth General Hospital Welcome. This pamphlet will give you some information
Ogden City School District Allergy Health and Emergency Care Plan for School. School: Grade: School Year:
 PARENTS: Please place student s picture here Ogden City School District Allergy Health and Emergency Care Plan for School Student Name: Student must avoid contact with known allergen. School staff must
PARENTS: Please place student s picture here Ogden City School District Allergy Health and Emergency Care Plan for School Student Name: Student must avoid contact with known allergen. School staff must
Welcome to our Chiropractic Office! P l e a s e P r i n t C l e a r l y a n d f i l l I n c o m p l e t e l y.
 Welcome to our Chiropractic Office! P l e a s e P r i n t C l e a r l y a n d f i l l I n c o m p l e t e l y. Print Name Email Street Address Phone City State Zip Date of Birth Please Check Sex: Male
Welcome to our Chiropractic Office! P l e a s e P r i n t C l e a r l y a n d f i l l I n c o m p l e t e l y. Print Name Email Street Address Phone City State Zip Date of Birth Please Check Sex: Male
WELCOME TO OUR PRACTICE
 LVPG INTERNAL MEDICINE Phone 484-661-4650 Fax 610-402-1153 3080 Hamilton Boulevard, Suite 350 Allentown, PA 18103 Office Hours: Monday: 8:00 a.m. 9:00 p.m. Tuesday Friday: 8:00am 5:00pm WELCOME TO OUR
LVPG INTERNAL MEDICINE Phone 484-661-4650 Fax 610-402-1153 3080 Hamilton Boulevard, Suite 350 Allentown, PA 18103 Office Hours: Monday: 8:00 a.m. 9:00 p.m. Tuesday Friday: 8:00am 5:00pm WELCOME TO OUR
Patient Demographic Sheet Chart # (clinic use only)
") Patient Demographic Sheet Chart # (clinic use only) Date: Annual Verification/Date/initials Best Contact Number to Reach You: Patient Information: Please List All Children in the Family Last First Middle
Patient Demographic Sheet Chart # (clinic use only) Date: Annual Verification/Date/initials Best Contact Number to Reach You: Patient Information: Please List All Children in the Family Last First Middle
Medication Administration Skill Checklist (to be accompanied by daily medication log for applicable students) 1 page
 1 page") See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication
See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication
Patient identifier/label: Page 1 of 6 PATIENT AGREEMENT TO SYSTEMIC THERAPY: CONSENT FORM CYTARABINE CONTINUOUS INFUSION
 Patient identifier/label: Page 1 of 6 CYTARABINE Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas Hospital King s College Hospital Lewisham Hospital
Patient identifier/label: Page 1 of 6 CYTARABINE Patient s surname/family name Patient s first names Date of birth Hospital Name: Guy s Hospital St. Thomas Hospital King s College Hospital Lewisham Hospital
PRESCRIBING PHYSCIAN ONLY.
 Return All Forms To: Administrative Address 985 Livingston Avenue North Brunswick, NJ 08902 Direct Phone/Fax: 732-737-8279 info@campjaycee.org Camp Address 223 Ziegler Road Effort, PA 18330 Phone: 570-629-3291
Return All Forms To: Administrative Address 985 Livingston Avenue North Brunswick, NJ 08902 Direct Phone/Fax: 732-737-8279 info@campjaycee.org Camp Address 223 Ziegler Road Effort, PA 18330 Phone: 570-629-3291
John L Ledbetter, M.D. Vince R. Forte, M.D. J. Hardy Gordon, M.D. Ronald L. Ellis, M.D.
 John L Ledbetter, M.D. Vince R. Forte, M.D. J. Hardy Gordon, M.D. Ronald L. Ellis, M.D. Board Certified Pain Medicine Anesthesiology Patient s Last Name First MI Mailing Address City State Zip Home Phone
John L Ledbetter, M.D. Vince R. Forte, M.D. J. Hardy Gordon, M.D. Ronald L. Ellis, M.D. Board Certified Pain Medicine Anesthesiology Patient s Last Name First MI Mailing Address City State Zip Home Phone
Understanding Health Care in America An introduction for immigrant patients
 Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
To be completed by healthcare provider
 Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Save up to $4,000 a year?!
 Save up to $4,000 a year?! Indication and Usage HYQVIA [Immune Globulin Infusion 10% (Human) with Recombinant Human Hyaluronidase] is an immune globulin with a recombinant human hyaluronidase indicated
Save up to $4,000 a year?! Indication and Usage HYQVIA [Immune Globulin Infusion 10% (Human) with Recombinant Human Hyaluronidase] is an immune globulin with a recombinant human hyaluronidase indicated