MS Medicaid Provider Enrollment
|
|
|
- Madison Melton
- 5 years ago
- Views:
Transcription


1 MS Medicaid Provider Enrollment
2 Agenda 1. Provider Enrollment Tips 2. Enrollment Package 3. General Application Information 4. Enroll Online Checking Application Status 7. Self Attestation 8. License Renewal 9. July 1 st Changes 10. FAQ s 11. Questions 5. Credentialing Checklist 6. Supporting Documentation Provider Disclosure Form
3 Provider Enrollment Tips Please print or type your application. Complete all applicable areas of the application. Be sure to review the Credentialing Checklist for your Provider Type for any specific information that may be required. Do not use Correction fluid/white-out on any part of the application. Original signatures are no longer required, however: Individual applications must be signed by the individual applying. Group applications must be signed by the owner of the group or a person granted signature authority by the Board of Directors Resolution Form. Retain a copy of your completed application for your records.
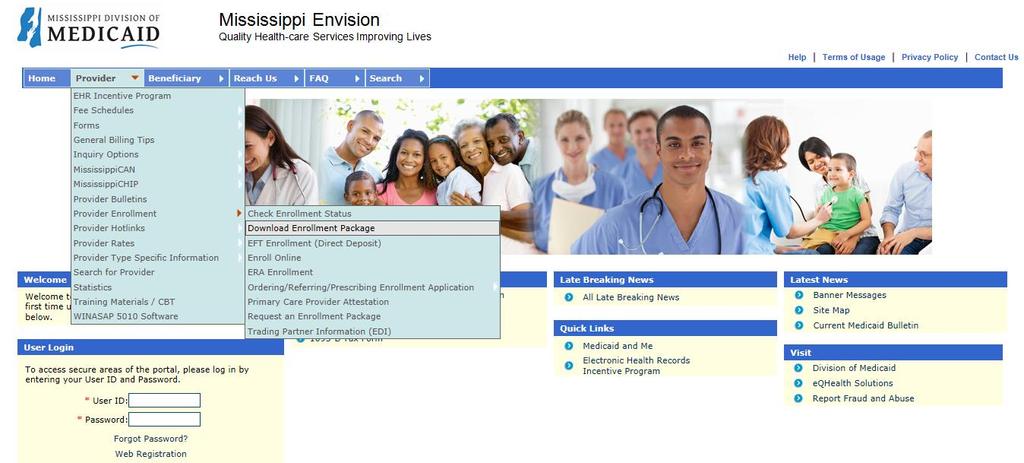
4 Enrollment Package
5 General Application Information Complete all addresses in Section 1 (page 2). The Social Security Number (individual) or Tax-id Number (group) should be entered in Section 2 (page 3). Be sure to select the appropriate Provider Type in which you are applying for. For all Waiver Services provider types, a proposal approval letter from the Division of Medicaid, as well as an approval letter from the Department of Health (for some waiver type cases) must be submitted with your completed enrollment application. (Effective July 1) For MD s and DO s, you must list your Specialty in Section 3 (page 5) of the application. If applying as a Group Provider, please indicate the active Individual Provider information in Section 4 (page 6).
6 General Application Information Cont. The Ownership Section (Section 7), pages 8-10 must be completed for all groups whether the owner is an Individual, County, City, or Corporation. NPI verification must be submitted. Must have confirmation from the NPPES site: Answer all sanction questions on page 10, and please mark none of these on page 10 if none of the questions apply. The application must be signed by the appropriate person on page 13 directly below the 6 statements (Section 11).


7 General Application Information Cont. Completed applications may be mailed in its entirety to the address below: Xerox State Healthcare ATTENTION: Provider Enrollment P.O. Box Jackson, MS Or faxed to:
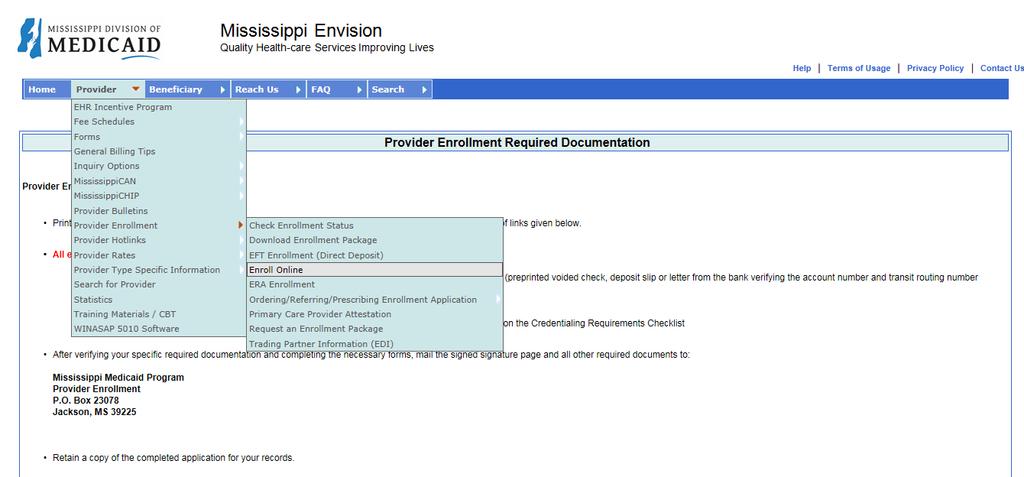
8 Enrollment Online

9 Enrollment Online Provider < Provider Enrollment < Enroll Online Create a New Application To submit a Provider Enrollment Application online, the Provider must enter a valid address to start the online application.

10 Checking Application Status

11 Checking Application Status Cont.

12 Checking Application Status Cont. Recall Your Existing Application Once the Provider starts the online application, the application will be given a Reference Number. The Provider can save the application and use the Reference Number to refer back to the saved application. Forgot Your Reference Number The Provider can enter valid to get the Reference Number associated with that address.


13 Credentialing Checklist
14 Supporting Documentation Additional or Supporting Documents will vary by Provider Types. You can find these requirements on the Credentialing Checklist within the application. However, the most basic requirements that are the same across the board are listed below: Application with signature Direct Deposit Authorization Agreement Voided check or other acceptable bank verification License Provider Participation Agreement W-9 Social Security or IRS Verification Civil Rights Compliance Packet NPI Verification CLIA form, if applicable Note: When completing the application online, please include the Application Tracking number on each supporting document.


15 Forms Provider Participation Agreement

16 Forms Board of Directors
17 Forms Board of Directors Resolution Forms This form is only required when there is more than one owner or if the owner is a corporation, group, city or county entity. This form is also required if there is only one owner, yet that owner would like to grant someone else signature authority. A person cannot authorize themselves. The form must be notarized. Only the person authorized is allowed to sign any and all documents contained in the application with the exception of the W-9. In lieu of this form, an organization may include their meeting minutes if it lists the person authorized to sign on behalf of the group. The minutes must be signed and notarized.

18 Forms Direct Deposit Authorization Agreement

19 Forms IRS Form W-9


20 Forms Civil Rights Compliance Package

21 Provider Disclosure Form
22 Provider Disclosure Form Cont. Individual Providers Individuals should fill out Section A. Please review and complete all other applicable sections and sign the document. Group Providers Groups should review and complete all applicable sections of the form and have the individual with signature authority sign the document.
23 Provider Attestation Mississippi Division of Medicaid (DOM) was granted the authority to continue reimbursing eligible providers, as determined by the Patient Protection and Affordable Care Act (PPACA), for an increased payment for certain Evaluation and Management (E&M) and Vaccine Administration codes. Effective July 1, 2016, reimbursement of certain primary care services provided by eligible providers will be at 100 percent of the Medicare Physician Fee Schedule. The DOM Primary Care Provider Fee Schedule is updated July 1 of each year based on 100 percent of the Medicare Physician Fee Schedule, which takes effect January 1 of each year. To receive the increased payment for dates of service (DOS) beginning 7/1/2016, eligible providers must send a completed and signed 7/1/2016 6/30/2018 Self-Attestation Statement form to Xerox Provider Enrollment by 6/30/2016 through one of the following means: msinquiries@xerox.com Fax: Postal mail: P. O. Box 23078, Jackson, MS 39225

24 Provider Attestation Form
25 Provider Attestation (OBGYN) Mississippi Division of Medicaid (DOM) was granted authority to continue reimbursing eligible providers, as determined by the Patient Protection and Affordable Care Act (PPACA), for an increased payment for certain primary care Evaluation and Management (E&M) and Vaccine Administration codes. Pursuant to HB 1560, effective July 1, 2016 providers who selfattest to a specialty designation in obstetric/gynecologic medicine by the American Congress of Obstetricians and Gynecologists (ACOG) will be eligible for an increased payment for certain primary care services. To receive the increased payment for dates of service (DOS) beginning 7/1/2016, eligible Obstetric/Gynecological providers must send a completed and signed 7/1/2016 6/30/2017 Obstetrician/Gynecologist (OB/GYN) Self-Attestation Statement form to Xerox Provider Enrollment by 6/30/2016 through one of the following means: msinquiries@xerox.com Fax: Postal mail: P. O. Box 23078, Jackson, MS Effective July 1, 2016, reimbursement of certain primary care services provided by eligible providers will be at 100 percent of the Medicare Physician Fee Schedule. The Medicaid Primary Care Provider Fee Schedule is updated July 1 of each year based on one hundred percent of the Medicare Physician Fee Schedule, which takes effect January 1 of each year.
26 Provider Attestation (OBGYN) Cont. Providers whose 7/1/2016 6/30/2017 Obstetrician/Gynecologist (OB/GYN) Self-Attestation Statement forms are ed, postmarked or faxed after 6/30/2016, may experience a delay in the effective date of the increased payment. Providers must notify Xerox of any change(s) to their completed 7/1/2016 6/30/2017 Obstetrician/Gynecologist (OB/GYN) Self-Attestation Statement form. Providers can verify the processing of self-attestation statement forms they have submitted electronically by accessing the Envision Web Portal at You can locate the form on the DOM website under the Forms section and the Envision Web Portal, or request it by calling the Xerox Call Center toll-free at

27 Provider Attestation Form (OBGYN)
28 Provider License Renewal License renewal depends on the provider type. Some provider licenses end on where other provider licenses don t. Letters are sent out at the 60 and 30 days prior to your license renewal time. An additional letter is also sent out once the license has been suspended due to non-renewal of license. Please contact the call center if you are unsure of the status of your license end date. The number of the call center is Any suspension of a provider s license will possibly result in non-payment of claims.
29 Effective July 1, 2016 Waiver Providers will be required to submit a proposal approval letter from the Division of Medicaid, as well as an approval letter from the Department of Health (for some Waiver Provider Types) along with their completed application. The Credentialing Checklist will be updated to include new requirements for Waiver Providers, such as the Medicaid Approval Proposal Letter. The Provider Disclosure Form will be required on all applications submitted on or after 7/1/2016.
30 Frequently Asked Questions Q. How long does it take to process an enrollment application? A. Generally, complete applications will take 6-8 weeks to be processed. Incomplete applications are returned. To avoid delays, please ensure all applications are complete with the required forms and attachments. Q. Should I hold claims until I receive a provider number? A. For initial enrollment, Yes. For providers re-enrolling, No. Q. Do I have to participate in Direct Deposit? A. Yes, all providers must participate in direct deposit.
31 Frequently Asked Questions Cont. Q. Why must we complete and submit a W-9? A. The W-9 is required by the IRS. Q. Why do we have to submit verification of social security and/or federal tax-id numbers? A. DOM must verify this information to comply with IRS requirements. Note: In accordance with CMS regulations, in January 2014, the Mississippi Division of Medicaid began requiring all Ordering, Referring, Prescribing, and Medicare-cost sharing physicians to be enrolled with Mississippi Medicaid. There is a separate application available.
32 Questions
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST. ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) ASSESSOR
 (Environmental Modifications) ASSESSOR") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) ASSESSOR (Enrollment packet is subject to change without notice)
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) ENVIRONMENTAL ACCESSIBILITY ADAPTATIONS (EAA) (Environmental Modifications) ASSESSOR (Enrollment packet is subject to change without notice)
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) Assistive Devices (Enrollment packet is subject to change without notice) Revised 03/15 GENERAL INFORMATION FOR PROVIDER ENROLLMENT Provider
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) Assistive Devices (Enrollment packet is subject to change without notice) Revised 03/15 GENERAL INFORMATION FOR PROVIDER ENROLLMENT Provider
MS Envision Web Portal Homepage
 Web Portal Review MS Envision Web Portal Homepage http://ms-medicaid.com Provider Tab (Non-Secure) Web Portal Non-Secure Features What s New Late Breaking News Current Medicaid Bulletin Provider Lookup
Web Portal Review MS Envision Web Portal Homepage http://ms-medicaid.com Provider Tab (Non-Secure) Web Portal Non-Secure Features What s New Late Breaking News Current Medicaid Bulletin Provider Lookup
Registered Dietician (Individual)
") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Registered Dietician (Individual) (Enrollment packet is subject to change without notice) GENERAL INFORMATION FOR THE INDIVIDUAL REGISTERED
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Registered Dietician (Individual) (Enrollment packet is subject to change without notice) GENERAL INFORMATION FOR THE INDIVIDUAL REGISTERED
Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013
 Wednesday, January 16, 2013") Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013 2 1 3 4 2 5 6 3 7 Applications received by PED after 60 days will be reviewed as new applications.
Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013 2 1 3 4 2 5 6 3 7 Applications received by PED after 60 days will be reviewed as new applications.
Family Planning Clinic
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Family Planning Clinic (Enrollment packet is subject to change without notice) (PT71) 07/10 Family Planning Clinic CHECKLIST OF FORMS
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Family Planning Clinic (Enrollment packet is subject to change without notice) (PT71) 07/10 Family Planning Clinic CHECKLIST OF FORMS
ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic
 Rural Health Clinic") LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic (Enrollment packet is subject to change without
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic (Enrollment packet is subject to change without
The Credentialing Process. Note! Contents are subject to change and are not a guarantee of payment.
 The Credentialing Process Note! Contents are subject to change and are not a guarantee of payment. Introduction to Credentialing BlueCross BlueShield of South Carolina, BlueChoice HealthPlan of South Carolina
The Credentialing Process Note! Contents are subject to change and are not a guarantee of payment. Introduction to Credentialing BlueCross BlueShield of South Carolina, BlueChoice HealthPlan of South Carolina
Alphabet Soup of Provider Credentialing. Anne Hanzel Alta Partners, LLC
 Alphabet Soup of Provider Credentialing Anne Hanzel Alta Partners, LLC Why is Credentialing Important? Patient Safety Build practice base Allow for discounted amounts Direct link to managed care systems
Alphabet Soup of Provider Credentialing Anne Hanzel Alta Partners, LLC Why is Credentialing Important? Patient Safety Build practice base Allow for discounted amounts Direct link to managed care systems
Provider Enrollment. August 2016
 Provider Enrollment August 2016 Overview Enrollment Requirements Provider Responsibilities Enrollment Process Affiliations Signatures and Supporting Documentation 2 Enrollment Requirements 3 Enrollment
Provider Enrollment August 2016 Overview Enrollment Requirements Provider Responsibilities Enrollment Process Affiliations Signatures and Supporting Documentation 2 Enrollment Requirements 3 Enrollment
Federally Qualified Health Center
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Federally Qualified Health Center (Enrollment packet is subject to change without notice) (PT72) 07/10 Revised 05/10 FQHC Provider Type
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Federally Qualified Health Center (Enrollment packet is subject to change without notice) (PT72) 07/10 Revised 05/10 FQHC Provider Type
Supervised Independent Living (SIL)
") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Supervised Independent Living (SIL) (Enrollment packet is subject to change without notice) PT89 07/10 GENERAL INFORMATION REGARDING
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Supervised Independent Living (SIL) (Enrollment packet is subject to change without notice) PT89 07/10 GENERAL INFORMATION REGARDING
Practitioners may be recredentialed at any time, but in no circumstance longer than a 36 month period.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
*NOTICE * THIS APPLICATION WAS REVISED IN JUNE 2015 PLEASE READ CAREFULLY -
 *NOTICE * THIS APPLICATION WAS REVISED IN JUNE 2015 PLEASE READ CAREFULLY - Initial License Application To Operate a Specialty Care Assisted Living Facility: SCALF Regulations regarding the application
*NOTICE * THIS APPLICATION WAS REVISED IN JUNE 2015 PLEASE READ CAREFULLY - Initial License Application To Operate a Specialty Care Assisted Living Facility: SCALF Regulations regarding the application
The Plan will not credential trainees who do not maintain a separate and distinct practice from their training practice.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process.
 CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Early Steps (Group)
 Early Steps (Group)") ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Early Steps (Group) (Enrollment packet is subject to change without notice) (PT29 Early Steps Group) Revised
ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Early Steps (Group) (Enrollment packet is subject to change without notice) (PT29 Early Steps Group) Revised
DM Quality Consulting, LLC
 DM Quality Consulting, LLC Providing an honest, compliant, quality service Medicare Provider Enrollment Paper Applications Physicians, non-physician practitioners, suppliers, hospitals and clinics must
DM Quality Consulting, LLC Providing an honest, compliant, quality service Medicare Provider Enrollment Paper Applications Physicians, non-physician practitioners, suppliers, hospitals and clinics must
Personal Emergency Response System
 LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Emergency Response System (Enrollment packet is subject
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Emergency Response System (Enrollment packet is subject
This letter is to let you know that you are due for re-credentialing as a participating provider for AmeriHealth Caritas Louisiana of Louisiana.
 ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
EPSDT Health Services
 LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) EPSDT Health Services (Enrollment packet is subject to change without
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) EPSDT Health Services (Enrollment packet is subject to change without
Personal Care Attendant
 LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Care Attendant (Enrollment packet is subject to change
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Care Attendant (Enrollment packet is subject to change
*NOTICE * THIS APPLICATION WAS REVISED IN JULY 2016 PLEASE READ CAREFULLY -
 *NOTICE * THIS APPLICATION WAS REVISED IN JULY 2016 PLEASE READ CAREFULLY - Change of Ownership License Application To Operate a Cerebral Palsy Treatment Facility Regulations affecting the application
*NOTICE * THIS APPLICATION WAS REVISED IN JULY 2016 PLEASE READ CAREFULLY - Change of Ownership License Application To Operate a Cerebral Palsy Treatment Facility Regulations affecting the application
NEW HAMPSHIRE MEDICAID EHR INCENTIVE PROGRAM. Reference Guide for Eligible Professionals
 NEW HAMPSHIRE MEDICAID EHR INCENTIVE PROGRAM Reference Guide for Eligible Professionals REVISION HISTORY Version Number Date Comments 1.0 March 1, 2012 Initial Distribution to Pilot Participants; CMS Review
NEW HAMPSHIRE MEDICAID EHR INCENTIVE PROGRAM Reference Guide for Eligible Professionals REVISION HISTORY Version Number Date Comments 1.0 March 1, 2012 Initial Distribution to Pilot Participants; CMS Review
Hospital Credentialing Application
 Hospital Credentialing Application Thank you for your interest in Superior HealthPlan. Please use this checklist to ensure you have all necessary contract and credentialing items to avoid processing delays.
Hospital Credentialing Application Thank you for your interest in Superior HealthPlan. Please use this checklist to ensure you have all necessary contract and credentialing items to avoid processing delays.
Federal law does not require state Medicaid programs to cover specific substance use disorder interventions
 Federal law does not require state Medicaid programs to cover specific substance use disorder interventions States have the option Coverage differs state-by-state Prior authorizations are often necessary
Federal law does not require state Medicaid programs to cover specific substance use disorder interventions States have the option Coverage differs state-by-state Prior authorizations are often necessary
Credentialing Application for Hospitals and Facilities
 Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Chiropractor
 Chiropractor") LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Chiropractor (Enrollment packet is subject to change without notice)
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Chiropractor (Enrollment packet is subject to change without notice)
LIBERTY DENTAL PLAN. Provider Credentialing Application. (* Required Fields) *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )
 *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )") (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
Provider Application Packet Respite Care Providers 1915(i) Intensive Behavioral Health Services for Children, Youth, and Families
 Intensive Behavioral Health Services for Children, Youth, and Families") Provider Application Packet Respite Care Providers 1915(i) Intensive Behavioral Health Services for Children, Youth, and Families To: From: Re: 1915(i) Program Applicants Maryland Department of Health
Provider Application Packet Respite Care Providers 1915(i) Intensive Behavioral Health Services for Children, Youth, and Families To: From: Re: 1915(i) Program Applicants Maryland Department of Health
Aetna Better Health Hospital Credentialing Packet Table of Contents
 Aetna Better Health Hospital Credentialing Packet 1. Cover Letter 2. Checklist 3. Medicaid Ownership Code Document 4. Credentialing Application 5. Behavioral Health Supplement 6. Medicaid Disclosure Form
Aetna Better Health Hospital Credentialing Packet 1. Cover Letter 2. Checklist 3. Medicaid Ownership Code Document 4. Credentialing Application 5. Behavioral Health Supplement 6. Medicaid Disclosure Form
2018 CHAMPS UPDATE INSIDE
 2018 CHAMPS UPDATE INSIDE Federal Requirements Mean HKD/HMP Dentists Must Enroll in CHAMPS You need to know this information if you accept Healthy Kids Dental or Healthy Michigan Plan patients. UPDATED
2018 CHAMPS UPDATE INSIDE Federal Requirements Mean HKD/HMP Dentists Must Enroll in CHAMPS You need to know this information if you accept Healthy Kids Dental or Healthy Michigan Plan patients. UPDATED
Optima Health New Provider Application Packet
 Optima Health New Provider Application Packet Thank you for your interest in becoming a participating provider in the Optima Health Network. Please review the following instructions to ensure acceptance
Optima Health New Provider Application Packet Thank you for your interest in becoming a participating provider in the Optima Health Network. Please review the following instructions to ensure acceptance
Application Checklist for Facilities
 Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Individual Educational Activity Eligibility Verification Form
 Individual Educational Activity Eligibility Verification Form New Jersey State Nurses Association is accredited as an approver of continuing nursing education with distinction by the American Nurses Credentialing
Individual Educational Activity Eligibility Verification Form New Jersey State Nurses Association is accredited as an approver of continuing nursing education with distinction by the American Nurses Credentialing
CRNA INITIAL CREDENTIALING APPLICATION
 CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
Provider Enrollment and Change Process Required Document Checklist
 Provider Enrollment and Change Process Required Document Checklist Provider Classification To avoid processing delays gather these items before you get started. If applying to network, complete the application
Provider Enrollment and Change Process Required Document Checklist Provider Classification To avoid processing delays gather these items before you get started. If applying to network, complete the application
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Children s Choice (Enrollment packet is subject to change without notice) Revised 01/15 GENERAL INFORMATION REGARDING WAIVER ENROLLMENTS
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Children s Choice (Enrollment packet is subject to change without notice) Revised 01/15 GENERAL INFORMATION REGARDING WAIVER ENROLLMENTS
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD.
 MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
BCBSNC Provider Application for Participation
 BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
PAYMENT ERROR RATE MEASUREMENT
 Published by First Health Services Corporation for the Alaska Department of Health & Social Services September 2007 Volume 2, Number 9 First Health Services Corp. 1835 S. Bragaw St., Suite 200 Anchorage,
Published by First Health Services Corporation for the Alaska Department of Health & Social Services September 2007 Volume 2, Number 9 First Health Services Corp. 1835 S. Bragaw St., Suite 200 Anchorage,
Network Participant Credentialing Application
 Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
(EHR) Incentive Program
 Incentive Program") REGISTRATION USER GUIDE For Eligible Professionals Medicare Electronic Health Record (EHR) Incentive Program DECEMBER 2010 (12.28.10 ver2) CONTENTS Step 1... Getting started 3 Step 2... Login instruction
REGISTRATION USER GUIDE For Eligible Professionals Medicare Electronic Health Record (EHR) Incentive Program DECEMBER 2010 (12.28.10 ver2) CONTENTS Step 1... Getting started 3 Step 2... Login instruction
AgeWell New York Provider Relations 1991 Marcus Avenue Suite M201 Lake Success, NY 11042
 Dear Provider/Facility: Thank you for your interest in becoming a network provider/facility for AgeWell New York, LLC. In accordance with our commitment to the quality of health care services delivered
Dear Provider/Facility: Thank you for your interest in becoming a network provider/facility for AgeWell New York, LLC. In accordance with our commitment to the quality of health care services delivered
Mississippi Medicaid Hospice Services Provider Manual
 Mississippi Medicaid Hospice Services Provider Manual Effective: January 2011 Revised: January 2017 Table of Contents I. Introduction II. Frequently Used Terms III. Getting Started Helpful Tips A. Before
Mississippi Medicaid Hospice Services Provider Manual Effective: January 2011 Revised: January 2017 Table of Contents I. Introduction II. Frequently Used Terms III. Getting Started Helpful Tips A. Before
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM
 ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
Ohio Home Care Waiver Provider Application Process
 Ohio Home Care Waiver Provider Application Process Provider Enrollment Website medicaid.ohio.gov Hover over the Providers Tab Hover over Enrollment and Support Click Provider Enrollment On the next page,
Ohio Home Care Waiver Provider Application Process Provider Enrollment Website medicaid.ohio.gov Hover over the Providers Tab Hover over Enrollment and Support Click Provider Enrollment On the next page,
NORTH CAROLINA MARRIAGE AND FAMILY THERAPY LICENSURE BOARD
 NORTH CAROLINA MARRIAGE AND FAMILY THERAPY LICENSURE BOARD Mailing Address: Post Office Box 5549, Cary, NC 27512 Phone: (919) 469-8081 Fax: (919) 336-5156 Email: ncmftlb@nc.rr.com Web: www.nclmft.org APPLICATION
NORTH CAROLINA MARRIAGE AND FAMILY THERAPY LICENSURE BOARD Mailing Address: Post Office Box 5549, Cary, NC 27512 Phone: (919) 469-8081 Fax: (919) 336-5156 Email: ncmftlb@nc.rr.com Web: www.nclmft.org APPLICATION
Values Accountability Integrity Service Excellence Innovation Collaboration
 n00256 Recredentialing Process Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: The purpose of recredentialing is to assure that Network Health Plan/Network
n00256 Recredentialing Process Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: The purpose of recredentialing is to assure that Network Health Plan/Network
Pfizer Patient Assistance Program
 Pfizer Patient Assistance Program Application for Patients This application form is for patients who would like to apply to receive INFLECTRA (infliximab-dyyb) for Injection, NIVESTYM (filgrastim-aafi)
Pfizer Patient Assistance Program Application for Patients This application form is for patients who would like to apply to receive INFLECTRA (infliximab-dyyb) for Injection, NIVESTYM (filgrastim-aafi)
Organizational Provider Credentialing Application
 Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
MassHealth Provider Billing and Services Updates & Upcoming Initiatives. Massachusetts Health Care Training Forum July 2011
 MassHealth Provider Billing and Services Updates & Upcoming Initiatives Massachusetts Health Care Training Forum July 2011 Agenda I. MassHealth Updates/Resources & Upcoming MassHealth Initiatives II. Paper
MassHealth Provider Billing and Services Updates & Upcoming Initiatives Massachusetts Health Care Training Forum July 2011 Agenda I. MassHealth Updates/Resources & Upcoming MassHealth Initiatives II. Paper
Included in this packet are: 1915(i) Program Applicants. Maryland Department of Health
 Program Applicants. Maryland Department of Health") Provider Application Packet Intensive In-Home Service Mobile Crisis Response 1915(i) Intensive Behavioral Health Services for Children, Youth, and Families To: From: Re: 1915(i) Program Applicants Maryland
Provider Application Packet Intensive In-Home Service Mobile Crisis Response 1915(i) Intensive Behavioral Health Services for Children, Youth, and Families To: From: Re: 1915(i) Program Applicants Maryland
EFFECTIVE DATE: 10/04. SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31
 SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
VNSNY CHOICE PRACTITIONER CREDENTIALING APPLICATION
 Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
Credentialing Verification Organization (CVO) Provider FAQ
 Provider FAQ") Credentialing Verification Organization (CVO) Provider FAQ 1. What is a CVO? TexasMedicalAssociation(TMA)andTexasMedicaidMCOsproposedastatewide CVO concept to facilitate provider credentialing, which was
Credentialing Verification Organization (CVO) Provider FAQ 1. What is a CVO? TexasMedicalAssociation(TMA)andTexasMedicaidMCOsproposedastatewide CVO concept to facilitate provider credentialing, which was
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s)
") Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
Template Language for Memorandum of Understanding between Duals Demonstration Health Plans and County Behavioral Health Department(s) Updated Draft February 14, 2013 In the duals demonstration, participating
Home and Community- Based Services Waiver Program. HP Provider Relations/October 2014
 Home and Community- Based Services Waiver Program HP Provider Relations/October 2014 Agenda Objectives Overview of the Home and Community- Based Services (HCBS) Waiver Program Member eligibility Billing
Home and Community- Based Services Waiver Program HP Provider Relations/October 2014 Agenda Objectives Overview of the Home and Community- Based Services (HCBS) Waiver Program Member eligibility Billing
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
UnitedHealthcare. Credentialing Plan
 UnitedHealthcare Credentialing Plan 2015-2016 Table of contents Section 1.0 Introduction... 1 Section 1.1 Purpose...1 Section 1.2 Credentialing Policy...1 Section 1.3 Authority of Credentialing Entity
UnitedHealthcare Credentialing Plan 2015-2016 Table of contents Section 1.0 Introduction... 1 Section 1.1 Purpose...1 Section 1.2 Credentialing Policy...1 Section 1.3 Authority of Credentialing Entity
(CARLSBAD CODE OF ORDINANCES - CHAPTER 24, ARTICLE III, SECTIONS ) Official Name of Organization: Mailing Address:
 Official Name of Organization: Mailing Address:") CITY OF CARLSBAD Planning, Engineering, and Regulation Department 114 S. Halagueno (PO Box 1569) Carlsbad, NM 88221 Phone (575) 885-1185 Fax (575) 628-8379 APPLICATION FOR AFFORDABLE HOUSING CONTRIBUTION
CITY OF CARLSBAD Planning, Engineering, and Regulation Department 114 S. Halagueno (PO Box 1569) Carlsbad, NM 88221 Phone (575) 885-1185 Fax (575) 628-8379 APPLICATION FOR AFFORDABLE HOUSING CONTRIBUTION
Medicaid Electronic Health Record (EHR) Incentive Program:
 Incentive Program:") Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Hospitals Presenters Yvonne Sanchez, HHSC Craig Earls, CGI February 10, 2011 Overview of EHR Incentive Program Rules and
Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Hospitals Presenters Yvonne Sanchez, HHSC Craig Earls, CGI February 10, 2011 Overview of EHR Incentive Program Rules and
National Provider Identifiers Registry
 The Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) mandated the adoption of standard unique identifiers for health care providers and
The Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) mandated the adoption of standard unique identifiers for health care providers and
State of California Health and Human Services Agency Department of Health Care Services
 TOBY DOUGLAS DIRECTOR EDMUND G. BROWN JR. GOVERNOR Dear Applicant: Thank you for your recent inquiry regarding participation in the Medi-Cal program. Please complete the enclosed Medi-Cal provider enrollment
TOBY DOUGLAS DIRECTOR EDMUND G. BROWN JR. GOVERNOR Dear Applicant: Thank you for your recent inquiry regarding participation in the Medi-Cal program. Please complete the enclosed Medi-Cal provider enrollment
Participant Direction Option (PDO) Training Developed for the Statewide Medicaid Managed Care Long Term Care Plans
 Training Developed for the Statewide Medicaid Managed Care Long Term Care Plans") Participant Direction Option (PDO) Training Developed for the Statewide Medicaid Managed Care Long Term Care Plans Presented by: Danielle Reatherford 1 Purpose The purpose of this presentation is to: Introduce
Participant Direction Option (PDO) Training Developed for the Statewide Medicaid Managed Care Long Term Care Plans Presented by: Danielle Reatherford 1 Purpose The purpose of this presentation is to: Introduce
INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG. Effective September 1, 2014
 FOR APR-DRG. Effective September 1, 2014") INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG Effective September 1, 2014 Who are we? eqhealth has a 16 year partnership with Mississippi Division of Medicaid (DOM) as the Utilization
INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG Effective September 1, 2014 Who are we? eqhealth has a 16 year partnership with Mississippi Division of Medicaid (DOM) as the Utilization
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: X60T Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: X60T Facility ID:
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY 3. NAME AND ADDRESS OF FACILITY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8L7Q Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8L7Q Facility ID:
Instructions and Application for Speech Language Pathologist Method 3, Meet all requirements for certifications(s) but do not have certification
 but do not have certification") HEALTH OCCUPATIONS PROGRAM Speech Language Pathology and Audiology P.O. Box 64882, St. Paul, Minnesota 55164-0882 Telephone: (651) 201-3726 Fax: (651) 201-3839 Email: health.slpa@state.mn.us Instructions
HEALTH OCCUPATIONS PROGRAM Speech Language Pathology and Audiology P.O. Box 64882, St. Paul, Minnesota 55164-0882 Telephone: (651) 201-3726 Fax: (651) 201-3839 Email: health.slpa@state.mn.us Instructions
Delegation Oversight 101: How to Pass Oversight Audits Session Code: TU01 Time: 8:00 a.m. 9:30 a.m. Total CE Credits: 1.5 Presenter: Angela Dorsey,
 Delegation Oversight 101: How to Pass Oversight Audits Session Code: TU01 Time: 8:00 a.m. 9:30 a.m. Total CE Credits: 1.5 Presenter: Angela Dorsey, MA and Sallye Marcus Delegation Oversight 101 - How to
Delegation Oversight 101: How to Pass Oversight Audits Session Code: TU01 Time: 8:00 a.m. 9:30 a.m. Total CE Credits: 1.5 Presenter: Angela Dorsey, MA and Sallye Marcus Delegation Oversight 101 - How to
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8MXL Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 8MXL Facility ID:
Provider Enrollment and Change Process Required Document Checklist
 Provider Enrollment and Change Process Required Document Checklist Provider Classification To avoid processing delays gather these items before you get started. If applying to network, complete the application
Provider Enrollment and Change Process Required Document Checklist Provider Classification To avoid processing delays gather these items before you get started. If applying to network, complete the application
MOUNT SINAI HEALTH PARTNERS IPA, LLC
 MOUNT SINAI HEALTH PARTNERS IPA, LLC PROVIDER APPLICATION FORM All providers associated with Mount Sinai Beth Israel, Mount Sinai Brooklyn, Mount Sinai St. Luke s, Mount Sinai West (formerly MS Roosevelt),
MOUNT SINAI HEALTH PARTNERS IPA, LLC PROVIDER APPLICATION FORM All providers associated with Mount Sinai Beth Israel, Mount Sinai Brooklyn, Mount Sinai St. Luke s, Mount Sinai West (formerly MS Roosevelt),
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 2FT5 Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: 2FT5 Facility ID:
Ann Land and Bertha Henschel Memorial Funds 2017 GRANT GUIDELINES SUMMARY
 s 2017 GRANT GUIDELINES SUMMARY The City of Sacramento s Commission invites you to apply for grants from the s. To be considered, applications must be received at the following address no later than 4:00
s 2017 GRANT GUIDELINES SUMMARY The City of Sacramento s Commission invites you to apply for grants from the s. To be considered, applications must be received at the following address no later than 4:00
UnitedHealthcare of Insurance Company of New York The Empire Plan. CREDENTIALING and RECREDENTIALING PLAN
 UnitedHealthcare of Insurance Company of New York The Empire Plan CREDENTIALING and RECREDENTIALING PLAN 2013-2014 2013 UnitedHealth Group The Empire Plan All Rights Reserved This Credentialing and Recredentialing
UnitedHealthcare of Insurance Company of New York The Empire Plan CREDENTIALING and RECREDENTIALING PLAN 2013-2014 2013 UnitedHealth Group The Empire Plan All Rights Reserved This Credentialing and Recredentialing
MEDICARE AND OTHER FEDERAL HEALTH CARE PROGRAMS PROVIDER/SUPPLIER ENROLLMENT APPLICATION INSTRUCTIONS General Application - HCFA 855
 I MEDICARE AND OTHER FEDERAL HEALTH CARE PROGRAMS PROVIDER/SUPPLIER ENROLLMENT APPLICATION INSTRUCTIONS General Application - HCFA 855 Upon completion, return this application and all necessary documentation
I MEDICARE AND OTHER FEDERAL HEALTH CARE PROGRAMS PROVIDER/SUPPLIER ENROLLMENT APPLICATION INSTRUCTIONS General Application - HCFA 855 Upon completion, return this application and all necessary documentation
Please Note: Please send all documentation related to the credentialing portion of this documentation to:
 Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: BSCproviderinfo@blueshieldca.com
Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: BSCproviderinfo@blueshieldca.com
Community Mental Health Centers PROVIDER TRAINING
 Community Mental Health Centers PROVIDER TRAINING June 18, 2008 & June 23, 2008 Revised July 22, 2008 LOUISIANA MEDICAID PROGRAM DEPARTMENT OF HEALTH AND HOSPITALS BUREAU OF HEALTH SERVICES FINANCING TABLE
Community Mental Health Centers PROVIDER TRAINING June 18, 2008 & June 23, 2008 Revised July 22, 2008 LOUISIANA MEDICAID PROGRAM DEPARTMENT OF HEALTH AND HOSPITALS BUREAU OF HEALTH SERVICES FINANCING TABLE
Brenda Fischer, Unit Supervisor 09/13/2012 Colleen B. Leach, Program Specialist 09/18/2012
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: LNUX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: LNUX PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Page 1 of 6 ADMINISTRATIVE POLICY AND PROCEDURE
 Page 1 of 6 SECTION: Contracts SUBJECT: Credentialing DATE OF ORIGIN: 6/1/08 REVIEW DATES: 8/1/15, 2/8/17 EFFECTIVE DATE: 12/1/17 APPROVED BY: EXECUTIVE DIRECTOR I. PURPOSE: To have a written system in
Page 1 of 6 SECTION: Contracts SUBJECT: Credentialing DATE OF ORIGIN: 6/1/08 REVIEW DATES: 8/1/15, 2/8/17 EFFECTIVE DATE: 12/1/17 APPROVED BY: EXECUTIVE DIRECTOR I. PURPOSE: To have a written system in
TRICARE SKILLED NURSING FACILITY APPLICATION. Please submit the completed application package to: Fax: Mail to:
 TRICARE SKILLED NURSING FACILITY APPLICATION Please submit the completed application package to: Fax: 855-831-7044 or Mail to: 1-877-988-9378 TRICARE SKILLED NURSING FACILITY PROVIDER APPLICATION Facility
TRICARE SKILLED NURSING FACILITY APPLICATION Please submit the completed application package to: Fax: 855-831-7044 or Mail to: 1-877-988-9378 TRICARE SKILLED NURSING FACILITY PROVIDER APPLICATION Facility
Facility and Ancillary Credentialing Application INSTRUCTIONS
 Facility and Ancillary Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided as
Facility and Ancillary Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided as
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00712
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: H0RJ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: H0RJ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Michelle McFarland, HFE NEII
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: PH3B Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY ID: PH3B Facility ID:
Provider Selection Criteria for PreferredOne Participating Practitioners
 Provider Selection Criteria for PreferredOne Participating Practitioners General Criteria 1. Practitioner must serve a specialty and/or geographic need for the good of the PreferredOne product for which
Provider Selection Criteria for PreferredOne Participating Practitioners General Criteria 1. Practitioner must serve a specialty and/or geographic need for the good of the PreferredOne product for which
ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING
 ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING Please attach copies of all applicable documents to the application: Copy of all Federal, State and/or local licenses required to operate
ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING Please attach copies of all applicable documents to the application: Copy of all Federal, State and/or local licenses required to operate
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
EMCARE HTN EMERGENCY PHYSICIANS National Provider Identifiers Registry
 1285700245 EMCARE HTN EMERGENCY PHYSICIANS National Provider Identifiers Registry The Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA)
1285700245 EMCARE HTN EMERGENCY PHYSICIANS National Provider Identifiers Registry The Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA)
Mary Heim, HPR-Social Work Specialist 09/03/2013
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: NKFZ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: NKFZ PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
TYPE OF CALL QUESTION ANSWER. from the CAQH database for the application process?
 Can Sandhills Center pull information from the CAQH database for the application process? This is a brand new credentialing application process, the entire application must be completed. Are there any
Can Sandhills Center pull information from the CAQH database for the application process? This is a brand new credentialing application process, the entire application must be completed. Are there any
MEDICAID ENROLLMENT PACKET
 MEDICAID ENROLLMENT PACKET Follow the steps below. This will prevent errors which will delay enrollment. Physicians Only: 1. Answer the one page questionnaire 2. SIGN EACH FORM where it indicates Signature
MEDICAID ENROLLMENT PACKET Follow the steps below. This will prevent errors which will delay enrollment. Physicians Only: 1. Answer the one page questionnaire 2. SIGN EACH FORM where it indicates Signature
APPLICATION CHECKLIST - IMPORTANT - Submit all items on the checklist below with your application to ensure faster processing.
 State of Florida Department of Business and Professional Regulation Board of Landscape Architecture Application for Licensure of a Business Entity: Certificate of Authorization Form # DBPR LA 2 1 of 6
State of Florida Department of Business and Professional Regulation Board of Landscape Architecture Application for Licensure of a Business Entity: Certificate of Authorization Form # DBPR LA 2 1 of 6
Connecticut Medicaid EHR Incentive Program Flexibility Checklist for Eligible Professionals for Meaningful Use Last Revision: May 27, 2015
 Connecticut Medicaid EHR Incentive Program Flexibility Checklist for Eligible Professionals for Meaningful Use Last Revision: May 27, 2015 The Medicaid EHR Incentive Program provides incentive payments
Connecticut Medicaid EHR Incentive Program Flexibility Checklist for Eligible Professionals for Meaningful Use Last Revision: May 27, 2015 The Medicaid EHR Incentive Program provides incentive payments
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00858
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2LL3 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: 2LL3 PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Behavioral Health Facility and Ancillary Credentialing Application
 Behavioral Health Facility and Ancillary Credentialing Application Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
Behavioral Health Facility and Ancillary Credentialing Application Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
RULES OF ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH CHAPTER FREESTANDING EMERGENCY DEPARTMENTS
 RULES OF ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH CHAPTER 420-5-9 FREESTANDING EMERGENCY DEPARTMENTS EFFECTIVE August 26, 2013 STATE OF ALABAMA DEPARTMENT OF PUBLIC HEALTH MONTGOMERY,
RULES OF ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH CHAPTER 420-5-9 FREESTANDING EMERGENCY DEPARTMENTS EFFECTIVE August 26, 2013 STATE OF ALABAMA DEPARTMENT OF PUBLIC HEALTH MONTGOMERY,
Blue Medicare Private-Fee-For-Service SM (PFFS) 2008 Medicare Advantage Terms and Conditions
 2008 Medicare Advantage Terms and Conditions") Blue Medicare Private-Fee-For-Service SM (PFFS) 2008 Medicare Advantage Terms and Conditions Medicare Advantage Table of Contents Page Plan Highlights...2 Provider Participation The Deeming Process...2
Blue Medicare Private-Fee-For-Service SM (PFFS) 2008 Medicare Advantage Terms and Conditions Medicare Advantage Table of Contents Page Plan Highlights...2 Provider Participation The Deeming Process...2
Mississippi Medicaid Diabetes Self-Management Training (DSMT) Provider Manual
 Provider Manual") Mississippi Medicaid Diabetes Self-Management Training (DSMT) Effective Date: May 1, 2015 Introduction: eqhealth Solutions Diabetes Self-Management Training Utilization Management Program includes prior
Mississippi Medicaid Diabetes Self-Management Training (DSMT) Effective Date: May 1, 2015 Introduction: eqhealth Solutions Diabetes Self-Management Training Utilization Management Program includes prior